public health approach to scaling-up art using who imai/imci tools dr sandy gove for the imai team...
TRANSCRIPT

Public health approach to scaling-up ART using WHO IMAI/IMCI tools
Dr Sandy Govefor the IMAI team and partners

G-8 in Gleneagles, Scotland in July 2005
they will “work to meet the financing needs for HIV/AIDS”
called on WHO, UNAIDS and other international bodies "…to develop and implement a package of HIV prevention, treatment and care," specifying a target of “as close as possible to universal access to treatment for all those who need it by 2010.”
Includes: Includes: WHO model essential package for WHO model essential package for HIV prevention, care, treatment & supportHIV prevention, care, treatment & support• List of interventionsList of interventions• Normative guidelinesNormative guidelines• Operational tools, capacity building materialsOperational tools, capacity building materials• Core information system: standardized patient Core information system: standardized patient monitoringmonitoring• Drug and diagnostic supply management Drug and diagnostic supply management

Universal access requires a massive effort. This calls for -
• a standardized and streamlined approach that can scale-up
• a decentralized and integrated public health approach
- in context multiple programmes and focal points with separate
activities, funding • a coherent programme of work for broad
implementation
- may span several national programmes and involve both government, NGO, FBO, private practitioner and workplace teams
Public health approach to scaling up HIV/AIDS services– address the health needs of the population
• Identify essential package of integrated HIV prevention, care, treatment and support interventions for health sector delivery
• Decentralization and integration of health services• Standardization and simplification of protocols and
procedures (to enable broad coverage)• Clinical team approach to patient management, including
task-shifting• Strengthening HIV prevention in health-care settings• Community mobilization to promote HIV testing and
prevention and prepare communities for treatment and adherence support
• Population-based HIV drug resistance and pharmacovigilance
• Free ART at the point of service delivery

Public health approach to scaling up HIV/AIDS services– address the health needs of the population
• Identify essential package of integrated HIV prevention, care, treatment and support interventions for health sector delivery
• Decentralization and integration of health services• Standardization and simplification of protocols and
procedures (to enable broad coverage)• Clinical team approach to patient management, including
task-shifting• Strengthening HIV prevention in health-care settings• Community mobilization to promote HIV testing and
prevention and prepare communities for treatment and adherence support
• Population-based HIV drug resistance and pharmacovigilance
• Free ART at the point of service delivery

WHO model essential package
Facility-based interventions
Interventions through
outreach to most at-risk populations
Community-based
interventions

Within the WHO model essential package for HIV prevention, care, and treatment
WHO operational tools for integrating interventions within the model essential package. These include:
IMAI integrated management of adolescent and adult illness
IMCI integrated management of childhood illness•acute and chronic HIV care•ART•prevention by PLHA•infant feeding counselling•special interventions for other most at-risk populations
IMPAC integrated management of pregnancy and childbirthPMTCT interventions integrated in
• antenatal care• labour and delivery• post-partum • newborn care

Standardization and simplification of protocols and procedures
WHO updated normative guidelines, based on expert groups
• Standardized first- and second-line ARV regimens• When to start, substitute, switch and stop• Updated ART and ARV prophylaxis regimens for PMTCT• Cotrimoxazole and PEP recommendations
IMAI/IMCI further simplifies and operationalizes these guidelines and provides tools to support implementation:
• management support• job aids and training for clinical teams and CHWs• strong follow-up after training- clinical mentoring,
supportive supervision• standard, simple patient monitoring system
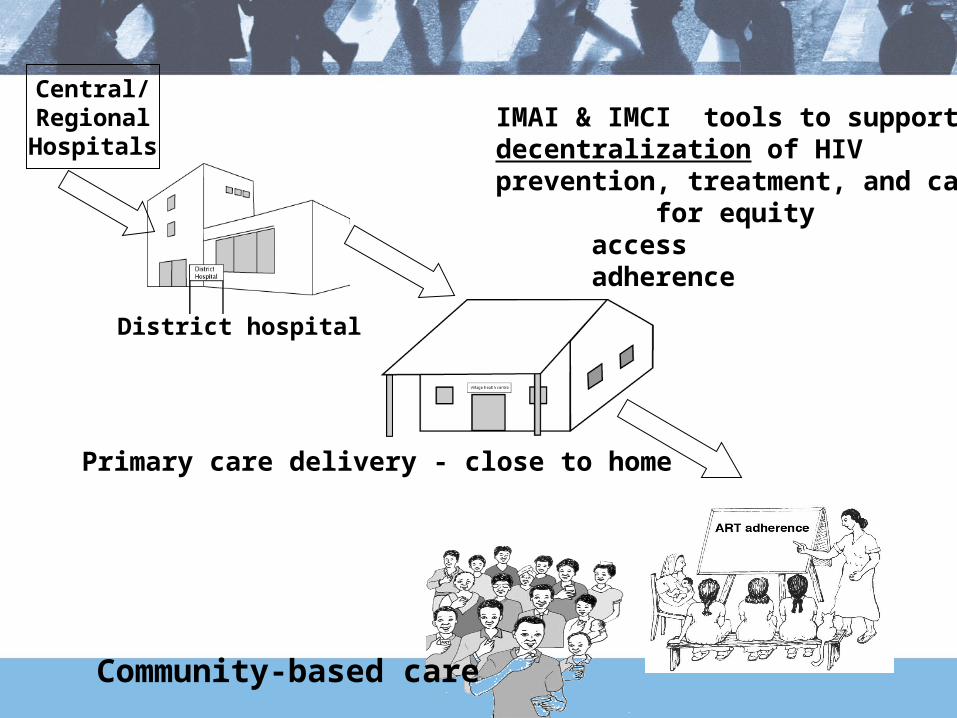
IMAI & IMCI tools to support decentralization of HIV prevention, treatment, and care- for equity
accessadherence
Primary care delivery - close to home
Community-based care
Central/RegionalHospitals
District hospital

Decentralization within a district network
Patient-centered: empower patients for self-management• Most symptoms; prevention by PLHA• When to seek care from health worker• Supported by treatment supporter/ CHW• In context community treatment literacy, prevention support
Nurse-led health centre teams (or clinical officers etc)• Acute and chronic HIV care and prevention• First-line ART in uncomplicated patients
Including initiation in children and pregnant women
Multipurpose district doctor or medical officer• Backs up health centre and outpatient primary care clinical
teams • Good distance communication• Regular on-site clinical mentoring
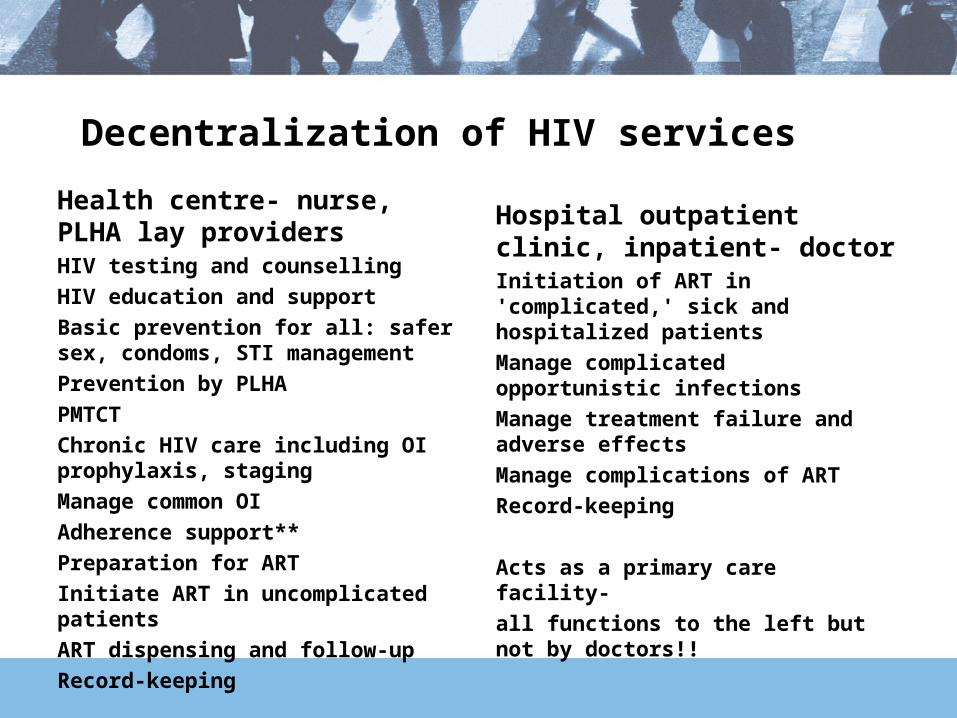
Decentralization of HIV services
Health centre- nurse, PLHA lay providersHIV testing and counsellingHIV education and support Basic prevention for all: safer sex, condoms, STI managementPrevention by PLHAPMTCTChronic HIV care including OI prophylaxis, stagingManage common OIAdherence support**Preparation for ARTInitiate ART in uncomplicated patients ART dispensing and follow-upRecord-keeping
Hospital outpatient clinic, inpatient- doctorInitiation of ART in 'complicated,' sick and hospitalized patientsManage complicated opportunistic infectionsManage treatment failure and adverse effectsManage complications of ARTRecord-keeping
Acts as a primary care facility-all functions to the left but not by doctors!!
Benefits to decentralization
Better support for deep commitment to good adherence • Support by community, CHW, other treatment supporters• Reduced transport time and costs for periodic visits
Lifetime chronic care is more feasible when close to home
More feasible to reach patients unlikely to travel to ART hospital:• Pregnant women• Children Seriously under-represented in those on ART

IntegrationIntegration of multiple interventions• Prevention, care and treatment integrated at point of
service• Coherent acute and chronic HIV case management
approach (integrated management of multi-system disease)
• HIV services integrated with management other diseases and conditions
HIV integrated within existing health system• Strengthens the health system• Assure delivery of basic care • Builds a district network

Why an integrated approach?
HTCPMTCT
HIV Care/ART
TB/HIVNational level
District level -
primary care facility
STI Targeted Interventions
Community Preparedness

Where does integration occur for an essential package?
Global and regionalAgreement on a priority set of interventions
NationalFlexible package for country adaptation
DistrictCollaboration between those responsible for
various HIV services, TB, maternal and child careClinical team
Coherent management guidelines Family approach to care
Community Treatment literacy and prevention promotion Strong links with health facility

Integrated approach for efficient scale-up of the essential package
One scale-up of HIV services at district level– Chronic HIV care, ART, T&C, PMTCT– All ages
All adult HIV care/ART sites should integrate:– PMTCT, other 'positive prevention' by PLHA– Paediatric HIV care/ ART
• Most rapid way to scale-up is integrated• Family-based care• Build on basic IMCI and paediatric referral care for
the most common conditions• Special emphasis on paediatric training needed

Integrated approach better serves HIV clients with other diseases (TB, malaria, STI) or conditions (pregnancy, IDU)
• Clinical co-management• Co-supervision by district teams (HIV, TB. MCH)• Co-sponsorship by national programmes- shared programme of work
Efficient management for patient (single clinic visit)and clinical team:• TB-HIV co-management• IDU-HIV co-management
– Special care for IDU integrated with HIV care and ART within primary care, opioid substitution therapy
• Pregnancy-HIV co-management for PMTCT• updated ART or ARV prophylaxis delivery integrated in
antenatal, L&D, post-partum and newborn care• train midwives and obstetricians in first-line ART and rapid
adherence preparation and support
IMAI/IMCI approach to scaling up integrated HIV prevention, care and treatment
Establish good chronic HIV care with clinical teams working within a district network
– district network model (facility-community hybrid)• hospital plus satellite health centres
plus community-based care– linked facility and community interventions– no parallel systems- HIV services are
integrated

Central, Regional,
University,
DISTRICT HOSPITAL
COMMUNITY
Clinical care- nurses, pharm techs; ART aid.Sometimes clinical/ health officer
Treatment supporters, health extension officers, other community health workers, peer support groups, CBOs
Doctors/health officers/ inpatient RN
Specialisedreferral
HEALTH CENTRE
Drugs, diagnostics, commodities, logistic support
National, Regional and District ART Management
Referral, B
ack-Referral; C
linical mentoring;
Supervision by District H
IV Managem
ent Team
Emphasis onstrongfacility-
community link
IMAI/IMCIIMAI/IMCI

IMAI/IMCI provide a flexible toolkit, for country adaptation
Fit to HIV epidemiology• Generalized or concentrated epidemic• Which populations are most at-risk
IDU, sex worker, MSMDiscordant seronegative partners of PLHA
Adapt to health system
Sociocultural adaptation
Not one size fits all!Other service delivery models
How can IMAI/IMCI be scaled up in the midst of a human resource crisis?
Emergency human resource strategy, supported by concrete tools for country adaptation:
• Task-shifting• PLHA workforce- to expand clinical team; as CHWs- trained
and paid • Prevention and care for health workers
– PEP, safe injections, universal precautions– Recognize and respond to burn-out– Clinical mentoring- attention to health worker needs, help with difficult
patients, career support• Rapid preparation of clinical teams with in-service training• Rapidly into pre-service training
Other WHO and partner efforts: retention schemes; special testing, care and treatment services for health workers (TTR)

Task-shifting
Specialized physiciansdoctorsDoctors health officers and nurses Nurses PLHA on clinical team:
ART aid (counsellor), triage/data clerkClinical team patient: self-management **Clinical team community- for case detection, treatment support, home-based care, simple monitoring
Build functional clinical teams linked to the community within a district system
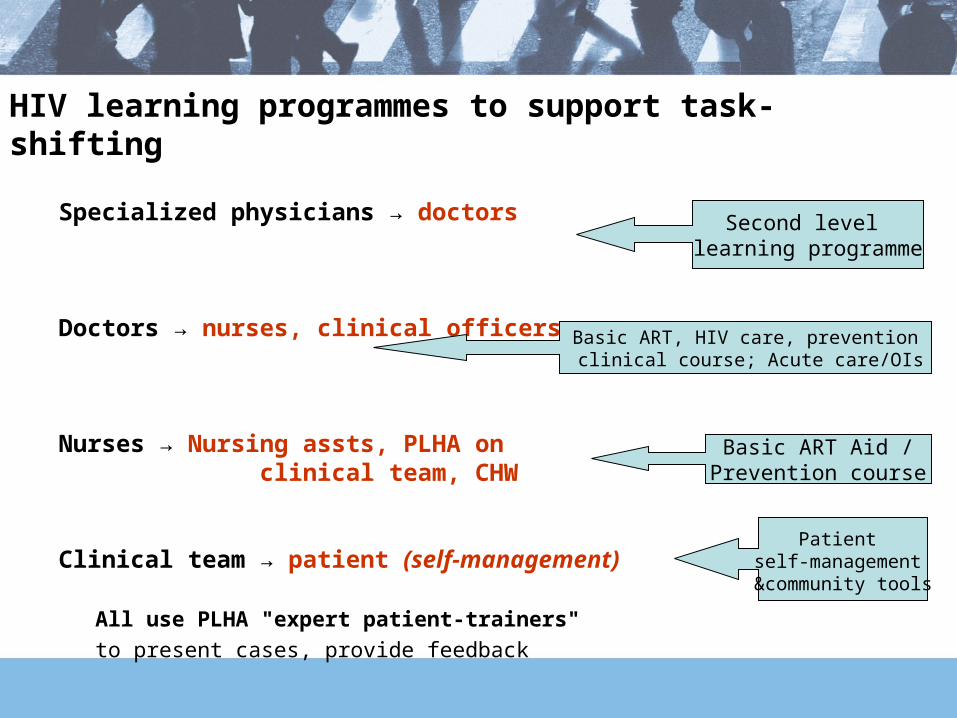
HIV learning programmes to support task-shifting
Specialized physicians → doctors
Doctors → nurses, clinical officers
Nurses → Nursing assts, PLHA on clinical team, CHW
Clinical team → patient (self-management)
Second level learning programme
Basic ART, HIV care, prevention clinical course; Acute care/OIs
Basic ART Aid /Prevention course
Patient self-management &community tools
All use PLHA "expert patient-trainers" to present cases, provide feedback

IMAI-IMCI: harmonized, modular short courses
TB-HIV
Week 1
Week 2,
follow-on
Chronic HIV Care with ART and Prevention
Acute Care:OI
IMCI-HIV
STI
PITC
Patient Monitoring
Reproductive choice/FP
Palliative care
PMTCT: infant feeding
PMTCT: antenatal/PP/L&D
Adolescents
Mental health
MSM, IDU, sex workers
Rapid scale-up is feasible
Ethiopia: 130 health centre clinical teams already prepared this year
Scale-up training is feasible • Continuous training over weeks
Challenges:• Volume clinical mentoring and supportive supervision
after training• Systematic linkages with community and outreach to
most at-risk populations• Drug and diagnostic supply management, logistics

Clinical mentoring: combine some individualized patient care with public health approach
For complicated patients: consultation, referral, on-site case review during on-site visits ,
Public health framework with more intensive clinical content for certain patients

Management support- HIV district coordinators course-
precedes clinical training
Planningintegratedservices
Targetedcommunity
interventions for
populationsat high risk
HIV care/ART
patientmonitoring
Capacitybuilding:
- clinical team:
- CHWs
Organizingpregnancy
relatedservices Antenatal,
PP/newbornPMTCTpatient
monitoring
Follow-upafter
training
Drug and diagnostic supply management

=
District hospital
HIV care/ART clinic
TB clinic:TB-HIV
Co-management
Antenatalclinic:
ART for PMTCT
=
Health centres:HIV care, ART, preventionTB-HIV co-managementPMTCT including ART
Decentralize, expand number of sitesDecentralize, expand number of sites

Standardized guidelines, training, management tools Share training, mentors, patient monitoring system within a district
Hospital
Health Centre
Health Centre
Health Centre
Health Centre
Health Post
Health Post
Health Post
Health Post
Health Post
Health Post
Health Post
Health Post
Health Post
Health Post
Health Post
Health Post
MOH
NGO or FBO
WorkplaceHIV
services
Scale up toward universal access is more feasible, sustainable
Privateproviders
Militaryservices

Challenges• Get patients on ART sooner:
• to reduce preART and early mortality on ART• easier for primary care teams to manage patient• prioritized use of CD4
• Inpatient testing and preparation/initiation of ART (severe wasting; persistent diarrhoea)- modify outpatient materials to prepare inpatient staff
• How to systematically scale-up home-based delivery through CHWs (linked with health facilities):– HIV testing and counselling, provide and link with services– more effective prevention with home delivery
• disclosure support, partner testing, risk reduction counselling especially for discordant couples
– cotrimoxazole, ART, TB, TB-ART treatment support