psychopharmacology of anxiety paul glue [email protected] april 2010
TRANSCRIPT


Objectives
• Definition
• (Re)Classification of anxiety
• Pharmacological theories of anxiety
• Pharmacology of antianxiety treatments– Are there better options on the horizon?

Anxiety is….• … a subjective experience of unpleasant anticipation,
accompanied by characteristic behavioural and physiological responses (e.g. avoidance, vigilance and arousal)
• Evolutionary value: to protect individuals from danger. • Present in most/?all higher animals – ? universal mechanism
by which organisms adapt to adverse conditions. • Symptoms:
– Cognitive (feelings of apprehension, fear)– Physical symptoms (shortness of breath, trembling, palpitations etc);– Endocrine and physiological changes
Spectrum
Normal Emotion Pathological Statesevere symptoms
& functional impairment

….and it’s very common
NZ Mental Health Survey 2006

DSM and anxietyClustering based on phenomenology; divorcing of depressive vs anxiety components

Factor Analysis of CIDI data from 10,641 participants in the Australian National Survey of Mental Health and Well-Being, a large-scale community
epidemiological survey of mental disorders

Where does anxiety arise in the brain?
• Multiple components• Amygdala (A) and insular cortex (B)
activation– key structures in emotional processing/integration
(Etkin Am J Psych 2007)

Drug treatments for anxiety
• Fast Onset-Effects noted within hours/days
-Generally act on amino acid systems (excitatory/inhibitory)
-Higher liability for tolerance, withdrawal on stopping Rx
• Delayed Onset-Effects noted after several weeks
-Act on modulatory central pathways (NE, 5HT)
-Lower liability for tolerance, withdrawal
Both Types-Effect size (mean symptom change) broadly similar for all agents; main
points of differentiation may be in speed of onset; types of side effects; pharmacodynamic interactions (e.g. alcohol); metabolic interactions (some SSRIs)

Available drugs
Experimental
Depression PTSDSADPDGAD OCD
Antidepressants (SSRIs, SNRIs, TCAs)
BDZs
Buspirone
Antiglutamate Rx
Subtype selective benzodiazepines
a2ds
anti-H1
clonidine
Overview of available drugs by DSM disorder
SlowOnset
FastOnset
quetiapine/antihistaminergic antipsychotics

Timecourse of SSRI and BDZ Effects in (e.g.) Panic Disorder
Pretreatment Treatment Withdrawal
Anx
iety
Sco
re
SSRI
Acute provocation by SSRIs
BDZs: faster onset of action
SSRIs: slower onset of actionBDZ
BDZs: high relapse rate
SSRIs: lowrelapse rates
~equivalentefficacy

Key Neurotransmitters in Anxiety
• Monoamines– Norepinephrine– Serotonin– Histamine
• GABA (gamma-aminobutyric acid)• Glutamate• Drugs affecting central excitatory
neurotransmitter release

Slow onset anti-anxiety drugs
• Antidepressants– Inhibit reuptake of serotonin
&/or norepinephrine
• Buspirone– Serotonin 1a partial agonist
• 6-8 weeks for full effect
• Antianxiety effects are presumably indirect - ? via BDNF
MAO
MAO
MAO
PRESYNAPTIC NEURON
POSTSYNAPTIC NEURON
SYNAPSE
Buspirone - autoreceptor antagonist
SSRIs/SNRIs – block transporter

Cortical Innervation – NE and 5HT Pathways
Ventral Tegmental AreaSubstantia Nigra
DOPAMINE
Common features: Cell bodies arising in upper brainstemRadiate to most cortical areasIntense arborization of dendritic terminals
Consistent with modulatory role
Substantia Nigra
NOREPINEPHRINE
DOPAMINE
Common features: Cell bodies arising in upper brainstemRadiate to most cortical areasIntense arborization of dendritic terminals
Consistent with modulatory role
Raphe Nuclei
SEROTONIN
NE
Common features: Cell bodies arising in upper brainstemRadiate to most cortical areasIntense arborization of dendritic terminals
Consistent with modulatory role on other cortical synapses

Pharmacological theories of anxiety • Serotonin theories (1): too much serotonin
– Observations: • increasing brain 5HT (acute SSRIs) increases anxiety• serotonin agonists (mCPP) are anxiogenic in panic disorder• 5HT1A, 2A and 3 receptor subtypes associated with anxiety in animals
– 5HT1A K/O mice highly fearful • drugs which decrease brain 5HT or 5HT partial agonists reduce anxiety
• Serotonin theories (2): too little serotonin : – Observations:
• 5HT depletion can increase sensitivity to anxiogenic probes • infusion of 5HT precursors are anxiolytic • endocrine responses to 5HT probes reduced in anxiety disorders• reduced 5HT in depression; depression and anxiety frequently comorbid• high variability in reported findings within and between anxiety disorders

– Observations: • increased NE firing/activity produces anxiety state
– stimulation of locus ceruleus; 2-antagonists (yohimbine/idazoxan)– plasma NE responses to stress higher in GAD vs controls (not all studies)
• inhibition of NE activity is anxiolytic (-blockers; 2-agonist clonidine)– Prazosin, clonidine effective against flashbacks in PTSD
• MHPG concs (NE metabolite) correlate with anxiety in panic d/o
– Hypothesis: • NE neuronal overactivity causes anxiety
– possibly due to reduced sensitivity of inhibitory (2) autoreceptor
– Problems: • not all panic disorder patients develop anxiety to NE probes
• highly variable results across different anxiety disorders (GAD, SP, PTSD)
• -blockers; 2-agonists are relatively weak anxiolytics
Pharmacological theories of anxiety - NE
agonist - inhibits cell firing
antagonist - increases cell firing
+
+
-
-
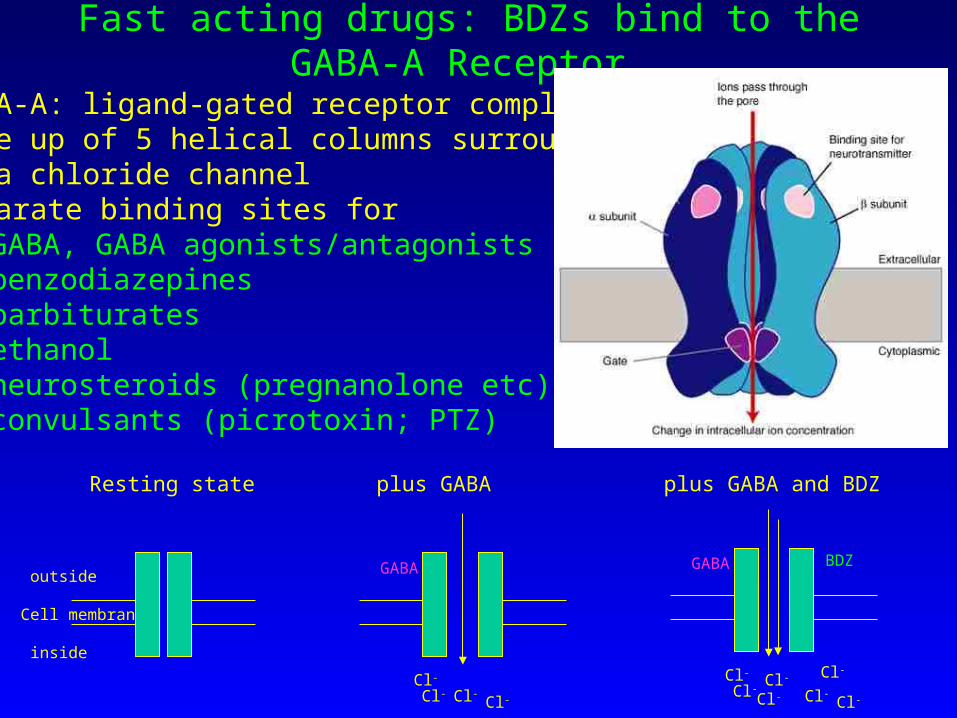
Fast acting drugs: BDZs bind to the GABA-A Receptor
•GABA-A: ligand-gated receptor complex•Made up of 5 helical columns surrounding a chloride channel•Separate binding sites for
•GABA, GABA agonists/antagonists •benzodiazepines•barbiturates•ethanol •neurosteroids (pregnanolone etc)•convulsants (picrotoxin; PTZ)
outside
Cell membrane
inside
Resting state plus GABA plus GABA and BDZ
GABA
Cl-Cl-
Cl-
Cl-
GABA
Cl-
Cl-
Cl-Cl-
Cl-
Cl- Cl-
BDZ

Benzodiazepine pharmacology
Partial Partial Inverse InverseAgonists Agonists Antagonists Agonists Agonists
Anxiolytic Neutral/ AnxiogenicAnticonvulsant no effect ConvulsantAmnestic PromnesticSedating Arousing
Diazepam Abecarnil Flumazenil FG7142LorazepamBretazenil DMCMClonazepam(all BDZs and Z-drugs in clinical use)

Pharmacological theories of Anxiety (1) - GABA theories
• Observations: • positive modulators of GABA-A receptor are anxiolytic (BDZs;
barbiturates; ethanol)
• negative modulators are anxiogenic (FG7142; metrazol) in normals
• flumazenil (BDZ antagonist) is anxiogenic in panic disorder but not in healthy controls; BDZs are less sedating/impairing in anxious patients than in controls
Agonists Antagonists Inverse -anxiolytic -neutral/no effect Agonists-diazepam, etc -flumazenil -anxiogenic
Normal
Panic Disorder
Agonists are Antagonistsless sedating are anxiogenic
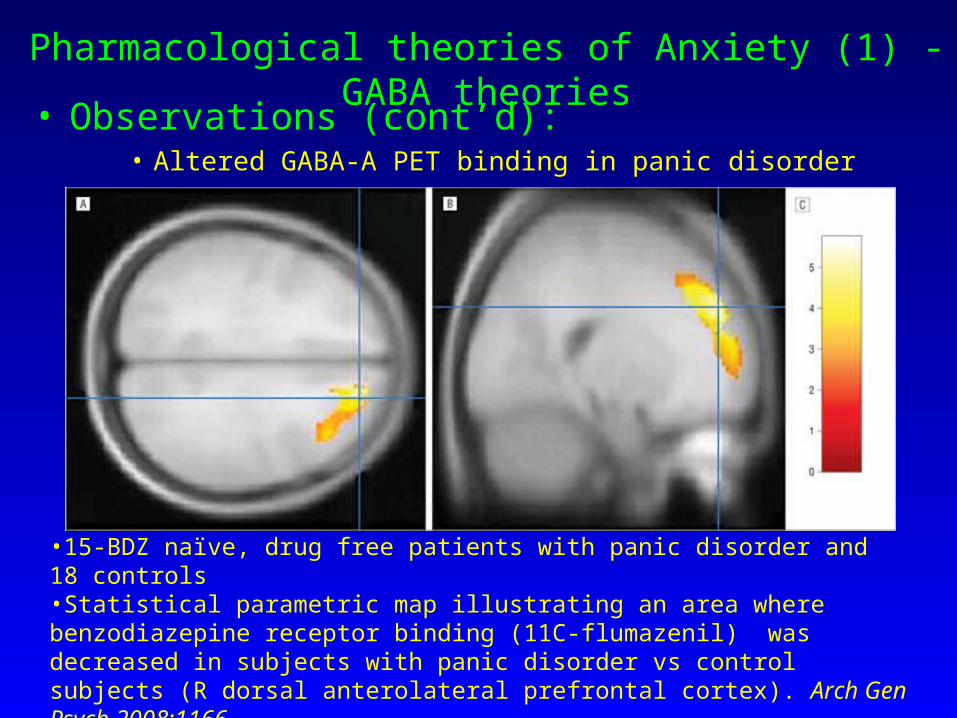
Pharmacological theories of Anxiety (1) - GABA theories• Observations (cont’d):
• Altered GABA-A PET binding in panic disorder
•15-BDZ naïve, drug free patients with panic disorder and 18 controls•Statistical parametric map illustrating an area where benzodiazepine receptor binding (11C-flumazenil) was decreased in subjects with panic disorder vs control subjects (R dorsal anterolateral prefrontal cortex). Arch Gen Psych 2008:1166

Can we make better benzodiazepines?

GABA-A subtype-selective benzodiazepines
- GABA-A receptor subtypes: most common type in the brain is a pentamer comprising 2 α's, 2 β's, and 1 γ (α2β2γ). Available BDZs are nonselective agonists.
- Selective agonists for:
> α1 subtype produce sedation and dependence
> α2 and α3 are anxiolytic
> α5 affect cognition and memory
- MK-0343: α2/α3 partial agonist - reduced effects on alertness, memory and postural stability in healthy volunteers vs lorazepam
- SL651498: full agonist at α2/3 subunits; partial agonist at α1 and α5 subunits
> neither drug yet tested in anxious patients – will they work??

α1 subunits and dependence liability:
GABA-A α1 subunit knockout mice show no tendency to increase consumption of midazolam compared with normal (wild type) mice Tan, Nature 2010, 463:769-774

Anxiety and Histamine
• Brain histamine neurons arise in tuberomammillary nucleus in the posterior hypothalamus. • Project throughout the nervous system• May stimulate the cerebral cortex either directly or
indirectly (5HT, ACh, galanin, GABA, substance P etc) • 4 receptors (H1-4) • Histamine is arousing/excitatory; increased release in
stressed animals; associated with anxiety related behaviours (no human data)

Antihistamines are effective anxiolytics
Generalized Anxiety Disorder– Antihistamines (hydroxyzine)
• 50mg/day; rapid onset; equivalent efficacy to buspirone, bromazepam
• No evidence of dependence, withdrawal• QT prolongation, delirium after OD
– Antipsychotic drugs (quetiapine, trifluoperazine) efficacious; rapid onset
• Much lower doses (~1/3-1/10) than those used for psychosis – presumably reflect antihistaminic effects
• Dose-response is unclear (50 - 150 - 300mg equivalent)
• No long term safety data
Quetiapine dose (mg/day)
0 50 100 150 200 250 300
-16
-14
-12
-10
-8
-6
-4
-2
0
Me
an
ch
an
ge
in
HA
M-A
sco
re
Glutamate and Anxiety• Glutamate is the most abundant transmitter in the CNS
– Fast, excitatory transmitter; receptors on almost all neurons. Transmitter in ~60% of neurons, esp cortex, limbic structures.
• Glutamate binds to 4 classes of receptor– three "ionotropic" receptor classes - ligand-gated ion channels which are
characterized by the different ligands that bind to them:• AMPA• kainic acid • N-methyl-D-aspartate or NMDA
– one G-protein coupled or "metabotropic" receptor class.• Both direct and indirect effects on neurotransmission
– Regulates release of many other neurotransmitters• Altered glutamate transmission linked with stress and anxiety
– Different pharmacological interventions with the glutamate system can influence behavioural responses in preclinical anxiety models
H2N
COOH COOH

LY354740
LY354740 in GAD• mGlu2/3 agonist (decreases release of excitatory AAs)• Study stopped early because of tox problems (seizures)
• LY354740 may be as effective as lorazepam 4-5mg/day, with a relatively rapid onset of action
• Too early to say if this approach will be available clinically
Neuropsychopharm 2008

Anxiety and Gabapentin/Pregabalin
III
III
IV
1extracellular
II-III
2
Binding siteBinding site
cytoplasmic
- Drugs effective in epilepsy, neuropathic pain and GAD. Do not work in MDD.- Bind to the 2- subunit of voltage-gated calcium channels and inhibit release of glutamate, substance P, NE, etc.
GABA
Gabapentin

Pregabalin = Alprazolam > placebo in GAD
-18
-16
-14
-12
-10
-8
-6
-4
-2
0
0 1 2 3 4 5
Mea
n c
han
ge
fro
m b
asel
ine
Placebo (n=85)
Pregabalin 300 mg/day (n=89)
Pregabalin 450mg/day (n=87)
Pregabalin 600mg/day (n=85)
Alprazolam 1.5mg/day (n=88)
Mean baseline HAM-A score = 25.
Rickels et al. Arch Gen Psychiatry. 2005;62:1022-1030.
Week EP
Pregabalin dose (mg/day)
0 100 200 300 400 500 600
Res
pond
er r
ate
(%)
0
10
20
30
40
50
60
70
…but no clear dose-response in GAD

Non-Pharmacological Treatments
• Simple behavioural methods (breathing; relaxation) effective in mild anxiety
• Certain psychotherapies (e.g. CBT) are as effective as SSRIs/TCAs in panic disorder and GAD– no clear advantage with combined CBT and drug Rx
• Behaviour therapy is as effective as SSRIs/TCAs in OCD
• Ideal combination(s) of drug therapy and psychological therapies not yet determined

The future for anxiety drug treatment• Are current diagnostic categories tenable?
…and will this be reflected in new DSM/ICD updates?
• What is appropriate/best polypharmacy?• How to best manage real-world patients?• Alternatives to BDZs as fast-acting drugs–
antihistamines; low dose quetiapine; clonidine• Best new drug prospects for 2015-2020
– Subtype-selective BDZs • (less sedation, amnesia; maybe lower dependence liability; same
efficacy)
– mGlu2/3 agonists
• Lots of recent drug failures as well– CRF1 antagonists; NK1 antagonists; CCK antagonists….