psychiatry dr n fernando 2 nd may 2006. content psychiatric history mental state examination assess...
TRANSCRIPT

PsychiatryPsychiatry
Dr N FernandoDr N Fernando
22ndnd May 2006 May 2006

ContentContent
• Psychiatric history• Mental state examination• Assess suicide risk• Multi-Disciplinary Team (MDT) )• Community Psychiatric Nurse (CPN)) Understand• Psychiatric Social Workers ) their roles• Occupational Therapists (OT) )• Impact of mental illness on relatives• Schizophrenia )• Affective disorders )• Anxiety ) Clinical features• Dementia ) &• Delerium ) their management • Eating Disorders )• Alcohol Misuse )

Psychiatric HistoryPsychiatric History
• A story……Chronological……detailed
• From before birth – Family history
• ….through birth & early adulthood – Personal, Educational, Psychosexual, Work history
• ….through life difficulties – Substance misuse, forensic
• ….status before the current episode – PMH, PSH, PPH, pre-morbid personality– Medications, allergies, social circumstances
• ….to the current presentation – PC & HPC

Psychiatric HistoryPsychiatric History
• PC/HPC• PMH/PSH/PPH• MEDS/ALLERGIES• Personal History
– Early– Schooling & Academic achievements– Sexual history & preferences/ Work history
• Substance use incl. alcohol, caffeine, nicotine• Forensic history• Family History• Current social circumstances• Pre-morbid personality

Mental State ExaminationMental State Examination
• Appearance & Behaviour• Speech• Mood (s) & (o)
• Thoughts – Disorders of form, content, flow– Deliberate self harm/suicidality
• Perceptions• Cognition
– Conscious level Orientation A&CMemory - STM,LTM Abstract thinking
• Insight
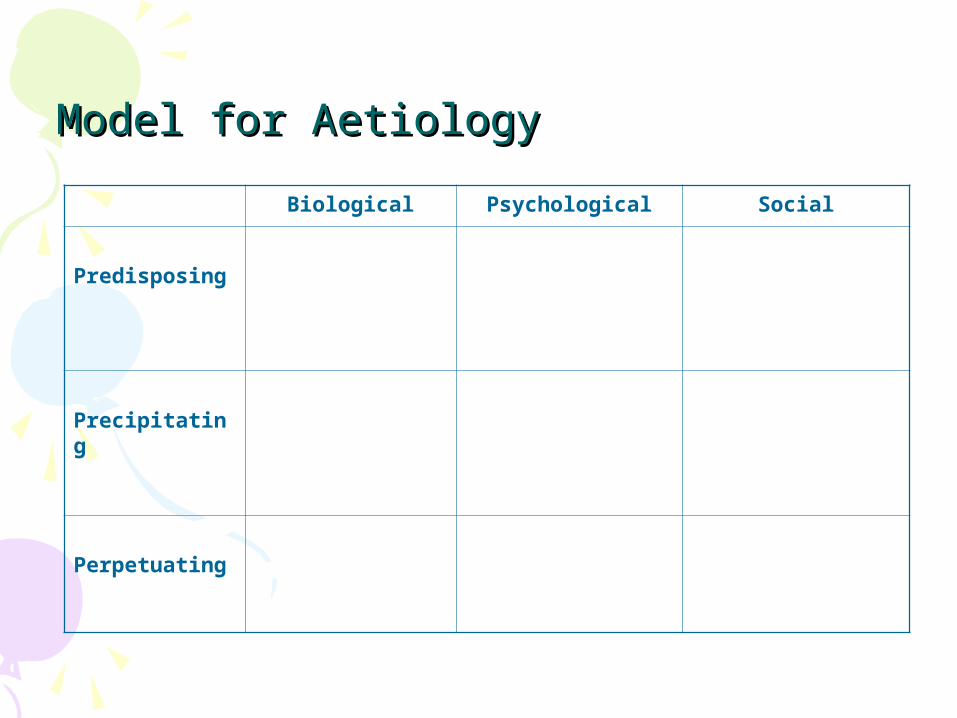
Model for AetiologyModel for Aetiology
Biological Psychological Social
Predisposing
Precipitating
Perpetuating

Model for AetiologyModel for Aetiology
Biological Psychological Social
Predisposing
Genetic LoadingGenderBrain Injury/LDPhysical IllnessSubstance MisusePrevious Psychiatric Hx
Personality factorsParental modellingCognitive factors – low IQ, Beck’s triad, cognitive distortions, locus of control
High EEParental discordPoor socio-economic factorsIsolationDebts
Precipitating
Non-complianceSubstance misusePhysical illness/traumaIatrogenic – drugsHormonal – MenopausePsychiatric illness
Poor insightAssault/conflictLoss of loved objectSingle word/comment
Significant life eventsIsolationLack of supportIncreasing stressorsChange of environment
Perpetuating
Brain InjuryNon-complianceSubstance misusePhysical illnessGenetic loading
Personality factorsCognitive factorsPoor insightAnxietyReduced motivation
IsolationPoor socio-economic factorsHigh EEFamily discord
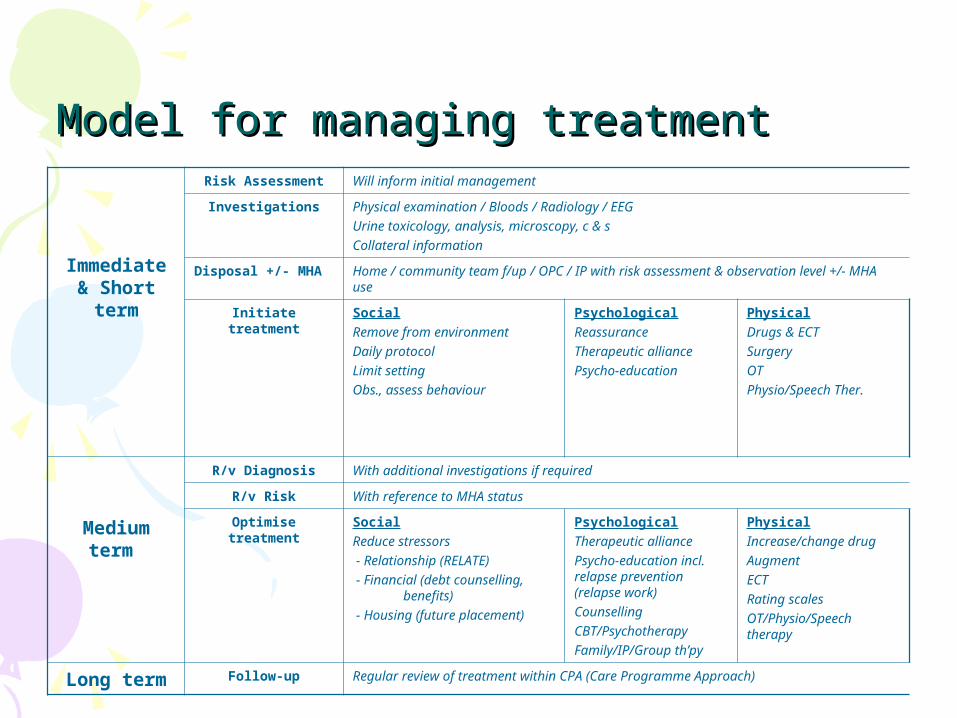
Model for managing treatmentModel for managing treatment
Immediate & Short
term
Risk Assessment Will inform initial management
Investigations Physical examination / Bloods / Radiology / EEGUrine toxicology, analysis, microscopy, c & sCollateral information
Disposal +/- MHA Home / community team f/up / OPC / IP with risk assessment & observation level +/- MHA use
Initiate treatment SocialRemove from environmentDaily protocolLimit settingObs., assess behaviour
PsychologicalReassuranceTherapeutic alliancePsycho-education
PhysicalDrugs & ECTSurgeryOTPhysio/Speech Ther.
Medium term
R/v Diagnosis With additional investigations if required
R/v Risk With reference to MHA status
Optimise treatment
SocialReduce stressors - Relationship (RELATE) - Financial (debt counselling,
benefits) - Housing (future placement)
PsychologicalTherapeutic alliancePsycho-education incl. relapse prevention (relapse work)CounsellingCBT/PsychotherapyFamily/IP/Group th’py
PhysicalIncrease/change drugAugmentECTRating scalesOT/Physio/Speech therapy
Long term Follow-up Regular review of treatment within CPA (Care Programme Approach)

Model for managing treatmentModel for managing treatment
Summary
• Talk, negotiate, dialog (therapeutic alliance, psychoeducation)• Informal formal (?MHA use)• Period of observation (best before initiating treatment)• Medication – if required
– Least toxic, least dose, shortest length (as possible)• Talking therapies
– Counselling, CBT, psychotherapy, IP therapy, Group • Follow up
– Review, optimise therapy– Aftercare - CPA (Care Programme Approach)– maintain therapeutic alliance, psychoeducation

Prognostic factorsPrognostic factorsGood Poor
Immediate
•Acute Onset•Family support•Rapid de-escalation of symptoms/signs•Older age group generally
•Poor insight•Physical illness•Poor response to past/present tx•Substance misuse
Longer term
•Good response to treatment•Good insight & engagement with services•Effective psycho-education
•Younger age group generally•Poor insight•Ongoing substance use•Disengagement with services•Chronic psychiatric illnesses•Physical illness

Multi-Disciplinary Team work (MDT)Multi-Disciplinary Team work (MDT)
• Basis of psychiatric diagnosis, treatment and management• Consensual decisions (most times)• Good communication skills• Important to include patient & carer in decisions• All professional have stake in patient care
– Doctors, ward staff, OT, psychologists, pharmacists, community staff, any other therapists working with patient
– Their concerns and views to be considered & documented• Final decision – ALL to be in agreement (if possible) thereby
sharing risk and responsibility• Care plan – jointly appraised, agreed and maintained• Medical staff have overall responsibility (RMO status)
– This is currently under review by DHS

Community Psychiatric Nurses (CPN)Community Psychiatric Nurses (CPN)
• Work within community teams• ‘Key-worker’ to coordinate care & liaise with RMO/wards,etc• Have experience of dealing with mental illness• Have good communication & organisation skills• Ideally have psycho-social skills • Work with challenging patients & their families including
psychoeducation• Have a good understanding of relapse signatures, particular
stressors and behaviour patterns of their clients• Understanding of other services that may benefit patient &
refer appropriately• Have confidence in managing & advising reg. medications• Give depot medications

Psychiatric Social WorkersPsychiatric Social Workers
• Experience in social work• Emphasis on mental health issues & impact on social
services• Appropriate use of services & benefits• Social history of patient• ASW work – Approved Social Worker (Section 12 approved)
– Coordinating mental health act assessments – Makes application for detention under MHA 1983– Aware of social circumstances that may impact on
presentation in community at time of MH assessment– Be aware of next of kin & their views– At MHA no other disposal apart from hospital admission– Be aware of changes in mental health law – Furnish reports to tribunals – patients under MHA 1983

Occupational Therapists (OT)Occupational Therapists (OT)
• Work within hospital or community• Have a wide range of OT background skills• Good communication & psycho-social skills to work with
highly challenging group of patients• Understanding of mental health & impact on daily
functioning• Understand medications and its similar impact• Assess patient’s level of activity and living skills
– ADL assessment – Activities of Daily Living– Compare with patients needs/desires and abilities
• Set up graduated activities to improve patient’s level of functioning in a manageable and sustainable programme
• Advocate for patient if required (reg. their functioning)

Impact of mental health on relativesImpact of mental health on relatives
• Can be significant & prolonged• Stressful;
– Concerns that they or their children may be affected– Dealing with someone not in touch with reality – constantly– Dealing with someone constantly breaching limits– Dealing with someone becoming ill & feeling unable to help– Dealing with disorganisation & aggression– Dealing with services not able to respond fast enough– Dealing with poor insight from affected relative & meds need
• Concern for relative– Can be excessive High expressed emotion (EE)
• Increase risk of physical illness & mental illness– Stress related & depression (Carer assessment useful)

Delusions – DefinitionDelusions – Definition
• Belief which is firmly held despite evidence to the contrary which is out with their religious, social and cultural experience
• Different from ‘overvalued idea’
• Many themes– Paranoid, Persecutory, Grandiose, Delusions of
reference, Guilt or worthlessness, Hypochondriachal, Religious, Sexual, etc…

Hallucinations - DefinitionHallucinations - Definition
• Perception in the absence of stimuli
• Can be normal experience – hypnogogic/hymnopompic
• Based on different senses– Auditory (2nd, 3rd person, running commentary, thought
echo)– Visual (commonly underlying organic condition)– Gustatory– Olfactory– Somatic (tactile & deep)

SchizophreniaSchizophrenia
• Fundamental & characteristic distortions of thinking & perception• Inappropriate or blunted affect• Delusions (secondary) & Perplexity common• Onset Acute or gradual• M=F - Later onset in women• Genetic component
– 1 parent affected 13% risk in kids– Both parents 46% risk in kids– 1 sibling affected 10% in other siblings– MZ twins 48% concordance
• Life events & expressed emotions associated with relapses• CT changes – predate illness
– Smaller temporal lobes by 15-20% & Enlarged ventricles– PET scans functional disturbances in frontal & temporal structures
• Cognitive changes – late feature generally

SchizophreniaSchizophrenia
First rank symptoms– 3rd person auditory hallucinations– Running commentary– Thought echo– Made feelings )– Made impulses )– Made actions ) Passivity– Thought insertion ) ) Phenomena– Thought withdrawal ) Thought )– Thought broadcasting ) Alienation )– Somatic passivity )– Delusional perception

SchizophreniaSchizophrenia
Definition: ICD 10 criteria– At least 1 month duration of symptoms– 1 clear CORE symptom or >= 2 if less clear or >=2 from Secondary group
CORE group - Thought echo, alienationDelusions of passivity, Delusional
perception3rd person, running commentarypersistent delusions
Secondary group -Persistent hallucinations – any modalityThought block/neologismsCatatonic behaviour/ Negative
symptoms
Significant & Consistent change in overall quality

Schizophrenia - TypesSchizophrenia - Types
• Paranoid– Commonest, hallucinations +/- delusions prominent
• Hebephrenic– starts bet 15-25yrs, poor prog.– Affective changes, irresponsible, inappropriate behaviour
• Catatonic– Prominent psychomotor disturbance, rarely seen in west
• Post Schizophrenic depression– Negative symptoms prominent usually, ^risk of suicide
• Residual Schizophrenia– At least one previous psychotic episode– Period of 1 year, where +ve -ve symptoms
• Simple Schizophrenia– Uncommon, insiduous and progressive– No previous psychotic episode, vagrancy may occur

SchizophreniaSchizophrenia
Negative symptoms
6 A’s
- Attention reduced- Avolition- Anhedonia- Affective blunting- Apathy- Alogia

Schizophrenia - managementSchizophrenia - management
Immediate & Short
term
Risk Assessment Risk to themselves, others, or risk of further deterioration of mental health
Investigations Physical examination / Bloods Urine toxicologyCollateral information
Disposal +/- MHA Home / community team f/up / OPC / IP with risk assessment & observation level +/- MHA use
Initiate treatment SocialRemove from environmentDaily protocolLimit settingObs., assess behaviour
PsychologicalReassuranceTherapeutic alliancePsycho-education
PhysicalAntipsychotic medicationsAnxiolyticsSleeping tablets
Medium term
R/v Diagnosis With additional investigations if required
R/v Risk With reference to MHA status
Optimise treatment
SocialReduce stressors - Relationship (RELATE) - Financial (debt counselling,
benefits) - Housing (future placement)
PsychologicalTherapeutic alliancePsycho-education incl. relapse prevention (relapse work)CounsellingCBTRefer CMHT if approp.
PhysicalIncrease/change drug
Augment
OT
Long term Follow-up Regular review of treatment within CPA (Care Programme Approach)

Schizophrenia - ManagementSchizophrenia - Management
Summary
Therapeutic allianceMHA use if appropriateMDT decisionsReduce stressorsSupport – psychological, psychoeducation, reduce EE
Drugs: AntipsychoticsAnxiolyticsAntidepressantsHypnotics (to aid sleep)

Schizophrenia - AntipsychoticsSchizophrenia - Antipsychotics
Summary
Therapeutic allianceMost appropriate choice – clinical basisAtypicals 1st line in new cases (NICE)
- Start low and increase as tolerated- Raise dose to therapeutic level- If no response in 4-6 weeks, consider change, seek help- Watch for side-effects
Side-effects;- Drowsiness, wt gain ) Reduce dose, another- reduced blood pressure ) drug to counter effects,- EPSE ) change to another- Sexual dysfunction)
Non-compliance- Consider depot medication
Treatment resistant (inadequate response to two a/p)- Clozaril (regular FBC, co-ordinated via CPMS – Clozaril Patient Monitoring Service)
Affective DisordersAffective Disorders
• Depression• Bipolar Affective Disorder (BPAD)• Hypomania• Mania• Persistent Mood Disorders
– Cyclothymia– Dysthymia

DepressionDepression
• Definition: ICD – 10 requirements– 2/52 duration of symptoms– 3 Core symptoms – Mood, Anhedonia, Anergia– 7 additional Sx.
• A&C worthlessness appetite• DSH acts hopelessness sleep self esteem
• Mild (at least 2 core + 2 other)– Distressed but able to function with ordinary work
• Moderate (at least 2 core + 3 other)– Will have considerable difficulty c/t with work
• Severe (All 3 core + 4 other or more)– Suicide a distinct risk & unlikely to continue with work– Need to look for psychotic symptoms

Depression - ManagementDepression - Management
Immediate & Short
term
Risk Assessment Risk to themselves, others, or risk of further deterioration of mental health
Investigations Physical examination / Bloods +/- RadiologyUrine toxicology, C&SCollateral information
Disposal +/- MHA Home / community team f/up / OPC / IP with risk assessment & observation level +/- MHA use
Initiate treatment SocialRemove from environmentDaily protocolObserve Mental state
PsychologicalReassuranceTherapeutic alliancePsycho-education
PhysicalAntidepressantAnxiolyticNight sedation
Medium term
R/v Diagnosis With additional investigations if required
R/v Risk With reference to MHA status
Optimise treatment
SocialReduce stressors - Relationship (RELATE) - Financial (debt counselling,
benefits) - Housing (future placement)
PsychologicalTherapeutic alliancePsycho-education incl. relapse prevention (relapse work)CounsellingCBT/psychotherapyRefer CMHT if required
PhysicalIncrease/change drugAugmentECTOccupational therapist
Long term Follow-up Regular review of treatment within CPA (Care Programme Approach)

Depression – Use of AntidepressantsDepression – Use of Antidepressants
• Discuss choice of drug with the patient– Therapeutic effects, adverse effects, discontinuation effects
• Start ANTIDEPRESSANTS– Titrate to recognised therapeutic dose– Assess efficacy over 4-6 weeks– Continue for 4-6 months at full treatment dose
• Consider long-term treatment in recurrent depression
• If no effect– Increase dose (to maximum dose if tolerated) & assess over 2/52– Try another antidepressant from another class
• Titrate as above
– Little improvement Treatments for refractory depression

Bipolar Affective Disorder (BPAD)Bipolar Affective Disorder (BPAD)
• >=2 episodes of mood/activity changes• Recovery complete between episodes• M = F• Usually abrupt onset of mania• Manic episode – last median of 4 months• Depressive episode – last median of 6 months• Often follow stressful life events• First episode occur at any age (Most freq bet 20-29 years)• Increasing age Increased frequency & length of episodes• 1-2% of population at some point in their lives• Genetic predisposition
– BPAD 11% risk of Depression (UP) in 1st degree relatives– BPAD 8% risk of BPAD in 1st degree relatives
• Morbidity & mortality is HIGH suicide/accidental deaths/concurrent illnesses

Bipolar Affective Disorder (BPAD)Bipolar Affective Disorder (BPAD)
Features
Elated moodGrandiose ideas & inflated self esteemIncreased energy & activityFlight of ideasPressure of speechIncreased libidoimpaired judgement & impulsive behaviourReduced need for sleepIncreased creativityImpaired attention & concentrationPsychotic symptoms
Bipolar Affective Disorder (BPAD)Bipolar Affective Disorder (BPAD)
Diagnosis
>=2 episodesAt least one should be maniaManic episode >= 1/52Depression >= 2/52
Rapid cycling = 4 or more episodes / year
Severity
Hypomania Mania Mania with psychotic features

Bipolar Affective Disorder (BPAD)Bipolar Affective Disorder (BPAD)
Hypomania- Increased mood & activity for at least a few days- interfere with work/social activity
Mania- Increased mood & activity for at least a week- Disrupt work/social activity
Mania with psychotic features- As above with psychotic features- most severe form

Bipolar Affective Disorder (BPAD)Bipolar Affective Disorder (BPAD)
MANAGEMENT
- Same as for depression & table- Important to gain therapeutic alliance- Consider admission +/- use of MHA- Assess RISKS carefully and address to reduce impact- Commence drug treatment if appropriate - Sedation/mood stabilisation (Lithium)/Antipsychotic
- Antidepressant (watch for rebound mania)- ECT
- Talking therapy- CBT based- Psychoeducation including Relapse signature work
- Social work involvement- reduce stressors – finances/housing, etc
- Follow-up review (CMHT & key-worker allocation)- Optimise social skills
- employment, self esteem, ADLs, etc..

Persistent Mood DisordersPersistent Mood Disorders
Cyclothymia
Persistent instability of moodOnset in early life (teens)Chronic courseNot severe to fulfill BPAD (Episodes <1/52 mania, <2/52 depres.)
Dysthymia
Chronic lowness of mood, prolonged periods of timeusually able to cope with ADLs & demandsBegins in early adulthoodLast for several yearsCan be associated with bereavement

Anxiety DisordersAnxiety Disorders
- Agoraphobia- Social phobia- Specific phobia- Panic Disorder- GAD- OCD- PTSD

AgoraphobiaAgoraphobia
Features- Most incapacitating of phobic disorders
- F:M = 3:1- Onset early in adult life (15-35 yrs)- Autonomic/psychological symptoms secondary to anxiety- terrified of collapse/left helpless in public- Anxiety generally restricted to; crowds/public places/travelling alone/travelling away from home. - Avoidance of phobic situation is prominent, can become housebound- presence of other disorders depression, obsessional symptoms, panic
Management- Ongoing assessment- Psychoeducation- CBT – Work with cognitions (homework), Graded exposure with relaxation- Graded activity - Drugs: SSRIs

Social PhobiaSocial Phobia
Features- 8% of all phobias- Centred around FEAR OF SCRUTINY by others- Lead to avoidance of social situation- Fear of vomiting in public- M = F- Associated with low self-esteem & fear of criticism- May present with blushing/hand tremor/nausea/urgency- Diagnosis:
- Anxiety cause of symptoms & restricted to certain situations- Avoidance of phobic situation
Management- Ongoing assessment- Psychoeducation- CBT – Work with cognitions (homework), Graded exposure with
relaxation- Drugs: SSRIs

Specific phobiasSpecific phobias
Features- restricted to highly specific situations- persistent irrational fear of object- contact with this immediate anxiety response- Avoidance of object- Fear/avoidance/distress interfere with individual’s life- Fear is recognised as being irrational/excessive- start in childhood/early adulthood
Management- Ongoing assessment- Psychoeducation- CBT – Graded exposure with relaxation- Drugs: SSRIs

Panic DisorderPanic Disorder
Features- Recurrent anxiety attacks, can be severe (panic)- Unpredictable & sudden onset- Almost always due to fear of dying/losing control/going mad- Attacks last for minutes only- 20% adults at least once in life; 2% in 1 yr freq to get P.D. diagnosis- Onset mid 20’s, 1st panic attack in late teens- Panic attack: Increase fear autonomic symptoms hurried exit
If this occurs in a situation avoid situation - Diagnosis:
- Panic attacks not in background of another disorder- Several severe autonomic attacks in last 1/12
- No objective danger, not only in specific circumstances, relatively free from anxiety between attacks
Management- Ongoing assessment- Psychoeducation- CBT – Recognise early warning signs, Relaxation, challenge avoidance- Hyperventillation can induce panic in vitro (useful in training)- (SSRIs)

Generalised Anxiety Disorder (GAD)Generalised Anxiety Disorder (GAD)
Features- Essential feature is anxiety, which is generalised, persistent and not restricted to any situation (‘free floating’)- +/- somatic symptoms- F > M, Variable course- Often related to chronic environmental stress- Diagnosis:
- Primary symptom of anxiety (most days, for weeks/months)- To include apprehension, motor tension, autonomic overactivity
Management- Ongoing assessment- Psychoeducation (Avoid caffeine)- CBT: Relaxation, Graded activity, assertiveness training- Drugs: Amitriptyline, Venlafaxine, Buspirone, Clonidine
Benzodiazepines – NOT advocated, can be used for short course- Yoga

Obsessive Compulsive Disorder (OCD)Obsessive Compulsive Disorder (OCD)
Features- Essential features Obsessive thoughts +/- Compulsive acts- Close relationship with depressive features- F = M- Prominent Anankastic features in personality- Onset childhood/early adulthood- Family history of OCD/Tourette Syndrome- Underlying the act is FEAR (of dirt, etc…) Ritual is way of reducing fear- Diagnosis: Obsessional thoughts +/- Compulsive acts most days 2/52
Be distressing/interfere with activitiesObsessional symptoms – recognised as own, resisted unsuccessfully, NOT pleasurable, repetitive (impulses & thoughts)Compulsive acts – stereotyped behaviour, repeated, not enjoyable, no useful task completed, attempts to resist, recognised as pointless, seen as preventing an unlikely event (‘magical undoing’)
Management- Ongoing assessment- Psychoeducation, distraction techniques (thought stopping)- CBT: Work with cognitions (homework), Exposure & response prevention- Drugs: SSRIs (at higher dose)
Clomipramine (past, can still use) BEST effects when combined with CBT

Post Traumatic Stress Disorder (PTSD)Post Traumatic Stress Disorder (PTSD)
Features- Delayed/protracted response to stressful situations- Excessive use of alcohol +/- drugs in majority- Recovery expected in majority; Small number chronic personality change- Diagnosis: - Within 6/12 (usually)
- Traumatic, exceptional event- Repetitive intrusive recollections, flashbacks OR Re-enactment of events in memory/imagery/dreams (nightmares)
Other Sx - Emotional numbing- Autonomic symptoms – hyperarousal, hypervigilence (startle reaction),
insomnia- Anxiety & depression – suicidal ideation- ‘Cues’ Increase arousal Avoidance of such cues
Management- Ongoing assessment- Psychoeducation- CBT: Aim of tx. Remove fear of situation/position
Vitro: Graded exposure (in imagery) & relaxation Vivo: Systematic desensitisation with relaxation
- Drugs: SSRIs (at higher dose)

DementiaDementia
Features- SYNDROME due to disease of brain- Chronic/progressive- Disturbance of multiple higher cortical function- Consciousness NOT clouded- Impaired cognition- Deterioration of emotional control/social behaviour/motivation- Memory - Affects registration, storage, retrieval of new information
- Previously learned material may not be affected- Thinking - Processing of information is affected, difficult to attend
more than one stimulus at a time- Reduced reasoning capacity- Reduced flow of ideas
- Diagnosis:- Primary Evidence of decline in both MEMORY and THINKING which is enough to affect ADLs- Clear consciousness- For at least 6/12 (for confident diagnosis)

DementiaDementia
Types
Alzheimer'sVascularLewy Body HIVParkinson’sPick’sHuntington’sCreutzfeldt-JakobNormal Pressure Hydrocephalus

Dementia – Alzheimer’s DiseaseDementia – Alzheimer’s Disease
Features- Primary degenerative brain disease- Usually in later life, but can occur earlier- Early onset +ve FH, rapid course, prominent features of temporal and
parietal lobe dysfunction - Down’s Syndrome increased risk of AD- May be associated with vascular dementia- Memory problem is main feature- 1% at 65y, 10% at 80y, 40% at 90y (Rule: doubling every 5 years)- Pathology: Marked reduction in population of neurones
Neurofibrillary tanglesNeuritic plaquesGranullovacuolar bodiesMarked reduction in enzyme choline acetyl-transferase
- Diagnosis:- Presence of dementia (see previous slide for guide)- Insidious onset & slow deterioration- Absence of features of systemic & other brain disease- Absence of sudden onset

DementiaDementia
Reversible causes of dementia
These need to be excluded
HypothyroidismHypercalcaemiaVitamin B12 deficiencyNiacin Deficiency (Folate)Normal pressure hydrocephalus Subdural haematomaSyphilitic
Dementia - ManagementDementia - Management
• Refer Memory Clinic• Differentiate from delerium/depression/paranoid disorders• Look for treatable causes (previous slide)• Physical investigations
– FBC/U&E/LFT/TFT/Gluc/VitB12&Folate/Syphilis serology/Ca&Phos/ESR– Urine analysis & culture– ECG & CXR– CT Brain
• Mini Mental State Examination MMSE (Memory Clinic)• Treatment; Treatable causes
Behavioural changes – non-pharmacological Drugs: Antidepressants
AnxiolyticsAntipsychoticsAnti-cholinesterase Inhibitors (Memory Clinic)
• Vascular Dementia – Reduce riskManage BPLow dose aspirin (note bleeding potential)Surgical treatment of carotid stenosis

Dementia - MMSEDementia - MMSE
• Yr, month, DoW, date, season 5• Place, Floor, city, county, country 5• 3 Objects to remember 3• WORLD backwards, serial 7’s 5• Recall 3 objects 3• Pen, watch – identify 2• Repeat phrase ‘No ifs ands or buts’ 1• 3 stage command 3• Read & follow instruction 1• Write sentence (verb & noun) 1• Interlocking pentagons 1
Total 30
26-30 normal, 20-25 mild, 13-20 moderate, <12 severe (These figures are guidelines only, correlate with clinical picture)

Acute Confusional State (Delerium)Acute Confusional State (Delerium)
Features- Rapid onset- Can be diurnally fluctuating- Any age, most common > 60y- Transient, fluctuating intensity- most recover within 4/52- BUT can last for 6/12 esp. with chronic liver disease, Carcinoma, SBE- Diagnosis: Impairment of consciousness & attention
Global disturbance of cognition- Impairment of recent memory & recall- Disorientation in time, severely of place & person- Perceptual distortions; illusions, hallucinations esp.
visual- +/- transient delusions
Psychomotor disturbances – hypo or hyperactivity, enhanced startle reaction
Disturbance of sleep-wake cycleEmotional disturbance

Acute Confusional State (Delerium)Acute Confusional State (Delerium)
Management
Dialogue with family, carers, ward staff
Safety – consider admission
Nurse separately if possible, well lit, approach away from blind spots
Full Examination – in detail
InvestigationsCommon causes – infections, constipation, overmedication, TIAsLook actively for physical basis Bloods, ECG, Radiology if appropriate
Treat as found

Anorexia NervosaAnorexia Nervosa
Features- Deliberate weight loss – induced and sustained by patient- Adolescent girls/young women (peak age 13-16yrs) F >> M- An independent syndrome (Inter-observer reliability, chronic form similar)- Aetiology unclear – increasing evidence of socio-cultural, biological and vulnerable
personality. Less evidence of specific psychological mechanisms
- Associated with under-nutrition Secondary biological features- Incidence 5:100,000 pa; Prevalence approx 1% of young females- Diagnosis: - Body wt maintained <=15% below expected or BMI <=17.5
- Wt loss is self induced – avoid fat, vomiting, purging, exercise, appetite suppressants +/- diuretics
- Body image distortion- Widespread endocrine disorder of H-P-Gonadal axis
- Amenorrhoea, Reduced sexual interest, Increased levels of GH & cortisol, changes in peripheral metabolism of thyroid hormones, abnormalities of insulin secretion- Onset before puberty
- Pubertal changes can be delayed/arrested
- Prognosis: 1/3rd better in 3y, 1/3rd better in 3-6y, 1/3rd better in 6-12y4% chronicMortality = 15%

Anorexia NervosaAnorexia Nervosa
Management
Cornerstone of therapy is talking therapy
<18y Family Therapy – to reduce EE, loosening of bonds (help with failure of individuation)
>18y Interpersonal Therapy
Self help and CBT does not work well- BUT behavioural structure similar for managing Bulimia Nervosa can be helpful if AN has improves
Treat any comorbid condition – i.e. depression
Bulimia NervosaBulimia Nervosa
Features- Preoccupation with control of body weight extreme measure to reduce
fattening effects of food- Age and sex distribution similar to Anorexia Nervosa- May be sequel to persistent AN- Vomiting electrolyte imbalance & physical problems (Tetany, etc..)- Incidence 2-15/100,000; Prevalence of approx 1%- Diagnosis: - Persistent preoccupation with eating and irresistable craving for
food – with strict dieting for ‘control’ Succumb to bingeing- Counteract fattening effects – self induced vomiting, purgative abuse, alternative periods of starving, drug use (suppressants, thyroid prep., diuretics)- Psychopathology – morbid dread of fatness
- Pt sets sharply defined wt threshold- +/- earlier episode of AN
-Prognosis: - 50% improve- 50% relapsing

Bulimia NervosaBulimia Nervosa
Management
Cornerstone is CBT
- ‘All or nothing thinking’- Work to change this and other harmful cognitions use of diary keeping and homework setting (Survey of friends, Are fat people unhappy/unsuccessful?, Are fat perople lonely?)- Behaviour modification
- Food dairy- Tight shopping list (Only what’s on it)- Limiting food (in home)- Set meal to set plan- Leave a little at end of meal throw to signify end of meal
- Self help books ‘Getting better bite by bite’ - 50% improve- Group therapy – for support- Interpersonal therapy

Self Harm - ‘DSH’Self Harm - ‘DSH’
Definition:- ‘a non-fatal act in which an individual deliberately causes self- injury or
ingests a substance in excess of any prescribed or generally recognised dose’
Kreitman (1977)Associations
- FOUR times as many stressful events in last 6/12- Early parental loss, history of parental neglect/abuse, Childhood sexual abuse- Personality factors (poor i/p problem solving skills)- Hopelessness & impulsiveness- Long term probs in marriage, kids, work, health- Unemployment (esp. in men but also women now)- Poor physical health (esp. epilepsy)- Psychiatric illness
- Depression (high rates: up to 90+ percent)- Psychotic (between 5-15%)- Alcohol & drug misuse
- About 50% had contact with NHS in the preceding week

Self Harm - ‘DSH’Self Harm - ‘DSH’
After DSH episode; outcomes
1. Repeat DSH (15-25% in first 12 months)Lots of Associated factors; Previous attempt, personality
disorder, alcohol and drug misuse, previous psychiatric tx, etc….
2. Risk of suicide (1-2% risk )This is x 100 higher than in general population10,000% increased risk than general population
At 8 years f/up 3% have committed suicide This is TWICE the expected no. from natural
causes (unclear why)
IMPORTANT to assess at time of presentation to prevent repetition and increased morbidity and mortality

Self Harm - ‘DSH’Self Harm - ‘DSH’
- Increasing since 1960s- Current rate of 3 per 1000 per year- 180,000 cases per year (60m pop)- Higher rates in UK than other Western European countries- Most common in young people- Male:Female = 1:1 (Peak age for men is older)
- High rates in- Divorced (men & women)
- teenage wives- lower social classes- high unemployment- overcrowding- many children in care, etc…

Self Harm - TreatmentsSelf Harm - Treatments
Studies have demonstrated that some treatmentsmay be of benefit
- Problem-solving therapy- Emergency contact card (controversial)- Behavioural therapy
Also delivery of well organized care has benefits of
- Recognition & treatment of major mental illness- Recognition & help for personal & social difficulties

Risk assessmentRisk assessment
Inform / predict / safety / legal / best practiceMandatory & done by all (not recognised)
If done following incident
Look at factors -- Before incident- Incident- After incident
If predicting Can use rating scale (TAG Score)

Risk assessment - method Risk assessment - method (Guidelines only….)(Guidelines only….)Before incident• Depressed? Suicidal thoughts? If so when, freq, last• What steps taken towards these plans? When? Where?• Did you act on it before? If so what was done and where?• (If not, what stopped you?)• Any pre-planning? Left any notes behind?• Use of any substances such as alcohol?• Harm to others? Elaborate…Incident• How were you found and by whom? How did you get to A&E?• What did you do and how?• What did you expect to happen?After incident• What are your thoughts about the attempt?• How does talking about this make you feel?• Future plans, thoughts of further self harm? If so, intent?• What help would make it easier?

Alcohol History - GuidelinesAlcohol History - Guidelines
• How long – From what age? Years?• Daily consumption?
– What time is first drink of day?– What do you drink and where?– How much do you drink and rate?– What time is last in day?– Any days without alcohol? – When did you start to drink daily?
• Other daily activities?• Presence of withdrawal symptoms?
– In morning or after abstinence?– Craving for alcohol?– What helps?
• Alcohol use – out of control?• Tolerance – need to drink more to have the same effect?• Medical complications? (esp. related to alcohol)
– Aware that alcohol is causing physical harm• Past history of alcohol detox’s and contact with services• Patient’s attitude towards drinking• (Depressive symptoms & DSH/suicidality)

Substance Misuse - AlcoholSubstance Misuse - Alcohol
Is this a problem?
- Alcohol misuse drinking that causes mental, physical or social harm to the individual
- CAGE questionnaire
- if >=2 positive then important to consider forDEPENDENT and HARMFUL use of alcohol and consider referral to ALCOHOL/DRUG
services

Substance Misuse - AlcoholSubstance Misuse - Alcohol
Dependent use (>= 3 in last year)
• Craving• Uncontrolled drinking – difficulty controlling consumption• Physiological withdrawal state• Tolerance• Salience of drinking – loss of other interests• C/t drinking despite evidence of harmful consequences
Substance Misuse - AlcoholSubstance Misuse - Alcohol
Harmful use – criteria
• Clear evidence alcohol is causing harm– Physical, psychological, Dysfunctional behaviour
• Nature of harm clearly identified
• Persistent use of alcohol – At least 1 month or repeatedly over 1 year

Substance Misuse - AlcoholSubstance Misuse - Alcohol
Management- Raise awareness of problem- Increase motivation to change- Withdraw alcohol (or controlled drinking)- Support and advice- CBT – social skills, relapse prevention- Marital therapy- Medication – disulfiram, acamprosate (reduce craving)- Community Alcohol Team (CAT)
- Community detox – Community Teams- Inpatient detox – Springfield, Wentworth- Community follow-up
- Support services – Alcoholic Anonymous, CAT