prospects for medical advances affecting the · pdf fileconstantijn panis baoping shang paul...
TRANSCRIPT
Prospects for Medical AdvancesAffecting the Elderly
Dana P. Goldman
Acknowledgements
RAND
Michael Hurd
Geoffrey Joyce
Emmett Keeler
Darius Lakdawalla
Stanford
Jay Bhattacharya
Alan Garber
Constantijn Panis
Baoping Shang
Paul Shekelle
Harvard
David Cutler
Funding was provided by NIA through the RAND RoybalCenter for Health Policy Simulation and the RAND AgingCenter. Original model developed with funding by CMS.
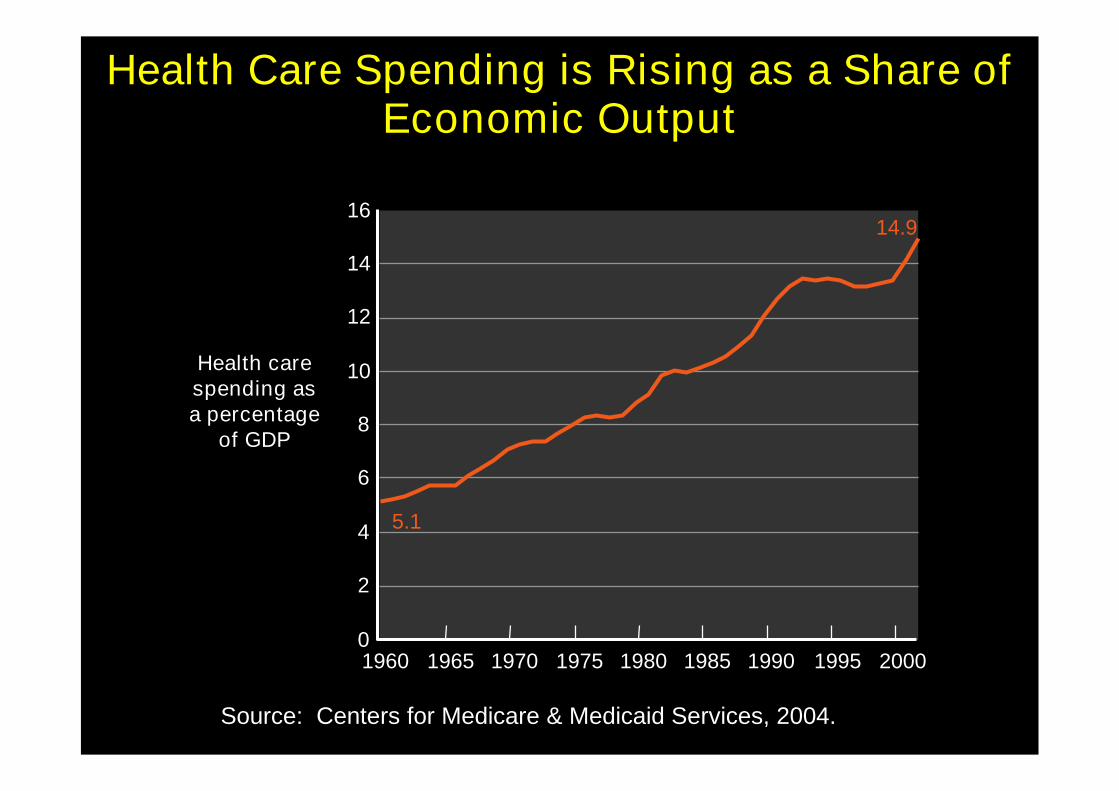
Health Care Spending is Rising as a Share ofEconomic Output
0
2
4
6
8
10
12
14
16
1960 1965 1970 1975 1980 1985 1990 1995 2000
5.1
14.9
Health carespending asa percentage
of GDP
Source: Centers for Medicare & Medicaid Services, 2004.
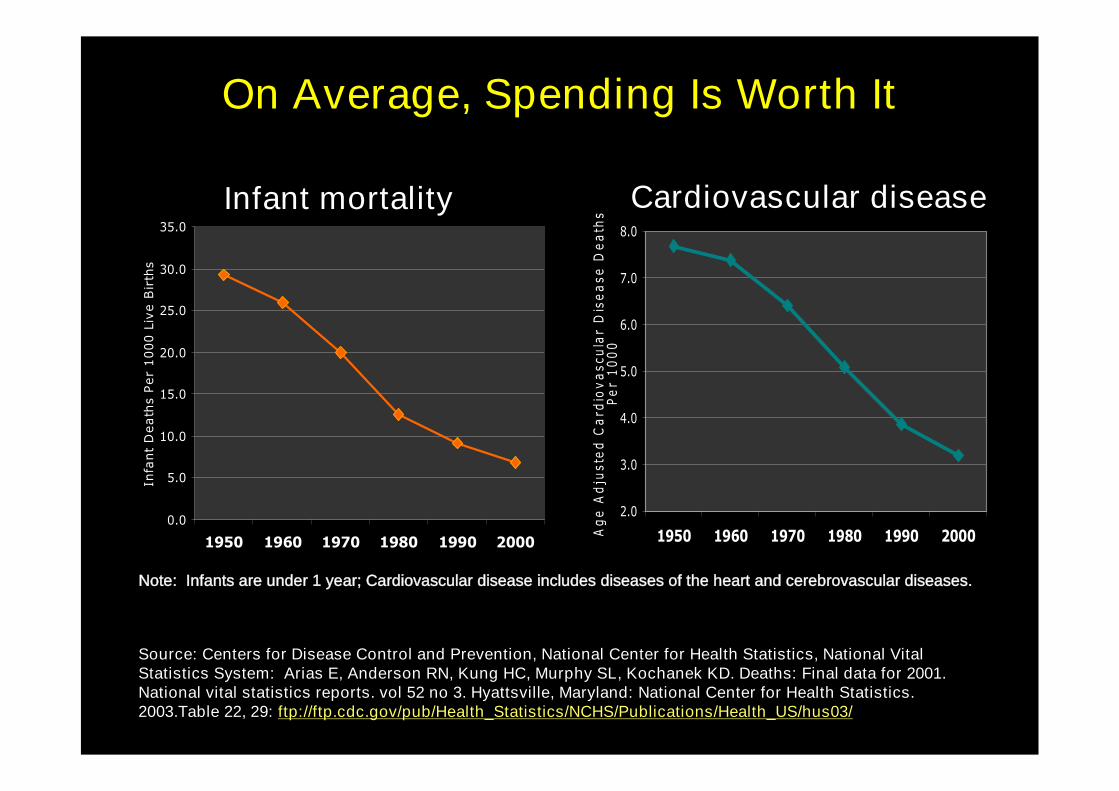
On Average, Spending Is Worth It
Source: Centers for Disease Control and Prevention, National Center for Health Statistics, National VitalStatistics System: Arias E, Anderson RN, Kung HC, Murphy SL, Kochanek KD. Deaths: Final data for 2001.National vital statistics reports. vol 52 no 3. Hyattsville, Maryland: National Center for Health Statistics.2003.Table 22, 29: ftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Publications/Health_US/hus03/
0.0
5.0
10.0
15.0
20.0
25.0
30.0
35.0
1950 1960 1970 1980 1990 2000
Infa
nt
Death
sPer
1000
Live
Bir
ths
Note: Infants are under 1 year; Cardiovascular disease includes diseases of the heart and cerebrovascular diseases.
2.0
3.0
4.0
5.0
6.0
7.0
8.0
1950 1960 1970 1980 1990 2000Ag
eA
dju
ste
dC
ard
iov
asc
ula
rD
ise
ase
De
ath
sP
er
10
00
Infant mortality Cardiovascular disease
5
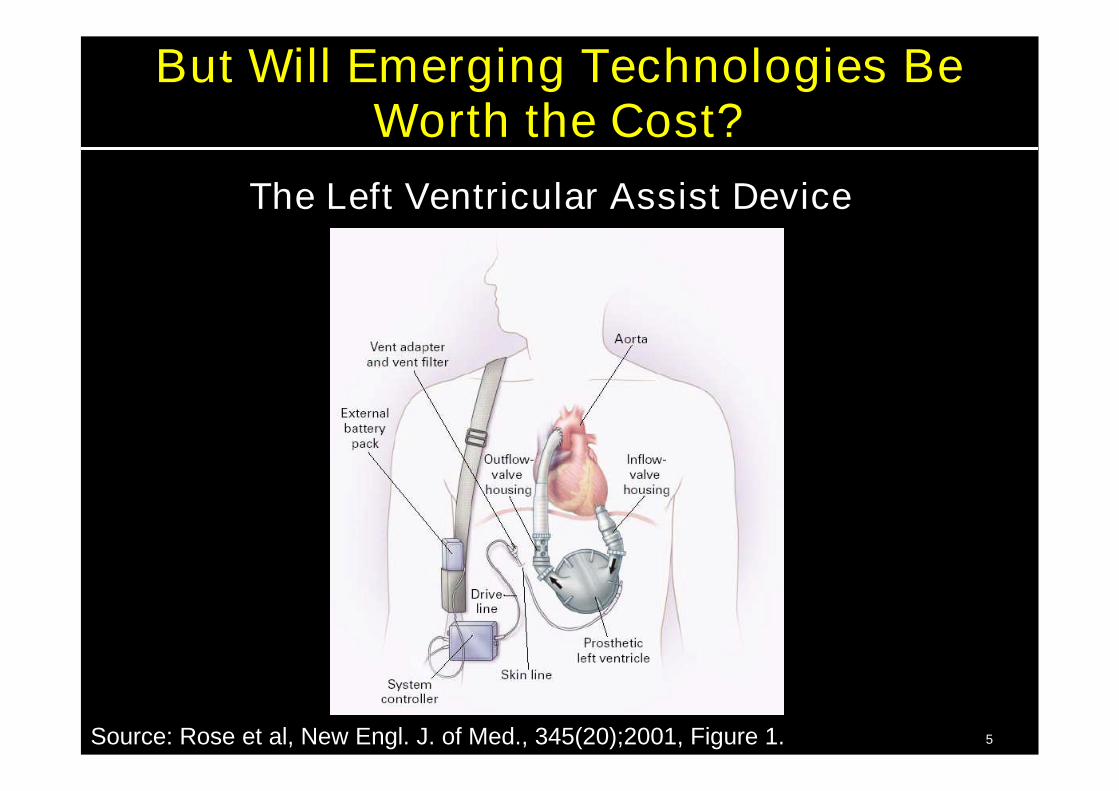
But Will Emerging Technologies BeWorth the Cost?
The Left Ventricular Assist Device
Source: Rose et al, New Engl. J. of Med., 345(20);2001, Figure 1.
Research Objectives
• Identify the key biomedical innovations andhealth trends likely to affect the elderly overthe next 30 years
• Model the effects on:
– Spending
– Disease
– Functional status
7
Convened Panels of Experts fromAround the Country
• Identified key breakthroughs in 3 clinicalareas:
– Cardiovascular disease
– Neurological disorders
– Cancer / biology of aging*
• Fourth panel of geriatricians and socialscientists
*Combined since cancer is now closely linked with the aging process at thecellular level.
8
Example:Intraventricular Defibrillators
Target: 50% of patients with heart failure50% of patients post AMI20% of patients with cardiomyopathy
Likelihood: 30% in 10 yrs30-40% in 20 yrs
Impact: Life expectancy of people with heart failureincreases 6-10 months
No impact on hospitalizations
Cost: $35,000 - $40,000 per case
~3.5 millionin 2004
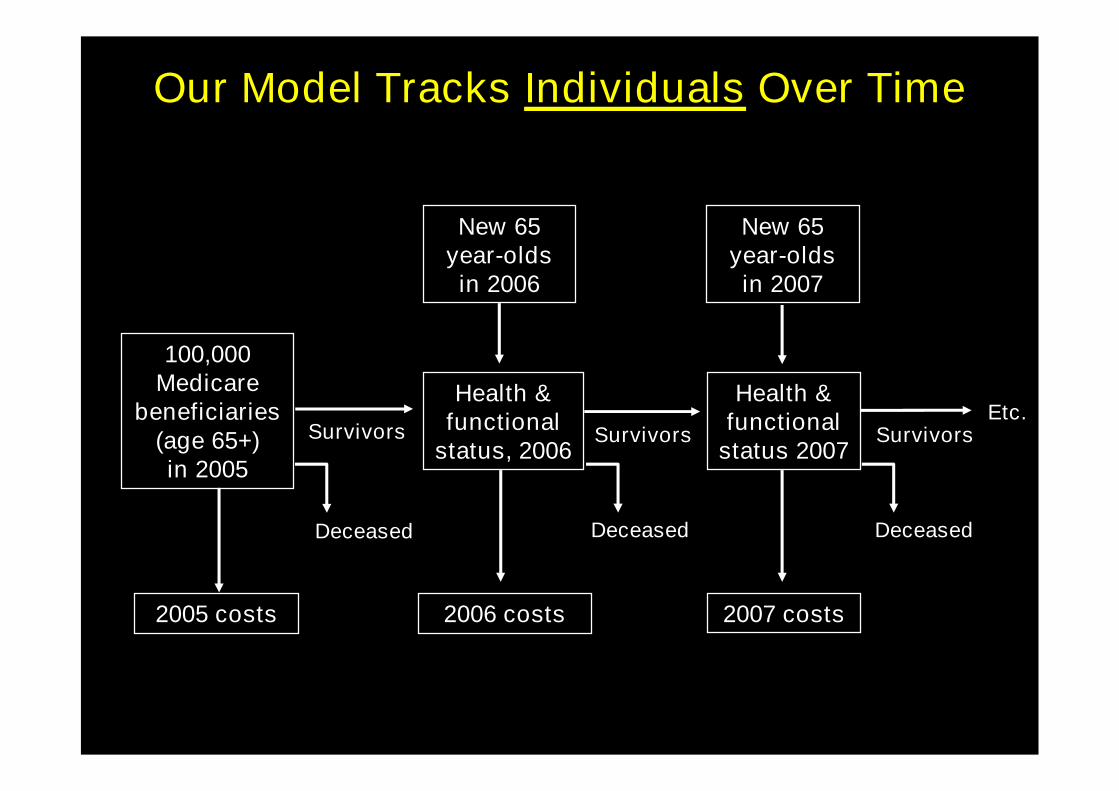
Etc.
New 65year-oldsin 2007
Deceased
Survivors
Deceased
Survivors
2007 costs
Health &functional
status 2007
Health &functional
status, 2006
Our Model Tracks Individuals Over Time
Survivors
New 65year-oldsin 2006
100,000Medicare
beneficiaries(age 65+)in 2005
2006 costs2005 costs
Deceased
10
Example 1:Compound to Extend Lifespan
• Overwhelming biomedical evidence thatreducing caloric intake of animals by 30%increases life expectancy by 25%– Chemical compounds can mimic this behavior
in rodents
• Such a pill could emerge for humans– Taken by everyone at a cost similar to
nutritional supplements ($1/day)
– Hazard of death decreases by 63%(equivalent to extending life by 15 years)
11
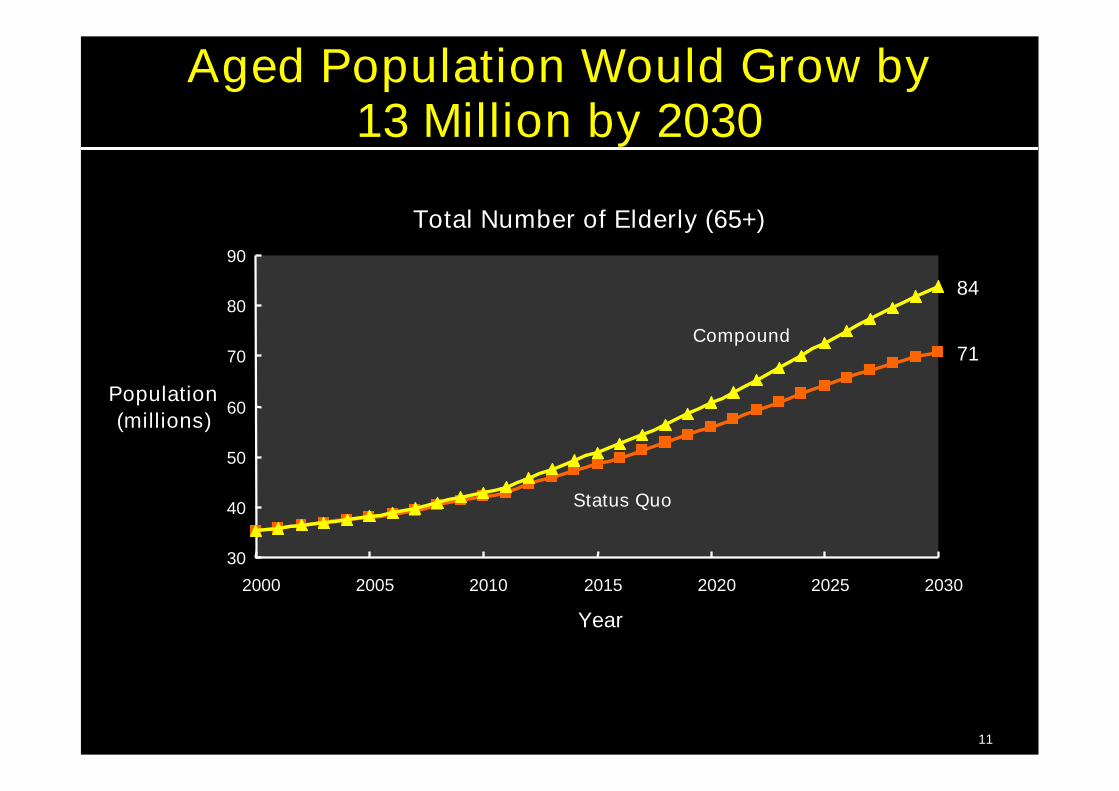
Aged Population Would Grow by13 Million by 2030
Total Number of Elderly (65+)
71
30
40
50
60
70
80
90
2000 2005 2010 2015 2020 2025 2030
Year
Population(millions)
Status Quo
84
Compound
12
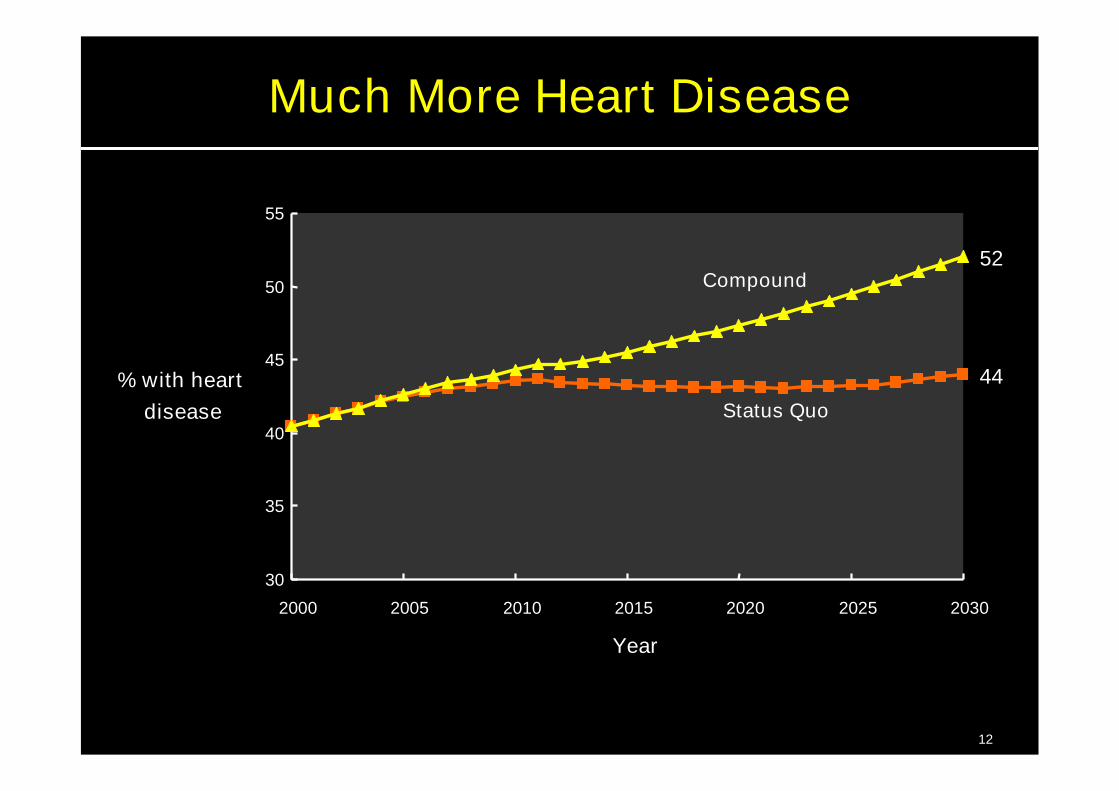
Much More Heart Disease
44
30
35
40
45
50
55
2000 2005 2010 2015 2020 2025 2030
Year
% with heartdisease Status Quo
52Compound
13
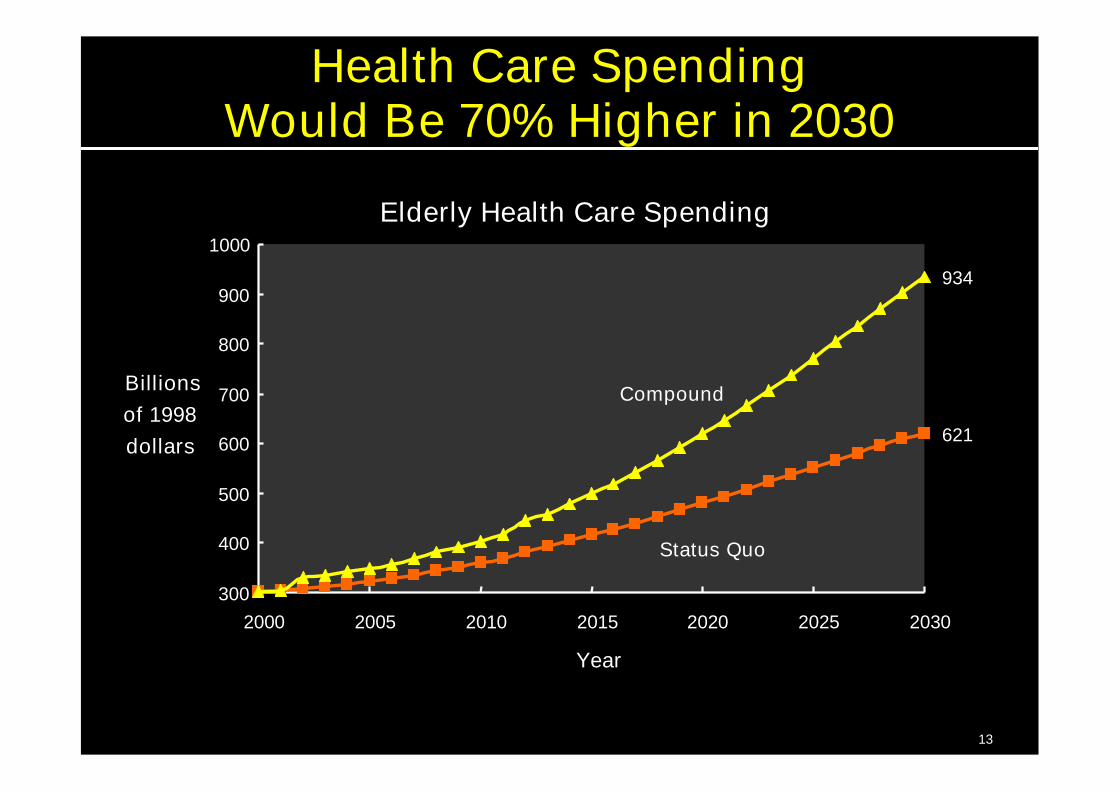
Health Care SpendingWould Be 70% Higher in 2030
Elderly Health Care Spending
621
300
400
500
600
700
800
900
1000
2000 2005 2010 2015 2020 2025 2030
Year
Billionsof 1998dollars
Status Quo
934
Compound
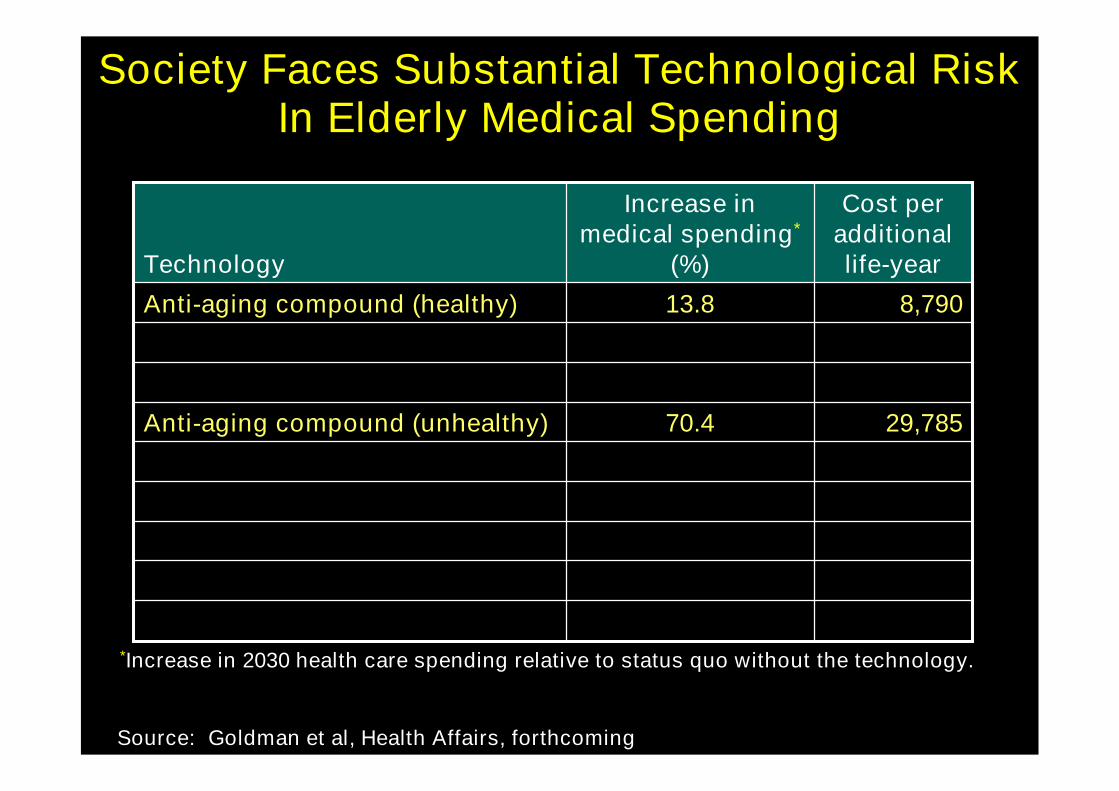
Society Faces Substantial Technological RiskIn Elderly Medical Spending
Source: Goldman et al, Health Affairs, forthcoming
29,78570.4Anti-aging compound (unhealthy)
8,79013.8Anti-aging compound (healthy)
Technology
Cost peradditionallife-year
Increase inmedical spending*
(%)
*Increase in 2030 health care spending relative to status quo without the technology.
15
Example 2:Intraventricular Cardioverter Defibrillators
• Currently used to treat patients with life-threatening arrhythmias– Shocks heart to restore natural rhythm– 26,000 procedures in 1988– $35,000 per procedure
• Scenario would expand their use– Implant in 50% of patients with heart failure or
myocardial infarction– Reduces risk of death by 10%
• Panel told us 35% chance of such an expansion

16
Will Reach 350,000 Procedures Annuallyby 2030
348,729
0
50,000
100,000
150,000
200,000
250,000
300,000
350,000
400,000
2000 2005 2010 2015 2020 2025 2030
Year
Num
ber
ofP
roce
dure
s
17
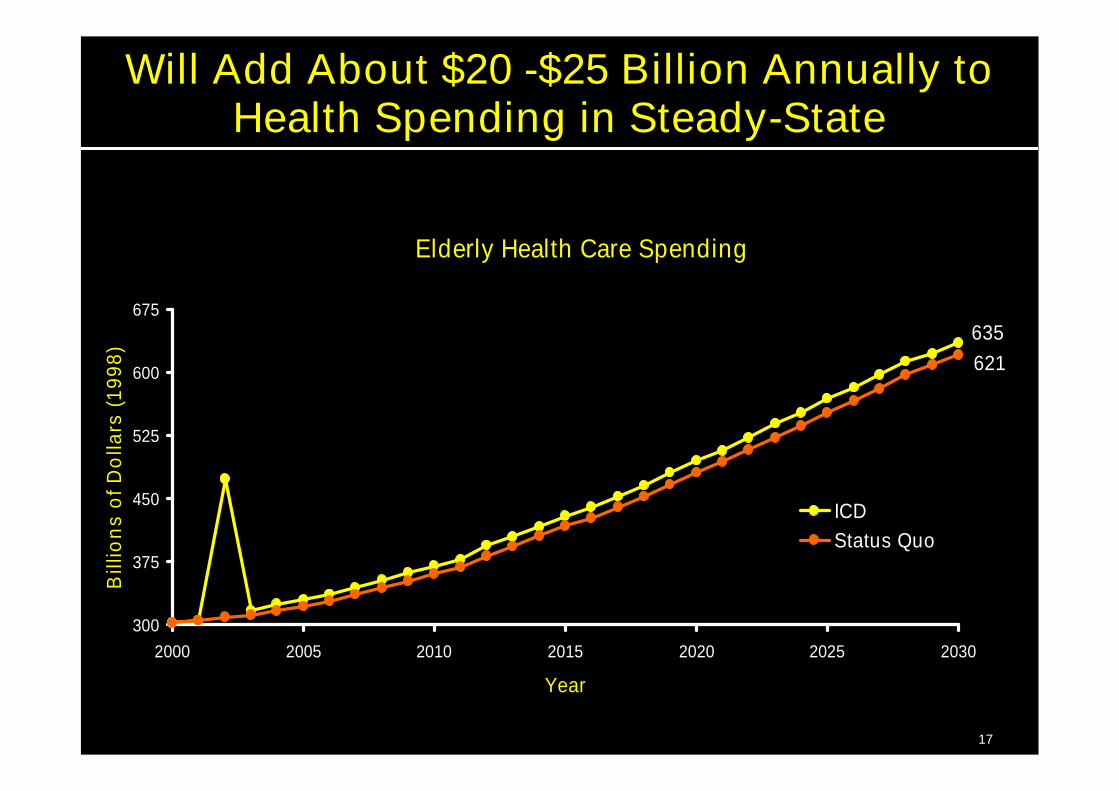
Will Add About $20 -$25 Billion Annually toHealth Spending in Steady-State
Elderly Health Care Spending
635621
300
375
450
525
600
675
2000 2005 2010 2015 2020 2025 2030
Year
Bill
ion
so
fDo
llars
(199
8)
ICDStatus Quo
18
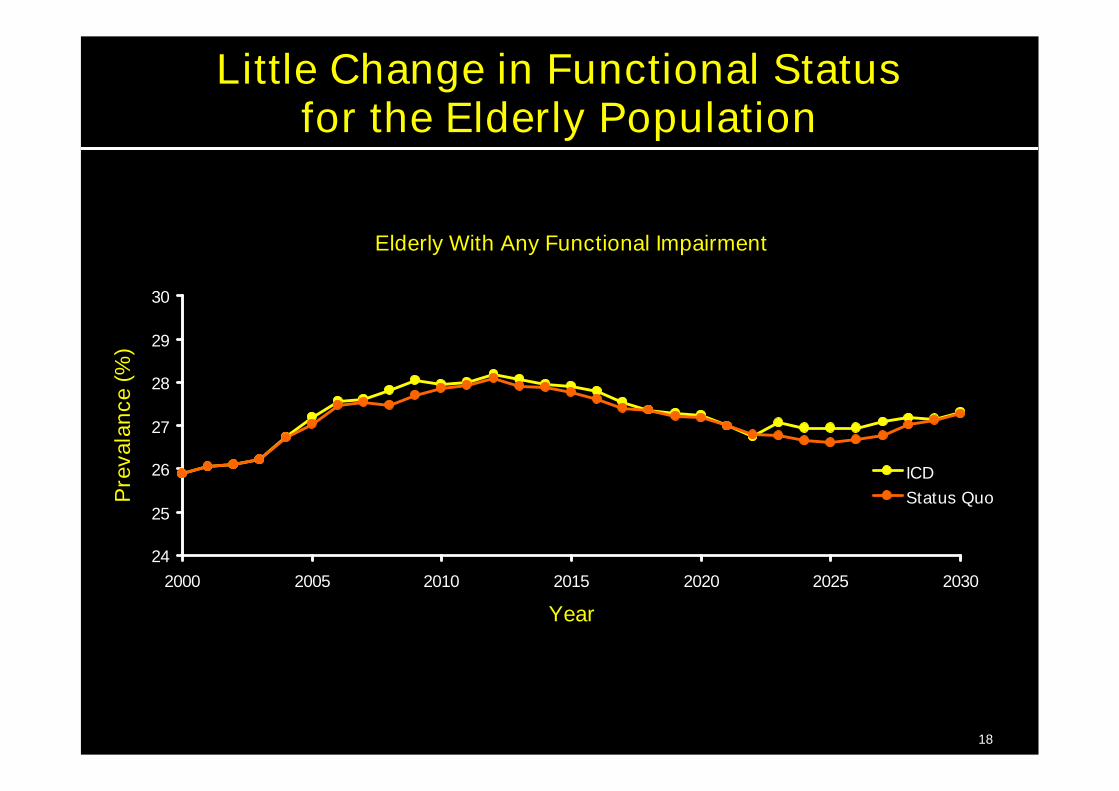
Little Change in Functional Statusfor the Elderly Population
Elderly With Any Functional Impairment
24
25
26
27
28
29
30
2000 2005 2010 2015 2020 2025 2030
Year
Pre
vala
nce
(%)
ICDStatus Quo

Society Faces Substantial Technological RiskIn Elderly Medical Spending
Source: Goldman et al, Health Affairs, forthcoming
29,78570.4Anti-aging compound (unhealthy)
103,0953.7Implantable cardio-defibrillators
8,79013.8Anti-aging compound (healthy)
Technology
Cost peradditionallife-year
Increase inmedical spending*
(%)
*Increase in 2030 health care spending relative to status quo without the technology.

Society Faces Substantial Technological RiskIn Elderly Medical Spending
Source: Goldman et al, Health Affairs, forthcoming
29,78570.4Anti-aging compound (unhealthy)
1,403,7402.3Pacemaker for atrial fibrillation
511,9622.3Left ventricular assist devices
498,8098.0Antiangiogenesis (cancer)
103,0953.7Implantable cardio-defibrillators
61,8840.5Telomerase inhibitors (cancer)
21,9050.4Treatment of acute stroke
18,2360.4Cancer vaccines
8,79013.8Anti-aging compound (healthy)
Technology
Cost peradditionallife-year
Increase inmedical spending*
(%)
*Increase in 2030 health care spending relative to status quo without the technology.
21
Key Findings• Substantial technological risk in Medicare
– Not just demographic risk caused by theaging of baby boomers
• Living longer is valuable, but not because itsaves money– Curing any one disease will not fix the
problem– Obesity may be an important exception
• Challenge is to figure out how we gettreatment to the patients who most need it