prospects for a clinical science of mindfulness-based ... · pdf filelimit the relevance and...
TRANSCRIPT

Prospects for a Clinical Science of Mindfulness-BasedIntervention
Sona Dimidjian University of Colorado BoulderZindel V. Segal University of Toronto Scarborough
Mindfulness-based interventions (MBIs) are at a pivotalpoint in their future development. Spurred on by an ever-increasing number of studies and breadth of clinical ap-plication, the value of such approaches may appear self-evident. We contend, however, that the public healthimpact of MBIs can be enhanced significantly by situatingthis work in a broader framework of clinical psychologicalscience. Utilizing the National Institutes of Health stagemodel (Onken, Carroll, Shoham, Cuthbert, & Riddle,2014), we map the evidence base for mindfulness-basedcognitive therapy and mindfulness-based stress reductionas exemplars of MBIs. From this perspective, we suggestthat important gaps in the current evidence base becomeapparent and, furthermore, that generating more of thesame types of studies without addressing such gaps willlimit the relevance and reach of these interventions. Weoffer a set of 7 recommendations that promote an inte-grated approach to core research questions, enhancedmethodological quality of individual studies, and increasedlogical links among stages of clinical translation in orderto increase the potential of MBIs to impact positively themental health needs of individuals and communities.
Keywords: mindfulness, psychotherapy, mindfulness-basedstress reduction, mindfulness-based cognitive therapy
The science and practice of mindfulness-based inter-vention (MBI) stands at a crossroads. It has wit-nessed exponential growth and interest in the last 15
years, with the establishment of research and clinical cen-ters dedicated to the study and delivery of MBIs and anattendant proliferation of academic journals, magazines,and books. Given this context of expansion, we invite apause in the forward movement to reflect on the durabilityand public health impact of this work. Our view is that suchreflection is best promoted by considering MBIs in thebroader framework of clinical psychological science andthe recently proposed National Institutes of Health (NIH)stage model (Onken et al., 2014). The NIH stage modelemerged from an interest in shaping the training of futuregenerations of clinical scientists by providing a well-artic-ulated view of the goals and process of clinical psycholog-ical science. Specifically, as presented by Onken and col-leagues (2014), the stage model is anchored in a vision
intended to unify various aspects of clinical science toward thecommon goal of developing maximally potent and implementableinterventions, while unveiling new avenues of science in which
basic and applied goals are of equally high importance . . . topropel the field to fulfill the public health goal of producingimplementable and effective treatment and prevention interven-tions. (p. 22)
In this paper, we use this framework to map MBI research,identify gaps in our knowledge and methods, and under-score priority questions and dilemmas for the future. Doingso allows us to identify both strengths and early indicationsof fault lines in the foundation of this rapidly developingfield.
We first describe the use of the NIH stage model as amap for organizing the MBI evidence base. Next, with theaim of increasing the public health impact of MBI scienceand practice, we apply the NIH stage model. We identifystrengths of the evidence base and its limitations, includingstages that have been under or overemphasized and path-ways among stages that are weak or underdeveloped. Wealso outline seven stage-based sets of recommendations forways in which the science and practice of MBI can beadvanced to increase public health impact. It is our hopethat by providing a broad and integrative framework at thiscritical juncture, we can help to chart a course that supportsdeliberate, intentional, effective, and coordinated work onMBIs.
Mapping the MBI Evidence BaseArticles were identified through searches of the PsycINFOand PubMed databases. Database records were queriedusing the search terms MBCT (i.e., mindfulness-based cog-nitive therapy), MBSR (i.e., mindfulness-based stress re-duction), and mindful* in the title or abstract fields forPubMed and in the title or subject fields for PsycINFO and
Editor’s note. This article is one of four in the special issue, “TheEmergence of Mindfulness in Basic and Clinical Psychological Science,”published in American Psychologist (October 2015). Richard J. Davidsonand Sona Dimidjian provided scholarly lead for the special issue.
Authors’ note. Sona Dimidjian, Department of Psychology and Neuro-science, University of Colorado Boulder; Zindel V. Segal, Department ofPsychology, University of Toronto Scarborough.
Sona Dimidjian and Zindel V. Segal receive royalties from GuilfordPress for work related to mindfulness-based cognitive therapy and are onthe advisory board of Mindful Noggin, which is part of NogginLabs, aprivate company specializing in customized web-based learning.
Correspondence concerning this article should be addressed to SonaDimidjian, Department of Psychology and Neuroscience, University ofColorado Boulder, 345 UCB, Boulder, CO 80309-0345. E-mail:[email protected]
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
593October 2015 ● American Psychologist© 2015 American Psychological Association 0003-066X/15/$12.00Vol. 70, No. 7, 593–620 http://dx.doi.org/10.1037/a0039589

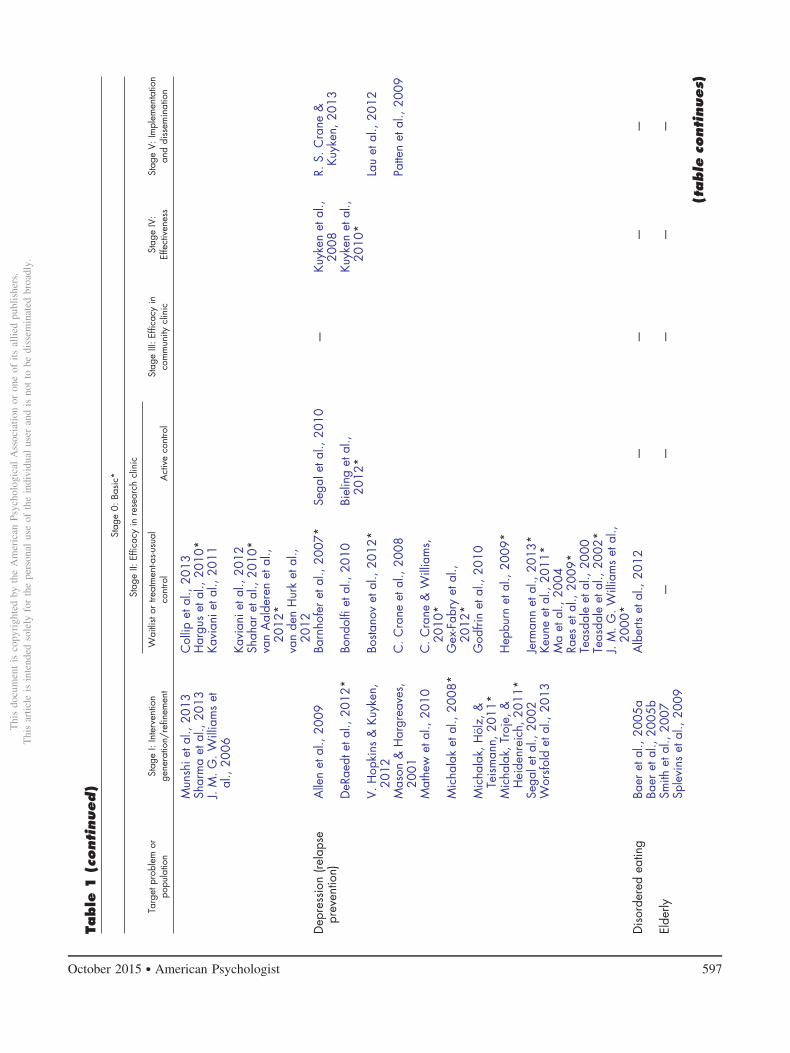
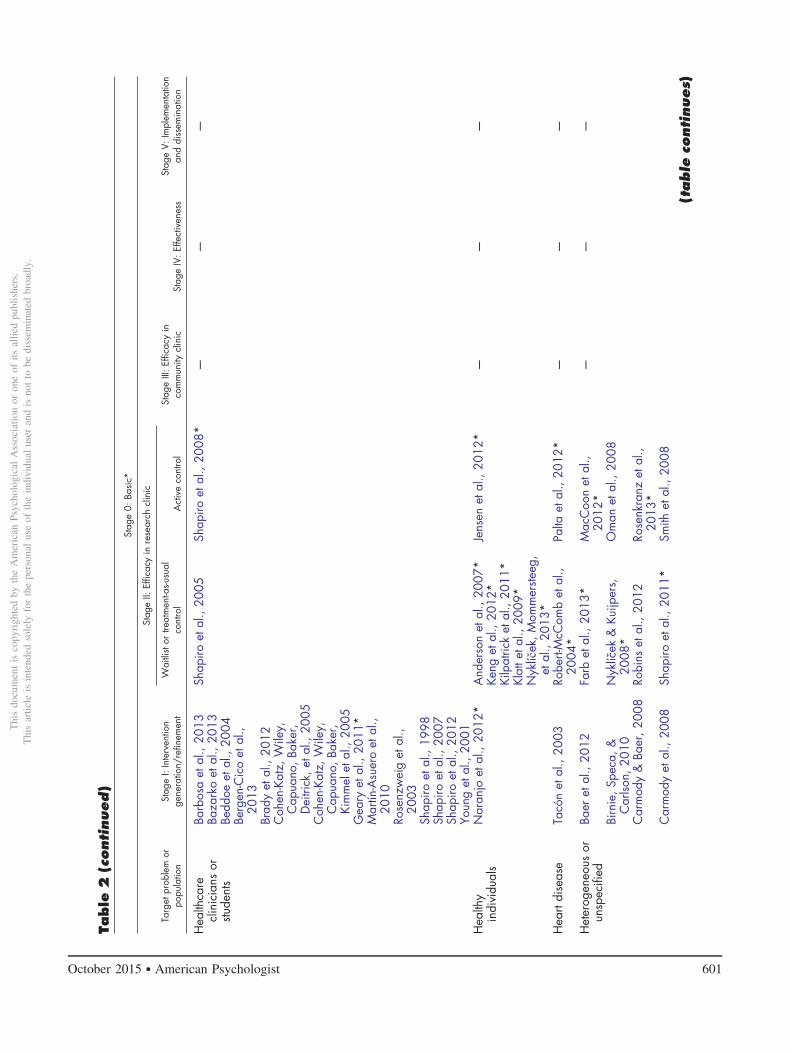
were limited to studies conducted with human subjects andpublished between January 1, 1985, and December 31,2013, in English, and in a peer-reviewed journal. Recordsfor the total number of articles returned from each querywere compiled and duplicates were removed, yielding3,217 articles in the initial search. Research assistants re-viewed the title and abstract of these records to confirmrelevance to the topic based on the article title and abstract.Articles were included if they addressed or MBCT orMBSR using case reports, open trials, controlled trials, ordevelopment of intervention fidelity measurement tools.Articles were excluded if they primarily examined topicssuch as trait or state mindfulness, trait or state mindfulnessrating scales, basic research on mindfulness techniqueswithout a clinical focus, or samples of experienced medi-tators. Interviews, personal essays or narratives, theoreticaland review articles, and meta-analyses also were excluded.Final inclusion decisions were made by the authors, result-ing in a total of 308 articles (MBCT n � 117, MBSR n �191). These were categorized by the authors for interven-tion type and target problem or population, and within eachtreatment model, by the appropriate stage based on Onkenet al. (2014) using the descriptions that follow. See Tables1 and 2 for the categorizations of the evidence base forMBCT and MBSR, respectively.
Specifically, we map at Stage 0 studies that use neu-roscience and behavioral, cognitive, affective, and socialscience methods to explicate the target of intervention andmechanisms of change. Two broad categories of basicresearch are relevant to clinical intervention. First, basicresearch studies can be conducted “upstream,” or tempo-rally preceding the other stages of research at any level ofanalysis that informs intervention development or modifi-cation. This work can offer a critical scientific foundation
for why and how an intervention may be helpful for aparticular problem or population. Second, basic researchmethods can be conducted in an integrated manner intandem with intervention research by assessing interven-tion outcomes on levels that extend beyond mental healthsymptom report and by answering questions about how anintervention works and for whom.
The scope of “upstream” basic research on the prob-lems targeted by MBIs is vast and beyond the scope of thisreview (e.g., studies identifying the pathophysiology ofmajor depression or anxiety disorders, etc.). Thus, ourmapping focuses on the second category of basic re-search—that which is integrated with applied research atStages I–V. These studies encompass varying degrees ofmethodological rigor; however, they share the commonelement of seeking to understand whether an MBI worksbeyond simply symptom report, as well as how and forwhom. Because this work integrates basic research para-digms as part of later stage intervention studies, it ismapped with an asterisk at the relevant later-stage study.
We include studies that examine multiple units ofanalysis to measure treatment outcome (e.g., measurementof neural circuits, physiology, performance on behavioralor cognitive tasks, etc.). For example, in a study testingMBSR with HIV-positive patients, Creswell, Myers, Cole,and Irwin (2009) examined the effects on biological mark-ers of disease progression (e.g., CD4 � T lymphocytes); asthis study integrates basic research methods to characterizeprecise biological outcomes within the context of a Stage IIstudy, it is denoted with an asterisk in Table 2. We alsoinclude studies that test mediation or moderation of inter-vention outcomes (even if only limited to one unit ofanalysis such as self-report). For example, Arch and Ayers(2013) measured self-report of baseline clinical severityand examined the extent to which such information couldidentify which treatment worked better for which patients;as this study integrated a focus on treatment moderation inthe context of a Stage II study, it is denoted in Table 2 withan asterisk.
Onken et al. (2014) define Stage I as “all activitiesrelated to the creation of a new intervention, or the modi-fication, adaptation, or refinement of an existing interven-tion (Stage IA), as well as feasibility and pilot testing(Stage IB)” (p. 28). This stage is also defined to encompassa focus on the development of training, supervision, andfidelity promotion materials. Our mapping at this stageincludes mainly feasibility and pilot testing studies includ-ing nonrandomized open-trial designs of an MBI, whetherconducted in the research lab or community settings. Mostof these studies focus on extending the MBI to a novelproblem or population, although some also represent earlyphase work in extending an MBI to a new setting. Some ofthese studies also examine the relationship between inter-vention exposure and outcome (e.g., dosage effects).
As defined by Onken et al. (2014),
Stage II research consists of testing of promising behavioralinterventions in research settings, with research therapists/pro-viders . . . Stage III is similar to Stage II research, except that
SonaDimidjian
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
594 October 2015 ● American Psychologist

instead of research providers and settings, it consists of testing ina community context while maintaining a high level of controlnecessary to establish internal validity. (pp. 28–29)
We map at Stage II efficacy trials of promising MBIsconducted in research settings, and at Stage III efficacytrials conducted in community settings, using communityproviders. These studies place a premium on internal va-lidity, and focus on testing efficacy and identifying mech-anisms of change. We extend the NIH model by mappingseparately at Stage II studies that use randomized designsthat test efficacy, with comparisons often to treatment-as-usual (TAU) or waitlist control (WLC) conditions andrandomized designs that test comparative or specific effi-cacy, with comparisons to an active control or an estab-lished treatment. Although the distinction between activecontrol and other comparison groups is relevant for StagesIII–V, we have not mapped those separately due to thepaucity of work at those stages. As more studies at thesestages are conducted, it will be vital for future efforts tomap the nature of the control and comparison conditions infiner granularity. Although Onken et al. (2014) allow forthe inclusion of nonrandomized designs at Stage II, wesuggest that the methodological rigor of randomized con-trolled trials has specific value for the future of research onMBI; thus, we map all nonrandomized designs at Stage I.
Stages IV and V cover effectiveness research andimplementation and dissemination research, respectively.As defined by Onken et al. (2014), effectiveness research(Stage IV) places a premium on external validity, as re-searchers examine interventions as implemented by com-munity providers under routine conditions “in the realworld.” Stage V places relatively less emphasis on theintervention itself and instead foregrounds the study ofmethods to increase the adoption, integration, scaling up,and sustainability of an intervention in everyday settings.An important contribution of the NIH model is defining
these stages as integral components of the clinical scienceendeavor. The inclusion of these stages codifies an inherentvalue that “intervention development is incomplete untilthe intervention is maximally potent and implementable forthe population for which it was developed” (Onken et al.,2014, p. 25).
The Clinical Application ofMindfulness and Current EvidenceBase: A “Bird’s Eye View”MBSR originated in the work of Jon Kabat-Zinn and col-leagues in 1979 at the University of Massachusetts MedicalCenter (Kabat-Zinn, 1990). Nearly a decade later, Segal,Williams, and Teasdale (2002) built upon this early foun-dation with the development of MBCT, extending andintegrating the framework and practices of MBSR withcognitive–behavioral therapy. Both of these interventionsare organized around the use of mindfulness meditation asa core intervention component, and engage such specificpractices as sitting meditation, walking meditation, bodyscan meditation, yoga, and a range of forms of daily infor-mal practice (e.g., mindful eating). These practices aretaught to support participants in developing mindfulness asskills or means to personal goals (e.g., prevention of de-pression or reduction of stress) and, to borrow from Lutz,Jha, Dunne, and Saron (2015), “a way of life.” Each sessionis delivered using an eight-session, weekly structure fea-turing extended experiential practice and inquiry aboutpractice. The essential role of daily formal and informalmindfulness practice is emphasized throughout. The role ofthe instructor in these interventions is multilayered andcomprises guiding practice (e.g., in person during classesand via audio recorded practice guides for participants touse between classes), embodying “mindfulness” using thebroadest conceptualization of this term (J. M. G. Williams& Kabat-Zinn, 2011), and delivering intervention specificcontent (e.g., about stress or depression risk). Instructorsare asked to teach from a foundation of their own personalmindfulness meditation practice.
Although other conceptually and clinically related in-terventions were developed in parallel to MBSR andMBCT (e.g., acceptance and commitment therapy; Hayes,Strosahl, & Wilson, 1999; and dialectical behavior therapy;Linehan, 1993), MBSR and MBCT are distinguished by thepredominant focus on mindfulness meditation practices,the 8-week course structure, active daily home practice ofmindfulness meditation, and the role and training require-ments of the instructor. Moreover, since the first studies ofMBCT and MBSR were published, multiple “next-gener-ation” MBI models have been developed. We focus, how-ever, on MBCT and MBSR as the target interventions forthis review because each has amassed a sufficient empiricalrecord to enable mapping of this nature. In a final section,we offer reflections about next-generation interventionsand recent findings that reflect promising advancements inthe field. As the field develops, we expect that updates toour mapping will be required for MBSR, MBCT, andrelated as well as next-generation interventions.
Zindel V.Segal
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
595October 2015 ● American Psychologist

Table
1N
atio
nalI
nstit
utes
ofH
ealth
Stag
eM
odel
Cla
ssifi
catio
nof
Min
dful
ness
-Bas
edC
ogni
tive
Ther
apy
Evid
ence
Base
Stag
e0:
Basi
c*
Targ
etpr
oble
mor
popu
latio
nSt
age
I:In
terv
entio
nge
nera
tion/
refin
emen
t
Stag
eII:
Effic
acy
inre
sear
chcl
inic
Stag
eIII
:Effi
cacy
inco
mm
unity
clin
icSt
age
IV:
Effe
ctiv
enes
sSt
age
V:Im
plem
enta
tion
and
diss
emin
atio
nW
aitli
stor
treat
men
t-as-u
sual
cont
rol
Act
ive
cont
rol
Anx
iety
Ceb
olla
iMar
tí&
Barr
achi
na,2
009
McM
anus
etal
.,20
12*
Piet
etal
.,20
10—
——
Cra
igie
etal
.,20
08M
.J.W
illia
ms
etal
.,20
11Ev
ans
etal
.,20
08H
erte
nste
inet
al.,
2012
Y.W
.Kim
etal
.,20
09B.
Kim
etal
.,20
10Ki
nget
al.,
2013
Lova
s&
Bars
ky,2
010
Bipo
lar
Dec
kers
bach
etal
.,20
12Pe
rich,
Man
icav
asag
ar,
Mitc
hell,
&Ba
ll,20
13
——
——
How
ells
etal
.,20
12*
J.M
.G.W
illia
ms
etal
.,20
08Iv
es-D
elip
erie
tal.,
2013
*M
iklo
witz
etal
.,20
09Pe
rich,
Man
icav
asag
ar,
Mitc
hell,
Ball,
&H
adzi
-Pav
lovi
c,20
13St
ange
etal
.,20
11W
eber
etal
.,20
10Bo
rder
line
pers
onal
itydi
sord
erH
uss
&Ba
er,2
007
——
——
—Sa
chse
etal
.,20
11C
areg
iver
s—
—O
ken
etal
.,20
10*
——
—C
hild
/Fam
ilyBa
ilie
etal
.,20
12Se
mpl
eet
al.,
2010
——
——
Lee
etal
.,20
08D
epre
ssio
n(re
sidu
alde
pres
sive
sym
ptom
s,ac
ute,
and
subc
linic
al)
Eise
ndra
thet
al.,
2011
Barn
hofe
ret
al.,
2009
Chi
esa
etal
.,20
12—
——
Finu
cane
&M
erce
r,20
06C
.Cra
neet
al.,
2012
*M
anic
avas
gar
etal
.,20
11Ke
nny
&W
illia
ms,
2007
Ges
chw
ind
etal
.,20
11
King
ston
etal
.,20
07G
esch
win
det
al.,
2012
*
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
596 October 2015 ● American Psychologist
Table
1(c
ontinued)
Stag
e0:
Basi
c*
Targ
etpr
oble
mor
popu
latio
nSt
age
I:In
terv
entio
nge
nera
tion/
refin
emen
t
Stag
eII:
Effic
acy
inre
sear
chcl
inic
Stag
eIII
:Effi
cacy
inco
mm
unity
clin
icSt
age
IV:
Effe
ctiv
enes
sSt
age
V:Im
plem
enta
tion
and
diss
emin
atio
nW
aitli
stor
treat
men
t-as-u
sual
cont
rol
Act
ive
cont
rol
Mun
shie
tal.,
2013
Col
lipet
al.,
2013
Shar
ma
etal
.,20
13H
argu
set
al.,
2010
*J.
M.G
.Will
iam
set
al.,
2006
Kavi
anie
tal.,
2011
Kavi
anie
tal.,
2012
Shah
aret
al.,
2010
*va
nA
alde
ren
etal
.,20
12*
van
den
Hur
ket
al.,
2012
Dep
ress
ion
(rela
pse
prev
entio
n)A
llen
etal
.,20
09Ba
rnho
fer
etal
.,20
07*
Sega
leta
l.,20
10—
Kuyk
enet
al.,
2008
R.S.
Cra
ne&
Kuyk
en,2
013
DeR
aedt
etal
.,20
12*
Bond
olfi
etal
.,20
10Bi
elin
get
al.,
2012
*Ku
yken
etal
.,20
10*
V.H
opki
ns&
Kuyk
en,
2012
Bosta
nov
etal
.,20
12*
Lau
etal
.,20
12
Mas
on&
Har
grea
ves,
2001
C.C
rane
etal
.,20
08Pa
tten
etal
.,20
09
Mat
hew
etal
.,20
10C
.Cra
ne&
Will
iam
s,20
10*
Mic
hala
ket
al.,
2008
*G
ex-F
abry
etal
.,20
12*
Mic
hala
k,H
ölz,
&Te
ism
ann,
2011
*G
odfri
net
al.,
2010
Mic
hala
k,Tr
oje,
&H
eide
nrei
ch,2
011*
Hep
burn
etal
.,20
09*
Sega
leta
l.,20
02Je
rman
net
al.,
2013
*W
orsf
old
etal
.,20
13Ke
une
etal
.,20
11*
Ma
etal
.,20
04Ra
eset
al.,
2009
*Te
asda
leet
al.,
2000
Teas
dale
etal
.,20
02*
J.M
.G.W
illia
ms
etal
.,20
00*
Dis
orde
red
eatin
gBa
eret
al.,
2005
aA
lber
tset
al.,
2012
——
——
Baer
etal
.,20
05b
Elde
rlySm
ithet
al.,
2007
——
——
—Sp
levi
nset
al.,
2009
(table
continues)
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
597October 2015 ● American Psychologist

Table
1(c
ontinued)
Stag
e0:
Basi
c*
Targ
etpr
oble
mor
popu
latio
nSt
age
I:In
terv
entio
nge
nera
tion/
refin
emen
t
Stag
eII:
Effic
acy
inre
sear
chcl
inic
Stag
eIII
:Effi
cacy
inco
mm
unity
clin
icSt
age
IV:
Effe
ctiv
enes
sSt
age
V:Im
plem
enta
tion
and
diss
emin
atio
nW
aitli
stor
treat
men
t-as-u
sual
cont
rol
Act
ive
cont
rol
Hea
lthca
restu
dent
sC
olla
rdet
al.,
2008
——
——
—H
opki
nset
al.,
2013
Rim
eset
al.,
2011
Ruth
set
al.,
2013
Het
erog
eneo
us/
Uns
peci
fied
R.S.
Cra
neet
al.,
2013
——
——
—
Gre
enet
al.,
2012
Hee
ren
etal
.,20
09*
Her
dtet
al.,
2012
Lang
don
etal
.,20
11Re
eet
al.,
2007
Schr
oeve
rset
al.,
2010
Troy
etal
.,20
13*
Med
ical
com
orbi
dity
Cha
mbe
rset
al.,
2012
Brot
toet
al.,
2012
*Ph
ilipp
otet
al.,
2012
N.J
.Tho
mps
onet
al.,
2010
van
Rave
steijn
etal
.,20
13—
Fitz
patri
cket
al.,
2010
Fole
yet
al.,
2010
Grif
fiths
etal
.,20
09Pa
rra-
Del
gado
etal
.,20
13O
’Hav
erD
ay,&
Hor
ton-
Deu
tsch,
2004
Rim
eset
al.,
2013
Shar
plin
etal
.,20
10Sk
ovbj
erg
etal
.,20
12va
nde
rLe
eet
al.,
2012
van
Son
etal
.,20
13*
Preg
nanc
yD
unn
etal
.,20
12—
——
——
Prob
lem
gam
blin
gde
Lisle
etal
.,20
11—
——
——
Psyc
hosi
s—
Lang
eret
al.,
2012
——
——
Slee
pYo
oket
al.,
2008
Britt
onet
al.,
2010
*—
——
—Br
itton
,Hay
nes,
etal
.,20
12*
Britt
on,S
haha
r,et
al.,
2012
*
*St
udie
sth
atin
tegr
ate
basi
cre
sear
chas
part
ofla
ter
stage
inte
rven
tion
studi
esar
ede
note
dat
the
rele
vant
late
rsta
gew
ithan
aste
risk.
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
598 October 2015 ● American Psychologist

Table
2N
atio
nalI
nstit
utes
ofH
ealth
Stag
eM
odel
Cla
ssifi
catio
nof
Min
dful
ness
-Bas
edSt
ress
Redu
ctio
nEv
iden
ceBa
se
Stag
e0:
Basi
c*
Targ
etpr
oble
mor
popu
latio
nSt
age
I:In
terv
entio
nge
nera
tion/
refin
emen
t
Stag
eII:
Effic
acy
inre
sear
chcl
inic
Stag
eIII
:Effi
cacy
inco
mm
unity
clin
icSt
age
IV:E
ffect
iven
ess
Stag
eV:
Impl
emen
tatio
nan
ddi
ssem
inat
ion
Wai
tlist
ortre
atm
ent-a
s-usu
alco
ntro
lA
ctiv
eco
ntro
l
Ado
lesc
ents
Jastr
owsk
iMan
oet
al.,
2013
Bieg
elet
al.,
2009
Sibi
nga
etal
.,20
13*
——
—
Anx
iety
Gol
din
etal
.,20
09*
Vølle
stad
etal
.,20
11*
Arc
h&
Aye
rs,2
013*
——
—G
oldi
net
al.,
2010
*A
rch
etal
.,20
13H
azle
tt-St
even
set
al.,
2012
Gol
din
etal
.,20
12*
Mill
er19
95G
oldi
net
al.,
2013
*Pa
tele
tal.,
2007
Hog
eet
al.,
2013
*Ra
pgay
etal
.,20
11Ja
zaie
riet
al.,
2012
Kosz
ycki
etal
.,20
07A
rthrit
is—
Prad
han
etal
.,20
07*
——
——
Asth
ma
——
Pber
teta
l.,20
12*
——
—C
ance
rA
berc
rom
bie
etal
.,20
07A
nder
sen
etal
.,20
13H
ende
rson
etal
.,20
12—
——
Alts
chul
eret
al.,
2012
Brän
ström
etal
.,20
13*
Birn
ie,G
arla
nd,&
Car
lson,
2010
Hof
fman
,Ers
ser,
Hop
kins
on,N
icho
lls,
etal
.,20
12C
ampb
elle
tal.,
2012
*La
belle
etal
.,20
10*
Car
lson
etal
.,20
03*
Leng
ache
ret
al.,
2009
Car
lson
etal
.,20
04*
Leng
ache
r,Re
ich,
etal
.,20
12C
arlso
n&
Gar
land
,20
05*
Leng
ache
ret
al.,
2013
*
Car
lson
etal
.,20
07*
Lerm
anet
al.,
2012
Deg
ieta
l.,20
13W
ürtz
en,D
alto
n,El
sass
,et
al.,
2013
Dob
kin
etal
.,20
08G
arla
ndet
al.,
2007
Gar
land
etal
.,20
13H
offm
an,E
rsse
r,&
Hop
kins
on,2
012
Kiev
iet-S
tijne
net
al.,
2008
(table
continues)
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
599October 2015 ● American Psychologist

Table
2(c
ontinued)
Stag
e0:
Basi
c*
Targ
etpr
oble
mor
popu
latio
nSt
age
I:In
terv
entio
nge
nera
tion/
refin
emen
t
Stag
eII:
Effic
acy
inre
sear
chcl
inic
Stag
eIII
:Effi
cacy
inco
mm
unity
clin
icSt
age
IV:E
ffect
iven
ess
Stag
eV:
Impl
emen
tatio
nan
ddi
ssem
inat
ion
Wai
tlist
ortre
atm
ent-a
s-usu
alco
ntro
lA
ctiv
eco
ntro
l
Kvill
emo
etal
.,20
11Le
ngac
her
etal
.,20
11Le
ngac
her,
Kip,
etal
.20
12*
Mac
kenz
ieet
al.,
2007
Mat
chim
etal
.,20
11*
Mat
ouse
ket
al.,
2011
*Sa
xeet
al.,
2001
*Sh
apiro
etal
.,20
03Ta
cón
etal
.,20
04Ta
cón
etal
.,20
11Ts
ang
etal
.,20
12W
eitz
etal
.,20
12W
itek-
Janu
sek
etal
.,20
08*
Wür
tzen
,Dal
ton,
And
erse
n,et
al.,
2013
*C
areg
iver
sEp
stein
-Lubo
wet
al.,
2011
—W
hite
bird
etal
.,20
13—
——
Min
oret
al.,
2006
Chr
onic
pain
Rose
nzw
eig
etal
.,20
10—
Esm
eret
al.,
2010
——
—
Plew
s-Oga
net
al.,
2005
Won
get
al.,
2011
Dep
ress
ion
histo
ryRa
mel
etal
.,20
04—
——
——
Dia
bete
sRo
senz
wei
get
al.,
2007
*H
artm
ann
etal
.,20
12*
——
——
Dis
orde
red
eatin
gKe
arne
y,M
ilton
,eta
l.,20
12—
——
——
Smith
etal
.,20
06Fi
brom
yalg
iaG
ross
man
etal
.,20
07Se
phto
net
al.,
2007
Schm
idte
tal.,
2011
——
—Ka
plan
etal
.,19
93Lu
shet
al.,
2009
*W
eiss
beck
eret
al.,
2002
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
600 October 2015 ● American Psychologist
Table
2(c
ontinued)
Stag
e0:
Basi
c*
Targ
etpr
oble
mor
popu
latio
nSt
age
I:In
terv
entio
nge
nera
tion/
refin
emen
t
Stag
eII:
Effic
acy
inre
sear
chcl
inic
Stag
eIII
:Effi
cacy
inco
mm
unity
clin
icSt
age
IV:E
ffect
iven
ess
Stag
eV:
Impl
emen
tatio
nan
ddi
ssem
inat
ion
Wai
tlist
ortre
atm
ent-a
s-usu
alco
ntro
lA
ctiv
eco
ntro
l
Hea
lthca
recl
inic
ians
orstu
dent
s
Barb
osa
etal
.,20
13Sh
apiro
etal
.,20
05Sh
apiro
etal
.,20
08*
——
—Ba
zark
oet
al.,
2013
Bedd
oeet
al.,
2004
Berg
en-C
ico
etal
.,20
13Br
ady
etal
.,20
12C
ohen
-Kat
z,W
iley,
Cap
uano
,Bak
er,
Dei
trick
,eta
l.,20
05C
ohen
-Kat
z,W
iley,
Cap
uano
,Bak
er,
Kim
mel
etal
.,20
05G
eary
etal
.,20
11*
Mar
tín-A
suer
oet
al.,
2010
Rose
nzw
eig
etal
.,20
03Sh
apiro
etal
.,19
98Sh
apiro
etal
.,20
07Sh
apiro
etal
.,20
12Yo
ung
etal
.,20
01H
ealth
yin
divi
dual
sN
aran
joet
al.,
2012
*A
nder
son
etal
.,20
07*
Jens
enet
al.,
2012
*—
——
Keng
etal
.,20
12*
Kilp
atric
ket
al.,
2011
*Kl
atte
tal.,
2009
*N
yklí�
ek,M
omm
erste
eg,
etal
.,20
13*
Hea
rtdi
seas
eTa
cón
etal
.,20
03Ro
bert-
McC
omb
etal
.,20
04*
Palta
etal
.,20
12*
——
—
Het
erog
eneo
usor
unsp
ecifi
edBa
eret
al.,
2012
Farb
etal
.,20
13*
Mac
Coo
net
al.,
2012
*—
——
Birn
ie,S
peca
,&C
arlso
n,20
10N
yklíc
ek&
Kuijp
ers,
2008
*O
man
etal
.,20
08
Car
mod
y&
Baer
,200
8Ro
bins
etal
.,20
12Ro
senk
ranz
etal
.,20
13*
Car
mod
yet
al.,
2008
Shap
iroet
al.,
2011
*Sm
ithet
al.,
2008
(table
continues)
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
601October 2015 ● American Psychologist

Table
2(c
ontinued)
Stag
e0:
Basi
c*
Targ
etpr
oble
mor
popu
latio
nSt
age
I:In
terv
entio
nge
nera
tion/
refin
emen
t
Stag
eII:
Effic
acy
inre
sear
chcl
inic
Stag
eIII
:Effi
cacy
inco
mm
unity
clin
icSt
age
IV:E
ffect
iven
ess
Stag
eV:
Impl
emen
tatio
nan
ddi
ssem
inat
ion
Wai
tlist
ortre
atm
ent-a
s-usu
alco
ntro
lA
ctiv
eco
ntro
l
Car
mod
y&
Baer
,200
9Si
mps
onet
al.,
2011
Car
mod
yet
al.,
2009
*C
hang
etal
.,20
04C
ordo
net
al.,
2009
*de
lRe
etal
.,20
13D
eyo
etal
.,20
09D
obki
net
al.,
2011
Evan
set
al.,
2011
Fang
etal
.,20
10*
Flug
elet
al.,
2010
Fris
vold
etal
.,20
12G
rees
onet
al.,
2011
*H
awtin
etal
.,20
11H
ölze
leta
l.,20
11*
Imel
etal
.,20
08*
Jha
etal
.,20
07*
Kerr
etal
.,20
11Ke
rrig
anet
al.,
2011
Mel
loni
etal
.,20
13*
Mor
one
etal
.,20
12Re
ibel
etal
.,20
01Ro
th19
97Ro
th&
Cre
aser
,199
7Ro
thet
al.,
2002
Roth
etal
.,20
04Sa
lmoi
rago
-Blo
tche
ret
al.,
2013
Thom
pson
etal
.,20
09W
eiss
etal
.,20
05H
IVJa
met
al.,
2010
*D
unca
net
al.,
2012
Cre
swel
leta
l.,20
09*
——
—
Robi
nson
etal
.,20
03*
Gay
ner
etal
.,20
12Se
yedA
linag
hiet
al.,
2012
*Si
bing
aet
al.,
2008
Sibi
nga
etal
.,20
11H
otfla
shes
Car
mod
yet
al.,
2006
Car
mod
yet
al.,
2011
——
——
Irrita
ble
bow
elsy
ndro
me
Kear
ney
etal
.,20
11Ze
rnic
keet
al.,
2013
Gar
land
etal
.,20
12*
Inso
mni
a—
—G
ross
etal
.,20
11*
——
—
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
602 October 2015 ● American Psychologist

Table
2(c
ontinued)
Stag
e0:
Basi
c*
Targ
etpr
oble
mor
popu
latio
nSt
age
I:In
terv
entio
nge
nera
tion/
refin
emen
t
Stag
eII:
Effic
acy
inre
sear
chcl
inic
Stag
eIII
:Effi
cacy
inco
mm
unity
clin
icSt
age
IV:E
ffect
iven
ess
Stag
eV:
Impl
emen
tatio
nan
ddi
ssem
inat
ion
Wai
tlist
ortre
atm
ent-a
s-usu
alco
ntro
lA
ctiv
eco
ntro
l
Intim
ate
partn
ervi
olen
ce/A
buse
Berm
udez
etal
.,20
13—
——
——
Dut
ton
etal
.,20
13Ki
mbr
ough
etal
.,20
10O
lder
adul
tsEr
nste
tal.,
2008
Cre
swel
leta
l.,20
12*
——
——
Gal
lego
s,H
oerg
er,
Talb
ot,K
rasn
er,e
tal
.,20
13*
Gal
lego
s,H
oerg
er,
Talb
ot,M
oyni
han,
etal
.,20
13*
Szan
ton
etal
.,20
11M
oyni
han
etal
.,20
13*
Youn
get
al.,
2010
Pers
onal
itydi
sord
ersy
mpt
oms
—N
yklíc
ek,v
anBe
ugen
,&D
enol
let,
2013
*—
——
—
Preg
nant
wom
en—
Viet
enet
al.,
2008
——
——
Pris
oner
sSa
mue
lson
etal
.,20
07—
——
——
Psor
iasi
s—
—Ka
bat-Z
inn
etal
.,19
98*
——
—
Postt
raum
atic
stres
sdi
sord
er/
Trau
ma
(am
ong
vete
rans
)
—Ke
arne
y,M
cDer
mot
t,et
al.,
2012
—N
iles
etal
.,20
12—
—
Kear
ney
etal
.,20
13
Smok
ing
Dav
iset
al.,
2007
*—
——
——
Som
atiz
atio
n—
—Fj
orba
ck,A
rend
t,et
al.,
2013
—Fj
orba
ck,C
arste
nsen
,et
al.,
2013
—
Stre
ssH
ölze
leta
l.,20
10*
——
——
—W
alac
het
al.,
2007
Stro
ke/T
raum
atic
brai
nin
jurty
Azu
lay
etal
.,20
13*
Joha
nsso
net
al.,
2012
*—
——
—Bé
dard
etal
.,20
03Bé
dard
etal
.,20
05Su
bsta
nce
abus
eC
arro
llet
al.,
2008
——
——
—La
nge
etal
.,20
11M
arcu
set
al.,
2003
*Va
llejo
etal
.,20
09Te
ache
rsG
old
etal
.,20
10—
——
——
Tinn
itus
Gan
set
al.,
2013
——
——
—Tr
ansp
lant
Gro
sset
al.,
2004
—G
ross
etal
.,20
10—
——
Krei
tzer
etal
.,20
05
*St
udie
sth
atin
tegr
ate
basi
cre
sear
chas
part
ofla
ter
stage
inte
rven
tion
studi
esar
ede
note
dat
the
rele
vant
late
rsta
gew
ithan
aste
risk.
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
603October 2015 ● American Psychologist

Multiple meta-analytic studies including MBSR andMBCT trials have been published in recent years (Goyal etal., 2014; Hofmann, Sawyer, Witt, & Oh, 2010; Piet &Hougaard, 2011), with generally convergent findings.These meta-analyses have been focused largely on thequestion, “do MBIs work?” And, although most have em-phasized problems with the methodological quality ofmany individual studies, the overall consensus appears tobe “yes.” We concur with these interpretations, and build-ing on this foundation, we think the field is ripe for con-sidering the evidence base from the broader “bird’s eyeview” of the NIH stage model.
Figure 1 illustrates the core stages of the NIH modelwith the color saturation of each stage corresponding to theproportional amount of published research on MBCT andMBSR, considered together, at each given stage. The NIHstage model was proposed not as a fixed and linear set ofsteps to take in chronological order, but rather as a set ofoverlapping and mutually informing points along a contin-uum of research. Within this context, there are indicationsthat some stages and links between stages warrant greaterattention. The greatest focus of activity in the MBI field hasbeen dedicated to the development and exploration of ap-plications of MBIs with novel populations and target prob-lems. This pattern may be implicit in the early developmentof a field; however, it also represents a point of vulnera-bility. If the weight of clinical and scientific attention
remains devoted to increasing the range of applicationsrather than the depth of the evidence base, public healthimpact may be limited. Or, put simply, with reference toTables 1 and 2, it would be misguided to prioritize increas-ing the number of rows in each table, without emphasizingsimultaneously the development and integration of studiesacross the columns. Here, we offer a set of seven recom-mendations for increasing the public health impact of thiswork.
Stage-Based Recommendations toIncrease the Public Health Impact ofMBI ResearchRecommendation 1. Attend to the Basics:Specify Intervention Targets and PopulationsA close link between basic and intervention research existsin the foundation of clinical innovation and research onMBIs. For example, the first application of mindfulnessmeditation for the prevention of depression was rooted inbasic research on the nature of depressive relapse. In suchstudies, formerly depressed patients were compared tohealthy controls before and after a sad mood induction;formerly depressed patients showed greater increases indepressogenic thinking styles, suggesting that a history ofdepression was associated with increased access to depres-sive cognition in the context of mild sad mood (Teasdale,1988). Moreover, studies suggested that such increasedaccess prospectively predicted relapse risk (Segal et al.,2006). This work identified a potential target for interven-tion (i.e., ruminative emotion-linked cognitive processes),a population for whom this target was relevant and identi-fiable (i.e., individuals with histories of recurrent depres-sion), and a logical basis for the application of mindfulnessmeditation (i.e., to enable regulation of dysphoric moodstates in ways that inhibited the activation of habitual,mood-linked mental content; Teasdale, Segal, & Williams,1995).
The rapid proliferation of new potential indications forMBIs risks neglecting the link between Stage 0 and sub-sequent stages. In an era in which specification of clearintervention targets and mediating processes of change isincreasingly prioritized, failure to attend to the “basics”may undermine the potential public health impact of re-search on MBIs. A glance at the range of problems forwhich MBIs are being applied suggests possible vulnera-bility in this regard. For example, recent studies haveextended MBCT to other populations and problems (e.g.,bipolar disorder, psychosis) based on the evidence of care-gaps in the psychosocial treatment of these groups; how-ever, such efforts have less frequently identified the targetsthat mindfulness practice is intended to engage, or thedegree to which the interventions alter (or fail to alter) suchtargets when they achieve their intended clinical effects.Although intervention studies suggest that MBCT haspromise for such patients, the basic research necessary tosupport a rationale for “why” is often lacking (although,see final section for recent exceptions).
Figure 1Evidence Base for Mindfulness-Based Interventions(i.e., Mindfulness-Based Stress Reduction andMindfulness-Based Cognitive Therapy) MappedAccording to the Adapted National Institutes of HealthStage Model
Note. Recommended pathways between stages are represented with solidarrows; pathways that should be undertaken with caution are represented withdotted arrows. Color saturation represents the proportion of the total number ofpublished studies of mindfulness-based interventions mapped at a given stage,with the specific percentage indicated at each stage.
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
604 October 2015 ● American Psychologist

Moreover, our mapping indicates that only a smallnumber of studies have explored candidate mediators ormoderators of outcome, and of these, even fewer havetested mediation formally or incorporated recent methodsthat move the field closer to a personalized medicine frame-work in which patient characteristics determine treatmentselection (e.g., DeRubeis et al., 2014). Exceptions includethe work of Vøllestad, Sivertsen, and Nielsen (2011), whodescribe a well-conceived analysis in which mindfulnessstatistically mediated changes in anxiety symptoms follow-ing MBSR, but owing to the absence of temporal prece-dence for these changes did not demonstrate true media-tion. Such efforts represent an advance beyond work thatsimply reports the magnitude of pre–post interventionchange of a potential mediator. Arch and Ayers (2013)provide another instructive example, in which patients withanxiety disorders were randomized to MBSR or cognitive–behavioral therapy, with results indicating the response tointervention depended in part on baseline depressive symp-tom severity comorbidity and anxiety sensitivity. Similarly,studies of MBCT suggest that effects may be moderated byvulnerability factors, including recurrent depressive epi-sode histories (Ma & Teasdale, 2004; Teasdale et al., 2000)and residual depressive symptoms (Segal et al., 2010).
Underemphasizing links to basic research and precisespecification of for whom and how a treatment works riskssituating the study of MBI less as science and more aspseudoscience in which mindfulness is seen as a panaceafor all problems. Absence of clear attention to both “bound-ary conditions” and “scientific plausibility” is often cited asa hallmark of pseudoscience (Lilienfeld, Lynn, & Lohr,2003). Future work on MBI will be strengthened by attend-ing to these requirements—specifying both what mindful-ness is not likely to help and, not only predicting that anMBI will produce clinical benefit, but also specifying plau-sible mechanisms by which such benefits are attained.Moreover, extensions of MBSR, MBCT, and other MBIs tonew populations and conditions may require modificationsand tailoring to address their salient pathogenic mecha-nisms; such work represents the heart of Stage I but re-quires close and iterative links to Stage 0 methods andconcepts. Many basic research studies have investigatedcorrelates of mindfulness meditation (see Lutz et al., 2015)and provide methods or proxy markers to consider forintegration in applied trials. In Tables 1 and 2, studiesidentified with asterisks in Stages I–V provide examples ofmovement to such integration.
Recommendation 2. Do Not ConflatePromise With EfficacyIn contrast to the relative paucity of Stage 0 studies, re-search efforts have saturated heavily Stage I. The nonran-domized and, most often, uncontrolled studies, mappedhere at Stage I, clearly support valid excitement about theuse of MBI in clinical settings across a wide range of targetpopulations and problems. This excitement, however, mustbe tempered, given the risk that the field will fail to ad-vance if Stage I research is seen as a sufficient “green light”to proceed to broad dissemination and implementation of
MBI, or if the field “stalls out” by simply amassing morestudies at Stage I. Thus, the NIH stage model underscoresthe value of the full cycle of research stages, and notablydoes not specify a direct pathway from Stage I to Stages IVor V. Among problems targeted by MBCT, only work ondepression and comorbid health and mental health condi-tions, and within MBSR studies, primarily work with pa-tients with cancer, show incremental progression fromStage I to subsequent stages. The sheer quantity of prom-ising uncontrolled studies cannot substitute for later stagestudies; researchers, practitioners, and the public must becautious not to conflate the fact that many studies exist atStage I with indications of efficacy or effectiveness.
Moreover, as the field focuses more on the incremen-tal progression of MBI research from Stage I to V, it willbe important to consider directly indications of both failureand harm. In fact, a “failed” individual trial in which theMBI does not outperform the comparator intervention maybe a “success” when viewing the advancement of the fieldbroadly. Such findings help to inform the “boundary con-ditions” necessary for scientific progress and strengthen thepathway between Stage I and Stage 0, in which failures inone context create fertile ground in the other. The field willbe well served by frank acknowledgment of failure ratherthan obscuring such findings with multiple or ambiguousprimary and secondary outcomes or falling victim to the“file drawer” problem in which failed trials simply are notpublished. An instructive example is provided by Craigie,Rees, Marsh, and Nathan (2008) regarding the relativelypoor performance of MBCT in an open trial when com-pared to benchmarks of cognitive–behavioral therapy inother studies targeting generalized anxiety disorder. Theyhighlight valuable questions that can be “sent back” toStage 0 about potential maintaining factors in generalizedanxiety disorder. In addition to addressing directly “failed”trials, it also will be important to consider potential harmfuleffects of MBI. With the exception of recent work byBritton and colleagues (2012), it is notable that few publi-cations have reported data on adverse effects of MBI. Thisarea will be important for future investigators to addressdirectly, consistent with recommendations for psychother-apy interventions generally (e.g., Dimidjian & Hollon,2010).
Recommendation 3. Engage the ThornyQuestion of Clinician TrainingTo be considered “complete,” Stage I work requires atten-tion not only to questions of “promise” but also to thethorny questions of clinician training. These questions areof particular salience given the unique expectations forMBI instructors, which require a personal practice in mind-fulness meditation in addition to professional training in theclinical approach. This element may challenge future im-plementation efforts and has received surprisingly littleattention to date in the scientific literature. Operationalizingthis requirement and developing scaffolding resources forinstructors learning MBIs are gaps that exist currently atStage I. In fact, few studies have examined measures ofinstructor fidelity (R. S. Crane et al., 2013; Segal, Teasdale,
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
605October 2015 ● American Psychologist

Williams, & Gemar, 2002). The lack of attention to devel-oping formal measures, methods, and standards for deter-mining instructor quality may have its roots in core guidingprinciples about how MBIs are best delivered. For exam-ple, in a cautionary note about overreliance on formalguidelines, Kabat-Zinn (2011) expressed,
It has always felt to me that MBSR is at its healthiest and bestwhen the responsibility to ensure its integrity, quality, and stan-dards of practice is being carried by each MBSR instructor him orherself . . . to keep it very real and close to our everyday experi-ence held in awareness with kindness and discernment. (p. 295)
It will be important for the field to grapple directly withtensions that may exist in the very foundation of the sci-entific study of MBI and that may be accentuated as re-search on these interventions expands from early Stage Iwork to larger, more distributed later stage studies.
Recommendation 4. It’s Time to Get SpecificAbout the Specific Effects of MBIThe main strength of Stage II research is the use of ran-domized designs and intervention controls that supportinference about causality. As Tables 1 and 2 illustrate, suchwork has been conducted with a greater emphasis on ran-domized comparisons to WLC or TAU than to activecontrols. Such designs permit valid inference aboutwhether the MBI produces an effect on the measuredoutcome but not about what, specifically, is driving theeffect. MBIs are multimodal interventions. Although itoften is assumed that mindfulness meditation is the “activeingredient,” findings are equivocal.
Segal et al. (2010) compared MBCT to maintenancepharmacotherapy, the current standard of care for prevent-ing depressive relapse, and a pill placebo condition. Thelack of differences in relapse prevention between MBCTand maintenance pharmacotherapy among patients withresidual depressive symptoms suggested that MBCT offersbenefit on par with pharmacological treatment, and thesuperiority of MBCT relative to the placebo control sug-gested that such benefits are specific to components ofMBCT rather than factors common to clinical care thatwere also present in the placebo condition—a crediblerationale, clear guidelines for action, expectancies for im-provement, and a positive working alliance with a treat-ment provider. However, this comparison did not controlfor other relevant dimensions such as time with clinicians,group support, and specific home practices. Thus, the ques-tion remains: is the mindfulness meditation componentspecifically efficacious?
MBCT showed no significant benefit as compared toan educational control for caregivers of dementia patients,although both active treatments outperformed a respite onlycontrol (Oken et al., 2010). In contrast, MBCT demon-strated superiority to psychoeducational controls for treat-ment refractory depressed patients (Chiesa, Mandelli, &Serretti, 2012), and specific benefits on some outcomes ascompared to a relaxation control for patients with tinnitus(Philippot, Nef, Clauw, de Romree, & Segal, 2012).
Studies of MBSR provide similarly complex findings,reporting failure to outperform an active control on primaryoutcomes but often mixed results on secondary outcomes.Studies of MBSR among patients with chronic pain havereported no significant differences on subjective reports,such as pain intensity, distress, quality of life, and mood, ascompared to a multidisciplinary pain intervention (Wong etal., 2011) or active control or waitlist (Schmidt et al.,2011). A comparison of MBSR and stress managementeducation among patients with generalized anxiety disorderalso found no evidence of superiority for MBSR on theprimary outcome of anxiety symptom severity, but reportedadvantage on secondary anxiety outcomes (Hoge et al.,2013). Finally, among nonclinical participants, comparisonbetween MBSR and an active control, the Health Enhance-ment Program, which was matched to MBSR in elementsthat were known to reduce stress but were not tied to thepractice of mindfulness (e.g., group support, physical ac-tivity), indicated no significant benefit associated withMBSR on subjective reports of wellbeing, some benefit ona behavioral pain task (MacCoon et al., 2012), and benefiton biological indices of stress provoked inflammatory re-sponse (Rosenkranz et al., 2013).
Interpretation of the mixed findings from studies usingactive control conditions is complicated even further by thefact that few active controls have been truly matched toMBSR or MBCT on all components except mindfulnessmeditation. For example, the degree to which participantsin control conditions are provided with equivalent supportfor home practice is difficult to determine from manypublished reports; MBSR and MBCT protocols typicallyinclude written and audio guide support for daily homepractice and it is not clear whether active controls matchthis element. Moreover, although some active controlscarefully match the frequency and duration of sessions(e.g., Philippot et al., 2012), others are structurally differ-ent, involving shorter sessions (e.g., Y. W. Kim et al.,2009). Also, few studies have tested the degree to whichinstructors find the interventions they are delivering to becredible, thus introducing the possibility of allegiance ef-fects contributing to differences in outcomes across groups.Even comprehensive active controls such as the HealthEnhancement Program introduce different teachers for eachmodule of the curriculum, unlike MBSR or MBCT inwhich the same teacher guides the group for the entire eightsessions (MacCoon et al., 2012). The challenge of devel-oping credible and structurally equivalent psychosocialprotocols to control for common factors is not new topsychotherapy research, but it is an important task for thefield in order to answer clearly the question of whethermindfulness meditation is an “active ingredient” of MBI.This recommendation is consistent with a recent meta-analysis of the clinical applications of meditation (Goyal etal., 2014), which reported small to moderate effects andlittle evidence of specific efficacy.
Testing the assumption that mindfulness meditation isspecifically efficacious is necessary but not sufficient toadvance the field. It is important also to understand moreprecisely about the nature of mindfulness meditation prac-
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
606 October 2015 ● American Psychologist

tice itself. Just how much meditation (if any) is required toachieve clinical benefit? The studies that touch upon thisquestion are mapped currently at Stage I because they relylargely on post hoc analyses of the association betweenpractice time or class attendance and change in symptomsor self-reported mindfulness skill. Findings are mixed, withsome studies supporting an association between amount ofpractice and clinical outcomes (Beddoe & Murphy,2004; Carmody & Baer, 2008; Collard, Avny, & Boni-well, 2008; del Re, Flückiger, Goldberg, & Hoyt, 2013;Farb, Segal, & Anderson, 2013; Gross et al., 2004;Rosenzweig et al., 2010; Shapiro, Bootzin, Figueredo,Lopez, & Schwartz, 2003; Shapiro, Jazaieri, & Goldin,2012), but not all (Carlson, Speca, Patel, & Goodey,2004; Dobkin & Zhao, 2011; A. Hopkins & Proeve,2013; MacCoon et al., 2012). The field requires Stage IIrandomized controlled trials that manipulate dosage orintervention duration as a primary aim. Similarly, basicresearch studies that examine the validity of methods ofassessing practice time and quality are essential. Suchfindings will bear directly on subsequent stages of research.One can easily imagine patients, referring providers, andhealth plan administrators asking questions such as, “Canwe deliver this in six sessions instead of eight?” or, “Doesit really matter if I practice 10 min a day rather than 45min?” Stage II studies are well poised to answer suchquestions.
Recommendation 5. Consider Skipping tobut Not Over Stage IIIStage III has been underemphasized in studies of MBI(and clinical psychological science generally). As de-fined by Onken et al. (2014), a Stage III study is “awell-controlled, internally valid study in a communitysetting with community therapists/providers” (p. 29).This stage of work has two primary functions in thedomain of MBI. First, it is well suited for efficacy testsof the type of self-guided materials that are widelyavailable, including workbooks and audio guides, and isrelevant for testing future applications of MBI usingweb-based or other technology-based delivery tools.Such interventions do not require clinician training ma-terials because they target the patient directly; thus, itmay be warranted, in some cases, for interventions toproceed directly from Stage I to Stage III. In such cases,the recommendations regarding appropriate control con-ditions at Stage II are of particular importance at StageIII. Stage III studies of self-guided materials may benefitfrom comparison to TAU to establish evidence of equiv-alent or superior benefit to standard of care in varioushealthcare domains. However, comparisons to activecontrols are critical to validate the specific efficacy ofthe mindfulness components over and above expectan-cies, contact time, and other potentially active ingredi-ents. Although there were insufficient studies at Stage IIIto allow us to map them at this level of granularity, wethink such distinctions are critical for the future devel-opment of the field. Second, tests of efficacy of instruc-tor delivered MBI in the community will help to deter-
mine whether results from Stage II studies “hold up”when the MBI is delivered in routine settings by com-munity providers. Thus, researchers are cautionedagainst “skipping” this stage of work; it is crucial forinforming which interventions justify movement toStage IV.
Of the studies we reviewed, only two were identi-fied that approached the criteria for Stage III. Thisclassification is arguable given the pilot nature of thework and the hybrid use of community and researchclinicians; however, both studies provide instructive ex-amples of the ways in which an MBI can be delivered inan innovative manner directly to recipients in the com-munity. N. J. Thompson et al. (2010) compared “dis-tance delivery” of MBCT via telephone or Internet forpatients with epilepsy and depressive symptoms (N �40), as compared to WLC, and the intervention wascofacilitated by a layperson with epilepsy and a master’sof public health student. Similarly, Niles and colleagues(2012) conducted a feasibility test (N � 33) of a mixeddelivery format in which veterans with posttraumaticstress disorder were randomized to either an MBSRintervention or a psychoeducation control, both of whichincluded two in person and six telephone-based sessions.
Recommendation 6. Efficacy Is Necessarybut Not Sufficient for EffectivenessOnly two trials of MBCT and one of MBSR were pub-lished prior to 2014 that addressed questions of effec-tiveness, with two focused specifically on economicoutcomes. Specifically, Kuyken et al. (2008) examinedthe effects of MBCT as compared to maintenance phar-macotherapy among patients treated in primary care,with results suggesting comparable relapse preventionand cost effectiveness as well as advantage of MBCT onindices of reducing residual depressive symptoms, psy-chiatric comorbidity, and quality of life. van Ravesteijn,Lucassen, Bor, van Weel, and Speckens (2013) exam-ined the cost-effectiveness of MBCT compared withTAU among patients with persistent medically unex-plained symptoms, with results indicating lower hospitalcosts and higher mental healthcare costs among patientsreceiving MBCT. Fjorback and colleagues (2013) alsoexamined economic outcomes of MBSR as compared tocare as usual for somatic symptom disorders, and sig-nificant benefits for MBSR were reported on disabilitypension outcomes.
Studies like these make good use of the “care-as-usual” control groups that can be a progress-limitingfactor for earlier stage work. The frequent calls for morerigorous active control groups and caution about care-as-usual comparisons miss the public health relevance ofsuch designs at Stage IV. Care-as-usual comparisons,particularly in the context of healthcare settings in whichsuch care can be precisely described, allow us to deter-mine whether an MBI adds incremental benefit to whatis available. Such studies provide a necessary foundationfor Stage IV and V work.
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
607October 2015 ● American Psychologist

Recommendation 7. Beware of DevelopingOrphan Innovations, Falling Off theImplementation Cliff, and Getting Caught in“Implementation Limbo”
Only three studies, two of which are purely descriptive,addressed as a primary aim questions relevant to the dis-semination or broad implementation of MBI. Specifically,R. S. Crane and Kuyken (2013) conducted a survey withparticipants in a workshop on implementation of MBCTand an online national survey of MBCT teachers and stake-holders. Results described a range of barriers and facilita-tors to MBCT implementation, including structural, polit-ical, cultural, educational, emotional and physical ortechnological factors. Lau and colleagues (2012) examinedpreferences of employees from large healthcare organiza-tions for MBCT targeting depression relapse preventiondelivered by in-person group, online group, in-person in-dividual, and telephone-based individual format. Finally,Patten and Meadows (2009) examined data from the Ca-nadian Community Health Survey to construct a simulationmodel that estimated the population density required tosupport sustained delivery of in-person MBCT. Resultssuggested that implementation of such group-based in-person approaches may be challenging in small populationcenters.
The lack of attention to Stage V work is a serious gapin an effort to develop a clinical science of MBI. Currentestimates suggest that, at best, only one in three people whostruggle with mental health problems will receive “at leastminimally adequate treatment” (Wang et al., 2005). Thereis a tremendous unmet need for care. If MBI approachesare to have a meaningful impact, they must overcome notonly barriers to dissemination and implementation that arecommon to other approaches (e.g., service costs, waitinglists, and distance to access intervention), but also uniquebarriers due to instructor competencies.
Given its early stage of development as a field, re-searchers and practitioners of MBIs may benefit from les-sons learned in the study of efforts to disseminate andimplement other psychosocial interventions. Three cau-tions are particularly salient. First, based on their experi-ence developing and disseminating a method of redistrib-uting “edible but not sellable” fresh produce to low incomepopulations, Evans and Clarke (2011) describe the problemof “orphan innovations,” in which effort is dedicated to thedesign and initial testing of an intervention but little care isallocated to the task of studying the reach of the interven-tion to contexts of need. Second, Weisz, Ng, and Bearman(2014) refer to the “implementation cliff” to describe the“voltage drop” that often occurs as interventions movethrough the clinical science process. As interventions are“scaled up” for dissemination in community settings orare delivered in successive generations following the orig-inal intervention developer, outcomes suffer. Third, Weisz(2014) also describes the problem of “implementationlimbo” in which resource constraints set the “bar” fortraining providers at ever lower levels:
If there is no evidence that 4 days of expert-led training, andsubsequent individual clinician supervision, are required to main-tain fidelity and benefit, then why not reduce cost with a 2-daytraining and group supervision and have local clinical staff con-duct the training and supervision? (p. 60)
Although it is too early to render definitive judgment on theclinical science of MBI, the saturation of studies at Stage Iand Stage II using WLC or TAU controls, and the relativepaucity of studies at later stages, highlights the risk ofneglecting promising interventions as “orphans” early inthe research process. Moreover, the relative lack of atten-tion to studying methods of training instructors that can bebroadly implemented may make MBI approaches vulnera-ble to both the implementation cliff and limbo. Fortunately,the emerging field of MBI also stands to learn from thesuccesses of others. Recent discussions have focused, inparticular, on the model of “disruptive innovation,” inwhich new technologies may be integrated in the service ofincreasing reach and access of MBI. Recommendationswithin general psychotherapy domains have included theexamination of novel delivery formats such as self-man-agement and self-help formats, brief or more parsimoniousadaptations, technology and media-driven delivery for-mats, and integration within broader healthcare packages(Kazdin & Blase, 2011; Rotheram-Borus, Swendeman, &Chorpita, 2012). Such avenues may represent great promisefor the dissemination and implementation of MBI; how-ever, they are likely also to raise complex questions that thefield must tackle. As Simon and Ludman (2009) note in adiscussion of disruptive innovation for cognitive–behav-ioral treatments,
Traditional therapists might be horrified by the prospect of anoverseas cognitive behavioral call center or live-chat center, avail-able whenever patients choose. But the expectations of health-care providers are not the same as evidence. And the evidence thatmatters concerns clinical benefit and economic value to patients,rather than appeal or value to providers. (p. 595).
It will be essential for clinical innovators and researchers toexamine methods of delivery for MBI that will providesuch evidence.
Indications of PromiseThere are encouraging indications that the field is movingin the directions highlighted in this review. Although ourcomprehensive mapping was limited to studies publishedthrough 2013, the field is advancing rapidly, and an exam-ination of notable studies published since 2014 indicatessignificant advances in three domains.
First, we find indicators that the field is becomingmore programmatic in its approach by anchoring clinicalintervention in basic research that specifies clear targets ofintervention and by testing proposed mechanisms ofchange. This is evident, for example, in recent work onsubstance use disorders that represent novel next-genera-tion interventions combining elements of MBSR or MBCT,singly, or with other interventions in novel ways. Forexample, Garland and colleagues (2014) tested both clini-cal outcomes and mediators of an MBI developed specifi-cally for chronic pain and prescription opioid misuse(mindfulness-oriented recovery enhancement) in the con-
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
608 October 2015 ● American Psychologist

text of a Stage II randomized clinical trial with an activecontrol (supportive group therapy). It may be valuable touse the mapping approach undertaken here to chart thedevelopment of these next-generation MBIs and the waysin which the structure and content of the interventions aremodified to fit the nature of the target problem or popula-tion. Moreover, an increased recent emphasis on identify-ing mediators of change in MBI represents an importantstep in advancing research in an integrated and systematicmanner (Gu, Strauss, Bond, & Cavanagh, 2015; van derVelden et al., 2015).
Second, more studies are incorporating active controlconditions that can help to address questions of specificefficacy. J. M. G. Williams et al. (2014) compared MBCTto TAU and to a cognitive psychoeducation program de-veloped to emphasize the didactic elements of relapseprevention without the experiential mindfulness practice.The results indicated no difference in relapse rates over a1-year follow-up among the three groups—a finding thatchallenges the specific efficacy of the mindfulness medita-tion component of MBCT. A subgroup analysis of patientswith histories of childhood trauma, however, indicatedsignificant benefit for MBCT. It is possible that MBCTmay show specific benefit for more vulnerable individuals,as was the case in the original studies that examined inter-vention differences by number of prior episodes (Ma &Teasdale, 2004; Teasdale et al., 2000). Although cautionshould be exercised in the interpretation of post hoc sub-group analyses, such findings may warrant “returning” towork at Stage 0 to help understand the nature of suchvulnerabilities, including mechanisms that might be pref-erentially addressed through training in mindfulness med-itation for such individuals.
Third, given that the stage model was developed tomaximize the public health impact of psychosocial treat-ments, it is encouraging that investigators are extendingpromising work at Stage I and II to examine questions ofeffectiveness, dissemination, and implementation. Thework of Bowen et al. (2014) provides an excellent exampleof rigorous movement toward Stage III research in whichthe MBI developed for preventing relapse in substanceabuse disorders (mindfulness-based relapse prevention)was tested in a randomized clinical trial with comparison toan active control (cognitive–behavioral relapse prevention)and TAU. This study represents a hybrid of Stage II and IIIresearch because research clinicians delivered the 8-weekintervention in community chemical dependency treatmentfacilities. Moreover, although TAU comparison groupshave been highly heterogeneous in prior studies, this studyrepresents an advance by implementing the study in thecontext of a specific healthcare setting that allowed TAU tobe clearly defined and measured. The use of comparisonconditions that address questions of high relevance tohealthcare consumers also signals an important advance.For example, the trial comparing MBCT (with support todiscontinue antidepressant medication) to maintenance an-tidepressant medication (Kuyken et al., 2015) has the po-tential to address the questions that are at the forefront formany patients seeking care. Specifically, patients and pro-
viders want to know how the MBI compares to otheravailable options. Findings from Kuyken et al. (2015)indicate that relapse rates are statistically equivalent inMBCT and maintenance antidepressant medication, thecurrent standard of care for recurrent depression. Finally,the potential for broad dissemination via web-based deliv-ery also may help to accelerate the pace of Stage III–Vresearch (Boettcher et al., 2014; Dimidjian et al., 2014).
SummaryThe science and practice of MBI has reached an importantpoint in its development. The last decade has witnessed anexponential rate of increase in the number of studies andthe breadth of clinical problems and populations targeted.We contend that the public health impact of this work islikely to be enhanced by situating work on MBI in abroader framework of clinical psychological science. Do-ing so highlights important lessons and gaps in our currentevidence base. Simply accumulating a greater number ofthe same types of studies without addressing such gaps isunlikely to advance the field. Although there are indica-tions from recent studies that the field is moving in apositive direction, an integrated and systematic approach tocore research questions, to the methodological quality ofindividual studies at each stage, and to increasing logicallinks among the stages will enhance our ability to impactpositively the mental health needs of individuals and com-munities.
REFERENCES
Abercrombie, P. D., Zamora, A., & Korn, A. P. (2007). Lessons learned:Providing a mindfulness-based stress reduction program for low-in-come multiethnic women with abnormal pap smears. Holistic NursingPractice, 21, 26–34. http://dx.doi.org/10.1097/00004650-200701000-00006
Alberts, H. J., Thewissen, R., & Raes, L. (2012). Dealing with problem-atic eating behaviour. The effects of a mindfulness-based interventionon eating behaviour, food cravings, dichotomous thinking and bodyimage concern. Appetite, 58, 847–851. http://dx.doi.org/10.1016/j.appet.2012.01.009
Allen, M., Bromley, A., Kuyken, W., & Sonnenberg, S. J. (2009). Par-ticipants’ experiences of mindfulness-based cognitive therapy: “Itchanged me in just about every way possible.” Behavioural andCognitive Psychotherapy, 37, 413–430. http://dx.doi.org/10.1017/S135246580999004X
Altschuler, A., Rosenbaum, E., Gordon, P., Canales, S., & Avins, A. L.(2012). Audio recordings of mindfulness-based stress reduction trainingto improve cancer patients’ mood and quality of life—A pilot feasibilitystudy. Supportive Care in Cancer, 20, 1291–1297. http://dx.doi.org/10.1007/s00520-011-1216-7
Andersen, S. R., Würtzen, H., Steding-Jessen, M., Christensen, J., Ander-sen, K. K., Flyger, H., . . . Dalton, S. O. (2013). Effect of mindfulness-based stress reduction on sleep quality: Results of a randomized trialamong Danish breast cancer patients. Acta Oncologica, 52, 336–344.http://dx.doi.org/10.3109/0284186X.2012.745948
Anderson, N. D., Lau, M. A., Segal, Z. V., & Bishop, S. R. (2007).Mindfulness-based stress reduction and attentional control. ClinicalPsychology & Psychotherapy, 14, 449–463. http://dx.doi.org/10.1002/cpp.544
Arch, J. J., & Ayers, C. R. (2013). Which treatment worked better forwhom? Moderators of group cognitive behavioral therapy versusadapted mindfulness-based stress reduction for anxiety disorders. Be-haviour Research and Therapy, 51, 434–442. http://dx.doi.org/10.1016/j.brat.2013.04.004
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
609October 2015 ● American Psychologist

Arch, J. J., Ayers, C. R., Baker, A., Almklov, E., Dean, D. J., & Craske,M. G. (2013). Randomized clinical trial of adapted mindfulness-basedstress reduction versus group cognitive behavioral therapy for hetero-geneous anxiety disorders. Behaviour Research and Therapy, 51, 185–196. http://dx.doi.org/10.1016/j.brat.2013.01.003
Azulay, J., Smart, C. M., Mott, T., & Cicerone, K. D. (2013). A pilot studyexamining the effect of mindfulness-based stress reduction on symp-toms of chronic mild traumatic brain injury/postconcussive syndrome.The Journal of Head Trauma Rehabilitation, 28, 323–331. http://dx.doi.org/10.1097/HTR.0b013e318250ebda
Baer, R. A., Carmody, J., & Hunsinger, M. (2012). Weekly change inmindfulness and perceived stress in a mindfulness-based stress reduc-tion program. Journal of Clinical Psychology, 68, 755–765. http://dx.doi.org/10.1002/jclp.21865
Baer, R. A., Fischer, S., & Huss, D. B. (2005a). Mindfulness and accep-tance in the treatment of disordered eating. Journal of Rational-Emotive& Cognitive-Behavior Therapy, 23, 281–300. http://dx.doi.org/10.1007/s10942-005-0015-9
Baer, R. A., Fischer, S., & Huss, D. B. (2005b). Mindfulness-basedcognitive therapy applied to binge eating: A case study. Cognitiveand Behavioral Practice, 12, 351–358. http://dx.doi.org/10.1016/S1077-7229(05)80057-4
Bailie, C., Kuyken, W., & Sonnenberg, S. (2012). The experiences ofparents in mindfulness-based cognitive therapy. Clinical Child Psy-chology and Psychiatry, 17, 103–119. http://dx.doi.org/10.1177/1359104510392296
Barbosa, P., Raymond, G., Zlotnick, C., Wilk, J., Toomey, R., III, &Mitchell, J., III. (2013). Mindfulness-based stress reduction training isassociated with greater empathy and reduced anxiety for graduatehealthcare students. Education for Health: Change in Learning &Practice, 26, 9–14.
Barnhofer, T., Crane, C., Hargus, E., Amarasinghe, M., Winder, R., &Williams, J. M. G. (2009). Mindfulness-based cognitive therapy as atreatment for chronic depression: A preliminary study. Behaviour Re-search and Therapy, 47, 366–373. http://dx.doi.org/10.1016/j.brat.2009.01.019
Barnhofer, T., Duggan, D., Crane, C., Hepburn, S., Fennell, M. J. V., &Williams, J. M. G. (2007). Effects of meditation on frontal alpha-asymmetry in previously suicidal individuals. Neuroreport for RapidCommunication of Neuroscience Research, 18, 709–712. http://dx.doi.org/10.1097/WNR.0b013e3280d943cd
Bazarko, D., Cate, R. A., Azocar, F., & Kreitzer, M. J. (2013). The impactof an innovative mindfulness-based stress reduction program on thehealth and well-being of nurses employed in a corporate setting. Jour-nal of Workplace Behavioral Health, 28, 107–133. http://dx.doi.org/10.1080/15555240.2013.779518
Bédard, M., Felteau, M., Gibbons, C., Klein, R., Mazmanian, D., Fedyk,K., & Mack, G. (2005). A mindfulness-based intervention to improvequality of life among individuals who sustained traumatic brain inju-ries: One year follow-up. Journal of Cognitive Rehabilitation, 23,8–13.
Bédard, M., Felteau, M., Mazmanian, D., Fedyk, K., Klein, R., Richard-son, J., . . . Minthorn-Biggs, M. B. (2003). Pilot evaluation of amindfulness-based intervention to improve quality of life among indi-viduals who sustained traumatic brain injuries. Disability and Rehabil-itation: An International, Multidisciplinary Journal, 25, 722–731. http://dx.doi.org/10.1080/0963828031000090489
Beddoe, A. E., & Murphy, S. O. (2004). Does mindfulness decrease stressand foster empathy among nursing students? The Journal of NursingEducation, 43, 305–312.
Bergen-Cico, D., Possemato, K., & Cheon, S. (2013). Examining theefficacy of a brief mindfulness-based stress reduction (Brief MBSR)program on psychological health. Journal of American College Health,61, 348–360. http://dx.doi.org/10.1080/07448481.2013.813853
Bermudez, D., Benjamin, M. T., Porter, S. E., Saunders, P. A., Myers,N. A., & Dutton, M. A. (2013). A qualitative analysis of beginningmindfulness experiences for women with post-traumatic stress disorderand a history of intimate partner violence. Complementary Therapies inClinical Practice, 19, 104–108. http://dx.doi.org/10.1016/j.ctcp.2013.02.004
Biegel, G. M., Brown, K. W., Shapiro, S. L., & Schubert, C. M. (2009).Mindfulness-based stress reduction for the treatment of adolescent
psychiatric outpatients: A randomized clinical trial. Journal of Consult-ing and Clinical Psychology, 77, 855–866. http://dx.doi.org/10.1037/a0016241
Bieling, P. J., Hawley, L. L., Bloch, R. T., Corcoran, K. M., Levitan,R. D., Young, L. T., . . . Segal, Z. V. (2012). Treatment-specific changesin decentering following mindfulness-based cognitive therapy versusantidepressant medication or placebo for prevention of depressive re-lapse. Journal of Consulting and Clinical Psychology, 80, 365–372.http://dx.doi.org/10.1037/a0027483
Birnie, K., Garland, S. N., & Carlson, L. E. (2010). Psychological benefitsfor cancer patients and their partners participating in mindfulness-basedstress reduction (MBSR). Psycho-Oncology, 19, 1004–1009. http://dx.doi.org/10.1002/pon.1651
Birnie, K., Speca, M., & Carlson, L. E. (2010). Exploring self-compassionand empathy in the context of mindfulness-based stress reduction(MBSR). Stress and Health: Journal of the International Society for theInvestigation of Stress, 26, 359–371. http://dx.doi.org/10.1002/smi.1305
Boettcher, J., Aström, V., Påhlsson, D., Schenström, O., Andersson, G., &Carlbring, P. (2014). Internet-based mindfulness treatment for anxietydisorders: A randomized controlled trial. Behavior Therapy, 45, 241–253. http://dx.doi.org/10.1016/j.beth.2013.11.003
Bondolfi, G., Jermann, F., der Linden, M. V., Gex-Fabry, M., Bizzini, L.,Rouget, B. W., . . . Bertschy, G. (2010). Depression relapse prophylaxiswith mindfulness-based cognitive therapy: Replication and extension inthe Swiss health care system. Journal of Affective Disorders, 122,224–231. http://dx.doi.org/10.1016/j.jad.2009.07.007
Bostanov, V., Keune, P. M., Kotchoubey, B., & Hautzinger, M. (2012).Event-related brain potentials reflect increased concentration abilityafter mindfulness-based cognitive therapy for depression: A random-ized clinical trial. Psychiatry Research, 199, 174–180. http://dx.doi.org/10.1016/j.psychres.2012.05.031
Bowen, S., Witkiewitz, K., Clifasefi, S. L., Grow, J., Chawla, N., Hsu,S. H., . . . Larimer, M. E. (2014). Relative efficacy of mindfulness-basedrelapse prevention, standard relapse prevention, and treatment as usualfor substance use disorders: A randomized clinical trial. Journal of theAmerican Medical Association Psychiatry, 71, 547–556. http://dx.doi.org/10.1001/jamapsychiatry.2013.4546
Brady, S., O’Connor, N., Burgermeister, D., & Hanson, P. (2012). Theimpact of mindfulness meditation in promoting a culture of safety on anacute psychiatric unit. Perspectives in Psychiatric Care, 48, 129–137.http://dx.doi.org/10.1111/j.1744-6163.2011.00315.x
Bränström, R., Kvillemo, P., & Åkerstedt, T. (2013). Effects of mindful-ness training on levels of cortisol in cancer patients. Psychosomatics,54, 158–164. http://dx.doi.org/10.1016/j.psym.2012.04.007
Britton, W. B., Haynes, P. L., Fridel, K. W., & Bootzin, R. R. (2010).Polysomnographic and subjective profiles of sleep continuity beforeand after mindfulness-based cognitive therapy in partially remitteddepression. Psychosomatic Medicine, 72, 539–548. http://dx.doi.org/10.1097/PSY.0b013e3181dc1bad
Britton, W. B., Haynes, P. L., Fridel, K. W., & Bootzin, R. R. (2012).Mindfulness-based cognitive therapy improves polysomnographic andsubjective sleep profiles in antidepressant users with sleep complaints.Psychotherapy and Psychosomatics, 81, 296–304. http://dx.doi.org/10.1159/000332755
Britton, W. B., Shahar, B., Szepsenwol, O., & Jacobs, W. J. (2012).Mindfulness-based cognitive therapy improves emotional reactivity tosocial stress: Results from a randomized controlled trial. BehaviorTherapy, 43, 365–380. http://dx.doi.org/10.1016/j.beth.2011.08.006
Brotto, L. A., Erskine, Y., Carey, M., Ehlen, T., Finlayson, S., Heywood,M., . . . Miller, D. (2012). A brief mindfulness-based cognitive behav-ioral intervention improves sexual functioning versus wait-list controlin women treated for gynecologic cancer. Gynecologic Oncology, 125,320–325. http://dx.doi.org/10.1016/j.ygyno.2012.01.035
Campbell, T. S., Labelle, L. E., Bacon, S. L., Faris, P., & Carlson, L. E.(2012). Impact of mindfulness-based stress reduction (MBSR) on at-tention, rumination and resting blood pressure in women with cancer: Awaitlist-controlled study. Journal of Behavioral Medicine, 35, 262–271.http://dx.doi.org/10.1007/s10865-011-9357-1
Carlson, L. E., & Garland, S. N. (2005). Impact of mindfulness-basedstress reduction (MBSR) on sleep, mood, stress and fatigue symptoms
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
610 October 2015 ● American Psychologist

in cancer outpatients. International Journal of Behavioral Medicine, 12,278–285. http://dx.doi.org/10.1207/s15327558ijbm1204_9
Carlson, L. E., Speca, M., Faris, P., & Patel, K. D. (2007). One yearpre–post intervention follow-up of psychological, immune, endocrineand blood pressure outcomes of mindfulness-based stress reduction(MBSR) in breast and prostate cancer outpatients. Brain, Behavior, andImmunity, 21, 1038–1049. http://dx.doi.org/10.1016/j.bbi.2007.04.002
Carlson, L. E., Speca, M., Patel, K. D., & Goodey, E. (2003). Mindful-ness-based stress reduction in relation to quality of life, mood, symp-toms of stress, and immune parameters in breast and prostate canceroutpatients. Psychosomatic Medicine, 65, 571–581. http://dx.doi.org/10.1097/01.PSY.0000074003.35911.41
Carlson, L. E., Speca, M., Patel, K. D., & Goodey, E. (2004). Mindful-ness-based stress reduction in relation to quality of life, mood, symp-toms of stress and levels of cortisol, dehydroepiandrosterone sulfate(DHEAS) and melatonin in breast and prostate cancer outpatients.Psychoneuroendocrinology, 29, 448–474. http://dx.doi.org/10.1016/S0306-4530(03)00054-4
Carmody, J., & Baer, R. A. (2008). Relationships between mindfulnesspractice and levels of mindfulness, medical and psychological symp-toms and well-being in a mindfulness-based stress reduction program.Journal of Behavioral Medicine, 31, 23–33. http://dx.doi.org/10.1007/s10865-007-9130-7
Carmody, J., & Baer, R. A. (2009). How long does a mindfulness-basedstress reduction program need to be? A review of class contact hoursand effect sizes for psychological distress. Journal of Clinical Psychol-ogy, 65, 627–638. http://dx.doi.org/10.1002/jclp.20555
Carmody, J., Baer, R. A., Lykins, E., & Olendzki, N. (2009). An empiricalstudy of the mechanisms of mindfulness in a mindfulness-based stressreduction program. Journal of Clinical Psychology, 65, 613–626. http://dx.doi.org/10.1002/jclp.20579
Carmody, J., Crawford, S., & Churchill, L. (2006). A pilot study ofmindfulness-based stress reduction for hot flashes. Menopause, 13,760–769. http://dx.doi.org/10.1097/01.gme.0000227402.98933.d0
Carmody, J. F., Crawford, S., Salmoirago-Blotcher, E., Leung, K.,Churchill, L., & Olendzki, N. (2011). Mindfulness training for copingwith hot flashes: Results of a randomized trial. Menopause, 18, 611–620. http://dx.doi.org/10.1097/gme.0b013e318204a05c
Carmody, J., Reed, G., Kristeller, J., & Merriam, P. (2008). Mindfulness,spirituality, and health-related symptoms. Journal of PsychosomaticResearch, 64, 393–403. http://dx.doi.org/10.1016/j.jpsychores.2007.06.015
Carroll, D., Lange, B., Liehr, P., Raines, S., & Marcus, M. T. (2008).Evaluating mindfulness-based stress reduction: Analyzing stories ofstress to formulate focus group questions. Archives of PsychiatricNursing, 22, 107–109. http://dx.doi.org/10.1016/j.apnu.2007.12.004
Cebolla i Martí, A., & Barrachina, M. T. M. (2009). The effects ofmindfulness-based cognitive therapy: A qualitative approach. Psychol-ogy in Spain, 13, 9–16.
Chambers, S. K., Foley, E., Galt, E., Ferguson, M., & Clutton, S. (2012).Mindfulness groups for men with advanced prostate cancer: A pilotstudy to assess feasibility and effectiveness and the role of peer support.Supportive Care in Cancer, 20, 1183–1192. http://dx.doi.org/10.1007/s00520-011-1195-8
Chang, V. Y., Palesh, O., Caldwell, R., Glasgow, N., Abramson, M.,Luskin, F., . . . Koopman, C. (2004). The effects of a mindfulness-basedstress reduction program on stress, mindfulness self-efficacy, and pos-itive states of mind. Stress and Health: Journal of the InternationalSociety for the Investigation of Stress, 20, 141–147. http://dx.doi.org/10.1002/smi.1011
Chiesa, A., Mandelli, L., & Serretti, A. (2012). Mindfulness-based cog-nitive therapy versus psycho-education for patients with major depres-sion who did not achieve remission following antidepressant treatment:A preliminary analysis. The Journal of Alternative and ComplementaryMedicine, 18, 756–760. http://dx.doi.org/10.1089/acm.2011.0407
Cohen-Katz, J., Wiley, S., Capuano, T., Baker, D. M., Deitrick, L., &Shapiro, S. (2005). The effects of mindfulness-based stress reduction onnurse stress and burnout: A qualitative and quantitative study, Part III.Holistic Nursing Practice, 19, 78–86. http://dx.doi.org/10.1097/00004650-200503000-00009
Cohen-Katz, J., Wiley, S. D., Capuano, T., Baker, D. M., Kimmel, S., &Shapiro, S. (2005). The effects of mindfulness-based stress reduction on
nurse stress and burnout, Part II: A quantitative and qualitative study.Holistic Nursing Practice, 19, 26–35. http://dx.doi.org/10.1097/00004650-200501000-00008
Cohen-Katz, J., Wiley, S. D., Capuano, T., Baker, D. M., & Shapiro, S.(2004). The effects of mindfulness-based stress reduction on nursestress and burnout: A quantitative and qualitative study. HolisticNursing Practice, 18, 302–308. http://dx.doi.org/10.1097/00004650-200411000-00006
Collard, P., Avny, N., & Boniwell, I. (2008). Teaching mindfulnessbased cognitive therapy (MBCT) to students: The effects of MBCTon the levels of mindfulness and subjective well-being. CounsellingPsychology Quarterly, 21, 323–336. http://dx.doi.org/10.1080/09515070802602112
Collip, D., Geschwind, N., Peeters, F., Myin-Germeys, I., van Os, J., &Wichers, M. (2013). Putting a hold on the downward spiral of paranoiain the social world: A randomized controlled trial of mindfulness-basedcognitive therapy in individuals with a history of depression. PLoSONE, 8, e66747. http://dx.doi.org/10.1371/journal.pone.0066747
Cordon, S. L., Brown, K. W., & Gibson, P. R. (2009). The role of mindful-ness-based stress reduction on perceived stress: Preliminary evidence forthe moderating role of attachment style. Journal of Cognitive Psychother-apy, 23, 258–269. http://dx.doi.org/10.1891/0889-8391.23.3.258
Craigie, M. A., Rees, C. S., Marsh, A., & Nathan, P. (2008). Mindfulness-based cognitive therapy for generalized anxiety disorder: A preliminaryevaluation. Behavioural and Cognitive Psychotherapy, 36, 553–568.http://dx.doi.org/10.1017/S135246580800458X
Crane, C., Barnhofer, T., Duggan, D. S., Hepburn, S., Fennell, M. V., &Williams, J. M. G. (2008). Mindfulness-based cognitive therapy andself-discrepancy in recovered depressed patients with a history ofdepression and suicidality. Cognitive Therapy and Research, 32, 775–787. http://dx.doi.org/10.1007/s10608-008-9193-y
Crane, C., & Williams, J. M. G. (2010). Factors associated with attritionfrom mindfulness-based cognitive therapy in patients with a history ofsuicidal depression. Mindfulness, 1, 10–20. http://dx.doi.org/10.1007/s12671-010-0003-8
Crane, C., Winder, R., Hargus, E., Amarasinghe, M., & Barnhofer, T.(2012). Effects of mindfulness-based cognitive therapy on specificity oflife goals. Cognitive Therapy and Research, 36, 182–189. http://dx.doi.org/10.1007/s10608-010-9349-4
Crane, R. S., Eames, C., Kuyken, W., Hastings, R. P., Williams, J. M.,Bartley, T., . . . Surawy, C. (2013). Development and validation of theMindfulness-Based Interventions: Teaching Assessment Criteria(MBI:TAC). Assessment, 20, 681– 688. http://dx.doi.org/10.1177/1073191113490790
Crane, R. S., & Kuyken, W. (2013). The implementation of mindful-ness-based cognitive therapy: Learning from the U.K. health serviceexperience. Mindfulness, 4, 246–254. http://dx.doi.org/10.1007/s12671-012-0121-6
Creswell, J. D., Irwin, M. R., Burklund, L. J., Lieberman, M. D., Arevalo,J. M., Ma, J., . . . Cole, S. W. (2012). Mindfulness-based stressreduction training reduces loneliness and pro-inflammatory gene ex-pression in older adults: A small randomized controlled trial. Brain,Behavior, and Immunity, 26, 1095–1101. http://dx.doi.org/10.1016/j.bbi.2012.07.006
Creswell, J. D., Myers, H. F., Cole, S. W., & Irwin, M. R. (2009).Mindfulness meditation training effects on CD4� T lymphocytes inHIV-1 infected adults: A small randomized controlled trial. Brain,Behavior, and Immunity, 23, 184–188. http://dx.doi.org/10.1016/j.bbi.2008.07.004
Davis, J. M., Fleming, M. F., Bonus, K. A., & Baker, T. B. (2007). A pilotstudy on mindfulness based stress reduction for smokers. BMC Com-plementary and Alternative Medicine, 7, 2. http://dx.doi.org/10.1186/1472-6882-7-2
Deckersbach, T., Hölzel, B. K., Eisner, L. R., Stange, J. P., Peckham,A. D., Dougherty, D. D., . . . Nierenberg, A. A. (2012). Mindfulness-based cognitive therapy for nonremitted patients with bipolar disorder.CNS Neuroscience & Therapeutics, 18, 133–141. http://dx.doi.org/10.1111/j.1755-5949.2011.00236.x
Degi, C. L., & Szilagy, T. (2013). Mindfulness-based stress reductionintervention in Romanian breast cancer inpatients. Cognition, Brain,Behavior: An Interdisciplinary Journal, 17, 135–148.
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
611October 2015 ● American Psychologist

de Lisle, S. M., Dowling, N. A., & Allen, J. S. (2011). Mindfulness-basedcognitive therapy for problem gambling. Clinical Case Studies, 10,210–228. http://dx.doi.org/10.1177/1534650111401016
Del Re, A. C., Flückiger, C., Goldberg, S. B., & Hoyt, W. T. (2013).Monitoring mindfulness practice quality: An important consideration inmindfulness practice. Psychotherapy Research, 23, 54–66. http://dx.doi.org/10.1080/10503307.2012.729275
De Raedt, R., Baert, S., Demeyer, I., Goeleven, E., Raes, A., Visser, A.,. . . Speckens, A. (2012). Changes in attentional processing of emo-tional information following mindfulness-based cognitive therapy inpeople with a history of depression: Towards an open attention for allemotional experiences. Cognitive Therapy and Research, 36, 612–620.http://dx.doi.org/10.1007/s10608-011-9411-x
DeRubeis, R. J., Cohen, Z. D., Forand, N. R., Fournier, J. C., Gelfand,L. A., & Lorenzo-Luaces, L. (2014). The Personalized AdvantageIndex: Translating research on prediction into individualized treatmentrecommendations. A demonstration. PLoS ONE, 9, e83875. http://dx.doi.org/10.1371/journal.pone.0083875
Deyo, M., Wilson, K. A., Ong, J., & Koopman, C. (2009). Mindfulnessand rumination: Does mindfulness training lead to reductions in theruminative thinking associated with depression? EXPLORE: The Jour-nal of Science and Healing, 5, 265–271. http://dx.doi.org/10.1016/j.explore.2009.06.005
Dimidjian, S., Beck, A., Felder, J. N., Boggs, J. M., Gallop, R., & Segal,Z. V. (2014). Web-based mindfulness-based cognitive therapy for re-ducing residual depressive symptoms: An open trial and quasi-experi-mental comparison to propensity score matched controls. BehaviourResearch and Therapy, 63, 83–89. http://dx.doi.org/10.1016/j.brat.2014.09.004
Dimidjian, S., & Hollon, S. D. (2010). How would we know if psycho-therapy were harmful? American Psychologist, 65, 21–33. http://dx.doi.org/10.1037/a0017299
Dobkin, P. L. (2008). Mindfulness-based stress reduction: What processesare at work? Complementary Therapies in Clinical Practice, 14, 8–16.http://dx.doi.org/10.1016/j.ctcp.2007.09.004
Dobkin, P. L., & Zhao, Q. (2011). Increased mindfulness: The activecomponent of the mindfulness-based stress reduction program? Com-plementary Therapies in Clinical Practice, 17, 22–27. http://dx.doi.org/10.1016/j.ctcp.2010.03.002
Duncan, L. G., Moskowitz, J. T., Neilands, T. B., Dilworth, S. E., Hecht,F. M., & Johnson, M. O. (2012). Mindfulness-based stress reduction forHIV treatment side effects: A randomized, wait-list controlled trial.Journal of Pain and Symptom Management, 43, 161–171. http://dx.doi.org/10.1016/j.jpainsymman.2011.04.007
Dunn, C., Hanieh, E., Roberts, R., & Powrie, R. (2012). Mindful preg-nancy and childbirth: Effects of a mindfulness-based intervention onwomen’s psychological distress and well-being in the perinatal period.Archives of Women’s Mental Health, 15, 139–143. http://dx.doi.org/10.1007/s00737-012-0264-4
Dutton, M. A., Bermudez, D., Matás, A., Majid, H., & Myers, N. L.(2013). Mindfulness-based stress reduction for low-income, predomi-nantly African American women with PTSD and a history of intimatepartner violence. Cognitive and Behavioral Practice, 20, 23–32. http://dx.doi.org/10.1016/j.cbpra.2011.08.003
Eisendrath, S., Chartier, M., & McLane, M. (2011). Adapting mindful-ness-based cognitive therapy for treatment-resistant depression. Cogni-tive and Behavioral Practice, 18, 362–370. http://dx.doi.org/10.1016/j.cbpra.2010.05.004
Epstein-Lubow, G., McBee, L., Darling, E., Armey, M., & Miller, I. W.(2011). A pilot investigation of mindfulness-based stress reduction forcaregivers of frail elderly. Mindfulness, 2, 95–102. http://dx.doi.org/10.1007/s12671-011-0047-4
Ernst, S., Welke, J., Heintze, C., Gabriel, R., Zöllner, A., Kiehne, S., . . .Esch, T. (2008). Effects of mindfulness-based stress reduction onquality of life in nursing home residents: A feasibility study.Forschende Komplementarmedizin, 15, 74–81. http://dx.doi.org/10.1159/000121479
Esmer, G., Blum, J., Rulf, J., & Pier, J. (2010). Mindfulness-based stressreduction for failed back surgery syndrome: A randomized controlledtrial. The Journal of the American Osteopathic Association, 110, 646–652.
Evans, S. H., & Clarke, P. (2011). Disseminating orphan innovations.Stanford Social Innovation Review, 42–47.
Evans, S., Ferrando, S., Carr, C., & Haglin, D. (2011). Mindfulness-basedstress reduction (MBSR) and distress in a community-based sample.Clinical Psychology & Psychotherapy, 18, 553–558. http://dx.doi.org/10.1002/cpp.727
Evans, S., Ferrando, S., Findler, M., Stowell, C., Smart, C., & Haglin, D.(2008). Mindfulness-based cognitive therapy for generalized anxietydisorder. Journal of Anxiety Disorders, 22, 716–721. http://dx.doi.org/10.1016/j.janxdis.2007.07.005
Fang, C. Y., Reibel, D. K., Longacre, M. L., Rosenzweig, S., Campbell,D. E., & Douglas, S. D. (2010). Enhanced psychosocial well-beingfollowing participation in a mindfulness-based stress reduction programis associated with increased natural killer cell activity. The Journal ofAlternative and Complementary Medicine, 16, 531–538. http://dx.doi.org/10.1089/acm.2009.0018
Farb, N. A. S., Segal, Z. V., & Anderson, A. K. (2013). Mindfulnessmeditation training alters cortical representations of interoceptive at-tention. Social Cognitive and Affective Neuroscience, 8, 15–26. http://dx.doi.org/10.1093/scan/nss066
Finucane, A., & Mercer, S. W. (2006). An exploratory mixed methodsstudy of the acceptability and effectiveness of mindfulness-basedcognitive therapy for patients with active depression and anxiety inprimary care. BMC Psychiatry, 6, 14. http://dx.doi.org/10.1186/1471-244X-6-14
Fitzpatrick, L., Simpson, J., & Smith, A. (2010). A qualitative analysis ofmindfulness-based cognitive therapy (MBCT) in Parkinson’s disease.Psychology and Psychotherapy, 83, 179–192. http://dx.doi.org/10.1348/147608309X471514
Fjorback, L. O., Arendt, M., Ornbøl, E., Walach, H., Rehfeld, E.,Schröder, A., & Fink, P. (2013). Mindfulness therapy for somatizationdisorder and functional somatic syndromes: Randomized trial withone-year follow-up. Journal of Psychosomatic Research, 74, 31–40.http://dx.doi.org/10.1016/j.jpsychores.2012.09.006
Fjorback, L. O., Carstensen, T., Arendt, M., Ornbøl, E., Walach, H.,Rehfeld, E., & Fink, P. (2013). Mindfulness therapy for somatizationdisorder and functional somatic syndromes: Analysis of economicconsequences alongside a randomized trial. Journal of PsychosomaticResearch, 74, 41–48. http://dx.doi.org/10.1016/j.jpsychores.2012.09.010
Flugel Colle, K. F., Vincent, A., Cha, S. S., Loehrer, L. L., Bauer, B. A.,& Wahner-Roedler, D. L. (2010). Measurement of quality of life andparticipant experience with the mindfulness-based stress reduction pro-gram. Complementary Therapies in Clinical Practice, 16, 36–40. http://dx.doi.org/10.1016/j.ctcp.2009.06.008
Foley, E., Baillie, A., Huxter, M., Price, M., & Sinclair, E. (2010).Mindfulness-based cognitive therapy for individuals whose lives havebeen affected by cancer: A randomized controlled trial. Journal ofConsulting and Clinical Psychology, 78, 72–79. http://dx.doi.org/10.1037/a0017566
Frisvold, M. H., Lindquist, R., & McAlpine, C. P. (2012). Living life inthe balance at midlife: Lessons learned from mindfulness. WesternJournal of Nursing Research, 34, 265–278. http://dx.doi.org/10.1177/0193945911424171
Gallegos, A. M., Hoerger, M., Talbot, N. L., Krasner, M. S., Knight, J. M.,Moynihan, J. A., & Duberstein, P. R. (2013). Toward identifying theeffects of the specific components of mindfulness-based stress reduc-tion on biologic and emotional outcomes among older adults. TheJournal of Alternative and Complementary Medicine, 19, 787–792.http://dx.doi.org/10.1089/acm.2012.0028
Gallegos, A. M., Hoerger, M., Talbot, N. L., Moynihan, J. A., & Duber-stein, P. R. (2013). Emotional benefits of mindfulness-based stressreduction in older adults: The moderating roles of age and depressivesymptom severity. Aging & Mental Health, 17, 823–829. http://dx.doi.org/10.1080/13607863.2013.799118
Gans, J. J., O’Sullivan, P., & Bircheff, V. (2013). Mindfulness basedtinnitus stress reduction pilot study. Mindfulness, 5, 322–333.
Garland, E. L., Gaylord, S. A., Palsson, O., Faurot, K., Douglas Mann, J.,& Whitehead, W. E. (2012). Therapeutic mechanisms of a mindfulness-based treatment for IBS: Effects on visceral sensitivity, catastrophizing,and affective processing of pain sensations. Journal of BehavioralMedicine, 35, 591–602. http://dx.doi.org/10.1007/s10865-011-9391-z
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
612 October 2015 ● American Psychologist

Garland, E. L., Manusov, E. G., Froeliger, B., Kelly, A., Williams, J. M.,& Howard, M. O. (2014). Mindfulness-oriented recovery enhancementfor chronic pain and prescription opioid misuse: Results from anearly-stage randomized controlled trial. Journal of Consulting andClinical Psychology, 82, 448–459. http://dx.doi.org/10.1037/a0035798
Garland, S. N., Carlson, L. E., Cook, S., Lansdell, L., & Speca, M. (2007).A non-randomized comparison of mindfulness-based stress reductionand healing arts programs for facilitating post-traumatic growth andspirituality in cancer outpatients. Supportive Care in Cancer, 15, 949–961. http://dx.doi.org/10.1007/s00520-007-0280-5
Garland, S. N., Tamagawa, R., Todd, S. C., Speca, M., & Carlson, L. E.(2013). Increased mindfulness is related to improved stress and moodfollowing participation in a mindfulness-based stress reduction programin individuals with cancer. Integrative Cancer Therapies, 12, 31–40.http://dx.doi.org/10.1177/1534735412442370
Gayner, B., Esplen, M. J., DeRoche, P., Wong, J., Bishop, S., Kavanagh,L., & Butler, K. (2012). A randomized controlled trial of mindfulness-based stress reduction to manage affective symptoms and improvequality of life in gay men living with HIV. Journal of BehavioralMedicine, 35, 272–285. http://dx.doi.org/10.1007/s10865-011-9350-8
Geary, C., & Rosenthal, S. L. (2011). Sustained impact of MBSR onstress, well-being, and daily spiritual experiences for 1 year in academichealth care employees. The Journal of Alternative and ComplementaryMedicine, 17, 939–944. http://dx.doi.org/10.1089/acm.2010.0335
Geschwind, N., Peeters, F., Drukker, M., van Os, J., & Wichers, M.(2011). Mindfulness training increases momentary positive emotionsand reward experience in adults vulnerable to depression: A random-ized controlled trial. Journal of Consulting and Clinical Psychology,79, 618–628. http://dx.doi.org/10.1037/a0024595
Geschwind, N., Peeters, F., Huibers, M., van Os, J., & Wichers, M.(2012). Efficacy of mindfulness-based cognitive therapy in relation toprior history of depression: Randomised controlled trial. The BritishJournal of Psychiatry, 201, 320–325. http://dx.doi.org/10.1192/bjp.bp.111.104851
Gex-Fabry, M., Jermann, F., Kosel, M., Rossier, M. F., Van der Linden,M., Bertschy, G., . . . Aubry, J.-M. (2012). Salivary cortisol profiles inpatients remitted from recurrent depression: One-year follow-up of amindfulness-based cognitive therapy trial. Journal of Psychiatric Re-search, 46, 80–86. http://dx.doi.org/10.1016/j.jpsychires.2011.09.011
Godfrin, K. A., & van Heeringen, C. (2010). The effects of mindfulness-based cognitive therapy on recurrence of depressive episodes, mentalhealth and quality of life: A randomized controlled study. BehaviourResearch and Therapy, 48, 738–746. http://dx.doi.org/10.1016/j.brat.2010.04.006
Gold, E., Smith, A., Hopper, I., Herne, D., Tansey, G., & Hulland, C.(2010). Mindfulness-based stress reduction (MBSR) for primary schoolteachers. Journal of Child and Family Studies, 19, 184–189. http://dx.doi.org/10.1007/s10826-009-9344-0
Goldin, P. R., & Gross, J. J. (2010). Effects of mindfulness-based stressreduction (MBSR) on emotion regulation in social anxiety disorder.Emotion, 10, 83–91. http://dx.doi.org/10.1037/a0018441
Goldin, P., Ramel, W., & Gross, J. (2009). Mindfulness meditationtraining and self-referential processing in social anxiety disorder: Be-havioral and neural effects. Journal of Cognitive Psychotherapy, 23,242–257. http://dx.doi.org/10.1891/0889-8391.23.3.242
Goldin, P., Ziv, M., Jazaieri, H., & Gross, J. J. (2012). Randomizedcontrolled trial of mindfulness-based stress reduction versus aerobicexercise: Effects on the self-referential brain network in social anxietydisorder. Frontiers in Human Neuroscience, 6, 295. http://dx.doi.org/10.3389/fnhum.2012.00295
Goldin, P., Ziv, M., Jazaieri, H., Hahn, K., & Gross, J. J. (2013). MBSRvs. aerobic exercise in social anxiety: FMRI of emotion regulation ofnegative self-beliefs. Social Cognitive and Affective Neuroscience, 8,65–72. http://dx.doi.org/10.1093/scan/nss054
Goyal, M., Singh, S., Sibinga, E. M., Gould, N. F., Rowland-Seymour, A.,Sharma, R., . . . Haythornthwaite, J. A. (2014). Meditation programs forpsychological stress and well-being: A systematic review and meta-analysis. Journal of the American Medical Association Internal Medi-cine, 174, 357–368. http://dx.doi.org/10.1001/jamainternmed.2013.13018
Green, S. M., & Bieling, P. J. (2012). Expanding the scope of mindful-ness-based cognitive therapy: Evidence for effectiveness in a hetero-
geneous psychiatric sample. Cognitive and Behavioral Practice, 19,174–180. http://dx.doi.org/10.1016/j.cbpra.2011.02.006
Greeson, J. M., Webber, D. M., Smoski, M. J., Brantley, J. G., Ekblad,A. G., Suarez, E. C., & Wolever, R. Q. (2011). Changes in spiritualitypartly explain health-related quality of life outcomes after mindfulness-based stress reduction. Journal of Behavioral Medicine, 34, 508–518.http://dx.doi.org/10.1007/s10865-011-9332-x
Griffiths, K., Camic, P. M., & Hutton, J. M. (2009). Participant experi-ences of a mindfulness-based cognitive therapy group for cardiac re-habilitation. Journal of Health Psychology, 14, 675–681. http://dx.doi.org/10.1177/1359105309104911
Gross, C. R., Kreitzer, M. J., Reilly-Spong, M., Wall, M., Winbush, N. Y.,Patterson, R., . . . Cramer-Bornemann, M. (2011). Mindfulness-basedstress reduction versus pharmacotherapy for chronic primary insomnia:A randomized controlled clinical trial. EXPLORE: The Journal ofScience and Healing, 7, 76–87. http://dx.doi.org/10.1016/j.explore.2010.12.003
Gross, C. R., Kreitzer, M. J., Russas, V., Treesak, C., Frazier, P. A., &Hertz, M. I. (2004). Mindfulness meditation to reduce symptoms afterorgan transplant: A pilot study. Advances in Mind-Body Medicine, 20,20–29.
Gross, C. R., Kreitzer, M. J., Thomas, W., Reilly-Spong, M., Cramer-Bornemann, M., Nyman, J. A., . . . Ibrahim, H. N. (2010). Mindfulness-based stress reduction for solid organ transplant recipients: A random-ized controlled trial. Alternative Therapies in Health and Medicine, 16,30–38.
Grossman, P., Tiefenthaler-Gilmer, U., Raysz, A., & Kesper, U. (2007).Mindfulness training as an intervention for fibromyalgia: Evidence ofpostintervention and 3-year follow-up benefits in well-being. Psycho-therapy and Psychosomatics, 76, 226–233. http://dx.doi.org/10.1159/000101501
Gu, J., Strauss, C., Bond, R., & Cavanagh, K. (2015). How do mindful-ness-based cognitive therapy and mindfulness-based stress reductionimprove mental health and wellbeing? A systematic review and meta-analysis of mediation studies. Clinical Psychology Review, 37, 1–12.http://dx.doi.org/10.1016/j.cpr.2015.01.006
Hargus, E., Crane, C., Barnhofer, T., & Williams, J. M. (2010). Effects ofmindfulness on meta-awareness and specificity of describing prodromalsymptoms in suicidal depression. Emotion, 10, 34–42. http://dx.doi.org/10.1037/a0016825
Hartmann, M., Kopf, S., Kircher, C., Faude-Lang, V., Djuric, Z., Aug-stein, F., . . . Nawroth, P. P. (2012). Sustained effects of a mindfulness-based stress-reduction intervention in type 2 diabetic patients: Designand first results of a randomized controlled trial (the HeidelbergerDiabetes and Stress Study). Diabetes Care, 35, 945–947.
Hawtin, H., & Sullivan, C. (2011). Experiences of mindfulness training inliving with rheumatic disease: An interpretative phenomenologicalanalysis. The British Journal of Occupational Therapy, 74, 137–142.http://dx.doi.org/10.4276/030802211X12996065859283
Hayes, S. C., Strosahl, K., & Wilson, K. G. (1999). Acceptance andcommitment therapy: An experiential approach to behavior change.New York, NY: Guilford Press.
Hazlett-Stevens, H. (2012). Mindfulness-based stress reduction for co-morbid anxiety and depression: Case report and clinical considerations.Journal of Nervous and Mental Disease, 200, 999–1003. http://dx.doi.org/10.1097/NMD.0b013e3182718a61
Heeren, A., Van Broeck, N., & Philippot, P. (2009). The effects ofmindfulness on executive processes and autobiographical memoryspecificity. Behaviour Research and Therapy, 47, 403–409. http://dx.doi.org/10.1016/j.brat.2009.01.017
Henderson, V. P., Clemow, L., Massion, A. O., Hurley, T. G., Druker, S.,& Hébert, J. R. (2012). The effects of mindfulness-based stress reduc-tion on psychosocial outcomes and quality of life in early-stage breastcancer patients: A randomized trial. Breast Cancer Research and Treat-ment, 131, 99–109. http://dx.doi.org/10.1007/s10549-011-1738-1
Hepburn, S. R., Crane, C., Barnhofer, T., Duggan, D. S., Fennell, M. J. V.,& Williams, J. M. G. (2009). Mindfulness-based cognitive therapy mayreduce thought suppression in previously suicidal participants: Findingsfrom a preliminary study. British Journal of Clinical Psychology, 48,209–215. http://dx.doi.org/10.1348/014466509X414970
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
613October 2015 ● American Psychologist

Herdt, J., Bührlen, B., Bader, K., & Hänny, C. (2012). Participation in anadapted version of MBCT in psychiatric care. Mindfulness, 3, 218–226.http://dx.doi.org/10.1007/s12671-012-0120-7
Hertenstein, E., Rose, N., Voderholzer, U., Heidenreich, T., Nissen, C.,Thiel, N., . . . Külz, A. K. (2012). Mindfulness-based cognitive therapyin obsessive-compulsive disorder: A qualitative study on patients’ ex-periences. BMC Psychiatry, 12, 185. http://dx.doi.org/10.1186/1471-244X-12-185
Hoffman, C. J., Ersser, S. J., & Hopkinson, J. B. (2012). Mindfulness-based stress reduction in breast cancer: A qualitative analysis. Comple-mentary Therapies in Clinical Practice, 18, 221–226. http://dx.doi.org/10.1016/j.ctcp.2012.06.008
Hoffman, C. J., Ersser, S. J., Hopkinson, J. B., Nicholls, P. G., Harrington,J. E., & Thomas, P. W. (2012). Effectiveness of mindfulness-basedstress reduction in mood, breast- and endocrine-related quality of life,and well-being in Stage 0 to III breast cancer: A randomized, controlledtrial. Journal of Clinical Oncology, 30, 1335–1342. http://dx.doi.org/10.1200/JCO.2010.34.0331
Hofmann, S. G., Sawyer, A. T., Witt, A. A., & Oh, D. (2010). The effectof mindfulness-based therapy on anxiety and depression: A meta-analytic review. Journal of Consulting and Clinical Psychology, 78,169–183. http://dx.doi.org/10.1037/a0018555
Hoge, E. A., Bui, E., Marques, L., Metcalf, C. A., Morris, L. K., Ro-binaugh, D. J., . . . Simon, N. M. (2013). Randomized controlled trialof mindfulness meditation for generalized anxiety disorder: Effects onanxiety and stress reactivity. Journal of Clinical Psychiatry, 74, 786–792. http://dx.doi.org/10.4088/JCP.12m08083
Hölzel, B. K., Carmody, J., Evans, K. C., Hoge, E. A., Dusek, J. A.,Morgan, L., . . . Lazar, S. W. (2010). Stress reduction correlates withstructural changes in the amygdala. Social Cognitive and AffectiveNeuroscience, 5, 11–17. http://dx.doi.org/10.1093/scan/nsp034
Hölzel, B. K., Carmody, J., Vangel, M., Congleton, C., Yerramsetti, S. M.,Gard, T., & Lazar, S. W. (2011). Mindfulness practice leads to in-creases in regional brain gray matter density. Psychiatry Research, 191,36–43. http://dx.doi.org/10.1016/j.pscychresns.2010.08.006
Hopkins, A., & Proeve, M. (2013). Teaching mindfulness-based cognitivetherapy to trainee psychologists: Qualitative and quantitative effects.Counselling Psychology Quarterly, 26, 115–130. http://dx.doi.org/10.1080/09515070.2013.792998
Hopkins, V., & Kuyken, W. (2012). Benefits and barriers to attendingMBCT reunion meetings: An insider perspective. Mindfulness, 3, 139–150. http://dx.doi.org/10.1007/s12671-012-0088-3
Howells, F. M., Ives-Deliperi, V. L., Horn, N. R., & Stein, D. J. (2012).Mindfulness based cognitive therapy improves frontal control in bipolardisorder: A pilot EEG study. BMC Psychiatry, 12, 15. http://dx.doi.org/10.1186/1471-244X-12-15
Huss, D. B., & Baer, R. A. (2007). Acceptance and change: The integra-tion of mindfulness-based cognitive therapy into ongoing dialecticalbehavior therapy in a case of borderline personality disorder withdepression. Clinical Case Studies, 6, 17–33. http://dx.doi.org/10.1177/1534650106290374
Imel, Z., Baldwin, S., Bonus, K., & Maccoon, D. (2008). Beyond theindividual: Group effects in mindfulness-based stress reduction.Psychotherapy Research, 18, 735–742. http://dx.doi.org/10.1080/10503300802326038
Ives-Deliperi, V. L., Howells, F., Stein, D. J., Meintjes, E. M., & Horn, N.(2013). The effects of mindfulness-based cognitive therapy in patientswith bipolar disorder: A controlled functional MRI investigation. Jour-nal of Affective Disorders, 150, 1152–1157. http://dx.doi.org/10.1016/j.jad.2013.05.074
Jam, S., Imani, A. H., Foroughi, M., SeyedAlinaghi, S., Koochak, H. E.,& Mohraz, M. (2010). The effects of mindfulness-based stress reduc-tion (MBSR) program in Iranian HIV/AIDS patients: A pilot study.Acta Medica Iranica, 48, 101–106.
Jastrowski Mano, K. E., Salamon, K. S., Hainsworth, K. R., AndersonKhan, K. J., Ladwig, R. J., Davies, W. H., & Weisman, S. J. (2013). Arandomized, controlled pilot study of mindfulness-based stress reduc-tion for pediatric chronic pain. Alternative Therapies in Health andMedicine, 19, 8–14.
Jazaieri, H., Goldin, P. R., Werner, K., Ziv, M., & Gross, J. J. (2012). Arandomized trial of MBSR versus aerobic exercise for social anxiety
disorder. Journal of Clinical Psychology, 68, 715–731. http://dx.doi.org/10.1002/jclp.21863
Jensen, C. G., Vangkilde, S., Frokjaer, V., & Hasselbalch, S. G. (2012).Mindfulness training affects attention: Or is it attentional effort? Jour-nal of Experimental Psychology: General, 141, 106–123. http://dx.doi.org/10.1037/a0024931
Jermann, F., Van der Linden, M., Gex-Fabry, M., Guarin, A., Kosel, M.,Bertschy, G., . . . Bondolfi, G. (2013). Cognitive functioning in patientsremitted from recurrent depression: Comparison with acutely depressedpatients and controls and follow-up of a mindfulness-based cognitivetherapy trial. Cognitive Therapy and Research, 37, 1004–1014. http://dx.doi.org/10.1007/s10608-013-9544-1
Jha, A. P., Krompinger, J., & Baime, M. J. (2007). Mindfulness trainingmodifies subsystems of attention. Cognitive, Affective & BehavioralNeuroscience, 7, 109–119. http://dx.doi.org/10.3758/CABN.7.2.109
Johansson, B., Bjuhr, H., & Rönnbäck, L. (2012). Mindfulness-basedstress reduction (MBSR) improves long-term mental fatigue afterstroke or traumatic brain injury. Brain Injury, 26, 1621–1628. http://dx.doi.org/10.3109/02699052.2012.700082
Kabat-Zinn, J. (1990). Full catastrophe living: Using the wisdom of yourbody and mind to face stress, pain, and illness. New York, NY: BantamBooks.
Kabat-Zinn, J. (2011). Some reflections on the origins of MBSR, skillfulmeans, and the trouble with maps. Contemporary Buddhism, 12, 281–306. http://dx.doi.org/10.1080/14639947.2011.564844
Kabat-Zinn, J., Wheeler, E., Light, T., Skillings, A., Scharf, M. J.,Cropley, T. G., . . . Bernhard, J. D. (1998). Influence of a mindfulnessmeditation-based stress reduction intervention on rates of skin clearingin patients with moderate to severe psoriasis undergoing phototherapy(UVB) and photochemotherapy (PUVA). Psychosomatic Medicine, 60,625–632. http://dx.doi.org/10.1097/00006842-199809000-00020
Kaplan, K. H., Goldenberg, D. L., & Galvin-Nadeau, M. (1993). Theimpact of a meditation-based stress reduction program on fibromyalgia.General Hospital Psychiatry, 15, 284–289. http://dx.doi.org/10.1016/0163-8343(93)90020-O
Kaviani, H., Hatami, N., & Javaheri, F. (2012). The impact of mindful-ness-based cognitive therapy (MBCT) on mental health and quality oflife in a sub-clinically depressed population. Archives of Psychiatry andPsychotherapy, 14, 21–28.
Kaviani, H., Javaheri, F., & Hatami, N. (2011). Mindfulness-based cog-nitive therapy (MBCT) reduces depression and anxiety induced by realstressful setting in non-clinical population. International Journal ofPsychology & Psychological Therapy, 11, 285–296.
Kazdin, A. E., & Blase, S. L. (2011). Rebooting psychotherapy researchand practice to reduce the burden of mental illness. Perspectives onPsychological Science, 6, 21–37. http://dx.doi.org/10.1177/1745691610393527
Kearney, D. J., McDermott, K., Malte, C., Martinez, M., & Simpson, T. L.(2012). Association of participation in a mindfulness program withmeasures of PTSD, depression and quality of life in a veteran sample.Journal of Clinical Psychology, 68, 101–116. http://dx.doi.org/10.1002/jclp.20853
Kearney, D. J., McDermott, K., Malte, C., Martinez, M., & Simpson, T. L.(2013). Effects of participation in a mindfulness program for veteranswith posttraumatic stress disorder: A randomized controlled pilot study.Journal of Clinical Psychology, 69, 14–27. http://dx.doi.org/10.1002/jclp.21911
Kearney, D. J., McDermott, K., Martinez, M., & Simpson, T. L. (2011).Association of participation in a mindfulness programme with bowelsymptoms, gastrointestinal symptom-specific anxiety and quality oflife. Alimentary Pharmacology & Therapeutics, 34, 363–373. http://dx.doi.org/10.1111/j.1365-2036.2011.04731.x
Kearney, D. J., Milton, M. L., Malte, C. A., McDermott, K. A., Martinez,M., & Simpson, T. L. (2012). Participation in mindfulness-based stressreduction is not associated with reductions in emotional eating oruncontrolled eating. Nutrition Research, 32, 413–420. http://dx.doi.org/10.1016/j.nutres.2012.05.008
Keng, S.-L., Smoski, M. J., Robins, C. J., Ekblad, A. G., & Brantley, J. G.(2012). Mechanisms of change in mindfulness-based stress reduction:Self-compassion and mindfulness as mediators of intervention out-comes. Journal of Cognitive Psychotherapy, 26, 270–280. http://dx.doi.org/10.1891/0889-8391.26.3.270
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
614 October 2015 ● American Psychologist

Kenny, M. A., & Williams, J. M. G. (2007). Treatment-resistant depressedpatients show a good response to mindfulness-based cognitive therapy.Behaviour Research and Therapy, 45, 617–625. http://dx.doi.org/10.1016/j.brat.2006.04.008
Kerr, C. E., Josyula, K., & Littenberg, R. (2011). Developing an observingattitude: An analysis of meditation diaries in an MBSR clinical trial.Clinical Psychology & Psychotherapy, 18, 80–93. http://dx.doi.org/10.1002/cpp.700
Kerrigan, D., Johnson, K., Stewart, M., Magyari, T., Hutton, N., Ellen,J. M., & Sibinga, E. M. (2011). Perceptions, experiences, and shifts inperspective occurring among urban youth participating in a mindful-ness-based stress reduction program. Complementary Therapies inClinical Practice, 17, 96–101. http://dx.doi.org/10.1016/j.ctcp.2010.08.003
Keune, P. M., Bostanov, V., Hautzinger, M., & Kotchoubey, B. (2011).Mindfulness-based cognitive therapy (MBCT), cognitive style, and thetemporal dynamics of frontal EEG alpha asymmetry in recurrentlydepressed patients. Biological Psychology, 88, 243–252. http://dx.doi.org/10.1016/j.biopsycho.2011.08.008
Kieviet-Stijnen, A., Visser, A., Garssen, B., & Hudig, W. (2008). Mind-fulness-based stress reduction training for oncology patients: Patients’appraisal and changes in well-being. Patient Education and Counsel-ing, 72, 436–442. http://dx.doi.org/10.1016/j.pec.2008.05.015
Kilpatrick, L. A., Suyenobu, B. Y., Smith, S. R., Bueller, J. A., Goodman,T., Creswell, J. D., . . . Naliboff, B. D. (2011). Impact of mindfulness-based stress reduction training on intrinsic brain connectivity. Neuro-Image, 56, 290–298. http://dx.doi.org/10.1016/j.neuroimage.2011.02.034
Kim, B., Lee, S. H., Kim, Y. W., Choi, T. K., Yook, K., Suh, S. Y., . . .Yook, K. H. (2010). Effectiveness of a mindfulness-based cognitivetherapy program as an adjunct to pharmacotherapy in patients withpanic disorder. Journal of Anxiety Disorders, 24, 590–595. http://dx.doi.org/10.1016/j.janxdis.2010.03.019
Kim, Y. W., Lee, S. H., Choi, T. K., Suh, S. Y., Kim, B., Kim, C. M., . . .Yook, K. H. (2009). Effectiveness of mindfulness-based cognitivetherapy as an adjuvant to pharmacotherapy in patients with panicdisorder or generalized anxiety disorder. Depression and Anxiety, 26,601–606. http://dx.doi.org/10.1002/da.20552
Kimbrough, E., Magyari, T., Langenberg, P., Chesney, M., & Berman, B.(2010). Mindfulness intervention for child abuse survivors. Journal ofClinical Psychology, 66, 17–33.
King, A. P., Erickson, T. M., Giardino, N. D., Favorite, T., Rauch,S. A. M., Robinson, E., . . . Liberzon, I. (2013). A pilot study of groupmindfulness-based cognitive therapy (MBCT) for combat veterans withposttraumatic stress disorder (PTSD). Depression and Anxiety, 30,638–645. http://dx.doi.org/10.1002/da.22104
Kingston, T., Dooley, B., Bates, A., Lawlor, E., & Malone, K. (2007).Mindfulness-based cognitive therapy for residual depressive symptoms.Psychology and Psychotherapy, 80, 193–203. http://dx.doi.org/10.1348/147608306X116016
Klatt, M. D., Buckworth, J., & Malarkey, W. B. (2009). Effects oflow-dose mindfulness-based stress reduction (MBSR-ld) on workingadults. Health Education & Behavior, 36, 601–614. http://dx.doi.org/10.1177/1090198108317627
Koszycki, D., Benger, M., Shlik, J., & Bradwejn, J. (2007). Randomizedtrial of a meditation-based stress reduction program and cognitivebehavior therapy in generalized social anxiety disorder. BehaviourResearch and Therapy, 45, 2518–2526. http://dx.doi.org/10.1016/j.brat.2007.04.011
Kreitzer, M. J., Gross, C. R., Ye, X., Russas, V., & Treesak, C. (2005).Longitudinal impact of mindfulness meditation on illness burden insolid-organ transplant recipients. Progress in Transplantation, 15, 166–172. http://dx.doi.org/10.7182/prtr.15.2.6wx56r4u323851r7
Kuyken, W., Byford, S., Taylor, R. S., Watkins, E., Holden, E., White, K.,. . . Teasdale, J. D. (2008). Mindfulness-based cognitive therapy toprevent relapse in recurrent depression. Journal of Consulting andClinical Psychology, 76, 966–978. http://dx.doi.org/10.1037/a0013786
Kuyken, W., Hayes, R., Barrett, B., Byng, R., Dalgleish, T., Kessler, D.,. . . Byford, S. (2015). Effectiveness and cost-effectiveness of mind-fulness-based cognitive therapy compared with maintenance antide-pressant treatment in the prevention of depressive relapse or recurrence
(PREVENT): A randomised controlled trial. Lancet. Advance onlinepublication. http://dx.doi.org/10.1016/S0140-6736(14)62222-4
Kuyken, W., Watkins, E., Holden, E., White, K., Taylor, R. S., Byford, S.,. . . Dalgleish, T. (2010). How does mindfulness-based cognitivetherapy work? Behaviour Research and Therapy, 48, 1105–1112. http://dx.doi.org/10.1016/j.brat.2010.08.003
Kvillemo, P., & Bränström, R. (2011). Experiences of a mindfulness-based stress-reduction intervention among patients with cancer. CancerNursing, 34, 24–31. http://dx.doi.org/10.1097/NCC.0b013e3181e2d0df
Labelle, L. E., Campbell, T. S., & Carlson, L. E. (2010). Mindfulness-based stress reduction in oncology: Evaluating mindfulness and rumi-nation as mediators of change in depressive symptoms. Mindfulness, 1,28–40. http://dx.doi.org/10.1007/s12671-010-0005-6
Langdon, S., Jones, F. W., Hutton, J., & Holttum, S. (2011). A grounded-theory study of mindfulness practice following mindfulness-based cog-nitive therapy. Mindfulness, 2, 270–281. http://dx.doi.org/10.1007/s12671-011-0070-5
Lange, B. (2011). Cocreating a communicative space to develop a mind-fulness meditation manual for women in recovery from substance abusedisorders. Advances in Nursing Science, 34, E1–E13. http://dx.doi.org/10.1097/ANS.0b013e3182272405
Langer, Á. I., Cangas, A. J., Salcedo, E., & Fuentes, B. (2012). Applyingmindfulness therapy in a group of psychotic individuals: A controlledstudy. Behavioural and Cognitive Psychotherapy, 40, 105–109. http://dx.doi.org/10.1017/S1352465811000464
Lau, M. A., Colley, L., Willett, B. R., & Lynd, L. D. (2012). Employee’spreferences for access to mindfulness-based cognitive therapy to reducethe risk of depressive relapse: A discrete choice experiment. Mindful-ness, 3, 318–326. http://dx.doi.org/10.1007/s12671-012-0108-3
Lee, J., Semple, R. J., Rosa, D., & Miller, L. (2008). Mindfulness-basedcognitive therapy for children: Results of a pilot study. Journal ofCognitive Psychotherapy, 22, 15–28. http://dx.doi.org/10.1891/0889.8391.22.1.15
Lengacher, C. A., Johnson-Mallard, V., Barta, M., Fitzgerald, S., Mos-coso, M. S., Post-White, J., . . . Kip, K. E. (2011). Feasibility of amindfulness-based stress reduction program for early-stage breast can-cer survivors. Journal of Holistic Nursing, 29, 107–117. http://dx.doi.org/10.1177/0898010110385938
Lengacher, C. A., Johnson-Mallard, V., Post-White, J., Moscoso, M. S.,Jacobsen, P. B., Klein, T. W., . . . Kip, K. E. (2009). Randomizedcontrolled trial of mindfulness-based stress reduction (MBSR) for sur-vivors of breast cancer. Psycho-Oncology, 18, 1261–1272. http://dx.doi.org/10.1002/pon.1529
Lengacher, C. A., Kip, K. E., Barta, M., Post-White, J., Jacobsen, P. B.,Groer, M., . . . Shelton, M. M. (2012). A pilot study evaluating theeffect of mindfulness-based stress reduction on psychological status,physical status, salivary cortisol, and interleukin-6 among advanced-stage cancer patients and their caregivers. Journal of Holistic Nursing,30, 170–185. http://dx.doi.org/10.1177/0898010111435949
Lengacher, C. A., Kip, K. E., Post-White, J., Fitzgerald, S., Newton, C.,Barta, M., . . . Klein, T. W. (2013). Lymphocyte recovery after breastcancer treatment and mindfulness-based stress reduction (MBSR) ther-apy. Biological Research for Nursing, 15, 37–47. http://dx.doi.org/10.1177/1099800411419245
Lengacher, C. A., Reich, R. R., Post-White, J., Moscoso, M., Shelton,M. M., Barta, M., . . . Budhrani, P. (2012). Mindfulness based stressreduction in post-treatment breast cancer patients: An examination ofsymptoms and symptom clusters. Journal of Behavioral Medicine, 35,86–94. http://dx.doi.org/10.1007/s10865-011-9346-4
Lerman, R., Jarski, R., Rea, H., Gellish, R., & Vicini, F. (2012). Improv-ing symptoms and quality of life of female cancer survivors: A ran-domized controlled study. Annals of Surgical Oncology, 19, 373–378.http://dx.doi.org/10.1245/s10434-011-2051-2
Lilienfeld, S. O., Lynn, S. J., & Lohr, J. M. (2003). Science and pseudo-science in clinical psychology. New York, NY: Guilford Press.
Linehan, M. M. (1993). Cognitive-behavioral treatment of borderlinepersonality disorder. New York, NY: Guilford Press.
Lovas, D. A., & Barsky, A. J. (2010). Mindfulness-based cognitivetherapy for hypochondriasis, or severe health anxiety: A pilot study.Journal of Anxiety Disorders, 24, 931–935. http://dx.doi.org/10.1016/j.janxdis.2010.06.019
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
615October 2015 ● American Psychologist

Lush, E., Salmon, P., Floyd, A., Studts, J. L., Weissbecker, I., & Sephton,S. E. (2009). Mindfulness meditation for symptom reduction in fibro-myalgia: Psychophysiological correlates. Journal of Clinical Psychol-ogy in Medical Settings, 16, 200–207. http://dx.doi.org/10.1007/s10880-009-9153-z
Lutz, A., Jha, A. P., Dunne, J., & Saron, C. D. (2015). Investigating thephenomenological matrix of mindfulness-related practices from a neu-rocognitive perspective. American Psychologist, 70, 632–658. http://dx.doi.org/10.1037/a0039585
Ma, S. H., & Teasdale, J. D. (2004). Mindfulness-based cognitive therapyfor depression: Replication and exploration of differential relapse pre-vention effects. Journal of Consulting and Clinical Psychology, 72,31–40. http://dx.doi.org/10.1037/0022-006x.72.1.31
MacCoon, D. G., Imel, Z. E., Rosenkranz, M. A., Sheftel, J. G., Weng,H. Y., Sullivan, J. C., . . . Lutz, A. (2012). The validation of an activecontrol intervention for mindfulness based stress reduction (MBSR).Behaviour Research and Therapy, 50, 3–12. http://dx.doi.org/10.1016/j.brat.2011.10.011
Mackenzie, M. J., Carlson, L. E., Munoz, M., & Speca, M. (2007). Aqualitative study of self-perceived effects of mindfulness-based stressreduction (MBSR) in a psychosocial oncology setting. Stress andHealth: Journal of the International Society for the Investigation ofStress, 23, 59–69. http://dx.doi.org/10.1002/smi.1120
Manicavasgar, V., Parker, G., & Perich, T. (2011). Mindfulness-basedcognitive therapy vs cognitive behaviour therapy as a treatment fornon-melancholic depression. Journal of Affective Disorders, 130, 138–144. http://dx.doi.org/10.1016/j.jad.2010.09.027
Marcus, M. T., Fine, M., Moeller, F. G., Khan, M. M., Pitts, K., Swank,P. R., & Liehr, P. (2003). Change in stress levels following mindful-ness-based stress reduction in a therapeutic community. Addictive Dis-orders & Their Treatment, 2, 63–68. http://dx.doi.org/10.1097/00132576-200302030-00001
Martín-Asuero, A., & García-Banda, G. (2010). The mindfulness-basedstress reduction program (MBSR) reduces stress-related psychologicaldistress in healthcare professionals. The Spanish Journal of Psychology,13, 897–905. http://dx.doi.org/10.1017/S1138741600002547
Mason, O., & Hargreaves, I. (2001). A qualitative study of mindfulness-based cognitive therapy for depression. British Journal of MedicalPsychology, 74, 197–212. http://dx.doi.org/10.1348/000711201160911
Matchim, Y., Armer, J. M., & Stewart, B. R. (2011). Effects of mindful-ness-based stress reduction (MBSR) on health among breast cancersurvivors. Western Journal of Nursing Research, 33, 996–1016. http://dx.doi.org/10.1177/0193945910385363
Mathew, K. L., Whitford, H. S., Kenny, M. A., & Denson, L. A. (2010).The long-term effects of mindfulness-based cognitive therapy as arelapse prevention treatment for major depressive disorder. Behaviouraland Cognitive Psychotherapy, 38, 561–576. http://dx.doi.org/10.1017/S135246581000010X
Matousek, R. H., Pruessner, J. C., & Dobkin, P. L. (2011). Changes in thecortisol awakening response (CAR) following participation in mindful-ness-based stress reduction in women who completed treatment forbreast cancer. Complementary Therapies in Clinical Practice, 17, 65–70. http://dx.doi.org/10.1016/j.ctcp.2010.10.005
McManus, F., Surawy, C., Muse, K., Vazquez-Montes, M., & Williams,J. M. (2012). A randomized clinical trial of mindfulness-based cogni-tive therapy versus unrestricted services for health anxiety (hypochon-driasis). Journal of Consulting and Clinical Psychology, 80, 817–828.http://dx.doi.org/10.1037/a0028782
Melloni, M., Sedeño, L., Couto, B., Reynoso, M., Gelormini, C., Faval-oro, R., . . . Ibanez, A. (2013). Preliminary evidence about the effectsof meditation on interoceptive sensitivity and social cognition. Behav-ioral and Brain Functions, 9, 47. http://dx.doi.org/10.1186/1744-9081-9-47
Michalak, J., Heidenreich, T., Meibert, P., & Schulte, D. (2008).Mindfulness predicts relapse/recurrence in major depressive disor-der after mindfulness-based cognitive therapy. Journal of Nervousand Mental Disease, 196, 630 – 633. http://dx.doi.org/10.1097/NMD.0b013e31817d0546
Michalak, J., Hölz, A., & Teismann, T. (2011). Rumination as a predictorof relapse in mindfulness-based cognitive therapy for depression. Psy-chology and Psychotherapy, 84, 230–236. http://dx.doi.org/10.1348/147608310X520166
Michalak, J., Troje, N. F., & Heidenreich, T. (2011). The effects ofmindfulness-based cognitive therapy on depressive gait patterns. Jour-nal of Cognitive and Behavioral Psychotherapies, 11, 13–27.
Miklowitz, D. J., Alatiq, Y., Goodwin, G. M., Geddes, J. R., Fennell,M. J. V., Dimidjian, S., . . . Williams, J. M. G. (2009). A pilot study ofmindfulness-based cognitive therapy for bipolar disorder. InternationalJournal of Cognitive Therapy, 2, 373–382. http://dx.doi.org/10.1521/ijct.2009.2.4.373
Miller, J. J., Fletcher, K., & Kabat-Zinn, J. (1995). Three-year fol-low-up and clinical implications of a mindfulness meditation-basedstress reduction intervention in the treatment of anxiety disorders.General Hospital Psychiatry, 17, 192–200. http://dx.doi.org/10.1016/0163-8343(95)00025-M
Minor, H. G., Carlson, L. E., Mackenzie, M. J., Zernicke, K., & Jones, L.(2006). Evaluation of a mindfulness-based stress reduction (MBSR)program for caregivers of children with chronic conditions. Social Workin Health Care, 43, 91–109. http://dx.doi.org/10.1300/J010v43n01_06
Morone, N. E., Lynch, C. P., Losasso, V. J., III, Liebe, K., & Greco, C. M.(2012). Mindfulness to reduce psychosocial stress. Mindfulness, 3,22–29. http://dx.doi.org/10.1007/s12671-011-0076-z
Moynihan, J. A., Chapman, B. P., Klorman, R., Krasner, M. S., Duber-stein, P. R., Brown, K. W., & Talbot, N. L. (2013). Mindfulness-basedstress reduction for older adults: Effects on executive function, frontalalpha asymmetry and immune function. Neuropsychobiology, 68, 34–43. http://dx.doi.org/10.1159/000350949
Munshi, K., Eisendrath, S., & Delucchi, K. (2013). Preliminary long-termfollow-up of Mindfulness-based cognitive therapy-induced remissionof depression. Mindfulness, 4, 354–361. http://dx.doi.org/10.1007/s12671-012-0135-0
Naranjo, J. R., & Schmidt, S. (2012). Is it me or not me? Modulation ofperceptual-motor awareness and visuomotor performance by mindful-ness meditation. BMC Neuroscience, 13, 88. http://dx.doi.org/10.1186/1471-2202-13-88
Niles, B. L., Klunk-Gillis, J., Ryngala, D. J., Silberbogen, A. K., Paysnick,A., & Wolf, E. J. (2012). Comparing mindfulness and psychoeducationtreatments for combat-related PTSD using a telehealth approach. Psy-chological Trauma: Theory, Research, Practice, and Policy, 4, 538–547. http://dx.doi.org/10.1037/a0026161
Nyklícek, I., & Kuijpers, K. F. (2008). Effects of mindfulness-based stressreduction intervention on psychological well-being and quality of life:Is increased mindfulness indeed the mechanism? Annals of BehavioralMedicine, 35, 331–340. http://dx.doi.org/10.1007/s12160-008-9030-2
Nyklícek, I., Mommersteeg, P. M. C., Van Beugen, S., Ramakers, C., &Van Boxtel, G. J. (2013). Mindfulness-based stress reduction andphysiological activity during acute stress: A randomized controlledtrial. Health Psychology, 32, 1110–1113. http://dx.doi.org/10.1037/a0032200
Nyklícek, I., van Beugen, S., & Denollet, J. (2013). Effects of mindful-ness-based stress reduction on distressed (Type D) personality traits: Arandomized controlled trial. Journal of Behavioral Medicine, 36, 361–370. http://dx.doi.org/10.1007/s10865-012-9431-3
O’Haver Day, P., & Horton-Deutsch, S. (2004). Using mindfulness-basedtherapeutic interventions in psychiatric nursing practice: Part I: De-scription and empirical support for mindfulness-based interventions.Archives of Psychiatric Nursing, 18, 164–169. http://dx.doi.org/10.1016/j.apnu.2004.07.003
Oken, B. S., Fonareva, I., Haas, M., Wahbeh, H., Lane, J. B., Zajdel, D.,& Amen, A. (2010). Pilot controlled trial of mindfulness meditation andeducation for dementia caregivers. The Journal of Alternative andComplementary Medicine, 16, 1031–1038. http://dx.doi.org/10.1089/acm.2009.0733
Oman, D., Shapiro, S. L., Thoresen, C. E., Plante, T. G., & Flinders, T.(2008). Meditation lowers stress and supports forgiveness among col-lege students: A randomized controlled trial. Journal of AmericanCollege Health, 56, 569–578. http://dx.doi.org/10.3200/JACH.56.5.569-578
Onken, L. S., Carroll, K. M., Shoham, V., Cuthbert, B. N., & Riddle, M.(2014). Reenvisioning clinical science: Unifying the discipline to im-prove the public health. Clinical Psychological Science, 2, 22–34.http://dx.doi.org/10.1177/2167702613497932
Palta, P., Page, G., Piferi, R. L., Gill, J. M., Hayat, M. J., Connolly, A. B.,& Szanton, S. L. (2012). Evaluation of a mindfulness-based interven-
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
616 October 2015 ● American Psychologist

tion program to decrease blood pressure in low-income African-Amer-ican older adults. Journal of Urban Health, 89, 308–316. http://dx.doi.org/10.1007/s11524-011-9654-6
Parra-Delgado, M., & Latorre-Postigo, J. M. (2013). Effectiveness ofmindfulness-based cognitive therapy in the treatment of fibromyalgia:A randomised trial. Cognitive Therapy and Research, 37, 1015–1026.http://dx.doi.org/10.1007/s10608-013-9538-z
Patel, S. R., Carmody, J., & Simpson, H. B. (2007). Adapting mindful-ness-based stress reduction for the treatment of obsessive-compulsivedisorder: A case report. Cognitive and Behavioral Practice, 14, 375–380. http://dx.doi.org/10.1016/j.cbpra.2006.08.006
Patten, S. B., Kennedy, S. H., Lam, R. W., O’Donovan, C., Filteau, M. J.,Parikh, S. V., & Ravindran, A. V., & the Canadian Network for Moodand Anxiety Treatments (CANMAT). (2009). Canadian Network forMood and Anxiety Treatments (CANMAT) clinical guidelines for themanagement of major depressive disorder in adults: I. Classification,burden and principles of management. Journal of Affective Disorders,117, S5–S14. http://dx.doi.org/10.1016/j.jad.2009.06.044
Patten, S. B., & Meadows, G. M. (2009). Population-based service plan-ning for implementation of MBCT: Linking epidemiologic data topractice. Psychiatric Services, 60, 1540–1542. http://dx.doi.org/10.1176/ps.2009.60.11.1540
Pbert, L., Madison, J. M., Druker, S., Olendzki, N., Magner, R., Reed, G.,. . . Carmody, J. (2012). Effect of mindfulness training on asthmaquality of life and lung function: A randomised controlled trial. Thorax,67, 769–776. http://dx.doi.org/10.1136/thoraxjnl-2011-200253
Perich, T., Manicavasagar, V., Mitchell, P. B., & Ball, J. R. (2013). Theassociation between meditation practice and treatment outcome inmindfulness-based cognitive therapy for bipolar disorder. BehaviourResearch and Therapy, 51, 338–343. http://dx.doi.org/10.1016/j.brat.2013.03.006
Perich, T., Manicavasagar, V., Mitchell, P. B., Ball, J. R., & Hadzi-Pavlovic, D. (2013). A randomized controlled trial of mindfulness-based cognitive therapy for bipolar disorder. Acta Psychiatrica Scan-dinavica, 127, 333–343. http://dx.doi.org/10.1111/acps.12033
Philippot, P., Nef, F., Clauw, L., de Romrée, M., & Segal, Z. (2012). Arandomized controlled trial of mindfulness-based cognitive therapy fortreating tinnitus. Clinical Psychology & Psychotherapy, 19, 411–419.http://dx.doi.org/10.1002/cpp.756
Piet, J., & Hougaard, E. (2011). The effect of mindfulness-based cognitivetherapy for prevention of relapse in recurrent major depressive disorder:A systematic review and meta-analysis. Clinical Psychology Review,31, 1032–1040. http://dx.doi.org/10.1016/j.cpr.2011.05.002
Piet, J., Hougaard, E., Hecksher, M. S., & Rosenberg, N. K. (2010). Arandomized pilot study of mindfulness-based cognitive therapy andgroup cognitive-behavioral therapy for young adults with social phobia.Scandinavian Journal of Psychology, 51, 403–410.
Plews-Ogan, M., Owens, J. E., Goodman, M., Wolfe, P., & Schorling, J.(2005). A pilot study evaluating mindfulness-based stress reduction andmassage for the management of chronic pain. Journal of GeneralInternal Medicine, 20, 1136–1138. http://dx.doi.org/10.1111/j.1525-1497.2005.0247.x
Pradhan, E. K., Baumgarten, M., Langenberg, P., Handwerger, B., Gilpin,A. K., Magyari, T., . . . Berman, B. M. (2007). Effect of mindfulness-based stress reduction in rheumatoid arthritis patients. Arthritis Careand Research, 57, 1134–1142. http://dx.doi.org/10.1002/art.23010
Raes, F., Dewulf, D., Van Heeringen, C., & Williams, J. M. G. (2009).Mindfulness and reduced cognitive reactivity to sad mood: Evidencefrom a correlational study and a non-randomized waiting list controlledstudy. Behaviour Research and Therapy, 47, 623–627. http://dx.doi.org/10.1016/j.brat.2009.03.007
Ramel, W., I, Goldin, P. R., Carmona, P. E., & McQuaid, J. R. (2004). Theeffects of mindfulness meditation on cognitive processes and affect inpatients with past depression. Cognitive Therapy and Research, 28,433–455. http://dx.doi.org/10.1023/B:COTR.0000045557.15923.96
Rapgay, L., Bystritsky, A., Dafter, R. E., & Spearman, M. (2011). Newstrategies for combining mindfulness with integrative cognitive behav-ioral therapy for the treatment of generalized anxiety disorder. Journalof Rational-Emotive & Cognitive-Behavior Therapy, 29, 92–119. http://dx.doi.org/10.1007/s10942-009-0095-z
Ree, M. J., & Craigie, M. A. (2007). Outcomes following mindfulness-based cognitive therapy in a heterogeneous sample of adult outpatients.Behaviour Change, 24, 70–86. http://dx.doi.org/10.1375/bech.24.2.70
Reibel, D. K., Greeson, J. M., Brainard, G. C., & Rosenzweig, S. (2001).Mindfulness-based stress reduction and health-related quality of life ina heterogeneous patient population. General Hospital Psychiatry, 23,183–192. http://dx.doi.org/10.1016/S0163-8343(01)00149-9
Rimes, K. A., & Wingrove, J. (2011). Pilot study of mindfulness-basedcognitive therapy for trainee clinical psychologists. Behavioural andCognitive Psychotherapy, 39, 235–241. http://dx.doi.org/10.1017/S1352465810000731
Rimes, K. A., & Wingrove, J. (2013). Mindfulness-based cognitive ther-apy for people with chronic fatigue syndrome still experiencing exces-sive fatigue after cognitive behaviour therapy: A pilot randomizedstudy. Clinical Psychology & Psychotherapy, 20, 107–117. http://dx.doi.org/10.1002/cpp.793
Robert-McComb, J. J., Tacon, A., Randolph, P., & Caldera, Y. (2004). Apilot study to examine the effects of a mindfulness-based stress-reduc-tion and relaxation program on levels of stress hormones, physicalfunctioning, and submaximal exercise responses. Journal of Alternativeand Complementary Medicine, 10, 819–827. http://dx.doi.org/10.1089/acm.2004.10.819
Robins, C. J., Keng, S. L., Ekblad, A. G., & Brantley, J. G. (2012). Effectsof mindfulness-based stress reduction on emotional experience andexpression: A randomized controlled trial. Journal of Clinical Psychol-ogy, 68, 117–131. http://dx.doi.org/10.1002/jclp.20857
Robinson, F. P., Mathews, H. L., & Witek-Janusek, L. (2003). Psycho-endocrine-immune response to mindfulness-based stress reduction inindividuals infected with the human immunodeficiency virus: A quasi-experimental study. Journal of Alternative and Complementary Medi-cine, 9, 683–694. http://dx.doi.org/10.1089/107555303322524535
Rosenkranz, M. A., Davidson, R. J., Maccoon, D. G., Sheridan, J. F.,Kalin, N. H., & Lutz, A. (2013). A comparison of mindfulness-basedstress reduction and an active control in modulation of neurogenicinflammation. Brain, Behavior, and Immunity, 27, 174–184. http://dx.doi.org/10.1016/j.bbi.2012.10.013
Rosenzweig, S., Greeson, J. M., Reibel, D. K., Green, J. S., Jasser, S. A.,& Beasley, D. (2010). Mindfulness-based stress reduction for chronicpain conditions: Variation in treatment outcomes and role of homemeditation practice. Journal of Psychosomatic Research, 68, 29–36.http://dx.doi.org/10.1016/j.jpsychores.2009.03.010
Rosenzweig, S., Reibel, D. K., Greeson, J. M., Brainard, G. C., & Hojat,M. (2003). Mindfulness-based stress reduction lowers psychologicaldistress in medical students. Teaching and Learning in Medicine, 15,88–92. http://dx.doi.org/10.1207/S15328015TLM1502_03
Rosenzweig, S., Reibel, D. K., Greeson, J. M., Edman, J. S., Jasser, S. A.,McMearty, K. D., & Goldstein, B. J. (2007). Mindfulness-based stressreduction is associated with improved glycemic control in type 2diabetes mellitus: A pilot study. Alternative Therapies in Health andMedicine, 13, 36–38.
Roth, B. (1997). Mindfulness-based stress reduction in the inner city.Advances, 13, 50–58.
Roth, B., & Creaser, T. (1997). Mindfulness meditation-based stressreduction: Experience with a bilingual inner-city program. The NursePractitioner, 22, 150–152, 154, 157 passim. http://dx.doi.org/10.1097/00006205-199703000-00013
Roth, B., & Robbins, D. (2004). Mindfulness-based stress reduction andhealth-related quality of life: Findings from a bilingual inner-city pa-tient population. Psychosomatic Medicine, 66, 113–123. http://dx.doi.org/10.1097/01.PSY.0000097337.00754.09
Roth, B., & Stanley, T. W. (2002). Mindfulness-based stress reduction andhealthcare utilization in the inner city: Preliminary findings. AlternativeTherapies in Health and Medicine, 8, 60–62, 64–66.
Rotheram-Borus, M. J., Swendeman, D., & Chorpita, B. F. (2012). Dis-ruptive innovations for designing and diffusing evidence-based inter-ventions. American Psychologist, 67, 463–476. http://dx.doi.org/10.1037/a0028180
Ruths, F. A., de Zoysa, N., Frearson, S. J., Hutton, J., Williams, J. M. G.,& Walsh, J. (2013). Mindfulness-based cognitive therapy for mentalhealth professionals: A pilot study. Mindfulness, 4, 289–295. http://dx.doi.org/10.1007/s12671-012-0127-0
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
617October 2015 ● American Psychologist
Sachse, S., Keville, S., & Feigenbaum, J. (2011). A feasibility study ofmindfulness-based cognitive therapy for individuals with borderlinepersonality disorder. Psychology and Psychotherapy, 84, 184–200.http://dx.doi.org/10.1348/147608310X516387
Salmoirago-Blotcher, E., Hunsinger, M., Morgan, L., Fischer, D., &Carmody, J. (2013). Mindfulness-based stress reduction and changein health-related behaviors. Journal of Evidence-Based Complemen-tary & Alternative Medicine, 18, 243–247. http://dx.doi.org/10.1177/2156587213488600
Samuelson, M., Carmody, J., Kabat-Zinn, J., & Bratt, M. A. (2007).Mindfulness-based stress reduction in Massachusetts correctional facil-ities. The Prison Journal, 87, 254–268. http://dx.doi.org/10.1177/0032885507303753
Saxe, G. A., Hébert, J. R., Carmody, J. F., Kabat-Zinn, J., Rosenzweig,P. H., Jarzobski, D., . . . Blute, R. D. (2001). Can diet in conjunctionwith stress reduction affect the rate of increase in prostate specificantigen after biochemical recurrence of prostate cancer? TheJournal of Urology, 166, 2202–2207. http://dx.doi.org/10.1016/S0022-5347(05)65535-8
Schmidt, S., Grossman, P., Schwarzer, B., Jena, S., Naumann, J., &Walach, H. (2011). Treating fibromyalgia with mindfulness-basedstress reduction: Results from a 3-armed randomized controlled trial.Pain, 152, 361–369. http://dx.doi.org/10.1016/j.pain.2010.10.043
Schroevers, M. J., & Brandsma, R. (2010). Is learning mindfulness asso-ciated with improved affect after mindfulness-based cognitive therapy?British Journal of Psychology, 101, 95–107. http://dx.doi.org/10.1348/000712609X424195
Segal, Z. V., Bieling, P., Young, T., MacQueen, G., Cooke, R., Martin, L.,. . . Levitan, R. D. (2010). Antidepressant monotherapy vs sequentialpharmacotherapy and mindfulness-based cognitive therapy, or placebo,for relapse prophylaxis in recurrent depression. Archives of GeneralPsychiatry,67,1256–1264.http://dx.doi.org/10.1001/archgenpsychiatry.2010.168
Segal, Z. V., Kennedy, S., Gemar, M., Hood, K., Pedersen, R., & Buis, T.(2006). Cognitive reactivity to sad mood provocation and the predictionof depressive relapse. Archives of General Psychiatry, 63, 749–755.http://dx.doi.org/10.1001/archpsyc.63.7.749
Segal, Z. V., Teasdale, J. D., Williams, J. M., & Gemar, M. C. (2002). Themindfulness-based cognitive therapy adherence scale: Inter-rater reli-ability, adherence to protocol and treatment distinctiveness. ClinicalPsychology & Psychotherapy, 9, 131–138. http://dx.doi.org/10.1002/cpp.320
Segal, Z. V., Williams, J. M., & Teasdale, J. D. (2002). Mindfulness-basedcognitive therapy for depression: A new approach to preventing re-lapse. New York, NY: Guilford Press.
Semple, R. J., Lee, J., Rosa, D., & Miller, L. F. (2010). A randomized trialof mindfulness-based cognitive therapy for children: Promoting mind-ful attention to enhance social-emotional resiliency in children. Journalof Child and Family Studies, 19, 218–229. http://dx.doi.org/10.1007/s10826-009-9301-y
Sephton, S. E., Salmon, P., Weissbecker, I., Ulmer, C., Floyd, A., Hoover,K., & Studts, J. L. (2007). Mindfulness meditation alleviates depressivesymptoms in women with fibromyalgia: Results of a randomized clin-ical trial. Arthritis and Rheumatism, 57, 77–85. http://dx.doi.org/10.1002/art.22478
SeyedAlinaghi, S., Jam, S., Foroughi, M., Imani, A., Mohraz, M., Djavid,G. E., & Black, D. S. (2012). Randomized controlled trial of mindful-ness-based stress reduction delivered to human immunodeficiency vi-rus-positive patients in Iran: Effects on CD4� T lymphocyte count andmedical and psychological symptoms. Psychosomatic Medicine, 74,620–627. http://dx.doi.org/10.1097/PSY.0b013e31825abfaa
Shahar, B., Britton, W. B., Sbarra, D. A., Figueredo, A. J., & Bootzin,R. R. (2010). Mechanisms of change in mindfulness-based cognitivetherapy for depression: Preliminary evidence from a randomized con-trolled trial. International Journal of Cognitive Therapy, 3, 402–418.http://dx.doi.org/10.1521/ijct.2010.3.4.402
Shapiro, S. L., Astin, J. A., Bishop, S. R., & Cordova, M. (2005).Mindfulness-based stress reduction for health care professionals: Re-sults from a randomized trial. International Journal of Stress Manage-ment, 12, 164–176. http://dx.doi.org/10.1037/1072-5245.12.2.164
Shapiro, S. L., Bootzin, R. R., Figueredo, A. J., Lopez, A. M., &Schwartz, G. E. (2003). The efficacy of mindfulness-based stress re-
duction in the treatment of sleep disturbance in women with breastcancer: An exploratory study. Journal of Psychosomatic Research, 54,85–91. http://dx.doi.org/10.1016/S0022-3999(02)00546-9
Shapiro, S. L., Brown, K. W., & Biegel, G. M. (2007). Teaching self-careto caregivers: Effects of mindfulness-based stress reduction on themental health of therapists in training. Training and Education inProfessional Psychology, 1, 105–115. http://dx.doi.org/10.1037/1931-3918.1.2.105
Shapiro, S. L., Brown, K. W., Thoresen, C., & Plante, T. G. (2011). Themoderation of mindfulness-based stress reduction effects by trait mind-fulness: Results from a randomized controlled trial. Journal of ClinicalPsychology, 67, 267–277. http://dx.doi.org/10.1002/jclp.20761
Shapiro, S. L., Jazaieri, H., & Goldin, P. R. (2012). Mindfulness-basedstress reduction effects on moral reasoning and decision making. TheJournal of Positive Psychology, 7, 504–515. http://dx.doi.org/10.1080/17439760.2012.723732
Shapiro, S. L., Oman, D., Thoresen, C. E., Plante, T. G., & Flinders, T.(2008). Cultivating mindfulness: Effects on well-being. Journal ofClinical Psychology, 64, 840–862. http://dx.doi.org/10.1002/jclp.20491
Shapiro, S. L., Schwartz, G. E., & Bonner, G. (1998). Effects of mind-fulness-based stress reduction on medical and premedical students.Journal of Behavioral Medicine, 21, 581–599. http://dx.doi.org/10.1023/A:1018700829825
Sharma, M. P., Sudhir, P. M., & Narayan, R. (2013). Effectiveness ofmindfulness-based cognitive therapy in persons with depression: Apreliminary investigation. Journal of the Indian Academy of AppliedPsychology, 39, 43–50.
Sharplin, G. R., Jones, S. B., Hancock, B., Knott, V. E., Bowden, J. A., &Whitford, H. S. (2010). Mindfulness-based cognitive therapy: An effi-cacious community-based group intervention for depression and anxi-ety in a sample of cancer patients. The Medical Journal of Australia,193, S79–S82.
Sibinga, E. M. S., Kerrigan, D., Stewart, M., Johnson, K., Magyari, T., &Ellen, J. M. (2011). Mindfulness-based stress reduction for urban youth.The Journal of Alternative and Complementary Medicine, 17, 213–218.http://dx.doi.org/10.1089/acm.2009.0605
Sibinga, E. M. S., Perry-Parrish, C., Chung, S. E., Johnson, S. B., Smith,M., & Ellen, J. M. (2013). School-based mindfulness instruction forurban male youth: A small randomized controlled trial. PreventiveMedicine, 57, 799–801. http://dx.doi.org/10.1016/j.ypmed.2013.08.027
Sibinga, E. M., Stewart, M., Magyari, T., Welsh, C. K., Hutton, N., &Ellen, J. M. (2008). Mindfulness-based stress reduction for HIV-in-fected youth: A pilot study. EXPLORE: The Journal of Science andHealing, 4, 36–37. http://dx.doi.org/10.1016/j.explore.2007.10.002
Simon, G. E., & Ludman, E. J. (2009). It’s time for disruptive innovationin psychotherapy. The Lancet, 374, 594–595. http://dx.doi.org/10.1016/S0140-6736(09)61415-X
Simpson, J., & Mapel, T. (2011). An investigation into the health benefitsof mindfulness-based stress reduction (MBSR) for people living with arange of chronic physical illnesses in New Zealand. The New ZealandMedical Journal, 124, 68–75.
Skovbjerg, S., Hauge, C. R., Rasmussen, A., Winkel, P., & Elberling, J.(2012). Mindfulness-based cognitive therapy to treat multiple chem-ical sensitivities: A randomized pilot trial. Scandinavian Journal ofPsychology, 53, 233–238. http://dx.doi.org/10.1111/j.1467-9450.2012.00950.x
Smith, A., Graham, L., & Senthinathan, S. (2007). Mindfulness-basedcognitive therapy for recurring depression in older people: A qualitativestudy. Aging & Mental Health, 11, 346–357. http://dx.doi.org/10.1080/13607860601086256
Smith, B. W., Shelley, B. M., Dalen, J., Wiggins, K., Tooley, E., &Bernard, J. (2008). A pilot study comparing the effects of mindfulness-based and cognitive-behavioral stress reduction. The Journal of Alter-native and Complementary Medicine, 14, 251–258. http://dx.doi.org/10.1089/acm.2007.0641
Smith, B. W., Shelley, B. M., Leahigh, L., & Vanleit, B. (2006). Apreliminary study of the effects of a modified mindfulness interventionon binge eating. Complementary Health Practice Review, 11, 133–143.
Splevins, K., Smith, A., & Simpson, J. (2009). Do improvements inemotional distress correlate with becoming more mindful? A study of
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
618 October 2015 ● American Psychologist

older adults. Aging & Mental Health, 13, 328–335. http://dx.doi.org/10.1080/13607860802459807
Stange, J. P., Eisner, L. R., Hölzel, B. K., Peckham, A. D., Dougherty,D. D., Rauch, S. L., . . . Deckersbach, T. (2011). Mindfulness-basedcognitive therapy for bipolar disorder: Effects on cognitive functioning.Journal of Psychiatric Practice, 17, 410–419. http://dx.doi.org/10.1097/01.pra.0000407964.34604.03
Szanton, S. L., Wenzel, J., Connolly, A. B., & Piferi, R. L. (2011).Examining mindfulness-based stress reduction: Perceptions from mi-nority older adults residing in a low-income housing facility. BMCComplementary and Alternative Medicine, 11, 44. http://dx.doi.org/10.1186/1472-6882-11-44
Tacón, A. M. (2011). Mindfulness: Existential, loss, and grief factors inwomen with breast cancer. Journal of Psychosocial Oncology, 29,643–656. http://dx.doi.org/10.1080/07347332.2011.615382
Tacón, A. M., Caldera, Y. M., & Ronaghan, C. (2004). Mindfulness-basedstress reduction in women with breast cancer. Families, Systems, &Health, 22, 193–203. http://dx.doi.org/10.1037/1091-7527.22.2.193
Tacón, A. M., McComb, J., Caldera, Y., & Randolph, P. (2003). Mind-fulness meditation, anxiety reduction, and heart disease: A pilotstudy. Family & Community Health: The Journal of Health Promo-tion & Maintenance, 26, 25–33. http://dx.doi.org/10.1097/00003727-200301000-00004
Teasdale, J. D. (1988). Cognitive vulnerability to persistent depression.Cognition and Emotion, 2, 247–274. http://dx.doi.org/10.1080/02699938808410927
Teasdale, J. D., Moore, R. G., Hayhurst, H., Pope, M., Williams, S., &Segal, Z. V. (2002). Metacognitive awareness and prevention of relapsein depression: Empirical evidence. Journal of Consulting and ClinicalPsychology, 70, 275–287. http://dx.doi.org/10.1037/0022-006X.70.2.275
Teasdale, J. D., Segal, Z., & Williams, J. M. G. (1995). How doescognitive therapy prevent depressive relapse and why should attentionalcontrol (mindfulness) training help? Behaviour Research and Therapy,33, 25–39. http://dx.doi.org/10.1016/0005-7967(94)E0011-7
Teasdale, J. D., Segal, Z. V., Williams, J. M. G., Ridgeway, V. A.,Soulsby, J. M., & Lau, M. A. (2000). Prevention of relapse/recurrencein major depression by mindfulness-based cognitive therapy. Journal ofConsulting and Clinical Psychology, 68, 615–623. http://dx.doi.org/10.1037/0022-006X.68.4.615
Thompson, B. (2009). Mindfulness-based stress reduction for people withchronic conditions. The British Journal of Occupational Therapy, 72,405–410. http://dx.doi.org/10.1177/030802260907200907
Thompson, N. J., Walker, E. R., Obolensky, N., Winning, A., Barmon, C.,Diiorio, C., & Compton, M. T. (2010). Distance delivery of mindful-ness-based cognitive therapy for depression: Project UPLIFT. Epilepsy& Behavior, 19, 247–254. http://dx.doi.org/10.1016/j.yebeh.2010.07.031
Troy, A. S., Shallcross, A. J., Davis, T. S., & Mauss, I. B. (2013). Historyof mindfulness-based cognitive therapy is associated with increasedcognitive reappraisal ability. Mindfulness, 4, 213–222. http://dx.doi.org/10.1007/s12671-012-0114-5
Tsang, S. C. H., Mok, E. S. B., Lam, S. C., & Lee, J. K. L. (2012). Thebenefit of mindfulness-based stress reduction to patients with terminalcancer. Journal of Clinical Nursing, 21, 2690–2696. http://dx.doi.org/10.1111/j.1365-2702.2012.04111.x
Vallejo, Z., & Amaro, H. (2009). Adaptation of mindfulness-basedstress reduction program for addiction relapse prevention. The Hu-manistic Psychologist, 37, 192–206. http://dx.doi.org/10.1080/08873260902892287
van Aalderen, J. R., Donders, A. R. T., Giommi, F., Spinhoven, P.,Barendregt, H. P., & Speckens, A. E. M. (2012). The efficacy ofmindfulness-based cognitive therapy in recurrent depressed patientswith and without a current depressive episode: A randomized controlledtrial. Psychological Medicine, 42, 989–1001. http://dx.doi.org/10.1017/S0033291711002054
van den Hurk, P. A. M., van Aalderen, J. R., Giommi, F., Donders,R. A. R. T., Barendregt, H. P., & Speckens, A. E. M. (2012). Aninvestigation of the role of attention in mindfulness-based cognitivetherapy for recurrently depressed patients. Journal of ExperimentalPsychopathology, 3, 103–120.
van der Lee, M. L., & Garssen, B. (2012). Mindfulness-based cognitivetherapy reduces chronic cancer-related fatigue: A treatment study.Psycho-Oncology, 21, 264–272. http://dx.doi.org/10.1002/pon.1890
van der Velden, A. M., Kuyken, W., Wattar, U., Crane, C., Pallesen, K. J.,Dahlgaard, J., . . . Piet, J. (2015). A systematic review of mechanismsof change in mindfulness-based cognitive therapy in the treatment ofrecurrent major depressive disorder. Clinical Psychology Review, 37,26–39. http://dx.doi.org/10.1016/j.cpr.2015.02.001
van Ravesteijn, H., Lucassen, P., Bor, H., van Weel, C., & Speckens, A.(2013). Mindfulness-based cognitive therapy for patients with medi-cally unexplained symptoms: A randomized controlled trial. Psycho-therapy and Psychosomatics, 82, 299–310. http://dx.doi.org/10.1159/000348588
van Son, J., Nyklícek, I., Pop, V. J., Blonk, M. C., Erdtsieck, R. J.,Spooren, P. F., . . . Pouwer, F. (2013). The effects of a mindfulness-based intervention on emotional distress, quality of life, and HbA(1c) inoutpatients with diabetes (DiaMind): A randomized controlled trial.Diabetes Care, 36, 823–830. http://dx.doi.org/10.2337/dc12-1477
Vieten, C., & Astin, J. (2008). Effects of a mindfulness-based interventionduring pregnancy on prenatal stress and mood: Results of a pilot study.Archives of Women’s Mental Health, 11, 67–74. http://dx.doi.org/10.1007/s00737-008-0214-3
Vøllestad, J., Sivertsen, B., & Nielsen, G. H. (2011). Mindfulness-basedstress reduction for patients with anxiety disorders: Evaluation in arandomized controlled trial. Behaviour Research and Therapy, 49,281–288. http://dx.doi.org/10.1016/j.brat.2011.01.007
Walach, H., Nord, E., Zier, C., Dietz-Waschkowski, B., Kersig, S., &Schüpbach, H. (2007). Mindfulness-based stress reduction as a methodfor personnel development: A pilot evaluation. International Journal ofStress Management, 14, 188–198. http://dx.doi.org/10.1037/1072-5245.14.2.188
Wang, P. S., Lane, M., Olfson, M., Pincus, H. A., Wells, K. B., & Kessler,R. C. (2005). Twelve-month use of mental health services in theUnited States: Results from the National Comorbidity Survey Rep-lication. Archives of General Psychiatry, 62, 629–640. http://dx.doi.org/10.1001/archpsyc.62.6.629
Weber, B., Jermann, F., Gex-Fabry, M., Nallet, A., Bondolfi, G., &Aubry, J. M. (2010). Mindfulness-based cognitive therapy for bipolardisorder: A feasibility trial. European Psychiatry, 25, 334–337. http://dx.doi.org/10.1016/j.eurpsy.2010.03.007
Weiss, M., Nordlie, J. W., & Siegel, E. P. (2005). Mindfulness-basedstress reduction as an adjunct to outpatient psychotherapy. Psychother-apy and Psychosomatics, 74, 108–112. http://dx.doi.org/10.1159/000083169
Weissbecker, I., Salmon, P., Studts, J. L., Floyd, A. R., Dedert, E. A., &Sephton, S. E. (2002). Mindfulness-based stress reduction and sense ofcoherence among women with fibromyalgia. Journal of Clinical Psy-chology in Medical Settings, 9, 297–307. http://dx.doi.org/10.1023/A:1020786917988
Weisz, J. R. (2014). Building robust psychotherapies for children andadolescents. Perspectives on Psychological Science, 9, 81–84. http://dx.doi.org/10.1177/1745691613512658
Weisz, J. R., Ng, M. Y., & Bearman, S. K. (2014). Odd couple? Reen-visioning the relation between science and practice in the dissemina-tion-implementation era. Clinical Psychological Science, 2, 58–74.http://dx.doi.org/10.1177/2167702613501307
Weitz, M. V., Fisher, K., & Lachman, V. D. (2012). The journey ofwomen with breast cancer who engage in mindfulness-based stressreduction: A qualitative exploration. Holistic Nursing Practice, 26,22–29. http://dx.doi.org/10.1097/HNP.0b013e31823c008b
Whitebird, R. R., Kreitzer, M., Crain, A. L., Lewis, B. A., Hanson, L. R.,& Enstad, C. J. (2013). Mindfulness-based stress reduction for familycaregivers: A randomized controlled trial. The Gerontologist, 53, 676–686. http://dx.doi.org/10.1093/geront/gns126
Williams, J. M. G., Alatiq, Y., Crane, C., Barnhofer, T., Fennell, M. J. V.,Duggan, D. S., . . . Goodwin, G. M. (2008). Mindfulness-based cog-nitive therapy (MBCT) in bipolar disorder: Preliminary evaluation ofimmediate effects on between-episode functioning. Journal of AffectiveDisorders, 107, 275–279. http://dx.doi.org/10.1016/j.jad.2007.08.022
Williams, J. M. G., Crane, C., Barnhofer, T., Brennan, K., Duggan, D. S.,Fennell, M. J., . . . Russell, I. T. (2014). Mindfulness-based cognitivetherapy for preventing relapse in recurrent depression: A randomized
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
619October 2015 ● American Psychologist

dismantling trial. Journal of Consulting and Clinical Psychology, 82,275–286. http://dx.doi.org/10.1037/a0035036
Williams, J. M. G., Duggan, D. S., Crane, C., & Fennell, M. J. V. (2006).Mindfulness-based cognitive therapy for prevention of recurrence ofsuicidal behavior. Journal of Clinical Psychology, 62, 201–210. http://dx.doi.org/10.1002/jclp.20223
Williams, J. M. G., & Kabat-Zinn, J. (2011). Mindfulness: Diverse per-spectives on its meaning, origins, and multiple applications at theintersection of science and dharma. Contemporary Buddhism, 12, 1–18.http://dx.doi.org/10.1080/14639947.2011.564811
Williams, J. M. G., Teasdale, J. D., Segal, Z. V., & Soulsby, J. (2000).Mindfulness-based cognitive therapy reduces overgeneral autobio-graphical memory in formerly depressed patients. Journal of AbnormalPsychology, 109, 150–155. http://dx.doi.org/10.1037/0021-843X.109.1.150
Williams, M. J., McManus, F., Muse, K., & Williams, J. M. G. (2011).Mindfulness-based cognitive therapy for severe health anxiety (hypo-chondriasis): An interpretative phenomenological analysis of patients’experiences. British Journal of Clinical Psychology, 50, 379–397.http://dx.doi.org/10.1111/j.2044-8260.2010.02000.x
Witek-Janusek, L., Albuquerque, K., Chroniak, K. R., Chroniak, C.,Durazo-Arvizu, R., & Mathews, H. L. (2008). Effect of mindfulnessbased stress reduction on immune function, quality of life and coping inwomen newly diagnosed with early stage breast cancer. Brain, Behav-ior, and Immunity, 22, 969–981. http://dx.doi.org/10.1016/j.bbi.2008.01.012
Wong, S. Y. S., Chan, F. W. K., Wong, R. L. P., Chu, M. C., Kitty Lam,Y. Y., Mercer, S. W., & Ma, S. H. (2011). Comparing the effectivenessof mindfulness-based stress reduction and multidisciplinary interven-tion programs for chronic pain: A randomized comparative trial. TheClinical Journal of Pain, 27, 724–734. http://dx.doi.org/10.1097/AJP.0b013e3182183c6e
Worsfold, K. E. (2013). Embodied reflection in mindfulness-based cog-nitive therapy for depression. The Humanistic Psychologist, 41, 54–69.http://dx.doi.org/10.1080/08873267.2012.732154
Würtzen, H., Dalton, S. O., Andersen, K. K., Elsass, P., Flyger, H. L.,Sumbundu, A., & Johansen, C. (2013). Who participates in a random-ized trial of mindfulness-based stress reduction (MBSR) after breastcancer? A study of factors associated with enrollment among Danishbreast cancer patients. Psycho-Oncology, 22, 1180–1185. http://dx.doi.org/10.1002/pon.3094
Würtzen, H., Dalton, S. O., Elsass, P., Sumbundu, A. D., Steding-Jensen,M., Karlsen, R. V., . . . Johansen, C. (2013). Mindfulness significantlyreduces self-reported levels of anxiety and depression: Results of arandomised controlled trial among 336 Danish women treated for StageI–III breast cancer. European Journal of Cancer, 49, 1365–1373.http://dx.doi.org/10.1016/j.ejca.2012.10.030
Yook, K., Lee, S. H., Ryu, M., Kim, K. H., Choi, T. K., Suh, S. Y., . . .Kim, M. J. (2008). Usefulness of mindfulness-based cognitive therapyfor treating insomnia in patients with anxiety disorders: A pilot study.Journal of Nervous and Mental Disease, 196, 501–503. http://dx.doi.org/10.1097/NMD.0b013e31817762ac
Young, L. A., & Baime, M. J. (2010). Mindfulness-based stress reduction:Effect on emotional distress in older adults. Complementary HealthPractice Review, 15, 59–64.
Young, L. E., Bruce, A., Turner, L., & Linden, W. (2001). Evaluation ofmindfulness-based stress reduction intervention. The Canadian Nurse,97, 23–26.
Zernicke, K. A., Campbell, T. S., Blustein, P. K., Fung, T. S., Johnson,J. A., Bacon, S. L., & Carlson, L. E. (2013). Mindfulness-based stressreduction for the treatment of irritable bowel syndrome symptoms:A randomized wait-list controlled trial. International Journal ofBehavioral Medicine, 20, 385–396. http://dx.doi.org/10.1007/s12529-012-9241-6
Thi
sdo
cum
ent
isco
pyri
ghte
dby
the
Am
eric
anPs
ycho
logi
cal
Ass
ocia
tion
oron
eof
itsal
lied
publ
ishe
rs.
Thi
sar
ticle
isin
tend
edso
lely
for
the
pers
onal
use
ofth
ein
divi
dual
user
and
isno
tto
bedi
ssem
inat
edbr
oadl
y.
620 October 2015 ● American Psychologist