prospective evaluation of three point of care devices for glycemia measurement in a neonatal...
TRANSCRIPT

Clinica Chimica Acta 425 (2013) 104–108
Contents lists available at ScienceDirect
Clinica Chimica Acta
j ourna l homepage: www.e lsev ie r .com/ locate /c l inch im
Prospective evaluation of three point of care devices for glycemiameasurement in a neonatal intensive care unit
Corinne Stadelmann Diaw a,1, Nicolas Piol a,1, Jocelyne Urfer b, Dominique Werner c, Matthias Roth-Kleiner a,⁎a Clinic of Neonatology, Department of Pediatrics, Centre Hospitalier Universitaire Vaudois (CHUV), University of Lausanne, CH-1011 Lausanne, Switzerlandb Department of Interdisciplinary Centers and Medical Logistic, Centre Hospitalier Universitaire Vaudois (CHUV), CH-1011 Lausanne, Switzerlandc Clinical Chemistry Laboratory, Centre Hospitalier Universitaire Vaudois (CHUV), University of Lausanne, CH-1011 Lausanne, Switzerland
⁎ Corresponding author at: Clinic of Neonatology, Centrdois, Av PierreDecker 2, CH-1011 Lausanne, Switzerland. T21 314 3477.
E-mail address: [email protected] (M. Roth-Klein1 Similar contributions.
0009-8981/$ – see front matter © 2013 Elsevier B.V. All rihttp://dx.doi.org/10.1016/j.cca.2013.07.021
a b s t r a c t
a r t i c l e i n f oArticle history:Received 13 May 2013Received in revised form 10 July 2013Accepted 19 July 2013Available online 29 July 2013
Keywords:GlycemiaPOCTPoint of careBlood glucose meterNeonatal hypoglycemia
Hypoglycemia, if recurrent, may have severe consequences on cognitive and psychomotor development ofneonates. Therefore, screening for hypoglycemia is a daily routine in every facility taking care of newborn infants.Point-of-care-testing (POCT) devices are interesting for neonatal use, as their handling is easy,measurements canbe performed at bedside, demanded blood volume is small and results are readily available. However, suchwholebloodmeasurements are challenged by awide variation of hematocrit in neonates and a spectrumof normal glu-cose concentration at the lower end of the test range. We conducted a prospective trial to check precision andaccuracy of the best suitable POCT device for neonatal use from three leading companies in Europe. Of thethree devices tested (Precision Xceed, Abbott; Elite XL, Bayer; Aviva Nano, Roche), Aviva Nano exhibited thebest precision. None completely fulfilled the ISO-accuracy-criteria 15197: 2003 or 2011. Aviva Nano fulfilledthese criteria in 92% of cases while the others were b87%. Precision Xceed reached the 95% limit of the 2003ISO-criteria for values ≤4.2 mmol/L, but not for the higher range (71%).Although validated for adults, new POCT devices need to be specifically evaluated on newborn infants beforeadopting their routine use in neonatology.
© 2013 Elsevier B.V. All rights reserved.
1. Introduction
In all facilities caring for newborn infants, screening for hypogly-cemia is of utmost importance. Although there is no agreement onthe lower normal limit of glycemia in newborn infants, valuesbelow 2.5 mmol/L, in particular when recurrent, may have a detri-mental impact on neurodevelopmental outcome [1–3]. Therefore,the ‘operational threshold’, meaning a glycemia level at which anintervention should be performed, is generally defined as glycemialevels ≤2.5 mmol/L [4,5]. Hence, there is an important need of glu-cose measurement for screening and management of hypoglycemiain neonates, as clinical signs are unspecific or in many casescompletely lacking. Three major criteria are required for such mea-surements in neonatology: 1) use of small blood samples, given thelimited total blood volume of neonates (80–100 ml/kg); 2) rapid re-sult availability; and 3) accurate and precise measure. The goldstandard for glucose measurement is the hexokinase method usedin many hospital laboratories. However, there is often an importanttime lag between the blood sampling and availability of the result.
e Hospitalier Universitaire Vau-el.:+41 21314 3223; fax:+41
er).
ghts reserved.
Furthermore, this method uses typically around 300 μl of blood foreach measurement. Point-of-care-testing (POCT) devices like portableblood glucose meters (BGM) respond perfectly to the first two of thethree criteria. However, they were primarily developed for self moni-toring of glycemia in adult diabetic patients, with the repetitive use ofone single device for the same patient [6]. Before using such devicesin neonatal intensive care units (NICU), particular issues have to be con-sidered: 1) One such device may be used once or repeatedly for thesame or very different patients ranging between extremely pretermbabies of b500 g to full term neonates of N4 kg. Therefore, such a deviceshould be able to give precise and accurate results in extremely differ-ent clinical situations. 2) Hematocrit, which can potentially confoundwhole blood glucose measurement, may vary between 20% and 70% inthe standard population of aNICU [7]. For these reasons, a newPOCTde-vice needs to be carefully investigated before being used in the neonatalpopulation. In general, BGM have shown a trend to overestimate glyce-mia values in neonates, leading to increased operational thresholds forhypoglycemia screeningwith suchmethods, and thus to overtreatmentand an increased number of useless blood tests in healthy newborns[8–11]. Although several suggestions for BGM selection in the neonatalpopulation and accuracy criteria for their use have been published, theirinvestigation in well-designed prospective studies in neonates is diffi-cult, regarding the ethical issue for additional blood sampling in thisvulnerable population [12–14]. With the help of an electronic patientdata acquisition system (DAS), we developed a method, within the

105C. Stadelmann Diaw et al. / Clinica Chimica Acta 425 (2013) 104–108
limits of our standard clinical procedure, to compare the results of dif-ferent POCT devices with the gold standard hexokinase method, with-out the need for additional blood sampling [15]. In collaboration withthree leading companies producing POCT devices, we tested prospec-tively their most appropriate BGM for bedside glycemia measurementin newborn infants over a one year period.
2. Materials and methods
2.1. Study design
This prospective study was performed between January 1st andDecember 31st 2010 in neonatal infants hospitalized at the Clinic ofNeonatology of the University Hospital of Lausanne (CHUV). Three ofthe leading companies in Europe in the field of POCT glucose measure-ment participated in an equal manner without, however, interfering inanyway neither in the planning and implementation of the study nor inthe analysis of the results. Theywere all asked to provide uswith twelvedevices of their potentially best POCT method for use in neonates. Thethree tested devices were: Precision Xceed (Abbott AG, Diabetes Care,Baar, Switzerland), Ascensia ELITE® XL (Bayer AG, Diabetes Care,Zurich, Switzerland), and Accu-Chek® Aviva Nano (Roche DiagnosticsAG, Rotkreuz, Switzerland). These test devices were randomly allocatedto 36 study nurses who received general information about the studyand a specific training on how to use their personal BGM which theyusedduring thewhole studyperiod. Characteristics of the three POCTde-vices are summarized in the online supplement (Online supplement —Online-Table 1).
2.2. Patients and sample selection
In accordance with our internal standard operating procedureregarding glucose measurement, the study nurses had to take into ac-count the BGM result. If it was≤3.0 mmol/L, they had to check glycemiaimmediately by sending 0.3 mL whole blood to the clinical chemistrylaboratory (CCL) of the CHUV. This volume of 0.3 mL whole blood wasdemanded in order to get theminimal required 60 μL of plasma volumenecessary to be able to perform the analysis, even if the hematocrit wasas high as 70%. Additionally, any planned glycemia test requested at theCCL was associated with a concomitant POCT measurement. All POCTtest results were immediately entered into the bedside electronic DAS(Metavision®, iMDsoft, Tel Aviv, Israel). Those from the CCL were auto-matically registered within 1 min after validation of the result in thelaboratory. Inclusion criteria of glycemia results for study purposeswere: 1) blood test performed and introduced into the DAS by one ofthe study nurses; 2) paired glycemia results from the same bloodsampling (first by POCT device, second by the CCL reference method)and 3) time interval b60 min between introduction of the two resultsinto the DAS which corresponds to the maximum allowed turnaroundtime. This time interval comprises the transfer of the blood sample tothe central laboratory, its reception, the centrifugation, the plasma de-cantation, the analysis itself and the validation of the result. The bloodsample was either anticoagulated with fluoride (if only glycemia wasdemanded) or with heparinate (if other analyses were required). Withthe computerized search engine of the DAS, all paired results meetingthese criteria were selected. The extracted raw data were transferredto an Excel table andmanually checked independently by two of the au-thors to verify the inclusion criteria. For clinical purposes, in some cases,part of the blood sampling was used to measure hematocrit. Thesevalues were used to analyze a potential influence of varying hematocritvalues on BGM performance. The method used for blood sampling hasbeen described recently [15]. The study was approved by the EthicsBoard for Research in Human of the Canton de Vaud. Because no addi-tional blood sampling was necessary for study purposes, no writtenconsent was requested.
2.3. Reference method
The reference method for plasma glucose measurement in the CCLwas the hexokinase/glucose-6-phosphate dehydrogenase method(Gluco-quant Glucose/HK, Modular P system, Roche Diagnostics AG,Rotkreuz, Switzerland), considered as gold standard.
2.4. Check of the performance of the POCT devices during the study
To discover any dysfunctional POCT device during the study period,all 36 BGM were tested with the respective control solutions providedby the three manufacturers (three concentration levels for PrecisionXceed and Elite XL, and two levels for Aviva Nano) at three time points:at the beginning of the study as part of the teaching and testing processof each study nurse, 6 months later in the middle of the study periodand at its end. All of the glucose determinations were within the toler-ated range indicated by the manufacturers and no BGM had to beexcluded from the study.
2.5. Quality control measurements of the POCT devices
Two within-run imprecision tests were conducted, one in an aque-ous and the second in a whole blood matrix. As aqueous matrices, thecontrol solutions (low and high glucose concentration), provided bythe manufacturers for their specific device were used. For the wholeblood matrix, the following protocol was used: 25 ml of venous wholeblood was drawn from a healthy volunteer donor and directly heparin-ized. The sample was kept three days at room temperature, leading toglycemia close to zero because of the naturally occurring glycolysis.The blood was then separated in 3 aliquots and spiked with differentvolumes of a concentrated glucose solution (100 mmol/L) in order togenerate final glucose concentrations of 2.2 mmol/L, 3.3 mmol/L and4.5 mmol/L, as assessed by the reference method. For both within-runimprecision tests three devices per company were randomly chosen.Twenty measurements were performed with each device on each ofthe five test solutions (2 aqueous and 3 whole blood solutions), leadingto n = 60 for each company and test solution.
2.6. ISO 15197 accuracy criteria: actual (2003) and proposed new (2011)
Accuracy of the three BGM was compared with ISO-criteria 15197,version 2003 and its proposed new version 2011 [14,16]. Toleratedrange for ISO criteria 15197:2003 is the following: for≥95% of samples,the difference of glycemia between POCT and reference method shouldbe within ±0.8 mmol/L for values ≤4.2 mmol/L and within ±20% forvalues N4.2 mmol/L. With the new ISO criteria 15197:2011, for ≥95%of samples, this tolerated difference should be within ±0.9 mmol/Lfor values ≤5.5 mmol/L and within ±15% for values N5.5 mmol/L.
2.7. Hematocrit measurements
For blood sampling in which a paired glycemia result and a simul-taneous hematocrit value was available, the influence of hematocriton accuracy of the BGM was assessed as described previously [15].Hematocrit was determined in the central laboratory of the CHUVon the automated Sysmex Hematology-Analyzer XE-2100 (SysmexDigitana AG, Horgen, Switzerland).
2.8. Statistics
Statistical analysis was performed using the software Analyse-it forMicrosoft Excel, version 2.20 (Analyse-it Software, Ltd. http://www.analyse-it.com, 2009). Agreement between each POCT method andthe gold standard was assessed using Passing and Bablok fits and biasplots, with the difference between the compared methods plottedagainst the reference method (modified Bland–Altman). Performance
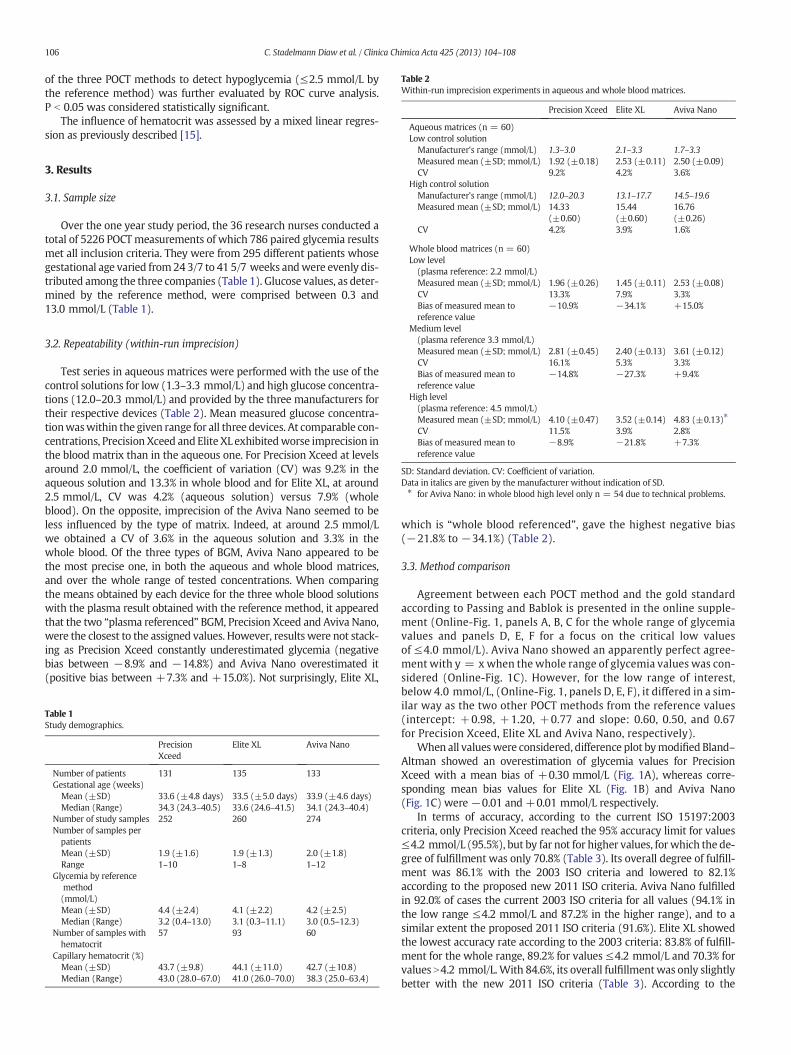
Table 2Within-run imprecision experiments in aqueous and whole blood matrices.
Precision Xceed Elite XL Aviva Nano
Aqueous matrices (n = 60)Low control solutionManufacturer's range (mmol/L) 1.3–3.0 2.1–3.3 1.7–3.3Measured mean (±SD; mmol/L) 1.92 (±0.18) 2.53 (±0.11) 2.50 (±0.09)CV 9.2% 4.2% 3.6%
High control solutionManufacturer's range (mmol/L) 12.0–20.3 13.1–17.7 14.5–19.6Measured mean (±SD; mmol/L) 14.33
(±0.60)15.44(±0.60)
16.76(±0.26)
CV 4.2% 3.9% 1.6%
Whole blood matrices (n = 60)Low level(plasma reference: 2.2 mmol/L)Measured mean (±SD; mmol/L) 1.96 (±0.26) 1.45 (±0.11) 2.53 (±0.08)CV 13.3% 7.9% 3.3%Bias of measured mean toreference value
−10.9% −34.1% +15.0%
Medium level(plasma reference 3.3 mmol/L)Measured mean (±SD; mmol/L) 2.81 (±0.45) 2.40 (±0.13) 3.61 (±0.12)CV 16.1% 5.3% 3.3%Bias of measured mean toreference value
−14.8% −27.3% +9.4%
High level(plasma reference: 4.5 mmol/L)Measured mean (±SD; mmol/L) 4.10 (±0.47) 3.52 (±0.14) 4.83 (±0.13)⁎
CV 11.5% 3.9% 2.8%Bias of measured mean toreference value
−8.9% −21.8% +7.3%
SD: Standard deviation. CV: Coefficient of variation.Data in italics are given by the manufacturer without indication of SD.⁎ for Aviva Nano: in whole blood high level only n = 54 due to technical problems.
106 C. Stadelmann Diaw et al. / Clinica Chimica Acta 425 (2013) 104–108
of the three POCT methods to detect hypoglycemia (≤2.5 mmol/L bythe reference method) was further evaluated by ROC curve analysis.P b 0.05 was considered statistically significant.
The influence of hematocrit was assessed by a mixed linear regres-sion as previously described [15].
3. Results
3.1. Sample size
Over the one year study period, the 36 research nurses conducted atotal of 5226 POCTmeasurements of which 786 paired glycemia resultsmet all inclusion criteria. They were from 295 different patients whosegestational age varied from24 3/7 to 41 5/7 weeks andwere evenly dis-tributed among the three companies (Table 1). Glucose values, as deter-mined by the reference method, were comprised between 0.3 and13.0 mmol/L (Table 1).
3.2. Repeatability (within-run imprecision)
Test series in aqueous matrices were performed with the use of thecontrol solutions for low (1.3–3.3 mmol/L) and high glucose concentra-tions (12.0–20.3 mmol/L) and provided by the three manufacturers fortheir respective devices (Table 2). Mean measured glucose concentra-tionwaswithin the given range for all three devices. At comparable con-centrations, Precision Xceed and Elite XL exhibitedworse imprecision inthe blood matrix than in the aqueous one. For Precision Xceed at levelsaround 2.0 mmol/L, the coefficient of variation (CV) was 9.2% in theaqueous solution and 13.3% in whole blood and for Elite XL, at around2.5 mmol/L, CV was 4.2% (aqueous solution) versus 7.9% (wholeblood). On the opposite, imprecision of the Aviva Nano seemed to beless influenced by the type of matrix. Indeed, at around 2.5 mmol/Lwe obtained a CV of 3.6% in the aqueous solution and 3.3% in thewhole blood. Of the three types of BGM, Aviva Nano appeared to bethe most precise one, in both the aqueous and whole blood matrices,and over the whole range of tested concentrations. When comparingthe means obtained by each device for the three whole blood solutionswith the plasma result obtained with the reference method, it appearedthat the two “plasma referenced” BGM, Precision Xceed and Aviva Nano,were the closest to the assigned values. However, results were not stack-ing as Precision Xceed constantly underestimated glycemia (negativebias between −8.9% and −14.8%) and Aviva Nano overestimated it(positive bias between +7.3% and +15.0%). Not surprisingly, Elite XL,
Table 1Study demographics.
PrecisionXceed
Elite XL Aviva Nano
Number of patients 131 135 133Gestational age (weeks)Mean (±SD) 33.6 (±4.8 days) 33.5 (±5.0 days) 33.9 (±4.6 days)Median (Range) 34.3 (24.3–40.5) 33.6 (24.6–41.5) 34.1 (24.3–40.4)
Number of study samples 252 260 274Number of samples perpatientsMean (±SD) 1.9 (±1.6) 1.9 (±1.3) 2.0 (±1.8)Range 1–10 1–8 1–12
Glycemia by referencemethod(mmol/L)Mean (±SD) 4.4 (±2.4) 4.1 (±2.2) 4.2 (±2.5)Median (Range) 3.2 (0.4–13.0) 3.1 (0.3–11.1) 3.0 (0.5–12.3)
Number of samples withhematocrit
57 93 60
Capillary hematocrit (%)Mean (±SD) 43.7 (±9.8) 44.1 (±11.0) 42.7 (±10.8)Median (Range) 43.0 (28.0–67.0) 41.0 (26.0–70.0) 38.3 (25.0–63.4)
which is “whole blood referenced”, gave the highest negative bias(−21.8% to −34.1%) (Table 2).
3.3. Method comparison
Agreement between each POCT method and the gold standardaccording to Passing and Bablok is presented in the online supple-ment (Online-Fig. 1, panels A, B, C for the whole range of glycemiavalues and panels D, E, F for a focus on the critical low valuesof ≤4.0 mmol/L). Aviva Nano showed an apparently perfect agree-ment with y = xwhen the whole range of glycemia values was con-sidered (Online-Fig. 1C). However, for the low range of interest,below 4.0 mmol/L, (Online-Fig. 1, panels D, E, F), it differed in a sim-ilar way as the two other POCT methods from the reference values(intercept: +0.98, +1.20, +0.77 and slope: 0.60, 0.50, and 0.67for Precision Xceed, Elite XL and Aviva Nano, respectively).
When all valueswere considered, difference plot bymodified Bland–Altman showed an overestimation of glycemia values for PrecisionXceed with a mean bias of +0.30 mmol/L (Fig. 1A), whereas corre-sponding mean bias values for Elite XL (Fig. 1B) and Aviva Nano(Fig. 1C) were −0.01 and +0.01 mmol/L respectively.
In terms of accuracy, according to the current ISO 15197:2003criteria, only Precision Xceed reached the 95% accuracy limit for values≤4.2 mmol/L (95.5%), but by far not for higher values, for which the de-gree of fulfillment was only 70.8% (Table 3). Its overall degree of fulfill-ment was 86.1% with the 2003 ISO criteria and lowered to 82.1%according to the proposed new 2011 ISO criteria. Aviva Nano fulfilledin 92.0% of cases the current 2003 ISO criteria for all values (94.1% inthe low range ≤4.2 mmol/L and 87.2% in the higher range), and to asimilar extent the proposed 2011 ISO criteria (91.6%). Elite XL showedthe lowest accuracy rate according to the 2003 criteria: 83.8% of fulfill-ment for the whole range, 89.2% for values ≤4.2 mmol/L and 70.3% forvalues N4.2 mmol/L.With 84.6%, its overall fulfillmentwas only slightlybetter with the new 2011 ISO criteria (Table 3). According to the

-4.5
-3.5
-2.5
-1.5
-0.5
0.5
1.5
2.5
3.5
4.5
0 5 10 15
IdentityTEa (0.8 or 20%)Bias (-0.01)
-4.5
-3.5
-2.5
-1.5
-0.5
0.5
1.5
2.5
3.5
4.5
0 5 10 15
Dif
fere
nce
Pre
cisi
on
Xce
ed -
Mo
du
lar
(mm
ol/L
)
Modular (mmol/L)
IdentityTEa (0.8 or 20%)Bias (0.30)
Dif
fere
nce
Elit
e X
L –
Mo
du
lar
(mm
ol/L
)
Modular (mmol/L)
-4.5
-3.5
-2.5
-1.5
-0.5
0.5
1.5
2.5
3.5
4.5
0 5 10Modular (mmol/L)
IdentityTEa (0.8 or 20%)Bias (0.01)
Dif
fere
nce
Avi
vaN
ano
–M
od
ula
r (
mm
ol/L
)
A B CISO-criteria 2003 (<0.8 or <20%) ISO-criteria 2003 (<0.8 or <20%)
ISO-criteria 2003 (<0.8 or <20%)
Fig. 1. Bias Plots for the three POCT methods. Difference of glycemia values between the POCT device and the reference method plotted against the reference (A: Precision Xceed; B: EliteXL; C: Aviva Nano).
107C. Stadelmann Diaw et al. / Clinica Chimica Acta 425 (2013) 104–108
proposed new 2011 ISO criteria, Aviva Nano and Precision Xceed weresimilar in the range ≤5.5 mmol/L (94.8% and 94.0% of fulfillment re-spectively) but Aviva Nano performed much better in the higherrange (83.5% versus 58.8%).
3.4. Sensitivity and specificity
The ROC curve analysis on the ability of the three types of BGMto correctly classify hypoglycemia (≤2.5 mmol/L by the referencemethod) and non-hypoglycemia showed a similar area under the ROCcurve for all three methods (Precision Xceed: 0.90; Elite XL: 0.89,Aviva Nano: 0.93; for more details, see Online-Table 2). In order not tomiss any hypoglycemia (sensitivity of 100%), the minimum cut-offwould have to be set at 3.2 mmol/L for Precision Xceed and at2.9 mmol/L for the two other devices. However, at such levels, specific-ity was only between 43% and 53% for the three BGM (Online-Table 2).
Table 3Degree of fulfillment of current (2003) and proposed new (2011) ISO accuracy criteria15197.
Precision Xceed Elite XL Aviva Nano
Total number of samples (n) 252 260 274
ISO criteria 15197: 2003Number of samples:With glycemia ≤4.2 mmol/L 156 186 188With glycemia N4.2 mmol/L 96 74 86
ISO criteria fulfilled*For glycemia ≤4.2 mmol/L 95.5% 89.2% 94.1%For glycemia N4.2 mmol/L 70.8% 70.3% 87.2%
Overall fulfillment* 86.1% 83.8% 92.0%
Proposed ISO criteria 15197: 2011Number of samples:With glycemia ≤5.5 mmol/L 167 201 195With glycemia N5.5 mmol/L 85 59 79
ISO criteria fulfilled†
For glycemia ≤5.5 mmol/L±0.3 mmol/L 58.1% 49.3% 62.1%±0.6 mmol/L 84.4% 76.6% 87.7%±0.9 mmol/L 94.0% 89.6% 94.9%
ISO criteria fulfilled†
For glycemia N5.5 mmol/Lb5% 25.9% 39.0% 43.0%b10% 41.2% 57.6% 73.4%b15% 58.8% 67.8% 83.5%
ISO criteria fulfilled†
For all values 82.1% 84.6% 91.6%
Data in bold are calculated percentages and not statistical values.† These are calculated percentages and not statistically evaluated means.
3.5. Influence of hematocrit
When plotting the difference of glycemia values between each POCTdevice and the reference method against the hematocrit (Online-Fig. 2in the online supplement), it appeared that all 3 BGM exhibited a signif-icant dependency on hematocrit. Slopes for Precision Xceed, Elite XLand Aviva Nano were −0.026 (p = 0.017), −0.020 (p = 0.007) and−0.020 (p = 0.013), respectively. This means that, depending on thedevice, every 10% hematocrit decrease led to a glycemia overestimationof 0.20 to 0.26 mmol/L.
4. Discussion
Blood glucose measurement in newborn infants is challenging, asnormal neonatal glycemia values are far below the normal rangefound in adults and may lie at the limit of performance of POCT de-vices. Therefore, BGM, if intended to be used in neonatology, shouldundergo a specific and careful evaluation in this particular population,ideally without supplementary need for blood sampling. In clinicalpractice, a differentiation between ‘blood glucose monitoring in neo-natal capillary blood’ and ‘screening for neonatal hypoglycemia’, asit may be done in the FDA approval for use of POCT devices in new-born infants, is not applicable in the daily routine. Performance of aPOCT device has to fulfill both indications in order to be useful inneonatology. This prospective study compared three different POCTdevices over one year in parallel and assessed their performanceagainst the simultaneous glycemia measurements by the hexokinasereference method. To our surprise, none of the three BGM fulfilledthe ISO 15197:2003 accuracy criteria on the whole range of glycemiameasurements [14]. The situation was quite similar with the new pro-posed ISO-criteria 15197:2011 [16]. One could anticipate that this wasdue to the biased sample selection with a relatively increased numberof samples with low glycemia values. But all three devices performedbetter in the lower glucose concentration range (≤4.2 mmol/L for2003 ISO criteria and ≤5.5 mmol/L for 2011 ISO criteria), with Preci-sion Xceed fulfilling the current 2003 ISO criteria (95.5%) and Avivanano almost fulfilling them (94.1%) as well as the proposed new2011 criteria (94.9%). The fact that ISO-criteria were not completelyfulfilled in this study, whereas in others some POCT devices seemedto have achieved this, is difficult to explain [17]. A limitation of ourstudy is that the clinical setting did not exactly match the laboratoryconditions described by the ISO requirements: 1) BGM were used atbedside, whereas measurements by the reference method wereperformed at distance from the NICU after transportation to the CCLand plasma separation, meaning a delay before completion of analy-sis. However, a turnaround time of b60 min between specimen col-lection and validation of the result was maintained. Delayed plasma

108 C. Stadelmann Diaw et al. / Clinica Chimica Acta 425 (2013) 104–108
separation is known to potentially affect the blood glucose level, butChan et al. showed that such changes corresponded to only a slightreduction of the initial glucose values [18]. Therefore, the clinicallyoriented study conditions might explain to some extent the over-estimation of BGM results, but as the conditions were the same forall three study devices, this does not explain the differences observedbetween them. 2) Due to the study protocol and the normal range ofglycemia values in newborns, the demanded distribution of blood glu-cose values by the ISO criteria (e.g. 10% of all samples should be in therange of 16.6 mmol/L to 22.2 mmol/L, and 5% N22.2 mmol/L) was notmaintained. Zero values were N16.6 mmol/L. However, as already men-tioned, all BGMs showed a better fulfillment of the ISO criteria in lowervalues, meaning that a strict application of the ISO study specificationwould probably evenworsen the results. With an overall 92% fulfillmentof both 2003 and 2011 ISO criteria, Aviva Nano appeared to be the mostaccurate of the three BGMs tested. The limited agreement, in particular ofthe Precision Xceed compared to the reference method might be due to,in part, its increased imprecision and, in the case of Elite XL, to the factthat it is “whole blood referenced”.
Repeated episodes of low glycemia values (b2.5 mmol/L) in new-born infants may compromise their long-term development [2,3]. Neo-nates, and in particular preterm infants, tend to have low glycemiavalues due to the transition from continuous transplacental glucosesupply during fetal life to the slowly increasing, intermittent nutrition,postnatally. Therefore,many newborn infants have to undergo frequentblood glucose measurements during their first postnatal days as ascreening for hypoglycemia. In order not to miss hypoglycemia, amajor criterion for the utilization of BGM in neonatology is a high sensi-tivity. Several studies with different POCT devices have highlighted atrend to overestimate glucose concentrationwhich led to a higher oper-ational threshold for resultsmeasured by these devices compared to thereference method [8–11,19]. We confirm these studies as a 100% sensi-tivity was only reached with minimal cut-off values of 2.9 (Elite XL andAviva Nano) and 3.2 mmol/L (Precision Xceed). At these levels, howev-er, specificity was just around 50%, meaning that half of the measure-ments below these cut-off values, which would need to be tested bythe reference method, wouldn't correspond to true hypoglycemia.When accepting a N95% sensitivity, the operational threshold wouldbe decreased insignificantly for the Aviva Nano to 2.8 mmol/L, but stillneeding one third of the samples to be controlled due to a specificityof 66.1% (data not shown).
As shown by different investigators recently [20–26], we confirmthat hematocrit interferes with blood glucose measurement by allthree POCT devices. The main trend, compared to the gold standard,was towards an overestimation of glycemia values in the low hemato-crit range. The association reached significance for all three BGM. Thisobservation might be of clinical importance, as there is a risk that realhypoglycemia could be missed in anemic patients.
5. Conclusion
None of the three tested POCT devices reached the goal of currentor proposed new ISO 15197 accuracy criteria over the whole range ofglycemia values. Altogether, Aviva Nano showed the best performance,both in terms of precision and accuracy. Before being used in neonatol-ogy, we suggest that all new BGM, although validated in the adultpopulation, need a specific and careful evaluation in newborn infantsin order to assess their limitations. In the rapidly evolving fieldof new BGM development, such clinical trials are only possiblewith a good collaboration between clinicians, laboratory staff andmanufacturers.
Supplementary data to this article can be found online at http://dx.doi.org/10.1016/j.cca.2013.07.021.
Acknowledgments
The study was jointly supported by the companies Abbott AG(Diabetes Care, Baar, Switzerland), Bayer AG (Diabetes Care, Zurich,Switzerland) and Roche Diagnostics AG (Rotkreuz, Switzerland),by providing the required glucometers, test strips and control solu-tions for the whole study period. We thank Dr. A. Horsch for the crit-ical revision of the manuscript.
References
[1] Wayenberg JL, Pardou A. Moderate hypoglycemia in the preterm infant: is it rele-vant? Arch Pediatr 2008;15:153–6.
[2] Duvanel CB, Fawer CL, Cotting J, Hohlfeld P,Matthieu JM. Long-termeffects of neonatalhypoglycemia on brain growth and psychomotor development in small-for-gestational-age preterm infants. J Pediatr 1999;134:492–8.
[3] Lucas A, Morley R, Cole TJ. Adverse neurodevelopmental outcome of moderateneonatal hypoglycaemia. Br Med J 1988;297:1304–8.
[4] CornblathM, Hawdon JM,Williams AF, et al. Controversies regarding definition of neo-natal hypoglycemia: suggested operational thresholds. Pediatrics 2000;105:1141–5.
[5] Cowett RM, Loughead JL. Neonatal glucose metabolism: differential diagnoses,evaluation, and treatment of hypoglycemia. Neonatal Netw 2002;21:9–19.
[6] Savoca R, Jaworek B, Huber AR. New “plasma referenced” POCT glucose monitoringsystems — are they suitable for glucose monitoring and diagnosis of diabetes? ClinChim Acta 2006;372:199–201.
[7] Jopling J, Henry E, Wiedmeier SE, Christensen RD. Reference ranges for hematocritand blood hemoglobin concentration during the neonatal period: data from a mul-tihospital health care system. Pediatrics 2009;123:e333–7.
[8] Bellini C, Serra G, Risso D, Mazzella M, Bonioli E. Reliability assessment of glucosemeasurement by HemoCue analyser in a neonatal intensive care unit. Clin ChemLab Med 2007;45:1549–54.
[9] Ho HT, Yeung WK, Young BW. Evaluation of “point of care” devices in the measure-ment of low blood glucose in neonatal practice. Arch Dis Child Fetal Neonatal Ed2004;89:F356–9.
[10] Michel A, Kuster H, Krebs A, et al. Evaluation of the Glucometer Elite XL device forscreening for neonatal hypoglycaemia. Eur J Pediatr 2005;164:660–4.
[11] Rosenthal M, Ugele B, Lipowsky G, Kuster H. The Accutrend sensor glucose analyzermay not be adequate in bedside testing for neonatal hypoglycemia. Eur J Pediatr2006;165:99–103.
[12] Sirkin A, Jalloh T, Lee L. Selecting an accurate point-of-care testing system: clinicaland technical issues and implications in neonatal blood glucose monitoring. J SpecPediatr Nurs 2002;7:104–12.
[13] MovaliaMK, OginoMT. Point of care glucose testing in neonatal hypoglycemia. PointCare 2006;5:95–9.
[14] International Organization for Standardization. In vitro diagnostic test systems —
requirements for blood-glucose monitoring systems for self-testing in managingdiabetes mellitus. Geneva, Switzerland: ISO 15197; 2003.
[15] Roth-Kleiner M, Stadelmann Diaw C, Urfer J, Ruffieux C, Werner D. Evaluation ofdifferent POCT devices for glucose measurement in a clinical neonatal setting. EurJ Pediatr 2010;169:1387–95.
[16] Hasslacher C, Kulozik F, PIatten I. Accuracy of self monitoring blood glucosesystems in a clinical setting: application of new planned ISO-standards. Clin 2012.http://dx.doi.org/10.7754/Clin.Lab.2012.120710.
[17] Freckmann G, Baumstark A, Jendrike N, et al. System accuracy evaluation of 27 bloodglucose monitoring systems according to DIN EN ISO 15197. Diabetes Technol Ther2010;12:221–31.
[18] Chan AY, Swaminathan R, Cockram CS. Effectiveness of sodium fluoride as a preser-vative of glucose in blood. Clin Chem 1989;35:315–7.
[19] Papp M, Sharief N. Comparison of two strip test methods of whole blood glucosemeasurement in the neonatal period. Acta Paediatr 2001;90:1042–6.
[20] Balion C, Grey V, Ismaila A, Blatz S, Seidlitz W. Screening for hypoglycemia at thebedside in the neonatal intensive care unit (NICU) with the Abbott PCx glucosemeter. BMC Pediatr 2006;6:28.
[21] Nuntnarumit P, Chittamma A, Pongmee P, Tangnoo A, Goonthon S. Clinical perfor-mance of the new glucometer in the nursery and neonatal intensive care unit.Pediatr Int 2011;53:218–23.
[22] St-Louis P, Ethier J. An evaluationof three glucosemeter systems and their performancein relation to criteria of acceptability for neonatal specimens. Clin Chim Acta 2002;322:139–48.
[23] Holtzinger C, Szelag E, DuBois JA, Shirey TL, Presti S. Evaluation of a new POCTbedside glucose meter and strip with hematocrit and interference corrections.Point Care 2008;7:1–6.
[24] Hussain K, Sharief N. The inaccuracy of venous and capillary blood glucose measure-ment using reagent strips in the newborn period and the effect of haematocrit. EarlyHum Dev 2000;57:111–21.
[25] Louie RF, Tang Z, Sutton DV, Lee JH, Kost GJ. Point-of-care glucose testing: effects ofcritical care variables, influence of reference instruments, and a modular glucosemeter design. Arch Pathol Lab Med 2000;124:257–66.
[26] Tang Z, Lee JH, Louie RF, Kost GJ. Effects of different hematocrit levels on glucosemeasurements with handheld meters for point-of-care testing. Arch Pathol LabMed 2000;124:1135–40.