props - communication.aau.dk · sociology, marketing and psychology. here after we do use the term...
TRANSCRIPT

PROPS Research Protocol
The usage of PRO data in psychiatric outpatient care - a pilot study.

Research Protocol PROPS_ver2_110416
Page 2/27
Table of Content 1. Project responsible .................................................................................................................................... 3
2. Collaborators ............................................................................................................................................. 3
3. Staff............................................................................................................................................................ 3
4. Background ................................................................................................................................................ 3
5. Problem ..................................................................................................................................................... 4
6. Hypotheses - tentative .............................................................................................................................. 4
7. State of the art ........................................................................................................................................... 5
8. Methods .................................................................................................................................................... 9
9. Material ................................................................................................................................................... 12
10. Purpose .................................................................................................................................................... 12
11. Statistical considerations ......................................................................................................................... 14
12. Implementation ....................................................................................................................................... 15
13. Biobank .................................................................................................................................................... 16
14. Testparticipants ....................................................................................................................................... 16
15. Side effects, risks and cons ...................................................................................................................... 17
16. Respect of the test participant’s mental integrity and data privacy ....................................................... 17
17. Application of EPJ data in the experiment .............................................................................................. 17
18. Budget and financies ............................................................................................................................... 17
19. Recruitment of test participants and test participant’s remuneration ................................................... 18
20. Informed Consent .................................................................................................................................... 19
21. Dissemination of research results ........................................................................................................... 19
22. Ethic research .......................................................................................................................................... 19
23. Disclosure of compensation or reimbursement schemes ....................................................................... 20
24. References ............................................................................................................................................... 20
Appendix A Description of Method ................................................................................................................. 23
Appendix B Description of the data requested from the EPJ .......................................................................... 23
Appendix C Documentation of the registration to the Datatilsyn .................................................................. 23
Appendix D Budget .......................................................................................................................................... 24
Appendix E Time schedule for the project ...................................................................................................... 26
Appendix F Test person information form ...................................................................................................... 27
Appendix G Informed Consent Document ...................................................................................................... 27

Research Protocol PROPS_ver2_110416
Page 3/27
1. Project responsible Professor, chief physician, dr.med. Jørgen Aagaard, Psychiatric Hospital/Aalborg University Hospital
Professor, Ph.D. Srikant Sarangi, Director of Danish Institute of Humanities and Medicine, Aalborg
University.
2. Collaborators Ms. Cs Morten Aagaard, Aalborg University.
The project aims to establish a praxis related study in which both clinician psychiatric expertise, humanistic-
communication expertise and competences in computer based cognitive support tools are represented. All
at a high level. Publication will take place in the psychiatric field as well as the communication field.
3. Staff Other collaborators will be involved ad hoc.
It is
Clinicians at outpatient clinic for psychosis at Aalborg Psychiatric Hospital, Aalborg University
Hospital. Primarily nurses.
Administrative staff at DIHM at Aalborg University.
Administrative staff at DIHM at Aalborg University Hospital.
4. Background For many good reasons it is preferred that most psychiatric patients are treated as outpatients.
Unfortunately are the psychiatric treatment not an elimination of foreign element in the patient’s body, but
a challenging life situation in which the symptoms do reoccur with smaller or stronger significance. One
serious consequence is that many outpatients have symptoms that return despite that they have been
declared free of symptoms and they return to the clinic or hospital again.
Within some psychiatric patient groups up to 70% of the patients drop out of treatment and are later
referred to the hospital again.
Thus, within the group of patients referred to an ordinary psychosis clinic at a psychiatric hospital, a very
high dropout is often the case, and most of these patients discontinue simultaneously with their
psychopharmacological treatment with increased risk of relapse and re-hospitalisation. For psychotic
patients who are affiliated a clinic for first onset schizophrenia (Opus) or a clinic for assertive community
treatment (ACT) with a low caseload, e.g. 8-10 patient/CM, the dropout rate and noncompliance rate is
rather low, however this principles of outpatient treatment is rather expensive (Aagaard et al.(2014)).
The target group for Mobil technology in this study is patient referred to an ordinary outpatient clinic for
psychotic disorders.

Research Protocol PROPS_ver2_110416
Page 4/27
The mobile technology has evolved through the last decade and is now mature and everybody property.
Some researchers claim that “Your mobile is the friend that accompany your 24x7” (Fogg, B.J) and there has
been developed a wealth of health apps that support individuals in monitoring of own individual state and
compliance with a plan for a set of behavioural changes. Exercises and weight loss are well-known topics.
Unfortunately, are the usage of mobile technology in ambulant psychiatric treatment faced with a number
of challenges that diminish the research and usage of mobile technology in ambulant psychiatric treatment.
5. Problem Unfortunately, ambulant treatment has significant limitations related to the fact that it is ambulant. First of
all, the treatment, that is the clinical conversations, is based on the patient’s ability to recall of the last
periods situations, challenges and solutions. The recall bias is a well-known bias in studies of the human
mind. But a special problem for this type of patient is their cognitive impairment. The recall bias is even
stronger with this patient group. Secondly patient’s compliance with the clinicians advises can be limited.
Studies show that patients compliance with medical treatment can be significantly limited. Thirdly, the
clinical support when patients are challenged is limited – which especially is a significant limitation in
situation of a crisis.
For reasons above it seems valuable to supplement the current ambulant treatment with a 24x7 present
treatment.
6. Hypotheses - tentative The 6 hypotheses that will be examined in the project:
1. The usage of PRO data app promotes parameters in ambulant psychiatric treatment: presence at
clinical conversations, dropout rates, hospitalisation and medical compliance.
2. The usage of PRO data app promotes higher experienced patient satisfaction the patient will
improve their ability to handle crisis’ when using the PRO data app.
3. There exist assessments forms that are neither qualitative nor quantitative.
4. The usage of such assessments forms that are neither qualitative nor quantitative prove valuable in
clinical settings.
5. The usage of visualised PRO data will influence the clinician conversations in terms of patient
relevance and value and patient’s compliance with behavioural advices.
6. The usage of PRO-data and supplied mobile technology set new demands to clinicians and the
organisation of the ambulant clinic.
The project is entitled “The usage of PRO data in psychiatric ambulant treatment – a pilot study. (PROPS)”.

Research Protocol PROPS_ver2_110416
Page 5/27
7. State of the art State of the art with the field using patient data is a challenge state to investigate. Despite a significant
interest, the field does not form one single body. The opposite seems to be the case. The field is scattered.
Due to this lack of a single body the PubMed search string is:
("Patient Reported Outcome"[All Fields] OR "Ecological Momentary Assessment"[All Fields] OR "Self report"
[All Fields]) AND "schizophrenia"[MeSH Terms]
The result is 335 items. “Self Report” is an ambiguous term and most likely the items of interest are approx.
100.
The field is divided into two “terms”. "Patient Reported Outcome” and "Ecological Momentary
Assessment".
At search in the meta-meta-research database scholar.google.com gives an indication which term is most
popular
Ecological momentary Assessment(EMA) 9820 posts
Patient Reported Outcome(PRO) 29.000 posts
When meta-meta databases counts items there is a risk that items are counted several times. That factor in
increasing with higher numbers and the amount of research using the term “Patient Reported Outcome” is
probably larger than the EMA research but most likely a factor 2-2.5 larger.
The PRO research is obviously within health research while EMA research takes place in heath, but also
sociology, marketing and psychology. Here after we do use the term “Patient Reported Outcome” (PRO)
because of those reasons. We are aware that valuable research takes place within the Ecological
Momentary Research (EMA).
Researcher do not recognise their research related to a new phenomenon, a new way of doing data
collection, but to the field itself. E.g. do the journal “Dialogues in clinical neuroscience” have PRO as a term
for their journal (Thibaut, F. (2016)), but unfortunately do only the editorial note use the term!
A final indication of a not so mature research is that neither of the terms, "Patient Reported Outcome" and
“Ecological Momentary Assessment” are not PubMed Mesh topic.
Furthermore, do the rapid technological development limit the relevance of “old” “Patient Reported
Outcome” research. Android and IPhone mobile technology was invented in 2007 and had a remarkable
impact on the possibilities for designing useful PRO apps. The technology was utilised in 2008. Today the
usage and the technology has changed. Research experiments and their dissemination last 3-4 year. We
have not excluded older research but has paid attention to the timestamps of the article and the bulk for
the referenced articles are later than 2010.
The strategy for identifying valuable articles has been
Find most quoted articles – and articles that refer to the articles

Research Protocol PROPS_ver2_110416
Page 6/27
Find journals with focus on innovation in research rather than RCT and study articles about PRO
and EMA
Find articles on that combine PRO or EMA with schizophrenia or psychiatry - and articles that refer
to the articles
All three strategies have been investigated while having awareness to the relevant articles publication year.
When the Patient Reported Outcome field in this way scattered this state is scattered as well. Despite that
fact there are a number of interesting observations of the current state of the art.
Observations 1: Definition
Most articles starting point is a specific medical field. E.g. Molecular Biology, Pharmacy research or
eventually psychiatry or schizophrenia though the last 2 fields are rare.
Few articles (Ilda et al (2012), Meyer et al(2009), Shiffman et al. (2009), Deshpande et al.(2011) make an
attempt to give an overview of the field PRO or EMA. Unfortunately, is the “…terms overlap and are used
inconsistently, and these reports of experience should be distinguished from expressions of preference
regarding health states” (Meyer et al (2009)).
Two definitions of PRO/EMA can elicit some of the differences.
In the EMA field one article by (Shiffman et al. (2009), p3-4) important. In that article they define “EMA as a
collection of methods for obtaining repeated real-time assessment of the individual’ behaviour and
experience.
1. Data are collected in real-world environments
2. Assessments focus on subjects’ current state
3. Moments are strategically selected for assessment
4. Subjects complete multiple assessments over time”
(Shiffman et al. (2009), p3-4)
In the same article, (Shiffman et al (2009)) points out that assessment collected can be introspective
assessment and it can be biological measures and it can be data about the current real-world setting of the
individual.
(Deshpande et al. (2011) is a represent for the Clinician perspective on patient’ data collection. First of all
(Deshpande et al. (2011), p137) states that “the measurements come directly from the patient”, opposite
to data collected by the clinician. They frame the term by declaring “The outcomes are broadly classified
into
1. clinical (e.g. cure, survival),
2. humanistic (e.g. role performance,
3. emotional status) and
4. economical (e.g. expenses, saving)
The only common denominator of the two articles are 1) The data is collected by the individual 2) The data
is introspective.

Research Protocol PROPS_ver2_110416
Page 7/27
The latter have the consequence that the focus in much PRO/EMA research is in QoL and HRQOL.
Observations 2: Positive effect
Despite the lack of clear definition within the field(s) there is a shared pleasure stating the fact that data
collected the individual do have many positive properties.
(Trull et all(2009)) states that “ (a) Real-time assessments increase accuracy and minimize retrospective
bias; (b) repeated assessments can reveal dynamic processes; (c) multimodal assessments can integrate
psychological, physiological, and behavioral data; (d) setting- or context-specific relationships of symptoms
or behaviors can be identified; (e) interactive feedback can be provided in real time; and (f) assessments in
real-life situations enhance generalizability.”
(Shiffman et al. (2009)) states that a number of bias can be eliminated: most important recall bias, but
social bias and cognitive heuristic bias as well.
The consequence of the elimination of bias and the high sampling rates are that PROdata give a detailed
documentation of states of moment trends. Due to the fact that the patient has collected them increases
the credibility of the analysis afterwards.
Due to the fact that these bias can be eliminated QoL studies are often the case in PRO investigations.
Studies within the psychiatric field a number of positive features are identified:
a) In the article “Routine outcome monitoring and feedback on physical or mental health status: evidence
and theory” (Carlier et al.(2012),p107) concludes that “PRO data appears especially effective for the
monitoring of patients who are not doing well in therapy. Further research into this topic and the clinical-
and cost-effectiveness of ROM is recommended”. In this way, PRO data could be an alternative to
traditional treatment, but no substantial argument is given.
b) Regarding the Patient-Clinician collaboration “On the basis of the evidence, incorporating subjective
assessments into the treatment process itself and in treatment evaluation is warranted. Routine assessment
of patient-reported outcomes (e.g.needs for care) might reduce potential discrepancy between patients and
professionals, and improve outcome, although there is little empirical evidence to support this assumption
at present.” A viewpoint that (Carlier (2012),p105) finds supported in his review “Consistently positive
results of ROM as an outcome measure were shown on the communication between patient and health care
professional, both on the short and longer period.”
c) In the review article “Patient Reported Outcome in schizophrenia (McCabe et al (2009)) (one of the only
reviews within the schizophrenia field) the conclusions are supporting the general positive judgement of
PRO data, but request solid evidence documenting the properties.
In general, the measurement of most important parameters of psychiatric treatment e.g. presence at
clinical conversations and medical compliance is absent in the articles reviewed.
Observation 3: PRO data focus on measurements
Most PRO data investigations use predefined assessments scales (McCabe et al (2009)). On the other hand,
(Sartorius (2014), p123 (Patient-reported outcomes in psychiatry) argues that PRO’ “…recognition of the
partnership role that the patients should have in research on outcome of mental illness.” Further, “In their
recognition, treatment, and prevention psychiatrists rely on their observations and on communication with

Research Protocol PROPS_ver2_110416
Page 8/27
people who suffer from these disorders”. Sartorious’ point is that PRO data and its usage ought to be an
integral part of psychiatric treatment.
He points out that PRO data collection not is for the sake of the clinician. But for the patient’ ability to recall
situations, challenges and periods and bring them into the treatment.
In that way PRO data collection balance to needs 1) sound, reproducible data collection 2) Support for the
patient-clinician collaboration.
Observation 4: Technology insight: Data collection can be specialised/individualised
A main trend in computer language and data modelling through the decades has been a strong focus on the
ability to model generic cases and that the same time model and handle specialised cases. Invention of
object orientated programming languages on example. Invention of XML is another.
In the literature review no experiments is reviewed in which the possibility of individualising the PROapp
and the data collection is an issue. When studying articles which aims to establish a sound theoretical
framework for EMA/PRO(Ilda et al(2012),Meyer et al(2009), Shiffman et al. (2009), Deshpande et al.
(2011) there is no discussion on this property and potential absent. When considering media or technology
the considerations in all three articles lack a reflection on the properties of modern software architecture.
Which includes considerations on the potential of individualisation of PROapps.
Regarding reviews, McCabe et al. (2007) gives an overview of 21 investigations in the article “Patient-
reported outcomes in schizophrenia”. None of the 21 outcome scales that do include some sort of
individualisation. Meyer, K. B., & Clayton, K. A. (2009) comes to the same conclusion in their review but
points out that QoL measurements should be individualised.
“The domain coverage of commonly used generic short forms varies substantially. Individualized
measurement of quality of life is possible, but resource intensive”
The consequence for PRO data is that you need not give all patients the same treatment but similar to the
research in the individualisation of medication schizophrenic patients can get each their PROapp.
Generalisation/Individualisation of PRO data and -collection is not a topic in any of the PRO/EMA data.
Observation 5: Technology insight: Enduser programming
Programming has been considered as a demanding technical discipline that produced software as an
artefact. During the last 10 years this way of developing software has met limitations. Most important is the
limitation that technical skilled engineers have to understand a domain. This has been a significant barrier
in a number of fields. For that reason Enduser development tools (Dietricht et al.(2013)) has emerged and it
is most likely that it is an attractive way of developing PROapps for patients.
The consequence for PRO data and PROapp is that the professional psychiatric competence can be
integrated in the PRO app far easier than before.
Observation 6: Technology insight: Missing PRO data visualised
In the literature review there has been no discussion on topics like: 1) How are PRO data presented for the
patient? 2) How are PRO data integrated in the clinician treatment?
Despite the fact that the PRO data may change the fundament for the clinician treatment. The articles in

Research Protocol PROPS_ver2_110416
Page 9/27
the review do not contain one single data visualisation of PRO data despite the fact that data visualisations
can be a strong communication tool in the clinician-patient collaboration.
The consequence for PRO data and PRO app is that the benefits are not harvested.
Conclusions - state of the art
The main conclusion is that the usage of PRO data can be highly valuable in the psychiatric ambulant
treatment. However, the field is scattered theoretically and the experiments are close related to traditions
within special fields of medicine. The PRO data collection is compromise between sound, reproducible data
collection and data collection that support patient-clinician collaboration.
The impact of the usage of PRO data on important psychiatric parameters like precedence and medical
compliance is not well investigated.
8. Methods The PROPS investigation is a pilot study due to the fact that the current state of research is scattered. The
PROPS project collects a number of data sources and that facilitates an open-ended research. The
hypothesis’ demands that the feasibility PRO data and -app of the in several means.
The PROPS investigation will be followed up by a case control investigation with higher demands to validity
and reproducibility of research results.
The purpose of the pilot study is to perform a holistic evaluation of the Demands, Effects and Impact of PRO
data. A visualisation of the 6 hypotheses of the pilot study can be viewed below.
Clinicial performanceH1,H5
Technologys organisational impact
H6
Patients satisfaction
H2,H5
New assesments
H3,H4
Evaluation of the usage of PROdata

Research Protocol PROPS_ver2_110416
Page 10/27
Figure 1 Overview of Pilot studies Hypothesis's
After examination of the 6 hypothesis the pilot study will be concluded in an external review in which the
usage of PRO data will be examined. The external review will be a seminar with researchers in psychiatry,
health communication and health researchers in general.
An experiment in real clinical settings
The investigation takes place at the ambulant clinic for psychotic disorders Psychiatric Hospital/Aalborg
University Hospital. The number of participants are limited to 10 test persons and the test takes 4 months.
In the project design it is an aim to 1) make the test conditions as close to real clinical settings as possible.
2) to ease innovation of the clinical praxis with PRO data and -app.
Regarding the latter, the used technologies already exist: the server being used are the one that is already
being used in RN/Psychiatric Hospital and the mobiles that are being used is the test persons own.
To facilitate the open-ended research several empirical sources will be designed.
N Empirical source Type When
1 Test person health journal Existing Health record data
Before and during the experiment
2 Department retrieved: Patient population
data regarding dropout hospitalisations
figures and attendance list.
Department administration data
During the experiment
3 Screening (clinician observation) Combined interview and questionnaire
Before the experiment
4 Assessment (introspective assessment) Mobil app During the experiment
5 Logdata (behavior) and accelerometer
data from usage of the app
Mobile app interaction During the experiment
6 Log of technical breakdowns and
inceptions where patients or clinicians are
challenged.
A log maintained by the
the PROPS project
During the experiment
7 Clinician interview Combined interview and questionnaire
After the experiment
8 Single patient interview Interview combined with
analysis of patient’ data
After the experiment
9 Focusgroup interview Interview After the experiment Table 1 Overview of empirical sources collected in the PROPS project
This set enables includes quantitative as well as qualitative. It includes different perspectives on the usage
of PROapp -and data: how the PROapp actually has been used (Logdata), test persons own subjective
viewpoint and clinicians view on the test person and his usage of the PROapp.

Research Protocol PROPS_ver2_110416
Page 11/27
Furthermore, a pretest and post-test conditions are collected which enable us to investigate a development
of a change of attitude and change in usage of the PROapp.
Finally, the logdata documents the actual usage of the PROapp. How often, when and what types of
functionalities are being logged. This facilitate that the PROPS investigation can triangulate real usages and
test person subjective experience.
A walkthrough of the hypotheses:
Below a description of the methods used to examine the single hypothesis. The methods used are in most
cases open methods.
Hypothesis 1
The usage of PRO data app promotes parameters in ambulant psychiatric treatment: presence at clinical
conversations, drop-out rates, hospitalisation and medical compliance.
General hospital register data concerning consultations, drop-outs, and measurements for drug compliance
in the specific outpatient’s clinic, compared to cases (test persons).
Hypothesis 2
The usage of PRO data app promotes higher experienced patient satisfaction the patient will improve their
ability to handle crisis’ when using the PRO data app.
The interview with the test persons aims to detect the level of satisfaction with the PROapp tool and their
ability to react adequately in states of crisis. Further, the individual test person primary contact nurse will
be interviewed concerning specific management of a crisis situation. In parallel, an observational study will
take place in form of a log data investigation.
Hypothesis 3
There exist assessments forms that are neither qualitative nor quantitative.
PROPS project develops a number of quasi-qualitative/quasi-quantitative assessment types (qqqqa). An
example of such qqqqa is circumflex model that can be designed as a Visual Analog Scale, as two
dimensional visualisations and as a randomised word cloud. This is a design study that makes use of the
PROPS projects interdisciplinary composition. A number of design will be elaborated and in a heuristic
evaluation workshop (Stone et al (2005), p525-556) will take place in which the design will be inspected
from a Health Communication and a Psychiatric Clinical perspective.
Hypothesis 4
The usage of such assessments forms that are neither qualitative nor quantitative prove valuable in clinical
settings.
The evaluation of the qqqqa takes place as heuristic inspections (Stone et al (2005), p525-556) involving the
users (test patients and clinicians. The log data will be analysed as well.
Hypothesis 5
The usage of visualised PRO data will influence the clinician conversations in terms of patient relevance and
value and patient’s compliance with behavioural advices.
Based on recorded data we will analyse how visualised PRO data is incorporated into the clinic consultation
– especially, its sequential positioning and the attendant explanations and understandings as manifest in
talk-in-interaction.

Research Protocol PROPS_ver2_110416
Page 12/27
Hypothesis 6
The usage of PRO-data and supplied mobile technology set new demands to clinicians and the organisation
of the ambulant clinic.
The empirical sources used is 6 and 7. Empirical source 6 “Log of technical breakdowns and inceptions
where patients or clinicians are challenged” will be analysed in 2 dimension: 1) Severity of breakdown –
classified in a … 2) Whether the breakdown is caused by the PROapp software as such or the breakdown
can be categorised as “childhood disease”. Furthermore, clinicians are interviewed with regards to changed
work procedures and benefits of the PRO data technology. Again the identified challenges are categorised
as “childhood disease”. Or properties of PROapp software. The interview template is not yet elaborated.
Conclusions
The PROPS investigation is a pilot study and a prerequisite for a larger clinical experiment with higher
validity and reliability. The outcome of the PROPS experiment is first of all an evaluation of the feasibility of
PRO data in clinician settings from multiple perspectives. The PROPS research project will be able to have a
realistic judgement of all the various positive properties of PRO data develop a realistic clinic adaptable
technological setup.
9. Material The data collected in the PROPS project is illustrated in section 8 Methods, p9.
The actual design of the 2-6 is a topic of the investigation and is to be elaborated.
The EPJ data which will be requested for the PROPS project is essential information regarding their
diagnosis and treatment which includes the patients actual treatment.
The app is a tool for the ambulant patient and contains 3 functionalities: Subjective symptom assessment,
crisis card and visual symptom diary. All three functions can be adapted to the patient abilities and needs.
The adaption takes place as an integral part of the clinician-patient collaboration in a manner that ensures
that the patient do not suffer or is harmed in any way. The app prompts/notifies the patient 1-3 times per
day and request the patient to do a self assessment. The app stores these assessments, log data from the
app and data collected from the accelerometer during usage of the app. These data are available in the
treatment at the hospital. The data are stored at the serverpark of RN. So are the clinicians application
which enables the clinician to adapt the app to the patient and inspect the collected patient data in the
meetings with the patient. The patient app is being downloaded from Appstores and adapted to the single
patient when the patient insert her patientcode. If the patient deletes the app, the app is deleted.
10. Purpose For many good reasons many psychiatric patients are treated ambulant. In the age of mobile technology, it
seems obvious that ambulant treatment can be improved by the usage of mobile technology. The
foundation for a treatment is insight in the patient situation, challenges, symptoms and subjective
experience of his/her disease and situation uninterpretated should be the foundation for the treatment.

Research Protocol PROPS_ver2_110416
Page 13/27
Data collected at home/in ordinary situation are more reliable due to the fact that the recall bias and social
bias is eliminated, support for the patient in form of crisis cards can be present at hand for the patient
when patient faces a crisis. Furthermore, do the patient-clinician get a new tool for a collaboration, data
visualisations which is a new insight to the patient state and development.
All these observations are positive and can be found in the research literature. One article obviously call it
….a new era in clinical research.
Unfortunately do the state of art in the research not form a uniform image rather the opposite. (A full state
of the art can be found in the section 7 State of the art). The research is scattered using various labels
where the most used are Patient Reported Outcome (PRO). The possibility that patients can collect data
themselves attract interest from many areas within Health science. Nevertheless, the research in PRO data
has not shaped uniform interest within psychiatry and the ordinary pubmed search for articles return
meager results.
No Query Posts Source
1 "Patient Reported Outcome"[All Fields] AND
("schizophrenia"[MeSH Terms] OR "schizophrenia"[All
Fields])
9 Pubmed
3 "Patient Reported Outcome"[All Fields] AND
"psychiatry"[MeSH Major Topic]
3 Pubmed
5 "Schizophrenia"[All Fields] AND "mhealth"[All Fields]) 61 Pubmed
6 "Ecological Momentary Assessment"[All Fields] AND
(schizoph[All Fields]
10 Pubmed
8 "Ecological Momentary Assessment"[All Fields] AND OR
"psychiatry"[All Fields])
130 Pubmed
Due to this scattered image the purpose of the PROPS pilot study is to evaluate the costs and benefits of
using PRO data in clinical settings. A follow-up by a case control study will be performed.
Another observation in the research literature about technology. Mobile technology develops at a fast pace
and technology used in 2008 is different to the one that is being used in 2015. The user/patient capability
to use mobiles are different too. The technology enables in 2015 that apps can individualised to the single
individual needs. Furthermore, the technology enables the classical divide in assessment design to be
questioned. Assessment need not only be numbers, categories or text, but more valuable assessment can
be developed.
The PRO data collected by the patient will have to be integrated in the clinician-patient collaboration.
Unfortunately, PRO articles have few articles where this is a topic. Data visualisation technologies fertilize
the collaboration by bringing data collected by the patient into the collaboration and the data is not a single
event but data shown on a timeline. Again this tool for collaboration has to be studied.
Implementation of new technology in the treatment of ambulant patients should not only fulfil demands to
a more successful treatment, but should function in the organisation, should be easily adaptable for the
patient, be valuable for the clinicians and improve the efficiency of the treatment of ambulant psychiatric
patients. The purpose of the pilot study is to do a holistic evaluation of the effects of the usage of PRO data

Research Protocol PROPS_ver2_110416
Page 14/27
app in the treatment of ambulant schizophrenic patients. The pilot study and the following external review
of the studys purpose is to design a larger and more valid in case control study.
11. Statistical considerations The PROPS project is benefitting from modern science challenge and burden. The low cost of data
collection and a significant number of valuable empirical sources that need to be triangulated.
PROPS is a pilot study with 10 participants, and with many data from different data sources. Only
descriptive statistics are applied.
Calculation of sample size for primary and secondary outcome measurements does not make sense.
However, when the results of the pilot study are available a new protocol for a PRO app case-control study
will be elaborated.
To enable data triangulation a data warehouse and a data visualisation worksheet will be elaborated. The
analysis of the empirical is methods from human science and medicine. The data warehouse can handle
both. So can the data visualisation worksheet.
1. Data warehouse
The data warehouse will form one uniform access to all data sources and enable to see each piece of data
by itself but most important will the data warehouse enable accessing related data fast. Most important get
access to all data about a patient.
What Technical format
1 Test person health journal Unknown. Most likely Excel
2 Department retrieved: Patient population data regarding
dropout and hospitalisation figures and attendance list.
Unknown. Most likely Excel
3 Screening (clinician observation) Excel
4 Assessment (introspective assessment) MS-SQL(resides at RN/KoncernIT)
5 Logdata (behavior) and accelerometer data from usage of
the app
MS-SQL(resides at RN/KoncernIT)
6 Log of technical breakdowns and inceptions where
patients or clinicians are challenged.
MS-SQL(resides at RN/KoncernIT)
7 Clinician interview MS-SQL(resides at RN/KoncernIT)
8 Patient Interview MS-SQL(resides at RN/KoncernIT)
9 Focusgroup interview MS-SQL(resides at RN/KoncernIT)

Research Protocol PROPS_ver2_110416
Page 15/27
2. Data visualisation
To combine and visualise the many data sources tableau has been chosen. The tableaus facilitate rapid
design of a large variety of graphs that can be combined in dashboards.
PROPS is a pilot study with 10 participants, and with many data from different data sources. Only
descriptive statistics are applied.
Calculation of sample size for primary and secondary outcome measurements does not make sense.
However, when the results of the pilot study are available a new protocol for a PRO app case-control study
will be elaborated.
Hypothesis 1
For the Performance Measurements Tableau will offer all descriptive statistics visualisations and
calculations. If further statistical analysis is required, the statistical equitation has to be formulated and
integrated in the Tableau workbook in the same manner as SPSS or SAS.
Hypotheses 2, 3, 5 and 6
The palette of methods has not yet been decided but dashboards that facilitates simple seeing the data can
rapidly be developed. Data dashboards that enable the researchers to study the same phenomena is easy
to develop as well. The PROPS project will develop its own data visualisations that is suitable for exactly
that kind of analysis activities that is most relevant. 5-15 dashboards can be elaborated.
If tableaus data visualisations do not seem appropriate, the data warehouse can be accessed directly and
data can be seen in other tools.
12. Implementation The pilot study takes place at an outpatient clinic for psychotic disorders at Aalborg University Hospital. The
patient data from the EPJ is gathered when the Informed Consent document have been signed by all test
patients.
The recruitment of test patients is the responsibility of the clinicians of the department at Brandevej in
collaboration with the PROPS project responsible.
The exacted data are kept in excel files and each patient are only identifiable by a randomized serial
number. The randomized serial number -test person identification table does on exists in one copy and this
only copy resides at the PROPS project responsible at the Aalborg University Hospital.
The PRO app data produces data and they are stored at a database at KoncernIT/RN. The handling of the
data while they are on the patients mobile, while being transmitted to the server and stored on the server
takes place according to the regulations and recommendations from Region Nord regarding the usage of
mobile phones. (Cornelliussen (2014)).
The instructions in usage of the PRO app, take place as an integral part of the ordinary treatment of the test
patients. So due the continuous evaluation of the use of the PRO app and its data and the technical
support.

Research Protocol PROPS_ver2_110416
Page 16/27
The final focusgroup interview of the test patients do also take place in the Brandevej department.
Regarding the PRO app it should be mentioned that there exists a PRO app toolkits which is the starting
point of the sw development. During the first 3 month of the project this PRO app toolkits app will be
tested intensively and the outpatient clinic suitable PRO app will be configured.
A permission to implement the pilot study at the head of the Psychiatry/Aalborg University Hospital will be
applied.
The Pilot study design contains a “Bring-Your-Own-Device”(BYOD) attitude, the PRO app toolkit are able to
create cross platform apps(Android and IPhone platform) and the server part is integrated in the ordinary
RN IT infrastructure. In that way the PROPS can converge from a pilot study to a tool for the outpatient
clinic at Brandevej.
Due to the fact that the PROPS project is a pilot study it is an aim that the administrative overhead is kept
minimal.
13. Biobank Not relevant.
14. Testparticipants The inclusion criteria are:
Patient diagnosed and treated for schizophrenia at least 1 year .
Men and women, age >18.
Informed consent.
Outpatients attending clinic for psychotic disorders,Psychiatric hospital,Brandevej, will be selected.
Outpatients are enrolled as independent patients and can at any stage of a treatment leave the
treatment.
The exclusion criteria are:
Patients that exhibit uncontrolled, random behaviour.
Patients that recently have made suicide attempts.
Patients enrolled in Assertive Community Treatment(ACT).
Actions taken as described in the “Informed consent” document, when exclusion criteria occur during
the test.
As mentioned in the section Ethic , the patient can leave during the test by of own will and can be
advised to do so by the project responsible.

Research Protocol PROPS_ver2_110416
Page 17/27
15. Side effects, risks and cons The test person is asked to install and use a PROPS mobile app during the test person. The PROPS mobile
app will prompt the test person 0-4 times per day.
The precautions are:
If any technical problems occur, they can contact the PROPS hotline. If problems related to the treatment
occurs, they can contact PROPS clinician.
It is possible that the test person mental state is influenced negatively. The test person is instructed (The
Informed Consent) that they are free to deinstall the PRODE mobile app anytime. Clinicians are instructed
to be aware of a negative change in the test person mental state and they can anytime stop the usage of
the PROPS mobile app too.
All interviews including the final focus group interview last in average 1 hour. There are 3 interviews
planned. There are no side effects of interviews besides that they can be tiresome. Nevertheless, a
debriefing after the focus group is offered to the test persons.
16. Respect of the test participant’s mental integrity and data privacy Information regarding the test person is protected by law regarding to handling of data privacy and in
accordance with health legislation. The project will be registered at The Danish Data Protection Agency.
There will be used data from the EPJ in the research project which is documented in Appendix B, p23.
Afterwards, additional information can be accessed only if the patient and clinician who have been
responsible for the treatment permit such access according to health legislation
The actual recruitment of patients is organised in this way: the clinicians of the ambulatory will be informed
about the experiment and the clinicians will select appropriate patients from the patient population.
17. Application of EPJ data in the experiment The EPJ data which will be requested for the PROPS project is essential information regarding their
diagnosis and treatment. The data include the patients actual treatment.
The purpose to of usage of the EPJ data is to verify the inclusion criteria and to use the EPJ data as data for
the analysis of the intervention.
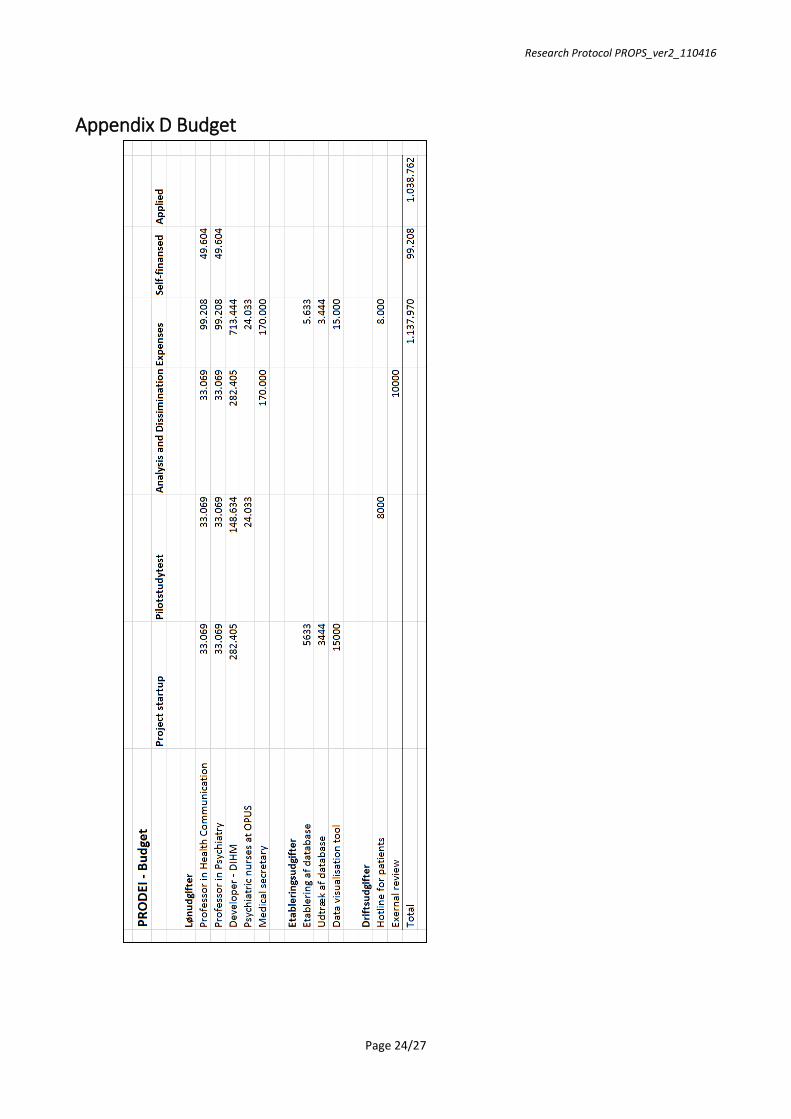
18. Budget and financies The pilot study investigation last totally 1 years. It includes software setup, clinician test, analysis and
dissemination of research results. The budget can be revised in Appendix D Budget.
Potential sources of funding are:
A.P. Møller Fonden
Augustinusfonden
Axel Muusfeldts Fond

Research Protocol PROPS_ver2_110416
Page 18/27
Danske Banks Fond
Den Bøhmske Fond
Det Obelske Familiefond
ENV- Fonden
Forløbsprogram for mennesker med psykiske lidelser - Socialstyrelsen
Frimodt-Heineke Fonden
Gangstedfonden
Harboefonden
Helsefonden
Jascha Fonden
Knud Højgaards Fond
Købmand Sven Hansen og hustru Ina Hansens Fond
Lundbeckfonden
Nordea-fonden
Torben og Alice Frimodts Fond
Aase og Ejnar Danielsens Fond
The investigations responsible and the collaborators in the PROPS project do not receive any kind of
support to implement the investigation. There is no commercial support. The PROPS project is exclusively
financed by public and private funds. When financial support will be obtained the support will be deposited
on a research account. The budget is accessible in Appendix D Budget.
19. Recruitment of test participants and test participant’s remuneration The test person does not receive remuneration or other kinds of support besides the ordinary clinician
treatment. The overall idea of the pilot project is to study the impact of the usage of Patient Reported
Outcome in the treatment of schizophrenic patients in real clinician settings.
The test persons are recruited among patients diagnosed with schizophrenia and referred to the outpatient
clinic for patients who suffer from a psychotic disorder at Psychiatric Hospital, Aalborg.
The principal investigator is responsible for recruitment of patients to the study.
When patients have shown interest in participation a meeting can be setup between Research test
responsible, patient, clinician and eventually patients relatives. If the patient still is willing to participate the
patient receives “Test person information form” (see Appendix F Test person information form) and
“Information Consent” (see Appendix G Informed Consent Document) and one week of consideration
before the final participation in the research project is confirmed.
After approximately 1-2 weeks the patient will be enrolled in the PROPS project. The participation in the
project is equal to attending ordinary clinician activities and the usage of a mobile app at home. The data
from the patients mobile (behavioural data and assessment data) will be used in the clinician activities.

Research Protocol PROPS_ver2_110416
Page 19/27
20. Informed Consent See description in section above (Recruitment of test participants and test participant’s remuneration). The
Form “S1” from ”samtykkeerklæringS1S122012.doc” is being used as Informed Consent confirmation.
21. Dissemination of research results Results of the research will be published regardless of the results are positive, negative or inconclusive. This
will take place as soon as possible with respect to high professional standards and according to the data
privacy regulations.
When results cannot be published in journals the results will be published elsewhere (e.g.
www.clinicaltrial.gov or www.clinicaltrialsregister.eu).
In the PROPS project the following guidelines regarding publication. To be (co-)author of a publication a
substantial contribution is required in minimum 2 areas. 1) Project planning/implementation of the
protocol, 2) Implementation of the data collection, 3) The statistical elaboration/analysis, 4) Elaboration of
the publication.
The PROPS project is already publishing results from PROPS project.
(Aagaard, M. (2016) – a poster representation and Aagaard, M. (2016) – an oral presentation. Both at
Comet2016.
22. Ethic research With regards to advantages of the participation:
Ambulant schizophrenia patients the offer to such patients are treatment that takes place at the hospital.
When using mobile technology treatment can be present 24x7. That is the patient can be assessed in real
world settings, the patient can have advices and support present 24x7. Truly ambulant treatment. The
patient will in the PROPS project gain from the experience of this ambulant treatment. The advantages,
challenges and disadvantages. Short term and long term.
With the regards to disadvantages of participation:
Ambulant schizophrenia patients will be using a mobile phone app that they can interact with or neglect.
However, a premium feature of Patient Reported Outcome data collection is that the software itself can
initiate an interaction. The mobile app can prompt the user for an assessment or possibly suggest a set of
behaviour (exercise or the like). Such prompt may in worst case cause unintended set of behaviours or
recalls that again lead the patient in a crisis being alone at home.
In our review in the PRO research we have not read about such cases and such backside of data collection is
not mentioned in the PRO research neither in the research field Ecological Momentary Assessment.
The PROPS project has three mechanisms to avoid such disaster. 1) During the recruitment of test persons,
patients that exhibit uncontrolled, random behaviour are not included. Patients that recently have made
suicide attempts I nether included. 2) While the test takes place the clinicians shall monitor the patients

Research Protocol PROPS_ver2_110416
Page 20/27
state and when the patients state changes to worse, consider if the patient should end her/his
participation. 3) Whenever the patient asks to leave the PROPS project the patient are free to do so.
The second disadvantage of the participation is that there exists a possibility that a test person actually gets
a great treatment by using the PRO app and gets dependent of the usage of the PROapp. In such cases do
the PROapp project find a suitable substitute.
23. Disclosure of compensation or reimbursement schemes The Patient Compensation Association, chapter 3 will cover harm which a test person may experience in
the PROPS project.
24. References
Albrechtslund, A. (2007). Ethics and technology design. Ethics and Information Technology, 9(1), 63-72.
Carlier, I. V., Meuldijk, D., Van Vliet, I. M., Van Fenema, E., Van der Wee, Nic JA, & Zitman, F. G. (2012). Routine outcome monitoring and feedback on physical or mental health status: Evidence and theory. Journal of Evaluation in Clinical Practice, 18(1), 104-110.
Chen, E. Y., Hui, C. L., Lam, M. M., Chiu, C. P., Law, C., Chung, D. W., et al. (2010). Maintenance
treatment with quetiapine versus discontinuation after one year of treatment in patients with remitted first episode psychosis: Randomised controlled trial. Bmj, 341, c4024.
Cornelliussen, S. Sikkerhed i mobile løsninger (sikkerhedskrav - mobility.docx) KoncernIT/RegionNord, accessed 02/2015
Csikszentmihalyi, M., & Larson, R. (1987). Validity and reliability of the experience-sampling method. The Journal of Nervous and Mental Disease, 175(9), 526-536.
Deshpande, P. R., Rajan, S., Sudeepthi, B. L., & Nazir, C. A. (2011). Patient-reported outcomes: A new era in clinical research. Perspectives in Clinical Research, 2(4), 137.
Dittrich, Y.,1964-, & IS-EUD 2013 (2013 : Copenhagen,Denmark). (2013). End-user development : 4th
international symposium, IS-EUD 2013, copenhagen, denmark, june 10-13, 2013. proceedings. Berlin; New York: Springer. Retrieved from http://dx.doi.org/10.1007/978-3-642-38706-7
Fogg, B. J. (2003). Persuasive technology: Using computers to change what we think and do. San Francisco, CA: Morgan Kaufmann.
Folker, M., Rasmussen, J., Pedersen, K., Brocks, N., & D’Auchamp, A. (2014). Digital mental sundhed–Kortlægning og technology roadmap for digitale værktøjer til fremme af mental sundhed og selvhjælp ved psykisk sygdom.
Folker, M., Rasmussen, J., Pedersen, K., Brocks, N., & D’Auchamp, A. (2014). Digital mental sundhed–Kortlægning og technology roadmap for digitale værktøjer til fremme af mental sundhed og selvhjælp ved psykisk sygdom.
Freudenreich, O., & McEvoy, J. P. (2012). Optimizing outcome with antipsychotic treatment in first-episode schizophrenia: Balancing efficacy and side effects. Clinical Schizophrenia & Related Psychoses, 6(3), 115-121.

Research Protocol PROPS_ver2_110416
Page 21/27
Hansen, T. (2011). AT FANGE FUGLENS FLUGT. om dagbogsmetoder og nogle hukommelsesmæssige grunde til at anvende dem. Retrieved 5/14, 2014, from http://www.hum.aau.dk/~tia/TilAfhentning/Hansen%202007%20DbUs.pdf
Henderson, C., Flood, C., Leese, M., Thornicroft, G., Sutherby, K., & Szmukler, G. (2004). Effect of joint crisis plans on use of compulsory treatment in psychiatry: Single blind randomised controlled trial. BMJ (Clinical Research Ed.), 329(7458), 136.
Ho, B., Andreasen, N. C., Ziebell, S., Pierson, R., & Magnotta, V. (2011). Long-term antipsychotic treatment and brain volumes: A longitudinal study of first-episode schizophrenia. Archives of General Psychiatry, 68(2), 128-137.
Hunter, R., Cameron, R., & Norrie, J. (2015). Using patient-reported outcomes in schizophrenia: The scottish schizophrenia outcomes study. Psychiatric Services,
Iida, M., Shrout, P. E., Laurenceau, J. P., & Bolger, N. (2012). Chapter 15, using diary methods in psychological research,p277-306. In H. Cooper (Ed.), APA handbook of research methods in psychology, vol I, foundations, planning, measures and psychometrics (). Washington. D.C: American Psychological Association.
Kashdan, T. B., & Collins, R. L. (2010). Social anxiety and the experience of positive emotion and anger in everyday life: An ecological momentary assessment approach. Anxiety, Stress, & Coping, 23(3), 259-272.
Kimhy, D., Myin-Germeys, I., Palmier-Claus, J., & Swendsen, J. (2012). Mobile assessment guide for
research in schizophrenia and severe mental disorders. Schizophrenia Bulletin, 38(3), 386-395. doi:10.1093/schbul/sbr186 [doi]
Krägeloh, C. U., Czuba, K. J., Billington, D. R., Kersten, P., & Siegert, R. J. (2014). Using feedback from
patient-reported outcome measures in mental health services: A scoping study and typology. Psychiatric Services,
Kurhila, J., Miettinen, M., Niemivirta, M., Nokelainen, P., Silander, T., & Tirri, H. (2001). Bayesian modeling in an adaptive on-line questionnaire for education and educational research. Proceedings of the 10th International PEG2001 Conference, pp. 194-201.
McCabe, R., Saidi, M., & Priebe, S. (2007). Patient-reported outcomes in schizophrenia. The British Journal of Psychiatry, 191(50), s21-s28.
Meyer, K. B., & Clayton, K. A. (2009). Measurement and analysis of patient-reported outcomes. Clinical Epidemiology: Practice and Methods, , 155-169.
Palmier-Claus, J. E., Rogers, A., Ainsworth, J., Machin, M., Barrowclough, C., Laverty, L., et al. (2013). Integrating mobile-phone based assessment for psychosis into people’s everyday lives and clinical care: A qualitative study. BMC Psychiatry, 13(1), 1.
Pluye, P., Grad, R. M., Stephenson, R., & Dunikowski, L. G. (2005). A new impact assessment method to evaluate knowledge resources. Paper presented at the Amia,
Rainer, T. (1978). The new diary: How to use a journal for self-guidance and expanded creativity JP Tarcher Los Angeles.
Reininghaus, U., & Priebe, S. (2012). Measuring patient-reported outcomes in psychosis: Conceptual and methodological review. The British Journal of Psychiatry: The Journal of Mental Science, 201(4), 262-267. doi:10.1192/bjp.bp.111.107615 [doi]

Research Protocol PROPS_ver2_110416
Page 22/27
Sartorius, N. (2014). Patient-reported outcomes in psychiatry. Dialogues in Clinical Neuroscience, 16(2), 123-124.
Sartorius, N. (2014). Patient-reported outcomes in psychiatry. Dialogues in Clinical Neuroscience, 16(2), 123-124.
Shiffman, S., Stone, A. A., & Hufford, M. R. (2008). Ecological momentary assessment. Annu.Rev.Clin.Psychol., 4, 1-32.
Shiffman, S. (2009). Ecological momentary assessment (EMA) in studies of substance use. Psychological Assessment, 21(4), 486.
Staniszewska, S., Haywood, K. L., Brett, J., & Tutton, L. (2012). Patient and public involvement in patient-reported outcome measures. The Patient-Patient-Centered Outcomes Research, 5(2), 79-87.
Stone, D., Jarrett, C., Woodroffe, M., & Minocha, S. (2005). User interface design and evaluation Morgan Kaufmann.
Thibaut, F. (2016). Dialogues in clinical neuroscience. Dialogues Clin Neurosci, 2014 Jun; 16(2), 01/03/2016.
Trull, T. J., & Ebner-Priemer, U. W. (2009). Using experience sampling methods/ecological momentary assessment (ESM/EMA) in clinical assessment and clinical research: Introduction to the special section.
Tversky, A., & Kahneman, D. (1973). Availability: A heuristic for judging frequency and probability. Cognitive Psychology, 5(2), 207-232.
Wiklund, I. (2004). Assessment of patient‐reported outcomes in clinical trials: The example of health‐related quality of life. Fundamental & Clinical Pharmacology, 18(3), 351-363.
Aagaard, J., Skadhede, S. C., Andersen, M. B., Kølbæk, P., Hastrup, L. H., Foldager, L., et al. (2014). Opsøgende psykoseteams i Region Nordjylland. Aalborg: Aalborg Universitetsforlag.
Aagaard, M. (2016). Visualisation of patient data – for patients(poster). Comet 2016,
Aagaard, M., Aagaard, J., & Sarangi, S. (2016). EMA-apps can improve outcome for assertive community treatment patients. A pilot study. Comet 2016, Aalborg University, Denmaerk.
aan het Rot, M., Hogenelst, K., & Schoevers, R. A. (2012). Mood disorders in everyday life: A systematic
review of experience sampling and ecological momentary assessment studies. Clinical Psychology Review, 32(6), 510-523.

Research Protocol PROPS_ver2_110416
Page 23/27
Appendix A Description of Method No data is collected besides the one that already has been described. The test persons are not exposed to
any kinds of investigation besides participation in the PROPS experiment.
Appendix B Description of the data requested from the EPJ The EPJ data which will be requested for the PROPS project is essential information regarding their
diagnosis and treatment. Which includes the patients actual treatment.
The purpose to of usage of the EPJ data is to verify the inclusion criteria and to use the EPJ data as data for
the analysis of the intervention.
Appendix C Documentation of the registration to The Danish Data
Protection Agency The protocol will be submitted to The Danish Data Protection Agency for registration.
Research Protocol PROPS_ver2_110416
Page 24/27
Appendix D Budget

Research Protocol PROPS_ver2_110416
Page 25/27

Research Protocol PROPS_ver2_110416
Page 26/27
Appendix E Time schedule for the project

Research Protocol PROPS_ver2_110416
Page 27/27
Appendix F Test person information form The template “Komitésystemets standardskabelon, februar 2009” will be adapted to the PROPS project.
Appendix G Informed Consent Document The PROPS project’ Informed Consent” template is “S1” in “samtykkeerklringS1S122012.doc” adapted to
the PROPS project.