prophylaxis in hemophilia peyman eshghi prof. of pediatric hematology &oncology pediatric...
TRANSCRIPT
Prophylaxis in hemophilia
Peyman Eshghi
Prof. of Pediatric Hematology &Oncology
Pediatric Congenital Hematologic Disorders Research Center
Mofid Children Hospital
S.B.M.U
Shiraz-3-93

Main topics
• Definitions and types of prophylaxis• Cost-effectiveness ; Availablity & Affordability• Early prophylaxis & Toleration to inhibitor development• Protocols:
• When to start; Dosage & Intervals ; When to stop;
• Adverse events & barriers in the prophylaxis
• Prophylaxis is the treatment by intravenous injection of factor concentrate to prevent anticipated bleeding and should be the goal of therapy to preserve normal musculoskeletal function. (Level 2)
• In patients with repeated bleeding, particularly into target joints, short-term prophylaxis for 4– 8 weeks can be used to interrupt the bleeding cycle. This may be combined with intensive physiotherapy or synoviorthesis. (Level 3)
• Prophylactic replacement of clotting factor has been shown to be useful even when factor levels are not maintained above 1 IU/ dL at all times
WFH Guidelines for management of hemophilia, 2013
WFH Guidelines for management of hemophilia, 2013



Main topics
• Definitions and types of prophylaxis• Cost-effectiveness ; Availablity & Affordability• Early prophylaxis & Toleration to inhibitor development• Protocols:
• When to start; Dosage & Intervals ; When to stop;
• Adverse events & barriers in the prophylaxis

Individual PK curve - FVIII Levels over Time
0 6 12 18 24 30 36 42 48 Time (hours)
0
20
80
60
40
100
FV
III
Le
ve
l ( %
)
single infusion of 50 + 5 IU/kg bodyweight FVIII at time zero
Goal of prophylaxis:
keep FVIII levels >1% all the time
Administration and dosing schedules
• There are two prophylaxis protocols currently in use for which there are long-term data:
The Malmo¨ protocol: o 25–40 IU kg1 per dose administered three times a week for those with hemophilia
A, and twice a week for those with hemophilia B.The Utrecht protocol:o 15–30 IU kg1 per dose administered three times a week for those with hemophilia
A, and twice a week for those with hemophilia B.
• Prophylaxis is best given in the morning to cover periods of activity.• The protocol should be individualized as much as possible based on age,
venous access, bleeding phenotype, activity, and availability of clotting factor concentrates.
WFH Guidelines for management of hemophilia, 2013

Antonio Coppola et al., Blood transfuse 2008; 6 (supp2)

ON-DEMAND VS. PROPHYLACTIC THERAPY OUTCOME AT DIFFERENT DOSES
France Netherlands Sweden (on demand) (Intermediate- (High dose dose prophylaxis) prophylaxis)
Dose adjustment clinical preinfusion factor level
Numbers 116 21 19Age at study analysis 23 21 16-22Age at start of home-treatment 8.9 9.1 NAAge at start of prophylaxis NA 4.6 2.6Annual number of Jointbleeds 16.3 5.3 3 Pettersson score 18.8 6.0 6.5Orthopaedic joint score 7.7 2.0 2.4Clotting consumption 1634 1828 3713 (IU kg-¹ year-¹)
Haemophilia 2003; 9 (Suppl.1): 27-31

intermediate dose prophylaxis would be equally or even less costly after two decades.


Individualizing the regimen
• Pharmacokinetic considerations: 3-fold variation in clearnce and half life of factors
• Clinical outcome
• Other factors on coaguability of patients

Canadian tailored prophylaxisFeldman et al. JTH 2006;4:1228-36
• Starting at 1 to 2 years old• Tailored (escalating-dose) prophylaxis (EscDose):
Low-dose prophylaxis regimen (step 1): Children begin prophylaxis with 50 FVIII units/kg, once a week [40%*]
Medium-dose prophylaxis (step 2) : The dose is escalated to 30 FVIII units/kg, twice a week [44%*]
Equivalent of Standard prophylaxis (step 3) :This Dose is further escalated to 25 FVIII units/kg, on alternate days [16%*]
• The dose escalation criteria : developing Three bleeds into any one joint in a 3-month period OR Four clinically significant soft tissue or joint-bleeds while on prophylaxis.• Need to CVA : 40% vs 90% in JOS (joint outcome study with SP)

• 191 severe/moderate HA children with arthropathy from 15 centers were enrolled to undergo :
an 8-week on-demand treatment: ‘optimal-dose’ therapy: 20 IU kg1 for the first infusion and 10 IU kg1 once or twice a day until recovery
followed by 6 to 12-week low dose secondary prophylaxis:10 IU kg1 twice a week
• significantly decreased bleeding (78.8% haemarthrosis and 68.9% severe bleedings) and improved daily activities with no increase in factor consumption

• 12-week low dose secondary prophylaxis-study period (for haemophilia A, factor VIII concentrate 10 IU kg)1 twice weekly; for haemophilia B, factor IX concentrate 20 IU kg)1 weekly
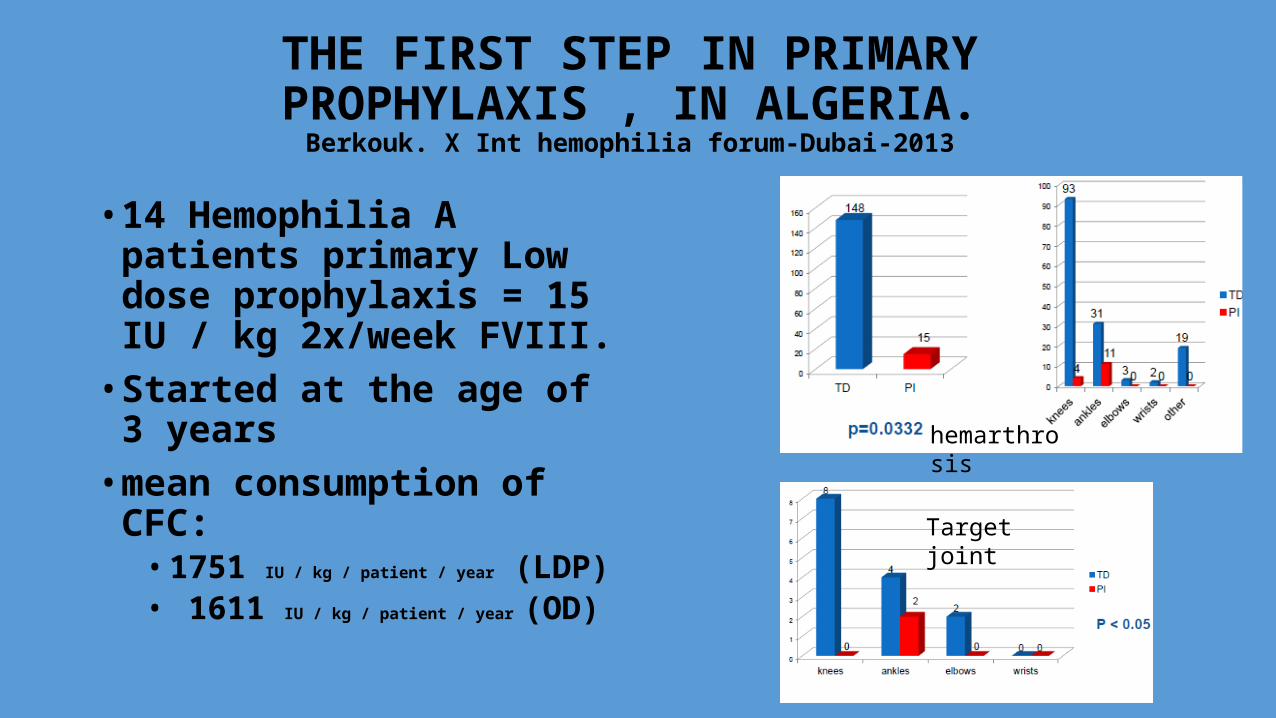
THE FIRST STEP IN PRIMARY PROPHYLAXIS , IN ALGERIA.
Berkouk. X Int hemophilia forum-Dubai-2013
• 14 Hemophilia A patients primary Low dose prophylaxis = 15 IU / kg 2x/week FVIII.
• Started at the age of 3 years• mean consumption of CFC:
• 1751 IU / kg / patient / year (LDP)• 1611 IU / kg / patient / year (OD)
Target joint
hemarthrosis

PAGE-431
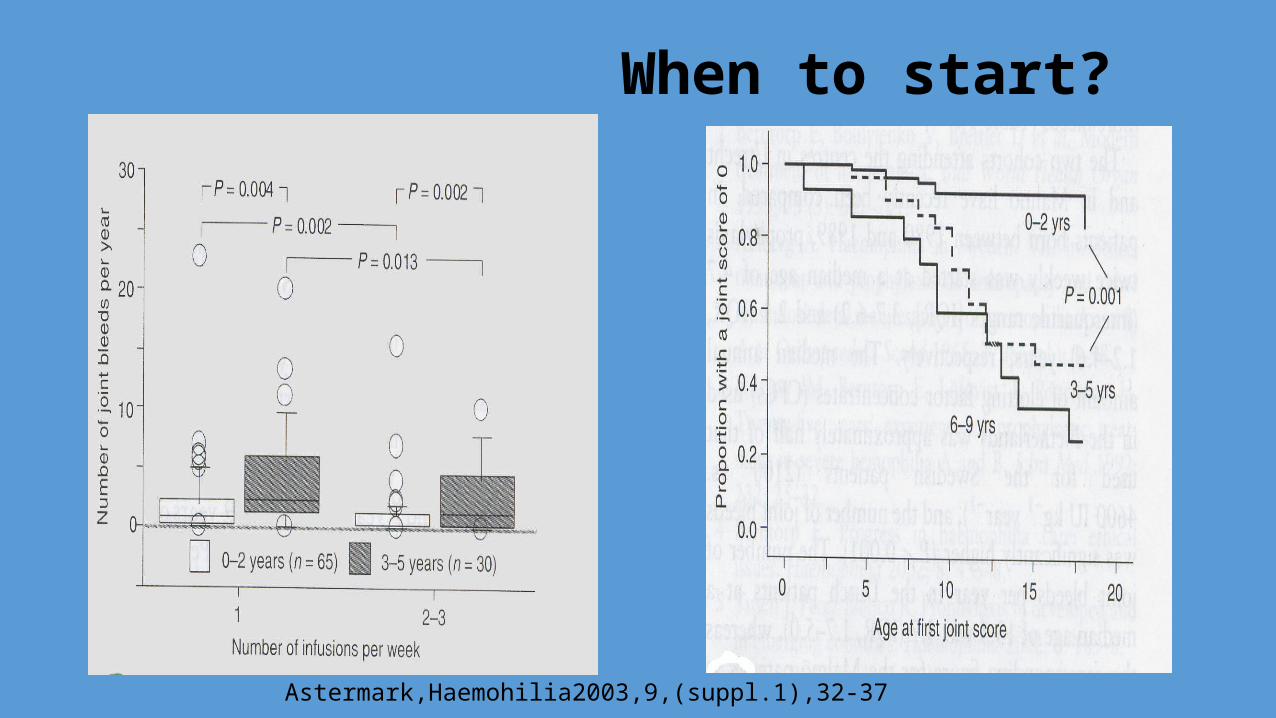
When to start?
Astermark,Haemohilia2003,9,(suppl.1),32-37

When should it be stopped, if at all?• some data suggest that a proportion of young adults can do
well off prophylaxis Fischer K, Van Der Bom JG, Prejs R et al.Discontinuation of prophylactic therapy ins evere haemophilia:
incidence and effects onoutcome. Haemophilia 2001; 7: 544–50.
1-Cost-benefit issue 2-scarcity of factor concentrates worldwide 3-mature joints may not vulnerable to bleed as growing joints Rooendaal et al.J of Rheumatol 200;27;1740-4
4-adults are less active and more cautious• In the adults with arthropathy : flexible prophylaxis with
lower doses and longer intervals vs on-demand therapy?

Main topics
• Definitions and types of prophylaxis• Cost-effectiveness ; Availablity & Affordability• Early prophylaxis & Toleration to inhibitor development• Protocols:
• When to start; Dosage & Intervals ; When to stop; etc
• Adverse events & barriers in the prophylaxis

Inhibitors develop at an early age
• Typically, inhibitors develop in early childhood within 10–20 exposure days to FVIII or FIX1
• •Rarely, treated adults can develop inhibitors (<3%)
Günter Auerswald ;Prof.-Hess-Kinderklinik ;Klinikum Bremen-Mitte
Factors influencing inhibitors
• Patient genetics :• Type of mutation • MHC class I/II genotype • Race • FHx • Polymorphic genes of cytokines
• Patient environment :• Intensive FVIII exposure, -immunologic challenge –immunisation; –infection; –surgery; –major
bleeding events -age of first infusion -immune system challenges;-peak treatment moment(<or>3-5days)
• Treatmen :• Type of factor • Therapeutic regimen• Continuous infusion
EMEA/CHMP/BPWP/123835/2006. Report on expert meeting on FVIII products and inhibitor development. Feb 28-Mar 2, 2006
AstermarkJ. Haemophilia 2006;12:52–60

Different influence of factors
Continuous infusion
CTLA4-318 TNFα A2 IL10 134

CANAL-study: treatment on demand
• Longer treatment / higher dose increase the risk of inhibitor development
Günter Auerswald ;Prof.-Hess-Kinderklinik ;Klinikum Bremen-Mitte

Danger model Antigen-Presenting Cells (APCs) are activated by endogenous danger signals from distressed or injured cells (e.g. exposure to pathogens, toxins, mechanical damage):E.g. if we give FVIII at the time that something else is causing damage (surgery, …), the immune system will associate that new molecule with the (unassociated) damage and respond to it.
Matzinger P. Expert,Rev.Clin.Immunol.2012; 8(4), 311-317; 3Mathinger P. Science 2001; 296,301
Antibody response
Tolerance
Günter Auerswald ;Prof.-Hess-Kinderklinik ;Klinikum Bremen-Mitte
Danger signals is everything that brings the immune system into an alarm position
Günter Auerswald ;Prof.-Hess-Kinderklinik ;Klinikum Bremen-Mitte

Inhibitor Development is caused by a Complex Interaction between Genetic and Environmental
Factors
While inherited genetic risk factors cannot be changed, it is thought that on a given genetic background, defined by the type of F8 gene mutations and polymorphisms of immune response genes, the environmental factors may allow to move a “high risk” patient to a “low risk” patient by choosing treatment regimens less prone to inhibitor development, such as early prophylaxis in the absence of hemorrhage
Oldenburg J. Genetic basis for inhibitor development. In: Rodriguez-Merchan et al (eds). Current and Future Issues in Hemophilia Care. 1st ed. Wiley-Blackwell; Oxford, 2011

NO BLEEDING DANGER SIGNAL
LESS INTENSIVE & LESS FREQUENT FACTOR EXPOSURE
AS POSSIBLE AS LATE EXPOSURE
WHAT SHOULD WE DO FOR PUP?

Treatment scheme for PUPs receiving the new prophylaxis
regimen Treatments

Comparison of standard prophylaxis with a new regimen

RODIN (Research Of Determinants of INhibitor
Development among pups with haemophilia) register)
Gouw SC, van der Bom JG, Ljung R et al. Factor VIII products and inhibitor development in severe hemophilia A. N Engl J Med 2013; 368: 231–9.
• The RODIN study supports the view that starting prophylaxis at an early age with a minimum number of on demand exposure days can reduce inhibitor risk
• Prophylaxis was started too late (after median of 15 on demand EDs (IQR 7-25) and at a median age of 16.7 months (IQR 12.4-24.4) .
• When started earlier after 0 EDs only 12% developed an inhibitor

Main topics
• Definitions and types of prophylaxis• Cost-effectiveness ; Availablity & Affordability• Early prophylaxis & Toleration to inhibitor development• Protocols:
• When to start; Dosage & Intervals ; When to stop; etc
• Adverse events & barriers in the prophylaxis

Adverse events in the prophylaxis:
• Transmission of pathogens• Inhibitor development : early treatment(especially < 6 months
age) with FVIII may be associated with an increased risk of Inhibitor development
• Allergic reactions : mainly with intermediate purity concentrate• Immunologic abnormality• Catheter related complications (infection, pneumothorax,
thrombosis…)• Sports-related injuries

Centeral venous line?R.LJUNG , Haemophilia(2003),9,suppl.,88-93Textbook of Haemophilia 2011,pp-128-129
• Most of the HTCs.(7/19 of centers in Europe) don`t use it for their patients at all• Main indications :
• HOME THERAPY• ITI• LONG TERM PROPHYLAXIS
• Infection is the most important complications(#0.2-1.6/1000days )especially in inhibitor patients.
• In the best of hands, a patient without inhibitors who has a Port - A - Cath and is on regular prophylaxis will have catheter - related infection at most
• Non-inhibitor:one every 5 – 10 years • Inhibitor: one infection per 1 – 2 years of use
• Catheter related thrombosis:• in most instances “ clinically silent, ”• related to the site of the catheter (jugular or subclavianvein), the type of concentrate used, or some
genetic thrombophilicfactor
• Some centers have successfully used arteriovenous fistulae in children as an alternative to a central venous line


Prophylaxis in Inhibitor Patients: Definitions
Primary (Early) prophylaxis* (long-term):Starts during ITI or after ITI failure
Aims: (1) to prevent target joint development (2) to avoid haemorrhages altogether
Secondary prophylaxis (intermittent or long-term) During ITI preventing breakthrough bleeds Perisurgical coverage Risk behavior, ICH risk, severe phenotype proregressive target joint Aims: (1) to stop progression of joint disease
(2) to prevent life threatening haemorrhages
Escuriola,-Ettingshausen personal communication Budapest symposium 2008

• We recommend to do synoverthesis ASAP if Target Joint developed:it should not be postponed after secondary prophylaxis in Inhibitor cases
• Intra-articular injections (e.g, steroids, hylan )may relieve persistent inflammation prior to a synovectomy

• a prospective, randomized, crossover study on 34 patients
• Dosage : 85 U/kg ± 15% TIW• Results:
• 62% reduction in all bleeding episodes (P<0.001),• 61% reduction in hemarthroses (P<0.001), • 72%reduction in target-joint bleeding

rFVIIa prophylaxis dosage:90 mcg/kg/day

Case discussion

case1
•6 month old sever HA•FH of HA with inhibitor•He has not have any joint bleeding yet
•He comes with a large hematoma on buttock
What do you do for him30U/kg FVIII daily until recovery
20-25 U/kg FVIII once and clinically follow him
nothing

case1
•He improved How do you mange him then?
A. 25 u/kg once weekly
B. 10-15 u/kg 1-2 times weekly (LD P.)
C. 20 u/kg 2-3 times per week (intermediate dose P.)
D. 30-40 u/kg 3 times per week (high dose P.)
E. 50 u/kg once weekly (escalated dose prophylaxis)
F. Wait till first Joint bleed then :A/B/C/D/E

case1
•He was on regimen A for 2 months
•Then after he has had one episode of hemarthrosis in his right knee and left ankle and left elbow
How do you mange him then?A. 50 u/kg once weekly (2nd
escalated dose prophylaxis)
B. 25 u/kg 2 times weekly
C. 25 u/kg 3 times weekly
D. 30-40 u/kg 3 times per week (2nd high dose P.)
E. 10-15 u/kg 2 times weekly (2nd LD P.)

case2
• 3 years old sever HA• He has already received
just on demand regimen• He had 3 times
spontaneous Joint bleeding in R ankle in last 3 months ,which improved completely and now he has no sign and symptom
How do you mange him then?A. 25 u/kg 3 times weekly for 8
weeksB. Synoverthesis C. Continuous secondary
prophylaxis with :A. 50 u/kg once weekly (escalated
dose prophylaxis)B. Intermediate dose P.(15-30u/kg
2-3 times per week)C. LD P. (10-15u/kg2 times per
week)
D. A & B

در پیشگیری از تر واجب....................... هموفیلی

است ایران زیست محیط نجات
باشید موفق
