prophylaxis and treatment of ifi in hematological patients l j12.pdf · prophylaxis and treatment...
TRANSCRIPT
Prophylaxis and treatment of IFI in Hematological patients
Livio Pagano
Istituto di Ematologia
Università Cattolica del Sacro Cuore
Roma

Robenshtok et al. J Clin Oncol 2007

Antifungal Activity Vori + Posa > 75% sensible, 50%, < 5%; mixed colours
AmB Fluco Itra Vori Caspo Posa
C. albicans
C. parapsilosis
C. tropicalis
C. glabrata
C. krusei
A. fumigatus
A. flavus
A. terreus
Zygomycetes
Fusarium spp.
Cortesy of B. de Pauw

Voriconazole Prophylaxis in allo-HSCTs
N patients IFD P-value
Wingard et al,
Blood 2010
(allo-HSCTs)
Voriconazole 305 16 aspergillosis*
3 candidemia
3 zygomycosis
0.11
*(0.05) Fluconazole 295 7 aspergillosis*
3 candidemia
2 zygomicosis
Marks et al,
Br J Haemat 2011
(allo-HSCTs)
Voriconazole 234 5 aspergillosis
0 candidemia
0 zygomycosis
Composite
endpoint:
Vori > Itra Itraconazole 255 1 aspergillosis
2 candidemia
0 zygomicosis

Standard azoles (n = 298)
Posaconazole (n = 304)
0
5
10
15
20
25
Nu
mb
er
of
IFIs
30
35
2
25
7
20
p < .001
Aspergillosis All IFIs
p < .001
Treatment phase*
4
33
14
26
p = .003
All IFIs Aspergillosis
p < .001
100-day period after randomization†
2%
1%
5%
1%
8%
7%
11%
9%
Cornely et al. N Engl J Med. 2007;356:348-359
*On-treatment period. †Fixed-time period.
Posaconazole prophylaxis in AML
IFDs incidence
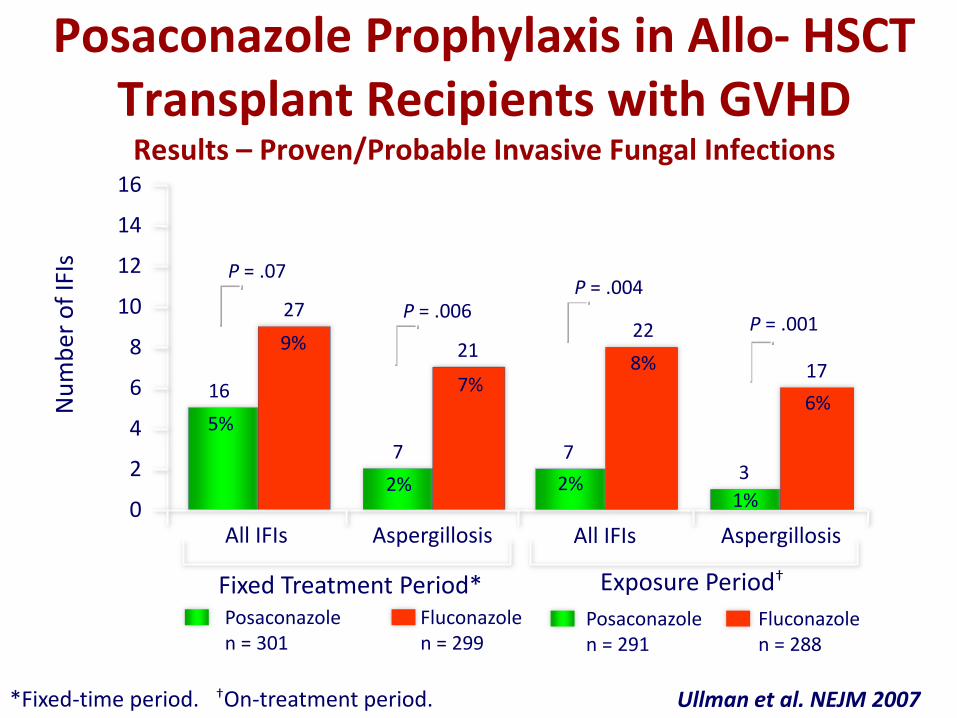
Posaconazole Prophylaxis in Allo- HSCT Transplant Recipients with GVHD
Results – Proven/Probable Invasive Fungal Infections
Fixed Treatment Period* Posaconazole
n = 291 Fluconazole n = 288
Posaconazole n = 301
Fluconazole n = 299
0
2
4
6
8
10
12
14
16
Nu
mb
er o
f IF
Is
P = .004
P = .001
Exposure Period†
7 3
22
17
All IFIs Aspergillosis
P = .07
P = .006
16
7
27
21
All IFIs Aspergillosis
5%
2% 2% 1%
9%
7% 8%
6%
*Fixed-time period. †On-treatment period. Ullman et al. NEJM 2007

FLUCO
VORICO
ITRA
POSA
CASPO
L-AmB
CT
ECIL-3
allo HSCT
C-I
A-I
-
A-I
C-I
B-I
A-I
A-I
-
-
C-I
C-I
neutropeni
German
allo HSCT
C-I
A-I
C-II
C-II
C-I
C-I
A-I
A-I
C-I
-
C-II
-
IDSA - - B-I A-I - -
British - - A-I A-I - -
AML-MDS
NCCN
allo HSCT
-
-
2B
2B
-
-
1
1
-
2B
2B
2B
International Guidelines on antifungal prophylaxis in AML and allo-HSCT

Years Type N° pts IFDs incidence%
RCT
Cornelly et al, NEJM 2007 2002-05 RCT 304 7 2%
Real life series
Michallet et al, Med Mycol 2011 2007-08 Pros 55 2 3.6%
Candoni et al, EHA 2011 2009-10 Retro 55 2 4%
Lerolle et al, ICAAC 2011 2007-10 Retro 209 8 3.8%
Hahn et al, Mycoses 2011 2007-08 Retro 21 1 5%
Egerer et al, Mycoses 2011 2007-09 Retro 76 1 1.3%
Vehreschild et al, JAC 2010 2006-08 Retro 77 3 3.9%
Busca et al, 5th TIMM 2011 2009-10 Retro 61 0 0
Ananda-Rajah,Haematol ‘11 2006-10 Retro 68 0 0
ALL STUDIES 622 17 2.7%
Posaconazole in AML
Proven/probable IFDs: 2.7% (0-5%)
Pagano et al. Haematologica 2012

703 patients recorded in SEIFEM 2010 study
No systemic prophylaxis or less than 7 days of prophylaxis 68 patients
260 patients with Posaconazole prophylaxis
93 patients with Itraconazole prophylaxis
508 patients with Systemic Prophylaxis
Not conventional AML therapy (Support or contenitive) 127 patients
353 patients with Posaconazole or Itraconazole Prophylaxis
7 patients others Prophylaxis (5 Voriconazole, 1 Caspofungin and 1 Ambisone)
148 patients with Fluconazole prophylaxis

Itraconazole
N°93 Posaconazole
N°260 p-value
Age (median[IQR]) 60 [49-67] 56 [44-65] 0.08
% of men 52.2% 45% 0.23
Duration of prophylaxis 21 [15-26] 21 [16-28] 0.70
Deep Neutropenia (>7days)
87 (93.5%) 240 (92.3%) 0.69
Median duration of neutropenia ( days [IQR])
22 [16-27.5] 23 [18-29] 0.25
CVC 75 (80.6%) 200 (76.9%) 0.45
Performance Status 0-1 2-4
72 (77.4%) 21 (22.6%)
204 (78.5%) 56 (21.5%)
0.83
Antracycline based chemotherapy (Y/N)
81/93 (87.1%) 242/260 (93.1%) 0.08
Comparison between the two groups
Main clinical characteristics and risk factors
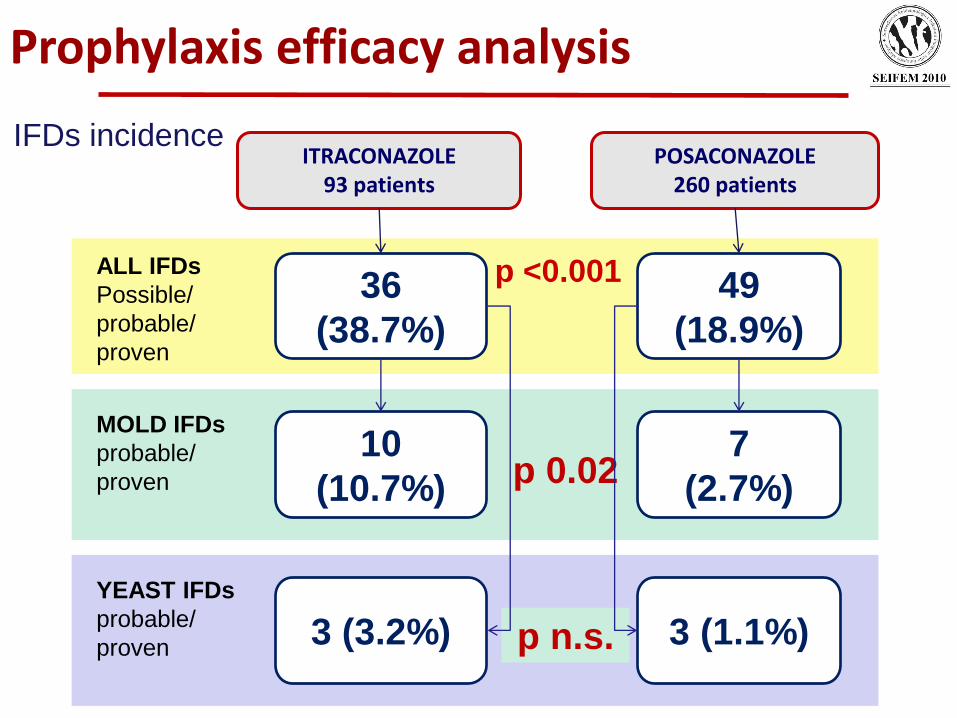
POSACONAZOLE 260 patients
ITRACONAZOLE 93 patients
36
(38.7%)
49
(18.9%)
ALL IFDs
Possible/
probable/
proven
p <0.001
3 (3.2%) 3 (1.1%)
YEAST IFDs
probable/
proven p n.s.
10
(10.7%)
7
(2.7%)
MOLD IFDs
probable/
proven p 0.02
Prophylaxis efficacy analysis
IFDs incidence

Courtesy of P. Donnelly
GM

Defining posaconazole efficacy: Secondary endpoints 1
Does POSA reduce incidence of possible IFDs?
0% 20% 40% 60% 80% 100%
POSA
ITRA
NO IFDs
possible
prov/prob
24%
15%
p 0.03
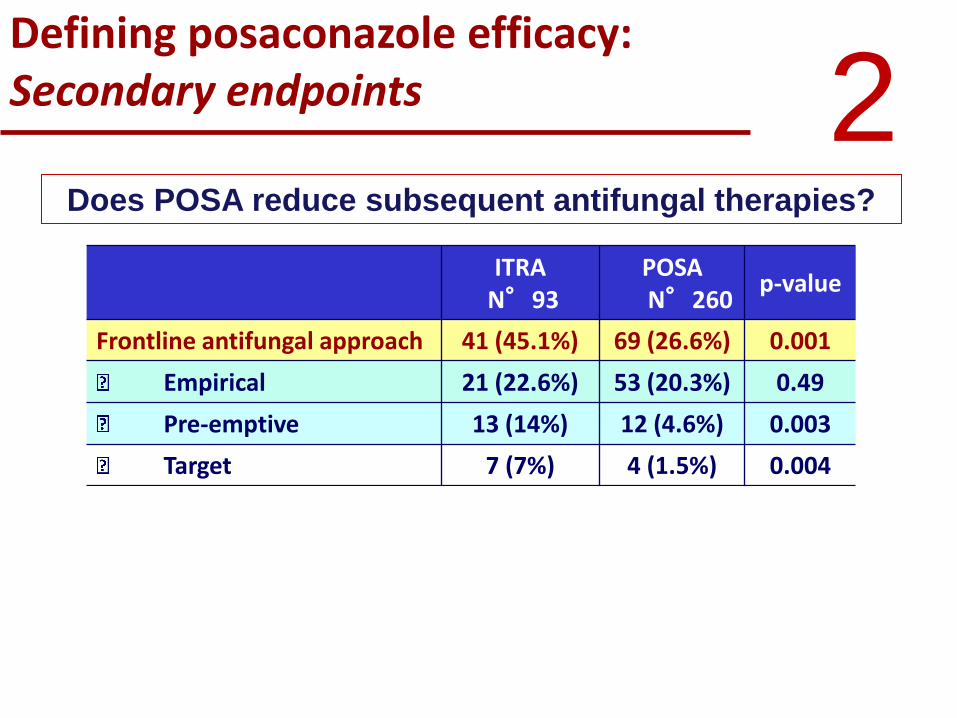
Defining posaconazole efficacy: Secondary endpoints
ITRA
N°93 POSA N°260
p-value
Frontline antifungal approach 41 (45.1%) 69 (26.6%) 0.001
Empirical 21 (22.6%) 53 (20.3%) 0.49
Pre-emptive 13 (14%) 12 (4.6%) 0.003
Target 7 (7%) 4 (1.5%) 0.004
Mean duration of frontline AF approach 15 [10-22] 12 [8-15] 0.05
Empirical 12 [8.5-19] 11 [7-14] 0.27
Pre-emptive 15 [9.5-24] 14 [10-26] 0.62
Target 18 [5-20] 12.5 [10-18] 0.46
2 Does POSA reduce subsequent antifungal therapies?

Defining posaconazole efficacy: Secondary endpoints 3
Does POSA reduce IFD-attributable mortality?
Itraconazole Posaconazole p-value
AM - Attributable mortality (%) 4/36 (11.1%) 2/49 (4.1%) 0.21
Molds AM 4/33 (12.1%) 0/46 (0%) 0.03
Yeasts AM 0/3 (0%) 2/3 (66.7%) 0.2
0%
20%
40%
60%
80%
100%
ITRA POSA
deaths
all cases
11% 4%

4 0.0
00.2
00.4
0
Pro
bab
ility
of d
ea
th
0 20 40 60 80 100analysis time
Itraconazole Posaconazole
Kaplan-Meier failure estimates
Pr>chi2 = 0.0023
Does POSA reduce overall mortality?
Defining posaconazole efficacy: Secondary endpoints
0 20 40 60 80 100
0.30
0.20
0.10
0.00
Posaconazole Fluconazole or Itraconazole
0.25
0.15
0.05
p = .04*
Cornelly et al NEJM 2006
In RCT posaconazole emerged as a valid antifungal prophylaxis in high risk patients
Our “real life” experience confirmed posaconazole to be an efficacious prophylaxis producing -reduction of proven/probable IFD -reduction of antifungal therapies -reduction of overall mortality
The role of diagnostic tools (i.e. galactomannan, PCR) after posaconazole remains to be defined, as well as the optimal management of febrile neutropenia:
EMPIRICAL or PRE-EMPTIVE ?
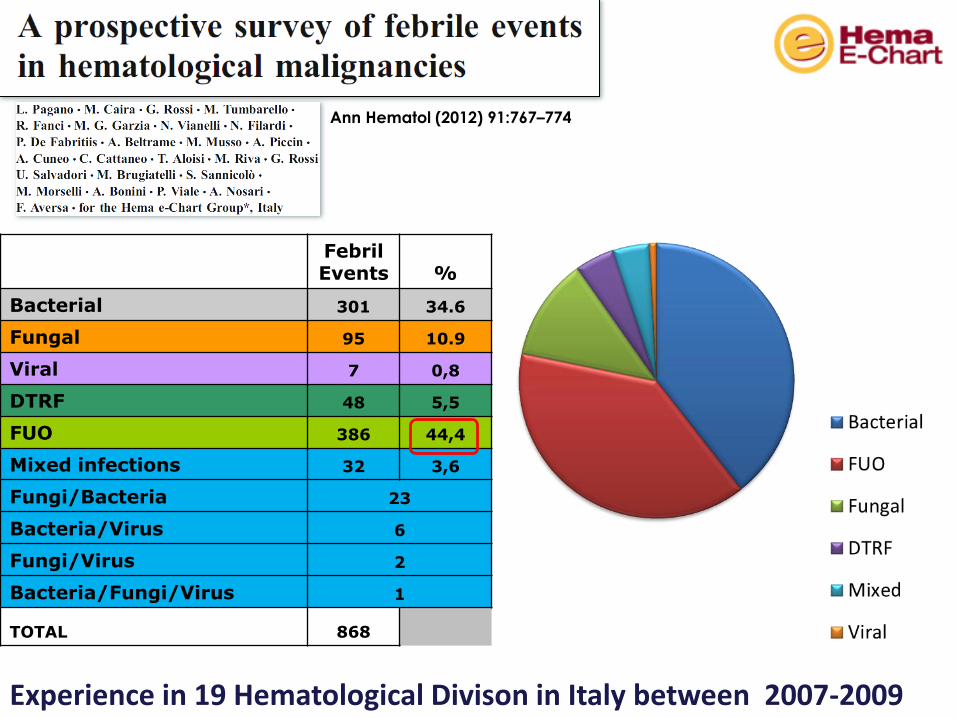
Febril Events %
Bacterial 301 34.6
Fungal 95 10.9
Viral 7 0,8
DTRF 48 5,5
FUO 386 44,4
Mixed infections 32 3,6
Fungi/Bacteria 23
Bacteria/Virus 6
Fungi/Virus 2
Bacteria/Fungi/Virus 1
TOTAL 868
Experience in 19 Hematological Divison in Italy between 2007-2009
Ann Hematol (2012) 91:767–774

Antifungal agent Daily dose Level of
Recommendation
Evidence for
Efficacy Safety
Liposomal AmB** 3 mg/kg A I I
Caspofungin** 50 mg A I I
ABLC 5 mg/kg B I I
ABCD 4 mg/kg B I I
Voriconazole 2x 3 mg/kg iv B I I
Itraconazole* 200 mg iv B I I
Micafungin 100 mg B II II
AmB deoxycholate** 0.5-1 mg/kg B/D I I
Fluconazole 400 mg iv C I I
ECIL 3: Antifungal drugs for Empirical Therapy
* FDA and **EMA-approved drugs for empirical therapy

Response rates (%) in studies on empirical antifungal therapy
d-AmB L-AMB Fluco Itra Vori Caspo ABCL
Viscoli et al 66 - 75 - - - -
Prentice et al 46 64 - - - - -
Malik et al 46 - 56 - - - -
White et al 43 - - - - - 50
Walsh et al 49 50 - - - - -
Winston et al 67 - 68 - - - -
Wingard et al - 42 - - - - 33
Boogaerts et al 38 - - 47 - - -
Walsh et al - 30 - - 24 - -
Walsh et al - 33 - - - 34 -
?

Period
o a r
isch
io
SURVEY
SYMPTOMATIC APPROACH
GM GM GM GM GM GM GM GM GM GM GM
TC TC TC
GMpos
GM GM GM
TC GMpos
Febbre
4gg
Courtesy of C. Girmenia
Maertens et al. Clin Infect Dis 2005
Girmenia et al. JCO 2009
PRE-EMPTIVE
DIAGNOSIC-DRIVEN
As a consequence it has been suggested to substitute the empirical approach with pre-emptive antifungal approach
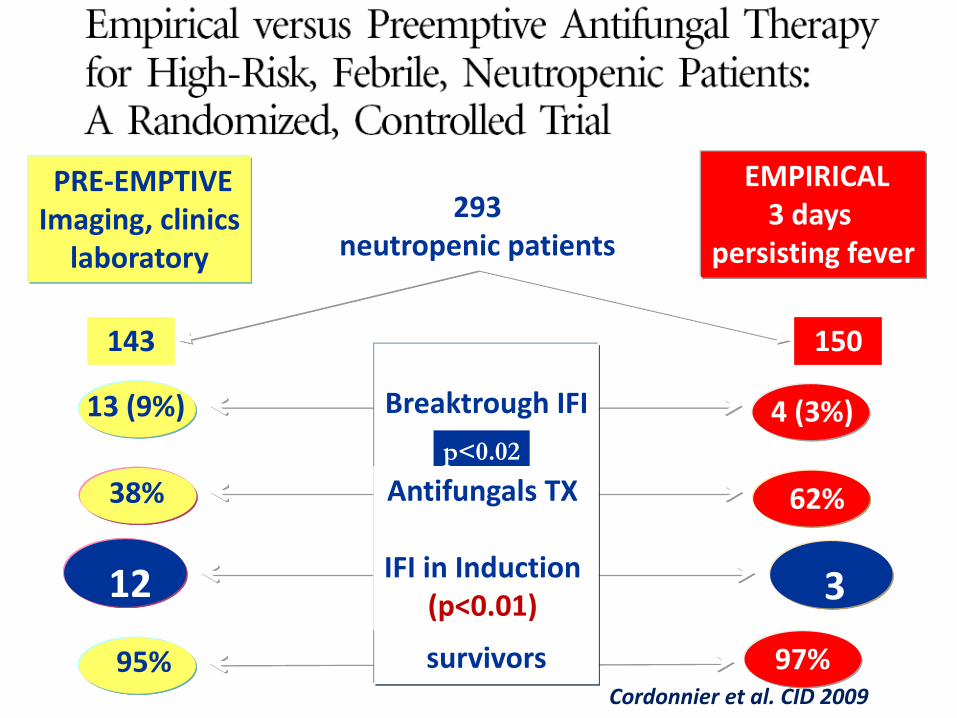
3 12
62% 38%
13 (9%) 4 (3%)
95% 97%
150 143
Breaktrough IFI
survivors
PRE-EMPTIVE Imaging, clinics
laboratory
EMPIRICAL 3 days
persisting fever
293 neutropenic patients
p<0.02
Antifungals TX
IFI in Induction (p<0.01)
Cordonnier et al. CID 2009
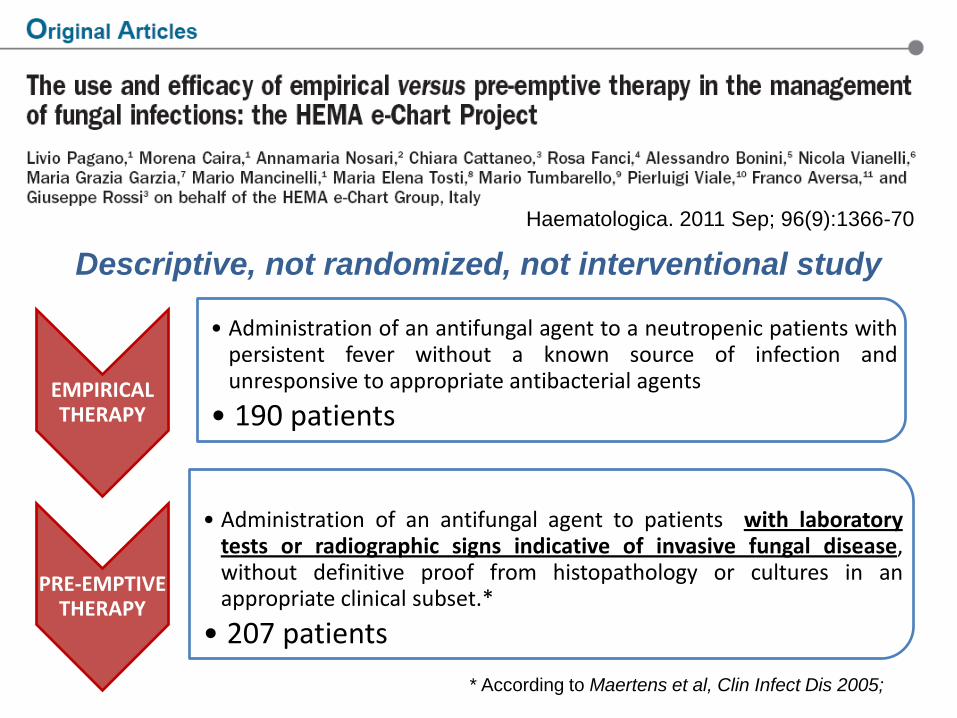
Descriptive, not randomized, not interventional study
Haematologica. 2011 Sep; 96(9):1366-70
EMPIRICAL THERAPY
• Administration of an antifungal agent to a neutropenic patients with persistent fever without a known source of infection and unresponsive to appropriate antibacterial agents
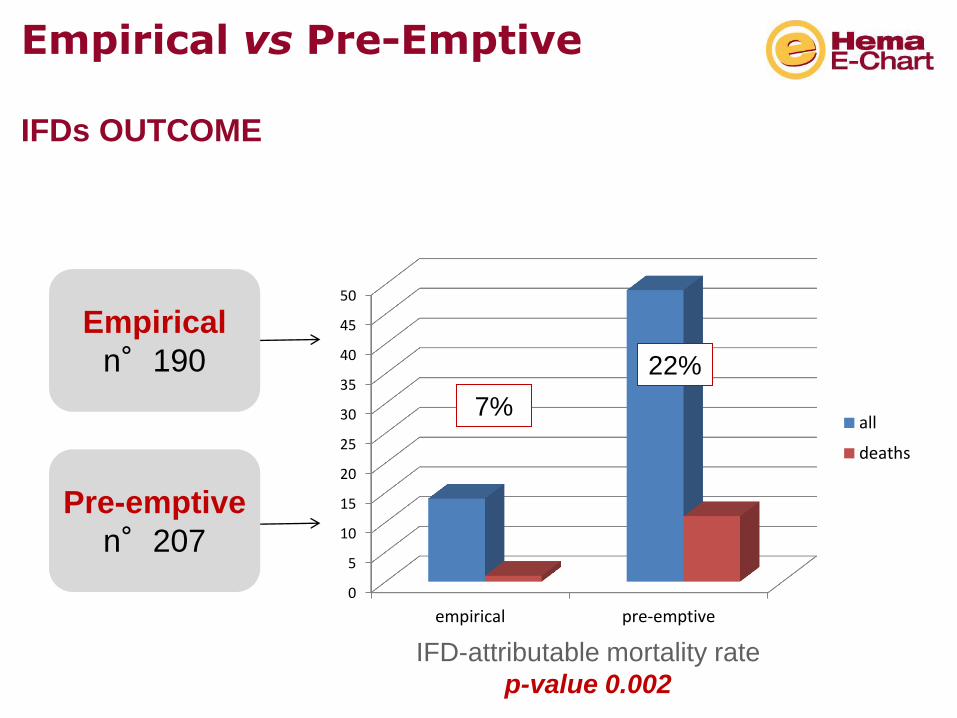
• 190 patients
PRE-EMPTIVE THERAPY
• Administration of an antifungal agent to patients with laboratory tests or radiographic signs indicative of invasive fungal disease, without definitive proof from histopathology or cultures in an appropriate clinical subset.*
• 207 patients
* According to Maertens et al, Clin Infect Dis 2005;

Empirical
n°190
Pre-emptive
n°207
Proven/probable
IFDs
14 (7.4%)
49 (23.7%)
p-value 0.001
Empirical vs Pre-Emptive IFDs incidence
Type of IFDs
Moulds 8
(57%)
Yeasts 6
(43%)
Moulds 40
(82%)
Yeasts 9
(18%)
57%
43%
82%
18%
Empirical
n°190
Pre-emptive
n°207
IFD-attributable mortality rate
p-value 0.002
Empirical vs Pre-Emptive IFDs OUTCOME
0
5
10
15
20
25
30
35
40
45
50
empirical pre-emptive
all
deaths
7%
22%

VARIABLES Dead (n°45) Survivors (n°352) P-value
UNIVARIATE ANALYSIS
Male sex 29 (64.4) 200 (56.8) 0.32
Age (year [mean SD]) 62 ±10 54 ±16 <0.001
Underlying HMs - AML - NHL - ALL - Other
34 (75.5) 6 (13.3) 4 (8.9) 1 (2.2)
287 (81.5)
24 (6.8) 21 (5.9) 20 (5.7)
0.33 0.13 0.5
Clinical factors - Central venous catheter - Neutropenia - Antifungal prophylaxis - Steroid use
21 (46.7) 40 (88.9) 20 (44.4) 6 (13.3)
180 (51.1) 326 (92.6) 194 (55.1)
27 (7.6)
0.57 0.38 0.17 0.19
Etiology - Yeasts - Molds
4 (8.9)
8 (17.8)
15 (4.3)
36 (10.2)
0.17 0.13
Empirical treatment 12 (26.7) 178 (50.6) 0.002
MULTIVARIATE ANALYSIS
Age (year [mean SD]) 0.006
Empirical antifungal treatment 0.01

Indication for empirical/preemptive antifungal therapy from International
Guidelines
BSH 2008 ECIL 2009 IDSA 2010
Empirical A Ib B II A I (for high risk)
Pre-emptive Not Reported
No Grading B II

What is better ???
Fever-driven ? Diagnostic-driven?
Taking in account: 1.Patients to treat 2.Toxicity 3.Efficacy of the approach 4.Outcome 5.Costs 6.Prophylaxis

AutoHSCT Kidney Tx Solid tumor Immune Disorder
ALL Heart transplantation CLL COPD AIDS NHL
AlloHSCT (GVHD) MDS (induction) AML (induction) Lung transplantation AlloHSCT (no GVHD) AML (consolidation) Liver transplantation
LOW RISK
INTERMEDIATE RISK
HIGH RISK
Underlying condition
Pagano et al, J Antimicrob Chemother, 2011

Toxicity of antifungal agents used in empirical and pre-emptive approach
D-AmB L-AmB Itra Caspo Vorico
Liver 20% 6-17% 3% 8% 8%
Renal 14% 5-11% 5% 2% 11%
Infusion-related 70% 30-50% 20% 35% 30%
Discontinuation 20% 7-15% 20% 5% 10%
OVERALL
TOXICITY
High Medium Low Very
Low
Low
Bogaert et al, Ann Int Med 2001; Walsh et al, N Eng J Med 1999, 2002, 2004

CT-scan Dose Efficacy (mSv)
Equal to standard thorax X-ray
Skull Cervical spine Dorsal spine Thorax Abdomen Lumbar spine
1.7 1.7 7.7 7.8 5.1 8.8
85 85
385 390 255 440
Warning: toxicity of exams ??!!??
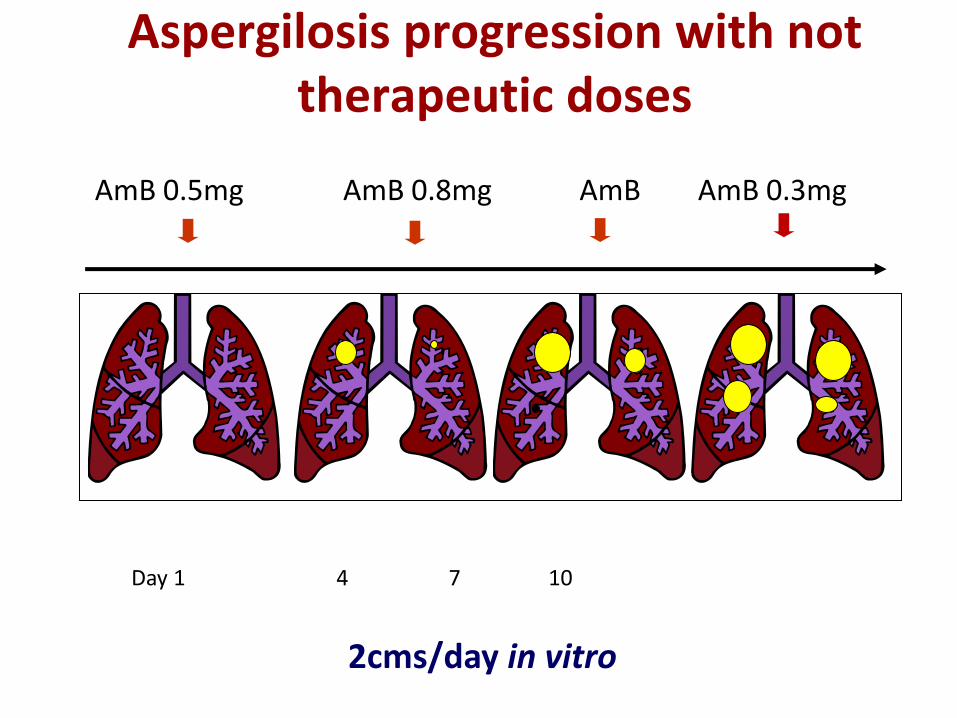
AmB 0.5mg AmB 0.8mg AmB AmB 0.3mg
Day 1 4 7 10
2cms/day in vitro
Aspergilosis progression with not therapeutic doses
0%
5%
10%
15%
20%
25%
30%
35%
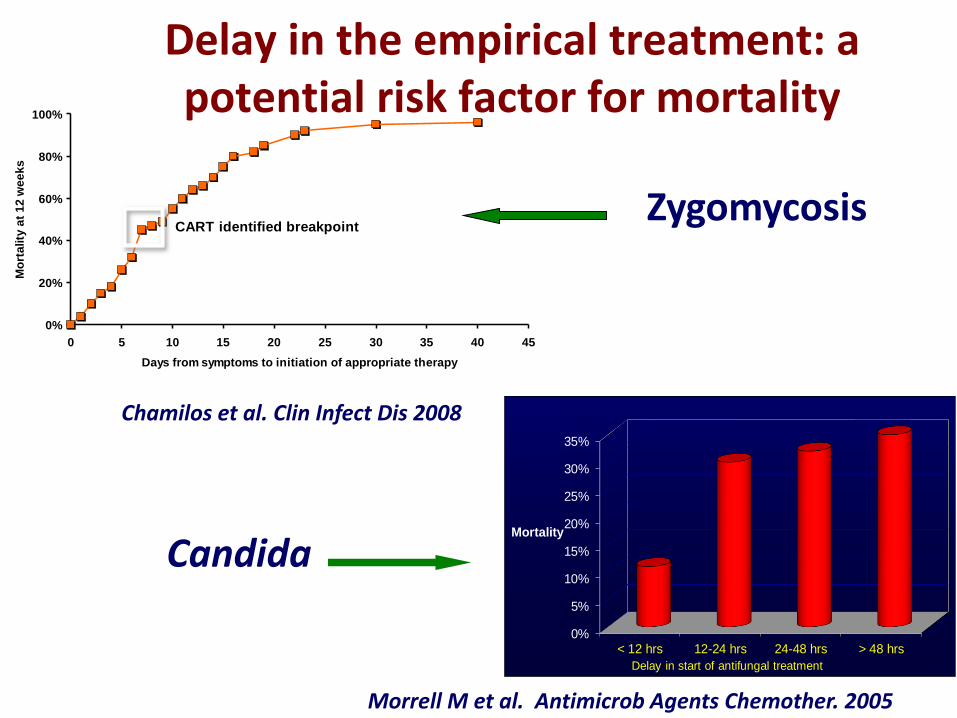
< 12 hrs 12-24 hrs 24-48 hrs > 48 hrs
Mortality
Delay in start of antifungal treatment
Morrell M et al. Antimicrob Agents Chemother. 2005
Delay in the empirical treatment: a potential risk factor for mortality
0%
20%
40%
60%
80%
100%
0 5 10 15 20 25 30 35 40 45
Days from symptoms to initiation of appropriate therapy
Mo
rta
lity
at
12
we
ek
s
CART identified breakpoint
Chamilos et al. Clin Infect Dis 2008
Zygomycosis
Candida

Incidence: 5.8% vs 12.6% (p 0.002)
AMR: 24% vs 13% (p: ns)
Caspofungin
Voriconazole
L-AmB
SEIFEM-C Report: Outcome in AML
CID 2007, 44: 1521-2
Only EMPIRIC
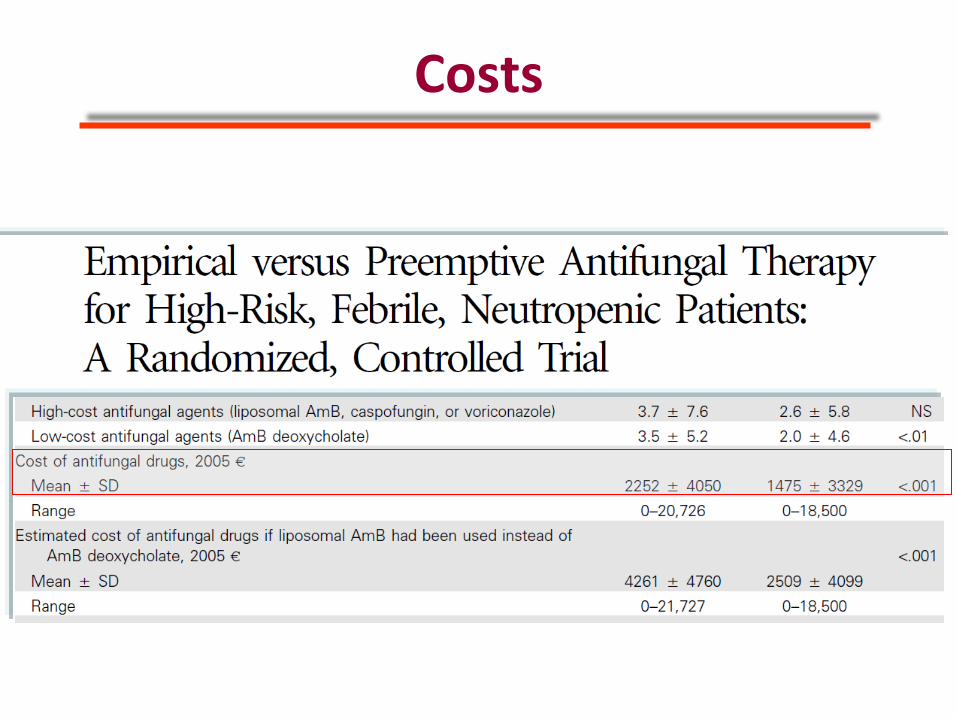
Costs

Courtesy of B de Pauw

n Death
(%)
IFI
(% )
AMR
Posaconazole prophylaxis 573
Antifungal therapy 131 (23%)
Empirical 104 (79%)
Voriconazole 3 1 (33%) 2(66) 0
Caspofungin 30 13 (43%) 17(56) 2
L-AmB 64 21 (33%) 37(58) 4
Pre-emptive 20 (15%)
Voriconazole 6 1 (17%) 0 0
Caspofungin 2 1 (50%) 0 0
L-AmB 10 2 (20%) 0 0
Target 12 (6%)
SEIFEM-2010 study Pre-hospital risk factors for IFD in newly diagnosed
Acute Myeloid Leukemia
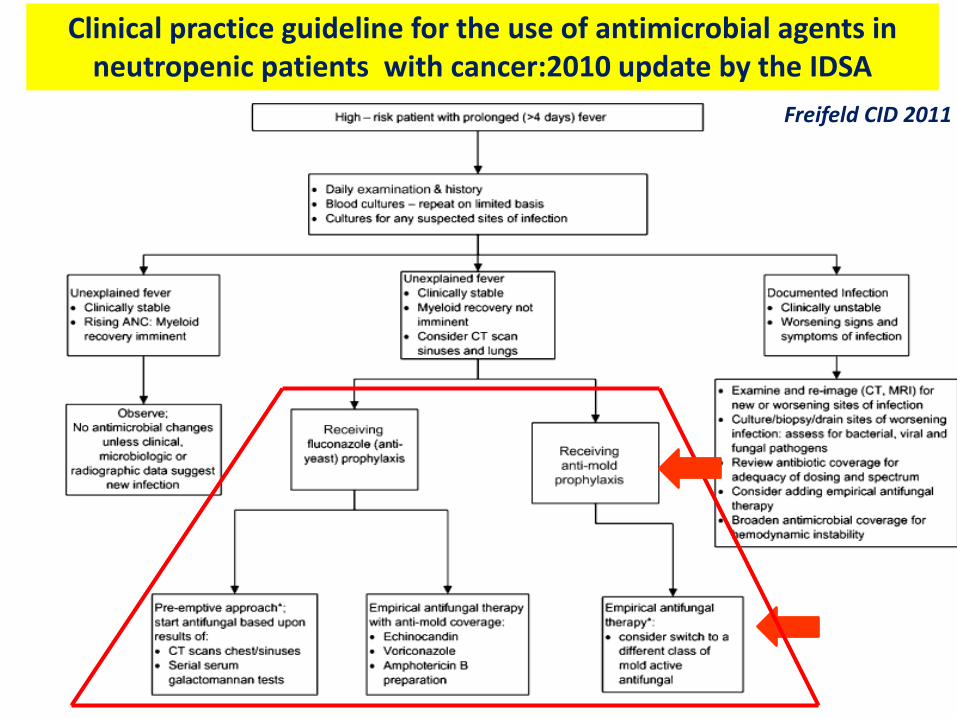
Clinical practice guideline for the use of antimicrobial agents in neutropenic patients with cancer:2010 update by the IDSA
Freifeld CID 2011

In my opinion Empirical antifungal therapy now-a-days plays an
important role in HM patients
It is mainly indicated in particular subset of patients at very high risk
Equally indicated Caspo and L-AmB
On the contrary, only a pre-emptive antifungal diagnostic strategy was advised for those at standard risk
Start an empirical treatment do not justify not performing a timely diagnostic work-up
As suggested by various Opinion Leaders, empirical therapy is a very useful tool to BUY TIME