promise & limitations of surgical checklists: how can we effectively use them to improve the...
TRANSCRIPT
Promise & limitations of surgical checklists:How can we effectively use them to improve
the quality of surgical care?
Shawn J. Rangel, MD, MSCE & J. William Sparks, MD
Northeast Regional Patient Safety & Quality Improvement Conference
February 5th, 2011



WHO checklist
Reality check- IHI map

Even the stars are using it!

So, will the WHO checklist save mankind?

Reality check: one size does not fit all…

• Review evidence supporting surgical safety checklists
• Attitudes toward the safety checklist at (CHB survey)
• Strategies for improving checklist utilization & relevance
• Next steps: IT, custom checklists & beyond…
Outline of today’s discussion

WHO study
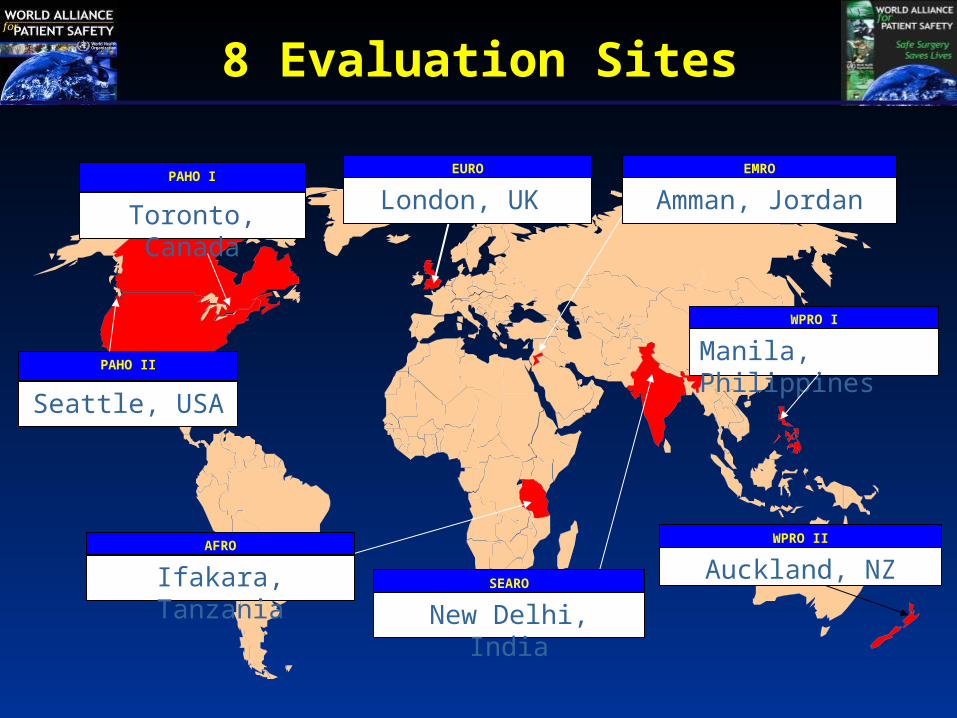
London, UK EURO EMRO
WPRO I
SEARO
AFRO
PAHO I
Amman, JordanToronto, Canada
New Delhi, India
Manila, Philippines
Ifakara, Tanzania
WPRO II
Auckland, NZ
PAHO II
Seattle, USA
8 Evaluation Sites
Methods
• 1 to 4 operating rooms targeted at each site
• 18-item checklist implemented (sign-in, time-out, sign-off)
• Pre-post intervention study design (general surgery cases)
• Primary outcome measure: aggregate 30-day major complication rate (NSQIP* defined)
*National Surgical Quality Improvement Project

Results: impact on morbidity & mortality(3 month comparison periods)
Baseline Checklist P value
Cases 3,733 3,955 -
Death 1.5% 0.8% 0.003
Any complication 11.0% 7.0% <0.001
Surgical site infection 6.2% 3.4% <0.001
Unplanned Reoperation 2.4% 1.8% 0.047

Limitations of the study
• Unknown influence of the Hawthorne effect
• Unable to prove causality (non-randomized design)
• Effect size may be exaggerated (developing nations)
• Only one of the eight centers was in the U.S.
• Pediatric patients not included in analysis
SURPASS

Intervention
The comprehensive “SURgical PAtient Safety System”:
Methods
•SURPASS implemented at 6 tertiary-care hospitals
•Pre-post intervention study design (3 month periods)
•12 adverse event categories audited
•Outcomes compared with five “control” hospitals
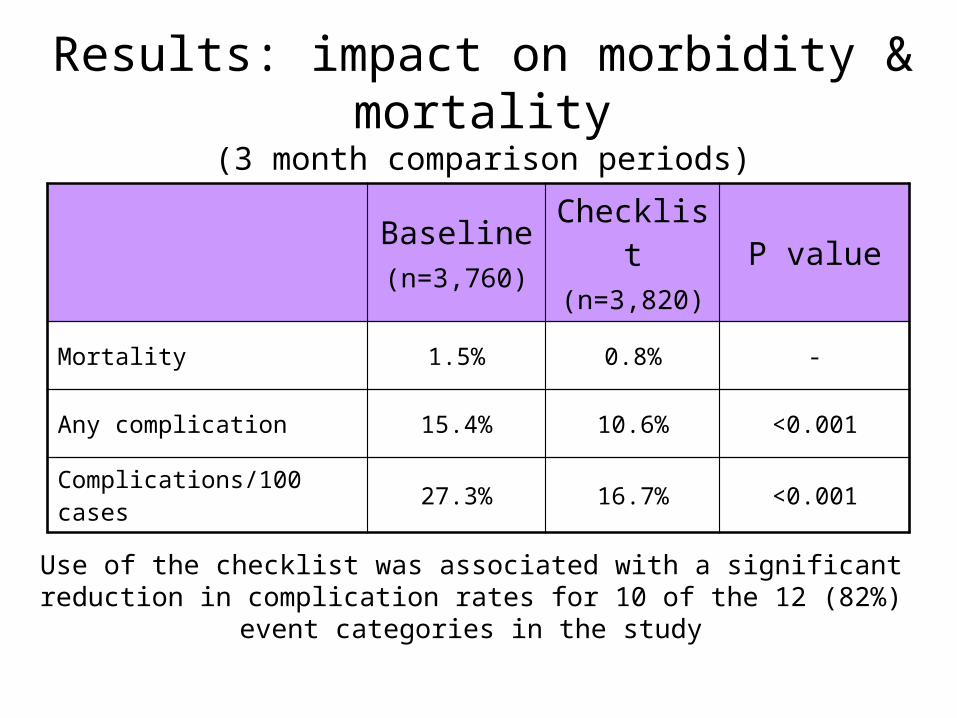
Results: impact on morbidity & mortality(3 month comparison periods)
Baseline(n=3,760)
Checklist(n=3,820)
P value
Mortality 1.5% 0.8% -
Any complication 15.4% 10.6% <0.001
Complications/100 cases 27.3% 16.7% <0.001
Use of the checklist was associated with a significant reduction in complication rates for 10 of the 12 (82%) event categories in the study

But, kids are not small adults!
Pediatric Safe Surgery Collaborative
• Children’s Hospital Boston Shawn J. Rangel (Study PI) Beth K. Norton (Co-study PI) Jessica Baxter
• Texas children’s Hospital Thomas Luerssen (site PI) Carrie Smith-Bruce
• Riley Children’s Hospital Fred Rescorla (Co-site PI) Charles Leys (Co-site PI) Margo Regas
• Denver Children’s Hospital Tammy Woolley (Site PI) Jenae Nieman
• Children’s Healthcare Atlanta Kurt Heiss (Site PI) Kawana Mitchell
• Children’s National Med Center Kurt Newman (Co-site PI) Rahul Shah (Co-site PI) Andrea Ewing-Thomas
• Children’s Hospital of Philadelphia Peter Mattei (Site PI) Lisa Czyzewski

Collaborative process
• Identification & recruitment of checklist champions
• Development of site-specific checklist
• Plan for piloting on small scale
• Obtaining buy-in from hospital leadership & peers
• Full implementation OR-wide
• Develop internal plan for auditing compliance
General study design
• Seven hospitals included as “checklist” implementers
• All inpatient procedures from 7 surgical services included
Cardiac, General, Neuro, Ortho, Plastics, Oto & Urology
• Pre-post intervention comparison design (9 months)
• Primary endpoint: Aggregate 30-day adverse event rate
• PHIS database used to identify events
• Results compared against seven control hospitals

Patient characteristics (demographics)
Checklist hospitals (n=7) Control Hospitals (n=7)
Pre-intervention(n=19,867)
Post-intervention(n=18,850)
Pre-intervention(n=15,616)
Post-intervention(n=15,298)
Age (mean years) 6.9 7.1 7.2 7.4
Sex (% male) 55.3 54.2 56.5 56.6
Insurance status : Government (%) Private (%) Other (%)
62.524.812.7
63.224.612.2
50.239
10.8
53.939.77.3
Race/ethnicity: African American(%) Hispanic (%)
20.216.9
18.517.5
10.623.3
10.826
Case Mix Index 6.1 6.1 5.5 5.5
Acuity of procedure(% emergent) 15.6 18.9 18.8 19.6
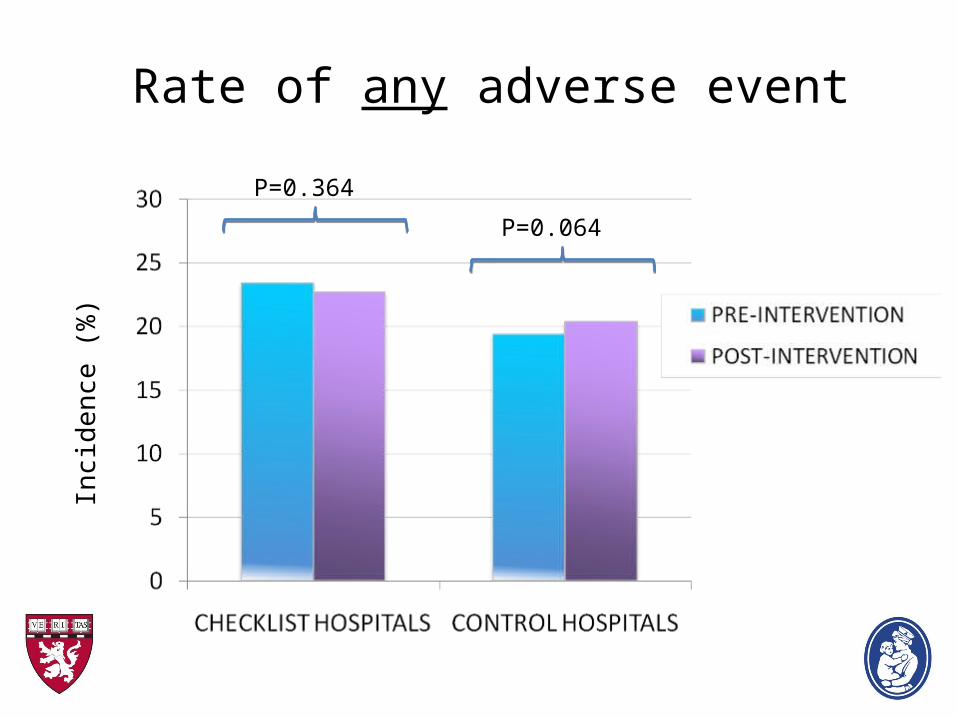
Rate of any adverse eventIn
cide
nce
(%
)
P=0.064
P=0.364
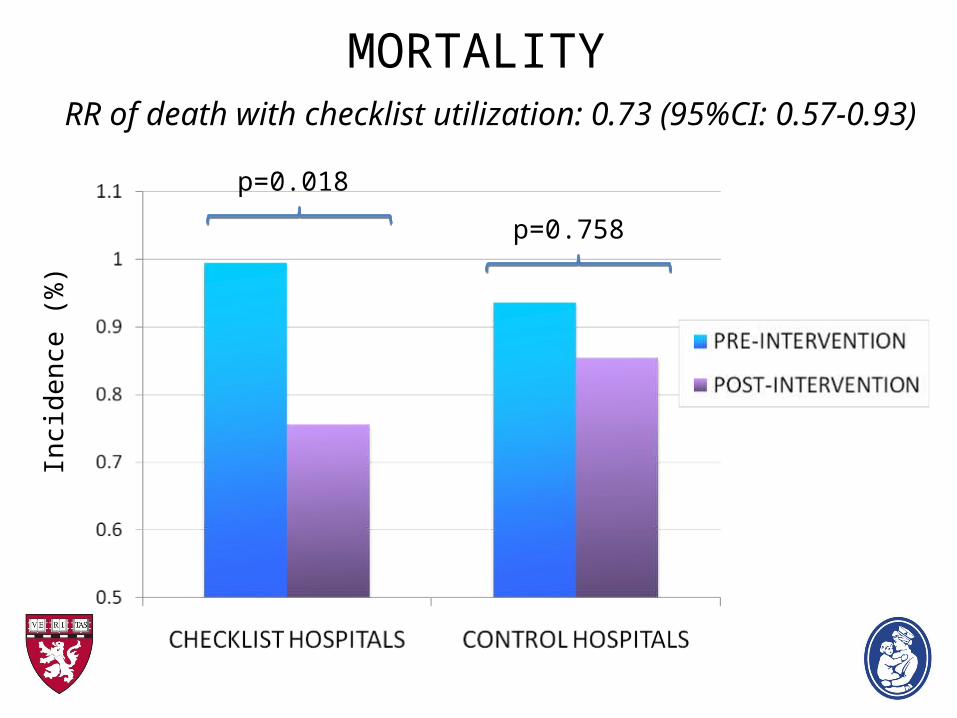
MORTALITY RR of death with checklist utilization: 0.73 (95%CI: 0.57-0.93)
Inci
den
ce (
%)
p=0.758
p=0.018

MORTALITY (High-risk specialties)In
cide
nce
(%
)
p=0.080p=0.332
p=0.064
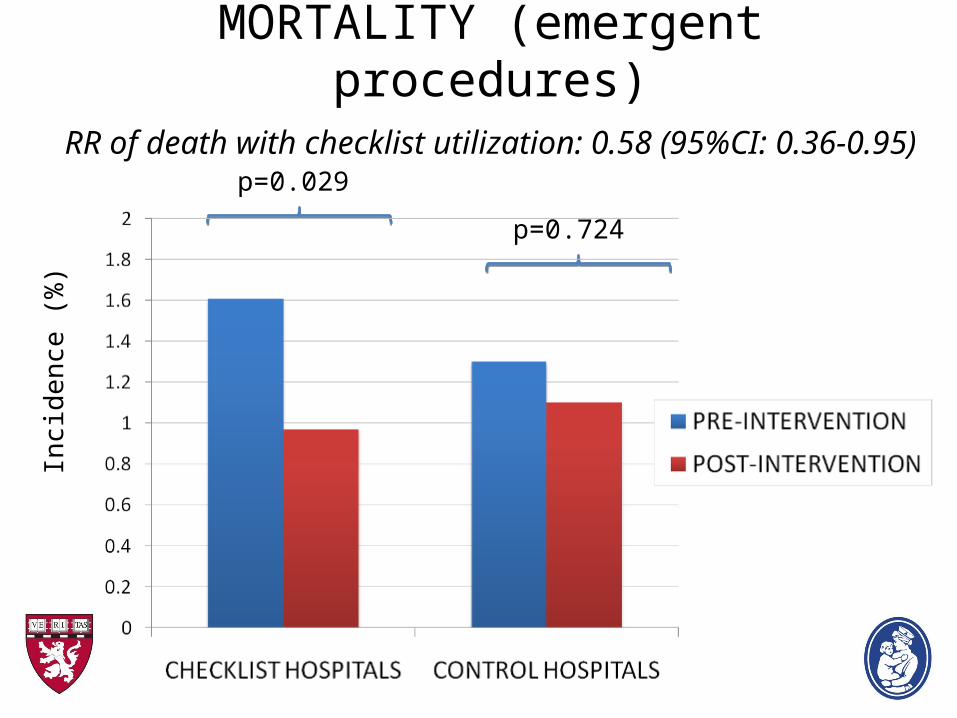
MORTALITY (emergent procedures)RR of death with checklist utilization: 0.58 (95%CI: 0.36-0.95)
Inci
den
ce (
%)
p=0.724
p=0.029
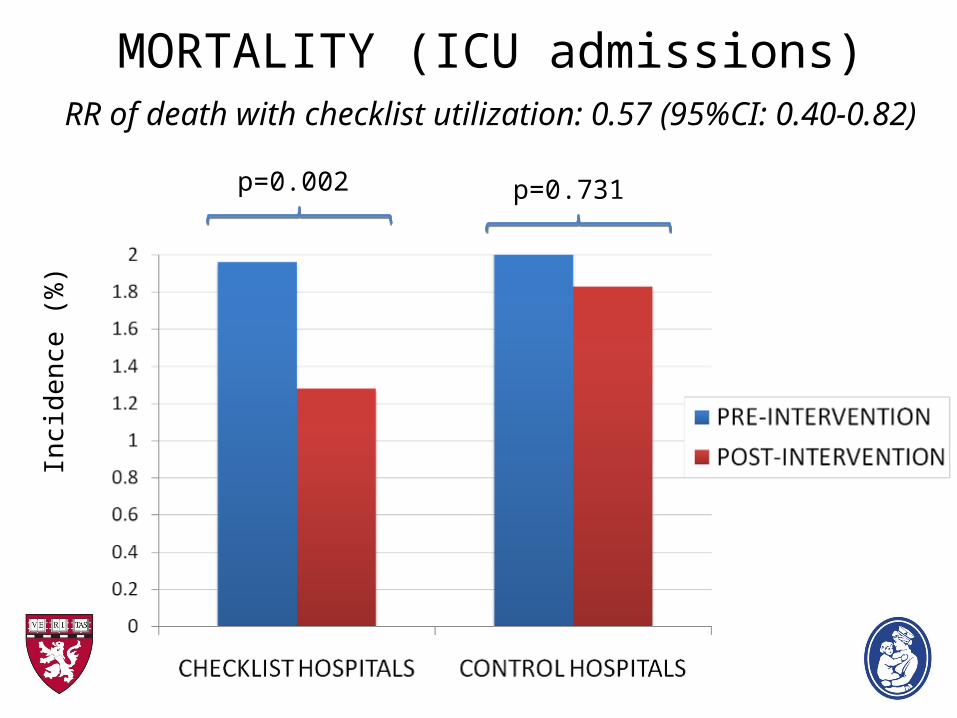
MORTALITY (ICU admissions)RR of death with checklist utilization: 0.57 (95%CI: 0.40-0.82)
Inci
den
ce (
%)
p=0.731p=0.002

Limitations of the study
• Unknown influence of the Hawthorne effect
• Unable to prove causality (non-randomized design)
• Reliance on administrative data for outcomes analysis
• Variation/degree of checklist compliance unknown
What can be concluded from the available data?
USE OF A SURGICAL SAFETY CHECKLIST
CAN SAVE LIVES !!!!!!
So then, how do people feel about using a surgical safety checklist?
--CHB Checklist Survey--
• Multidisciplinary targeting (3-headed monster!)
• Assess attitudes towards the checklist
• Gain insight on CHB’s current safety culture
• Obtain feedback for improving checklist utility

Checklist survey:Responses by specialty (n=177)
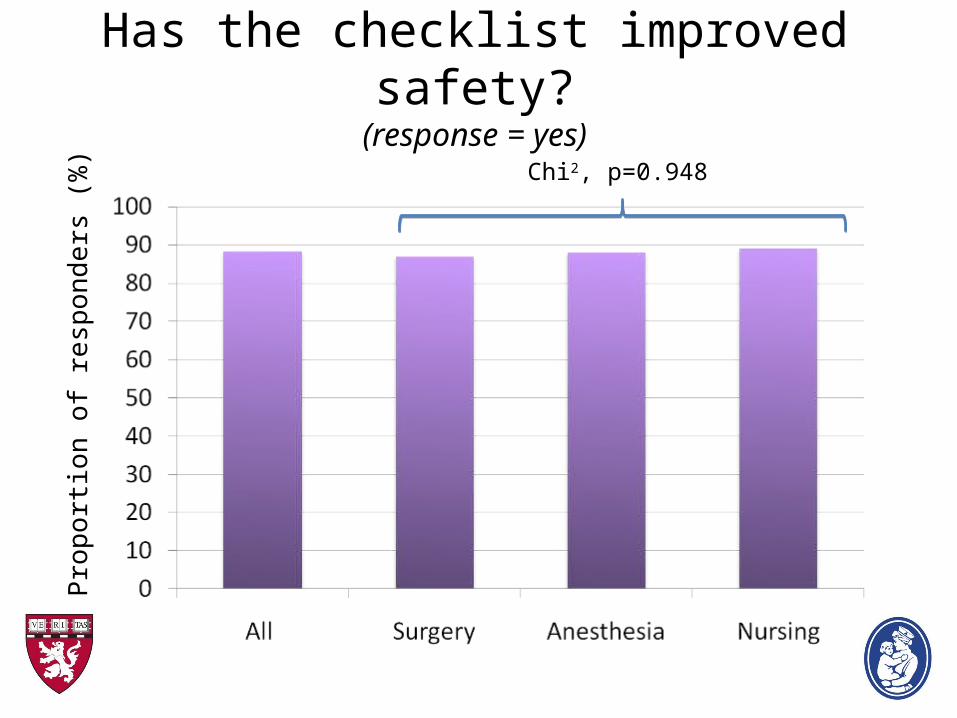
Has the checklist improved safety?(response = yes)
Pro
port
ion
of r
esp
ond
ers
(%
)
Chi2, p=0.948

How has the checklist improved safety?P
ropo
rtio
n of
re
spo
nde
rs (
%)
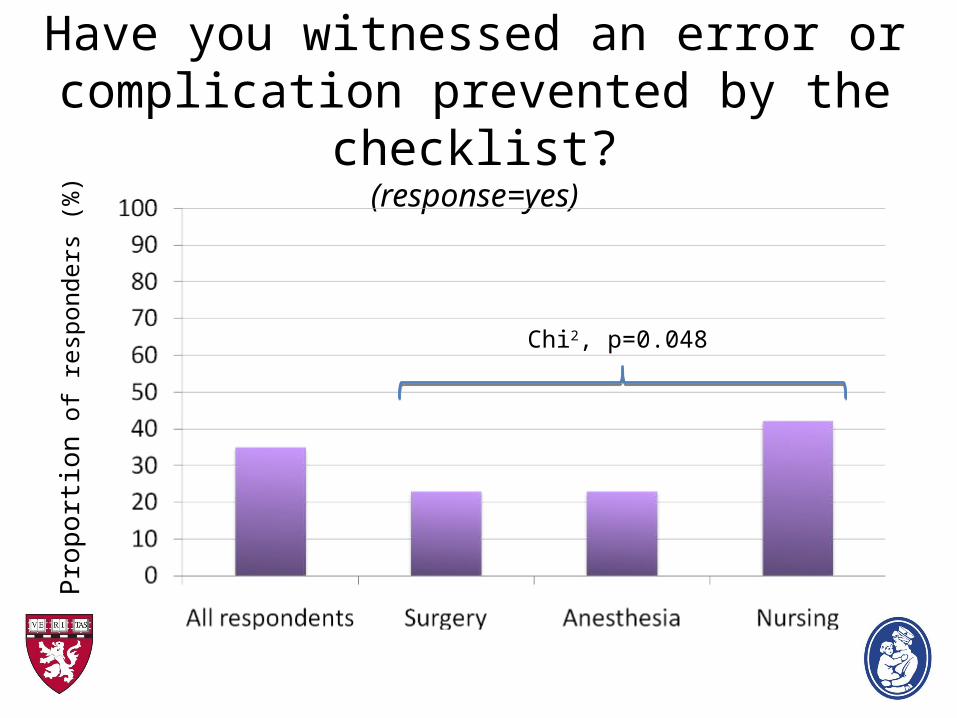
Have you witnessed an error or complication prevented by the checklist?
(response=yes)
Pro
port
ion
of
resp
onde
rs (
%)
Chi2, p=0.048

Has the checklist improved efficiency?(response=yes)
Pro
port
ion
of r
esp
ond
ers
(%
)
Chi2, p=0.110
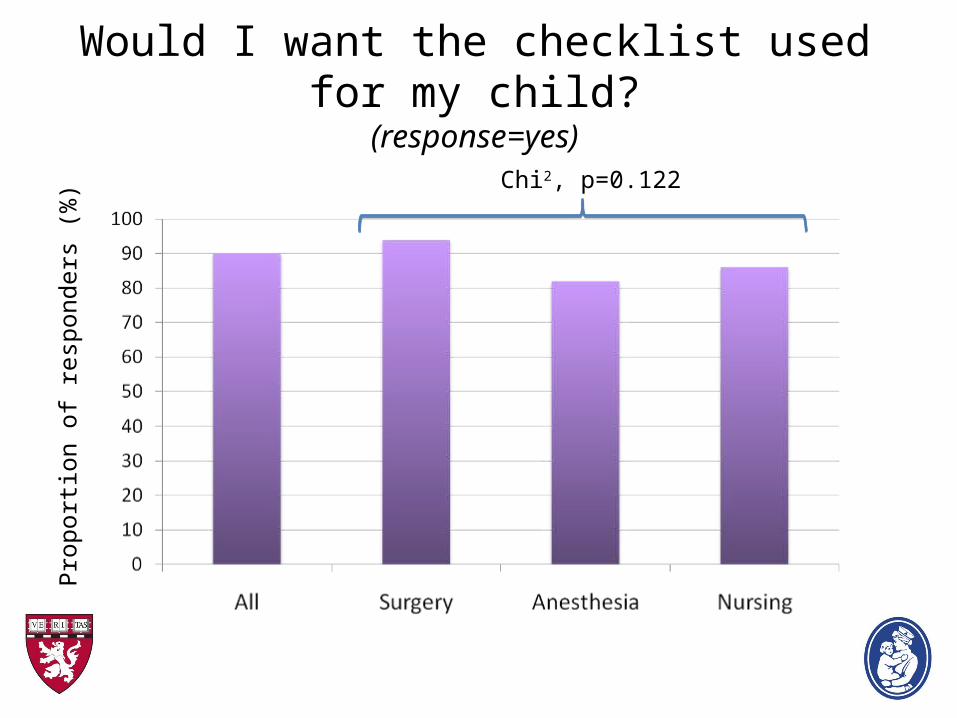
Would I want the checklist used for my child?(response=yes)
Pro
port
ion
of r
espo
nder
s (%
)
Chi2, p=0.122

Content adequacy of current checklist?P
ropo
rtio
n of
res
pond
ers
(%)
Chi2, p=0.987
Chi2, p=0.987
Chi2, p=0.987

So, is everyone in love with the checklist??
“This checklist is bullsh&! and just reinforces the
Betty Crocker approach to medicine !!”
“This is probably the most important surgical safety
intervention we could ever implement !!”
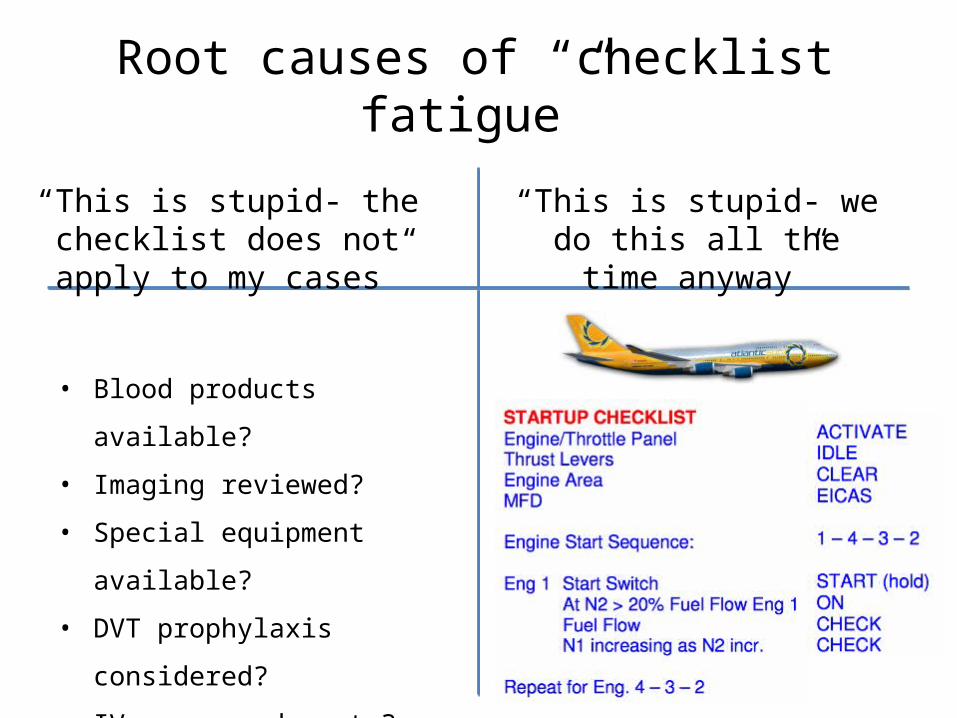
“This is stupid- we do this all the time anyway”
“This is stupid- the checklist does not apply to my cases”
• Blood products available?
• Imaging reviewed?
• Special equipment available?
• DVT prophylaxis considered?
• IV access adequate?
Root causes of “checklist fatigue”
So then, how can we improve the effectiveness of our checklist?
• Implementation of forcing cues into work flow
• Incorporation of a more effective auditing system
• Transition to a “quality”-centered checklist paradigm
• Development of customized checklists

Change in the checklist paradigm: transitioning from “safety” to “quality”
Surgical Quality
Value-based
Efficient
Effective
Safe

Variation in the use of surgical antibiotic prophylaxis for common pediatric procedures
How can we accomplish these goals?

How can we accomplish these goals?
Take home lessons….
• EFFECTIVE use of surgical checklists CAN SAVE LIVES!
• Checklist MUST be team-based and emphasize communication!
• Checklists HAVE to be developed with input from ALL stakeholders
• Leadership ABSOLUTELY has to be on board!

YOU ARE THE FUTURE OF SAFETY CULTURE!!!
And finally….