progress report: t he national lf and sth programme in bangladesh
DESCRIPTION
Progress report: t he national LF and STH programme in Bangladesh. By Dr. Rouseli Haq Program Manager Filariasis Elimination STH Control Program, DGHS, MoHFW 2014 RPRG Meeting WHO Region. Background Information. Geography and Population 155 Million (WHO) - PowerPoint PPT PresentationTRANSCRIPT

Progress report:the national LF and STH programme
in Bangladesh
By Dr. Rouseli HaqProgram Manager
Filariasis Elimination STH Control Program, DGHS, MoHFW2014
RPRG MeetingWHO Region

Background Information
• Geography and Population– 155 Million (WHO)– 142 Million (2011 National Census)– Tropical Rainforest (Ecological zones)

Political & Health Administrative Divisions:
Divisions : 7
Districts : 64
Sub-districts (Upa-zila): 485
Unions: 6,766
Wards (3 in each union)
Villages : 87,316
Municipalities :223

LF Burden Bangladesh • Population at risk: 70 million at baseline
• Total no of endemic districts: 34
• Mf rate baseline: 10.8% (Range >1% to 15%)
• Estimated morbidity status: 2% to 3.9%
(in endemic districts)
• Total no of districts requiring Mass Drug Administration (MDA): 19
• MDA using Albendazole and DEC started: in 2001
• MDA scale-up to reach all districts: in 2008
• MDA to be stopped in 18 districts by 2014 September.

MAP
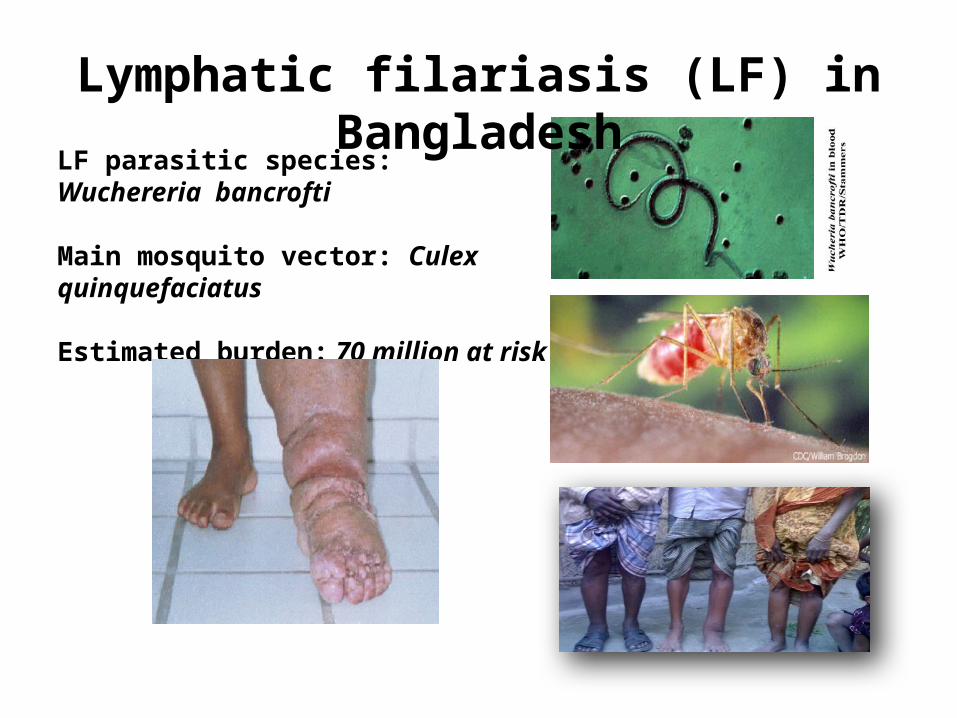
LF parasitic species: Wuchereria bancrofti
Main mosquito vector: Culex quinquefaciatus
Estimated burden: 70 million at risk
Lymphatic filariasis (LF) in Bangladesh
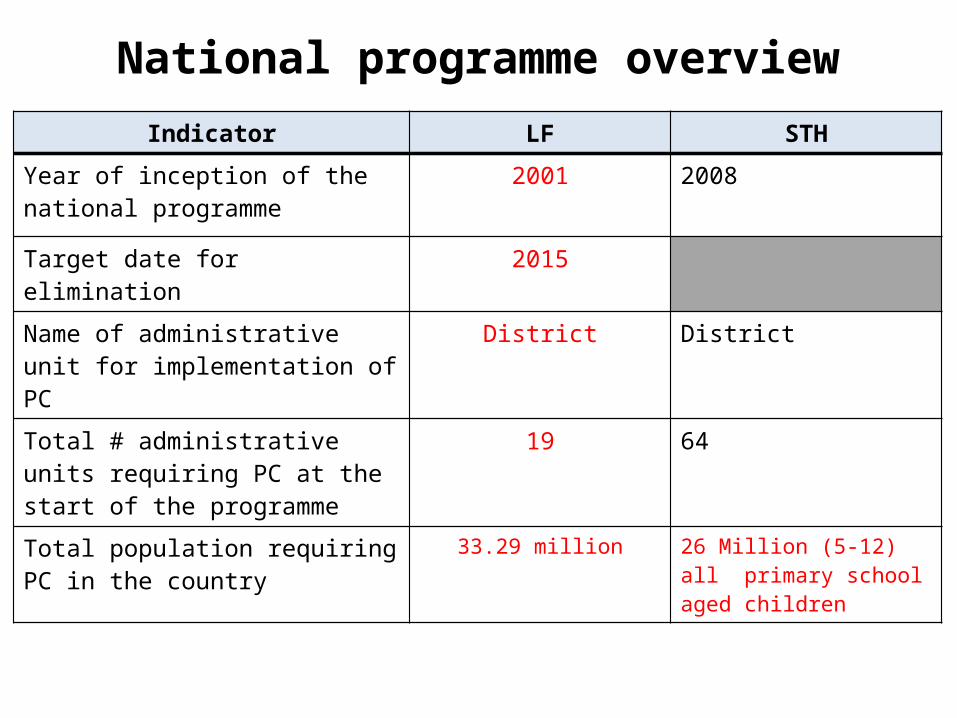
National programme overviewIndicator LF STH
Year of inception of the national programme
2001 2008
Target date for elimination 2015
Name of administrative unit for implementation of PC
District District
Total # administrative units requiring PC at the start of the programme
19 64
Total population requiring PC in the country
33.29 million 26 Million (5-12) all primary school aged children

PC Programme Financing
• Contributors to the 2013 programme costs (and rough estimate of contributions by each if available):
Contributor Funding (US$)National government 9.5 MillionSub-national government N/AInternal donors (___) N/AExternal donors (_USAID/CNTD/WHO__)
.33 Million
• Others (Children Without Worm, USA, (CWW) Johnson & Johnson (J&J) Vermox 500_)
1.38 Million

PC programme achievements 2013
Indicator Targeted Achieved
M&E
Total # sentinel and spot check sites surveyed (LF) 16 16Total # sentinel sites surveyed (STH) 12 12
Total # IUs where stopping-MDA TAS implemented (LF) 5 5Total # IUs which passed TAS and stopped MDA (LF) 5 5Total # IUs where surveillance TAS implemented (LF) 5 5
MMDP# IUs where hydrocele surgeries performed 3 3# IUs where lymphedema and ADLA management provided 7 5
Activities
Targeted Achieved#
administrative units for PC
# people#
administrative units for PC
# people
PCMDA2 (DEC + ALB) 4 8,660,332 4 7,133,685T3 (ALB/MBD) for STH 1st round 64 25,740,459 64 25,326,154T3 (ALB/MBD) for STH 2nd round 64 26,072,380 64 25,680,788

Progress Towards LF Elimination
DefinitionsStarted MDA ≥5 MDA rounds Surveillance MMDP access
MMDP access
Surveillance post-MDA
≥5 MDA rounds
Started MDA
0% 20% 40% 60% 80% 100%
37%
53%
100%
100%

Progress Towards STH scale up
5100694251812939*Coverage =
2008 2009 2010 2011 2012 201391.00%
92.00%
93.00%
94.00%
95.00%
96.00%
97.00%
98.00%
99.00%
100.00%
94.00%
97.50%
98.48%99.00% 99.00%
98.44%
% Coverage

PC coverage, 2013
*65% for LF and 75% for STH**reported coverage was verified by coverage survey or similar independent activity
PC type#
administrative units receiving
PC
# administrative units with
reported coverage above target*
# administrative units where
coverage was verified**
MDA2 (DEC + ALB) 4 4 4
T3 (ALB/MBD) for STH 1st round 64 64 64
T3 (ALB/MBD) for STH 2nd round 64 64 64

Impacts of MDA in Sentinel Sites (LF)# SS/SC sites
Sentinel Sites<1% mf
Sentinel Sites≥1% mf
Spot Check sites
<1% mf
Spot Check sites
≥1% mf
Baseline surveys 4 18 43 3
Latest surveys (post-MDA)
4 0 12 0
PC Monitoring and Evaluation
• Fifteen supervision trips in each round has performed by the staff from the National Program in order to better supervise the management of the De-worming week at all lower levels primary school
• Identify problems for implementation of MDA and facilitate problem solving
• Ensure the child awareness on the De-worming week• Observe ingestions drugs among the eligible children’s• Observe any adverse affect and reports to take necessary
action.

Three Tires of Supervision For STH
Supervision done in school
Supervisors from
Sub-dist.
Supervisors from Dist.
Level
Supervisor from
Central Level

PC Monitoring and Evaluation• SAE protocol
It is in place and being used, and managed within NTD programme. SAE is included in preparation of PC intervention.

Progress to date in assessing transmission #
# administrative units currently eligible for surveys to stop mass treatment 4
# administrative units where surveys to stop mass treatment were conducted 4
# administrative units where criteria was passed and mass treatment stopped 3
• Justification for stopping MDA without TAS in the above IU s N/A
• Integrated assessment of STH considered? N/A
LF Transmission Assessment Survey to stop MDA

LF Transmission Assessment: Forecasting
YearNumber of IUs to
be coveredTAS1 TAS2 TAS3
Total number of EUs
ICT/LF ST Required*
2014 4 6 10152
2015 9 5 20 33840
2016 4 6 10152
2017 9 13 21996
2018 4 6 10152
2019
2020
*sum of the total sample size required for each EU assessed;

Integrated Vector Management (LF)
• Describe any activities targeted to control LF vectors (including those conducted by other programmes)
N/A• Describe monitoring and evaluation of such
activities

LF MMDP – StrategyLF
National policy exist? Yes
Organizational placement within the government (who is responsible?)
Program Manager
How integrated with the health service? Provide morbidity management service through community clinic at community level
Training of service providers conducted (by who? How frequent?)
By the program trainers, twice in a year.
Patient mobilization and registration (by who? How?)
By local health staffs (Health assistant, CHCP)

LF MMDP – monitoring and evaluation
LFDescribe how MMDP services are currently monitored and reported to the national programme
Recently program has initiated the MMDP services to the patient at community clinic, Every Tuesday patients are coming to the CC for morbidity management.
How is “access” determined? N/A
Is there any quality assessment of provided services?
N/A

Best Practices
• MDA done among 35 million populations of 19 districts with >80% coverage.
• 7,908 Lymphoedema patient s were trained on morbidity control management.
• 20,000 Kit Box were distributed among Lymphoedema patients of 10 districts.
• Training of Doctors, District & Upa-zila manager, Paramedic, Health worker, Formal/ informal leaders, Teachers, NGOs workers, Medical Technologist were conducted.
• Social awareness through IEC activities-– i) Advocacy meeting– ii) Audiovisual- Documentary spot, duco-drama, TV spot, Radio jingel– iii) Advertisement through Mass media- Newspaper, Radio, Television– iv) Poster, leaflet, festoon, Bill board, Newsletter, Training module etc.
• 15 districts stopped MDA in 2011, 2012 & 2013 other 4 districts is ready for stop MDA in 2014 s a part of elimination of the disease.
Challenges and “Issues” for LF
• Strengthening IEC program• Evaluation of non endemic district• Developing sustainable surveillance• Capacity building-Human resource, training• Strengthening monitoring and evaluation• Morbidity control by using Community Clinics as Bangladesh
has very good Primary Health Care (PHC) infrastructure• Funding for Community Clinic, home based morbidity
control programme • New technology for morbidity control and expansion of
program with involving NGOs, Volunteers• Elimination of Lymphatic Filariasis through MDA by 2015

Challenges and “Issues” for STH
• Reaching “out of School” ,working , street children• Lack of awareness due to inadequate IEC activities• Mass Psychogenic illness during de-worming
week• Improvement of water, sanitation, and hygiene
and health education through school based approach for parasite control
• Coordination with partners working on STH control
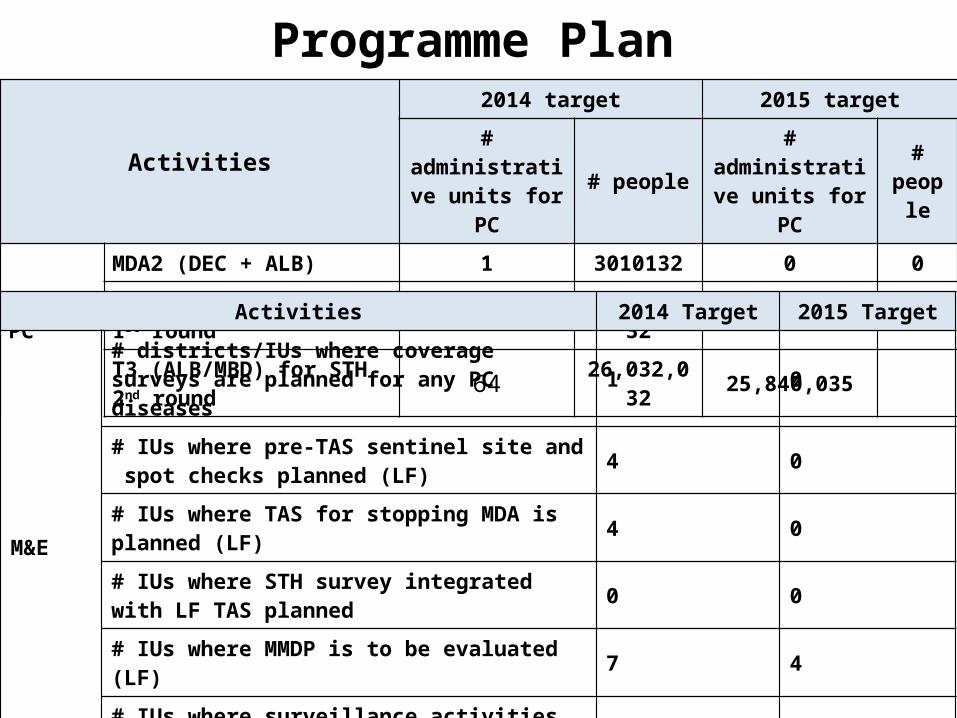
Programme Plan Activities
2014 target 2015 target# administrative
units for PC # people # administrative units for PC
# people
PC
MDA2 (DEC + ALB) 1 3010132 0 0
T3 (ALB/MBD) for STH 1st round 64 26,032,032 25,840,035
T3 (ALB/MBD) for STH 2nd round 64 26,032,032 25,840,035
Activities 2014 Target 2015 Target
M&E
# districts/IUs where coverage surveys are planned for any PC diseases 1 0
# IUs where pre-TAS sentinel site and spot checks planned (LF) 4 0
# IUs where TAS for stopping MDA is planned (LF) 4 0# IUs where STH survey integrated with LF TAS planned 0 0
# IUs where MMDP is to be evaluated (LF) 7 4# IUs where surveillance activities are to be carried out (LF) 10 14
MMDP # IUs where MMDP services newly initiated (LF) 4 5IVM # IUs where IVM coordinated to target LF vectors 0 0

PC medicine request for 2015 ALB (LF) ALB (STH) MBD DEC
required 51,680,070
in stock
in pipeline
requested to WHO 51,680,070
requested toMDP (IVM) or ITI (AZI)
Procured from other sources(source, # tablets and target age group)