program disclosure - :: cldf
TRANSCRIPT


Program Disclosure
• This activity has been planned and implemented in accordance with
the Essential Areas and Policies of the Accreditation Council for
Continuing Medical Education (ACCME) through the joint
providership of Purdue University College of Pharmacy and the
Chronic Liver Disease Foundation. Purdue University School of
Pharmacy is accredited by the ACCME to provide continuing
medical education for physicians.
• This program is supported by an educational grant from Salix
Pharmaceuticals.

Program Disclosure (cont.)
• Credit Designation –Purdue University College of Pharmacy designates this live activity
for a maximum of .5 AMA PRA Category 1 Credit(s) ™. Physicians should claim only the
credit commensurate with the extent of their participation in the activity.
• Faculty Disclosure Statement- All faculty and staff involved in the planning or
presentation of continuing education activities sponsored/provided by Purdue University
College of Pharmacy are required to disclose to the audience any real or apparent
commercial financial affiliations related to the content of the presentation or enduring
material. Full disclosure of all commercial relationships must be made in writing to the
audience prior to the activity.
• Nursing Accreditation Statement - Purdue University Continuing Nursing Education is
accredited as a provider of continuing nursing education by the American Nurses
Credentialing Center's Commission on Accreditation. This program has been approved for
.5 contact hours.
• Pharmacist Accreditation Statement - Purdue University College of Pharmacy is
accredited by the Accreditation Council for Pharmacy Education as a provider of
continuing pharmacy education. This is knowledge based, continuing education activity of
Purdue University, an equal access/equal opportunity institution. Universal Activity Number
(UAN): 0018-9999-15-007-L01-P, .5 contact hours (.5 CEU).
Faculty, Staff and Reviewer Disclosure
Statement
• Medical Writer: Lisa Pedicone, PhD- No Relevant Relationships
• All faculty, staff and reviewers involved in the planning, review or presentation of
continuing education activities sponsored/provided by Purdue University College of
Pharmacy are required to disclose to the audience any relevant commercial financial
affiliations related to the content of the presentation or enduring material. Full disclosure
of all commercial relationships must be made in writing to the audience prior to the
activity.
“All additional planning committee members, Chronic Liver Disease Foundation
and Purdue University College of Pharmacy staff have no relationships to disclose.”

Educational Objectives
• Discuss the natural history and complications of cirrhosis
including management options
• Review data on the screening, diagnosis
and management of chronic liver disease
• Describe the importance of linking patients with chronic
liver disease into specialty care

Case 1
• Paul is a 62 year old black man who presents to the ER
with severe abdominal pain.
• PMHx: “liver problem” years ago when drinking
– Developed ascites but resolved with abstinence
• Exam: Diffusely tender abdomen with some guarding
• Labs:
– CBC: WBC 7.2, Hb 10.1, Plts 71
– CMP: Alb 3.4, TB 1.2, AST 32, ALT 25, AP 251, Cr 1.2
– Viral hepatitis screen: negative
• CT with large heterogeneous mass

Discussion
1. Does Paul have cirrhosis?
– What do you suspect is the reason for his pain?
2. How do you diagnose cirrhosis?
– Biopsy
– Imaging
– Non-invasive markers? And for which etiologies?
– Transient elastography?
3. What would you do next?

Compensated Cirrhosis May Be
Difficult to Recognize
• Asymptomatic (compensated)
– Subtle clues may be overlooked • Thrombocytopenia
• Muscle wasting
• AST>ALT without alcohol consumption
• Liver enzymes may not be abnormal
– Etiology may be remote • Prior alcohol use
• Uncontrolled DM and obesity
• Decompensated (Symptomatic)
– Portal hypertension: ascites, OHE, variceal bleeding – Hepatic failure: Jaundice, Coagulopathy
From http://digestive.niddk.nih.gov/ddiseases/pubs/cirrhosis/. Accessed January 2014.
Trichrome stain micrograph from http://en.wikipedia.org/wiki/Cirrhosis. Accessed January 2014.

History --or
Physical --or
Examination
Laboratory or
Studies
Radiographic
Studies
Physical examination
findings consistent with
liver disease or high
suspicion for chronic liver
disease
Confirm history via signs
and symptoms of chronic
liver disease and positive
risk factors
Confirm history via signs and
symptoms of chronic liver disease
and positive risk factors and
screen for hallmark physical
examination findings
Diagnosis of Cirrhosis and
Chronic Liver Failure
Obtain liver panel*, CBC with platelets, PT/INR, and targeted serologic studies to determine etiology
Obtain abdominal imaging for confirmation of cirrhosis and HCC screening
Refer for possible liver biopsy if diagnosis of cirrhosis is uncertain, as well as possible determination of etiology via
histology if not readily determinable through serologic testing and if potential benefit outweighs risk of procedure
*Tests typically include ALT, AST, alkaline phosphatase, and -glutamyltransferase, total, direct and indirect serum bilirubin, and serum albumin.
Adapted from Heidelbaugh JJ, Bruderly M. Am Fam Physician 2006;74:756-762.

Non-Invasive Markers
• Indirect biomarkers
– APRI, FIB4 etc
• Direct biomarkers
– Fibrotest, Fibrosure, etc
• Transient Elastography
• Clinically obvious cirrhosis does not require confirmation

Prevalence of Cirrhosis
1. Schuppan D, Afdhal NH. Lancet 2008;371(9615):838-851.
2. Available at http://pubs.niaaa.nih.gov/publications/surveillance83/Cirr05.htm; Accessed February 2015.
3. Khungar V, Poordad F. Clin Liver Dis 2012;16:73-89.
• The prevalence of cirrhosis, both worldwide and in
the US, is unknown1
– Cirrhosis is an outcome of a variety of causes; underlying
cause is commonly used for surveillance purposes2
– Compensated cirrhosis often goes undetected for
prolonged periods of time1
• Experts estimate that 5.5 million people in the
United States have cirrhosis3

Annual Prevalence Rates Between 1996 and 2006 Among HCV-Infected Veterans
Progressive Increase in Incidence of
HCV-Related Cirrhosis and HCC in US
El-Serag HB. Gastroenterology 2012;142:1264–1273.
He
pa
toc
ellu
lar C
an
ce
r (HC
C)
Cirrhosis
Decompensated
Cirrhosis
HCC
1996
20%
18%
16%
14%
12%
10%
8%
6%
4%
5%
4%
3%
2%
1%
0%1997 1998 1999 2000 2001 2002 2003 2004 2005 2006
Cir
rho
sis
an
d
De
co
mp
en
sa
ted
Cir
rho
sis

Liver Cancer Projected to Be the 3rd Leading
Cause of Cancer-Related Death by 2030
“Projecting Cancer Incidence and Deaths to 2030: The
Unexpected Burden of Thyroid, Liver and Pancreas
Cancers in the United States.”
• Cancer incidence/deaths projected for 2020 and 2030
• Breast, prostate, and lung cancers remain top cancer
diagnoses
• Lung cancer is projected to remain top cancer killer
– Pancreas and liver cancers projected to surpass breast, prostate, and
colorectal cancers to become the 2nd and 3rd leading causes of cancer-
related death
Cancer Res. 1–9. 2014 AACR
Early Recognition Allows
Preventative Measures
• HCC screening
• Screening for varices
• Recognition of encephalopathy
• Recognition of ascites
• Life style and nutrition counseling
• Early intervention when decompensation first recognized

HCC Screening
• HCC detected after the onset of symptoms has a
very poor prognosis
– With 0-10% survival at 5 years
• Early recognition can improve outcomes
– Resection or liver transplantation
– 5-year disease-free survival of greater than 50%
• Screening with Ultrasound recommended at 6 month
intervals in all individuals with cirrhosis
• MUST RECOGNIZE CIRRHOSIS

HCC Diagnostic Algorithm
"Bruix J and M Sherman, Hepatology, Vol 53, No. 3, 2011.”
Arterial hypervascularity
AND venous or delayed
phase washout
Liver nodule
Repeat US at 3 months
Growing/changing
character
Investigate
according
to size
Other contrast
Enhanced study (CT or MRI)
< 1 cm > 1 cm
4-phase MDCT/ dynamic
contrast enhanced MRI
Arterial hypervascularity
AND venous or delayed
phase washout Stable
Yes No
No
Biopsy
Yes
HCC

Case 2
• Tim is a 56 year old white man with HCV cirrhosis complicated by
ascites and non-bleeding varices. He is listed for transplantation
with a MELD of 17.
• His wife calls his coordinator because Tim has been sleeping all day.
• The coordinator advises her to take Tim to the nearest ER.
• Primary complications of cirrhosis include:
– Ascites
– Jaundice
– Variceal hemorrhage
– Hepatic encephalopathy
• Other complications that can occur include:
– Hepatocellular carcinoma
– Spontaneous bacterial peritonitis
– Hepatic hydrothorax
– Hepatorenal syndrome
– Portopulmonary hypertension
– Portal vein thrombosis
– Hepatopulmonary syndrome
How would you explain Tim’s symptoms?
Lefton HB et al. Med Clin N Am 2009;93:787-799.

Overt Hepatic Encephalopthy (OHE)
• Overt hepatic encephalopathy (OHE) occurs in:
‒ 30% to 45% of cirrhotic patients
‒ 10% to 50% of patients with TIPS
• Covert hepatic encephalopathy (CHE) affects
approximately 20% to 60% of patients with liver disease
– Has been called subclinical encephalopathy or minimal
encephalopathy (MHE) in the past
TIPS = transjugular intrahepatic portosystemic shunt.
Mullen KD, et al. Semin Liver Dis. 2007;27(Suppl 2):32-47.
Mullen KD, Prakash RK. Clin Liver Dis 2012;16:91-93,
Poordad FF. Aliment Pharmacol Ther. 2006;25(Suppl 1):3-9.

Diagnosis of OHE
• Clinical recognition of the distinctive neurologic features of HE
• Knowledge that underlying cirrhosis is present
• Exclusion of other etiologies of neurologic and/or metabolic
abnormalities
• Identification of precipitating factors
• Grading the severity
Adapted from:
Mullen KD. Semin Liver Dis. 2007;27(suppl 2):3-9.
Lawrence KR, Klee JA. Pharmacotherapy. 2008;28(8):1019-1032.

Common Less Common
• Confusion or coma
• Asterixis
• Loss of fine motor skills
• Hyper-reflexia
• Cognitive deficits detected by
special testing
• Babinski sign
• Slow, monotonous speech
• Extrapyramidal-type movement
disorders
• Clonus
• Decerebrate posturing
• Decorticate posturing
• Hyperventilation
• Seizures*
Neurologic Manifestations of OHE
*Seizures seen primarily in type A HE.
Mullen KD. Semin Liver Dis. 2007;27(suppl 2):3-9.

Other Causes of Altered Mental Status*
• Intracranial hematomas
• Thyroid dysfunction
• Hypoglycemia
• Hypoxia
• Hypercapnia
• Drug intoxication
*Most entities can be diagnosed by brain imaging or laboratory tests. Severe sepsis can cause encephalopathy or precipitate HE.
Mullen KD. Semin Liver Dis. 2007;27(suppl 2):3-9.
• Hypoglycemia
• Hyperglycemia
• Acidosis
• Encephalitis
• Severe sepsis
• Uremia

Characterization of HE Stages
Normal Covert HE I II III IV
Overt HE Stages
Categorization is often arbitrary and
varies between raters
Simple Clinical
Diagnosis
Worsening cognitive dysfunction
coma
Bajaj JS, et al. Hepatology. 2009;50:2014-2021.
Grade Features
0 No abnormalities detected
I Trivial lack of awareness; Euphoria or anxiety; short attention span; Impairment of addition
or subtraction
II Lethargy or apathy, Disorientation for time, Obvious personality change, Inappropriate
behavior
III Somnolence to semi-stupor, Responsive to stimuli, Confused, Gross disorientation, Bizarre
behavior
IV Coma, unable to test mental state
West Haven Criteria

Measuring Serum Ammonia Level in
Patients with Altered Mental Status
Elgouhari HM, O’Shea R. Cleve Clin J Med 2009;76:252-254.
• One’s clinical impression is the main guide to diagnosing
hepatic encephalopathy (HE)
• A normal or modestly elevated blood ammonia level does not
rule out a diagnosis of HE
• Blood ammonia testing may be helpful if there is no clear
evidence of underlying chronic liver disease
– An increased blood ammonia level may have prognostic value
(e.g., acute liver failure) or may be the basis for further
evaluation for uncommon metabolic disorders (e.g., urea cycle
disorders)

How would you manage Tim?

Patient with possible OHE
Confirm that it is HE: Yes
No HE: Other causes of
altered mental status
Initiate empiric treatment for HE;
Search for precipitating factor
Precipitating factors
found
Precipitating factors
not found
Treatment directed to
the precipitating factor
Evaluate for liver transplant
Proposed Algorithm for
Inpatient OHE Management
Adapted from Bajaj JS. Aliment Pharmacol Ther 2010;31:537-547 and Prakash R, Mullen KD. Nat Rev Gastroenterol
Hepatol 2010;7:515-525
• Admit to ICU for grade 3 HE
• Continue HE therapy with lactulose
and rifaximin

Treatment Approach for Acute
Overt Hepatic Encephalopathy
• Precipitating factors:
– GI bleeding
– Infection
– Sedating medications
– Electrolyte abnormalities
– Constipation
– Renal Failure

76%
24%
44% 49%
0
10
20
30
40
50
60
70
80
Reversal of HE Death
% o
f P
ati
en
ts
Lactulose + Rifaximin
Lactulose + Placebo
48/63 25/57 15/63 28/57
P=0.004
P=<0.05 • Treatment was given
through nasogastric
tube and continued until
recovery of HE or a
maximum of 10 days
• Hospital stay was
shorter with lactulose +
rifaximin than with
lactulose + placebo
(5.8±3.4 vs. 8.2±4.6
days, P=0.001)
Treatment Approach for Acute Overt Hepatic
Encephalopathy: Lactulose + Rifaximin vs. Lactulose
Sharma BC et al. Am J Gastroenterol 2013;108:1458-1463.
General supportive and nutritional interventions
General supportive care • Fall precautions in disoriented patients
• Prevention of infections--changing IV lines, prevent
aspiration pneumonia, isolation
Nutritional support • Regular protein diets are recommended
• Consider addition of branched-chain amino acids
(valine, leucine, and isoleucine) and zinc; consider
eliminating wheat and milk proteins
Khungar V, Poordad F. Clin Liver Dis 2012;16:73-89.
Treatment Approach for Acute
Overt Hepatic Encephalopathy
• Treatment goals
– Prevention of recurrent episodes of HE
– Improvement of daily functioning
– Evaluation for liver transplant
Outpatient Management after
an Episode of OHE
Bajaj JS. Aliment Pharmacol Ther. 2010;31:537-547.

Sharma BC et al. Gastroenterology. 2009;137:885-891.
Prophylactic Treatment of HE
• Treating patients with covert HE to prevent
development of a first episode is referred to as
primary prophylaxis of HE
• Preventing recurrence of HE in patients who had a
previous episode of HE is referred to as
secondary prophylaxis of HE
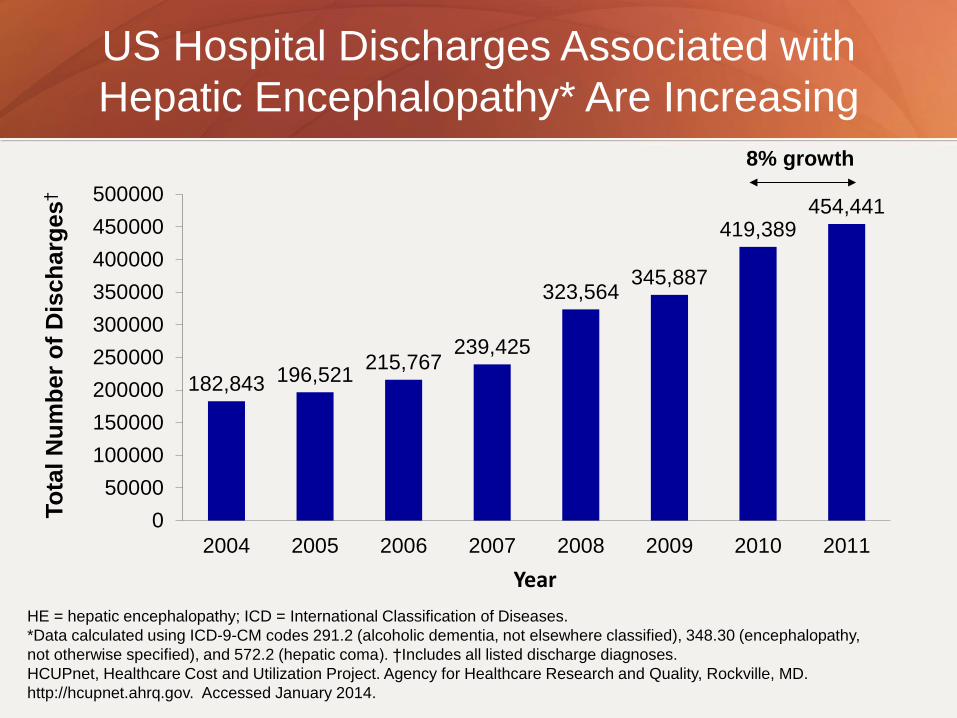
182,843 196,521 215,767
239,425
323,564 345,887
419,389 454,441
0
50000
100000
150000
200000
250000
300000
350000
400000
450000
500000
2004 2005 2006 2007 2008 2009 2010 2011
To
tal N
um
be
r o
f D
isch
arg
es
†
8% growth
Year
US Hospital Discharges Associated with
Hepatic Encephalopathy* Are Increasing
HE = hepatic encephalopathy; ICD = International Classification of Diseases.
*Data calculated using ICD-9-CM codes 291.2 (alcoholic dementia, not elsewhere classified), 348.30 (encephalopathy,
not otherwise specified), and 572.2 (hepatic coma). †Includes all listed discharge diagnoses.
HCUPnet, Healthcare Cost and Utilization Project. Agency for Healthcare Research and Quality, Rockville, MD.
http://hcupnet.ahrq.gov. Accessed January 2014.

Hospital Readmissions Among Patients with
Decompensated Cirrhosis are Common
• Retrospective study of 402 patients
from an academic transplant center
• Follow-up time censored at death,
elective admissions such as
transplant or post-procedure
observation, or the date of last clinic
note; median follow-up was 203 days
• Population included cirrhotic patients
hospitalized for ascites, spontaneous
bacterial peritonitis, renal failure,
hepatic encephalopathy, or variceal
hemorrhage
• Median time to first readmission was
67 days
• Median number of readmissions was
2 (range 0-40); overall rate was 3
hospitalizations/person-years
14%
37%
69%
0
10
20
30
40
50
60
70
80
Within1 wk
Within1 mo
Overall
Hospital Readmissions
Volk ML et al. Am J Gastroenterol 2012;107:247-252.
% o
f P
atients

100
80
60
40
20
0
Su
rviv
al, %
0 12 24 36 48
Months
42% survival at
1 year 23% survival at
3 years
Overt HE Is Associated with a
Poor Prognosis
• <50% survival at 1 year after diagnosis of HE;
<25% survival at 3 years
Bustamante et al. J Hepatol. 1999;30:890-895.

Other Management Concerns
• Tim’s OHE is well controlled on medical therapy.
He returns after his hospitalization for follow-up to
pre-transplant clinic.
• On review on his medication list his MD sees that
he is on a beta-blocker as primary prophylaxis.
• Would you continue this medication?
Background
• Non-selective beta-blockers (NSBBs) prevent
portal hypertensive bleeding in patients with
cirrhosis.
• But studies suggest NSBB use is associated
with decreased survival in patients with
refractory ascites.
– NSBBs may reduce perfusion of vital organs

NSBBs Increase AKI
• Nested case-control of liver transplant waitlist
registrants at Mayo clinic
– Cases developed AKI (2-3 fold increase in serum Cr)
– Matched by MELD-Na score, age at registration, baseline
creatinine, and follow-up duration
• Impact of NSBB on AKI incidence was different
according to the presence of ascites:
– NSBB use with ascites was associated with development of AKI
(hazard ratio [HR], 2.79; 95% confidence interval [CI], 1.40-5.54),
– Without ascites, NSBB was protected (HR, 0.19; 95% CI, 0.06-0.60)

Conclusions
• Cirrhosis can be asymptomatic
• Screening and surveillance of life threatening
complications can allow early recognition and
preventative strategies
• Individuals with symptomatic cirrhosis and
liver cancer should be considered for liver
transplantation
– Linkage to experienced providers is instrumental