profiles of adaptive functioning: autism spectrum disorders, mental retardation, and beyond....
TRANSCRIPT

Profiles of Adaptive Functioning: Autism Spectrum Disorders, Mental Retardation,
and Beyond.
California Association of School Psychologists
February 17, 2005 8:30-10:15
Sara S. Sparrow, PhD
Yale Child Study Center

Speech PathologyPsychology
Doman-DelacatoMeasurement Dilemmas
How I Discovered Adaptive Behavior

4 AREAS FOR TODAY• NEW FEATURE OF THE VINELAND II• CHANGES IN THE PURPOSES OF
ADAPTIVE BEHAVIOR ASSESSMENTS
• RECENT RESEARCH ON EFFECTS OF INTERVENTION WITH PERSONS WTH HIGH FUNCTIONING ASD
• CLINICAL APPLICATIONS AND ADAPTIVE PROFILES

Adaptive Behavior Assessment
Working our way back:
30 years since Pl 94-142 (1975)
16 years earlier AAMD (1959)
24 years earlier Edgar Doll published
The Vineland Social Maturity Scale (1935)

Purpose
Diagnosis of Mental Retardation

Things Have Changed
More and more assessing adaptive behavior has had broader applications
One reason is that different research has demonstrated that there appear to be
different profiles for various diagnostic groups

USES OF ADAPTIVE BEHAVIOR ASSESSMENTS
– Confirming or establishing diagnosis– Special services qualification– Program planning– Progress reporting/tracking– Identifying changes over time

USES, conintued
– Mental Retardation– Early Childhood Special Education– Autism Spectrum Disorders– Traumatic Brain Injury– Adult Mental Problems– As a measure to support the diagnosis of other
disabilities– Death Penalty Cases and
– Many others

A word about Death penalty cases:
Atkins versus Virginia.
Psychologists will be increasingly asked to provide testimony in these cases, mainly regarding adaptive functioning
A Virginia court just ruled that Atkins did not meet criteria for a diagnosis of mental retardation
2005
Supreme Court rules that individuals with (chronological) age under 18 years cannot be executed.
What about mental age?
THUS
• Implications for the development of the Vineland II

Introducing the Vineland-II
VINELAND-II Overview
• Because clinicians have different needs when it comes to assessing adaptive behavior, we now offer four forms:
--Survey Interview Form– NEW Parent/Caregiver Rating Form– Teacher Rating Form– Expanded Interview Form
MAJOR NEW FEATURES• Ages: Birth to 90 years of age• New Norms• Increase Item density at floor and
ceiling• Extensive investigation and
elimination of item bias• Increase items relevant to ASD and
young children• Eliminate outdated items• Increase Items reflecting our
society’s technological advances• Subdomain standard scores• New Maladaptive
Other New Features
• Parent Caregiver Forms
• Teacher report Form – – Daily Living Skills
• Personal Subdomain• Academic Subdomain• School-Community Subdomain

• Attention Deficit/Hyperactivity Disorder• Autism – nonverbal• Autism – verbal• Learning Disability• Mental Retardation – Mild (child)• Mental Retardation – Moderate (child)• Mental Retardation – Mild (adult)• Mental Retardation – Moderate (adult)• Emotional Disturbance• Visual Impairment• Hearing Impairment
Validity Evidence: 11 Clinical Groups

• Vineland Adaptive Behavior Scales• Adaptive Behavior Assessment
System (ABAS)• WISC III• WAIS-III• BASC-2
Validity Evidence: Criterion

SUBDOMAIN
V-SCALED SCORESMean = 15
SD = 3

VINELAND II NEW MALADAPTIVE
DOMAIN
STILL BOTH MINOR AND MAJOR
MALADAPTIVE
FACTOR ANALYTIC STUDIESREVEALED
THREE FACTORS

Internalizing Items• Is overly dependent • Avoids others and prefers to be alone • Has eating difficulties • Has sleep difficulties • Refuses to go to work or school because of
fear, feelings of rejection, or isolation • Is overly anxious or nervous • Cries or laughs too easily • Has poor eye contact • Is sad for no clear reason • Avoids social interaction • Lacks energy or interest in life
Externalizing Items
• Is impulsive• Has temper tantrums• Intentionally disobeys or defies those in
authority• Taunts, teases, or bullies• Is inconsiderate or insensitive of others• Lies, cheats, or steals• Is physically aggressive• Is stubborn or sullen• Says embarrassing things or asks embarrassing
questions in public• Behaves inappropriately at the urging of others
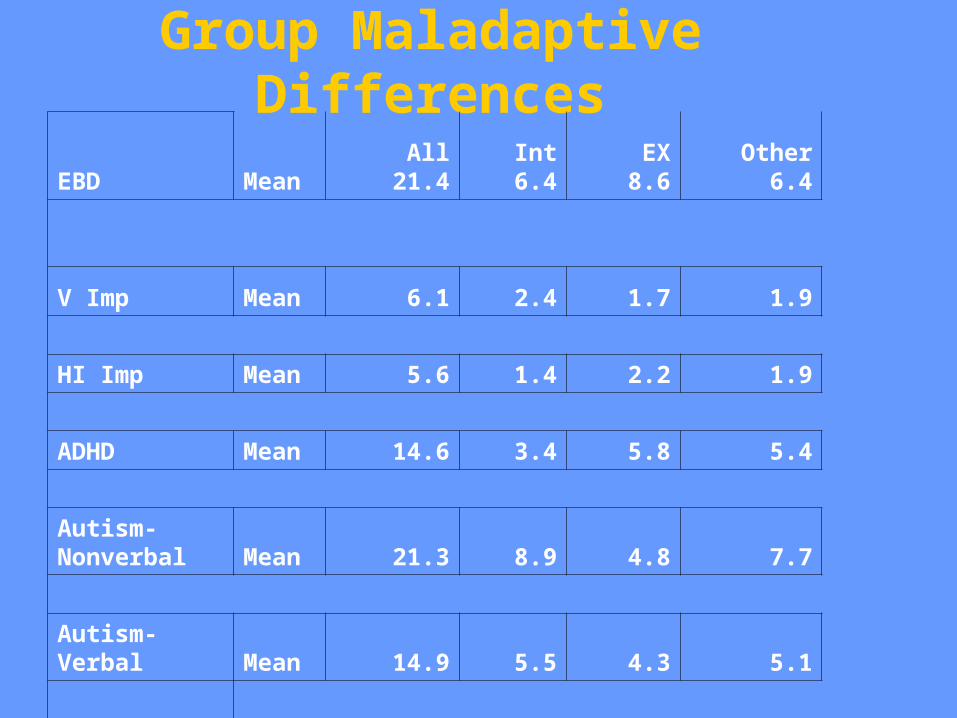
Group Maladaptive Differences
EBD MeanAll
21.4Int6.4
EX8.6
Other6.4
V Imp Mean 6.1 2.4 1.7 1.9
HI Imp Mean 5.6 1.4 2.2 1.9
ADHD Mean 14.6 3.4 5.8 5.4
Autism-Nonverbal Mean 21.3 8.9 4.8 7.7
Autism-Verbal Mean 14.9 5.5 4.3 5.1

Maladaptive Behavior by Age for Individuals with MR
School-aged children with MR (all levels) had maladaptive means significantly higher than age matched clinical groups but < 1SD difference.
Adults (19-90) with MR (all levels) had maladaptive means significantly higher than age matched clinical groups AND school aged groups with MR

Maladaptive Behaviors by Age for Individuals with MR
Differences were greatest in the adult severe-profound group
Only Internalizing behaviors fell into the “elevated range” (the highest level) for this group
Adaptive Functioning of Mental Retardation Groups
For all levels and ages, mean levels of all domains and the adaptive behavior composite were at least 2SD below the mean

25
40
55
70
85
100
Mild Moderate Severe Mild Moderate Severe Verbal Non-verbal
ADHD EBD LD Visual Hearing
MR (6 - 18) MR (Adult) Autism High Incidence Sensory Impairment
AB
C S
td. S
co
re

Severe Moderate Mild
6
7
8
9
10
11
12
13
14
15
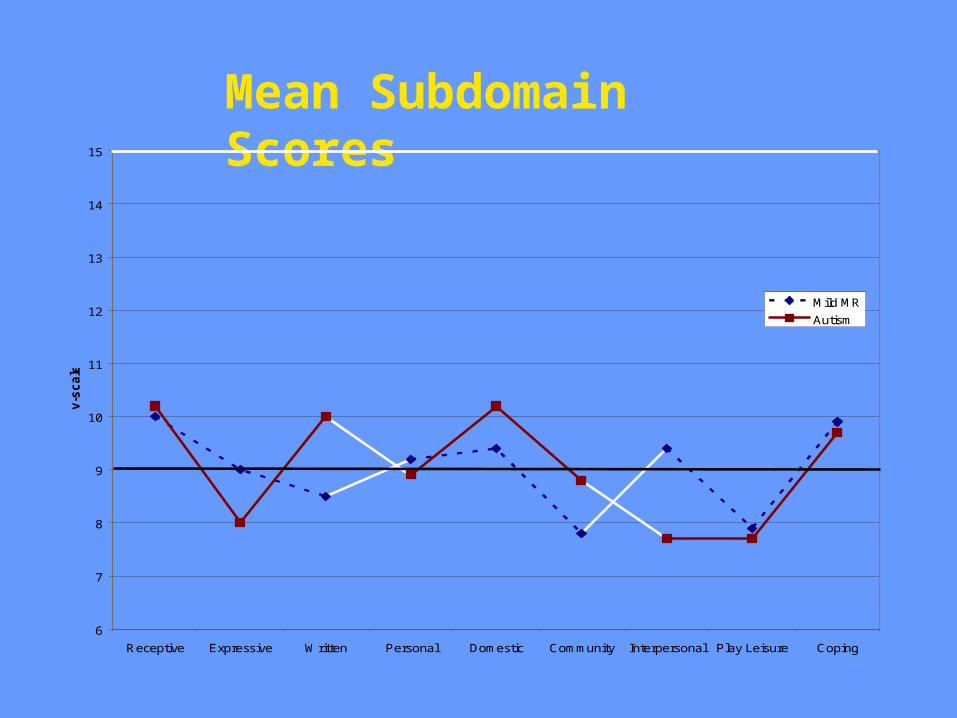
Receptive Expressive Written Personal Domestic Community Interpersonal Play Leisure Coping
v-s
ca
le
Mild MR
Autism
Mean Subdomain Scores

6
7
8
9
10
11
12
13
14
15
Receptive Expressive Written Personal Domestic Community Interpersonal Play Leisure Coping
v-s
ca
le
Autism
Mod MR
Mean Subdomain Scores
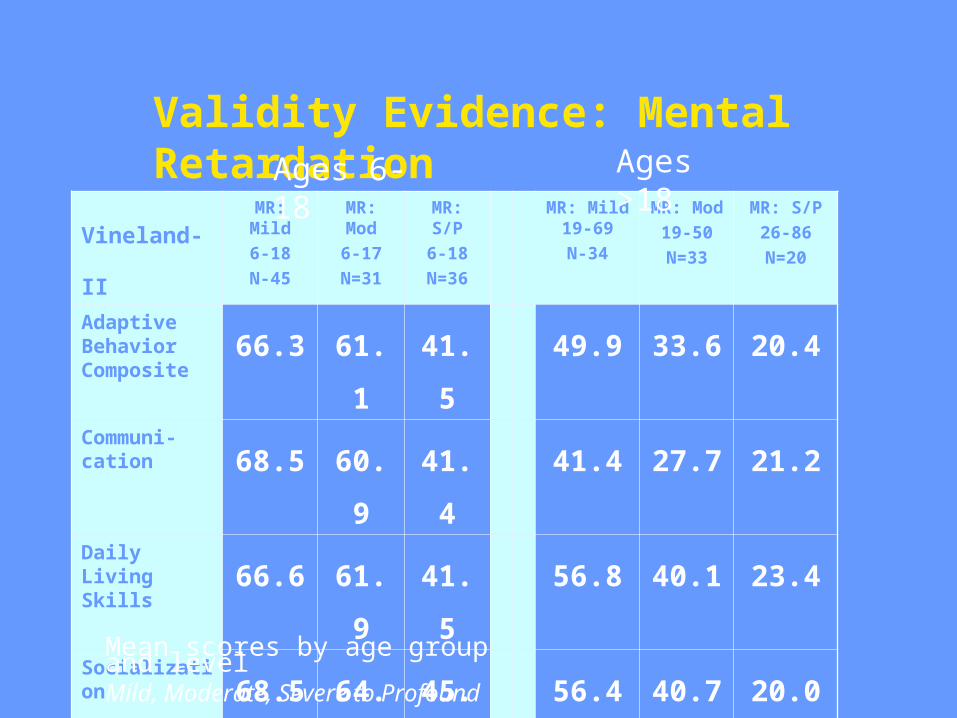
Validity Evidence: Mental Retardation
Vineland-IIMR: Mild
6-18
N-45
MR: Mod
6-17
N=31
MR: S/P
6-18
N=36
MR: Mild 19-69
N-34
MR: Mod
19-50
N=33
MR: S/P
26-86
N=20
Adaptive Behavior Composite
66.3 61.1 41.5 49.9 33.6 20.4
Communi-cation 68.5 60.9 41.4 41.4 27.7 21.2
Daily Living Skills 66.6 61.9 41.5 56.8 40.1 23.4
Socialization68.5 64.3 45.0 56.4 40.7 20.0
Ages 6-18 Ages >18
Mean scores by age group and levelMild, Moderate, Severe to Profound

Validity Evidence: Autism, ADHD, EBD, LD
Vineland-II
AutismVerbal3-16N=46
Autism Nonverbal
3-16
N=31
ADHD
6-18
N=55
EBD
8-17
N=34
LD
7-17
N=56
Adaptive Behavior Composite
65.7 50.7 94.1 85.7 95.3Communi-cation 68.4 47.0 92.4 87.2 91.2Daily Living Skills 67.8 52.5 99.5 92.2 98.4Socialization 64.4 51.0 94.2 82.4 98.3Motor(Ages 3-6 only) 81.2 67.4
Mean scores by age group and disability
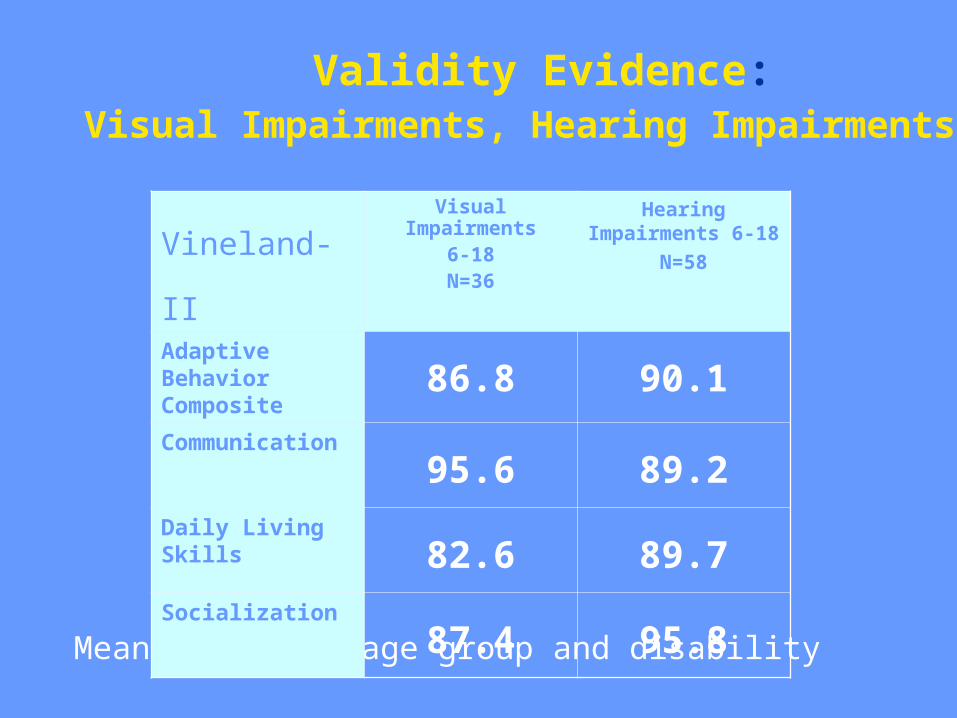
Validity Evidence:
Mean scores by age group and disability
Vineland-IIVisual Impairments
6-18N=36
Hearing Impairments 6-18
N=58
Adaptive Behavior Composite
86.8 90.1
Communication
95.6 89.2
Daily Living Skills
82.6 89.7
Socialization
87.4 95.8
Visual Impairments, Hearing Impairments

• Documented significant deficits for MR groups (at least 2 SDs below mean)
• Demonstrated expected mean score changes for mild, moderate, and severe to profound levels of mental retardation
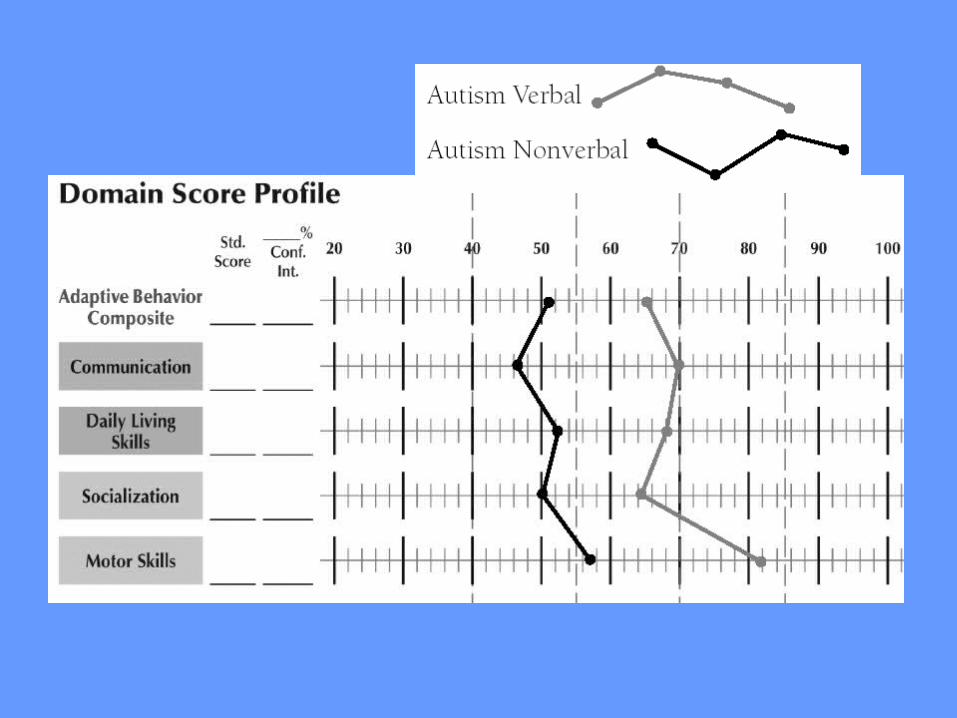
• Differentiated between Verbal and Nonverbal Autism groups
• Demonstrated distinctive profile patterns
Clinical Group Summary
Vineland-II differentiates clinical groups from nonclinical groups.

• Vineland Adaptive Behavior Scales• Adaptive Behavior Assessment
System (ABAS)• WISC III• WAIS-III• BASC-2
Validity Evidence: Criterion

Vineland-II and Vineland ABS
Ages 0-2N=25
Ages 3-6
N=29
Ages 7-
18N=70
Adaptive Behavior Composite .87 .94 .89Communication .69 .89 .89Daily Living Skills
.76 .96 .91
Socialization .89 .95 .71Motor .93 .90Correlations corrected for restriction of range
High degree of
consistency between
forms
IMPORTANT
THERE APPEARS TO BE NO FLYNN
EFFECT

Correlations corrected for restriction of range
Vineland-II and WISC-III and WAIS-III
WISC-III FSIQ 6-16N=28
WAIS-IIIFSIQ17-68N=83
Adaptive Behavior Composite .12 .20Communication .36 .30Daily Living Skills
.25 .06
Socialization -.39 .27
Documents the distinct difference between IQ and Adaptive Behavior.
Confirms the need to assess both when making diagnostic decisions.
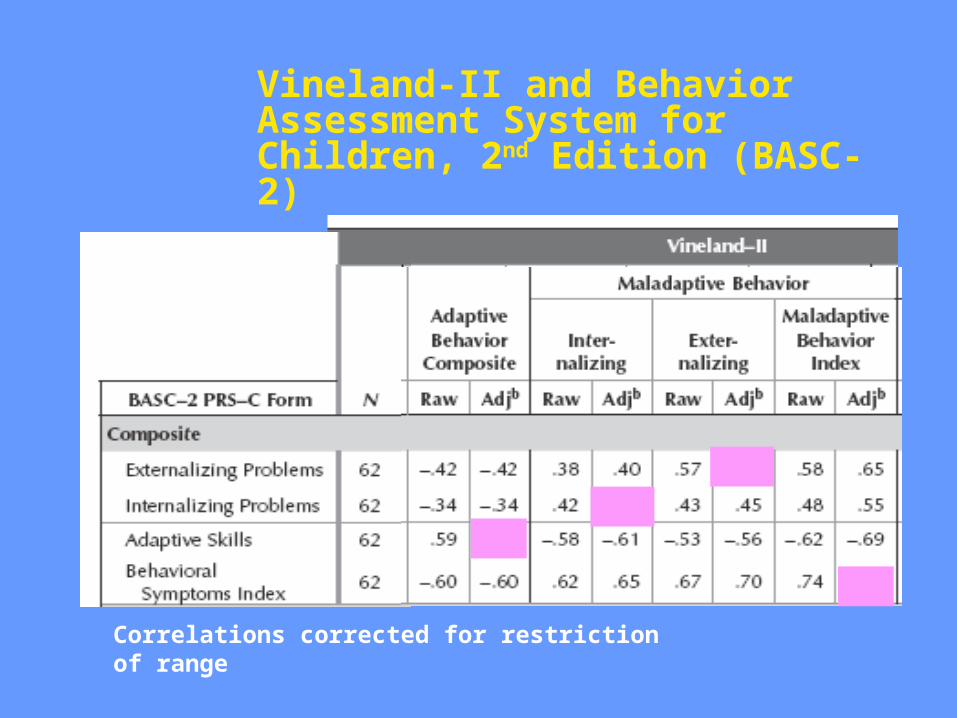
Vineland-II and Behavior Assessment System for Children, 2nd Edition (BASC-2)
Ages 6-11
Correlations corrected for restriction of range
Conclusions
• Much is the same but much is better!ManualCriteriaCase studies
Summer 2006• Teacher checklist Winter 2006• Expanded Form

Adaptive Profiles from Research Studies
Since 1984 over 1400 studies have been published investigating adaptive functioning in the following groups:
Mental retardation Autism SpectrumClosed Head Injury Hearing ImpairedHomeless HIVLearning disability GiftedEmotionally Disturbed Spina BifidaTourette Syndrome Conduct DisorderCocain Exposed Low BirthweightChildren exposed to Violence ETC.!

Groups with Mental Retardation Non Specific MRAll levels of MRGenetic Forms of MR
Fragile XDown Syndrome Praeder WilliWilliam Syndrome
Special Olympics
Groups on the Autism Spectrum
PDD NOS
Asperger Syndrome
High functioning Autism
Low functioning Autism
Multiplex
Nonverbal Learning Disability (?)
Atypical and Normally DevelopingChildren
Sparrow, S.S. Rescorla, L.A., Provence, S., Condon, S.O., Goudreau, D., Cicchetti, D.V., (1986). Follow-up of “atypical” children Journal of American Academy of Child Psychiatry. 25, 2:181-185.

Atypical and NormallyDeveloping
ChildrenGroup AGE FIQ VIQ PIQ
Atypical
Development 10.1 110 111 108
Normally
Developing 10.4 112 111 112
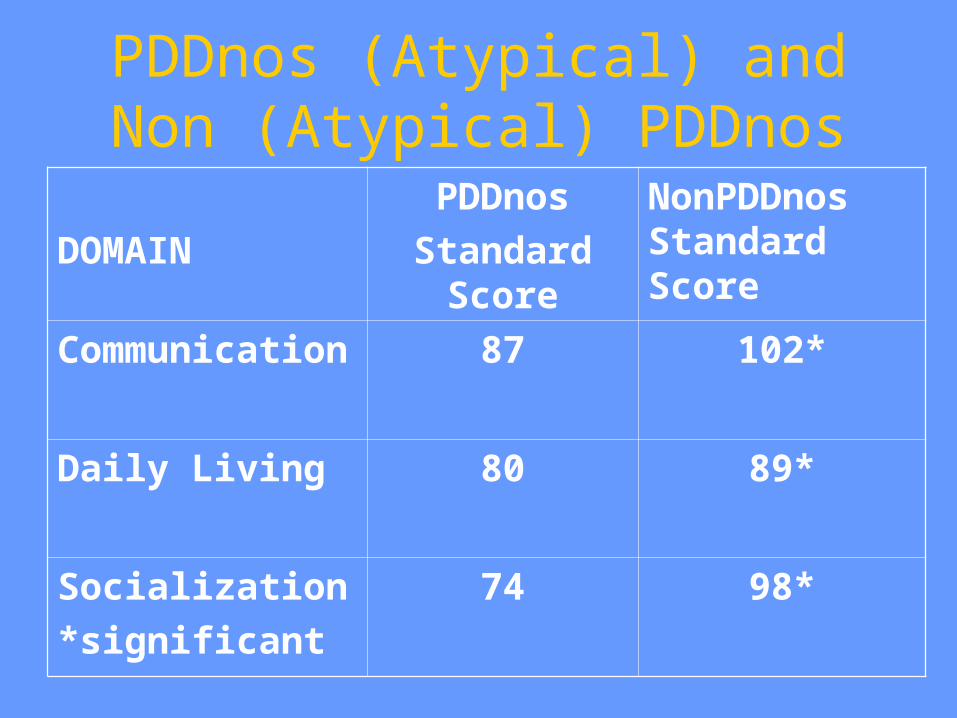
PDDnos (Atypical) and Non (Atypical) PDDnos
DOMAIN
PDDnos
Standard Score
NonPDDnos Standard Score
Communication 87 102*
Daily Living 80 89*
Socialization
*significant
74 98*

Social Deficits In Autism
Volkmar, F.R., Sparrow, S.S., Goudreau, D., Cicchetti, D.V., Paul, R., Cohen, D.J., (1987) Social deficits in autism: An operational approach using the Vineland Adaptive Behavior Scales. Journal of the American Academy of Child and Adolescent Psychiatry. 26,
2:156-161.
AUTISM
• Carter,A. S., Volkmar,F. R., Sparrow,S. S., Wang,J. J., Lord,C., Dawson,G., Fombonne,E., Loveland,K., Mesibov,G., Schopler,E., (1998),The Vineland Adaptive Behavior Scales - Supplementary Norms for Individuals with Autism, Journal of Autism & Developmental Disorders, 28:4, pp. 287-302.

AUTISM AND ASPERGER
Dissanayake,Cheryl, Macintosh,Kathleen, (2003), Mind reading and social functioning in children with autistic disorder and Asperger's disorder. Pp 213-239
Individual differences in theory of mind: Implications for typical and atypical development. Repacholi,Betty, Slaughter,Virginia (Editors), Macquarie Monographs in Cognitive Science, Psychology Press, New York, NY.
Subject Characteristics
Age and IQ matched children with mental retardation without and with autism
Mean age 11.8Mean IQ 54Vineland scores were so low we had to
use age equivalents/mental age ratiosThus, if Adaptive Behavior was
consistent with MA, Score should benear 100.

SOCIAL DEFICITS IN AUTISM
DOMAIN AUTISTIC
ABDomain/MA
NONAUTISTIC ABDomain/MA
Communication 66 81*
Daily Living 97 95
Socialization
*significant
39 70*

SOCIAL DEFICITS IN AUTISM
Communication
SUBDOMAIN
AUTISTIC
Age Equivalent
NONAUTISTIC Age Equivalent
Receptive 3.2 3.5*
Expressive 2.9 4.4*
Written
*significant
4.4 5.1
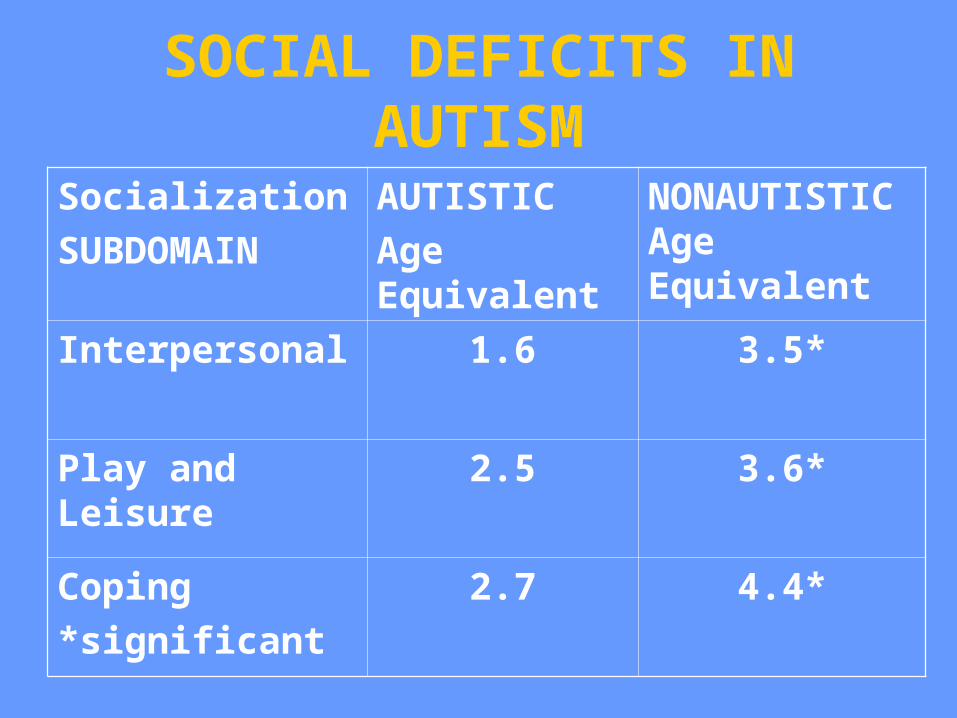
SOCIAL DEFICITS IN AUTISM
Socialization
SUBDOMAIN
AUTISTIC
Age Equivalent
NONAUTISTIC Age Equivalent
Interpersonal 1.6 3.5*
Play and Leisure 2.5 3.6*
Coping
*significant
2.7 4.4*

Other Populations
Precocious readers (not hyperlexic)
IQs: 121 to 122
Ages: 3-2 to 4-9
Asperger and high functioning autism

• Ami Klin
• Fred R. Volkmar
• Celine Saulnier
• Kathy Lord
• Domenic V. Cicchetti•All the participating families from the Yale Child Study Center and the Autism and Communication Disorders Center at the University of Michigan
• NICHD grant 5-PO1-HD03008
Special Thanks

• Autism symptoms have a severe impact on a person’s ability to meet the demands of everyday life
• Extreme variability in symptomatology and cognitive ability affects daily functioning
• “Higher-functioning” individuals, despite potential, fail to translate their skills to real-life adaptation
Recent Research in ASD

• Increasing focus on early diagnosis & intensive intervention = progress
• Still enormous variability in outcome– 12% achieving “very good outcome”
– 60% with “poor” or “very poor outcome” (Howlin, Goode, Hutton, & Rutter, 2004)
• Cognitive & language measures
• Does higher cognitive ability = greater outcome in adulthood???
• Translating potential into real-life skills becomes critical – Adaptive Behavior
Outcome in ASD
• “Real-life” Skills
• Vineland Adaptive Behavior Scales (Sparrow, Balla, & Cicchetti, 1984)
– Communication Daily Living Skills
– Socialization Motor
• Communication & Socialization skills = central & defining features
• Deficits in adaptive skills fall below cognitive ability across the spectrum– Significant deficits in socialization
– Intermediate deficits in communication(Bolte & Pustka, 2002; Carter et al., 1998)
Adaptive Functioning in Autism

Adaptive Communication

Adaptive Social Skills
• Consistent findings: – Adaptive impairments exist beyond MR– No entitlement for services without MR
• Inconsistent findings:(Freeman, Del’Homme, Guthrie, & Zhang, 1999; Liss et al., 2001; Schatz & Hamden-Allen, 1995; Szatmari, Bryson, Boyle, Streiner, & Duku, 2003)
– Positive relationship• e.g., Vineland Communication & VIQ• Early language and nonverbal IQ predicting
outcome for both comm. & socialization skills
– Negative relationship
Relationship between IQ and Adaptive Functioning
•Equally unclear relationship:
– Stable relationship
(e.g., Schatz & Hamden-Allen, 1995)
– Increase in AF w/ age
(e.g. Freeman et al., 1999)
– Decrease in AF w/ age
(e.g. Szatmari et al., 2003)
Relationship between Age and Adaptive Functioning

• Varying measures to assess severity of autism symptoms–Autism Behavior Checklist
–Childhood Autism Rating Scale
–Autism Diagnostic Observation Schedule
• Other factors (e.g., adaptive behavior and language) appear to be stronger predictors of outcome than severity of symptoms
• Very little research on relationship between symptomatology and adaptive behavior
Autism Symptomatology

• Cognitive potential may or may not play a role in positive outcomes
• Severity of autism symptoms may or may not play a role in positive outcomes
• Early detection and intensive intervention are beneficial to some, but not all, individuals on the spectrum
• “Real-life” skills are important for outcome– adaptive communication & social skills
Many Unanswered Questions

• Examines relationship between adaptive behavior (ability) and severity of symptoms (disability)– Vineland Adaptive Behavior Scales
– Autism Diagnostic Observation Schedule
• Investigates nature of ability & disability in relation to:
– Age
– IQ
– Diagnostic Classification
Present Study

Total Sample• 187 males with a diagnosis of an ASD• Diagnosis based on ADI, ADOS, & clinical
judgment of 2 licensed clinicians • Verbal IQ > 70• Age range from 7 to 18 years
Yale Site• N = 84
– Autism=32; Asperger’s=35; PDD-NOS=17
Michigan Site• N = 103
– Autism=31; Asperger’s=1; PDD-NOS=66
Participants
• Autism Diagnostic Observation Schedule
(Lord, Rutter, DiLavore, & Risi, 1999)
• Vineland Adaptive Behavior Scales (Sparrow, Balla, & Cicchetti, 1984)
• Intelligence Scales
– Yale: Wechsler scales: WISC-III, WAIS-R (The Psychological Corporation)
– Michigan: Mix of Wechsler scales, Differential Ability Scales, & Stanford-Binet
Measures

Characterization by SiteYale(n=84)
Mean (SD)Michigan(n=103)Mean (SD)
Age 12.4 (2.9) 10.0 (2.4)IQ
Full Scale Verbal Performance
99.8 (20.6)104.7 (21.3) 94.5 (19.7)
99.0 (17.1) 101.2 (18.3) 98.5 (18.9)
Vineland*
Communication Socialization
72.2 (17.1) 52.0 (11.5)
83.5 (20.0) 67.0 (15.4)
ADOS**
Communication Social
4.0 (1.5) 9.5 (2.6)
3.2 (1.7) 6.5 (3.0)
Note. ADOS Commun. scores range 0-8 & Social scores 0-14*For Vineland scores, higher numbers indicate greater ability**For ADOS scores, higher numbers indicate greater disability

Real-life (adaptive functioning) in higher functioning individuals with autism and
PDDs
• N=187• Autism, AS, and PDD-NOS• Socialization (Vineland): Mean 52 Yale
(SD 12.6)• Interpersonal Age Equivalent: Yale
Mean 3.6 years (SD 1.7 years)
From Klin, Saulnier, Sparrow, Cicchetti, Lord & Volkmar (submitted)

Real-life (adaptive functioning) in higher functioning individuals with autism and
PDDs
• Social ability and disability: two relatively dissociated domains (correlation)!!!!!!!
• Social disability is not correlated with age (stable)• Social ability is negatively correlated with age (decline
relative to peers, relative to increasing demands of the environment)
• Most programs emphasize reduction of symptoms
• Conclusion: all programs should prioritize adaptive functioning (REAL-LIFE SKILLS)
From Klin, Saulnier, Sparrow, Cicchetti, & Volkmar (submitted)

High Functioning ASD

Prototypical Comparative Profiles
Based on our work and those of many others
These are group data and some affected individuals may not demonstrate the prototypical profiles

ASPERGER AND AUTISM
• Szatmari,Peter; Archer,Lynda; Fisman,Sandra; Streiner,David L. (1995), Asperger's syndrome and autism: Differences in behavior, cognition, and adaptive functioningJournal of the American Academy of Child & Adolescent Psychiatry, Dec. 34:12, pp.1662-1671.

ASPERGER AND AUTISM
Klin, A., Volkmar, F.R., Sparrow, S.S., Cicchetti, D.V., and Rourke, B.P.
(1995). Validity and Neuropsychological Characterization of Asperger
Syndrome. Journal of Child Psychology and Psychiatry. 36:1127-1140.
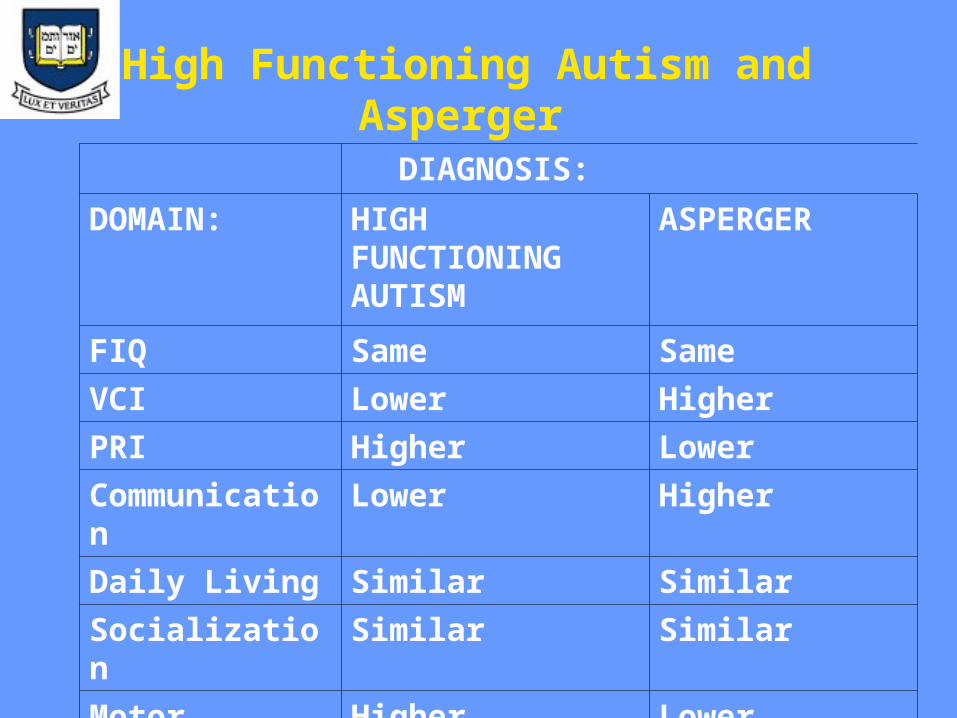
High Functioning Autism and Asperger
DIAGNOSIS:
DOMAIN: HIGH FUNCTIONING AUTISM
ASPERGER
FIQ Same Same
VCI Lower Higher
PRI Higher Lower
Communication Lower Higher
Daily Living Similar Similar
Socialization Similar Similar
Motor Higher Lower

ADHD
Roizen,N. J., Blondis,T. A., Irwin,M., Stein,M.(1994) Adaptive functioning in children with attention-deficit hyperactivity disorder, Archives of Pediatrics & Adolescent Medicine Nov,148:11, pp 1137-1142.

ADHD, ADD
• Stein,Mark A., Szumowski,Emily, Blondis,Thomas A. (1995) Adaptive skills dysfunction in ADD and ADHD children, The Journal of Child Psychology and Psychiatry and Allied Disciplines, May, pp.36, 663-670.

DOMAIN DIAGNOSISNORMAL ADHD
I.Q. Same Same
Communication Higher Lower
Daily Living Higher Lower
Socialization Higher Lower
Motor Similar Similar
Cognitive and Adaptive Profiles of Normally developing
children and ADHD
DOWN-SYNDROME
Dykens,E. M.,Hodapp,R. M., Evans,D. W.(1994)
Profiles and Development of Adaptive Behavior in Children with Down-Syndrome,
American Journal of Mental Retardation, March, 98:5, pp. 580- 587

Cognitive and Adaptive Profilesof
Nonspecific MR and Down syndrome
DIAGNOSIS
DOMAIN NON -SPECIFIC MR
DOWN SYNDROME
I.Q. Same Same
Communication Higher Lower
Daily Living Similar Similar
Socialization Lower Higher
Motor Higher Lower
DOWN-SYNDROME
Burack,J. A.; Shulman,C.; Katzir,E.; Schaap,T.; Brennan,J. M.; Iarocci,G.; Wilansky,P.; Amir,N.(1999) Cognitive and behavioural development of Israeli males with fragile X and Down Syndrome International Journal of Behavioral Development, JUNE, 23:2, pp. 519-531

• Cicchetti,Domenic V., Sparrow,Sara S.(1990)Assessment of adaptive behavior in young children, pp173-196, Johnson,James H., Goldman, Jacquelin, Developmental assessment in clinical child psychology: A handbook. Pergamon general psychology series, 163 Pergamon Press, Inc, Elmsford, NY.
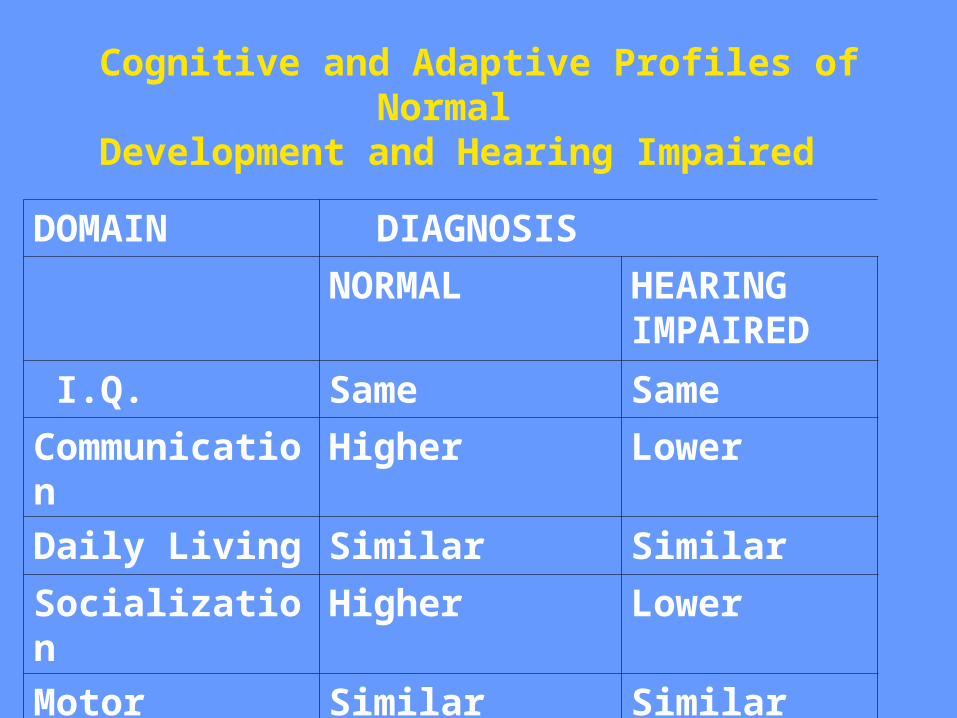
Cognitive and Adaptive Profiles of Normal Development and Hearing Impaired
DOMAIN DIAGNOSIS
NORMAL HEARING IMPAIRED
I.Q. Same Same
Communication Higher Lower
Daily Living Similar Similar
Socialization Higher Lower
Motor Similar Similar
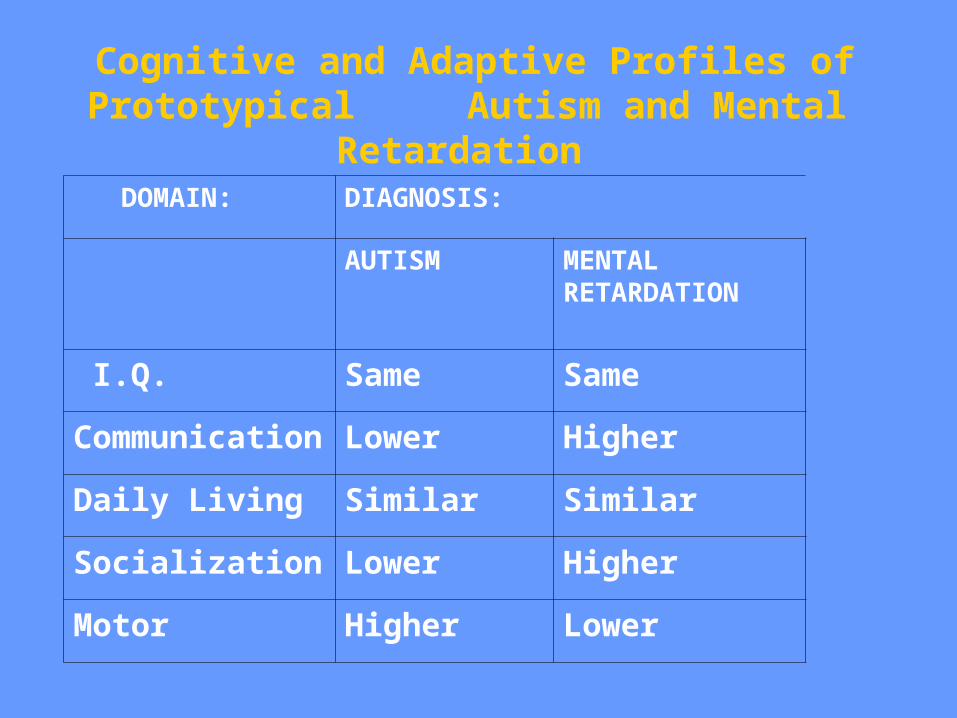
Cognitive and Adaptive Profiles of Prototypical Autism and Mental Retardation
DOMAIN: DIAGNOSIS:
AUTISM MENTAL RETARDATION
I.Q. Same Same
Communication Lower Higher
Daily Living Similar Similar
Socialization Lower Higher
Motor Higher Lower

ConclusionsAssessment of Adaptive functioning is important
for individuals within any diagnostic categoryDetermining how everyday life (adaptive
functioning) is affected by nature or nurture (or both) should be our goal
Research and clinical work has shown us how different profiles are found in different groups
Aside:(Program planning and assessment of change after intervention are other goals of adaptive behavior assessment)