prof. susan kurrle - university of sydney - clinical practice guidelines for dementia in australia
TRANSCRIPT

ClinicalPracticeGuidelinesforDementiainAustralia
BrisbaneMarch21st 2016
sydney.edu.au/medicine/cdpc/
SusanKurrle
Geriatrician,HornsbyKu-ring-gaiandEurobodallaHealthServicesDirector,NHMRCCognitiveDeclinePartnershipCentre
CurranProfessorinHealthCareofOlderPeopleFacultyofMedicine,UniversityofSydney
WhoistheNHMRCCDPC?• PartnershipbetweenNHMRC,DepartmentofHealth,Alzheimer’sAustralia,and3agedcareproviders(BrightwaterCareWA,HammondCareNSWandVic,andHelpingHandSA)
• Partnersdriveresearchagendawhichiscarriedoutbyateamofresearchandsystembasedinvestigators(cliniciansandagedcareproviders)
• Stronginputfromconsumersfrominitiationtocompletionofprojects
• $25millionfundingover5years• FundingbeganinFeb2014
WhoistheCDPC?• Investigatorteamisamixtureofclinicians,researchers,consumers,andagedcareprovidersandpractitioners
• Investigatorsinclude:– Medicine,nursing,physiotherapy,psychology,occupationaltherapy,pharmacy,socialwork
– Law,sociology,healtheconomics,changemanagement• Consumersincludepeoplewithdementiaandcarers ofpeoplewithdementia,whoaremembersofAlzheimer’sAustraliaConsumerDementiaResearchNetwork
• Theteamcovers5states,10universities,otherinstitutions(eg RDNS,SouthernNSWLHD,NSWACI)and15professions,andincludesurbanandruralsites
NHMRCCDPC• ObjectivesofPartnershipCentre:– Implementationofcurrentknowledge– Synthesisanddisseminationofcurrentresearch– Collaborativeresearch– Capacitybuilding
• MajorfocusofPartnershipCentreisonknowledgetranslationie knowingtodoing
• ProjectsforCentrearedevelopedtogether byPartnersandInvestigatorteammembers
• End-user/Consumerinvolvementseenasessentialfromthebeginningoftheprocess
CognitiveDeclinePartnershipCentre(CDPC)
• Aimistoimprovethelivesofpeoplelivingwithdementia,andtodevelopandcommunicateresearchtoimprovethecareofpeoplewithdementia
• Focusisparticularlyonthe“care”areaofcognitiveandassociatedfunctionaldecline
• Onewaytoachievethatisthroughthedevelopmentanddisseminationofbestpracticeguidelinesforthemanagementofpeoplewithdementia

Whydoguidelines?
• Therewerenone• Dementiaiscommon(9%overage65,25%overage80)
• DementiaisaNationalHealthPriority• Dementiaisthe2nd highestcauseofdeath• ClinicalPracticeGuidelineshavebeenshowntoimprovequalityandconsistencyofcareforarangeofconditions
Whyaretheseguidelinesimportant?
• DementiaisnotmanagedconsistentlywellinAustralia,thereislotsofroomforimprovement,andtheseguidelinesoutlinehowthatcanbedone.
• Consumershavehadextensiveinvolvementintheirdevelopmentandtheircontributionhasbeenincrediblyvaluable
• HavingGuidelinesgivesdementia“clinicallegitimacy”

Howdidwedoit?• Wetookexistinginternationalguidelines(fromNICEintheUK)andusedtheADAPTEprocesstomodifyandadaptthemtoAustralianconditions
WhatistheADAPTEprocess?• Systematicapproachtotheadaptingofguidelinesdevelopedinonesettingforuseinadifferentsetting
• ToolkitdevelopedbyagroupofcollaboratorsinCanadaandEuropetopromotetheuseofclinicalpracticeguidelinesthroughtheadaptationofexistingguidelines

Howdidwedoit?• AspartoftheADAPTEprocess,weconductedaseriesofmini-systematicreviewsaroundeachrecommendationtoensureevidencewasuptodate(wheretherewasevidenceavailable)
• UsedtheGRADEapproach(GradingofRecommendations,Assessment,DevelopmentandEvaluation)whichprovidesasystemforrating thequalityofevidence,andstrengthofrecommendation,foreachindividualoutcome(asusedbyCochraneCollaboration)

Howdidwedoit?• FormedaconsultativeGuidelineAdaptationCommitteeof21people:consumers,representativesfromATSI andCALDcommunities,clinicians,andresearchersinthedementiafield
• providedregularconsultationandcommentsviaemailoneachrecommendation,with3facetofacemeetingsforfinalconsensus
• ClassifiedeachrecommendationaccordingtoNHMRCStandardsasEBR,CBRorPP
• ClassifiedeachEBRaccordingtoGRADE
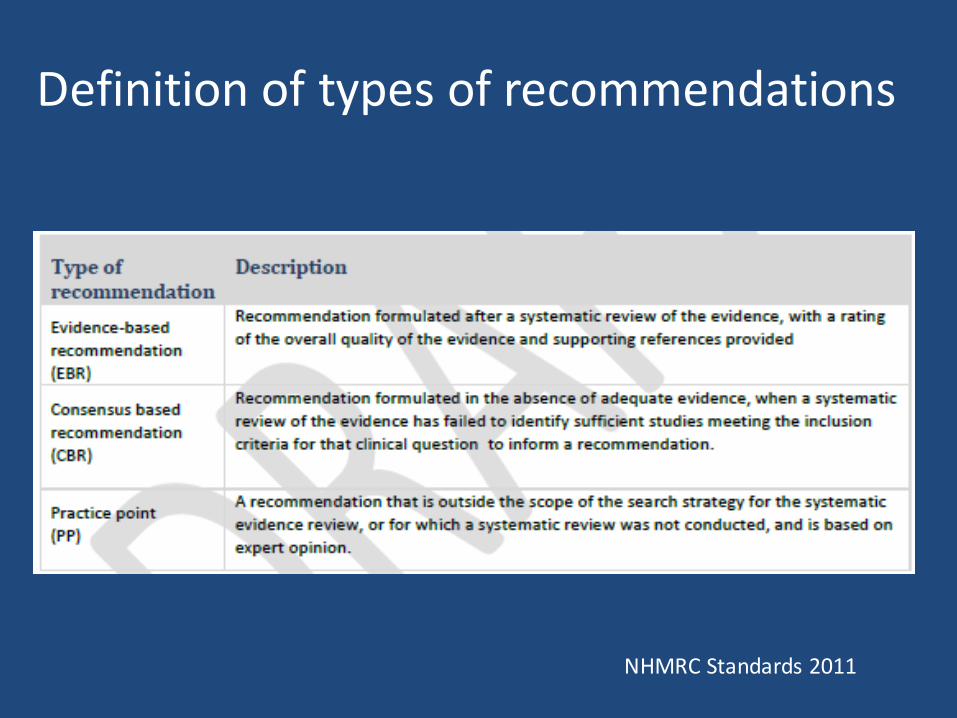
Definitionoftypesofrecommendations
NHMRCStandards2011

DefinitionofGRADEratings
GRADEWorkingGroup2013

Howdidwedoit?• Guidelineswereputoutforpublicconsultationandreviewfor45daysin2015,andreceived70submissions.Somemodificationsweremadeasaresult
• FinalversionwasapprovedinFebruary2016bytheNHMRCCouncil
• Finalversioncontains109 recommendationswith29 evidencebasedrecommendations

Howdidwedoit?
• TheGuidelineswereofficiallylaunchedbytheMinisterofHealthLeyonMarch16th 2016

WebaddressforGuidelines

Examplesofrecommendations:Barriers,screening
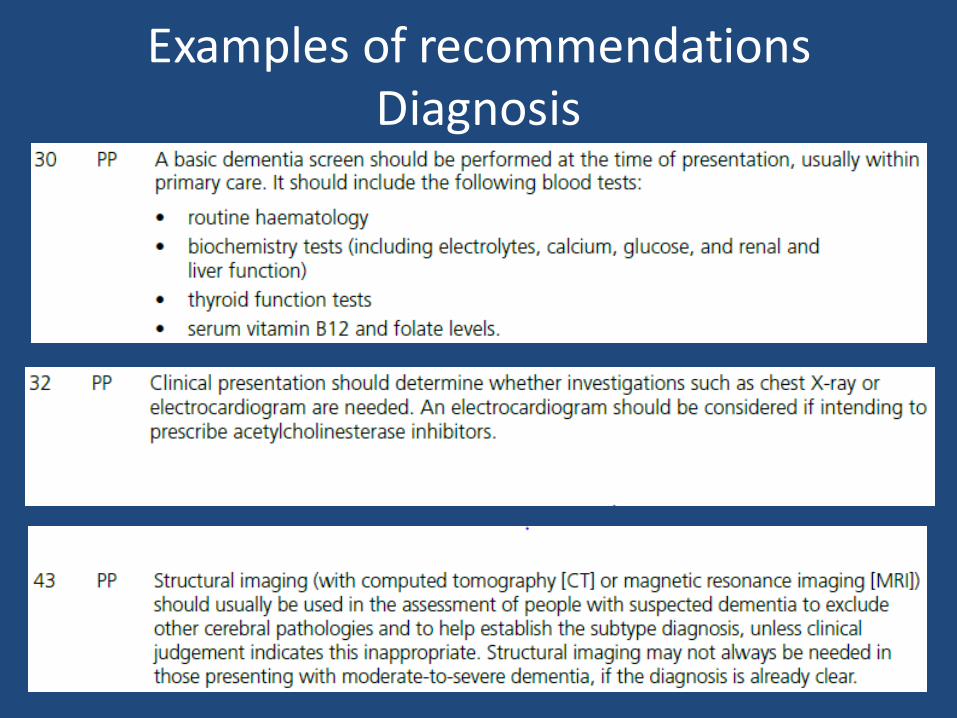
ExamplesofrecommendationsDiagnosis

Examplesofrecommendations:Treatment
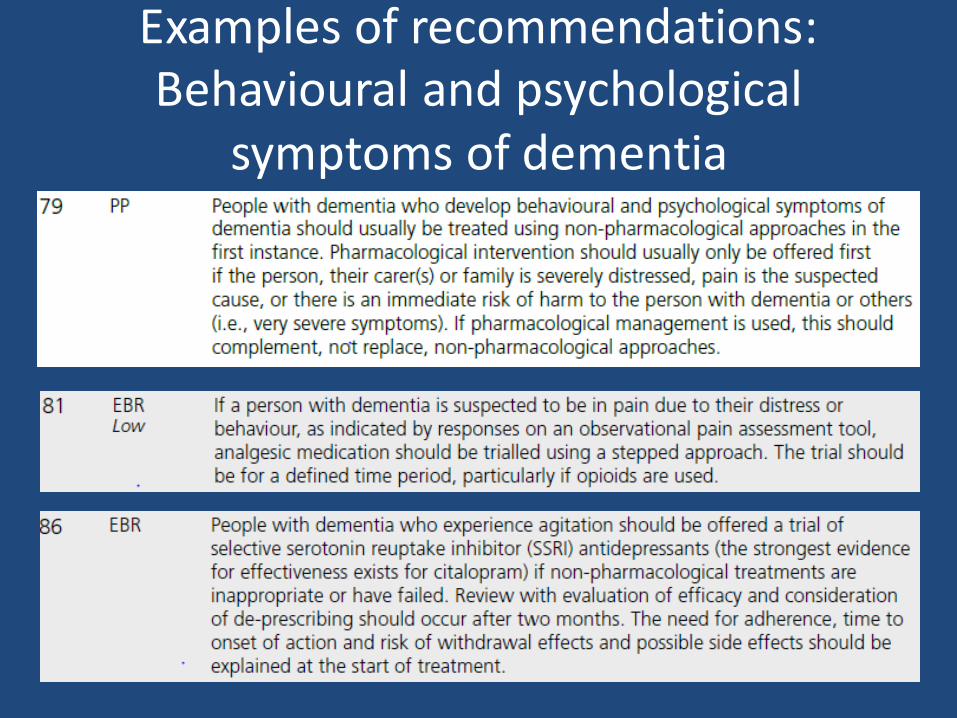
Examplesofrecommendations:Behavioural andpsychological
symptomsofdementia
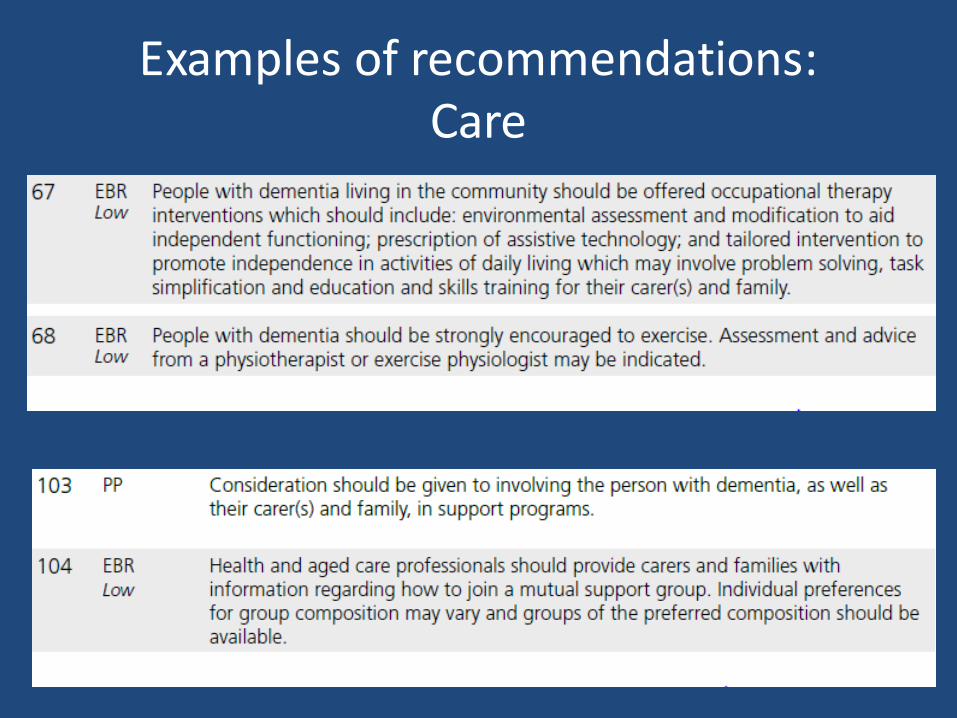
Examplesofrecommendations:Care

HowwilltheGuidelinesimprovecare?
• Timelydiagnosis– Memorylossisnotanormalpartofageing– Peopleleavethediagnosistoolate– Providesasystematicapproachonhowtomakethediagnosisandwhattreatmentsareavailable
• Addressinglegalissues– Organise affairs– POAetc
• ManagementofBPSD– Morethan20recommendations– Avoiduseofantipsychotics
Prioritiesforfurtherresearch• Earlyidentification– doesitresultinimprovedoutcomes?
• Memoryassessmentservices– aretherebenefits,whatisoptimalconfiguration?
• Cognitiveassessmenttools– whatisbeingusedandaretheyappropriate?
• Communicatingthediagnosis– isthereanoptimalwaytodothis?
• Organisation ofservices– whatismosteffectiveandefficientway?
Prioritiesforfurtherresearch• Respitecare– flexibleandinnovativeformsofrespiteandtheireffectonthepersonwithdementiaandtheircarer
• RoleofGPandhowtheyinteractwithotherservices
• Physicalandcognitiverehabilitation– when,whatandhowmuch?
• Driving– howtosupportpeoplewithdementiatokeepdrivingifable,andhowtoencouragecessation
• Consentandcapacityassessmentfornondementiaspecialists
Prioritiesforimplementation• Referraltomemoryservices• Communicatingthediagnosis• Organisation ofcare• Trainingforstaffandstudents• Promotingfunctionalindependence• BPSD• Reducingoverprescriptionofantipsychotics• Supportforcarers
Reflectionsondevelopingaguideline• Howdoyousynthesise evidencewhenthereoftenisn’tany?– Manypracticepoints,fewevidencebasedrecommendations
• Howdoyouincluderepresentativesfromeveryprofessionalandcaregroup?– Youcan’t,beasinclusiveaspossible
• Howdoyoucounterentrenchedviewsfromprofessionals?– Muchconsultationanddiscussion,majorityrules
• Howdoyoucounterconflictsofinterest?– Excludethemfromdiscussiononthatrecommendation
QUESTIONS?