primary cns lymphoma (pcnsl) what is the optimal...
TRANSCRIPT

Primary CNS Lymphoma (PCNSL)
What is the optimal treatment?
Dr Kate Cwynarski
Consultant Haematologist
UCLH
LONDON

Outline: PCNSL
●Induction
–Chemoimmunotherapy
●Consolidation
–PBSCT
–WBRT
●Relapsed disease
–Chemotherapy
–Non-chemotherapy
–Immunotherapy

PCSNL is rare but incidence is increasing
● Represents approx 2-4% extra-nodal NHL
5% Primary CNS tumours
● Incidence about 1 / 100 000 / year
About 60% of patients > 60 years at diagnosis
Makino et al, Surg Neurol 2006; Olson et al, Cancer 2002; Panageas et al, Cancer 2007

Primary CNS Lymphoma (PCNSL)
Aggressive lymphoma entity with a unique
localisation
Drug delivery to CNS
Surrounding brain tissue is highly vulnerable

The Blood Brain Barrier
Mechanisms That Prevent
Drug Delivery To The CNS
1. Plasma protein binding
2. Endothelial tight junctions
3. Active drug efflux
Factors Influencing BBB
Penetration
1. Plasma concentration
2. Lipid solubility
3. Hydrostatic pressure
within tumour
4. Route of administration
(IV vs IA)
5. Disruption of BBB
6. Drug metabolism

Prognosis In PCNSL
● IELSG Score
– Age >60
– ECOG >0
– Elevated LDH
– Elevated CSF protein
– Deep brain lesions
● MSKCC Score
– Age >50
– KPS <70

Therapy Of PCNSL
● High dose methotrexate
● Cytarabine
● Ifosfamide
● Temozolamide
● Thiotepa
● Rituximab
● Whole Brain Radiotherapy
● Conventional Chemotherapy
● High Dose Therapy + Auto-SCT
Induction Consolidation

●
PCNSL [≤ 65 ys. + PS 0-3] or [65-70 ys. + PS ≤2]
®
® WBRT 36 Gy
± boost 9 Gy
BCNU 400 mg/m2 d.1
Thiotepa 5 mg/Kg x 2/d; d.2-3
+ APBSCT www.ielsg.org
4 c. MTX 3.5 g/m2 d.1
araC 2 g/m2 x 2/d, d. 2-3
every 3 weeks
ARM A
4 c. rituximab 375 mg/m2 d-5 & 0
MTX 3.5 g/m2 d.1
araC 2 g/m2 x 2/d, d. 2-3
every 3 weeks ARM B
4 c. rituximab 375 mg/m2 d-5 & 0
MTX 3.5 g/m2 d.1
araC 2 g/m2 x 2/d, d. 2-3
Thiotepa 30 mg/m2 d.4
every 3 weeks ARM C
Response assessment after 2° & 4° courses and after consolidation
CR – PR - SD PD – tox
SC harvest
WBRT 40 Gy
± boost 9 Gy
IELSG-32

Feasibility and Toxicity
A (n= 75) B (n= 69) C (n= 75) p
Actually delivered courses 223 (74%) 236 (86%) 274 (91%)
RDI Methotrexate 92% 84% 85% NS
RDI Cytarabine 87% 81% 80% NS
RDI Rituximab - 82% 83% NS
RDI Thiotepa - - 76% -
G4 neutropenia 99 (44%) 119 (50%) 153 (56%) 0.01
G4 thrombocytopenia 116 (52%) 140 (59%) 200 (73%) 0.0001
G4 anemia 9 ( 4%) 6 ( 3%) 14 ( 5%) NS
G≥3 febrile neutrop./infections 43 (19%) 31 (13%) 45 (16%) NS
G4 hepatotoxicity 6 ( 3%) 3 ( 1%) 1 ( 1%) NS
G4 nephrotoxicity 0 ( 0%) 0 ( 0%) 1 ( 1%) NS
Interruptions x toxicity (/pts) 9 (12%) 5 ( 7%) 4 ( 5%) NS
Toxic deaths (/ pts) 7 ( 9%) 3 ( 4%) 3 ( 4%) NS
Autologous stem cell collection 48/51 (94%) 44/46 (96%) 60/64 (94%) NS
Median APBSC (x 106 c/kg bw) 12.3 15 8.2 NS

MATRix: Efficacy
0 12 24 36 48 60
Months
0,0
0,2
0,4
0,6
0,8
1,0
Pro
babili
ty,
PF
S
Arm A
Arm B
Arm C
A
A vs. B= 0·06, HR= 0·68, 95%CI=0·45 - 1·02
A vs. C= 0·0001, HR= 0·66, 95%CI=0·53 - 0·81
B vs. C= 0·049, HR= 0·63, 95%CI=0·40 - 0·99
0 12 24 36 48 60
Months
0,0
0,2
0,4
0,6
0,8
1,0
Pro
babili
ty,
OS
Arm A
Arm B
Arm C
B
A vs. B= 0·14, HR= 0·73, 95%CI=0·48 - 1·11
A vs. C= 0·0004, HR= 0·65, 95%CI=0·52 - 0·83
B vs. C= 0·02, HR= 0·57, 95%CI=0·35 - 0·93
Ferreri, Cwynarski, Pulczynski et al, Lancet Haematology 2016
Median follow up 40 (19-76) months

Therapy Of PCNSL
● High dose methotrexate
● Cytarabine
● Ifosfamide
● Temozolamide
● Thiotepa
● Rituximab
● Whole Brain Radiotherapy
● Conventional Chemotherapy
● High Dose Therapy + Autologous Stem Cell Transplant
Induction Consolidation

Neurotoxicity
● Causes
– Lymphoma
– Chemotherapy
– WBRT Post chemotherapy (even worse pre-)
● Clinical Irreversible leukoencephalopathy
● Radiological
● Neurocognitive MMSE, Neuropsychological
● Quality of life Correa 2012, Abrey 2005
The role of whole brain radiation in primary CNS lymphoma.
Kasenda B et al, Blood. 2016

●
PCNSL [≤ 65 ys. + PS 0-3] or [65-70 ys. + PS ≤2]
®
® WBRT 36 Gy
± boost 9 Gy
BCNU 400 mg/m2 d.1
Thiotepa 5 mg/Kg x 2/d; d.2-3
+ APBSCT www.ielsg.org
4 c. MTX 3.5 g/m2 d.1
araC 2 g/m2 x 2/d, d. 2-3
every 3 weeks
4 c. rituximab 375 mg/m2 d-5 & 0
MTX 3.5 g/m2 d.1
araC 2 g/m2 x 2/d, d. 2-3
every 3 weeks
4 c. rituximab 375 mg/m2 d-5 & 0
MTX 3.5 g/m2 d.1
araC 2 g/m2 x 2/d, d. 2-3
Thiotepa 30 mg/m2 d.4
every 3 weeks
Response assessment
CR – PR - SD PD – tox
SC harvest
WBRT 40 Gy
± boost 9 Gy
IELSG-32
R2:
CR vs PR/PD
A vs B vs C

EFFICACY: PFS
0 12 24 36 48 60
Months
0,0
0,2
0,4
0,6
0,8
1,0
Pro
babili
ty,
PF
S
arm D
arm E
A
p= 0.17
Randomization Primary
endpoint
P0* P1 α 1 - β Estimated
sample
Minimum N° of
progression-free
survivors at 2 ys.
2nd 2-yr PFS 65% 85% 5% 95% 52/ arm 40
ITT Arm D Arm E
First 104 pts (52/ARM) 40 (77%) 40 (77%)
0 12 24 36 48 60
Months
0,0
0,2
0,4
0,6
0,8
1,0
Pro
babili
ty,
PF
S
WBRT
ASCT
B
p= 0.62
ITT PP

EFFICACY: OS
102 (47%) pts are alive:
- 44 (75%) in arm D
- 37 (63%) in arm E
- 21 pts excluded from R2.
Causes of death Arm D Arm E Non R2
lymphoma 11 15 62
treatment toxicity 0 2 13
toxicity during salvage therapy 1 1 0
neurocognitive decline while NED 0 1 1
late infective complications 3 1 2
car accident 0 0 1
acute erythroid leukaemia 0 1 0
sudden death (> 1 yr) 0 1 0
unknown 0 0 1
ITT
PP

Progression free and overall survival:
UK Experience Auto-SCT in PCNSL
(n=78)
● Median PFS and OS not reached
PFS % OS %
1 year 86 86
2 year 76.6 82
5 year 71.8 74.5
Kassam et al, BMT 2017

Management challenges in treating
older patients
● - High proportion of elderly pts
- Poor PS at presentation
- Biopsy not performed
- Palliative treatment considered
- Therapeutic consensus is lacking

PRIMAIN Trial
Kasenda, et al. Leukemia 2016

PRIMAIN Trial - Efficacy
Kasenda et al, Leukaemia 2016

HDT And AutoSCT In Older Patients
With PCNSL?
● 50% of patients with PCNSL >65yrs
● Prognosis of older patients worse
● Ability to tolerate intensive therapy restricted
● WBRT associated with greater neurotoxicity in
older patients

HDT And AutoSCT In Older Patients
With PCNSL
Schorb et al BMT 2017
• Retrospective, multicentre
• Germany/France/UK
• Median age 68.5 (65-77)
• n=52
• KPS 80% (30-100%)
• 71% first line
• Median F/U 20/12
• Thiotepa based HDT

HDT And AutoSCT In Older Patients
With PCNSL
Schorb et al BMT 2017

0 5 10 15 20 25 30
0.0
0.2
0.4
0.6
0.8
1.0
Survival Time (Months)
Su
rviv
al p
rob
ab
ility
PFS2: 2.2 months [0-29.6]
OS2: 3.5 months [0-29.6]
Management and outcome of Primary CNS
Lymphoma at first relapse/progression: Analysis of
256 patients from the French LOC NetworkSSION
Langnier-Lemercier et al, Neuro-Oncol 2016

Prognosis of relapses/refractory PCNSL OS according to duration of first remission
LOC data base (N = 256 R/R patients)
Langnier-Lemercier et al, Neuro-Oncol 2016
0 5 10 15 20 25 30
0.0
0.2
0.4
0.6
0.8
1.0
Survival Time (Months)
Su
rviv
al p
rob
ab
ility
Relapsed patients
Refractory patients
PFS 1 ≥ 1 year
PFS 1 < 1 year
OS2= 2.1mo
OS2= 3.7mo
OS2= NR

A Phase I/II Study of Thiotepa, Ifosphamide, Etoposide
and Rituximab (TIER) for the treatment of relapsed and
refractory PCNSL
Rituximab 375mg/m2
Etoposide 250mg/m2
Ifosphamide 2g/m2
Thiotepa 20-50mg/m2
GCSF(mobilising)
q21d
0 1 2 3 5
8
GCSF
CI: Chris Fox Bloodwise TAP Study

PCNSL previously treated with a
HD-MTX-based therapy
Relapsed/refractory disease
Eligible for TIER
2 cycles of protocol
treatment
Response
assessment:
multimodal MRI
PBSC mobilisation
PD Off-
study
F/U data
≥SD 3rd cycle
TIER
Local decision re
consolidation
therapy
- Thiotepa/BCNU
HDT-ASCT
recommended

Illerhaus et al. Manuscript in prep
Relapsed PCNSL: The German Approach
(Kasenda et al, Leukemia 2017
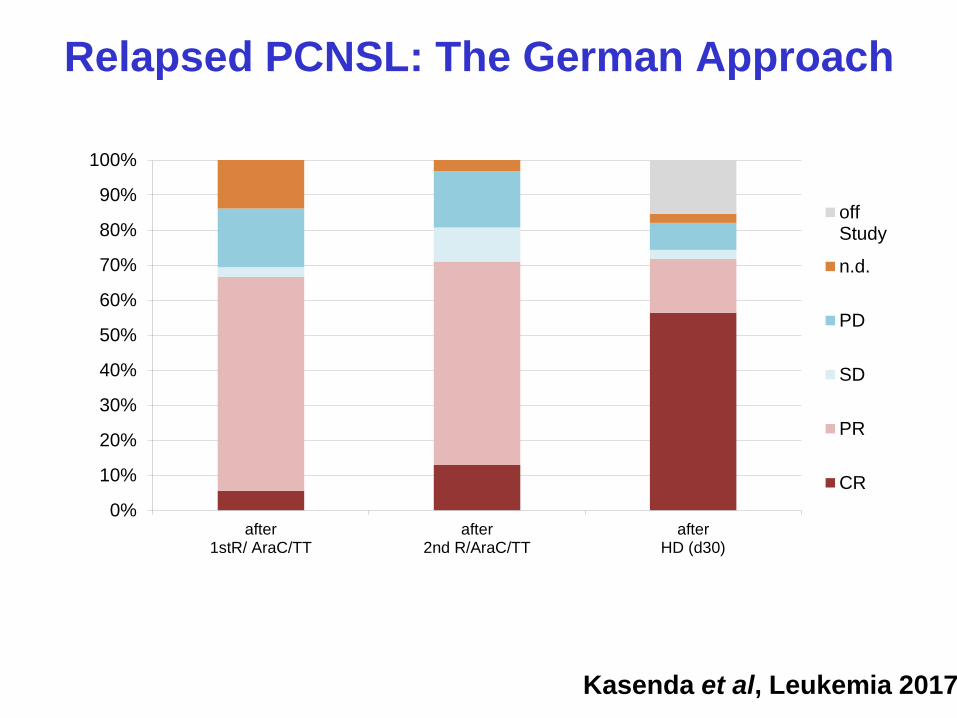
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
after1stR/ AraC/TT
after2nd R/AraC/TT
afterHD (d30)
offStudy
n.d.
PD
SD
PR
CR
Illerhaus et al. Manuscript in prep
Relapsed PCNSL: The German Approach
(Kasenda et al, Leukemia 2017

Med FU: 45.2 Mo
Med OS: n.r
3y OS: 50.9 %
50.9%
Illerhaus et al. Manuscript in prep
Relapsed PCNSL: The German Approach
(Kasenda et al, Leukemia 2017

iLOC: Ibrutinib Monotherapy in Relapse or Refractory
Primary CNS Lymphoma (PCNSL) and Primary
Vitreo-Retinal Lymphoma (PVRL). Results of the final
analysis of the primary end-point
Sylvain Choquet, Caroline Houillier, Fontanet Bijou, Roch Houot, Eileen Boyle, Remy Gressin, Emmanuelle Nicolas-Virelizier, Maryline Barrie, Cécile Moluçon-Chabrot, Marie Blonski, Abderrazak El Yamani, Marie-Laure Lelez, Aline Clavert, Solène Coisy, Marjan Ertault de la Bretonnière, Valérie Touitou, Nathalie Cassoux, Sami Boussetta, Florence Broussais, Benedicte Gelas-Dore, Noélie Barzic, Hervé Ghesquières, Khê Hoang-Xuan, Carole Soussain

Rationale
1. PCNSL: ABC-DBCL
2. Mutations of MYD88
and CD79b
3. Unmet medical needs
4. Activity of Ibrutinib in
systemic ABC-
DLBCL
HE
S
CD 10 BCL6 MUM1
4%
51 %
45 %
96 %
Camilleri-Broët S, Blood 2006; Montesinos-Rongen,
Leukemia 2008; Gonzalez-Aguiar, Clin Cancer Res 2012;
Advani, J Clin Oncol 2013; Chapuy, Blood 2016

iLOC study: Main Features
● Prospective multicenter phase II.
● Relapse/Refractory DLBCL- PCNSL or PVRL
● > 18 y
● ECOG PS < 2
● 1-4 previous lines of chemotherapy
● Corticosteroids allowed during the first cycle

Schedule: Ibrutinib in relapsed PCNSL
Ibrutinib : 560 mg/day until disease progression or TRT
Therapeutic Response Evaluations: IPCG criteria
Soussain et al, ICML 2017

Primary Objective
● DC rate (CR + CRu + PR + SD) after 2 cycles of treatment or at treatment discontinuation.
● Response evaluation according to IPCG criteria
– Evaluated locally by investigators.
– Central review of MRI

Methods
● Two-stage Simon’s design
– Ineffective treatment if the DC rate < 10% (H0)
– Effective treatment if the DC rate > 30% (H1)
– Risk 1-sided α = 0.05 and power = 80%
● Sample size
– Stage 1: 18 patients with an efficacy threshold of 3 patients (ASH abstract # 784): DC in 15/18 patients
– Stage 2: 35 patients with an efficacy threshold of 7 patients
Patients are evaluable for response if they received 90 % of the planned dose for the first month of treatment

iLOC
Patients evaluable for response
N=43 patients
Patients Enrolled
N=52 patients
Early treatment discontinuation < 1 month : N = 9 (PD in 8, toxicity in 1)
End of treatment : N = 32
On going treatment
N=11 patients
Sept 30, 2015 – July 6, 2016
May 2017

Patient characteristics
Age (range) 70 (range 52-81)
Gender ratio M: F 19: 24
PS 0-1
PS 2
33 (77%)
10 (23%)
> 2 lines of treatment 26 (60%)
ASCT n=4; WBRT n=1
Relapse vs refractory disease 30 (70%) vs 13 (30%)
Disease assessment at start of
treatment:
Brain parenchyma/Spinal cord
Intraocular
29 (inc 5 with IO)
14 (inc 2 with CSF)
Corticosteroids during Course 1 14
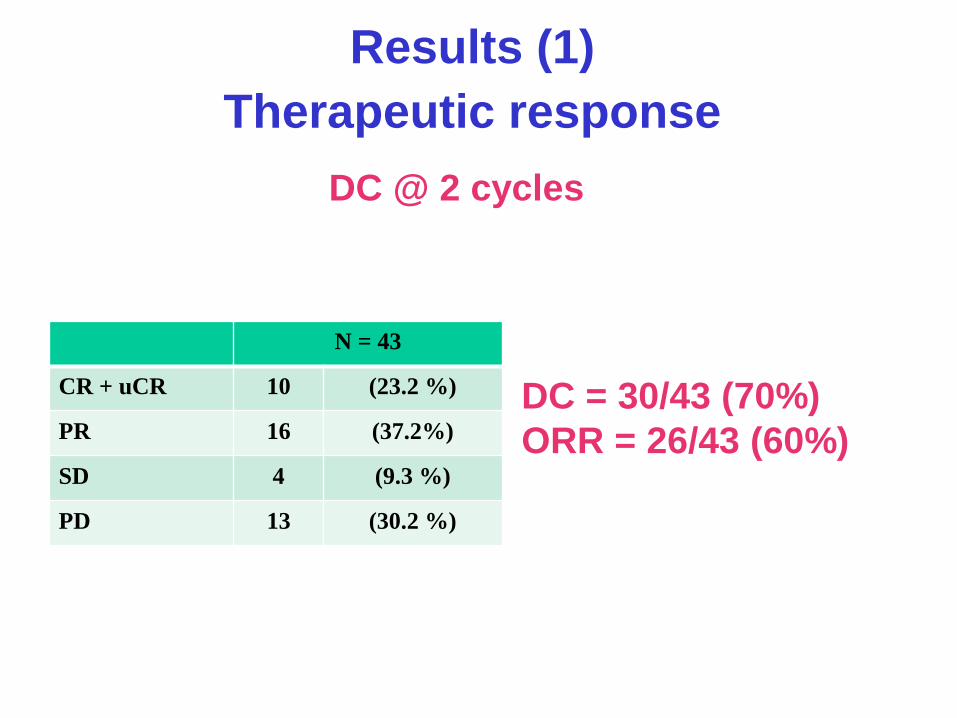
Results (1)
Therapeutic response
DC @ 2 cycles
DC = 30/43 (70%)
ORR = 26/43 (60%)
N = 43
CR + uCR 10 (23.2 %)
PR 16 (37.2%)
SD 4 (9.3 %)
PD 13 (30.2 %)

Results (2)
Previous corticosteroids therapy
DC @ 2 cycles
N = 43
CR + uCR 10 (23.2 %)
PR 16 (37.2%)
SD 4 (9.3 %)
PD 13 (30.2 %)
Corticosteroid
No
(n = 29)
Yes
(n = 14)
CR + uCR 10 0
PR 12 4
SD 2 2
PD 5 8

DC according to site of disease
● Brain or spinal cord involvement at baseline : N = 29
DC @ 2 cycles = 16/29 (55 %)
– CR : 4; PR: 10 (ORR = 14/29, 48 %), including 5 nearly CR
– SD: 2
– PD: 13
● IO involvement at baseline: n = 19
DC @ 2 cycles = 16 (84 %)
– CR : 10; PR: 4 (ORR = 14/19, 74%)
– SD: 2; ND: 1; inconclusive : 2
● CSF involvement at baseline: n = 4
– CR: 3
– Not done in 1

Duration of Ibrutinib treatment
● Median follow-up = 9.2 m
● DC rate (70%) @ 2 months
● Median number of cycles = 6
21 patients > 6 months
11 patients > 12 months
● Discontinations of treatment
in 32 patients
– PD: N = 25
– Toxicity of study treatment: N =3
– Other : N = 4 0 2 4 6 8 10 12 14 16 18 20 22
Cycle evaluable
Progression evaluable
EOT Evaluable
Death Evaluable

Duration of treatment according to site of
disease involvement at baseline
No parenchyma involvement
(n = 14)
Parenchyma Involvement
(n = 29)
12 months 6 months
Before @ 2
months
@ 18 months

Adverse events
N=52 AE Intensity
1 3 (5.7%) 2 25 (47.2%) 3 16 (30.2%) 4 5 (9.4%) 5 4 (7.5%) Missing 1
Relationship with Ibrutinib Related 15 (28.3%) Unrelated 37 (69.8%) Not applicable 1 (1.9%) Missing 1
N=52 Patients Events
Ae 22 (42.3%) 54 Infection 7 (13.5%) 11
General Disorders 5 (9.6%) 5
Blood And Lymphatic System Disorders 4 (7.7%) 7
Nervous System Disorders 4 (7.7%) 4 Cardiac Disorders 3 (5.8%) 3 Gastrointestinal Disorders 3 (5.8%) 8
Vascular Disorders 3 (5.8%) 3 Psychiatric Disorders 2 (3.8%) 2 Respiratory, Disorders 2 (3.8%) 3
Eye Disorders 1 (1.9%) 3 Hepatic Disorder 1 (1.9%) 1 Metabolism And Nutrition Disorders 1 (1.9%) 1
Renal And Urinary Disorders 1 (1.9%) 1 Surgical And Medical Procedures 1 (1.9%) 1

SAE of special interest
● Ventricular hemorrhage (n= 2)
● Hyphema (n = 1)
● Atrial fibrillation (n =2)
● Two cases of Pulmonary Aspergillosis
– At 1 months with a favourable outcome
– After a severe flu and 21 days of ibrutinib with a
fatal outcome

Conclusions
1. Manageable toxicity
2. ‘Proof of concept’ of activity of ibrutinib in R/R
PCNSL with a DC rate (70%) @ 2 months
– Responses in the brain, IO, CSF, spinal cord
3. Single agent ibrutinib can be considered as a
treatment alternative in selected patients
4. Benefit of ibrutinib in combination with
chemotherapy at relapse and in first-line treatment of
PCNSL
5. Role of ibrutinib monotherapy in first-line PVRL

CheckMate 647: A Phase 2, Open-Label Study of
Nivolumab in Relapsed/Refractory PCNSL or
Relapsed/Refractory Primary Testicular
Lymphoma
Lakshmi Nayak,1 Fabio M Iwamoto,2 Andrés José María Ferreri,3 Armando Santoro,4 Samuel
Singer,5 Connie Batlevi,6 Tracy T. Batchelor,7 James Rubenstein,8 Patrick Johnston,9
Radhakrishnan Ramchandren,10 Carole Soussain,11 Jan Drappatz,12 Kevin Becker,13 Mathias
Witzens-Harig,14 Gerald Illerhaus,15 Alex F. Herrera,16 Aisha Masood,17 Margaret Shipp1
1Dana-Farber Cancer Institute, Boston, MA, USA; 2Columbia University Medical Center, New York, NY, USA; 3IRCCS
San Raffaele Scientific Institute, Milan, Italy; 4Humanitas Cancer Center – Humanitas University, Rozzano–Milan, Italy; 5Hackensack University Medical Center, Hackensack, NJ, USA; 6Memorial Sloan Kettering Cancer Center, New York,
NY, USA; 7Massachusetts General Hospital, Boston, MA, USA; 8University of California San Francisco Medical Center,
San Francisco, CA, USA; 9Mayo Clinic, Rochester, MN, USA; 10Barbara Ann Karmanos Cancer Institute, Detroit, MI,
USA; 11Institut Curie, Hôpital René-Huguenin, Saint-Cloud, France; 12Hillman Cancer Center, University of Pittsburgh
Medical Center, Pittsburgh, PA, USA; 13Yale Cancer Center, New Haven, CT, USA; 14University Hospital Heidelberg,
Heidelberg, Germany; 15Klinikum Stuttgart, Stuttgart, Germany; 16City of Hope, Duarte, CA, USA; 17Bristol-Myers
Squibb, Princeton, NJ, USA
Presented at the 14th International Conference on Malignant Lymphoma (ICML); Lugano, Switzerland; June 14–17, 2017

Preclinical & clinical studies have shown that
lymphoid malignancies with 9p24.1/PD-L1/PD-L2
alterations are genetically predisposed to rely on
PD-1 mediated immune evasion
Immune evasion in lymphoid malignancies

PD–L1 and PD-L2 protein expression is increased
via PD–L1 and PD-L2 copy gain and transcription
is further induced via JAK2/STAT signaling
1. Green et al. Blood 2010;116:3268–77; 2. Hao et al. Clin Cancer Res 2014;20:2674–83; 3. Roemer et al. J Clin Oncol 2016; 34:2690.
9p24.1 Amplicon Block
1) JAK2 amplification
3) JAK-2-induced
PD-1 ligand
transcription and
cellular proliferation
2) Increased JAK2
protein expression
and kinase activity
–log10
(Q value) 2 4
p24.2
p24.2
JAK2 PD-L1/2
0
p24.1
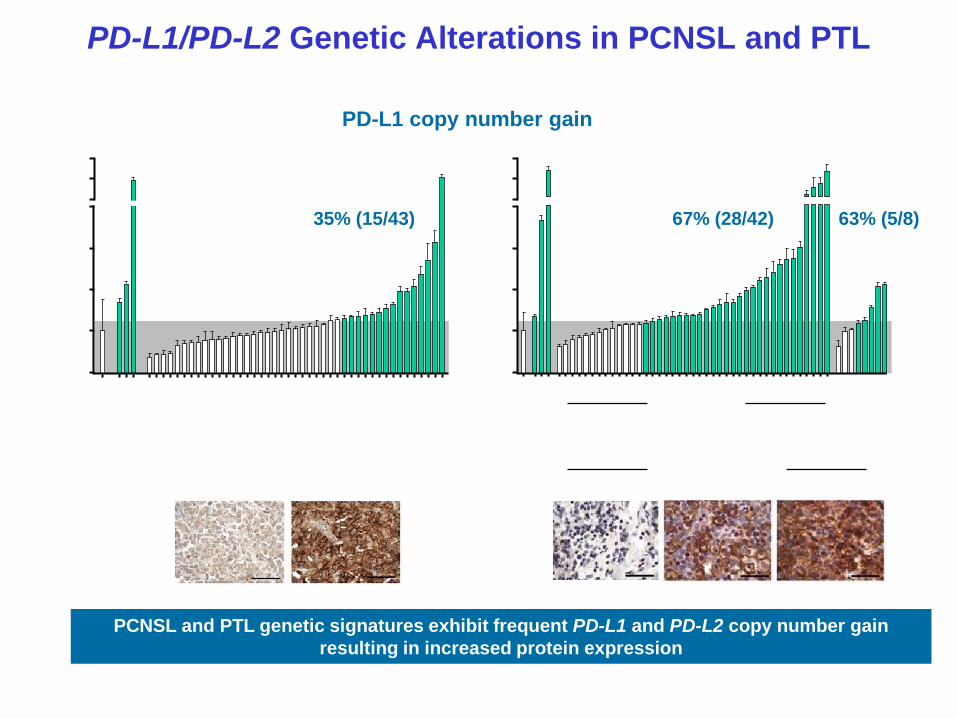
PD-L1/PD-L2 Genetic Alterations in PCNSL and PTL
EBV = Epstein-Barr virus; PD-1 = programmed death-1
Chapuy B et al. Blood 2016;127:869–81.
PCNSL and PTL genetic signatures exhibit frequent PD-L1 and PD-L2 copy number gain
resulting in increased protein expression
2
0
EBV- (n=42)
PTL (n=43) PCNSL (n=50)
EBV+ (n=8)
35% (15/43) 67% (28/42) 63% (5/8)
PD-L1 copy number gain
0
4
6
8
16
Co
py N
um
ber
No
rmals
L
428
S
UP
DH
1
HD
LM
2 1 7 22 41 43
2
4
6
8
16
Co
py N
um
be
r
No
rma
ls
L428
S
UP
DH
1
HD
LM
2 4 15 39 44 49
case #7
PD
-L1
case #43
PD
-L1
case #4 case #39 case #49
Cases with copy gain are highlighted in blue. Error bars reflect standard
deviation

Targeting the PD-1 Pathway in PCNSL and PTL with Nivolumab
PD-1 = programmed death-1
1. Chapuy B et al. Blood 2016;127:869–81; 2. Roemer M et al. J Clin Oncol 2016;34:2690–7; 3. Ansell SM et al. N Engl J Med
2015;372:311–9; 4. Younes A et al. Lancet Oncol 2016;17:1283–94;
Nivolumab is a fully-human immunoglobulin G4 monoclonal antibody targeting the
programmed death-1 (PD-1) receptor immune checkpoint pathway
PD-L1/PD-L2 genetic alterations in PCNSL and PTL1 suggest targeting the PD-1
pathway may be a promising therapeutic strategy, as seen in classical Hodgkin
lymphoma2–4

Clinical Case Series With Off-Label Nivolumab
Characteristics N=5
Tumor type
• Primary refractory PCNSL = 1
• Recurrent PCNSL = 3
• CNS recurrence of PT = 1
Median age (range), years 64 (54–85)
Median KPS (range), % 70 (40–80)
Treatment history
All pts treated with standard regimens
including HD-MTX based chemotherapy, ASCT
and WBRT
Nayak L et al. Blood 2017; doi: 10.1182/blood-2017-01-764209

Case Series: Responses to Nivolumab in R/R PCNSL or PTL
Patient #1 #2 #3 #4 #5
Disease
Primary
refractory
PCNSL
Recurrent
PCNSL
Recurrent
PCNSL
Recurrent
PCNSL
CNS recurrence
of PTL
Presenting
symptoms
Visual field deficit
& cognitive
change
Cognitive change
Nausea,
vomiting,
ataxia
Asymptomatic Aphasia,
impaired LOC
KPS, % 70 80 50 80 40
Radiographic
response CR CR PR CR CR
Neurologic/
clinical
response
Complete
Resolution
Complete
Resolution Resolution
Stable
(asymptomatic) Resolution
KPS, % 90 80 70 80 80
PFS, months 13+ 17 17+ 14 14+
Clinical Case Series With Off-Label Nivolumab
Nayak L et al. Blood 2017; doi: 10.1182/blood-2017-01-764209

Case Series: Responses to Nivolumab in R/R PCNSL or PTL
Median number of treatments to objective radiographic response was 3 (range, 2–4)
Persistent ocular disease was observed in 1 patient
Clinical Case Series With Off-Label Nivolumab
Patient #1 #2 #3 #4 #5
Disease
Primary
refractory
PCNSL
Recurrent
PCNSL
Recurrent
PCNSL
Recurrent
PCNSL
CNS recurrence
of PTL
Presenting
symptoms
Visual field deficit
& cognitive
change
Cognitive change
Nausea,
vomiting,
ataxia
Asymptomatic Aphasia,
impaired LOC
KPS, % 70 80 50 80 40
Radiographic
response CR CR PR CR CR
Neurologic/
clinical
response
Complete
Resolution
Complete
Resolution Resolution
Stable
(asymptomatic) Resolution
KPS, % 90 80 70 80 80
PFS, months 13+ 17 17+ 14 14+
KPS = Karnofsky performance status; LOC = level of consciousness; PFS = progression-free survival, CR = complete response, PR = partial
response
Nayak L et al. Blood 2017; doi: 10.1182/blood-2017-01-764209 [Epub ahead of print]

Case Series: Responses to Nivolumab in R/R PCNSL or PTL
All patients were alive at a median follow-up of
17 months
KPS = Karnofsky performance status; LOC = level of consciousness; PFS = progression-free survival, CR = complete response, PR = partial
response Nayak L et al. Blood 2017; doi: 10.1182/blood-2017-01-764209 [Epub ahead of print]
Clinical Case Series With Off-Label Nivolumab
Patient #1 #2 #3 #4 #5
Disease
Primary
refractory
PCNSL
Recurrent
PCNSL
Recurrent
PCNSL
Recurrent
PCNSL
CNS recurrence
of PTL
Presenting
symptoms
Visual field deficit
& cognitive
change
Cognitive change
Nausea,
vomiting,
ataxia
Asymptomatic Aphasia,
impaired LOC
KPS, % 70 80 50 80 40
Radiographic
response CR CR PR CR CR
Neurologic/
clinical
response
Complete
Resolution
Complete
Resolution Resolution
Stable
(asymptomatic) Resolution
KPS, % 90 80 70 80 80
PFS, months 13+ 17 17+ 14 14+

Case Series: Complete Radiographic Response to
Nivolumab in a Patient With Primary Refractory PCNSL
Baseline Post-nivolumab
CR at 2 months
CR sustained at 13 months
Primary refractory PCNSL
Head CTs with contrast, #1
CR = complete response
Nayak L et al. Blood 2017; doi: 10.1182/blood-2017-01-764209 [Epub ahead of print]

CheckMate 647
Study design A phase 2, open-label, single-arm, 2-cohort study
of nivolumab in R/R PCNSL or R/R PTL
Primary objective ORR by BICR
Secondary objectives
• PFS
• DOR
• OS
Planned enrollment
Total: 65 patients
• PCNSL : 45 patients
• PTL : 20 patients
Estimated completion December 2019
ClinicalTrials.gov ID NCT02857426
BICR = blinded Independent Central Review; DOR = duration of response; ORR = overall response rate; OS = overall survival.

CheckMate 647: Study Design
Endpoints
Primary
• ORR
Secondary
• PFS
• DOR
• OS
Nivo 240 mg IV
Q2W
Cycles 1–8
Treatment until disease progression, unacceptable toxicity, or 2-year maximum duration
Follow-up
RR PCNSL N≈45
RR PTL N≈20
Nivo 480 mg IV
Q4W
Cycle 9+
Nivo = nivolumab; Q2W = every 2 weeks; Q4W = every 4 weeks
Month
Cycle 8
4
Treatment
end
24
Treatment
start
0

CheckMate 647: Key Eligibility Criteria
Inclusion Criteria
• Adults aged ≥18 years
• Progressed on or did not respond to ≥1 line of
standard of care therapy
• PCNSL patients: Measurable disease on MRI with
≥1 extranodal lesion
• PTL patients: ≥1 extranodal or nodal lesion
• Karnofsky performance status of ≥70
• Dose of dexamethasone or equivalent ≤ 2 mg/day
allowed 14 days prior to first dose of nivolumab

CheckMate 647: Key Eligibility Criteria
Exclusion Criteria
• Prior treatment with checkpoint inhibitors or T cell co-stimulatory drugsa
• Intraocular PCNSL with no evidence of measurable brain disease
• Patients with brain stem lesions
• PTL patients with prior history of allogeneic transplantation <6 months
before screening
• Dexamethasone requirement of >2mg/day within the 14 days prior to
first dose of nivolumab
• Prior active malignancy within 3 years
• Concurrent autoimmune disease
aIncludes antibodies that target PD-1, PD-L1, PD-L2, CD137, CTLA-4, or any agent targeting T-cell co-stimulation
or checkpoint pathways
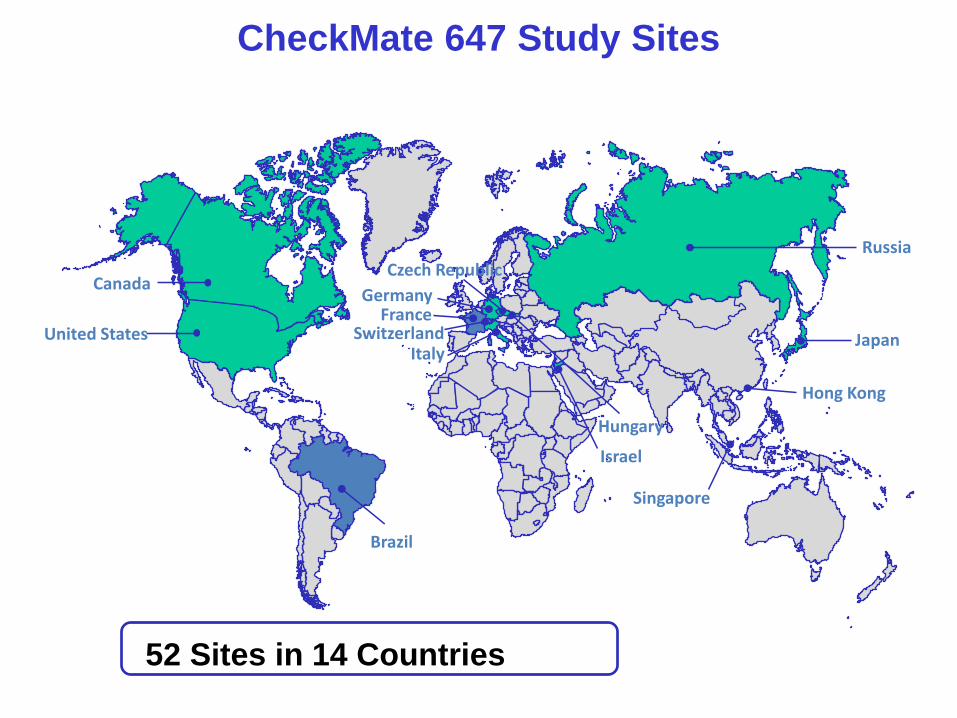
CheckMate 647 Study Sites
United States
Canada
Russia
Japan Italy
Germany
Czech Republic
Hungary
Israel
Singapore
Brazil
France
Hong Kong
Switzerland
52 Sites in 14 Countries

Summary
● PCNSL and PTL are rare, aggressive B-cell NHLs with limited treatment
options and high unmet need
– Patients experience high relapse rates and poor outcomes
● Nivolumab is a checkpoint inhibitor that targets PD-1 to restore T-cell
antitumor immune responses
● Genetic alterations prevalent in PCNSL and PTL indicate targeting the
PD-1 pathway may be a promising therapeutic strategy
● A case series in 5 patients with R/R PCNSL or R/R PTL suggested
nivolumab may be an effective treatment option for these patients
● The Phase 2 CheckMate 647 study (NCT02857426) is currently enrolling
patients with R/R PCNSL and R/R PTL

Relapse of PCNSL
1. Decreased incidence of R/R with the new generations of induction treatment?
2. Repeated MRIs optimal for follow-up?
3. Strong biomarkers are needed to assess minimal residual disease (MRD)
4. Long survivors with salvage chemotherapy followed by ASCT
5. On going studies are testing new drugs as an alternative consolidation treatment
6. Strong signals of activity of iMids (Lenalidamide) and BTK-inhibitors (Ibrutinib) and PD1-inhibitors

Key points and outstanding issues
● PCNSL is potentially curable
● Performance score is prognostic
● Chemotherapy should be considered for ‘all’
● Role of immunotherapy is clear
● In whom/How can we avoid radiotherapy?
● Role of stem cell transplantation? When?
● Effective salvage strategies emerging
● Long term neurocognitive sequaele