prevention of perinatal hiv transmission in 2016 · prevention of perinatal hiv ... avoid...
TRANSCRIPT

Emily Adhikari, MD Division of Maternal-Fetal Medicine
Obstetrics and Gynecology University of Texas Southwestern Medical Center
February 20, 2018
Prevention of Perinatal HIV Transmission

None

Understand the prenatal, intrapartum, and postnatal
management of HIV and current controversies
Describe first-line antiretroviral therapy (ART) regimens
for use in pregnancy
Describe the contraceptive options available to HIV-
infected women
State the reproductive options for safer conception
among serodiscordant couples

CDC HIV Surveillance Report 2016

CDC 2014

CDC 2012
People living with HIV

0
20
40
60
80
100
120
2011 2012 2013 2014 2015 2016 2017
Lost to follow up
Delivered elsewhere
SAB/EAB/SB
Delivered pregnancies,liveborn >24 weeks
2 2 1 No. of baby seroconversions
0 0 0 1

0
20
40
60
80
100
120
2011 2012 2013 2014 2015 2016 2017
Diagnosed >1 year prior topresentation
Diagnosed ≤ 1 year prior to presentation
*Preliminary data
*

0
20
40
60
80
100
120
140
2011 2012 2013 2014 2015 2016 2017
HIV-exposed babies
1 1 2 0 2 2 Number of seroconversions 2
Courtesy Mary Mallory, RN,PNP

Note. Data include persons with a diagnosis of HIV infection regardless of stage of disease at diagnosis.
Diagnoses of Perinatally Acquired HIV Infection among Children Born in the United
States and Puerto Rico, Birth Years 2009–2013, by Area of Residence
N = 345
CDC 2015

JAMA Peds, 2017

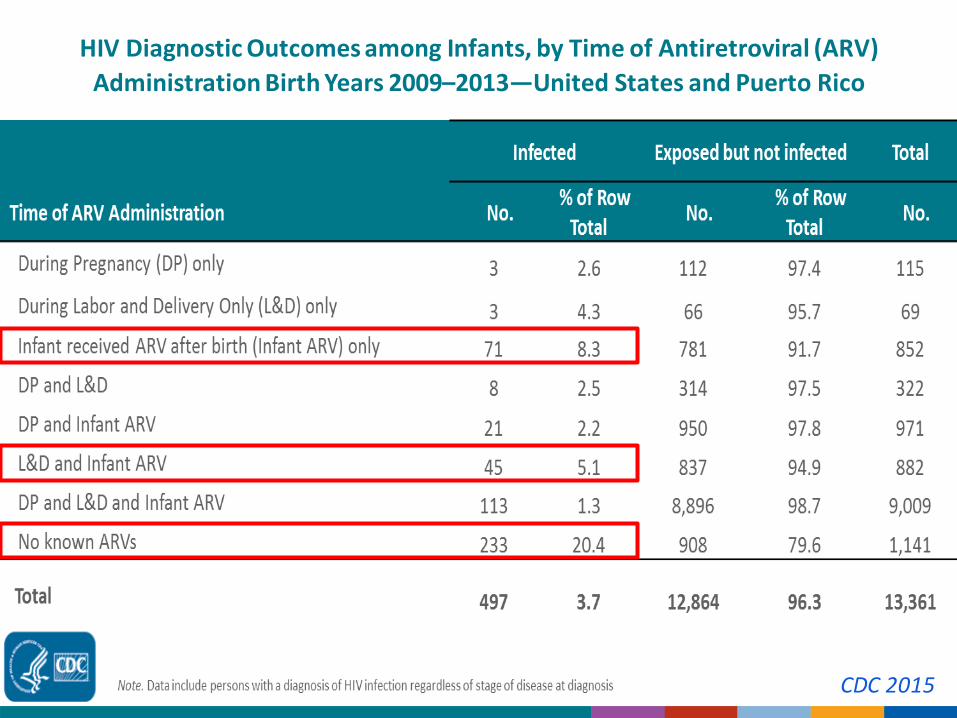
HIV Diagnostic Outcomes among Infants, by Time of Antiretroviral (ARV)
Administration Birth Years 2009–2013—United States and Puerto Rico
CDC 2015
● Intrauterine (before 36 weeks) ~20% of cases
● Detection of HIV in newborn at 1–2 days of life
● Peripartum ~80% of cases ● Onset of placental separation
● Mother-to-fetus microtransfusions
● Labor and rupture of membranes
● Detection of HIV at weeks to months of life
Minimize (eliminate) the risk of perinatal HIV
transmission
Optimize the health of the mother while minimizing
adverse pregnancy outcomes
Establish (or re-establish) HIV care during and after
delivery
Minimize interruptions in therapy and risk of viral
resistance
Plan for contraception or future safe conception

● Without ART during pregnancy, the risk of transmission
from mother to infant is 1 in 4.
● The risk of perinatal transmission can be <1% with:
● Highly active ART therapy (HAART) for mom (prior to conception ideally)
● Intrapartum AZT
● Elective Cesarean section as appropriate
● Formula feeding
● Infant prophylaxis



Mofenson, NEJM,1999

24.50
9.10
3.80
1.20 0.00
5.00
10.00
15.00
20.00
25.00
30.00
1993 1994 1999 2002
Perinatal HIV Transmission Rate per 100
Cooper, Combination ART for pregnant women with HIV, JAID Human Retrovir, 2002
ZDV alone
cART without PI
cART with PI
No ART
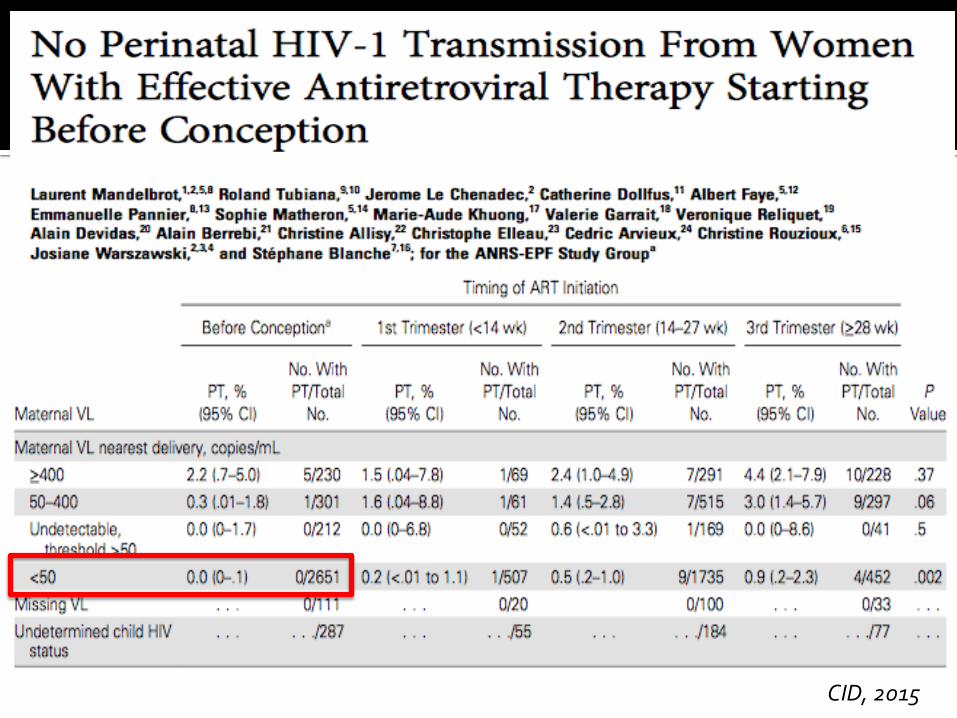
CID, 2015

● Without ART during pregnancy, the risk of transmission
from mother to infant is 1 in 4.
● The risk of perinatal transmission can be <1% with:
● Highly active ART therapy (HAART) for mom (prior to conception ideally)
● Intrapartum AZT
● Elective Cesarean section as appropriate
● Formula feeding
● Infant prophylaxis

Intravenous (IV) zidovudine:
Should be administered to women living with HIV with HIV RNA >1,000 copies/mL (or unknown HIV RNA) near delivery (AI),
Is not required for women receiving ART regimens who have HIV RNA ≤50 copies/mL during late pregnancy and near delivery and no concerns regarding adherence to the ART regimen (BII).

CID, 2013

Obstetrics & Gynecology, 2017

● Without ART during pregnancy, the risk of transmission
from mother to infant is 1 in 4.
● The risk of perinatal transmission can be <1% with:
● Highly active ART therapy (HAART) for mom (prior to conception ideally)
● Intrapartum AZT
● Elective Cesarean section as appropriate
● Formula feeding
● Infant prophylaxis

● Cesarean section recommended:
● For women with HIV RNA levels >1,000 near time of
delivery
● Schedule at 38 weeks if for viral load; 39 weeks
otherwise
● Benefits of Cesarean unclear after ROM or onset of labor,
or for women with HIV RNA levels <1,000 on combination
ARVs
● Trial of Labor after Cesarean (TOLAC)…

In women with an HIV RNA >1,000 copies/mL or unknown HIV RNA level who present in spontaneous labor or with ruptured membranes, there is insufficient evidence to determine whether cesarean reduces the risk of perinatal HIV transmission. Management of women originally scheduled for cesarean delivery because of HIV infection who present in labor must be individualized at the time of presentation (BII).

Obstetrics & Gynecology, 2017

● Maternal Factors
● High viral load
● Low CD4+ lymphocyte count
● Maternal systemic co-infections
● STDs: ulcerative diseases
● Maternal IV drug use
● No ART or prophylaxis

● Obstetric Factors
● ?Length of ruptured membranes
● Chorioamnionitis
● Vaginal delivery (if VL > 1000)
● Invasive procedures
● Infant Factors
● Prematurity
● Breastfeeding
How long is too long?
Should I do a c-section after 4 hours of rupture?
What if my patient is in active labor?
What if my patient is remote from delivery?

AJOG, 1995

AIDS, 2001

AJOG, 2012

BJOG, 2016
Data on the association of duration of rupture of membranes (ROM) and perinatal transmission in the era of effective antiretroviral therapy (ART) are reassuring.
…BUT

JAIDS, 2002

Recommendations for Use of Antiretroviral Drugs in Pregnant HIV-1-Infected Women for Maternal Health and Interventions to Reduce Perinatal HIV
Transmission in the United States.
www.aidsinfo.nih.gov

2.19.18 AIDSinfo.nih.gov


2.19.18 AIDSinfo.nih.gov

2.19.18 AIDSinfo.nih.gov

● Current practice at PHHS is to administer IV ZDV to all
HIV-positive women regardless of viral load
● Continue oral ART regimen during labor
● Avoid invasive procedures
● Active management of labor
● Avoid methergine
Preterm Birth Drug interactions
● Women taking antiretroviral therapy may be at
increased risk for preterm delivery, low birth
weight infants (<2500g) and small-for-gestational
age infants (BW <10th centile for GA).
● RR ranges 1.2 - 3.4 in 19 studies reporting an
association, but data are heterogeneous
● In 2 studies evaluating risk of spontaneous preterm
birth in association with ART use: no association
● What about the PROMISE study?

● RCT of antepartum treatment regimens: ZDV alone,
ZDV-based ART, TDF-based ART
● Efficacy outcomes: + Infant HIV at 1 week, infant HIV-
free survival
● Safety outcomes: Maternal, infant safety outcomes,
adverse pregnancy outcomes:
● Preterm delivery (<37wks), early preterm (<34wks)
● Low (<2500g) or very low (<1500g) infant birth weight


Hypertensive disorders of pregnancy – not recorded
Strongly associated with adverse pregnancy outcomes (preterm birth, low birth weight, neonatal death, stillbirth)
Spontaneous versus iatrogenic preterm birth
TDF – LPV/r interaction?

In women who are receiving a cytochrome P450 (CYP) 3A4 enzyme inhibitor (e.g., a protease inhibitor, cobicistat), methergine should be used only if no alternative treatments for postpartum hemorrhage are available and the need for pharmacologic treatment outweighs the risks. If methergine is used, it should be administered in the lowest effective dose for the shortest possible duration (BIII).

● Maternal Child Health postpartum visit (MFM clinic)
● Refer mother for continued HIV care
● Confirm ART dosage changes if needed postpartum
(atazanavir)
● Monitor for adherence and postpartum depression
● HIV testing and follow-up of neonate and other children
● Follow-up of sexual/needle-sharing partners

● Primary, gynecologic/obstetric, and family planning
services
● Mental health services
● Substance abuse treatment
● Coordination of care through case management for
the woman, her children, and other family members
● HIV-infected women can use all available contraceptive
methods
● For those on boosted PI regimen (atazanavir/ritonavir) :
● Implant, progestin-only pill, combined hormonal
contraceptives = 2
● DMPA = 1
● IUD: Initiation = 1/2 , Continuation = 1
● Emergency contraception should be offered
CDC, Medical Eligibility Criteria for Contraception 2016

Stewart, Interpregnancy HIV Control, AJOG, 2014

Adams, Clinical Infectious Diseases, 2015

Unpublished data
n = 579 deliveries
Followed up to MFM clinic postpartum 465 (80%)
Followed up to HIV clinic within 1 year postpartum
390 (67%)
Median time to HIV clinic visit (days) 50 [29-103]
Deliveries at Parkland between Jan 1, 2005 – June 30, 2015
Data presented as n (%) or median [Q1, Q3] as appropriate

● ART for the infected partner until VL undetectable
● Consider pre-exposure prophylaxis (PrEP)
● Discordance between plasma and genital viral loads reported
● ARV drugs vary in ability to penetrate the genital tract
Female with HIV: artificial insemination (partner’s sperm)
Male with HIV: donor sperm with artificial insemination
• Sperm preparation techniques
• Semen analysis recommended to HIV-infected males before conception is attempted
Timed, peri-ovulatory intercourse without a condom after partner with HIV has achieved viral suppression on ART.

Once daily Truvada:
Start 1 month prior to attempting to conceive; continue for 1 month after conception
● Timed, periovulatory unprotected intercourse only (AFTER partner is fully suppressed)
● HIV, STDs, and pregnancy tests q3months (Cr q6 months)
● Check Hep B status, vaccinate
● Adherence is critical
● Anyone at ongoing risk of HIV acquisition is a candidate
● If new HIV infection documented during PrEP: stop PrEP and stop attempting to conceive. Refer to HIV specialist.
● Pregnancy and breastfeeding are NOT contraindications
● Abstinence recommended during pregnancy
● Discuss symptoms, risk of acute HIV infection during
pregnancy (and risk of vertical transmission).
● PrEP when the HIV-infected partner is receiving cART and
suppressed has not been well studied

https://dctakesonhiv.com/prep/african_american_women

Needs at Parkland: - PreP on formulary - Medical home for non-pregnant women in serodiscordant relationships on PreP
Obstetrics & Gynecology, 2016

Summary
Women with HIV are living longer and having more babies
Elimination of perinatal transmission is possible
Simplified ART regimens are recommended over Combivir/Kaletra
Some areas of obstetrics still controversial
Postpartum follow up is key
Providers should inquire about patient and partner HIV status and
offer safe conception counseling
PrEP is recommended for women at high risk of HIV acquisition

Barbara McElwee, WHNP
Scott Roberts, MD
Vanessa Rogers, MD
Linda Andoseh, NP
Arti Barnes, MD
Jeanne Sheffield, MD
Casey Senter, MD
Cece Cheng, MD
Mary Ann Kelly, RN
Don McIntire, PhD
Catherine Eppes, MD
Mary Mallory, RN, PNP