prevention and treatment of pain in pediatric trauma...
TRANSCRIPT

Stefan J. Friedrichsdorf, MD, FAAPMedical Director, Department of Pain Medicine, Palliative Care & Integrative MedicineChildren's Hospitals and Clinics of Minnesota, Minneapolis/St. Paul, MN
Associate Professor of Pediatrics, University of Minnesota Medical School
[email protected] Twitter: @NoNeedlessPain
Prevention and Treatment of Pain in Pediatric Trauma Patients.
Learning Objectives
• Critically review risks and safety of analgesic under-treatment versus over-treatment in hospitalized infants and children with trauma pain
• Evaluate assumptions about opioid use in children
• Discuss how multiple agents, interventions, rehabilitation, psychological and integrative (“non-pharmacologic”) therapies act synergistically for more effective pediatric pain control with fewer side effects than a single analgesic or modality
5-year old Marius: Procedural Pain Management
”Redningskvinder” Channel Tv3 - Http://Www.Tv3.Dk/Redningskvinder. (Episode 7, Season 4.) 2014

Don't have enough staff for pediatric pain control...?
Funny, how there is always enough staff to
restrain a child.
Pediatric Analgesia in 1985 “Papoose Boards”
Pain after trauma injury: Multifactorial
• Acute pain• Tissue damage, repetitive trauma
• Procedural pain• Dressing changes, intravenous access
• Neuropathic pain Portilla AS1, Bravo GL, Miraval FK, Villamar MF, Schneider JC, Ryan CM, Fregni F J Burn Care Res. 2013 Jan-Feb;34(1):e48-52. A feasibility
study assessing cortical plasticity in chronic neuropathic pain following burn injury.
• Psycho-spiritual-spiritual pain
• Chronic pain• Chronic post surgical pain
• Pain can persist after healing Dauber et al. Chronic persistent pain after severe burns. A survey of 358 burn survivors. Pain Med 2002; 3:6-17.
• n=358; burns covering an average of 59% of their bodies
• 12 years laster: 52% of respondents reported ongoing burn-related pain

So, how do we treat the individual pain patient in front of us ?
Hmhh... Spoiler Alert: Crystal-clear answer on 3rd last slide!
Pediatric Pain - Status Quo
• Under treatment of pain in children
• Parents expect pain to be relieved Forgeron PA, Finley GA, Arnaout M. Pediatric pain prevalence and
parents' attitudes at a cancer hospital in Jordan. J Pain Symptom Manage. 2006; 31(5):440-8.
• Priorities of parents of hospitalized children "Taking care of pain" rated as second highest priority (1st: getting right diagnosis) Ammentorp J, Mainz J, Sabroe S. Parents’
priorities and satisfaction with acute pediatric care. Arch Pediatr Adolesc Med 2005;159:127-131
• Parents’ greatest distress: failing to protect their child from pain Tiedeman, M. (1997). Anxiety responses of parents during and
after the hospitalisation of their 5 - to -11 year old children. Journal of Pediatric Nursing, 12(2), 110-119. Melnyk BM. Intervention studies involving parents of hospitalized young children: an analysis of the past and future recommendations. J Pediatr Nurs. 2000 Feb;15(1):4-13.
• Assumption: everything possible is done Anand’s neonatal surgery studies
Pediatric Pain - Status Quo
• USA: adults receive more than two - three times as many analgesic doses as children (with identical diagnoses) (1) Eland JM, Anderson JE: The experience of pain in
children. In: Jacox A (ed). Pain: a source book for nurses and other health care professionals. Boston: Little Brown & C0; 1977:453-78 (2) Beyer JE, DeGood DE, Ashley LC, Russell GA. Patterns of postoperative analgesic use with adults and children following cardiac surgery. Pain. 1983 Sep;17(1):71-81. (3) Schechter NL, Allen DA, Hanson K. Status of pediatric pain control: a comparison of hospital analgesic usage in children and adults. Pediatrics. 1986 Jan;77(1):11-5.
• Compared to adults, pediatric patients receive fewer and/or incorrectly dosed analgesics in daily routine Ellis, J. A., O’Connor, B. V., Cappelli, M., Goodman, J., Blouin, R.,
& Reid, C. W. (2002). Pain in hospitalized pediatric patients: How are we doing? Clinical Journal of Pain, 18, 262-269.
• The younger children are, the less likely they receive appropriate analgesia Broome ME,
Richtsmeier A, Maikler V, Alexander M. Pediatric pain practices: a national survey of health professionals. J Pain Symptom Manage. 1996 May;11(5):312-20.; Nikanne E, Kokki H, Tuovinen K. Postoperative pain after adenoidectomy in children. Br J Anaesth. 1999 Jun;82(6):886-9.

Inappropriate Analgesia: Why Bother...?
• Children with persistent pain suffer more physical symptoms in adult life, more anxiety and more depression 1946 Medical Research Council and 1958 National Child
Development Study
• Inadequate analgesia for initial procedures in children diminishes effect of adequate analgesia in subsequent procedures Weisman SJ, Bernstein B,
Schechter NL: Consequences of inadequate analgesia during painful procedures in children. Arch Pediatr Adolesc Med 1998. 152:147-9
• NICU: increased morbidity & mortality Anand KJ, Barton BA, McIntosh N, Lagercrantz H, Pelausa E, Young TE,
et al. Analgesia and sedation in preterm neonates who require ventilatory support: results from the NOPAIN trial. Neonatal Outcome and Prolonged Analgesia in Neonates. Arch Pediatr Adolesc Med. 1999 Apr;153(4):331-8
• Pain ratings at 4-6 months routine vaccination higher for circumcised versus uncircumcised boys Taddio A, Katz J,
Ilersich AL, Koren G. Effect of neonatal circumcision on pain response during subsequent routine vaccination. Lancet. 1997;349(9052):599-603.
• Up to 25% of adults have fear of needles with most fears developing in childhood: avoidance of health care (including non-adherence with vaccination schedules Taddio A, Chambers CT, Halperin SA, et al. Inadequate pain
management duringchildhood immunizations: the nerve of it. Clin Ther 2009;31(Suppl 2):S152-67.)
Trauma & post-traumatic stress disorder (PTSD)
• US soldiers after serious combat injury: Use of morphine during trauma care reduces risk of subsequent development of PTSD Holbrook TL, Galarneau MR,
Dye JL, Quinn K, Dougherty AL. Morphine use after combat injury in Iraq and post-traumatic stress disorder. The New England journal of medicine. 2010 Jan 14;362(2):110-7.
• Children (n=48) with injury that led to hospital treatment: Morphine was associated with lower levels of PTSD at follow-up 6 months later Nixon RD, Nehmy TJ, Ellis AA, Ball SA,
Menne A, McKinnon AC. Predictors of posttraumatic stress in children following injury: The influence ofappraisals, heart rate, and morphine use. Behaviour research and therapy. 2010 Aug;48(8) 810-5.
• 6-16 year-olds (n=24) with acute burns: Children receiving higher doses of morphine had greater reduction in PTSD symptoms over 6 months Saxe G, Stoddard F, Courtney D, Cunningham K, Chawla N, Sheridan R,
et al. Relationship between acute morphine and the course of PTSD in children with burns. Journal of the American Academy of Child and Adolescent Psychiatry. 2001 Aug;40(8):915-21.
• 12- to 48-month-old (n=70) children with acute burns admitted to major pediatric burn center: Management of pain with higher doses of morphine associated with decreasing number of symptoms of PTSD in months after major trauma. Stoddard FJ,
Jr., Sorrentino EA, Ceranoglu TA, Saxe G, Murphy JM, Drake JE, et al. Preliminary evidence for the effects of morphine on posttraumatic stress disorder symptoms in one- to four-year-olds with burns. J Burn Care Res. 2009 Sep-Oct;30(5):836-43.
Myths and Barriers to Using Opioids
Case Scenario:
• You are taking care of a child with severe acute somatic nociceptive pain following major trauma. It crosses your mind to administer a strong opioid such as morphine, fentanyl, or hydromorphone.
• What would be the most common concerns you might hear from your colleagues or parents arguing against opioid use in this child?
Common Opioid Assumptions
• Addiction “chronic relapsing condition characterized by persistent, compulsive dependence on a behavior or substance despite adverse consequences”
• Tolerance ≠ addiction• Pseudo-addiction
• Over Sedation / Respiratory Depression
• Ileus / Constipation
• Medication “Too strong”
• Masking symptoms
• Abdominal Pain Ranji SR, Goldman LE, Simel DL, Shojania KG. Do opiates affect the clinical evaluation of patients with abdominal pain? JAMA 2006: 296:1764-74
• Opioids after major cranial surgery in children do NOT result in altered mental status nor respiratory depression Maxwell LG. PAIN MANAGEMENT FOLLOWING
MAJOR INTRACRANIAL SURGERY IN PEDIATRIC PATIENTS: A PROSPECTIVE COHORT STUDY IN THREE ACADEMIC CHILDREN’S HOSPITALS Pediatric Critical Care Medicine: May 2014 - Volume 15 - Issue 4_suppl - p 77. Abstracts of the 7th World Congress on Pediatric Critical Care
• As always... Think first !(e.g. compartment syndrome?)... analgesia second...
How Do We Manage Acute Pain in Children?
•Dosing at regular intervals (“By the Clock”)
• Adapting treatment to the individual child (“With the Child”)
• Using the appropriate route of administration (“By the appropriate route)
• Using a two-step strategy (“By the Analgesic Ladder”)
WHO guidelines on the pharmacological treatment of persisting pain in children with medical illnesses (2012)
WHO Principle 1: Dosing at Regular Intervals
• PRN (“as needed”)
• PRN = Patient Receives Nothing
• When pain is constantly present, analgesics should be administered, while monitoring side-effects, at regular intervals
• “By the clock” and NOT as an “as needed” (or pro re nata “PRN”) basis
• Regular scheduling ensures a steady blood level, reducing the peaks and troughs of PRN (“as needed”) dosing
• PRN (as needed) only:
• May take several hours & higher opioid doses to relieve pain
• Results in cycle of undermedication and pain, alternating with periods of overmedication and drug toxicity American Pain Society: Principles of Analgesic Use in the
Treatment of Acute Pain and Cancer Pain 2008. 24-27
WHO Principle 2: Adapting Treatment to the Individual Child
• Treatment should be tailored to the individual child and opioid analgesics should be titrated on an individual basis
• At analgesic dosing: no sedation expected
• The effective dose is what relieves the pain
• Different children may respond differently to same dose
• Effective dose must be adjusted to child’s needs
• Dose of strong opioids: only the sky is the limit
• Assess response frequently
• Pain Scales
• Look for opioid-induced side effects and toxicity
Regular (!) Pain Assessment
• One-dimensional self-report scores
• Multi-dimensional rating scores

What are we measuring...?
(1) Nociceptive Pain: arises from the activation of peripheral nerve endings (nociceptors) that respond to noxious stimulation
• Somatic (for example, muscles, joints)
• Chronic somatic pain typically well localized & often results from degenerative processes (such as arthritis)
• Visceral (internal organs)
(2) Neuropathic Pain: resulting from injury to, or dysfunction of, the somatosensory system.
• Central pain: caused by a lesion or disease of the central somatosensory nervous system
(3) Psycho-social-spiritual-emotional Pain / Total Pain
(4) Chronic Pain• Pain beyond expected time of
healing
Pain in children with impaired communication
• Non-communicating Children’s Pain Checklist - Revised (NCCPC-R); postoperative Version (NCCPC-PV) Breau LM, McGrath PJ, Camfield
CS, Finley GA. Psychometric properties of the non-communicating children's pain checklist-revised. Pain 2002;99(1-2):349-357.
• Pediatric Pain Profile (PPP) Hunt A, Goldman A, Seers K, Crichton N,
Mastroyannopoulou K, Moffat V, Oulton K, Brady M. Clinical validation of the paediatric pain profile. Dev Med Child Neurol 2004;46(1):9-18.
• r-FLACC Malviya S, Voepel-Lewis T, Burke C, Merkel S, Tait
AR. The revised FLACC observational pain tool: improved reliability and validity for pain assessment in children with cognitive impairment. Paediatr Anaesth 2006;16(3):258-265.
High specificity, low sensitivity…? Don’t forget:
• Withdrawal: WAT-1 score Franck, L et al, (2008) Ped Crit Care Med, Vol 9, no. 6 Neonatal Abstinence Scoring Tool (Finnegan) Finnegan LP. Neonatal abstinence. In: Nelson NM, ed. Current Therapy
in Neonatal–Perinatal Medicine. 2nd ed. Toronto, Ontario: BC Decker Inc; 1990
• Delirium: CAPD Traube, C., et al., Cornell Assessment of Pediatric Delirium: a valid, rapid, observational tool for screening delirium in the
PICU. Crit Care Med, 2014. 42(3): p. 656-63.
• Sedation: SBS score Curley, M.A., et al., State Behavioral Scale: a sedation assessment instrument for infants and young children
supported on mechanical ventilation. Pediatr Crit Care Med, 2006. 7(2): p. 107-14.
Measuring pain alone…?
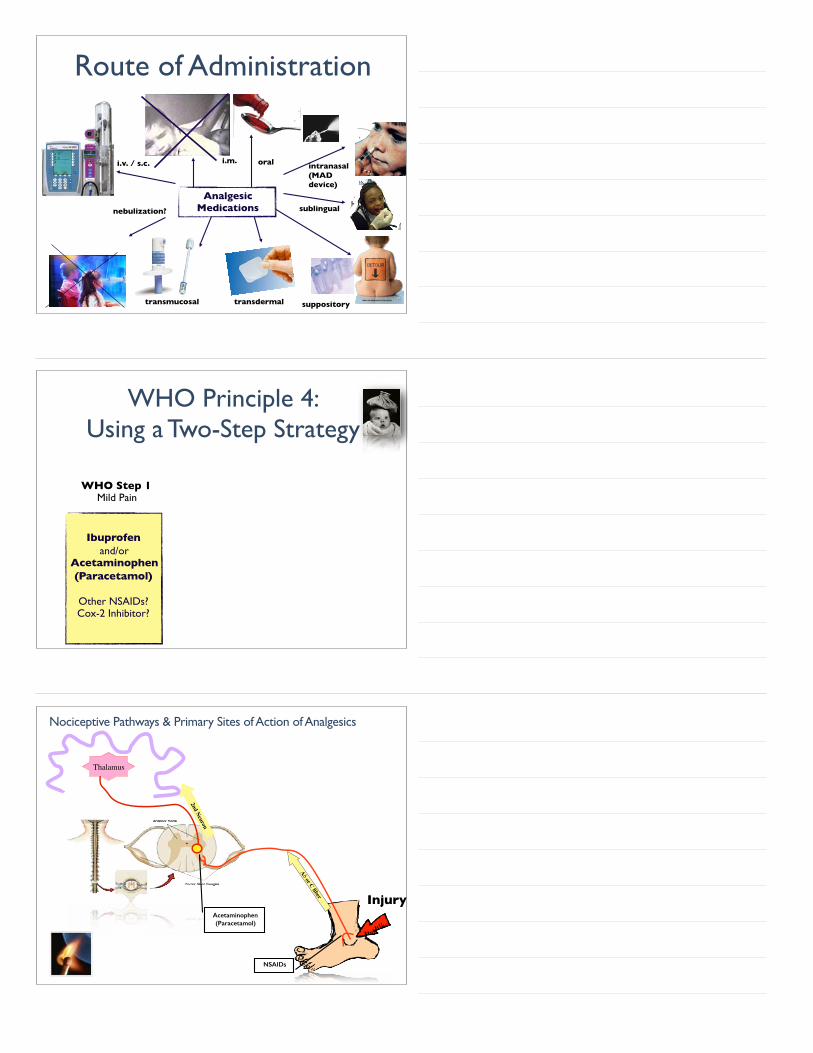
Route of Administration
orali.v. / s.c. intranasal (MAD device)
nebulization?
suppositorytransdermal
i.m.
sublingual
transmucosal
Analgesic Medications
WHO Principle 4: Using a Two-Step Strategy
WHO Step 1Mild Pain
Ibuprofenand/or
Acetaminophen(Paracetamol)
Other NSAIDs?Cox-2 Inhibitor?
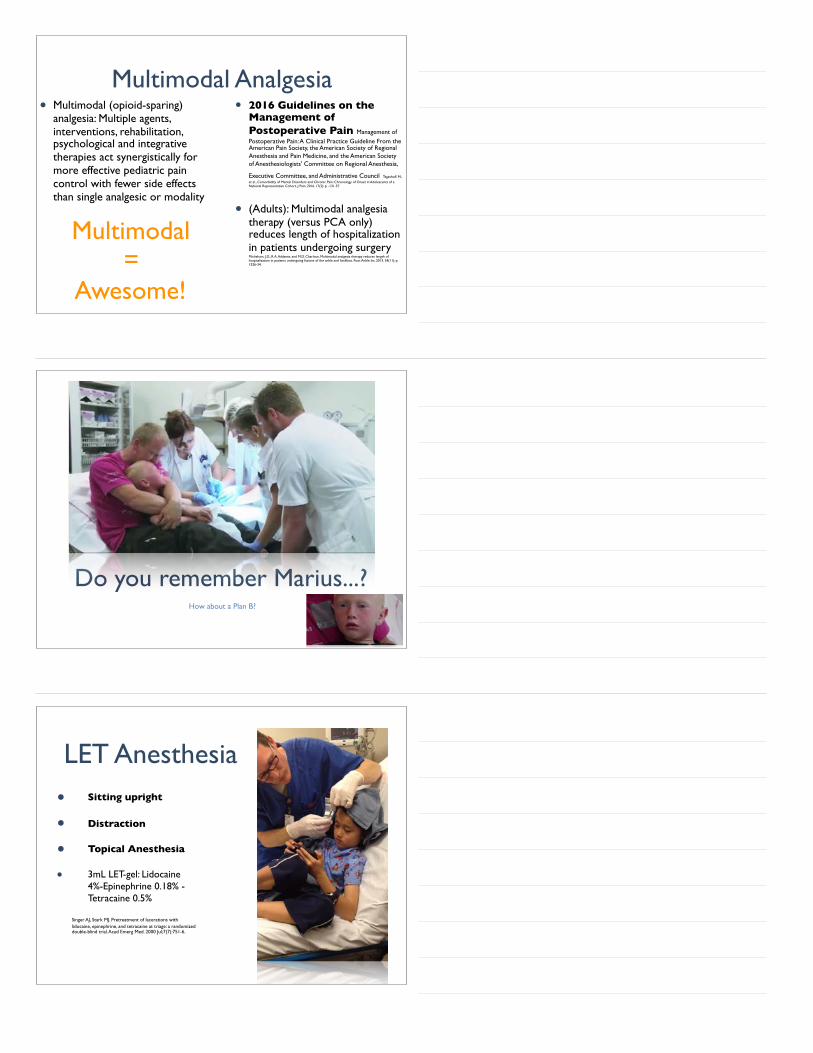
Aδ or C fiber
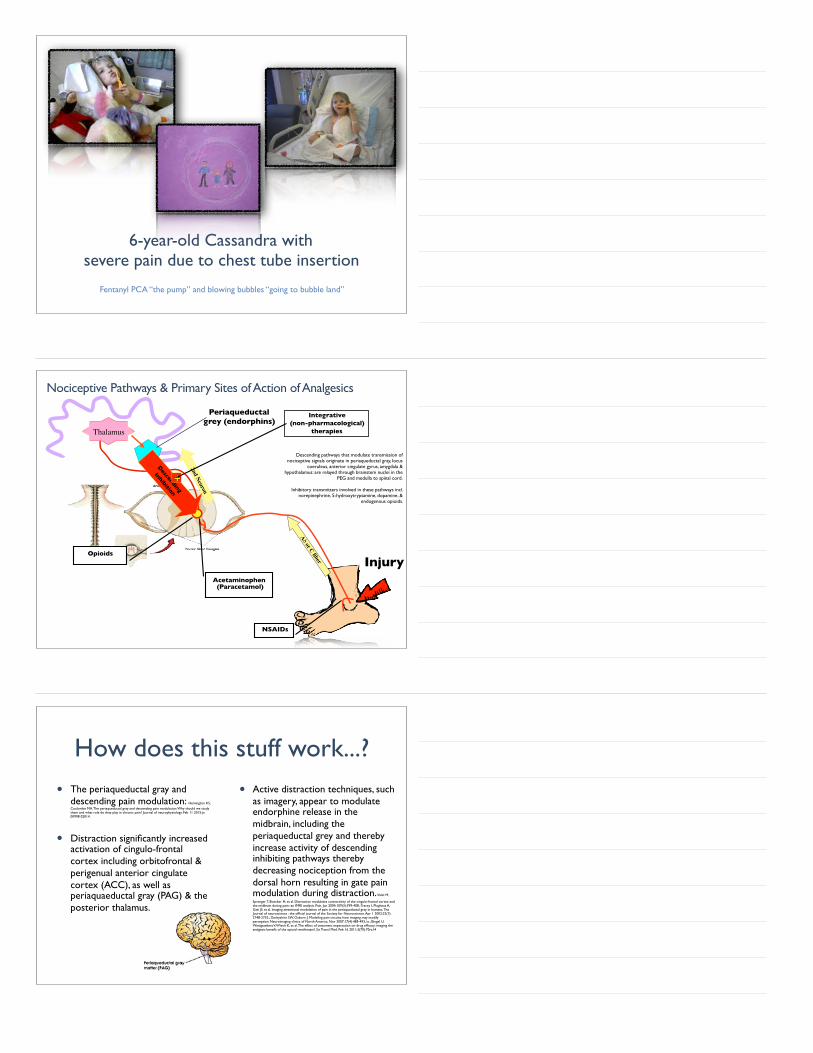
Nociceptive Pathways & Primary Sites of Action of Analgesics
Injury
Thalamus
NSAIDs
Acetaminophen (Paracetamol)
2nd Neuron

Citius, Altius, Fortius...?• Ibuprofen salts: fast-acting
formulations Moore, R.A., et al., Faster, higher, stronger? Evidence for formulation and efficacy for ibuprofen in acute pain. Pain, 2014. 155(1): p. 14-21.
• Advil® Film-Coated Tablets, contains 266 mg of ibuprofen sodium (equivalent to 200 mg of standard ibuprofen)
• Produced significantly better analgesia over 6h, fewer re-medications than standard formulations
• 200-mg fast-acting ibuprofen (NNT 2.1; 95% confidence interval 1.9-2.4) was as effective as 400 mg standard ibuprofen (NNT 2.4; 95% CI 2.2-2.5), with faster onset of analgesia.
• More rapid absorption, faster initial pain reduction, good overall analgesia in more patients at the same dose, and probably longer-lasting analgesia, but with no higher rate of patients reporting adverse events.
• However, earlier onset preferred in other pain condition, such as chronic nociceptive or neuropathic pain? Peloso, P.M., Faster, higher, stronger: to the gold medal podium? Pain, 2014. 155(1): p. 4-5.
WHO Principle 4: Using a Two-Step Strategy
WHO Step 1Mild Pain
Ibuprofenand/or
Acetaminophen(Paracetamol)
Other NSAIDs?Cox-2 Inhibitor?
Morphine
or fentanyl,
hydromorphone, oxycodone, methadone
(UK: diamorphine)
WHO Step 2Moderate to Severe Pain
Aδ or C fiber
Nociceptive Pathways & Primary Sites of Action of Analgesics
Injury
Thalamus
NSAIDs
Acetaminophen (Paracetamol)
2nd Neuron
Opioids
Opioids• Pre-synaptic nerve terminal
i Neurotransmitter release
• Post-synaptic nerve terminal:hMembrane hyperpolarization
=> suppress neuronal excitability

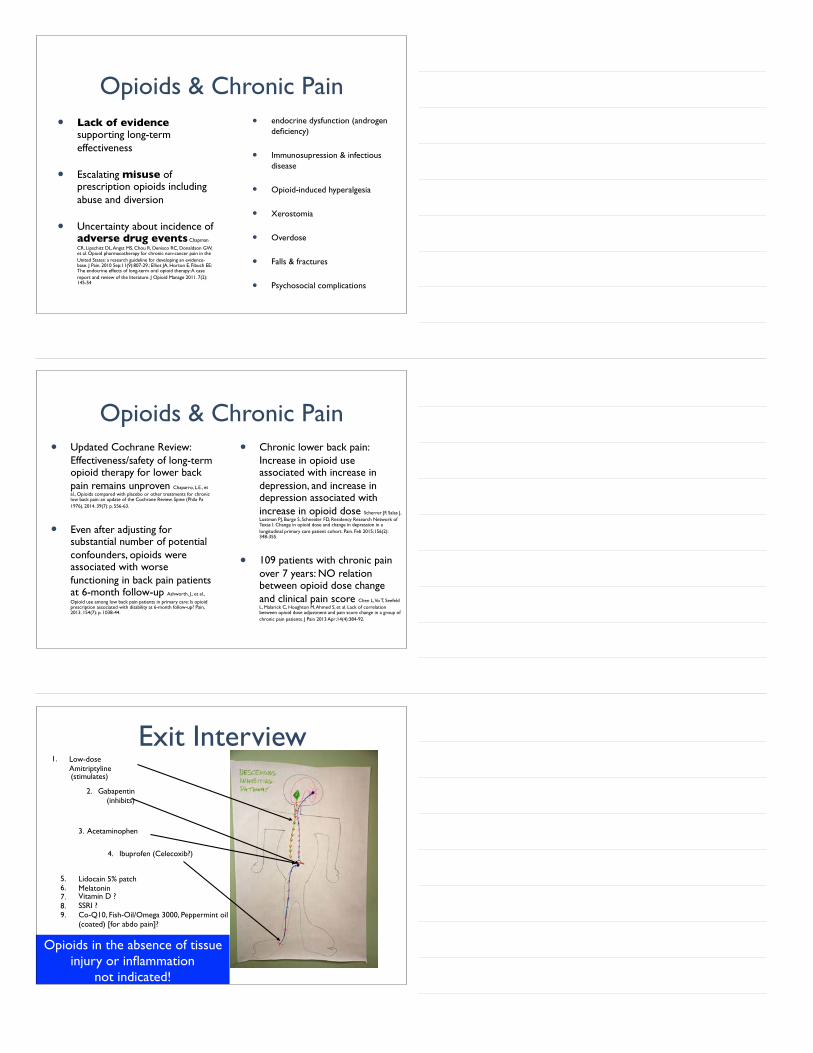
Non-Opioids• Acetaminophen / Paracetamol• NSAIDs
Multimodal (Opioid-sparing) Analgesia
Integrative TherapiesSuch as:• Massage• Distraction• Deep Breathing• Biofeedback• Aromatherapy• Hypnosis
Opioids• Tramadol („weak“)• Morphine („strong“)
4 WHO-Principles• “By the clock”
Integrative Pain ManagementState of the art pain management in the 21st century demands that pharmacological management must be combined with supportive and integrative, non-pharmacological therapies to manage a child's pain.
• Physical methods (e.g. cuddle/hug, massage, comfort positioning, heat, cold, TENS)
• Cognitive behavioral techniques (e.g. guided imagery, hypnosis, abdominal breathing, distraction, biofeedback)
• Acupuncture, acupressure, aromatherapy
Integrative Pain & Symptom Management
A Pediatrician’s Top 10 Apps for Distraction & Pain Management http://NoNeedlessPain.org
6-year-old Cassandra withsevere pain due to chest tube insertion
Fentanyl PCA “the pump” and blowing bubbles “going to bubble land”
Aδ or C fiber
Nociceptive Pathways & Primary Sites of Action of Analgesics
Injury
Thalamus
NSAIDs
Acetaminophen (Paracetamol)
2nd Neuron
Opioids
Periaqueductalgrey (endorphins)
Descending
Inhibition
+
Integrative (non-pharmacological)
therapies
Descending pathways that modulate transmission of nociceptive signals originate in periaqueductal gray, locus
coeruleus, anterior cingulate gyrus, amygdala & hypothalamus: are relayed through brainstem nuclei in the
PEG and medulla to spinal cord.
Inhibitory transmitters involved in these pathways incl. norepinephrine, 5-hydroxytryptamine, dopamine, &
endogenous opioids.
How does this stuff work...?
• The periaqueductal gray and descending pain modulation: Hemington KS,
Coulombe MA. The periaqueductal gray and descending pain modulation: Why should we study them and what role do they play in chronic pain? Journal of neurophysiology. Feb 11 2015:jn 00998 02014.
• Distraction significantly increased activation of cingulo-frontal cortex including orbitofrontal & perigenual anterior cingulate cortex (ACC), as well as periaquaeductal gray (PAG) & the posterior thalamus.
• Active distraction techniques, such as imagery, appear to modulate endorphine release in the midbrain, including the periaqueductal grey and thereby increase activity of descending inhibiting pathways thereby decreasing nociception from the dorsal horn resulting in gate pain modulation during distraction. Valet M,
Sprenger T, Boecker H, et al. Distraction modulates connectivity of the cingulo-frontal cortex and the midbrain during pain--an fMRI analysis. Pain. Jun 2004;109(3):399-408.; Tracey I, Ploghaus A, Gati JS, et al. Imaging attentional modulation of pain in the periaqueductal gray in humans. The Journal of neuroscience : the official journal of the Society for Neuroscience. Apr 1 2002;22(7):2748-2752.; Derbyshire SW, Osborn J. Modeling pain circuits: how imaging may modify perception. Neuroimaging clinics of North America. Nov 2007;17(4):485-493, ix.; Bingel U, Wanigasekera V, Wiech K, et al. The effect of treatment expectation on drug efficacy: imaging the analgesic benefit of the opioid remifentanil. Sci Transl Med. Feb 16 2011;3(70):70ra14
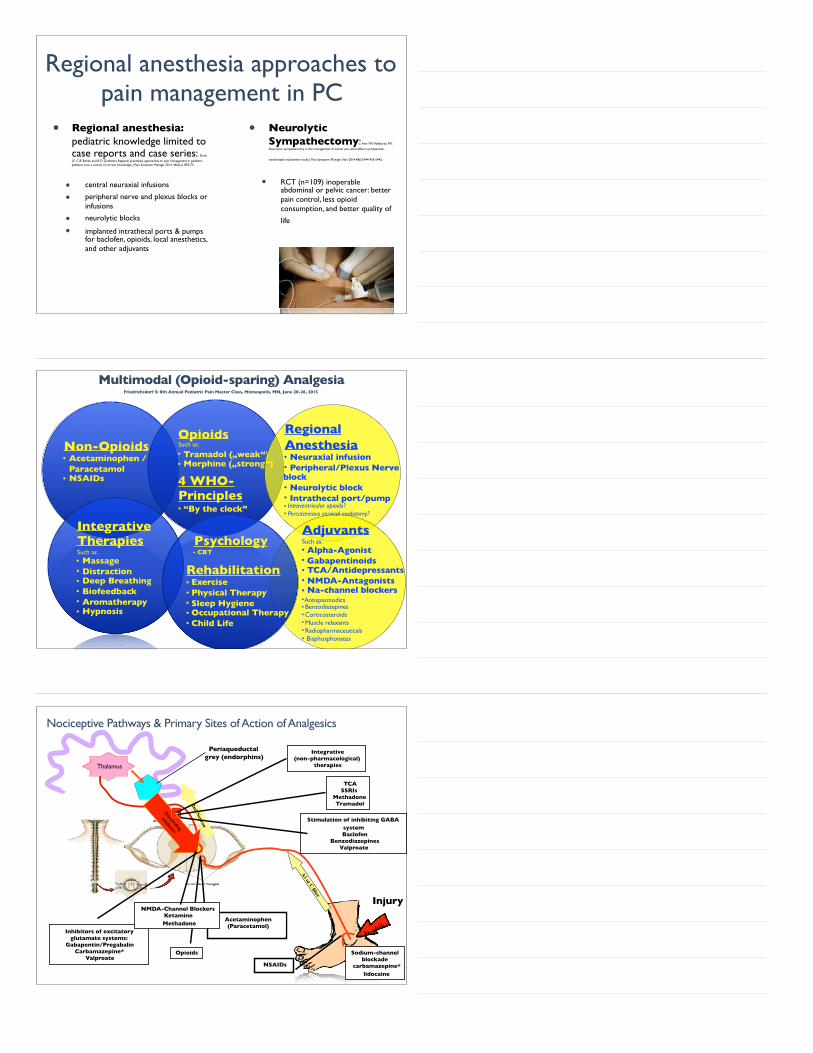
Regional anesthesia approaches to pain management in PC
• Regional anesthesia: pediatric knowledge limited to case reports and case series: Rork,
J.F., C.B. Berde, and R.D. Goldstein, Regional anesthesia approaches to pain management in pediatric palliative care: a review of current knowledge. J Pain Symptom Manage, 2013. 46(6): p. 859-73.
• central neuraxial infusions
• peripheral nerve and plexus blocks or infusions
• neurolytic blocks
• implanted intrathecal ports & pumps for baclofen, opioids, local anesthetics, and other adjuvants
• Neurolytic Sympathectomy: Amr YM, Makharita MY.
Neurolytic sympathectomy in the management of cancer pain-time effect: a prospective,
randomized multicenter study. J Pain Symptom Manage. Nov 2014;48(5):944-956 e942.
• RCT (n=109) inoperable abdominal or pelvic cancer: better pain control, less opioid consumption, and better quality of
life
Non-Opioids• Acetaminophen / Paracetamol• NSAIDs
Multimodal (Opioid-sparing) AnalgesiaFriedrichsdorf S: 8th Annual Pediatric Pain Master Class, Minneapolis, MN, June 20-26, 2015
Integrative TherapiesSuch as:• Massage• Distraction• Deep Breathing• Biofeedback• Aromatherapy• Hypnosis
OpioidsSuch as:
• Tramadol („weak“)• Morphine („strong“)
4 WHO-Principles• “By the clock”
AdjuvantsSuch as:• Alpha-Agonist• Gabapentinoids • TCA/Antidepressants• NMDA-Antagonists• Na-channel blockers• Antispasmodics• Benzodiazepines• Corticosteroids• Muscle relaxants• Radiopharmaceuticals • Bisphosphonates
Rehabilitation• Exercise• Physical Therapy• Sleep Hygiene• Occupational Therapy• Child Life
Psychology• CBT
Regional Anesthesia• Neuraxial infusion• Peripheral/Plexus Nerve block• Neurolytic block• Intrathecal port/pump• Intraventricular opioids?• Percutaneous cervical cordotomy?
Aδ or C fiber
Nociceptive Pathways & Primary Sites of Action of Analgesics
Injury
Thalamus
NSAIDs
Acetaminophen (Paracetamol)
2nd Neuron
Periaqueductalgrey (endorphins)
Descending
Inhibition
+
Integrative (non-pharmacological)
therapies
TCA SSRIs
Methadone Tramadol
Opioids
Inhibitors of excitatory glutamate systems:
Gabapentin/Pregabalin Carbamazepine*
Valproate
NMDA-Channel Blockers Ketamine Methadone
Stimulation of inhibiting GABA system
Baclofen Benzodiazepines
Valproate
Sodium-channel blockade
carbamazepine* lidocaine

• Pain lasting > 3-6 months: Time definition arbitrary
• Pain that extends beyond the expected period of healing • hence lacks the acute warning function of physiological nociception
Turk DC, Okifuji A. Pain terms and taxonomies of pain. In: Bonica JJ, Loeser JD, Chapman CR, Turk DC, Butler SH. Bonica's management of pain. Hagerstwon, MD: Lippincott Williams & Wilkins; 2001; Treede RD, Rief W, Barke A, et al. A classification of chronic pain for ICD-11. Pain. Jun 2015;156(6):1003-1007.
Chronic Pain in Children
Chronic-on-acute Pain
• Approximately 5% of children and teenagers in general population have significant pain related dysfunction King S, Chambers CT, Huguet A, MacNevin RC, McGrath PJ, Parker L, et al. The epidemiology of chronic pain in children and adolescents revisited: a systematic review. Pain. 2011 Dec;152(12):2729-38.
• In USA: > 3.7 million children
• USA - Age 0-17: 74.3 million children (2014): http://www.childstats.gov/americaschildren/tables/pop1.asp
• At least (!) 5 % of children with sickle cell disease, inflammatory bowel disease, rheumatoid arthritis, congenital heart disease, or cancer are expected to display chronic pain in addition to their underlying somatic pain episode
Transition from acute to chronic pain
• Chronic post surgical pain (CPSP) after Surgery: last at least 2 months, other causes were excluded
• 2-17 years: 13% Fortier, M.A., et al., Acute to chronic postoperative pain in children: preliminary findings. J Pediatr Surg, 2011. 46(9): p. 1700-5.
• 1 year after surgery, 22% of children developed moderate to severe CPSP with minimal functional disability. Page MG, Stinson J,
Campbell F, Isaac L, Katz J. Identification of pain-related psychological risk factors for the development and maintenance of pediatric chronic postsurgical pain. J Pain Res. 2013;6:167-180.
• 18% of children developed CPSP; associated with parental catastrophizing . Rabbitts, J.A., et al., Trajectories of postsurgical pain in children: risk factors and impact of late pain recovery on long-term health outcomes after major surgery. Pain, 2015. 156(11): p. 2383-9.

Communication with Patient / Family
• Pain is real!
• First “function” gets better, then “pain” (not other way around)
• Positive Expectation = Self-fulfilling prophecy
• Physical Therapy• Daily home exercise
• Integrative Medicine• Self-Hypnosis• Biofeedback• Progressive Muscle relaxation• Daily home exercise
• Passive: Massage, Acupuncture • Psychology (...if missing school)• Normalize Life
• Sports/Exercise• Sleep-hygiene• Social: Having daily fun• School: Attending full-time (or school-re-entry plan)
• Family Coaching• Medications...???
Communication with Patient / Family What is the Hard Work...and non-negotiable...?
Medications ???
Opioids & Chronic Pain• Lack of evidence
supporting long-term effectiveness
• Escalating misuse of prescription opioids including abuse and diversion
• Uncertainty about incidence of adverse drug events Chapman
CR, Lipschitz DL, Angst MS, Chou R, Denisco RC, Donaldson GW, et al. Opioid pharmacotherapy for chronic non-cancer pain in the United States: a research guideline for developing an evidence-base. J Pain. 2010 Sep;11(9):807-29.; Elliot JA, Horton E, Fibuch EE: The endocrine effects of long-term oral opioid therapy: A case report and review of the literature. J Opioid Manage 2011. 7(2): 145-54
• endocrine dysfunction (androgen deficiency)
• Immunosupression & infectious disease
• Opioid-induced hyperalgesia
• Xerostomia
• Overdose
• Falls & fractures
• Psychosocial complications
Opioids & Chronic Pain• Updated Cochrane Review:
Effectiveness/safety of long-term opioid therapy for lower back pain remains unproven Chaparro, L.E., et al., Opioids compared with placebo or other treatments for chronic low back pain: an update of the Cochrane Review. Spine (Phila Pa 1976), 2014. 39(7): p. 556-63.
• Even after adjusting for substantial number of potential confounders, opioids were associated with worse functioning in back pain patients at 6-month follow-up Ashworth, J., et al.,
Opioid use among low back pain patients in primary care: Is opioid prescription associated with disability at 6-month follow-up? Pain, 2013. 154(7): p. 1038-44.
• Chronic lower back pain: Increase in opioid use associated with increase in depression, and increase in depression associated with increase in opioid dose Scherrer JF, Salas J, Lustman PJ, Burge S, Schneider FD, Residency Research Network of Texas I. Change in opioid dose and change in depression in a longitudinal primary care patient cohort. Pain. Feb 2015;156(2):348-355.
• 109 patients with chronic pain over 7 years: NO relation between opioid dose change and clinical pain score Chen L, Vo T, Seefeld L, Malarick C, Houghton M, Ahmed S, et al. Lack of correlation between opioid dose adjustment and pain score change in a group of chronic pain patients. J Pain 2013 Apr;14(4):384-92.
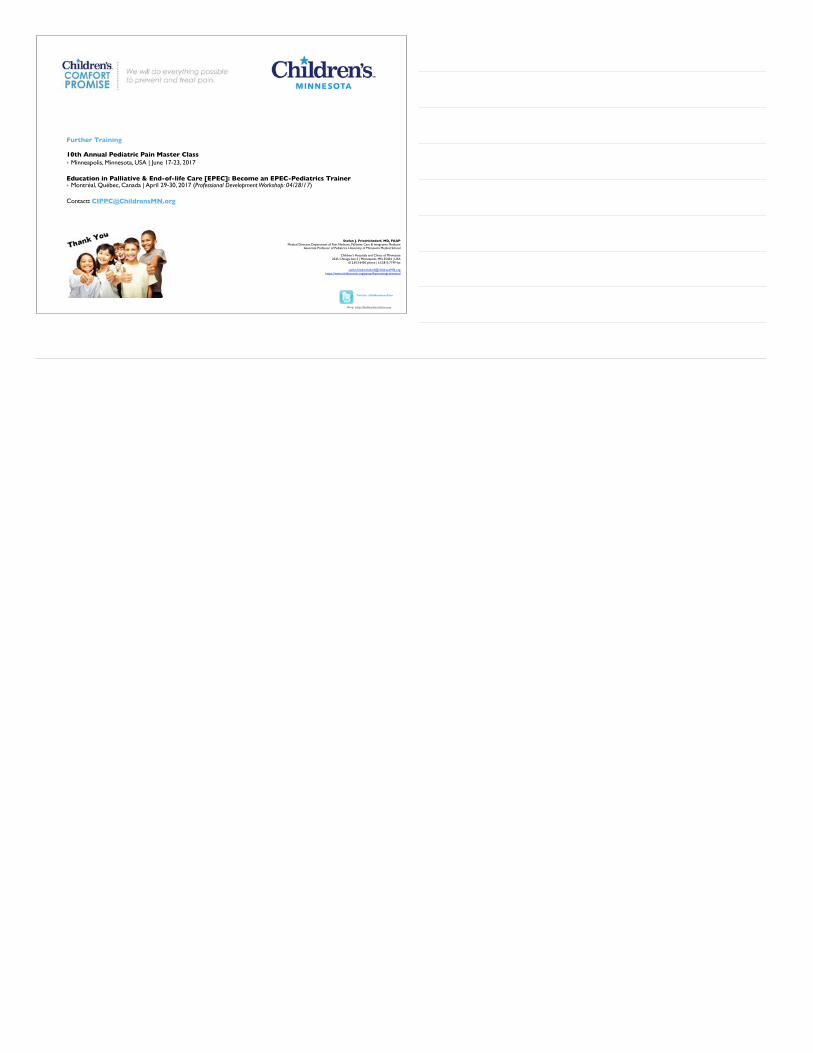
1. Low-dose Amitriptyline(stimulates)
Opioids in the absence of tissue injury or inflammation
not indicated!
2. Gabapentin(inhibits)
3. Acetaminophen 4. Ibuprofen (Celecoxib?)
5. Lidocain 5% patch6. Melatonin7. Vitamin D ?8. SSRI ?9. Co-Q10, Fish-Oil/Omega 3000, Peppermint oil
(coated) [for abdo pain]?
Exit Interview
Multimodal Analgesia• Multimodal (opioid-sparing)
analgesia: Multiple agents, interventions, rehabilitation, psychological and integrative therapies act synergistically for more effective pediatric pain control with fewer side effects than single analgesic or modality
• 2016 Guidelines on the Management of Postoperative Pain Management of Postoperative Pain: A Clinical Practice Guideline From the American Pain Society, the American Society of Regional Anesthesia and Pain Medicine, and the American Society of Anesthesiologists' Committee on Regional Anesthesia,
Executive Committee, and Administrative Council Tegethoff, M.,
et al., Comorbidity of Mental Disorders and Chronic Pain: Chronology of Onset in Adolescents of a National Representative Cohort. J Pain, 2016. 17(2): p. -131-57
• (Adults): Multimodal analgesia therapy (versus PCA only) reduces length of hospitalization in patients undergoing surgery Michelson, J.D., R.A. Addante, and M.D. Charlson, Multimodal analgesia therapy reduces length of hospitalization in patients undergoing fusions of the ankle and hindfoot. Foot Ankle Int, 2013. 34(11): p. 1526-34.
Multimodal=
Awesome!
Do you remember Marius...?How about a Plan B?
LET Anesthesia• Sitting upright
• Distraction
• Topical Anesthesia
• 3mL LET-gel: Lidocaine 4%-Epinephrine 0.18% -Tetracaine 0.5%
Singer AJ, Stark MJ. Pretreatment of lacerations with lidocaine, epinephrine, and tetracaine at triage: a randomized double-blind trial. Acad Emerg Med. 2000 Jul;7(7):751-6.

74
54.0%
56.0%
58.0%
60.0%
62.0%
64.0%
Q3 2014Q4 2014Q1 2015Q2 2015Q3 2015
Picker Systemwide: Pain controlled all the time
63.6%63.7%
59.9%
56.9%
55.2%
Usually/Always 91.8% 91.7% 90.7% 93.6% 93.9%
Locationssurveyed:Surgery,NICU,SCN,ICC,ED&Med/Surg,CriticalCareRoll-out
IV Access Under Nitrous Gas22 months-old, Lidocaine 4% cream in place, needed IV for radiologic procedure, history of challenging IV access in the past
Thanks to Patricia D. Scherrer MD, Medical Director, Sedation ServicesChildren's Hospitals and Clinics of Minnesota
Crystal clear answer:
So, how do we treat the individual pain patient in front of us ?
Σωκράτη Sōkrátēs; 470/469 – 399 BC

Pain
WithdrawalDelirium
Nociceptive Pain
Neuropathic Pain
Visceral Pain
Psychological pain
Anxiety
Depression
Spiritual Pain
Social Pain
Chronic Pain
Poor sleep hygiene
Mental Health
School absenteeism
Total Pain
Deconditined
Racial Disparity
Conclusions• Withholding evidence-based
analgesia to hospitalized infants / children in pain not only unethical, but causes immediate and long-term harm
• Potential risks in safety of analgesics are real, but manageable; cannot justify denying administration of pain medications to pediatric patients
• Use multimodal (opioid-sparing) analgesia: Multiple agents, interventions, rehabilitation, psychological and integrative therapies act synergistically for more effective pediatric pain control with fewer side effects than single analgesic or modality
Further Links• The New York Times (Dec 16, 2015) essay by Dr. Stefan Friedrichsdorf “When a Baby Dies” http://
opinionator.blogs.nytimes.com/2015/12/16/when-a-baby-dies/?_r=1
• Video: Kiran Stordalen and Horst Rechelbacher Pediatric Pain, Palliative and Integrative Medicine Clinic Tour https://vimeo.com/122654881
• “Children’s Comfort Promise: Doing everything possible to treat and prevent pain.” Eliminating Needle Pain in children (Feb 2015) Staff video: http://vimeo.com/106286508
• Short Movie: Meet the Interdisciplinary Chronic Pain Clinic Team at Children’s Minnesota: LittleStars TV https://www.youtube.com/watch?t=13&v=Bb1fHxfjdWI
• Video: Tour of the Kiran Stordalen and Horst Rechelbacher Pediatric Pain, Palliative and Integrative Medicine Clinic at Children's Hospitals and Clinics of Minnesota and an overview of the three programs that are offered at Children's under this clinic. https://vimeo.com/123357296
• Short Movie: LittleStarsFilm 'Kali's Story - Beyond the NICU': This amazing pediatric palliative care short movie (7 min) features 8-year-old Kali's journey at Children's Hospitals and Clinics of Minnesota from NICU to today, receiving care by the Pain & Palliative & Integrative Medicine program while inpatient, in the clinic, and at home (Jan 22, 2015) http://www.littlestars.tv/short-films/beyond-the-nicu
Twitter: @NoNeedlessPain
Stefan J. Friedrichsdorf, MD, FAAP Medical Director, Department of Pain Medicine, Palliative Care & Integrative Medicine
Associate Professor of Pediatrics, University of Minnesota Medical School
Children's Hospitals and Clinics of Minnesota2525 Chicago Ave S | Minneapolis, MN 55404 | USA
612.813.6450 phone | 612.813.7199 fax
[email protected]://www.childrensmn.org/painpalliativeintegrativemed
Further Training
10th Annual Pediatric Pain Master Class • Minneapolis, Minnesota, USA | June 17-23, 2017
Education in Palliative & End-of-life Care [EPEC]: Become an EPEC-Pediatrics Trainer• Montréal, Québec, Canada | April 29-30, 2017 (Professional Development Workshop: 04/28/17)
Contact: [email protected]
Blog: http://NoNeedlessPain.org