pressure ulcers evidenced based presentation michelle scarlett
TRANSCRIPT

Pressure Ulcers
Evidenced Based Presentation
Michelle Scarlett

Purpose and Objective of presentation
• Educate about Pressure Ulcers and it’s presentation• Introduce a case scenario• Preventable Measures• Current treatment/intervention • Gaps in reducing frequency• Encouraging the use of current methods

Video on Pressure Ulcershttp://www.youtube.com/watch?v=Eyuguc7KKC4

Statistics• “Pressure ulcers are the 3rd most costly complications following
cancer and cardiovascular disease”• Incidence rate 0.4-38 % and prevalence has been reported to be 3.5 -
69%• The acceptable incident rate is less than 2%• 2/3 of pressure sores occur in the elderly above 70 years of age• In spinal cord injury patients, pressure ulcers occur in 30-85 % of
patients in the first month of injury.• Paraplegics and quadriplegics are likely to have multiple ulcers.• The National Pressure Ulcer Advisory Panel reported in 2005 a
68.8% mortality rate in the elderly with stage 3-4 pressure ulcers, because of secondary systemic complications.

Case scenario
HPI: Patient was a 64 year old white female diagnosed with Alzheimer's. She presented to the hospital on October 4, 2012 from her nursing home, following an obstructed bowel for which she had to have surgery. At the time of her assessment it was noted that the patient had a stage 3 pressure ulcer of her left buttocks that was progressively turning into a stage 4 ulcer. The patient was about 250 lbs with impaired mobility of her lower extremities. She was listed to be repositioned every two hours and have her wound flushed with saline solution to assist with healing. However, instead of the ulcer getting better the ulcer got worst. According to the doctor's notes it appears that client wasn’t being repositioned in the nursing home as often as she should have and the conditioned may have continued to get worst if someone didn’t take note to the fact that she hadn’t had a bowel movement in almost a week.

PathophysiologyA pressure ulcer is an irregularly shaped, depressed area that results from necrosis of the epidermis and/or dermis layers of the skin. Prolonged pressure causes inadequate circulation, ischemic ulceration, and tissue breakdown. Muscle tissue seems particularly susceptible to ischemia. Pressure ulcers may occur in any area of the body but occur mostly over bony prominences that can include the occiput, thoracic and lumbar vertebrae, scapula, coccyx, sacrum, greater trochanter, ischial tuberosity, lateral knee, medial and lateral malleolus, metatarsals, and calcaneus. Some 96% of pressure ulcers develop in the lower part of the body, with the hip and buttock region accounting for almost 70% of all pressure sores.

Other Names
• Bed sores• Decubitus ulcers• Decubiti• Pressure sores


Stages• Stage I- Nonblanchable erythema; involves changes in the
underlying vessels of the skin; bright red color that does not resolve after 30 min of pressure relief; can be painful and tender
• Stage II- Partial thickness skin loss of epidermis and dermis; cracks or blisters on skin with erythema and/or indurations
• Stage III- Full-thickness skin loss of epidermis and dermis; extends down to subcutaneous tissue; appears as a crater or covered by black eschar, wound base usually not painful; indistinct borders; may have sinus tracts or undermining present.
• Stage IV- Full-thickness skin loss with extensive destruction of tissue, muscle, bone, and/or supporting structures; appears as a deep crater or is covered by thick eschar; wound base not painful; may have sinus tracts and undermining present
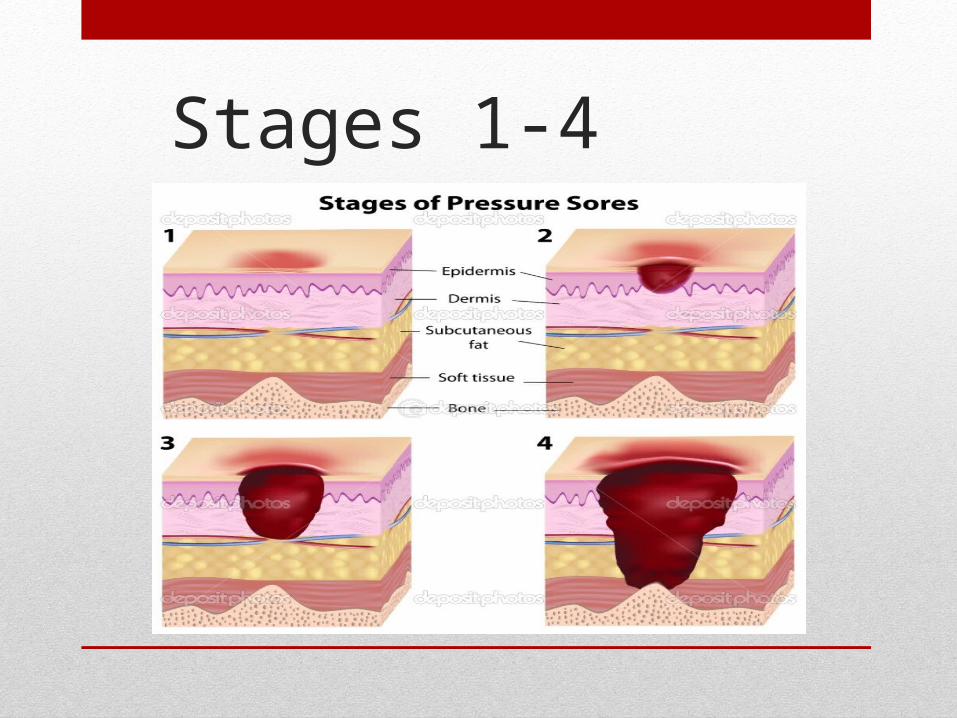
Stages 1-4

Other Stages
• Suspected deep tissue injury-Area of localized, discolored intact skin that is purple or maroon-red in color. It may also appear as a blood-filled blister resulting from damage to underlying soft tissue. Preceding skin changes may include skin that is painful, firm, boggy, or that has a different temperature compared to the surrounding skin

Other Stages
Unstageable-Full-tissue thickness loss in which the base of the ulcer is covered by slough or an eschar and, therefore, the true depth of the damage cannot be estimated until these are removed.
At Risk Patients
• Bedridden- limited mobility
• Incontinent-moisture causes maturation of skin
• Obese-more weight bearing on bony prominences
• Poor nutrition-balance of vitamins-C, Zinc and other trace minerals
• Mobility is impaired-failure to make postural changes
• Cognitively impaired to state need for change and repositioning
• I “As a nurse you have to do skin inspections!”

Nursing Diagnoses
• Ineffective peripheral tissue perfusion related to reduced interrupted blood flow as evidenced by presence of inflamed, necrotic lesions.

Pressure Ulcers affect and can cause• Increased hospital stay• Patients more prone to infections• Loss of self-esteem• Loss of earnings• Amputation• Death
Medical and Nursing Interventions and Care Guidelines from current research literature supporting international best practice of Repositioning !!!
• Study: Randomized study on 213 Irish and white patients from 12 long-term hospital settings at risk of developing pressure ulcers. 77% were women, 65 % over 80 years old. 70 % low risk of malnutrition. 77% limited activity. 79 % bed ridden.
• Data: Braden scale-risk assessment, MUST- nutrition, EPAUP-classification
• Results: 3 (3%) patients in the experimental group and 13 (11%) in the controlled group developed a pressure ulcer.
• Conclusion: Repositioning older adults at risk of pressure ulcers every three hours at night, using the 30 degree tilt, reduces the incidence of ulcers. The study supports the intervention that repositioning patients is a vital preventive method in avoiding pressure ulcers.
• Study based on: http://www.pressureulcerguidelines.org/therapy/

30 degree tilt versus 90 degree tilt

Medical and Nursing Interventions and Care Guidelines from current research literature supporting
• The objective of this study was to evaluate the effects of nutrition intervention on nutritional states and healing of pressure ulcers by standardizing or unified factors including nursing, care and treatment in a multicenter open randomized trial.
• Tube-fed patients with Stage III-IV pressure ulcers were selected. The control group (30 patients) received the same nutrition management as before participating in this trial, whereas the intervention group (30 patients) was given calories in the range of Basal Energy Expenditure (BEE) × 1.1 × 1.3 to 1.5. The intervention period was 12 weeks. The efficacy and safety were evaluated based on the nutritional states and the sizes of ulcers (length × width), and on the incidence of adverse events related to the study, respectively. The calories administered to the control and intervention groups were 29.1±4.9 and 37.9±6.5 kcal/kg/day, respectively. Significant interactions between the presence or absence of the intervention and the intervention period were noted for nutritional states ( p<0.001 for body weight, p<0.05 for prealbumin). Similarly, the size of ulcers differed significantly between subjects in the intervention group and in the control group ( p<0.001). The results suggest that nutrition intervention could directly enhance the healing process in pressure ulcer patients.
Medical and Nursing Interventions and care guidelines as applied to specific patient• Pressure Ulcer Classification- Stage 3• Debridement- Removing dead tissues• Assessment, Monitoring & Cleansing- to prevent urine and feces from
entering the wound• Nutrition for Healing- increase protein, vitamin and calorie intake• Pain Assessment & Management-medication- diazepam, baclofen, or
dantrolene sodium• Support Surfaces for Treatment-pillows to relieve pressure on the
opposite side and between bony prominences and air birds• Dressings-Hydrocolloid dressings (DuoDerm)• Biophysical Agents • Negative Pressure Wound Therapy • Growth Factors & Biological Dressings

Gaps
• More research needs to be completed regarding the right intervals to reposition patients to reduce their risk of pressure ulcers.
• Studies needs to be focus on the situation of the patient and how to reduce prevalence in their case, as current intervention may not be as effective for all bedridden individuals.

Pertinent NCLEX style Questions• You are caring for a patient and noticed a superficial
ulcer on the patient’s buttock that appears as a shallow crater involving the epidermis and the dermis. Which of the following stages would you say best describes this break in skin integrity?
• Stage I• Stage II• Stage III• Stage IV

Pertinent NCLEX style Questions
Which of the following interventions is most appropriate for preventing pressure ulcers in a bedridden elderly client?
1. Slide instead of lift the client when turning.
2. Turn and reposition the client at least every 8 hours.
3. Apply lotion after bathing the client, and vigorously massage her skin.
4. Post a turning schedule at the client's bedside, and adapt position changes to her situation.

Don’t forget!!- people who can’t turn themselves need your help!!
References
• Agrawal, K., & Chauhan, N. (2012). Pressure ulcers: Back to the basics. Indian Journal Of Plastic Surgery, 45(2), 244-254.
• Moore, Z., Cowman, S., & Conroy, R. (2011). A randomised controlled clinical trial of repositioning, using the 30° tilt, for the prevention of pressure ulcers. Journal Of Clinical Nursing, 20(17/18), 2633-2644. doi:10.1111/j.1365-2702.2011.03736.x
• Ohura, T., Nakajo, T., Okada, S., Omura, K., & Adachi, K. (2011). Evaluation of effects of nutrition intervention on healing of pressure ulcers and nutritional states (randomized controlled trial). Wound Repair & Regeneration, 19(3), 330-336. doi:10.1111/j.1524-475X.2011.00691.x
• Unbound Medicine-Disease and Disorders-http://nursing.unboundmedicine.com/nursingcentral/ub/view/Diseases-and-Disorders/73697/all/Pressure_Ulcer

Questions?????