presented by dr. jameel t miro. does trauma management differ for the pregnant ? yes no physiologic...
TRANSCRIPT

Trauma In Pregnancy
Two for One: Caring for the Pregnant Trauma Patient
Presented by DR. Jameel T Miro

Does trauma management differ for the pregnant ?
Yes No
Physiologic and Anatomic changes of pregnancy
Two patients requiring treatment!!!
ATLS Protocol the same
Priorities same
as in non-pregnant patient

What is the Incidence and why its an important topic ?The Leading cause of non-obst. mortality
-46%Trauma during pregnancy – 10%So many morbidities
Preterm Labor in 11.4 % P. Abruption in 1.58 %
Dead Mother = Dead FetusMost common cause of fetal death from
trauma is maternal death

What is the types of trauma? Causes of Trauma
MVA 54.6 %
Domestic abuse & Assault 22.3%
Falls 21.8 %
Penetrating inj.1.3 %
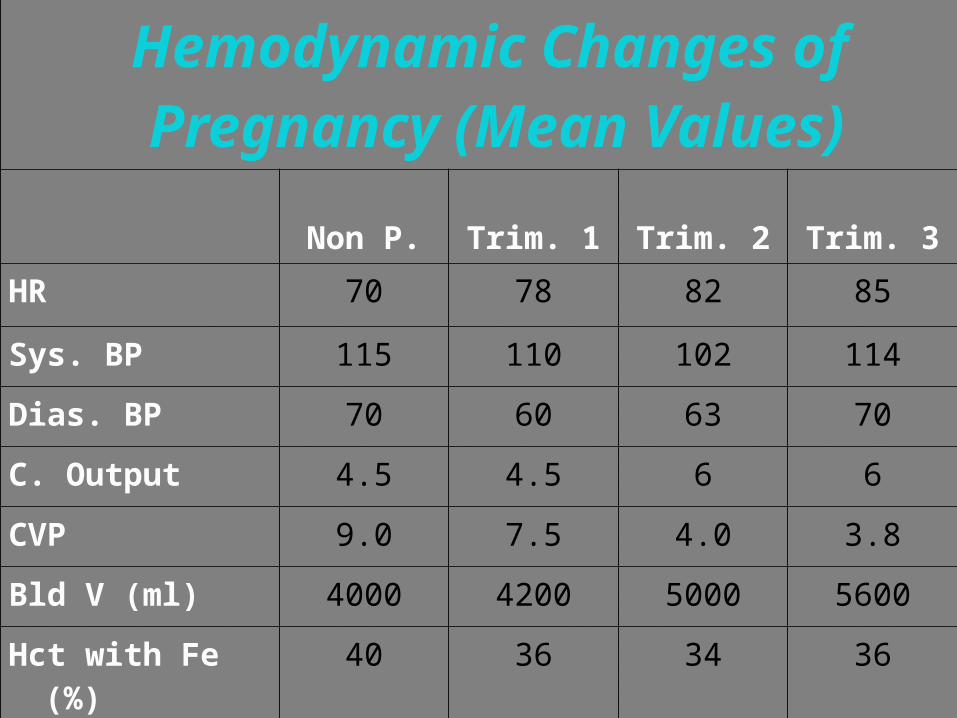
Hemodynamic Changes of Pregnancy (Mean Values)
Non P. Trim. 1 Trim. 2 Trim. 3
HR 70 78 82 85
Sys. BP 115 110 102 114
Dias. BP 70 60 63 70
C. Output 4.5 4.5 6 6
CVP 9.0 7.5 4.0 3.8
Bld V (ml) 4000 4200 5000 5600
Hct with Fe (%) 40 36 34 36
WBC (cell/mm3 ) 7200 9100 9700 9800

Anatomic changesIntestinal tract is displaced upward and posterior
As gestation continues the uterus becomes more vulnerable as the walls thin and there is less protection by amniotic fluid

Why we should know the physiological changes in pregnancy
Normal pregnant vital signs mimic hypo perfusion
Assessment more difficultFetus can be in distress while mother appears stable
Retroperitoneal bleeding more common to non pregnant.

What is the approach? AIRWAY + SPINErecall the increased risk of aspiration
consider early endotracheal intubation.
assume full stomach sellick’s maneuver

Breathing
auscultate for breath sounds and pulse oximetry
A chest tube thoracostomy : placed 1 or 2 intercostal spaces higher than usual to avoid diaphragmatic injury.
By 3rd trimester increase the need of oxygen 10-20%
Fetal oxygenation may be comprmized Exlude the lethal causes : tension
pnemothorax , flail chest etc.
CirculationAssess maternal circulation + IV access
If greater than 20 weeks’ gestation should be placed in the left-lateral decubitus position
Early crystalloid fluid replacement
fetal distress maybe the first sign of maternal hemodynamic compromise ( so it’s a vital sign )

secondary surveyHEAD TO TOE include the back Remember the Baby (fetal assessment)
CTG at least 4 hrPregnancy history Fundal height The uterus for tenderness and
contractionssterile speculum examinationThe cervix

What is the radiographic diagnostic modalities ?
Plain Films – X-raysUltrasoundCT & MRICardiotocographic MonitoringDPLLaparotomy

Radiographic risks Risk of 1 rad to fetus is approx. 0.003
< 5-10 rads causesNo risk on congenital malformation, abortions or intra-uterine growth ret.
Smaller risk of increase in childhood cancer
Radiation doses > 10 rads6 % chance of severe mental ret.< 3 % chance childhood cancer.

Ultrasound
Best modality to assess both fetus and mother
Not sensitive:Colonic lesionsBiliary tree lesionsSub-placental hematoma
Safe procedure

FAST?? How much fluid can FAST detect? 250 cc total 100 cc in Morison’s pouch
Does FAST replace CT?
Only at the extremes. Unstable patient, (+) FAST OR Stable patient, low force injury, (-) FAST
consider observing patient.

CT SCAN Complementary to U/S & DPL
Penetrating wounds of flank & back
Can miss diaphragmatic and bowel injuries
Spiral CT reduces radiation exposure by 14-30 %

Diagnostic peritoneal lavageCT & U/S are better in stable patient.
Hypotensive unstable pt. Can be performed in any trimester Gravid uterus does not reduce the accuracy of DPL for OR
does not assess retroperitoneal hemorrhage or intra-uterine pathology

Special consedrationFetomaternal HemorrhageAbruptio PlacentaRuptured Uterus Penetrating Injury If below
uterine fundus visceral injury less likely (0%) Fetal death rate is 67%
Stabbing Injury Rare, only 19 cases reported in literature ( Laprotomy)
Injury Severity Scorehead, face, thorax, abdomen, extremities
(incl. pelvis).1 Minor, 2 Moderate, 3 Serious, 4
Severe, 5 Critical, 6 Maximal (currently untreatable).
ISS = A^2 + B^2 + C^2 A Polytrauma is defined as ISS >= 16Indication of severity , prognosis and
hospital stay

Perimortem Cesarean Section ~200 successful cases reported in the
literature
Maternal CPR <5 minutes, fetal survival excellent
<23 weeks gestation survival chance is 0%
Maternal CPR >20 minutes, fetal survival unlikely

summeryABC secondary survey ….. Fetous !!Limit radiation to 5 radsHigh index of suspicion for abruptio placenta.
If mother unstable or arrested , with viable fetous conider primortem c/s !!!

Remember
What is Best for the Mother is Best for the
Fetus!

Thank you