presented by corbin wilson, executive director, jps physician group tammy walsh, director of...
TRANSCRIPT
Presented by Corbin Wilson, Executive Director, JPS Physician GroupTammy Walsh, Director of Finance, JPS Physician Group
Considerations of Integrating Physician Group Operations
and some suggestions on how to get it right!

2

3
a CPA/consulting group,
conducted a study in response to a clear need and
current trends. Nearly every health system and hospital
their healthcare team interacted with has recently
acquired physician groups, is actively seeking to acquire
them, or both. Yet, nearly every health system and
hospital with integrated physician groups is realizing
substantial operating losses from those groups.
An Integration Trends Study

4
The Survey
• The survey included 80 hospitals/ health systems• The survey had 30 questions and
was taken using Survey Monkey• The survey was broken down into
4 sections Background Structure Operations Opinions

5
Analyzing the data
Once they received all the responses, they analyzed the answers from each as it related to
the question…
“What is your average annual
loss per physician?”
6
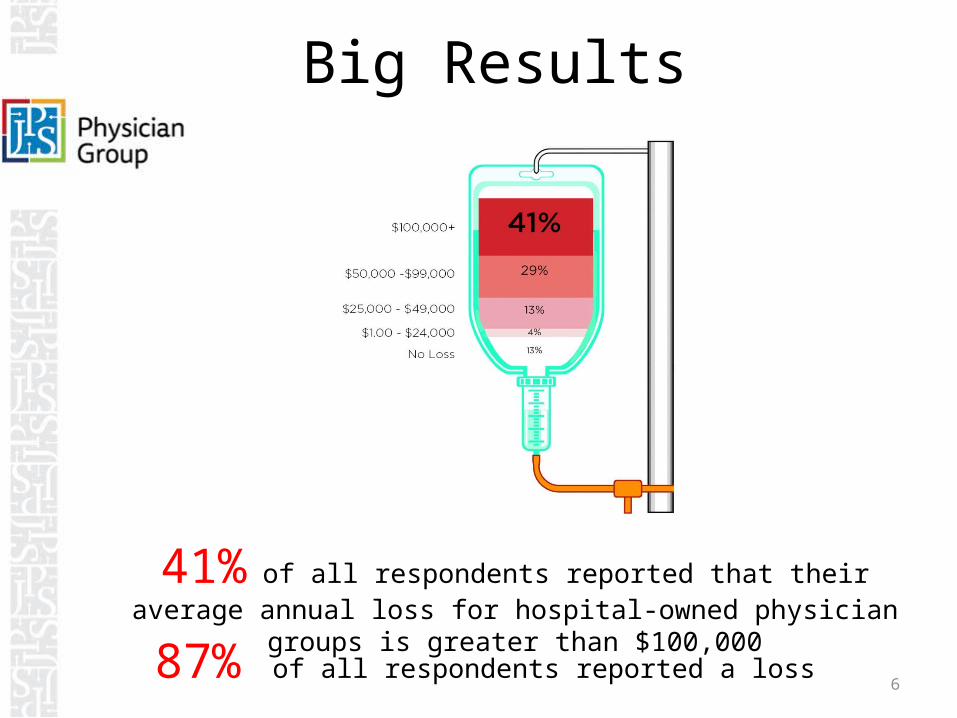
41% of all respondents reported that their average annual loss for hospital-owned physician groups is greater
than $100,00087% of all respondents reported a loss
Big Results
7
Other stats from the study
When it came to losses…• The size of the hospital didn’t
matter• The more physicians
employed, the more likely operating losses became
• Length of contracts did not impact results
• Method of physician compensation had little impact
When it came to Governance . . .
8
Less than a quarter of respondents reported that their hospital had a unique
board of directors that oversaw the operations of the
physician group(s)• Autonomy
• Engagement
• Control• Management
9
Does every physician group acquisition need
to have a positive bottom line to be beneficial to
hospitals?
10
Not necessarily….But hospitals need to manage these practices as effectively as they can. Hospitals benefit from the tradeoff of
additional revenue streams to the hospital for losses on employed
physicians; as compensation criteria changes, that tradeoff becomes less
sustainable
11
87% reported losses
41% losses over
$100K
Why are hospitals losing money on physician
groups?
70% losses over $50K
12
• Employing specialty and sub specialty physicians to meet needed service gaps
• Employing whomever is available, not necessarily following a strategy
• Employing for clinical quality support of other providers and the hospital
• Lack of leadership or professional practice management experience
• Enticing employment with unsustainable initial compensation & benefits
• Failure to take advantage of non-clinical other revenue sources/programs available to provider groups
Because . . .

13
The compensation model does not drive profitable results or includes unaligned incentives

14
Compensation Model Flaws
• The model needs to incentivize volumes of patient delivery and the payor mix; physicians work harder and smarter with correct productivity goals
• Negotiated compensation is not realistic to actual market forces; minimum base is too high, productivity incentives are too rich, or additional non-productivity compensation builds up
15
Compensation Model Flaws
• Pure productivity based compensation without regard to actual collections and cost often result in unfavorable financial results
• Discipline to communicate and adjust annual plan for lower results, including terminating underperformers, is sometimes lacking
16
Understand Operations
• Operations can become disjointed or hospital-centric; the business of physician practices differs from the hospital
• Billing, Payor Contracting, Credentialing, Collections for Professional Services
• Hospital/Provider based billing and global billing• Integration of computer systems for EHR, billing, and
practice management
17
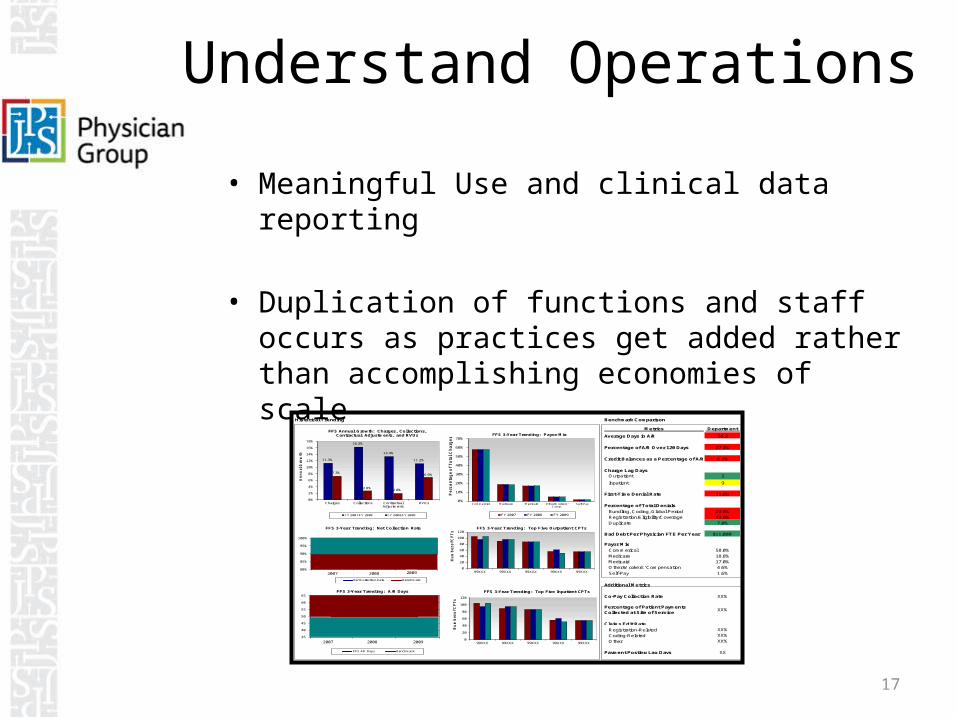
Understand Operations
• Meaningful Use and clinical data reporting
• Duplication of functions and staff occurs as practices get added rather than accomplishing economies of scale
Historical Trending Benchmark Comparison
Metrics Department
Average Days in A/R 56.2
Percentage of A/R Over 120 Days 27.1%
Credit Balances as a Percentage of A/R 6.4%
Charge Lag DaysOutpatient 2
Inpatient 9
First-Time Denial Rate 11.0%
Percentage of Total Denials
Bundling, Coding, Global Period 20.0%
Registration/Eligibility/Coverage 42.0%
Duplicate 7.0%
Bad Debt Per Physician FTE Per Year $11,000
Payor Mix
Commerical 58.0%
Medicare 18.8%
Medicaid 17.0%
Other/Workers' Compensation 4.6%
Self-Pay 1.6%
Additional Metrics
Co-Pay Collection Rate XX%
Percentage of Patient Payments Collected at Site of Service
XX%
Claims Edit Rate
Registration-Related XX%
Coding-Related XX%
Other XX%
Payment Posting Lag Days XX
11.3%
16.3%
13.4%
11.2%
7.3%
2.8%2.0%
6.9%
0%
2%
4%
6%
8%
10%
12%
14%
16%
18%
Charges Collections ContractualAdjustments
RVUs
An
nu
al G
row
th
FFS Annual Growth: Charges, Collections, Contractual Adjustments, and RVUs
FY 2007/FY 2008 FY 2008/FY 2009
80%
85%
90%
95%
100%
0 0
FFS 3-Year Trending: Net Collection Rate
Net Collection Rate Benchmark
2007
35
40
45
50
55
60
65
0 0
FFS 3-Year Trending: A/R Days
FFS AR Days Benchmark
0%
10%
20%
30%
40%
50%
60%
70%
Commercial Medicare Medicaid Other/Workers'Comp.
Self-Pay
Pe
rc
en
tag
e o
f T
ota
l C
ha
rg
es FFS 3-Year Trending: Payor Mix
FY 2007 FY 2008 FY 2009
0
20
40
60
80
100
120
99XXX 99XXX 99XXX 99XXX 99XXX
Nu
mb
er o
f C
PT
s
FFS 3-Year Trending: Top Five Outpatient CPTs
0
20
40
60
80
100
120
99XXX 99XXX 99XXX 99XXX 99XXX
Nu
mb
er o
f C
PT
s
FFS 3-Year Trending: Top Five Inpatient CPTs
2007 2008 2009
2008 2009
18
Physicians Experience
• Administrative, management, and billing functions less efficient than promised
• Confusing compensation model with data integrity concerns
• Equity (Financial) issues and Quality issues among employed physicians
• IT solutions lacking• Decision rights and integration in Health System
confusing – lack of practice autonomy• Limited ability for physician to implement
necessary changes – you are now an employee!

19
Physician Integration done right!
20
Understanding what the physician & group values and its goals in selling its
practice will lead to a more positive, transparent
agreement and long term relationship
21
• Strategic Recruitment Program• Effective/efficient practice management
structure and support• Data rich; frequent reporting and tracking
of clinical quality, patient satisfaction, and financial results
What Works
22
• Address different generational culture and goals among physician group (schedules, benefits, etc)
• Physician leadership development and support; physicians must participate and lead in the planning process & future governance not just quality & utilization
• Hospital as sole-member of 501(a) organization with LIMITED reserved powers in bylaws
What Works
23
• Compliant, Stark, Anti-Kickback, OIG/CMS (ASA considerations)
• Design a compensation model that aligns Hospital and Physician goals with an objective methodology for calculating physician compensation
• Transparency, understandability and data integrity will engender trust with the physicians
• Plans must evolve to align with changing reimbursement systems
Compensation Plans

24
Compensation Plans
• Plans should reward integration with the system– Consider leaving certain
ancillaries with physician practice.
– Determine equitable allocation of bundled payments among practices.
– Provide appropriate coverage payments and stipends rather than cover losses.

25
Compensation Plans
Maximize productivity & revenue growth while preparing for transition toward quality, satisfaction, and population health based system
– Incorporate Value Based criteria lightly, as supplemental, to begin knowledge build towards transition

26
As with Hospitals, recruit the best Physician Practice
Management
• Provider side experience and balanced approach are key
• Benchmarking and data driven decision making
• IT technology and resources• Avoid overlay of excessive
bureaucracy

27
Keeping an independent mindset
• Encourage provider involvement and leadership
• They are your partner – not your employee • Structure enterprise governance where
providers have influence on decision making & management
28
Healthcare reform is trying to line doctors and hospitals up in one
continuum… these entities need to learn to work cohesively and in a financially
sustainable model

29
Tammy WalshTreasurer/Finance DirectorJPS Physician [email protected]
Corbin WilsonCEO, Executive DirectorJPS Physician [email protected]