presentation1 resom 12
TRANSCRIPT

COURSE OUTLINECOURSE OUTLINEUNIT I: THE HISTORICAL DEVELOPMENT OF HEALTH CARE UNIT I: THE HISTORICAL DEVELOPMENT OF HEALTH CARE DELIVERY SYSTEMDELIVERY SYSTEM1.1: INTRODUCTION TO HEALTHCARE DELIVERY SYSTEM AND 1.1: INTRODUCTION TO HEALTHCARE DELIVERY SYSTEM AND DEFINITION OF TERMSDEFINITION OF TERMS1.1.1. Introduction1.1.1. Introduction1.1.2. History of the Ethiopian Healthcare Delivery System1.1.2. History of the Ethiopian Healthcare Delivery System1.1.3. Historical Background of Modern Medicine in Ethiopia1.1.3. Historical Background of Modern Medicine in Ethiopia1.2: BASIC EVENTS IN HISTORY OF ETHIOPIAN HEALTHCARE 1.2: BASIC EVENTS IN HISTORY OF ETHIOPIAN HEALTHCARE DELIVERY SYSTEMDELIVERY SYSTEM1.2.1. The Basic Health Service Period (BHS) from 1953-19741.2.1. The Basic Health Service Period (BHS) from 1953-19741.2.2. The Primary Health Care (PHC) Period (from 1978-1991)1.2.2. The Primary Health Care (PHC) Period (from 1978-1991)1.2.3. Sector wide Approach Period (199…….)1.2.3. Sector wide Approach Period (199…….)1.2.4. The Traditional Medicine Practice in Ethiopia1.2.4. The Traditional Medicine Practice in EthiopiaUNIT II: THE CURRENT ETHIOPIAN HEALTH POLICYUNIT II: THE CURRENT ETHIOPIAN HEALTH POLICY2.1: GENERAL POLICY2.1: GENERAL POLICY2.2: PRIORITIES OF THE POLICY2.2: PRIORITIES OF THE POLICY2.3: GENERAL STRATEGIES2.3: GENERAL STRATEGIES1.2.4. The Traditional Medicine Practice in Ethiopia1.2.4. The Traditional Medicine Practice in Ethiopia

UNIT II: THE CURRENT ETHIOPIAN HEALTH POLICYUNIT II: THE CURRENT ETHIOPIAN HEALTH POLICY2.1: GENERAL POLICY2.1: GENERAL POLICY2.2: PRIORITIES OF THE POLICY2.2: PRIORITIES OF THE POLICY2.3: GENERAL STRATEGIES2.3: GENERAL STRATEGIESUNIT III: STRUCTURE OF HEALTHCARE SERVICE UNIT III: STRUCTURE OF HEALTHCARE SERVICE
ORGANIZATIONORGANIZATION3.1: STRUCTURE OF THE HEALTHCARE SERVICE 3.1: STRUCTURE OF THE HEALTHCARE SERVICE
ORGANIZATIONORGANIZATION3.1.1. Introduction3.1.1. Introduction3.1.2. Administrative Structure of the Healthcare System 3.1.2. Administrative Structure of the Healthcare System
OrganizationsOrganizations3.2: CONTRIBUTORS OF HEALTH CARE PROVISION IN 3.2: CONTRIBUTORS OF HEALTH CARE PROVISION IN
ETHIOPIAETHIOPIA3.2.1 The Government3.2.1 The Government3.2.2 Private Providers3.2.2 Private Providers3.2.3 Nongovernmental Agencies (NGO’s)3.2.3 Nongovernmental Agencies (NGO’s)3.2.4 International Health Agencies3.2.4 International Health Agencies
UNIT IV: COMPONENTS OF THE HEALTH CARE DELIVERY UNIT IV: COMPONENTS OF THE HEALTH CARE DELIVERY SYSTEMSYSTEM
4.1: COMPONENTS OF HEALTHCARE DELIVERY SYSTEM4.1: COMPONENTS OF HEALTHCARE DELIVERY SYSTEM4.1.1. Introduction4.1.1. Introduction4.1.2. The Current 4 Tiers System4.1.2. The Current 4 Tiers System4.1.3. Major Components and Actors of Healthcare Delivery 4.1.3. Major Components and Actors of Healthcare Delivery
SystemSystem4.2: THE HEALTH CARE FACILITIES AND SERVICES THEY 4.2: THE HEALTH CARE FACILITIES AND SERVICES THEY
PROVIDEPROVIDE4.2.1. The Primary Healthcare Unit (PHCU)4.2.1. The Primary Healthcare Unit (PHCU)4.2.2. District Hospital and Services Provided4.2.2. District Hospital and Services Provided4.2.3. Zonal/Regional Hospitals and Services Provided4.2.3. Zonal/Regional Hospitals and Services Provided4.2.4. Referral Hospitals4.2.4. Referral Hospitals4.3: HEALTHCARE WORKFORCE AT DIFFERENT LEVELS 4.3: HEALTHCARE WORKFORCE AT DIFFERENT LEVELS
OF HEALTH FACILITIESOF HEALTH FACILITIES4.3.1 Human Resource (healthcare workforce) Requirement4.3.1 Human Resource (healthcare workforce) Requirement

UNIT V: HEALTH SERVICE PROGRAMSUNIT V: HEALTH SERVICE PROGRAMS5.1: THE HEALTH POLICY, PLANS AND STRATEGIES5.1: THE HEALTH POLICY, PLANS AND STRATEGIES5.1.1. Introduction5.1.1. Introduction5.1.2. The HSDP-III5.1.2. The HSDP-III5.2: ESSENTIAL HEALTH SERVICE PACKAGE5.2: ESSENTIAL HEALTH SERVICE PACKAGE5.2.1. Introduction5.2.1. Introduction5.2.2. The Health Service Extension Program (HSEP)5.2.2. The Health Service Extension Program (HSEP)5.2.3. Family Health Services (Maternal and Child Health 5.2.3. Family Health Services (Maternal and Child Health
Care)Care)5.2.4. Prevention and Control of Disease5.2.4. Prevention and Control of Disease5.2.5. Medical Services5.2.5. Medical Services5.2.6. Hygiene and Environmental Health5.2.6. Hygiene and Environmental Health5.3: HUMAN RESOURCE DEVELOPMENT5.3: HUMAN RESOURCE DEVELOPMENT5.3.1 Introduction5.3.1 Introduction5.4: PHARMACEUTICAL SERVICE5.4: PHARMACEUTICAL SERVICE5.4.1 Pharmaceutical Services5.4.1 Pharmaceutical Services

5.5: IEC AND HEALTH INFORMATION MANAGEMENT 5.5: IEC AND HEALTH INFORMATION MANAGEMENT SYSTEM (HIMS)SYSTEM (HIMS)
5.5.1. Information, Education and Communication (IEC)5.5.1. Information, Education and Communication (IEC)Health Information Management System (HMIS)Health Information Management System (HMIS)5.6: MONITORING AND EVALUATION (M&E) AND 5.6: MONITORING AND EVALUATION (M&E) AND
HEALTHCARE FINANCINGHEALTHCARE FINANCING5.6.1. Monitoring and Evaluation (M&E)5.6.1. Monitoring and Evaluation (M&E)5.6.2. Healthcare Financing5.6.2. Healthcare FinancingUNIT VI: HEALTHCARE SYSTEM REGULATIONUNIT VI: HEALTHCARE SYSTEM REGULATION6.1: HEALTHCARE SYSTEM REGULATIONS6.1: HEALTHCARE SYSTEM REGULATIONS6.1.1 Introduction6.1.1 Introduction6.1.2. Regulation of Credentialing Health Manpower6.1.2. Regulation of Credentialing Health Manpower6.1.3. Professional Associations6.1.3. Professional Associations6.2. HEALTH INFORMATION SYSTEMS POLICIES AND 6.2. HEALTH INFORMATION SYSTEMS POLICIES AND
PROCEDURESPROCEDURES6.2.1. Introduction6.2.1. Introduction6.2.2. HIS Policies and Procedures6.2.2. HIS Policies and Procedures6.2.3. Health Information Related I6.2.3. Health Information Related I

UNIT VII: HEALTHCARE SERVICE PLANNINGUNIT VII: HEALTHCARE SERVICE PLANNING7.1: HEALTHCARE SERVICE PLANNING7.1: HEALTHCARE SERVICE PLANNING7.1.1 Introduction: definitions of key terms7.1.1 Introduction: definitions of key terms7.1.2 Health Service Planning7.1.2 Health Service Planning7.1.3 Strategies and Approaches used in Health Service 7.1.3 Strategies and Approaches used in Health Service
PlanningPlanning7.2. RESOURCE IDENTIFICATION7.2. RESOURCE IDENTIFICATION7.2.1 Introduction to Classification (and Identification) of 7.2.1 Introduction to Classification (and Identification) of
ResourceResourceTEXTBOOKS/REFERENCE BOOKS AND MANUALTEXTBOOKS/REFERENCE BOOKS AND MANUAL1. Module Handouts are distributed to the students as textbook1. Module Handouts are distributed to the students as textbook2. HSDP I, II,III, FMoH2. HSDP I, II,III, FMoH3. Harmonization Manual, FMOH3. Harmonization Manual, FMOH4. Chali Jirra et al. Health service Planning and management 4. Chali Jirra et al. Health service Planning and management
for health science students.for health science students.5. Jonathans. Rakich et.al Managing health service 5. Jonathans. Rakich et.al Managing health service
organization, third edition, 1992 Maryland, USAorganization, third edition, 1992 Maryland, USA

ABBREVIATIONSABBREVIATIONSAIDS Acquired Immune Deficiency SyndromeAIDS Acquired Immune Deficiency SyndromeART Anti retroviral therapyART Anti retroviral therapyBHS Basic Health Service PeriodBHS Basic Health Service PeriodBOC Basic obstetric careBOC Basic obstetric careCHP Community health promotersCHP Community health promotersCOC Comprehensive obstetric careCOC Comprehensive obstetric careCSRP Civil service reform programCSRP Civil service reform programDACA The Drug Administration and Control AuthorityDACA The Drug Administration and Control AuthorityDKA Diabetic Keto acidosisDKA Diabetic Keto acidosisEHNRI Ethiopian health nutrition research instituteEHNRI Ethiopian health nutrition research instituteEOC Emergency obstetric careEOC Emergency obstetric careEPA Ethiopian public health associationEPA Ethiopian public health associationESOG Ethiopian society of obstetrics and gynecologyESOG Ethiopian society of obstetrics and gynecologyFP Family PlanningFP Family Planning

FMIS Financial management information systemFMIS Financial management information systemFMOH Federal ministry of healthFMOH Federal ministry of healthGO Government organizationGO Government organizationHC Health centerHC Health centerHCF Health care financeHCF Health care financeHIMS Health information management systemHIMS Health information management systemHIV Human immune virusHIV Human immune virusHOS HospitalHOS HospitalHP Health postHP Health postHSEP Health service extension programHSEP Health service extension programIDSR Integrated Disease Surveillance and ReportIDSR Integrated Disease Surveillance and ReportIMR Infant mortality rateIMR Infant mortality rateLMIS Logistics management information systemLMIS Logistics management information systemM&E Monitoring and evaluationM&E Monitoring and evaluation

MCH Maternal and Child HealthMCH Maternal and Child HealthMCHC Maternal and child health careMCHC Maternal and child health careMDGS Millennium development goalsMDGS Millennium development goalsMIS Management information systemMIS Management information systemMMR Maternal mortality rateMMR Maternal mortality rateNAC National advisory committeeNAC National advisory committeeNGOS Nongovernmental organizationNGOS Nongovernmental organizationPASS Pharmaceutical Administration and Supply ServicesPASS Pharmaceutical Administration and Supply ServicesPHC Primary health carePHC Primary health carePMTCT Prevention of mother to child transitionPMTCT Prevention of mother to child transitionRHB Regional Health BureauRHB Regional Health BureauSNNPR Southern Nations and nationality peoples regionSNNPR Southern Nations and nationality peoples regionSWOT Strength Weakness Opportunity ThreatSWOT Strength Weakness Opportunity ThreatTFR Total fertility rateTFR Total fertility rateTLCP Tuberculosis leprosy control programTLCP Tuberculosis leprosy control programU5MR Under five mortality rateU5MR Under five mortality rate

MCH Maternal and Child HealthMCH Maternal and Child HealthMCHC Maternal and child health careMCHC Maternal and child health careMDGS Millennium development goalsMDGS Millennium development goalsMIS Management information systemMIS Management information systemMMR Maternal mortality rateMMR Maternal mortality rateNAC National advisory committeeNAC National advisory committeeNGOS Nongovernmental organizationNGOS Nongovernmental organizationPASS Pharmaceutical Administration and Supply ServicesPASS Pharmaceutical Administration and Supply ServicesPHC Primary health carePHC Primary health carePMTCT Prevention of mother to child transitionPMTCT Prevention of mother to child transitionRHB Regional Health BureauRHB Regional Health BureauSNNPR Southern Nations and nationality peoples regionSNNPR Southern Nations and nationality peoples regionSWOT Strength Weakness Opportunity ThreatSWOT Strength Weakness Opportunity ThreatTFR Total fertility rateTFR Total fertility rateTLCP Tuberculosis leprosy control programTLCP Tuberculosis leprosy control programU5MR Under five mortality rateU5MR Under five mortality rate

1.1.1. Introduction1.1.1. IntroductionHealth care delivery system is a network of integrated Health care delivery system is a network of integrated
components designed to work together coherently,to components designed to work together coherently,to provide healthcare to a population in various settings. provide healthcare to a population in various settings. Concepts from general systems theory are useful Concepts from general systems theory are useful inunderstanding the structure and operation of a nation’s inunderstanding the structure and operation of a nation’s health system. For this purpose the following must health system. For this purpose the following must beidentified:beidentified:
The major actors, which can further be classified as :The major actors, which can further be classified as :– healthcare users/consumershealthcare users/consumers– healthcare providershealthcare providers– policy makers/regulatorspolicy makers/regulators
Their resources, which can be further classified as:Their resources, which can be further classified as:– fundingfunding– personnelpersonnel– facilityfacility– technologytechnology– informationinformation

The mechanism through which they interactThe mechanism through which they interact
The external forces which affect the processThe external forces which affect the process
The healthcare delivery system like all systems is The healthcare delivery system like all systems is dynamic with many feedbacks loops among dynamic with many feedbacks loops among providers, consumers and regulators, allowing for providers, consumers and regulators, allowing for change in the system’s performancechange in the system’s performance
1.1.2. History of the Ethiopian Healthcare Delivery 1.1.2. History of the Ethiopian Healthcare Delivery SystemSystem
Ethiopia has one of the worst health statuses, with Ethiopia has one of the worst health statuses, with poor environmental condition and inadequate poor environmental condition and inadequate healthservices. Long periods of civil strife, rapid healthservices. Long periods of civil strife, rapid population growth and environmental degradation population growth and environmental degradation have furtheraggravated these health problems.have furtheraggravated these health problems.

The country has a new health policy and The country has a new health policy and strategy; the health service is to be re-strategy; the health service is to be re-organized into a more costeffectiveand organized into a more costeffectiveand efficient system that can contribute better to efficient system that can contribute better to the overall socio-economic development the overall socio-economic development effort of the country. To understand the effort of the country. To understand the current healthcare system we must look back current healthcare system we must look back to the historical background of modern to the historical background of modern medicine in Ethiopia, and the role traditional medicine in Ethiopia, and the role traditional medicine plays.medicine plays.
1.1.3. Historical Background of Modern 1.1.3. Historical Background of Modern Medicine in EthiopiaMedicine in Ethiopia

There have been occasional contacts between There have been occasional contacts between modern medical practitioners and Ethiopians modern medical practitioners and Ethiopians prior to the end of the 19th-century.A prior to the end of the 19th-century.A Portuguese “barber surgeon” was known to Portuguese “barber surgeon” was known to be at the courts of King Lebne-Dengel in the be at the courts of King Lebne-Dengel in the 15th century: then the German missionary, 15th century: then the German missionary, by the name of Peter Heiling, was at the by the name of Peter Heiling, was at the court to Emperor Fasiledes in the 16th court to Emperor Fasiledes in the 16th century, and several others have been century, and several others have been recorded.recorded.

If we reflect back in history, the years just before If we reflect back in history, the years just before and after the turn of the millennium can be and after the turn of the millennium can be considered as a centenary for health services in considered as a centenary for health services in Ethiopia. It was just at the end of the 19th and the Ethiopia. It was just at the end of the 19th and the beginning of the 20th centuries that modern beginning of the 20th centuries that modern health care was introduced in the country. The health care was introduced in the country. The first modern health care facility in the country (a first modern health care facility in the country (a Russian Red Cross Hospital) was established in Russian Red Cross Hospital) was established in Addis Ababa in 1987 with a capacity of 50 beds. It Addis Ababa in 1987 with a capacity of 50 beds. It is interesting to note that the mission produced a is interesting to note that the mission produced a small booklet in Amharic of 22 pages, which was small booklet in Amharic of 22 pages, which was to serve as a textbook for Ethiopian staff. The to serve as a textbook for Ethiopian staff. The Russian mission stayed in the country for ten Russian mission stayed in the country for ten years,years,

and in 1906 the hospital was closed. Following and in 1906 the hospital was closed. Following that a leprosarium and hospital were opened that a leprosarium and hospital were opened in Harar in 1901 and 1903 respectively. In in Harar in 1901 and 1903 respectively. In the year 1909 the first public hospital Menilik the year 1909 the first public hospital Menilik II established on the site of the Russian II established on the site of the Russian hospital. At the beginning it had 30 beds .The hospital. At the beginning it had 30 beds .The hospital has been in operation ever since on hospital has been in operation ever since on the same site and even today it’s called by its the same site and even today it’s called by its original name, “Menilik II hospital”.original name, “Menilik II hospital”.

After Minilk II Emperor Hilesilase I continued and the After Minilk II Emperor Hilesilase I continued and the reform drive of Emperor Halile Selassie I during reform drive of Emperor Halile Selassie I during 1917- 1935 focused on economic and social 1917- 1935 focused on economic and social conditions that included health expansion and conditions that included health expansion and management reforms. This drive was interrupted management reforms. This drive was interrupted during the brief occupation of Ethiopia by the during the brief occupation of Ethiopia by the Italians. Until Soon after the liberation of Ethiopia in Italians. Until Soon after the liberation of Ethiopia in 1941 the period of reconstruction time that a 1941 the period of reconstruction time that a Department called “Public Health Directorate” was Department called “Public Health Directorate” was established under the then powerful Ministry of established under the then powerful Ministry of Interior (MOI). The first director of the unit was a Interior (MOI). The first director of the unit was a British Doctor known by the name Colonel British Doctor known by the name Colonel Maclean. It was made responsible for the Maclean. It was made responsible for the establishment of the first hospital, and for the establishment of the first hospital, and for the general problems in the health field.general problems in the health field.

During that time, there were several Christian During that time, there were several Christian missions operating in the country, they missions operating in the country, they provide health care to the people in addition provide health care to the people in addition to their religious and sometimes educational to their religious and sometimes educational activities. In 1922 another hospital was activities. In 1922 another hospital was established in Addis Abeba. An American established in Addis Abeba. An American missionary named Dr. Thomas Lambie missionary named Dr. Thomas Lambie collected money, erected a building in the collected money, erected a building in the Gulele area, and established a hospital with Gulele area, and established a hospital with 70 beds. This hospital had 4 medical doctors 70 beds. This hospital had 4 medical doctors and 5 nurses on its staff.and 5 nurses on its staff.

The hospital was converted into a research The hospital was converted into a research Institute in 1942, then into the Institutes of Institute in 1942, then into the Institutes of Pasteur in 1950. In 1964 it was converted Pasteur in 1950. In 1964 it was converted into the central laboratory and research into the central laboratory and research institute, and finally it was merged with institute, and finally it was merged with Ethiopian Nutrition Institute (ENI), today it’s Ethiopian Nutrition Institute (ENI), today it’s called Ethiopian Health and Nutrition called Ethiopian Health and Nutrition Research Institutes (ENHRI).Research Institutes (ENHRI).

Because of expansion of health service Because of expansion of health service government has taken Major step in the government has taken Major step in the autonomous development of health care autonomous development of health care which did not happen until the formal which did not happen until the formal establishment of the Ministry of Public establishment of the Ministry of Public Health (MOPH) in 1948. By 1948 there were Health (MOPH) in 1948. By 1948 there were already several hospitals in the country. At already several hospitals in the country. At that time, the majority of hospitals, and that time, the majority of hospitals, and health facilities were run by different mission health facilities were run by different mission organizations.organizations.

In speaking of the historical development of In speaking of the historical development of health services in Ethiopia, one must mention health services in Ethiopia, one must mention the contribution of first Ethiopian medical the contribution of first Ethiopian medical doctors. Dr. Martin Workineh. As a child of doctors. Dr. Martin Workineh. As a child of three years he was found on the battlefield three years he was found on the battlefield after the battle of Maqdela (1868). The boy after the battle of Maqdela (1868). The boy was taken and educated in India and later in was taken and educated in India and later in Britain, sponsored by two officers, Colonel Britain, sponsored by two officers, Colonel Charles Chamberlain and Colonel Martin, and Charles Chamberlain and Colonel Martin, and after them he was named Charles Martin. after them he was named Charles Martin. After the first aborted Italian invasion of After the first aborted Italian invasion of Ethiopia in 1896,Ethiopia in 1896,

Martin arrived in Addis Abeba, where a he Martin arrived in Addis Abeba, where a he pitched a tent in the center of the city and run pitched a tent in the center of the city and run a clinic, treating patients free of charge. a clinic, treating patients free of charge. During that time he learned who his parents During that time he learned who his parents were and found his grandmother, who told were and found his grandmother, who told him his name was Workineh. Hakim him his name was Workineh. Hakim Workineh as he was popularly known served Workineh as he was popularly known served not only as a physician but also as a not only as a physician but also as a diplomat, he died at the age of 84 in 1952.diplomat, he died at the age of 84 in 1952.

The second Ethiopian medical doctor was Dr. The second Ethiopian medical doctor was Dr. Melaku Beyan, who early in this century Melaku Beyan, who early in this century obtained his medical degree at Howard obtained his medical degree at Howard University in the United States. He was chief University in the United States. He was chief medical officer of the Ethiopia Army during medical officer of the Ethiopia Army during the Italian invasion from Somalia in 1935. the Italian invasion from Somalia in 1935. Dr. Melaku died in exile during the Italian Dr. Melaku died in exile during the Italian occupation of Ethiopia.occupation of Ethiopia.

Whatever medical developments there was in Whatever medical developments there was in the country, it was disrupted during the the country, it was disrupted during the Italian occupation. After the war, another Italian occupation. After the war, another hospital was established named after hospital was established named after Princess Tsehay who was the first Ethiopian Princess Tsehay who was the first Ethiopian nurse, having graduated in England during nurse, having graduated in England during the war. Look at table 1 for the detail of the war. Look at table 1 for the detail of historical events in the Ethiopian health care historical events in the Ethiopian health care delivery system Period Date Event 1520-delivery system Period Date Event 1520-1526 Foreign medical contacts with 1526 Foreign medical contacts with Portuguese Barber surgeon 1830s and Portuguese Barber surgeon 1830s and 1840s French and British missions,1840s French and British missions,
introduced vaccination Period of Unification and introduced vaccination Period of Unification and Independence 1856 Use of small pox vaccine Independence 1856 Use of small pox vaccine officially promoted by Emperor Tewdros 1896officially promoted by Emperor Tewdros 1896
Battle of AdewaBattle of Adewa
Russian red cross mission published first medical text Russian red cross mission published first medical text in Amaharicin Amaharic
Dr (Hakim) Workeneh return to EthiopiaDr (Hakim) Workeneh return to Ethiopia
1987 The first hospital in Ethiopia Established by the 1987 The first hospital in Ethiopia Established by the Russian red cross mission Power struggleRussian red cross mission Power struggle
1909 The first Government hospital Minilk II opened1909 The first Government hospital Minilk II opened
1930 The first public health low endorsed Emergence 1930 The first public health low endorsed Emergence of Absolutismof Absolutism

Early 1930s Early 1930s First health budget allocatedFirst health budget allocated Public latrine introduced Public latrine introduced 19351935 Minilk II started training the first medical auxiliaries Minilk II started training the first medical auxiliariesDr Melaku Beyane the first trained Dr return to EthiopiaDr Melaku Beyane the first trained Dr return to EthiopiaEthiopian Red cross society established in JulyEthiopian Red cross society established in JulyOutbreak of Italio- Ethiopian warOutbreak of Italio- Ethiopian warFrom Libration to RevolutionFrom Libration to Revolution1941 Bureau of Hygiene established with in the ministry of 1941 Bureau of Hygiene established with in the ministry of
interiorinterior1942 School of medical service started1942 School of medical service started1947 Ministry of Health Established1947 Ministry of Health Established1948 Medical education board established1948 Medical education board established1950 University collage of Addis Ababa started1950 University collage of Addis Ababa started1952 Policy decision on developing Health center1952 Policy decision on developing Health center

1957-1961 The first five year development plan planed1957-1961 The first five year development plan planed1959 Malaria eradication program launched1959 Malaria eradication program launched1963-1967 The second five year plan planed1963-1967 The second five year plan planed1968 Planning division ministry of public health established1968 Planning division ministry of public health established1969/1970 Small pox eradication program launched1969/1970 Small pox eradication program launched1970 Malaria eradication program converted to control 1970 Malaria eradication program converted to control
programprogramThe Derge PeriodThe Derge Period1974 Ethiopian revolution1974 Ethiopian revolution1975 Launching of the National Democratic Revolutionary 1975 Launching of the National Democratic Revolutionary
programprogram1976-1980 The 5 year rural health development program1976-1980 The 5 year rural health development program1978 Adoption of primary health care1978 Adoption of primary health care1984 Ten years perspective Development plan1984 Ten years perspective Development plan1991 Fall of Derge Regime1991 Fall of Derge Regime

EPRDF RegimeEPRDF Regime
1991-1995 Transition time1991-1995 Transition time
1993 Development of health policy and 1993 Development of health policy and strategystrategy
1998-2002 Health sector development 1998-2002 Health sector development program Iprogram I
2003-2007… Health sector development 2003-2007… Health sector development program IIprogram II
1.2.1. The Basic Health Service Period 1.2.1. The Basic Health Service Period (BHS) from 1953-1974(BHS) from 1953-1974
For Ethiopia (following the WHO For Ethiopia (following the WHO recommendation), BHS was seen as a long recommendation), BHS was seen as a long term strategy for providing adequate and term strategy for providing adequate and essential health care by making available a essential health care by making available a HC for a population of 50,000 and a Clinic HC for a population of 50,000 and a Clinic for a population of 5,000. A new chapter in for a population of 5,000. A new chapter in the development of health services was the development of health services was opened when, with the assistance of opened when, with the assistance of international organizations, Gondar Public international organizations, Gondar Public Health College and training center was Health College and training center was established in 1952.established in 1952.

The Institute trained three categories of health The Institute trained three categories of health personnel; public health officers, community personnel; public health officers, community nurses and sanitarians, who were intended nurses and sanitarians, who were intended to serve in the health centers, a new type of to serve in the health centers, a new type of the institution. One health center was the institution. One health center was supposed to serve 50,000 people, with the supposed to serve 50,000 people, with the help of satellite health stations.help of satellite health stations.
The first organized training of health personnel The first organized training of health personnel can be traced back to 1945, when a six-can be traced back to 1945, when a six-month course was offered to all hospital month course was offered to all hospital orderlies, who were then upgraded to the orderlies, who were then upgraded to the status of “dressers”.status of “dressers”.

• The first nursing school was established in The first nursing school was established in Addis Abeba by the Red Cross society in Addis Abeba by the Red Cross society in 1950. The training center for medical and 1950. The training center for medical and health technicians was established in 1963 health technicians was established in 1963 within Menilik II hospital. The first medical within Menilik II hospital. The first medical school was established in 1962.school was established in 1962.
• Due to the slow development of general Due to the slow development of general health services and subject to some health services and subject to some international pressure, special projects to international pressure, special projects to combat individual disease were embarked combat individual disease were embarked upon. The most important project is the upon. The most important project is the Malaria eradication project, established in Malaria eradication project, established in 1959;1959;

the TB control project, a Leprosy control the TB control project, a Leprosy control project, the Ethiopian nutrition institutes, and project, the Ethiopian nutrition institutes, and the small pox eradication service are the small pox eradication service are examples of the bigger projects. Some of examples of the bigger projects. Some of these projects are still in existence.these projects are still in existence.

1.2.2. The Primary Health Care (PHC) 1.2.2. The Primary Health Care (PHC) Period (from 1978-1991)Period (from 1978-1991)
Change in Government from Imperial Rule to Change in Government from Imperial Rule to Military Rule followed by subsequent political Military Rule followed by subsequent political orientation into socialist ideology after 1974 orientation into socialist ideology after 1974 brought with it radical changes in the health brought with it radical changes in the health policy of Ethiopia which in some ways policy of Ethiopia which in some ways provided the foundation for further provided the foundation for further development of health care delivery system. development of health care delivery system. Also in 1977 the WHO set a goal of Also in 1977 the WHO set a goal of providing “health for all by the year 2000” providing “health for all by the year 2000” which aims at achieving a level of healthwhich aims at achieving a level of health

that enables every citizen of the world to lead a that enables every citizen of the world to lead a socially and economically productive life. The socially and economically productive life. The strategy to meet this goal was later defined in strategy to meet this goal was later defined in the 1978 WHO/UNICEF joint meeting at the 1978 WHO/UNICEF joint meeting at Alma-Ata. In this meeting it was declared that Alma-Ata. In this meeting it was declared that the primary health care strategy is the key to the primary health care strategy is the key to meet the Goal of “Health for all by the year meet the Goal of “Health for all by the year 2000”.2000”.

After the World Health Assembly (in 1978), After the World Health Assembly (in 1978), Ethiopia fully endorsed that the target of Ethiopia fully endorsed that the target of governments and WHO should be the governments and WHO should be the attainment of a level of health that would attainment of a level of health that would enable all people to lead a socially and enable all people to lead a socially and economically productive life by the year economically productive life by the year 2000. This was commonly known as “Health 2000. This was commonly known as “Health for All by the year 2000”, also known as the for All by the year 2000”, also known as the “Declaration of Alma-Ata”“Declaration of Alma-Ata”

• A) The declaration of PHCA) The declaration of PHC• The declaration of PHC focused on the following The declaration of PHC focused on the following
main concepts:main concepts:• 1. Equitable distribution1. Equitable distribution• Health services must be shared equally, distributed Health services must be shared equally, distributed
by all people irrespective of their ability to pay and by all people irrespective of their ability to pay and all (rich or poor, urban or rural) must have access to all (rich or poor, urban or rural) must have access to health services. Primary health care aims to health services. Primary health care aims to address the current imbalance in health care by address the current imbalance in health care by shifting the centre of gravity from cities where a shifting the centre of gravity from cities where a majority of the health budget is spent to rural areas majority of the health budget is spent to rural areas where a majority of people live in most countries.where a majority of people live in most countries.

2. Active community 2. Active community participation/Involvementparticipation/Involvement
Active community participation/involvement is:Active community participation/involvement is:
The process by which individuals and families The process by which individuals and families assume responsibility for the community and assume responsibility for the community and develop the capacity to contribute to their develop the capacity to contribute to their and the community’s development.and the community’s development.
A means by which communities can play a A means by which communities can play a more influential role in health development, more influential role in health development, in which the emphasis is on strengthening in which the emphasis is on strengthening the capacity of communities to determine the capacity of communities to determine their own needs and take appropriate action.their own needs and take appropriate action.

Community Involvement is the process of Community Involvement is the process of involving the community in the planning, involving the community in the planning, implementing and monitoring and implementing and monitoring and evaluation unlike participation. Communities evaluation unlike participation. Communities should not be passive recipients of services should not be passive recipients of services everybody should be involved according to everybody should be involved according to his ability and the Health system is his ability and the Health system is responsible forresponsible for
• Explaining and advisingExplaining and advising• Providing clear information about the favorable and Providing clear information about the favorable and
adverse consequences of the interventions being adverse consequences of the interventions being proposed as well as their relative cost.proposed as well as their relative cost.

– The communities should be actively involved inThe communities should be actively involved in
The assessment of the situationThe assessment of the situation
Problem IdentificationProblem Identification
Priority setting and making decisionsPriority setting and making decisions
Sharing responsibility in the planning Sharing responsibility in the planning implementing, monitoring and evaluationimplementing, monitoring and evaluation

3. Intra and Inter-sectoral linkages3. Intra and Inter-sectoral linkages
Primary health care involves in addition to the Primary health care involves in addition to the health sector, all related sectors and aspects health sector, all related sectors and aspects of national and community development, in of national and community development, in particular agriculture, animal husbandry, particular agriculture, animal husbandry, food, industry, education, housing, public food, industry, education, housing, public works, communication and other sectors.works, communication and other sectors.

B) The four cornerstones in Primary Health B) The four cornerstones in Primary Health CareCare
The four cornerstones in Primary Health Care The four cornerstones in Primary Health Care (or Pre- requisites for PHC) are:(or Pre- requisites for PHC) are:
1. Active community 1. Active community participation/Decentralization/participation/Decentralization/
2. Intra and Inter-sectoral linkages2. Intra and Inter-sectoral linkages
3. Use of appropriate Technology3. Use of appropriate Technology
4. Political commitment /Support Mechanism 4. Political commitment /Support Mechanism made Available/made Available/

C) The Components/Elements of PHCC) The Components/Elements of PHC
There are twelve elements of PHC on There are twelve elements of PHC on implementation in Ethiopia. Of these implementation in Ethiopia. Of these elements from number one to eight are the elements from number one to eight are the components by which implementation began components by which implementation began while the last four were added later on.while the last four were added later on.
1. Immunization-immunization against the 1. Immunization-immunization against the major infectious diseases (six childhood major infectious diseases (six childhood diseases)diseases)
2. Food supply and proper nutrition-promotion 2. Food supply and proper nutrition-promotion of food supply and proper nutritionof food supply and proper nutrition

Improve food supply and proper nutrition.Improve food supply and proper nutrition.Correction of faulty feeding practices.Correction of faulty feeding practices.Treatment and rehabilitation of malnourished Treatment and rehabilitation of malnourished
children.children.Treatment and prevention of nutritional Treatment and prevention of nutritional
diseases.diseases.3. Water and sanitation-an adequate supply of 3. Water and sanitation-an adequate supply of
safe and basic sanitation.safe and basic sanitation.4. Prevention and treatment of locally endemic 4. Prevention and treatment of locally endemic
disease and injuries.disease and injuries.5. Maternal and Child Health (MCH) and 5. Maternal and Child Health (MCH) and
Family Planning (FP). Main functions are:Family Planning (FP). Main functions are:

Antenatal careAntenatal careDelivery careDelivery carePostnatal carePostnatal careChild careChild careFamily planningFamily planning6. Provision of essential drugs6. Provision of essential drugs7. Health Education7. Health EducationFor promoting healthFor promoting healthFor prevention of diseaseFor prevention of diseaseFor maintenance of healthFor maintenance of healthEducation to deal with the disease.Education to deal with the disease.

8. Control of communicable diseases8. Control of communicable diseases
9. Mental health9. Mental health
10. Dental health10. Dental health
11. Control of ARI11. Control of ARI
12. Controls of HIV/AIDS and other STDs.12. Controls of HIV/AIDS and other STDs.
The 1985 review of PHC implementation The 1985 review of PHC implementation attempts in Ethiopia revealed the following attempts in Ethiopia revealed the following achievements.achievements.

Expansion of health services to the broad Expansion of health services to the broad masses especially by establishing new masses especially by establishing new health station and health posts.health station and health posts.
Expansion of immunization program against Expansion of immunization program against six major communicable diseases.six major communicable diseases.
Increasing number of medical and paramedical Increasing number of medical and paramedical personnelpersonnel
Increased health propaganda attempts to Increased health propaganda attempts to improve health consciousness of the improve health consciousness of the population by building the promotion of population by building the promotion of health information to the people.health information to the people.

• Problems encountered in PHC Problems encountered in PHC implementation in Ethiopiaimplementation in Ethiopia– Nature of community involvement (poor Nature of community involvement (poor
community participation)community participation)– Political and social organizationPolitical and social organization– Political and bureaucratic unwillingnessPolitical and bureaucratic unwillingness– Structure and tradition of formal health systemStructure and tradition of formal health system– Lack of resource planning and management.Lack of resource planning and management.
– difference of vision between community and difference of vision between community and health professionalshealth professionals
– Misunderstandings:Misunderstandings:– PHC is community based carePHC is community based care– It is only for poor people in developing countriesIt is only for poor people in developing countries– It is for rural areaIt is for rural area– PHC is cheap, etc.PHC is cheap, etc.

• 1.2.3. Sector wide Approach Period 1.2.3. Sector wide Approach Period (199…….)(199…….)
• The government of Derge is overthrown by The government of Derge is overthrown by EPRDF in 1991 and transitional government EPRDF in 1991 and transitional government was established for 1991-1995. During this was established for 1991-1995. During this period health policy and strategy were period health policy and strategy were developed.developed.
• Currently the Ethiopian government is Currently the Ethiopian government is following a twenty-year health development following a twenty-year health development implementation strategy, known as the implementation strategy, known as the Health Sector Development Program Health Sector Development Program (HSDP), with a series of five-year investment (HSDP), with a series of five-year investment programs.programs.

• HSDP proposes a sector-wide approach to HSDP proposes a sector-wide approach to achieve the government’s objectives.achieve the government’s objectives.
• The Health Sector Development Program, The Health Sector Development Program, launched by the government in 1998, was launched by the government in 1998, was devised after studying the kind of health devised after studying the kind of health problems that affect Ethiopia and problems that affect Ethiopia and researching their root causes. It also took researching their root causes. It also took into consideration emerging serious health into consideration emerging serious health issues such as HIV/AIDS and put a strong issues such as HIV/AIDS and put a strong emphasis on the needs of the rural Ethiopia, emphasis on the needs of the rural Ethiopia, where overwhelming majority of the where overwhelming majority of the country’s citizens live.country’s citizens live.
Sector wide approach-based health care Sector wide approach-based health care delivery system is owned by the state, but its delivery system is owned by the state, but its implementation is firmly based on strong implementation is firmly based on strong partnership between the Central partnership between the Central Government, the Regional Government, the Government, the Regional Government, the Health Development Partners, the Private Health Development Partners, the Private and NGO sectors. The focus of health and NGO sectors. The focus of health delivery system is expansion and delivery system is expansion and improvement in the quality of care and is improvement in the quality of care and is guided by the eight components of the guided by the eight components of the Health Sector Strategic Plan (HSDP) at all Health Sector Strategic Plan (HSDP) at all levels.levels.

The eight components of HSDP are:The eight components of HSDP are:
1) Health service Delivery and Quality of care.1) Health service Delivery and Quality of care.
2) Health facility Rehabilitation and Expansion.2) Health facility Rehabilitation and Expansion.
3) Human Resource Development.3) Human Resource Development.
4) Strengthening Pharmaceutical Services.4) Strengthening Pharmaceutical Services.
5) Information, Education and Communication.5) Information, Education and Communication.
6) Health Management Information Systems.6) Health Management Information Systems.
7) Healthcare Financing.7) Healthcare Financing.
8) Monitoring and Evaluation.8) Monitoring and Evaluation.

1.2.4. The Traditional Medicine Practice in 1.2.4. The Traditional Medicine Practice in EthiopiaEthiopia
Long before the advent of modern medicine, Long before the advent of modern medicine, Ethiopia had its own method for combating Ethiopia had its own method for combating disease. These methods are usually referred disease. These methods are usually referred to as Ethiopian traditional medicine. Not only to as Ethiopian traditional medicine. Not only was a traditional medicine structure operation was a traditional medicine structure operation prior to the advent of modern medicine, but it prior to the advent of modern medicine, but it can be said that even today the rural can be said that even today the rural populations depend on it.populations depend on it.
Ethiopian traditional practitioners practiced not Ethiopian traditional practitioners practiced not only curative but also preventive medicine, only curative but also preventive medicine, and the firstand the first

““Cordon Sanitaire” was established in Gondar Cordon Sanitaire” was established in Gondar as early as 1830 G.C. Similar actions were as early as 1830 G.C. Similar actions were taken in the whole country in 1918 G.C. taken in the whole country in 1918 G.C. during the notorious influenza pandemic during the notorious influenza pandemic variolization was very widespread as a variolization was very widespread as a means of preventing small pox, and in certain means of preventing small pox, and in certain times in the 18th century the variolization was times in the 18th century the variolization was even compulsory.even compulsory.

The traditional Ethiopian pharmacopoeia The traditional Ethiopian pharmacopoeia comprised items from the animal and comprised items from the animal and vegetable kingdoms. And even some vegetable kingdoms. And even some minerals (e.g. floss from iron melting). minerals (e.g. floss from iron melting). Counter-irritants (burning of the skin over the Counter-irritants (burning of the skin over the diseased part of the body), bleeding and diseased part of the body), bleeding and cupping were other routinely used cupping were other routinely used procedures. Several surgical procedures, procedures. Several surgical procedures, including trepanation and Cesarean section, including trepanation and Cesarean section, have been repeatedly reported, but probably have been repeatedly reported, but probably the greatest skills were observed in bone-the greatest skills were observed in bone-setting (‘Wegesha’), including even setting (‘Wegesha’), including even operations and insertions of sheep’s bone.operations and insertions of sheep’s bone.

In connection with traditional medical practices, In connection with traditional medical practices, one has to mention some harmful one has to mention some harmful procedures that have been widely practiced procedures that have been widely practiced in the country, such as female circumcision, in the country, such as female circumcision, removal of tonsils by means of a nail, uvula removal of tonsils by means of a nail, uvula cutting, and pulling healthy children’s teeth.cutting, and pulling healthy children’s teeth.
In recent times the Ministry of Health has been In recent times the Ministry of Health has been making an effort to integrate traditional making an effort to integrate traditional medicine into the general network of health medicine into the general network of health services, particularly since the skills of services, particularly since the skills of certain healers are known to be effective.certain healers are known to be effective.

Among the most prominent practitioners, bone-Among the most prominent practitioners, bone-setters (wogeshas), herbalist’s (kitel betash), setters (wogeshas), herbalist’s (kitel betash), traditional birth attendants and particularly traditional birth attendants and particularly different types of “spiritual healers” can be different types of “spiritual healers” can be useful in general, and the people appreciate useful in general, and the people appreciate their services.their services.
Formal recognition to traditional medicine in Formal recognition to traditional medicine in Ethiopia was given in 1942 (Proclamation Ethiopia was given in 1942 (Proclamation 27), where legitimacy of the practice was 27), where legitimacy of the practice was acknowledged as long as it does not have acknowledged as long as it does not have negative consequence on health.negative consequence on health.

Despite the relatively rapid expansion of Despite the relatively rapid expansion of modern medicine, traditional medicine (TM) modern medicine, traditional medicine (TM) is still the predominanthealth care resource is still the predominanthealth care resource in Ethiopia. World Health Organization in Ethiopia. World Health Organization estimated that 80% of the population in estimated that 80% of the population in developingcountries and as many as 90% of developingcountries and as many as 90% of the Ethiopians use TM for their illnessesthe Ethiopians use TM for their illnesses
UNIT II: THE CURRENT ETHIOPIANUNIT II: THE CURRENT ETHIOPIANHEALTH POLICYHEALTH POLICYIntroductionIntroductionIn the first unit of the module we have seen the In the first unit of the module we have seen the
historical development of health care delivery historical development of health care delivery system insystem in
Ethiopia period by period from early exposure Ethiopia period by period from early exposure of medical practice to the current sector wide of medical practice to the current sector wide approach.approach.
In this unit we will see the general policy, In this unit we will see the general policy, priories of policy and general strategies of priories of policy and general strategies of the policy in Ethiopia context.the policy in Ethiopia context.
ObjectivesObjectives
On completion of this unit students should be On completion of this unit students should be able to:able to:
State the ten points on general policyState the ten points on general policy
Identify the general strategies of health policyIdentify the general strategies of health policy
State the eight health policy prioritiesState the eight health policy priorities
2.1: General Policy2.1: General Policy– Democratization and decentralization of the Democratization and decentralization of the
health service system.health service system.– Development of preventive and promotive Development of preventive and promotive
components of health care.components of health care.

– Development of an equitable and acceptable standard of Development of an equitable and acceptable standard of health service system that will reach all segments of the health service system that will reach all segments of the population within the limits of resources.population within the limits of resources.
– Promoting and strengthening of intersectoral activities.Promoting and strengthening of intersectoral activities.– Promotion of attitudes and practices conducive to the Promotion of attitudes and practices conducive to the
strengthening of national self-reliance in health strengthening of national self-reliance in health development by mobilizing and maximally utilizing development by mobilizing and maximally utilizing internal and external resources.internal and external resources.
– Assurance of accessibility of health care for all segments Assurance of accessibility of health care for all segments of the population.of the population.
– Working closely with neighboring countries, regional and Working closely with neighboring countries, regional and international organizations to share information and international organizations to share information and strengthen collaboration in all activities contributory to strengthen collaboration in all activities contributory to health development including the control of factors health development including the control of factors detrimental to health.detrimental to health.

– Development of appropriate capacity building Development of appropriate capacity building based on assessed needs.based on assessed needs.
– Provision of health care for the population on a Provision of health care for the population on a scheme of payment according to ability with scheme of payment according to ability with special assistance mechanisms for those who special assistance mechanisms for those who cannot afford to pay.cannot afford to pay.
– Promotion of the participation of the private Promotion of the participation of the private sector and nongovernmental organizations in sector and nongovernmental organizations in health care.health care.

2.2: Priorities of the Policy2.2: Priorities of the PolicyInformation, Education and Communication (I.E.C) of health shall Information, Education and Communication (I.E.C) of health shall
be given appropriate prominence to enhance health awareness be given appropriate prominence to enhance health awareness and to propagate the important concepts and practices of self-and to propagate the important concepts and practices of self-responsibility in healthresponsibility in health
Emphasis shall be given to:Emphasis shall be given to:
The control of communicable diseases, epidemics The control of communicable diseases, epidemics and diseases related to malnutrition and poor living and diseases related to malnutrition and poor living conditions;conditions;
The promotion of occupational health and safety;The promotion of occupational health and safety;
The development of environmental health;The development of environmental health;
The rehabilitation of the health infrastructureThe rehabilitation of the health infrastructure
The development of an appropriate health service The development of an appropriate health service management system;management system;
– Appropriate support shall be given to the curative Appropriate support shall be given to the curative and rehabilitative components of health including and rehabilitative components of health including mental health.mental health.
– Due attention shall be given to the development Due attention shall be given to the development of the beneficial aspects of Traditional Medicine of the beneficial aspects of Traditional Medicine including related research and its gradual including related research and its gradual integration into Modern Medicine.integration into Modern Medicine.
– Applied health research addressing the major Applied health research addressing the major health problems shall be emphasized.health problems shall be emphasized.
– Provision of essential medicines, medical Provision of essential medicines, medical supplies and equipment shall be strengthened.supplies and equipment shall be strengthened.
– Development of human resources with emphasis Development of human resources with emphasis on expansion of the number of frontline and on expansion of the number of frontline and middle level oriented training shall be middle level oriented training shall be undertaken.undertaken.

– Special attention shall be given to the health Special attention shall be given to the health needs of:needs of:
The family particularly women and children;The family particularly women and children;
Those in the forefront of productivity;Those in the forefront of productivity;
Those hitherto most neglected regions and Those hitherto most neglected regions and segments of population including the majority segments of population including the majority of the rural population, pastoralists, the urban of the rural population, pastoralists, the urban poor and national minorities,poor and national minorities,
Victims of man-made and natural disasters.Victims of man-made and natural disasters.
2.3: General Strategies2.3: General StrategiesDemocratization within the system shall be Democratization within the system shall be
implemented by establishing health councils with implemented by establishing health councils with strong community representation at all levels and strong community representation at all levels and health committees at grass-root levels to participate health committees at grass-root levels to participate in identifying major health problems, budgeting, in identifying major health problems, budgeting, planning, implementation, monitoring and evaluating planning, implementation, monitoring and evaluating health activities.health activities.
Decentralization shall be realized through transfer of Decentralization shall be realized through transfer of the major parts of decision-making, health care the major parts of decision-making, health care organization, capacity building, planning, organization, capacity building, planning, implementation and monitoring to the regions with implementation and monitoring to the regions with clear definition of roles.clear definition of roles.
Intersectoral collaboration shall be emphasized Intersectoral collaboration shall be emphasized particularly in:particularly in:

– Enriching the concept and intensifying the Enriching the concept and intensifying the practice of family planning for optimal family practice of family planning for optimal family health and planned population dynamics.health and planned population dynamics.
– Formulating and implementing an appropriate Formulating and implementing an appropriate food and nutrition policy.food and nutrition policy.
– Acceleration the provision of safe and adequate Acceleration the provision of safe and adequate water for urban and rural populations.water for urban and rural populations.
– Developing safe disposal of human, household, Developing safe disposal of human, household, agricultural, and industrial wastes, and agricultural, and industrial wastes, and encouragement of recycling.encouragement of recycling.
– Developing measures to improve the quality of Developing measures to improve the quality of housing and work premises for health.housing and work premises for health.

– Participation in the development of community Participation in the development of community based facilities for the care of the physically and based facilities for the care of the physically and mentally disabled, the abandoned, street mentally disabled, the abandoned, street children and the aged.children and the aged.
– Participating in the development of day-care Participating in the development of day-care centers in factories and enterprises, school centers in factories and enterprises, school health and nutrition programmes.health and nutrition programmes.
– Undertakings in disaster management, Undertakings in disaster management, agriculture, education, communication, agriculture, education, communication, transportation, expansion of employment transportation, expansion of employment opportunities and development of other social opportunities and development of other social services.services.
– Developing facilities for workers’ health and Developing facilities for workers’ health and safety in production sectors.safety in production sectors.

• Health Education shall be strengthened Health Education shall be strengthened generally and for specific target populations generally and for specific target populations through the mass media, community leaders, through the mass media, community leaders, religious and cultural leaders, professional religious and cultural leaders, professional associations, schools and other social associations, schools and other social organizations for:organizations for:– Inculcating attitudes of responsibility for self-care Inculcating attitudes of responsibility for self-care
in health and assurance of safe environment.in health and assurance of safe environment.– Encouraging the awareness and development of Encouraging the awareness and development of
health promotive life-styles and attention to health promotive life-styles and attention to personal hygiene and healthy environment.personal hygiene and healthy environment.
– Enhancing awareness of common communicable Enhancing awareness of common communicable and nutritional diseases and the means for their and nutritional diseases and the means for their prevention.prevention.

– Inculcating attitudes of participation in community Inculcating attitudes of participation in community health development.health development.
– Identifying and discouraging harmful traditional Identifying and discouraging harmful traditional practices while encouraging their beneficial practices while encouraging their beneficial aspects.aspects.
– Discouraging the acquisition of harmful habits Discouraging the acquisition of harmful habits such as cigarette smoking, alcohol consumption, such as cigarette smoking, alcohol consumption, drug abuse and irresponsible sexual behavior.drug abuse and irresponsible sexual behavior.
– Creating awareness in the population about the Creating awareness in the population about the rational use of drugs.rational use of drugs.

• Promotive and Preventive activities shall address:Promotive and Preventive activities shall address:– Control of common endemic and epidemic communicable Control of common endemic and epidemic communicable
and nutritional diseases using appropriate general and and nutritional diseases using appropriate general and specific measures.specific measures.
– Prevention of diseases related to affluence and ageing from Prevention of diseases related to affluence and ageing from emerging as major health problems.emerging as major health problems.
• Prevention of environmental pollution with Prevention of environmental pollution with hazardous chemical wasteshazardous chemical wastes
• Human Resource Development shall focus on:Human Resource Development shall focus on:• Developing of the team approach to health care.Developing of the team approach to health care.• Training of community based task-oriented frontline and Training of community based task-oriented frontline and
middle level health workers of appropriate professional middle level health workers of appropriate professional standards: and recruitment and training of these standards: and recruitment and training of these categories at regional and local levels.categories at regional and local levels.
• Training of trainers, managerial and supportive categories Training of trainers, managerial and supportive categories with appropriate orientation to the health service with appropriate orientation to the health service objectives.objectives.
• Developing of appropriate continuing education for all Developing of appropriate continuing education for all categories of workers in the health sector.categories of workers in the health sector.
• Developing workers within their respective systems of Developing workers within their respective systems of employment.employment.

• Availability of Drugs, supplies and Equipment shall be Availability of Drugs, supplies and Equipment shall be assured by:assured by:
• Preparing lists of essential and standard drugs and Preparing lists of essential and standard drugs and equipment for all levels of the health service system and equipment for all levels of the health service system and continuously updating such lists.continuously updating such lists.
• Encouraging national production capability of drugs, Encouraging national production capability of drugs, vaccines, supplies and equipment by giving appropriate vaccines, supplies and equipment by giving appropriate incentives to firms, which are engaged in manufacture, incentives to firms, which are engaged in manufacture, research and developmentresearch and development
• Developing a standardized and efficient system for Developing a standardized and efficient system for procurement, distribution, storage and utilization of the procurement, distribution, storage and utilization of the products.products.
• Developing quality control capability to assure efficacy Developing quality control capability to assure efficacy and safety of products.and safety of products.
• Developing maintenance and repair facilities for Developing maintenance and repair facilities for equipment.equipment.
• Traditional Medicine shall be accorded appropriate attention by:Traditional Medicine shall be accorded appropriate attention by:
• Identifying and encouraging utilization of its Identifying and encouraging utilization of its beneficial aspects.beneficial aspects.
• Coordinating and encouraging research including its Coordinating and encouraging research including its linkage with modern medicine.linkage with modern medicine.
• Developing appropriate regulation and registration Developing appropriate regulation and registration for its practice.for its practice.– Health systems Research shall be given due emphasis by:Health systems Research shall be given due emphasis by:
• Identifying priority areas for research in health.Identifying priority areas for research in health.• Expanding applied research on major health problems and health Expanding applied research on major health problems and health
service systems.service systems.• Strengthening the research capabilities of national institutions and Strengthening the research capabilities of national institutions and
scientists in collaboration with the responsible agencies.scientists in collaboration with the responsible agencies.• Developing appropriate measures to assure strict observance of Developing appropriate measures to assure strict observance of
ethical principles in research.ethical principles in research.

– Family Health Services shall be promoted by:Family Health Services shall be promoted by:• Assuring adequate maternal health care and referral Assuring adequate maternal health care and referral
facilities for high risk pregnancies.facilities for high risk pregnancies.• Intensifying family planning for the optimal health of the Intensifying family planning for the optimal health of the
mother, child and family.mother, child and family.• Inculcating principles of appropriate maternal nutrition.Inculcating principles of appropriate maternal nutrition.• Maintaining breast-feeding and advocating home-made Maintaining breast-feeding and advocating home-made
preparation, production and availability of weaning foods preparation, production and availability of weaning foods at affordable prices.at affordable prices.
• Expanding and strengthening immunization services, Expanding and strengthening immunization services, optimization of access and utilization.optimization of access and utilization.
• Encouraging early utilization of available health care Encouraging early utilization of available health care facilities for management of common childhood diseases facilities for management of common childhood diseases particularly diarrhoeal diseases and acute respiratory particularly diarrhoeal diseases and acute respiratory infections.infections.
• Addressing the special health problems and related Addressing the special health problems and related needs of adolescents.needs of adolescents.
• Encouraging paternal involvement in family health.Encouraging paternal involvement in family health.• Identifying and discouraging harmful traditional practices Identifying and discouraging harmful traditional practices
while encouraging their beneficial aspects.while encouraging their beneficial aspects.
• Referral System shall be developed by:Referral System shall be developed by:• Optimizing utilization of health care facilities at all levels.Optimizing utilization of health care facilities at all levels.• Improving accessibility of care according to needsImproving accessibility of care according to needs• Assuring continuity and improved quality of care at all Assuring continuity and improved quality of care at all
level.level.• Rationalizing costs for health care seeders and providers Rationalizing costs for health care seeders and providers
for optimal utilization of health care facilities at all levelsfor optimal utilization of health care facilities at all levels• Strengthening the communication within the health care Strengthening the communication within the health care
system.system.
• Diagnostic and Supportive Services for health care shall Diagnostic and Supportive Services for health care shall be developed by:be developed by:
• Strengthening the scientific and technical bases of health Strengthening the scientific and technical bases of health care.care.
• Facilitating prompt diagnosis and treatment.Facilitating prompt diagnosis and treatment.• Providing guidance in continuing care.Providing guidance in continuing care.
• Health Management information system shall Health Management information system shall be organized by:be organized by:– Making the system appropriate and relevant for Making the system appropriate and relevant for
decision making, planning, implementing, decision making, planning, implementing, monitoring and evaluation.monitoring and evaluation.
– Maximizing the utilization of information at all Maximizing the utilization of information at all levelslevels
– Developing central and regional information Developing central and regional information documentation centers.documentation centers.

• Health Legislations shall be revised by.Health Legislations shall be revised by.
• Up-dating existing public health laws and Up-dating existing public health laws and regulations.regulations.
• Developing new rules and regulations to help Developing new rules and regulations to help in the implementation of the current policy in the implementation of the current policy and addressing new health issuesand addressing new health issues
• Strengthening mechanisms for Strengthening mechanisms for implementation of health laws and regulationsimplementation of health laws and regulations

– Health Service Organization shall be Health Service Organization shall be systematized and rationalized by:systematized and rationalized by:
• Standardizing the human resource, physical Standardizing the human resource, physical facilities and operational systems of the facilities and operational systems of the health units at all levels.health units at all levels.
• Defining and instituting the catchments areas Defining and instituting the catchments areas of health units and referral systems based on of health units and referral systems based on assessment of pertinent factors.assessment of pertinent factors.
• Regulating private health care and Regulating private health care and professional development by appropriate professional development by appropriate licensing.licensing.

– Administration and Management of the health Administration and Management of the health system shall be strengthened and made more system shall be strengthened and made more effective and efficient by:effective and efficient by:• Restructuring and organizing at all levels in line with Restructuring and organizing at all levels in line with
the present policy of decentralization and the present policy of decentralization and democratization of decision-making and management.democratization of decision-making and management.
• Combining departments and services which are Combining departments and services which are closely related and rationalizing the utilization of closely related and rationalizing the utilization of human and material resources.human and material resources.
• Studying the possibility of designating under Studying the possibility of designating under secretaries to ensure continuity of service.secretaries to ensure continuity of service.
• Creating management boards for national hospitals, Creating management boards for national hospitals, institutions and organizations.institutions and organizations.
• Allowing health institutions to utilize their income to Allowing health institutions to utilize their income to improve their services.improve their services.
• Ensuring placement of appropriately qualified and Ensuring placement of appropriately qualified and motivated personnel at all levels.motivated personnel at all levels.

– Financing the Health services shall be through public, private Financing the Health services shall be through public, private and international sources and the following options shall be and international sources and the following options shall be considered and evaluated.considered and evaluated.
• Raising taxes and revenues.Raising taxes and revenues.• Formal contribution or insurance by public employees.Formal contribution or insurance by public employees.• Legislative requirements of a contributory health fund for Legislative requirements of a contributory health fund for
employee of the private sector.employee of the private sector.• Individual or group health insurance.Individual or group health insurance.• Voluntary contributions.Voluntary contributions.

UNIT III: STRUCTURE OF HEALTHCAREUNIT III: STRUCTURE OF HEALTHCARE
SERVICE ORGANIZATIONSERVICE ORGANIZATION
UNIT OUTLINEUNIT OUTLINE
1. Structure of the healthcare service 1. Structure of the healthcare service organizationorganization
• FederalFederal
• RegionalRegional
• District/WoredaDistrict/Woreda

2. The roles of various agencies in health 2. The roles of various agencies in health promotionpromotion
• GovernmentGovernment
• Multi-laterals (e.g. WHO [world Health Multi-laterals (e.g. WHO [world Health Organization ])Organization ])
• Bi-laterals (e.g. USAID [United States Bi-laterals (e.g. USAID [United States Agency for International Development ])Agency for International Development ])
• NGOs (e.g. AMREF [African Medical and NGOs (e.g. AMREF [African Medical and Research Foundation])Research Foundation])
• Private providers (PO’s)Private providers (PO’s)

3.1: Structure of the Healthcare Service 3.1: Structure of the Healthcare Service OrganizationOrganization
3.1.1. Introduction3.1.1. Introduction• The mechanism through which health services are The mechanism through which health services are
organized and delivered in Ethiopia function as a organized and delivered in Ethiopia function as a complex system, in which providers, consumers and complex system, in which providers, consumers and regulators of the health service interact. The system regulators of the health service interact. The system responds to changes in the external environment responds to changes in the external environment which include changes in:which include changes in:
• Medical knowledge and technology,Medical knowledge and technology,• Political and economic situation of the country,Political and economic situation of the country,• Social norms and valuesSocial norms and values• Population health and disease processes.Population health and disease processes.

• Understanding the work of the major players Understanding the work of the major players within the national health system and the within the national health system and the many ways in which they interact provides a many ways in which they interact provides a basis for managing the system to improve basis for managing the system to improve accessibility, quality and cost of the accessibility, quality and cost of the services .The health care delivery system in services .The health care delivery system in Ethiopia is a universal national system and in Ethiopia is a universal national system and in order to understand the system the major order to understand the system the major actors within the system must be identified, actors within the system must be identified, the resources on which these actors depend the resources on which these actors depend must be identified and the external must be identified and the external environment which affects these actors must environment which affects these actors must also be identified. The major actors are:also be identified. The major actors are:

• the healthcare providersthe healthcare providers
• the healthcare consumersthe healthcare consumers
• the policymakers and regulatorsthe policymakers and regulators
• The resources used by these actors include:The resources used by these actors include:
• fundingfunding
• facilityfacility
• personnelpersonnel
• technologytechnology
• InformationInformation
• The various components are organized into The various components are organized into the following structures:the following structures:

3.1.2. Administrative Structure of the 3.1.2. Administrative Structure of the Healthcare System OrganizationsHealthcare System Organizations
• The health service organization and The health service organization and management used to be centralized with management used to be centralized with very little community participation.very little community participation.
• This had an undesirable impact on efficiency, This had an undesirable impact on efficiency, resource allocation, human resource resource allocation, human resource development, and utilizationof health development, and utilizationof health services.services.

• A decentralized system was put into place A decentralized system was put into place when in 1990, under the transitional when in 1990, under the transitional government , Ethiopia became a Federal government , Ethiopia became a Federal Democratic Republic composed of 9 National Democratic Republic composed of 9 National Regional States (NRS) which are; Tigray, Regional States (NRS) which are; Tigray, Afar, Amhara , Oromia, Somalia, Afar, Amhara , Oromia, Somalia, Benishangul-Gumuz, Southern Nations Benishangul-Gumuz, Southern Nations Nationalities and Peoples Region Nationalities and Peoples Region (SNNPR),Gambella, and Harari, (SNNPR),Gambella, and Harari, Administrative states (Addis Ababa city Administrative states (Addis Ababa city administration and Dire Dawa council).administration and Dire Dawa council).
• The national regional states as well as the The national regional states as well as the two cities administrative councils are further two cities administrative councils are further divided into six hundred eleven woredas and divided into six hundred eleven woredas and around 15,000 kebeles (5,000 Urban and around 15,000 kebeles (5,000 Urban and 10,000 Rural).10,000 Rural).
• Arguably, the most significant policy Arguably, the most significant policy influencing the Health Sector Development influencing the Health Sector Development Program (HSDP) design and implementation Program (HSDP) design and implementation is the policy on decentralization. This is well is the policy on decentralization. This is well articulated within the constitution and in a articulated within the constitution and in a number of major and supplementary number of major and supplementary proclamations, and provides the proclamations, and provides the administrative context in which health sector administrative context in which health sector activities take place.activities take place.

• Important steps have been taken in the Important steps have been taken in the decentralization of the health care system. decentralization of the health care system. Decision-making processes in the development and Decision-making processes in the development and implementation of the health system are shared implementation of the health system are shared between the Federal Ministry of Health (FMOH), between the Federal Ministry of Health (FMOH), the Regional Health Bureaus (RHBs) and the the Regional Health Bureaus (RHBs) and the Woreda Health Offices (WHO). As a result of recent Woreda Health Offices (WHO). As a result of recent policy measures taken by the Government, the policy measures taken by the Government, the FMoH and the RHBs are made to function more on FMoH and the RHBs are made to function more on policy matters and technical support, while the policy matters and technical support, while the woreda health offices have been made to play the woreda health offices have been made to play the pivotal roles of managing and coordinating the pivotal roles of managing and coordinating the operation of the primary health care services at the operation of the primary health care services at the woreda levels.woreda levels.

• The powers and duties of the Ministry of The powers and duties of the Ministry of Health (MOH) according to proclamation 4/87 Health (MOH) according to proclamation 4/87 are to:are to:
– Cause the expansion of health servicesCause the expansion of health services
• Establish and administer referral hospitals as Establish and administer referral hospitals as well as study and research centerswell as study and research centers
• Determine standards to be maintained by Determine standards to be maintained by health services; except insofar as such power health services; except insofar as such power is expressly given by law to another organ, is expressly given by law to another organ, issue licenses to and supervise hospitals and issue licenses to and supervise hospitals and health services established by foreign health services established by foreign organizations and investorsorganizations and investors

• Determine qualifications of professionals required Determine qualifications of professionals required for engaging in public health services at various for engaging in public health services at various levels; issue certificates of competence to samelevels; issue certificates of competence to same
• Cause the study of traditional medicines; organize Cause the study of traditional medicines; organize research and experimental centers for sameresearch and experimental centers for same
• Cause research to be undertaken on traditional Cause research to be undertaken on traditional medicines and, for this purpose, organize centers medicines and, for this purpose, organize centers for research and experimentfor research and experiment
• Devise and follow up the implementation of ways Devise and follow up the implementation of ways and means of preventing and eradicating and means of preventing and eradicating communicable diseasescommunicable diseases
• Undertake the necessary quarantine controls to Undertake the necessary quarantine controls to protect public healthprotect public health

– Structure of the Ethiopian Health SystemStructure of the Ethiopian Health System
I. Structure of Federal Ministry of Health I. Structure of Federal Ministry of Health (FMoH(FMoH))
• The FMOH is responsible for setting the The FMOH is responsible for setting the health policy and giving technical support. health policy and giving technical support. The organogram below represents the The organogram below represents the administrative structure of the FMOH.administrative structure of the FMOH.
• organogram of the federal ministry of healthorganogram of the federal ministry of health• Minister of HealthMinister of Health• Vice MinisterVice Minister• Legal and Medico-legal ServiceLegal and Medico-legal Service• Public Relation ServicePublic Relation Service• Plan and Program DepartmentPlan and Program Department• Pharmaceutical Supply and Administration ServicePharmaceutical Supply and Administration Service• Disease Prevention and control Dept.Disease Prevention and control Dept.• Malaria and vector borne disease prevention teamMalaria and vector borne disease prevention team• HIV/AIDS and other STD prevention and control HIV/AIDS and other STD prevention and control
teamteam• TB and leprosy prevention and controlTB and leprosy prevention and control

• Other diseases prevention and control teamOther diseases prevention and control team• Hygiene and Env’tal Health DeptHygiene and Env’tal Health Dept• Water quality and sanitary control teamWater quality and sanitary control team• Food, drink and herbal preservation control TeamFood, drink and herbal preservation control Team• Quarantine service teamQuarantine service team• Industrial and other institution health control systemIndustrial and other institution health control system• Family Health DeptFamily Health Dept• Health and Nutrition Research InstituteHealth and Nutrition Research Institute• Health Service teamHealth Service team• Specialized hospitalsSpecialized hospitals• Health psychosocial educator and training teamHealth psychosocial educator and training team• Health Educator CenterHealth Educator Center• Panel of assessorsPanel of assessors• Babies, children and yoBabies, children and yo

• Family planning teamFamily planning team
• Women’s healthcare teamWomen’s healthcare team
• Health Service and Training DeptHealth Service and Training Dept
• Audit ServiceAudit Service
• Organization and Management ServiceOrganization and Management Service
• Women’s Affairs DepartmentWomen’s Affairs Department
• Administrator and Finance ServiceAdministrator and Finance Service
• Service Delivery Administrative PopulationService Delivery Administrative Population

– Ethiopian health facilities, their administrative Ethiopian health facilities, their administrative bodies and the population served by thembodies and the population served by them
• Health Centers (PHCU) Woreda Health Health Centers (PHCU) Woreda Health Office 25,000Office 25,000
• District Hospitals Zonal health department District Hospitals Zonal health department 250.000250.000
• Zonal Hospitals Regional health bureaus Zonal Hospitals Regional health bureaus 1,000,0001,000,000
• Specialized Hospitals Ministry of health Specialized Hospitals Ministry of health 5,000,0005,000,000

• II. Structure of Regional Health Bureau (RHB)II. Structure of Regional Health Bureau (RHB)• Organogram of regional health bureausOrganogram of regional health bureaus• Bureau HeadBureau Head• AdvisorAdvisor• Regional Laboratory Auditing serviceRegional Laboratory Auditing service• Administration and Logistics Planning and Administration and Logistics Planning and
Programming serviceProgramming service• Hospital Desk AssistanceHospital Desk Assistance• Disease prevention and Health programs Disease prevention and Health programs
DepartmentDepartment• Surveillance teamSurveillance team• Child Health TeamChild Health Team• Pharmacy and Traditional med. TeamPharmacy and Traditional med. Team
• Health workers Training SchoolHealth workers Training School• Maternal and Reproductive Health teamMaternal and Reproductive Health team• Health service organization and Expansion teamHealth service organization and Expansion team• Training TeamTraining Team• Health sanitation Health sanitation • Coding and Processing TeamCoding and Processing Team• TB and HIV/AIDS and STI prevention TeamTB and HIV/AIDS and STI prevention Team• Family Health DepartmentFamily Health Department• Health service organization and Expansion Health service organization and Expansion
DepartmentDepartment• Training Health coding and Guideline HeadTraining Health coding and Guideline Head• Public relationPublic relation• Deputy Bureau HeadDeputy Bureau Head• Regional LaboratoryRegional Laboratory

III. Structure of District/Woreda Health Office III. Structure of District/Woreda Health Office (WrHO)(WrHO)
Organogram of district/woreda health officesOrganogram of district/woreda health offices• Woreda health office HeadWoreda health office Head• Deputy Woreda health office HeadDeputy Woreda health office Head• Maternal and child health teamMaternal and child health team• Communicable disease and surveillance teamCommunicable disease and surveillance team• HIV control teamHIV control team• Environmental health teamEnvironmental health team• Malaria control teamMalaria control team• Health extension programHealth extension program• Logistics and pharmacy unitLogistics and pharmacy unit• Planning and program unitPlanning and program unit

3.2: Contributors of Health Care Provision in 3.2: Contributors of Health Care Provision in EthiopiaEthiopia
IntroductionIntroduction
• The main healthcare providers in Ethiopia are:The main healthcare providers in Ethiopia are:
• the Governmentthe Government
• Private providersPrivate providers
• Non-governmentNon-government
• International Health Agencies:International Health Agencies:– Multilateral AgenciesMultilateral Agencies– Bilateral AgenciesBilateral Agencies

3.2.1 The Government3.2.1 The Government• For many countries, especially in the developing For many countries, especially in the developing
countries, it is very likely that the government countries, it is very likely that the government remain theremain the
• largest single provider of health care giving an largest single provider of health care giving an impression of dominating health care provision.impression of dominating health care provision.
3.2.2 Private Providers3.2.2 Private Providers• Private providers work for profit and increasingly Private providers work for profit and increasingly
the private providers are getting involved in the the private providers are getting involved in the delivery of health services. Nearly all pharmacies delivery of health services. Nearly all pharmacies (drug stores) are privately owned. The role of (drug stores) are privately owned. The role of private hospital and clinics and medical services is private hospital and clinics and medical services is growing especially in urban areas and those who growing especially in urban areas and those who afford can be managed there and help in reducing afford can be managed there and help in reducing load at government facilities.load at government facilities.

3.2.3 Nongovernmental Agencies (NGO’s3.2.3 Nongovernmental Agencies (NGO’s))• NGO’s are sometimes known “people to people” aid; NGO’s are sometimes known “people to people” aid;
their activities are sometimes very specific, for their activities are sometimes very specific, for example targeting Trachoma and cataracts. Where example targeting Trachoma and cataracts. Where as some have more general agendas, for example as some have more general agendas, for example aid for orphans.aid for orphans.
• They are usually funded by voluntary donations They are usually funded by voluntary donations although some act under contract to governments although some act under contract to governments and other agencies. The largest and NGO is the and other agencies. The largest and NGO is the international Red Cross which has national offices international Red Cross which has national offices within most countries.within most countries.
• Other well known NGO’s are USAID, CDC, Oxford Other well known NGO’s are USAID, CDC, Oxford Famine Relief (OXFAM), Care international, save Famine Relief (OXFAM), Care international, save the children.the children.

3.2.4 International Health Agencies3.2.4 International Health Agencies• International Health agencies play an auxiliary role. They International Health agencies play an auxiliary role. They
are funded by member governments.are funded by member governments.• A) Multilateral AgenciesA) Multilateral Agencies• The leader among such agencies is the World Health The leader among such agencies is the World Health
Organization (WHO), which began its work in 1948Organization (WHO), which began its work in 1948• in Geneva under the United Nation (UN) .Its headquarters, in Geneva under the United Nation (UN) .Its headquarters,
is in Geneva. It has six regional offices andis in Geneva. It has six regional offices and• representatives in most of its 200 member countries. Its representatives in most of its 200 member countries. Its
tasks are:tasks are:• to review and approve policies and program initiativesto review and approve policies and program initiatives• to coordinate and promote technical cooperation among to coordinate and promote technical cooperation among
countriescountries• facilitate training and technical assistancefacilitate training and technical assistance• assimilate, analyze and disseminate health related dataassimilate, analyze and disseminate health related data

• A good example of its achievement is the way A good example of its achievement is the way it leads in the eradication of smallpox in 1979.it leads in the eradication of smallpox in 1979.
• Other such multilateral agencies are:Other such multilateral agencies are:• UNICEF – a program concerned with the UNICEF – a program concerned with the
healthcare of infants and childrenhealthcare of infants and children• United Nation Development Program (UNDP)United Nation Development Program (UNDP)• World Bank (WB)World Bank (WB)• UNAIDS – is a program for HIV/AIDSUNAIDS – is a program for HIV/AIDS• Food and Agriculture Organization (FAO)Food and Agriculture Organization (FAO)• United Fund for Population Activities (UNFPA)United Fund for Population Activities (UNFPA)

B) Bilateral AgenciesB) Bilateral Agencies• The most industrialized nations provide aid on a The most industrialized nations provide aid on a
country to country basis, attempting to match the country to country basis, attempting to match the recipients need with the donor’s objectives and recipients need with the donor’s objectives and capacity to assist, usually subjects to political capacity to assist, usually subjects to political considerations. The United States links aid to considerations. The United States links aid to democratic reforms and human rights.democratic reforms and human rights.
• In 2004 only five countries met the United Nations In 2004 only five countries met the United Nations target of contributing 0.7% of gross national product target of contributing 0.7% of gross national product in official development assistance. These countries in official development assistance. These countries are Norway, Denmark, the Netherlands, are Norway, Denmark, the Netherlands, Luxembourg, and Sweden. In contrast to the United Luxembourg, and Sweden. In contrast to the United States provided only 0.16% and the UK 0.36%.States provided only 0.16% and the UK 0.36%.

• Donor countries often rely on their own Donor countries often rely on their own expertise through competitive bidding to expertise through competitive bidding to design, implement, anddesign, implement, and
• monitor projects funded under bilateral monitor projects funded under bilateral agreements, sometimes requiring that the agreements, sometimes requiring that the donors own products and services be used. donors own products and services be used. It is critical that such development assistance It is critical that such development assistance is effectively placed, and fairly counted, so as is effectively placed, and fairly counted, so as to help build sustainable capacities for all the to help build sustainable capacities for all the people of the world.people of the world.

UNIT IV: COMPONENTS OF THEUNIT IV: COMPONENTS OF THE
HEALTHCARE DELIVERY SYSTEMHEALTHCARE DELIVERY SYSTEM
IntroductionIntroduction• The universal goal of any health systems is to The universal goal of any health systems is to
ensure access to high-quality services to all ensure access to high-quality services to all members of its society for as little cost as possible. members of its society for as little cost as possible. The decentralized health policy has different levels The decentralized health policy has different levels of health care delivery systems (Primary health of health care delivery systems (Primary health care unit, district hospital, zonal hospital and care unit, district hospital, zonal hospital and referral hospital). In this unit we will deal with the referral hospital). In this unit we will deal with the components of health care delivery system level by components of health care delivery system level by level and see the activities carried out in each level.level and see the activities carried out in each level.

4.1: Components of Healthcare Delivery 4.1: Components of Healthcare Delivery SystemSystem
4.1.1. Introduction4.1.1. Introduction
• The universal goal of any health systems is to The universal goal of any health systems is to ensure access to high-quality services to all ensure access to high-quality services to all members of its society for as little cost as members of its society for as little cost as possible. This involves three key areas:possible. This involves three key areas:
• accessibilityaccessibility
• quality and,quality and,
• cost efficiencycost efficiency

• Efforts to increase access to care within the Efforts to increase access to care within the system may lead to higher costs, while system may lead to higher costs, while efforts to limit health-care costs may have efforts to limit health-care costs may have adverse effects on access. In order to adverse effects on access. In order to address gaps in the accessibility and quality address gaps in the accessibility and quality of healthcare services new strategies have of healthcare services new strategies have been implemented by replacing the old six been implemented by replacing the old six tier system in to the new four tier system. tier system in to the new four tier system. There are efforts to reorganize the 4 tier There are efforts to reorganize the 4 tier system into 3 tiers, but this has not been system into 3 tiers, but this has not been finalized.finalized.

4.1.2. The Current 4 Tiers System4.1.2. The Current 4 Tiers System• The current 4 tiers system is organized as:The current 4 tiers system is organized as:• First tier: Primary Healthcare Unit (which is made First tier: Primary Healthcare Unit (which is made
up of 1 health center and 5 health posts, serving up of 1 health center and 5 health posts, serving 25,000 people)25,000 people)
• Second tier: District Hospital (serving 250,000 Second tier: District Hospital (serving 250,000 peoplepeople
• Third tier: Zonal hospital (serving 1 million people)Third tier: Zonal hospital (serving 1 million people)• Fourth tier: Referral Hospital.Fourth tier: Referral Hospital.• Health care tier system with their basic parametersHealth care tier system with their basic parameters
– Zonal/Regional Hospital (ref) 1,000,000 populationZonal/Regional Hospital (ref) 1,000,000 population– District Hospital 250,000 populationsDistrict Hospital 250,000 populations– Primary health care unit (PHCU) With 5 CHPs 25,000 Primary health care unit (PHCU) With 5 CHPs 25,000
populationpopulation– Referral Hospital 5,000,000 populationReferral Hospital 5,000,000 population

• Main Issues Addressed by the PyramidMain Issues Addressed by the Pyramid• The above figure depicts the basic parameters and The above figure depicts the basic parameters and
levels of health care interactions within the pyramid levels of health care interactions within the pyramid and out of the pyramid. It illustrates the referral and out of the pyramid. It illustrates the referral linkages and administrative supervisory linkage linkages and administrative supervisory linkage pathways with the population served at each level pathways with the population served at each level of health care unit.of health care unit.
• The base of the pyramid is formed by primary The base of the pyramid is formed by primary health care unit that consists of a single health health care unit that consists of a single health center with five health posts and supervised by center with five health posts and supervised by Woreda Health Office (WrHO) and expected to Woreda Health Office (WrHO) and expected to report to the supervising woreda. Also the referral report to the supervising woreda. Also the referral system linkage in the primary health care unit is system linkage in the primary health care unit is arranged in such a way that all the five health posts arranged in such a way that all the five health posts refer their patients/cases to the Health Centers refer their patients/cases to the Health Centers (HC) for better management and cases that need (HC) for better management and cases that need referral from HC are referred to District Hospital.referral from HC are referred to District Hospital.

• At the second line of the pyramid is district hospital. At the second line of the pyramid is district hospital. It is accountable to receive referral from HC and It is accountable to receive referral from HC and should give feedback to them, and cases that should give feedback to them, and cases that cannot be managed at district hospital level are cannot be managed at district hospital level are referred to Zonal hospital and the last level of referred to Zonal hospital and the last level of referral system within the country will last at the referral system within the country will last at the level of specialized hospital Administrative level of specialized hospital Administrative accountability is shown by a broken line arrow at accountability is shown by a broken line arrow at the right side of the pyramid. Regarding to the the right side of the pyramid. Regarding to the supervision and administrative support in the supervision and administrative support in the hierarchy of FMOH, FMoH supervises RHB, and hierarchy of FMOH, FMoH supervises RHB, and RHB supervises WrHO through delegated actor RHB supervises WrHO through delegated actor known as zonal Health Departments (ZHD). And known as zonal Health Departments (ZHD). And the ZHDs supervise WrHO and woreda Health the ZHDs supervise WrHO and woreda Health office supervise PHCUoffice supervise PHCU

4.1.3. Major Components and Actors of 4.1.3. Major Components and Actors of Healthcare Delivery SystemHealthcare Delivery System
• The major components and actors of the healthcare The major components and actors of the healthcare delivery system are:delivery system are:
• The health facilitiesThe health facilities• Health PostsHealth Posts• Health CentersHealth Centers• • • Beds=10Beds=10• • • Ts+13+15Ts+13+15• • • NTs=12NTs=12• District Hospitals (Primary Hospitals)District Hospitals (Primary Hospitals)• • • Beds=50Beds=50• • • Ts=33Ts=33• • • NTs=35NTs=35

• Zonal Hospitals (Regional Hospitals)Zonal Hospitals (Regional Hospitals)
• • Beds=100Beds=100• Ts= 60Ts= 60• NTs=50NTs=50
• Specialized Hospitals (Referral Hospitals)Specialized Hospitals (Referral Hospitals)• 250 beds250 beds• Ts= 120Ts= 120• NTS= 50NTS= 50
• Note:Note: Ts = Technical staff; NTs= Non- Ts = Technical staff; NTs= Non-technical stafftechnical staff

• The health workforce/personnelThe health workforce/personnel• Medical staff: Are the personnel consisting of Medical staff: Are the personnel consisting of
physician who have received extensive training and physician who have received extensive training and granted to give clinical service.granted to give clinical service.
• Administrative staff: staffs who are involved in Administrative staff: staffs who are involved in leadership and management like Chief Executive leadership and management like Chief Executive OfficerOfficer
• (CEO), Chief Financial Officer, Chief Information (CEO), Chief Financial Officer, Chief Information Officer Etc…Officer Etc…
• Supportive staff: clinical supports are activities Supportive staff: clinical supports are activities carried out by pharmaceutical service, food and carried out by pharmaceutical service, food and nutritionservices, Health Information management, nutritionservices, Health Information management, social work and social service, patient advocacy social work and social service, patient advocacy service, purchasing central supply and material service, purchasing central supply and material supply management servicessupply management services

4.2: The Health Care Facilities and Services 4.2: The Health Care Facilities and Services they Providethey Provide
• In order to properly implement the In order to properly implement the delivery of health services the role of each delivery of health services the role of each type of health facility/institution is type of health facility/institution is determined. This in turn determines the determined. This in turn determines the professional mix of the staff assigned to each professional mix of the staff assigned to each type of health facility.type of health facility.

4.2.1. The Primary Healthcare Unit (PHCU)4.2.1. The Primary Healthcare Unit (PHCU)
• The PHCU consists of Health Post and The PHCU consists of Health Post and Health center. The Health Sector Health center. The Health Sector Development Program document of the Development Program document of the Ministry of Health (MOH) describes PHCU is Ministry of Health (MOH) describes PHCU is an important component of the Health an important component of the Health System in Ethiopia.System in Ethiopia.

• A comprehensive PHCU services is to be A comprehensive PHCU services is to be delivered through community-based health delivered through community-based health services by the HealthExtension Program services by the HealthExtension Program (HEP) at Health Posts (HP) and household (HEP) at Health Posts (HP) and household levels, and further through Health levels, and further through Health Centers(HC) and p. Basically the PHCU is Centers(HC) and p. Basically the PHCU is the health service delivery organized and the health service delivery organized and managed at District level withinthe managed at District level withinthe decentralized system of the Ethiopian decentralized system of the Ethiopian Government at the Woreda Health System Government at the Woreda Health System (WHS)(WHS)
A) Health PostsA) Health Posts• The Health Post (HP) represents the first The Health Post (HP) represents the first
contact of the health care system and it is contact of the health care system and it is considered the first contact level between the considered the first contact level between the service provider and the client. The HP service provider and the client. The HP provides mainly preventive and Promotive provides mainly preventive and Promotive services (health education), but also some services (health education), but also some limited services of very basic curative care. limited services of very basic curative care. Most cases are referred to the next level, the Most cases are referred to the next level, the Health Center, which is still within the first tier Health Center, which is still within the first tier (i.e. within the PHCU). The HP provides its (i.e. within the PHCU). The HP provides its services to a catchment population of services to a catchment population of approximately 3,000-5,000.approximately 3,000-5,000.
• All community-based health services All community-based health services provided at outreach site and house hold provided at outreach site and house hold level services and at the HP are level services and at the HP are administratively supervised by Woreda administratively supervised by Woreda Health Office and Kebele Council and Health Office and Kebele Council and technically by the Health Centers in the technically by the Health Centers in the catchments area. A health post is run by two catchments area. A health post is run by two Health Extension Workers (HEWs). Health Extension Workers (HEWs). Summary of Job accomplished by HEWSummary of Job accomplished by HEW

• Provide health educationProvide health education• Promote community nutritionPromote community nutrition• Provide Antenatal Health Care (ANC)Provide Antenatal Health Care (ANC)• Provide Postnatal Care (PNC)Provide Postnatal Care (PNC)• Promote and provide family planning servicePromote and provide family planning service• Implement hygiene and environmental health serviceImplement hygiene and environmental health service• Provide first aid and basic clinical serviceProvide first aid and basic clinical service• Provide delivery serviceProvide delivery service• Implement immunization serviceImplement immunization service• Collect and maintain population health dataCollect and maintain population health data

B) Health CenterB) Health Center• The Health Center (HC) with its five satellite The Health Center (HC) with its five satellite
Health Posts, is designed to render integrated Health Posts, is designed to render integrated promotive, preventive, basic curative and promotive, preventive, basic curative and rehabilitative services. The Health Centre (HC) rehabilitative services. The Health Centre (HC) represents the first level of the health care system for represents the first level of the health care system for curative services, and serves a catchment population curative services, and serves a catchment population of 25,000. A standard HC has a capacity of 10 beds of 25,000. A standard HC has a capacity of 10 beds and provides 24 hour emergency medical care and provides 24 hour emergency medical care services, treatment of common medical problems, services, treatment of common medical problems, basic obstetric care, basic laboratory and basic obstetric care, basic laboratory and pharmaceutical services. The medical conditions that pharmaceutical services. The medical conditions that are expected to be managed at this level are are expected to be managed at this level are handled by:handled by:
• Clinical officers/Health OfficersClinical officers/Health Officers
• Nurses and,Nurses and,
• Midwives.Midwives.
• The function of the Health Center is The function of the Health Center is organized into five components based on the organized into five components based on the Health Service Extension Program.Health Service Extension Program.
– Family health service: Family Health Services that are Family health service: Family Health Services that are expected to be provided at this level include:expected to be provided at this level include:

I. Maternal and newborn care services including:I. Maternal and newborn care services including:• antenatal care (ANC),antenatal care (ANC),• delivery and newborn care services,delivery and newborn care services,• postnatal care (PNC), andpostnatal care (PNC), and• family planning (FP)family planning (FP)
II. Child health services including:II. Child health services including:• Integrated management of childhood illnesses (IMCI)Integrated management of childhood illnesses (IMCI)• Growth monitoring and promotionGrowth monitoring and promotion• ImmunizationImmunization• Adolescent reproductive health services (ARH) andAdolescent reproductive health services (ARH) and• Promotion of essential nutrition action (ENA).Promotion of essential nutrition action (ENA).

• Communicable Disease Prevention and Communicable Disease Prevention and Control Services: services provided under Control Services: services provided under this component are related to the following this component are related to the following major categories:major categories:
• Tuberculosis and Leprosy:Tuberculosis and Leprosy:– Clinical diagnosis and treatment,Clinical diagnosis and treatment,– Management of complications and adverse Management of complications and adverse
drug reactions,drug reactions,– Training, advice and treatment of leprosy Training, advice and treatment of leprosy
patients on disability,patients on disability,– Refer cases to the HP for follow up when Refer cases to the HP for follow up when
supported by established mechanism of supported by established mechanism of information and patient flow systemsinformation and patient flow systems

b) HIV/AIDS and STI: the services provided at the b) HIV/AIDS and STI: the services provided at the HC level are:HC level are:– IEC on transmission and prevention of HIV/AIDS and STI,IEC on transmission and prevention of HIV/AIDS and STI,– Support and guidance to families on home-based care,Support and guidance to families on home-based care,– Condom promotion and distribution,Condom promotion and distribution,– VCT and PMTCT services,VCT and PMTCT services,– Treatment of common opportunistic infections such as Treatment of common opportunistic infections such as
TB, PCP, toxoplasmosis, and candidiasis in diagnosed TB, PCP, toxoplasmosis, and candidiasis in diagnosed HIV/AIDS casesHIV/AIDS cases
– Identification and referral of patients eligible for ART,Identification and referral of patients eligible for ART,– Follow up of ART patients with no complications,Follow up of ART patients with no complications,– Provide Syndromic management of STIProvide Syndromic management of STI
c) Epidemic diseases:c) Epidemic diseases: Ensure adequate and Ensure adequate and timely preparedness, Investigate, confirm timely preparedness, Investigate, confirm and provide free treatment to cases of and provide free treatment to cases of epidemics of all the reportable epidemic epidemics of all the reportable epidemic prone disease.prone disease.
• Epidemic prone diseasesEpidemic prone diseases– CholeraCholera– Diarrhea with blood (Shigella)Diarrhea with blood (Shigella)– MeaslesMeasles– MeningitisMeningitis– PlaguePlague– Viral hemorrhagic feversViral hemorrhagic fevers– Yellow feverYellow fever

• Diseases targeted for elimination/eradicationDiseases targeted for elimination/eradication• Acute flaccid paralysis(AFP/Polio)Acute flaccid paralysis(AFP/Polio)• MeaslesMeasles• Neonatal TetanusNeonatal Tetanus• LeprosyLeprosy• Dracunculiasis (Guinea worm)Dracunculiasis (Guinea worm)• Other diseases of public health importance Other diseases of public health importance • Pneumonia in children less than 5 yrs of agePneumonia in children less than 5 yrs of age• Diarrhea in children less than 5 yrs of ageDiarrhea in children less than 5 yrs of age• New AIDS casesNew AIDS cases• MalariaMalaria• OnchocerciasisOnchocerciasis• Sexually transmitted infections(STIs)Sexually transmitted infections(STIs)• TrypanosomiasisTrypanosomiasis• TuberculosisTuberculosis

d) Rabies:d) Rabies:• Provision of full course of anti rabies vaccination,Provision of full course of anti rabies vaccination,• Refer clinical cases of RabiesRefer clinical cases of Rabies• Basic Curative Care and Treatment of Major Basic Curative Care and Treatment of Major
Chronic Conditions and injuries: Under this Chronic Conditions and injuries: Under this category the major services that are expected are:category the major services that are expected are:– First Aid for common injuries and emergency conditions,First Aid for common injuries and emergency conditions,– Treatment of major chronic condition,Treatment of major chronic condition,– Treatment of mental disorders andTreatment of mental disorders and– Treatment of common infections and complicationsTreatment of common infections and complications
4. Hygiene and Environmental Health Services: 4. Hygiene and Environmental Health Services: activities under this component are mainly related activities under this component are mainly related to giving technical assistance and supportive to giving technical assistance and supportive supervision to HEW on various environmental supervision to HEW on various environmental health service issues including:health service issues including:

• School health education,School health education,
• Prison health service,Prison health service,
• Control of rodents and insects,Control of rodents and insects,
• Provision of water quality control,Provision of water quality control,
• Personal hygiene and others.Personal hygiene and others.
• 5. Health Education and Communication: 5. Health Education and Communication: Similar to the previous component, the major Similar to the previous component, the major activities under this component is to provide activities under this component is to provide technical assistance and supportive technical assistance and supportive supervision to HP in the provision of IEC supervision to HP in the provision of IEC materialsmaterials

4.2.2. District Hospital and Services Provided4.2.2. District Hospital and Services Provided• The district hospital represents the third level within The district hospital represents the third level within
the PHCU, of the health system and has the the PHCU, of the health system and has the capacity of 30-50 beds and provides 24 hour capacity of 30-50 beds and provides 24 hour emergency service for a population of 250,000. It emergency service for a population of 250,000. It serves as a referral center for the five Health serves as a referral center for the five Health Centers under its catchments and will have the Centers under its catchments and will have the capacity of providing treatment of basic acute and capacity of providing treatment of basic acute and chronic medical problems, Comprehensive chronic medical problems, Comprehensive Emergency Obstetric Care (CEOC), basic Emergency Obstetric Care (CEOC), basic emergency surgical interventions, dental and emergency surgical interventions, dental and mental health services. These hospitals will also mental health services. These hospitals will also serve as a training site for clinical officers and mid serve as a training site for clinical officers and mid level health workers.level health workers.
• In addition to the following services, District In addition to the following services, District Hospital provides all of the essential health Hospital provides all of the essential health services that are provided by the Health Center.services that are provided by the Health Center.
• Comprehensive Essential Obstetric CareComprehensive Essential Obstetric Care– Provision of basic emergency obstetric care servicesProvision of basic emergency obstetric care services– Provision of obstetric and gynecologic procedures Provision of obstetric and gynecologic procedures
including (minor and major procedures)including (minor and major procedures)
2) Emergency Surgical Procedures:2) Emergency Surgical Procedures:– Basic life saving proceduresBasic life saving procedures– emergency major procedures and minor procedures)emergency major procedures and minor procedures)
3) Emergency Medicine, like:3) Emergency Medicine, like:• Diabetic ketoacidosis (DKA)Diabetic ketoacidosis (DKA)• Acute poisoningAcute poisoning• Severe and complicated malariaSevere and complicated malaria• Status asthmaticsStatus asthmatics• Seizure disorders and othersSeizure disorders and others

4) Laboratory and pharmacy services4) Laboratory and pharmacy services4.2.3. Zonal/Regional Hospitals and Services 4.2.3. Zonal/Regional Hospitals and Services
ProvidedProvided• Generally these hospitals have the capacity of 150-Generally these hospitals have the capacity of 150-
200 beds and provides 24 hours service. It will have 200 beds and provides 24 hours service. It will have the four major departments:the four major departments:
• Internal MedicineInternal Medicine• General SurgeryGeneral Surgery• Paediatrics andPaediatrics and• Gynaecology and ObstetricsGynaecology and Obstetrics• Additional specialities such as Ophthalmology, Additional specialities such as Ophthalmology,
Radiology, Orthopaedics, Dentistry and Psychiatry.Radiology, Orthopaedics, Dentistry and Psychiatry.• These hospitals serve as a training site for medical These hospitals serve as a training site for medical
doctors and other healthcare workers. The major doctors and other healthcare workers. The major services at this level include:services at this level include:
a. Management of Childhood Illnessesa. Management of Childhood Illnesses• The Hospital provides outpatient and in-patient The Hospital provides outpatient and in-patient
management of infant and child health, in management of infant and child health, in accordance with. National Standard Treatment accordance with. National Standard Treatment Guidelines at Hospital Level. This includes Guidelines at Hospital Level. This includes preventive, curative (assessing, classifying and preventive, curative (assessing, classifying and treating) promotive, and rehabilitative care.treating) promotive, and rehabilitative care.
b. Adult Medical Serviceb. Adult Medical Service• The Hospital provides outpatient and in-patient The Hospital provides outpatient and in-patient
management of adults in all life stages in management of adults in all life stages in accordance with the Standard Treatment Guidelines accordance with the Standard Treatment Guidelines for hospital care. This includes the provision of for hospital care. This includes the provision of preventive, curative, promotive, and rehabilitative preventive, curative, promotive, and rehabilitative care.care.

• As much health care as possible is provided As much health care as possible is provided in ambulatory basis;in ambulatory basis;
• Patients are admitted and kept in hospital Patients are admitted and kept in hospital only when this is absolutely essential, for only when this is absolutely essential, for physical, medical, mental or social reasons.physical, medical, mental or social reasons.
• The hospital provides the second level of The hospital provides the second level of inpatient admissions for hospitalized care.inpatient admissions for hospitalized care.
• Ongoing management of patients referred to Ongoing management of patients referred to or from the health centers and Primary or from the health centers and Primary Hospitals are provided.Hospitals are provided.

• c. Women’s Medical Servicec. Women’s Medical Service• The Hospital provides that part of the The Hospital provides that part of the
comprehensive package of promotive, comprehensive package of promotive, preventive, curative and rehabilitative preventive, curative and rehabilitative reproductive health services for women who reproductive health services for women who requires medical and special resources not found requires medical and special resources not found in health centers or clinics. The hospital provides in health centers or clinics. The hospital provides a 24-hour service for acute gynecological and a 24-hour service for acute gynecological and obstetric problems and deliveries of most high-obstetric problems and deliveries of most high-risk pregnancies. The focus of the outpatient risk pregnancies. The focus of the outpatient clinic is on taking referrals from health centers clinic is on taking referrals from health centers and clinics and referring patients back with and clinics and referring patients back with information and adviceinformation and advice

• d. Trauma and Emergency Surgical Serviced. Trauma and Emergency Surgical Service• The hospital provides:The hospital provides:• A 24 hour emergency, resuscitation service, A 24 hour emergency, resuscitation service,
advanced trauma and cardiac life supportadvanced trauma and cardiac life support• Treatment and observation of medical and surgical Treatment and observation of medical and surgical
and emergenciesand emergencies• Treatment and reporting of accidents, gunshots, Treatment and reporting of accidents, gunshots,
and physical abuseand physical abuse• Referral of patients to specialized hospitals.Referral of patients to specialized hospitals.• Arrangements to deal with disaster situations.Arrangements to deal with disaster situations.• Surgery for minor and serious conditionsSurgery for minor and serious conditions• Common major elective surgeriesCommon major elective surgeries
• e. Pharmaceutical servicee. Pharmaceutical service
• The pharmaceutical service supplies and The pharmaceutical service supplies and dispenses essential drugs and medical dispenses essential drugs and medical supplies. It selects drugs and medical supplies. It selects drugs and medical supplies, purchases these from an identified supplies, purchases these from an identified supplier to maintain adequate quantities, supplier to maintain adequate quantities, receives, records, stores them and ensures receives, records, stores them and ensures appropriate controls are in place. It appropriate controls are in place. It dispenses prescribed drugs, encouraging dispenses prescribed drugs, encouraging rational use by the prescribers as well as rational use by the prescribers as well as patient compliance and appropriate use.patient compliance and appropriate use.
• f. Laboratory Servicef. Laboratory Service• The basic functions include:The basic functions include:• Conducting all the routine tests including quality Conducting all the routine tests including quality
control and some tests that the hospital activity control and some tests that the hospital activity requiresrequires
• Taking specimens and sending themTaking specimens and sending them• Helping in training technician assistants with further Helping in training technician assistants with further
technical supervisiontechnical supervision• Preparing reagents and recording themPreparing reagents and recording them• Keeping equipments in a good statusKeeping equipments in a good status• Preparing a monthly report about the lab activitiesPreparing a monthly report about the lab activities• Taking safety measures in the laboratoryTaking safety measures in the laboratory

• 4.2.4. Referral Hospitals4.2.4. Referral Hospitals
• In addition to the services in the general In addition to the services in the general hospital, specialized hospitals have hospital, specialized hospitals have additional departments likeadditional departments like
• Pathology, Anaesthesiology, ENT, Pathology, Anaesthesiology, ENT, Dermatology and sub-specialities. Such level Dermatology and sub-specialities. Such level of hospitals will also serve as a teaching of hospitals will also serve as a teaching centre for medical doctors and different types centre for medical doctors and different types of specialists. In Ethiopia we have five of specialists. In Ethiopia we have five hospitals to such level (Tikur Anbesa, St hospitals to such level (Tikur Anbesa, St Pawlos, Amanuel, St Petros and ALERT)Pawlos, Amanuel, St Petros and ALERT)

• 4.3.1 Human Resource (healthcare workforce) 4.3.1 Human Resource (healthcare workforce) RequirementRequirement
• The other major component of the healthcare delivery system The other major component of the healthcare delivery system is the healthcare work force. They play a crucial role based is the healthcare work force. They play a crucial role based on the service delivered at the facilities. Number and type of on the service delivered at the facilities. Number and type of personnel required varies depending on the type of facility personnel required varies depending on the type of facility they are posted at. The human resource requirement for they are posted at. The human resource requirement for each level of care is established based on the expected each level of care is established based on the expected services at each level, the workload and service standard by services at each level, the workload and service standard by using the Workload Indicator for Staffing Needs (WISN) using the Workload Indicator for Staffing Needs (WISN) method. The average HRH requirement for each level of care method. The average HRH requirement for each level of care is summarized in the following Table (look at table 4.1). is summarized in the following Table (look at table 4.1). However, as the work load may vary across facilities, each However, as the work load may vary across facilities, each facility need to develop its staffing requirement on case by facility need to develop its staffing requirement on case by case basis.case basis.
• The make-up of the healthcare work force can be categorized The make-up of the healthcare work force can be categorized as:as:

• Medical staffMedical staff• Administrative staffAdministrative staff• Supportive staffSupportive staff• A) Medical StaffA) Medical Staff• Medical staff includes the professional Medical staff includes the professional
occupations such as:occupations such as:• Physicians of all categoriesPhysicians of all categories: – in Ethiopia there is : – in Ethiopia there is
shortage of medical doctors, and also concerns shortage of medical doctors, and also concerns about the distribution of doctors across geographic about the distribution of doctors across geographic areas. There is also misdistribution over rural areas. There is also misdistribution over rural verses urban areas.verses urban areas.
• NursesNurses – constitute the largest healthcare – constitute the largest healthcare profession. The primary paths to becoming a nurse profession. The primary paths to becoming a nurse are by obtaining a BSc or a diploma in nursing. are by obtaining a BSc or a diploma in nursing. Their responsibilities include performing patient Their responsibilities include performing patient assessments, providing nursing care, and assessments, providing nursing care, and administer patient care services.administer patient care services.

• Health Officers – receive their training through a Health Officers – receive their training through a university-based program, and have expanding university-based program, and have expanding responsibilities with the healthcare delivery systemresponsibilities with the healthcare delivery system
• 4.1: Average number and professional types 4.1: Average number and professional types required at different health facility levelsrequired at different health facility levels
• Other professional components of the health Other professional components of the health workforce include dentists, dental hygienists, workforce include dentists, dental hygienists, social workers, pharmacists, therapists, social workers, pharmacists, therapists, nutritionists. The application of medical nutritionists. The application of medical technologies and equipment requires additional technologies and equipment requires additional technicians with specialized skills, such as technicians with specialized skills, such as radiology technicians, laboratory technicians, and radiology technicians, laboratory technicians, and pharmacy technicians.pharmacy technicians.

• B) Administrative StaffB) Administrative Staff• The leader of the administrative staff is the medical director, The leader of the administrative staff is the medical director,
who is going to be replaced by Hospital CEO’s according to who is going to be replaced by Hospital CEO’s according to the new human resource development strategy. The CEO is the new human resource development strategy. The CEO is responsible for coordinating the health services provided at responsible for coordinating the health services provided at that facility. While department staff nurses are accountable that facility. While department staff nurses are accountable to the head nurse, the head nurses are accountable to the to the head nurse, the head nurses are accountable to the matron. The matron is in turn accountable to the medical matron. The matron is in turn accountable to the medical director of the hospital.director of the hospital.
• C) Support StaffC) Support Staff• Support staff provides support services to patients, medical Support staff provides support services to patients, medical
staff, and employees.staff, and employees.• Clinical support staffClinical support staff• Food and nutrition servicesFood and nutrition services• Health record servicesHealth record services• Social servicesSocial services• Central supply servicesCentral supply services
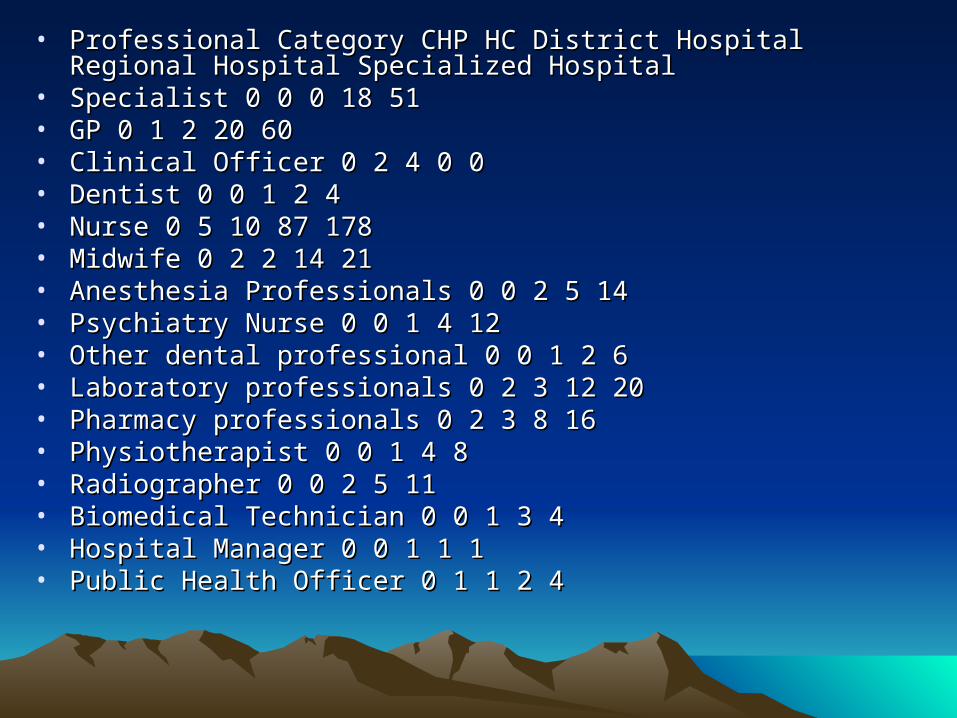
• Professional Category CHP HC District Hospital Regional Hospital Professional Category CHP HC District Hospital Regional Hospital Specialized HospitalSpecialized Hospital
• Specialist 0 0 0 18 51Specialist 0 0 0 18 51• GP 0 1 2 20 60GP 0 1 2 20 60• Clinical Officer 0 2 4 0 0Clinical Officer 0 2 4 0 0• Dentist 0 0 1 2 4Dentist 0 0 1 2 4• Nurse 0 5 10 87 178Nurse 0 5 10 87 178• Midwife 0 2 2 14 21Midwife 0 2 2 14 21• Anesthesia Professionals 0 0 2 5 14Anesthesia Professionals 0 0 2 5 14• Psychiatry Nurse 0 0 1 4 12Psychiatry Nurse 0 0 1 4 12• Other dental professional 0 0 1 2 6Other dental professional 0 0 1 2 6• Laboratory professionals 0 2 3 12 20Laboratory professionals 0 2 3 12 20• Pharmacy professionals 0 2 3 8 16Pharmacy professionals 0 2 3 8 16• Physiotherapist 0 0 1 4 8Physiotherapist 0 0 1 4 8• Radiographer 0 0 2 5 11Radiographer 0 0 2 5 11• Biomedical Technician 0 0 1 3 4Biomedical Technician 0 0 1 3 4• Hospital Manager 0 0 1 1 1Hospital Manager 0 0 1 1 1• Public Health Officer 0 1 1 2 4Public Health Officer 0 1 1 2 4

• HIT 0 1 2 4 8HIT 0 1 2 4 8• Dietician 0 0 0 2 4Dietician 0 0 0 2 4• Social Worker 0 0 0 2 4Social Worker 0 0 0 2 4• Health Extension Worker 2 0 0 0 0Health Extension Worker 2 0 0 0 0• 2 16 33 195 4262 16 33 195 426• Administrative support servicesAdministrative support services• Registration clerksRegistration clerks• accountingaccounting• SecretariesSecretaries• Security personnelSecurity personnel• CleanerCleaner

• UNIT V: HEALTH SERVICE PROGRAMSUNIT V: HEALTH SERVICE PROGRAMS• IntroductionIntroduction• The first Health Sector Development Program (HSDP) was launched in The first Health Sector Development Program (HSDP) was launched in
1977 and currently we are on the third HSDP. In this unit we will deal 1977 and currently we are on the third HSDP. In this unit we will deal with health service programs of Ethiopia. A key aspect of health service with health service programs of Ethiopia. A key aspect of health service program is the Essential Health Service Package (EHSP), which program is the Essential Health Service Package (EHSP), which specifies the basic services that should be available at a certain level of specifies the basic services that should be available at a certain level of the health system.the health system.
• Unit OutlineUnit Outline• 1. Health policy, plans and strategies1. Health policy, plans and strategies• 2. Essential health service package2. Essential health service package• 1. The Health Service Extension Program (HSEP)1. The Health Service Extension Program (HSEP)• 2. Family health service2. Family health service• 3. Prevention and control of disease3. Prevention and control of disease• 4. Medical Services4. Medical Services• 5. Hygiene and environmental health5. Hygiene and environmental health• 3. Human resource development3. Human resource development• 4. Pharmaceutical service4. Pharmaceutical service• 5. IEC and HMIS5. IEC and HMIS• 6. Monitoring and evaluation and health care financing6. Monitoring and evaluation and health care financing

• 5.1: The Health Policy, Plans and Strategies5.1: The Health Policy, Plans and Strategies• Lesson objectivesLesson objectives• At the end of the lesson the learners should be able At the end of the lesson the learners should be able
to:to:• 1. State major goals of HSDP1. State major goals of HSDP• 2. Explain the current Ethiopian health policy2. Explain the current Ethiopian health policy• 5.1.1. Introduction5.1.1. Introduction• As a means of achieving the goals of the health As a means of achieving the goals of the health
policy (refer Ethiopian health policy), the policy (refer Ethiopian health policy), the government has formulated a twenty-year health government has formulated a twenty-year health sector development strategy, which is being sector development strategy, which is being implemented through a series of five-year plans. The implemented through a series of five-year plans. The implementation of the first Health Sector implementation of the first Health Sector Development Program (HSDP) was launched inDevelopment Program (HSDP) was launched in
• 1997, and now the third HSDP is under way. (Please 1997, and now the third HSDP is under way. (Please refer to the HSDP III manual.)refer to the HSDP III manual.)
• 5.1.2. The HSDP-III5.1.2. The HSDP-III
• The ultimate goal of HSDP-III is to improve The ultimate goal of HSDP-III is to improve the health status of the Ethiopian people the health status of the Ethiopian people through provision of adequate and optimum through provision of adequate and optimum quality of promotive, preventive, basic quality of promotive, preventive, basic curative and rehabilitative health services to curative and rehabilitative health services to all segments of the population. Contributing all segments of the population. Contributing to this overall goals, there are 3 sub-goals. to this overall goals, there are 3 sub-goals. These are:These are:
– To improve maternal healthTo improve maternal health– To reduce child mortalityTo reduce child mortality
• To combat HIV/AIDS, malaria, TB and other To combat HIV/AIDS, malaria, TB and other diseasesdiseases

• 5.1: Summary of HSDP III focus areas and outcomes5.1: Summary of HSDP III focus areas and outcomes• Focus areas Outcome Vehicles BloodlinesFocus areas Outcome Vehicles Bloodlines• Maternal healthMaternal health• MMR 871 to 600MMR 871 to 600• CPR> 60%CPR> 60%• 30,000 HEWs30,000 HEWs• Health Officers: 5,000Health Officers: 5,000• Health Posts: 13,635Health Posts: 13,635• Health Center: 3,200Health Center: 3,200• Train GP’sTrain GP’s• Improve QAImprove QA• • • HMISHMIS• • • LogisticsLogistics• • • Human resourceHuman resource• • • Finance harmonizationFinance harmonization

• Child HealthChild Health– U5MR 123/1000 to 85/1000U5MR 123/1000 to 85/1000– IMR 77/1000 to 45/1000IMR 77/1000 to 45/1000– Immunization >85%Immunization >85%
• HIV/TBHIV/TB * Maintain prevalence of HIV at 3.5% * Maintain prevalence of HIV at 3.5%• MalariaMalaria * 20 million ITNs * 20 million ITNs• The above table describes nation-wide priorities. The above table describes nation-wide priorities.
“Priorities” means activities that have been selected “Priorities” means activities that have been selected as the most important and urgent for improving the as the most important and urgent for improving the health of Ethiopians. When resources are in short health of Ethiopians. When resources are in short supplysupply – money, staff, managers’ time, drugs, etc. – money, staff, managers’ time, drugs, etc. – then they will be allocated first to the priority – then they will be allocated first to the priority activities.activities.

• In other words the 5 targets related to family In other words the 5 targets related to family planning, immunization, HIV/TB, and the distribution planning, immunization, HIV/TB, and the distribution of nets to be used in malaria prevention are the of nets to be used in malaria prevention are the most important priorities in the Ethiopian healthcare most important priorities in the Ethiopian healthcare delivery system.delivery system.
• These broad sub-goals are then described in more These broad sub-goals are then described in more detail through 8 major objectives:detail through 8 major objectives:
– To cover all rural kebeles with HEP to achieve universal primary To cover all rural kebeles with HEP to achieve universal primary health care coverage by 2008health care coverage by 2008
– To reduce the MM ratio to 600 per 100,000 live births from 871To reduce the MM ratio to 600 per 100,000 live births from 871– To reduce the under 5 mortality rate from 123 to 85 per 1,000 live To reduce the under 5 mortality rate from 123 to 85 per 1,000 live
births and the infant mortality rate from 77 to 45 per 1,000 populationbirths and the infant mortality rate from 77 to 45 per 1,000 population– To reduce the total fertility rate from 5.9 to 4To reduce the total fertility rate from 5.9 to 4– To reduce the adult incidence of HIV from 0.68 to 0.65 and maintain To reduce the adult incidence of HIV from 0.68 to 0.65 and maintain
the pre-valence of HIV at 3.5%the pre-valence of HIV at 3.5%– To reduce morbidity attributed to malaria from 22% to 10%To reduce morbidity attributed to malaria from 22% to 10%– To reduce the case fatality rate of malaria in age groups 5 years and To reduce the case fatality rate of malaria in age groups 5 years and
above from 4.5% to 2% and the case fatality rate in under 5 children above from 4.5% to 2% and the case fatality rate in under 5 children from 5% to 2%from 5% to 2%
– To reduce mortality attributed to TB from 7% to 4% of all treated To reduce mortality attributed to TB from 7% to 4% of all treated casescases

• These objectives are then re-structured as 8 These objectives are then re-structured as 8 implementation components, to reflect the implementation components, to reflect the way in which healthservices are delivered way in which healthservices are delivered and financed:and financed:
• Health service delivery and quality of careHealth service delivery and quality of care• Access to services: health facility construction, Access to services: health facility construction,
expansion and transportexpansion and transport• Human resource developmentHuman resource development• Pharmaceutical servicePharmaceutical service• Information, education and communication (IE&C)Information, education and communication (IE&C)• Health management information systemHealth management information system• Monitoring and EvaluationMonitoring and Evaluation• Health care financing.Health care financing.

• In effect, components 1 describe the main In effect, components 1 describe the main health service delivery activities and health service delivery activities and components 2 -7 are the inputs and activities components 2 -7 are the inputs and activities required to provide these services.required to provide these services.
• In addition to the HSDP, Ethiopia is in the In addition to the HSDP, Ethiopia is in the process of implementing the Millennium process of implementing the Millennium Development GoalsDevelopment Goals
• (MDGs). The MDGs came out of the UN (MDGs). The MDGs came out of the UN Millennium Declaration, assuring the right of Millennium Declaration, assuring the right of each person on the planet to health, each person on the planet to health, education, shelter and security. The important education, shelter and security. The important role health plays in achieving the MDGs is role health plays in achieving the MDGs is clearly reflected.clearly reflected.
• The 8 MDG Goals are:The 8 MDG Goals are:• Eliminate Poverty and hungerEliminate Poverty and hunger• Ensure primary education for allEnsure primary education for all• Promote gender equality andPromote gender equality and• Reduce juvenile mortalityReduce juvenile mortality• Better maternal careBetter maternal care• Combat HIV/AIDs, Malaria and other diseasesCombat HIV/AIDs, Malaria and other diseases• Ensure a sustainable environmentEnsure a sustainable environment• Build a global partnership for developmentBuild a global partnership for development
• Of the above MDGs, goal 4, 5, and 6 are Of the above MDGs, goal 4, 5, and 6 are addressed by the health sector.addressed by the health sector.

• 5.2: Essential Health Service Package5.2: Essential Health Service Package• Lesson Objectives:Lesson Objectives:• At the end of this lesson the learners should be able to:At the end of this lesson the learners should be able to:
• Describe the five components of Essential Health Service Package Describe the five components of Essential Health Service Package (EHSP)(EHSP)
• Identify the components of packages that will be carried out by the Identify the components of packages that will be carried out by the Health extension workersHealth extension workers
• State the goal of Family health servicesState the goal of Family health services• Mention the goal of medical serviceMention the goal of medical service• Identify diseases which are of top priorityIdentify diseases which are of top priority• State the priority activities/interventions area in HIV/AIDS and malaria State the priority activities/interventions area in HIV/AIDS and malaria
Prevention and Control ProgrammePrevention and Control Programme• Explain the need for TB and Leprosy Control Programme (TLCP)Explain the need for TB and Leprosy Control Programme (TLCP)• Identify the role of each facility level in TB leprosy Control programIdentify the role of each facility level in TB leprosy Control program• Identify the objectives of hygiene and environmental subcomponentsIdentify the objectives of hygiene and environmental subcomponents• List the diseases given due emphasis in HSDP II programList the diseases given due emphasis in HSDP II program• State minimum standard expected in health care delivery at different State minimum standard expected in health care delivery at different
levelslevels• Describe the importance of having base line information on key Describe the importance of having base line information on key
indicators like TFR, MMR, U5MR?indicators like TFR, MMR, U5MR?
• 5.2.1. Introduction5.2.1. Introduction• The best way of understanding the healthcare The best way of understanding the healthcare
delivery system is to break down the “Essential delivery system is to break down the “Essential health Service Package” provided at hospitals, health Service Package” provided at hospitals, health centers and health posts.health centers and health posts.
• A key aspect of this component is the A key aspect of this component is the Essential Health Service Package (EHSP), which Essential Health Service Package (EHSP), which specifies the basic services that should be available specifies the basic services that should be available at a certain level of the health system. EHSP at a certain level of the health system. EHSP consists of an essential package for the community consists of an essential package for the community level, plus basic curative care and the treatment of level, plus basic curative care and the treatment of major chronic conditions to be provided at health major chronic conditions to be provided at health centers. The EHSP has five components:centers. The EHSP has five components:
• The Health Service Extension Program (HSEP)The Health Service Extension Program (HSEP)• Family health serviceFamily health service• Prevention and control of diseasePrevention and control of disease• Medical ServicesMedical Services• Hygiene and environmental healthHygiene and environmental health

• 5.2.2. The Health Service Extension Program 5.2.2. The Health Service Extension Program (HSEP)(HSEP)
• The HSEP is a community based healthcare The HSEP is a community based healthcare delivery system which focuses on preventive health delivery system which focuses on preventive health service. This basic healthcare coverage is service. This basic healthcare coverage is implemented at the health post level. Each health implemented at the health post level. Each health post has a catchment of 5000 people, and is staffed post has a catchment of 5000 people, and is staffed by 2 HEWs. The HSEP has 16 major packages by 2 HEWs. The HSEP has 16 major packages which fall into the 4 major components:which fall into the 4 major components:
• Hygiene and environmental sanitationHygiene and environmental sanitation• Family health servicesFamily health services• Disease prevention and controlDisease prevention and control• Health education and communicationHealth education and communication

• 5.2.3. Family Health Services (Maternal and 5.2.3. Family Health Services (Maternal and Child Health Care)Child Health Care)
• The goal is to reduce deaths and illnesses The goal is to reduce deaths and illnesses associated with pregnancy, childbirth, and early associated with pregnancy, childbirth, and early childhood diseases.childhood diseases.
• This is done by educating mothers and community This is done by educating mothers and community midwives on birth spacing, contraception, antenatal midwives on birth spacing, contraception, antenatal care, delivery practices, child health and nutrition.care, delivery practices, child health and nutrition.
• Health workers also diagnose and provide basic Health workers also diagnose and provide basic clinical treatment for common childhood illnesses clinical treatment for common childhood illnesses including respiratory infections, measles, malaria, including respiratory infections, measles, malaria, pneumonia, and diarrhea. Childhood vaccines, pneumonia, and diarrhea. Childhood vaccines, vitamin A, oral rehydration treatment, tetanus vitamin A, oral rehydration treatment, tetanus vaccines to pregnant women, and anti-malarial vaccines to pregnant women, and anti-malarial drugs are provided.drugs are provided.

• A) Maternal HealthA) Maternal Health• Nearly half (49.7%) of Ethiopia’s population is Nearly half (49.7%) of Ethiopia’s population is
female, of which 47% are in the range 15-49 female, of which 47% are in the range 15-49 years of age. Total Fertility Rate (TFR) is years of age. Total Fertility Rate (TFR) is estimated at 5.9. According to data from estimated at 5.9. According to data from health facilities across the country, pregnancy health facilities across the country, pregnancy related problems account for 13.8% of in-related problems account for 13.8% of in-patient mortality among women of child patient mortality among women of child bearing age. The Maternal mortality Rate bearing age. The Maternal mortality Rate (MMR), estimated at 871 per 100,000 live (MMR), estimated at 871 per 100,000 live births, is one of the highest in the world. The births, is one of the highest in the world. The major causes of maternal mortality include major causes of maternal mortality include delivery, other pregnancy related delivery, other pregnancy related complications and abortion.complications and abortion.

• B) Child HealthB) Child Health
• Like in many developing countries, children Like in many developing countries, children less than 15 years of age constitute 44.7%; of less than 15 years of age constitute 44.7%; of this around 40% are under five years of age, this around 40% are under five years of age, and 8% are under one years of age.and 8% are under one years of age.
• In year 2000, the under-five mortality rate In year 2000, the under-five mortality rate (U5MR) was estimated at 166, while infant (U5MR) was estimated at 166, while infant mortality and neonatal mortality rates were mortality and neonatal mortality rates were estimated at 97 and 49 per 1000 live births estimated at 97 and 49 per 1000 live births respectively. Assuming a steady annual respectively. Assuming a steady annual decrease, the U5 MR is currently estimated decrease, the U5 MR is currently estimated at 146.6.at 146.6.
• The major causes of under-five mortality have been The major causes of under-five mortality have been pneumonia (28.9%), malaria (21.6%) and diarrhea pneumonia (28.9%), malaria (21.6%) and diarrhea (6.7%), all types of pneumonia and malaria are the (6.7%), all types of pneumonia and malaria are the major causes of death among infants, with each major causes of death among infants, with each accounting for 39.7% and 21.1% of deaths accounting for 39.7% and 21.1% of deaths respectively. High maternal fertility, especially early respectively. High maternal fertility, especially early first pregnancy and short birth intervals, have also first pregnancy and short birth intervals, have also been strongly associated with increased under-five been strongly associated with increased under-five mortality.mortality.
• Malnutrition has been a major underlying cause of Malnutrition has been a major underlying cause of an estimated 57% of deaths, while HIV/AIDS an estimated 57% of deaths, while HIV/AIDS underlies 11% of deaths, particularly those due to underlies 11% of deaths, particularly those due to pneumonia, according to FMOH documents. Half of pneumonia, according to FMOH documents. Half of Ethiopia’s children under-five are stunted (52%), Ethiopia’s children under-five are stunted (52%), while 11% are estimated to be wasted.while 11% are estimated to be wasted.

• The government has adopted an Integrated Management of The government has adopted an Integrated Management of Childhood Illnesses (IMCI) as its key strategy towards Childhood Illnesses (IMCI) as its key strategy towards reducing under-five mortality and morbidity, and promoting reducing under-five mortality and morbidity, and promoting healthy growth and development of children. The strategy healthy growth and development of children. The strategy focuses on key child survival interventions, proven to be focuses on key child survival interventions, proven to be effective in reducing childhood mortality. These effective in reducing childhood mortality. These interventions include:interventions include:
• Improved birth interval,Improved birth interval,• improved antenatal care coverage both for TT2 and improved antenatal care coverage both for TT2 and
measlesmeasles• improved coverage of skilled deliveryimproved coverage of skilled delivery• prevention of mother to child transmission of HIV/ AIDSprevention of mother to child transmission of HIV/ AIDS• promotion of exclusive breast feeding in the first 6 months, promotion of exclusive breast feeding in the first 6 months,
complementary feeding after 6 months and continued complementary feeding after 6 months and continued breast feedingbreast feeding
• treatment of fever, ARI and diarrheatreatment of fever, ARI and diarrhea• vitamin A supplementationvitamin A supplementation• delivery of safe drinking water and sanitationdelivery of safe drinking water and sanitation• provision of insecticide treated nets (ITNs)provision of insecticide treated nets (ITNs)

• IndicatorIndicator• HSDP-I HSDP-IIHSDP-I HSDP-II• Baseline Target Achievement Target AchievementBaseline Target Achievement Target Achievement• DPT3 59.3 70-80% 51.5 70 70.1DPT3 59.3 70-80% 51.5 70 70.1• CPR 9.8% 15-20% 18.7 24%, 25.2CPR 9.8% 15-20% 18.7 24%, 25.2• ANC 5% - 30 45 41.5ANC 5% - 30 45 41.5• Assisted delivery 3.5% - 7% 25 12.4Assisted delivery 3.5% - 7% 25 12.4• TT2 for pregnant - - 27 70% 43.3TT2 for pregnant - - 27 70% 43.3• TT2 for nonpregnantTT2 for nonpregnant• - - 14.8 32 25.8- - 14.8 32 25.8• PNC coverage 3.5 - 6.8 20 13.6PNC coverage 3.5 - 6.8 20 13.6• C) Steps takenC) Steps taken

A National Reproductive Health Taskforce with A National Reproductive Health Taskforce with technical working group for Making technical working group for Making Pregnancy Safer (MPS), family planning, Pregnancy Safer (MPS), family planning, nutrition, STIs/HIV, logistics and adolescent nutrition, STIs/HIV, logistics and adolescent RH have been formed to assist the RH have been formed to assist the programme with resource mobilization, programme with resource mobilization, monitoring and development of appropriate monitoring and development of appropriate policies and guidelines.policies and guidelines.

Making Pregnancy Safer was launched in 2001 and Making Pregnancy Safer was launched in 2001 and implemented in four regions on pilot basis. Health implemented in four regions on pilot basis. Health workers were also trained on basic emergency workers were also trained on basic emergency maternal and newborn lifesaving obstetric services, maternal and newborn lifesaving obstetric services, EOC, cesarean section and anesthesia. 10 hospitals EOC, cesarean section and anesthesia. 10 hospitals and over 40 HCs were equipped with basic essential and over 40 HCs were equipped with basic essential equipment and supplies, and vehicles were procured equipment and supplies, and vehicles were procured and distributed to enhance programme and distributed to enhance programme implementation and the referral system. The review implementation and the referral system. The review of the programme conducted in year 2003 revealed of the programme conducted in year 2003 revealed improvement in the quality of service and handling of improvement in the quality of service and handling of obstetric emergencies that stimulated the rapid obstetric emergencies that stimulated the rapid scaling up of the programme coverage.scaling up of the programme coverage.
• 5.2: Summary of Targets and 5.2: Summary of Targets and Achievements during HSDP-I and II in Achievements during HSDP-I and II in Maternal and ChildMaternal and Child
• Health ServicesHealth Services– With regard to child health, IMCI was adopted nationally in With regard to child health, IMCI was adopted nationally in
1997 as a major strategy to reduce childhood mortality and 1997 as a major strategy to reduce childhood mortality and morbidity and promote childhood development. It has three morbidity and promote childhood development. It has three components :components :
– improving the skills of health workers,improving the skills of health workers,– improving health systems,improving health systems,– Improving family and community practices.Improving family and community practices.
• The main activities under IMCI are The main activities under IMCI are prevention and control of ARI, diarrhea, prevention and control of ARI, diarrhea, malaria, malnutrition, measles and malaria, malnutrition, measles and HIV/AIDS.HIV/AIDS.

– Interagency Coordination Committee (ICC) has been Interagency Coordination Committee (ICC) has been established and meets regularly to address issues on established and meets regularly to address issues on improving routine EPI, supplementary immunization activities improving routine EPI, supplementary immunization activities and disease surveillance. This committee also plays a key and disease surveillance. This committee also plays a key role in resource mobilization for EPI.role in resource mobilization for EPI.
– In addition to the scheduled vaccination programs, In addition to the scheduled vaccination programs, supplemental immunization of polio, measles and neonatal supplemental immunization of polio, measles and neonatal tetanus was introduced in order to reach the remote areas of tetanus was introduced in order to reach the remote areas of the country, strengthen the routine immunization activity and the country, strengthen the routine immunization activity and eradicate/eliminate the 3 vaccine preventable diseases.eradicate/eliminate the 3 vaccine preventable diseases.

– Training was given to mid-level managers and cold chain Training was given to mid-level managers and cold chain technicians using Midlevel Managers and Immunization in technicians using Midlevel Managers and Immunization in Practice Modules. The programme has also replaced the Practice Modules. The programme has also replaced the reusable syringe by AD syringe and all injection vaccines reusable syringe by AD syringe and all injection vaccines were given using the disposable syringes and safety boxes.were given using the disposable syringes and safety boxes.
– Introduction of the Reaching Every District (RED) strategy, Introduction of the Reaching Every District (RED) strategy, where most woredas have been developing micro-plans.where most woredas have been developing micro-plans.

• Major constraints encountered during the Major constraints encountered during the implementation of MCH programmes were:implementation of MCH programmes were:– understaffing and high turnover of both technical understaffing and high turnover of both technical
and managerial staff at all levelsand managerial staff at all levels– inadequate follow-up and supportive supervisioninadequate follow-up and supportive supervision– shortage of transportationshortage of transportation– lack of motivation of service providerslack of motivation of service providers– poorly functioning of outreach sites and weak poorly functioning of outreach sites and weak
referral systemreferral system– high vaccine wastage rates,high vaccine wastage rates,– critical shortage of basic equipment for the critical shortage of basic equipment for the
management of emergency obstetrics at facility management of emergency obstetrics at facility levellevel
– Short supply of contraceptives and vaccines.Short supply of contraceptives and vaccines.

• The following are the future directions towards the The following are the future directions towards the improvement of MCH service.improvement of MCH service.
• Operationalize the harmonization of maternal and child health Operationalize the harmonization of maternal and child health programs with the Health Extension Programme.programs with the Health Extension Programme.
• Accelerate capacity building at the Regional and District level Accelerate capacity building at the Regional and District level for planning, training, follow up and support supervision.for planning, training, follow up and support supervision.
• Building the capacity of training institutions to scale-up IMCI Building the capacity of training institutions to scale-up IMCI pre-service training through training of instructors and pre-service training through training of instructors and provision of financial and material support.provision of financial and material support.
• Involve NGOs and the private sector to scale up maternal Involve NGOs and the private sector to scale up maternal and child health interventions.and child health interventions.
• Strengthen the collaboration and integration among relevant Strengthen the collaboration and integration among relevant programs like RBM, EPI, Nutrition, MPS, IMCI and HIV/AIDS programs like RBM, EPI, Nutrition, MPS, IMCI and HIV/AIDS etc., to avoid duplication of efforts and maximize the impact.etc., to avoid duplication of efforts and maximize the impact.
• Optimally utilize the opportunity of the child survival initiative Optimally utilize the opportunity of the child survival initiative to scale up maternal and child health interventions.to scale up maternal and child health interventions.
• Introduce new vaccines against Hepatitis B and Haemophilus Introduce new vaccines against Hepatitis B and Haemophilus Influenzae.Influenzae.

• 5.2.4. Prevention and Control of Disease5.2.4. Prevention and Control of Disease• The health service program gives priority to the The health service program gives priority to the
prevention and control of HIV/AIDS, malaria, prevention and control of HIV/AIDS, malaria, tuberculosis, leprosy, blindness and onchocerciasis.tuberculosis, leprosy, blindness and onchocerciasis.
• A) HIV/AIDS Prevention and Control ProgrammeA) HIV/AIDS Prevention and Control Programme• It is now more than two decades since the It is now more than two decades since the
HIV/AIDS epidemic started in Ethiopia. HIV/AIDS HIV/AIDS epidemic started in Ethiopia. HIV/AIDS was recognized as top priority from the very was recognized as top priority from the very beginning of HSDP. There is a National HIV/AIDS beginning of HSDP. There is a National HIV/AIDS Policy supporting disease prevention and case Policy supporting disease prevention and case management (including home-base care), management (including home-base care), strengthen IEC/BCC, mobilization of resources and strengthen IEC/BCC, mobilization of resources and coordinating multisectoral effort to ensure proper coordinating multisectoral effort to ensure proper containment of the spread of the disease and containment of the spread of the disease and reduce its adverse socio-economic consequences.reduce its adverse socio-economic consequences.

• The priority intervention areas are:The priority intervention areas are:• IEC/BCC,IEC/BCC,• Condom promotion and distribution,Condom promotion and distribution,• Voluntary counseling and testing (VCT),Voluntary counseling and testing (VCT),• Management of sexually transmitted infections Management of sexually transmitted infections
(STIs),(STIs),• Blood safety,Blood safety,• Infection prevention/universal precaution,Infection prevention/universal precaution,• Prevention of mother to child transmission of HIV Prevention of mother to child transmission of HIV
(PMTCT),(PMTCT),• Management of opportunistic infections,Management of opportunistic infections,• Care and support to the infected and affected,Care and support to the infected and affected,• Legislation and human rights and surveillance and Legislation and human rights and surveillance and
researchresearch

• In order to facilitate the implementation of these In order to facilitate the implementation of these interventions, a number of guidelines, manuals and interventions, a number of guidelines, manuals and other relevant documents have been prepared on other relevant documents have been prepared on counseling, case management, home-based care counseling, case management, home-based care and other areas.and other areas.
• The policy on supply and use of anti retroviral drugs The policy on supply and use of anti retroviral drugs has been implemented within the framework of the has been implemented within the framework of the existing HIV/AIDS Prevention and Control Policy and existing HIV/AIDS Prevention and Control Policy and Strategy. In addition, intensive and continuous Strategy. In addition, intensive and continuous advocacy has been conducted leading to the advocacy has been conducted leading to the involvement of more and more NGOs, UN and involvement of more and more NGOs, UN and Bilateral Organizations, CBOs and the community at Bilateral Organizations, CBOs and the community at large in the prevention and control of HIV/AIDS.large in the prevention and control of HIV/AIDS.

Six strategic issues have been identified in the HIV/AIDS Six strategic issues have been identified in the HIV/AIDS prevention and control strategic plan, these are:prevention and control strategic plan, these are:
• Capacity buildingCapacity building• Community mobilization and involvementCommunity mobilization and involvement• Integration with health programmesIntegration with health programmes• Leadership and mainstreamingLeadership and mainstreaming• Coordination and networkingCoordination and networking• targeted responsetargeted responseChallenges faced in the implementation of the program Challenges faced in the implementation of the program
are:are:• Weak coordination and communication at all levelsWeak coordination and communication at all levels• Inadequate implementation of blood safety proceduresInadequate implementation of blood safety procedures• Scarcity and insufficient implementation of guidelines related Scarcity and insufficient implementation of guidelines related
to HIV/AIDSto HIV/AIDS• Shortage of supplies required to provide care and supportShortage of supplies required to provide care and support

B) Malaria and Other Vector-borne Diseases Prevention B) Malaria and Other Vector-borne Diseases Prevention and Controland Control
• Malaria is the leading cause of morbidity and mortality in the Malaria is the leading cause of morbidity and mortality in the country. Three quarters of the landmass of the country is country. Three quarters of the landmass of the country is malarious and around two-thirds of the population is at risk of malarious and around two-thirds of the population is at risk of infection. Considerable attention has been given to malaria infection. Considerable attention has been given to malaria in order to reduce the overall burden of the disease. The in order to reduce the overall burden of the disease. The prevention and control of malaria is achieved by:prevention and control of malaria is achieved by:
• Distribution of effective drugs to all health facilities, including Distribution of effective drugs to all health facilities, including health postshealth posts
• Distribution of insecticide treated bed netsDistribution of insecticide treated bed nets• Provide health education to communities to maximize use of Provide health education to communities to maximize use of
bed netsbed nets• Spraying of DDT as per planSpraying of DDT as per plan• Training of health professionals in malaria control and Training of health professionals in malaria control and
preventionprevention

• C) Tuberculosis and Leprosy Control C) Tuberculosis and Leprosy Control Programme (TLCP)Programme (TLCP)
• The general objective of the TLCP is to The general objective of the TLCP is to reduce the incidence and prevalence of TB reduce the incidence and prevalence of TB and Leprosy as well as the occurrence of and Leprosy as well as the occurrence of disability and psychological suffering related disability and psychological suffering related to both diseases and the mortality resulting to both diseases and the mortality resulting from TB to such an extent that both diseases from TB to such an extent that both diseases are no longer public health problems. The are no longer public health problems. The general objective has been specified for the general objective has been specified for the various TLCP activities as follows:various TLCP activities as follows:

• Case detection: to diagnose TB and Leprosy Case detection: to diagnose TB and Leprosy patients at an early stage of the disease to the patients at an early stage of the disease to the extent that the case detection rate of new smear extent that the case detection rate of new smear positive pulmonary TB patients is at least 70% of positive pulmonary TB patients is at least 70% of the estimated incidence and the proportion of the estimated incidence and the proportion of disability grade II among new leprosy patients is disability grade II among new leprosy patients is less than 10%.less than 10%.
• Treatment: to achieve and maintain success rate of Treatment: to achieve and maintain success rate of at least 85% of newly detected smear positive at least 85% of newly detected smear positive pulmonary TB patients (PTB+) and extra pulmonary pulmonary TB patients (PTB+) and extra pulmonary TB patients treated with DOTS. For Leprosy, TB patients treated with DOTS. For Leprosy, treatment should achieve a treatment completion treatment should achieve a treatment completion rate of at least 85% and prevention of Leprosy rate of at least 85% and prevention of Leprosy related disability during chemotherapy should be related disability during chemotherapy should be below 3%.below 3%.

DOTs/MDT is expanded to all regions. For instance, DOTs/MDT is expanded to all regions. For instance, 86% of woredas in the country and 50% of the 86% of woredas in the country and 50% of the government health facilities are implementing government health facilities are implementing DOTS/MDT (32% in 2000). The treatment success DOTS/MDT (32% in 2000). The treatment success rate, which is the main indicator of programme rate, which is the main indicator of programme effectiveness, has reached 76%. The treatment effectiveness, has reached 76%. The treatment defaulter rate has also decreased from10% in defaulter rate has also decreased from10% in 1998/99 to 7% in 2000/01 and then to 5% in 1998/99 to 7% in 2000/01 and then to 5% in 2003/04 for patients on short-term chemotherapy. 2003/04 for patients on short-term chemotherapy. Additionally, encouraging results were seen in the Additionally, encouraging results were seen in the areas of integration of DOTs/MDT into the routine areas of integration of DOTs/MDT into the routine health service delivery. Standardized national health service delivery. Standardized national treatment manual and basic microscopy services treatment manual and basic microscopy services are also put in place.are also put in place.

• Challenges with regard to implementation of TLCP are:Challenges with regard to implementation of TLCP are:• Shortage and high turnover of staffShortage and high turnover of staff• Inadequacy of on-the-job training and supervisionInadequacy of on-the-job training and supervision• Inadequate involvement of communities in the Inadequate involvement of communities in the
implementation of DOTSimplementation of DOTS• Poor communication between the public and private TB care Poor communication between the public and private TB care
providers.providers.• In order to alleviate these problems, there is a need to In order to alleviate these problems, there is a need to
strengthen the programme implementation capacity at all strengthen the programme implementation capacity at all levels of the health system including capacity for the levels of the health system including capacity for the efficient use of financial resources. There should be proper efficient use of financial resources. There should be proper planning for staff allocation and regular training. Involvement planning for staff allocation and regular training. Involvement of the Health Posts in TLCP implementation and of the Health Posts in TLCP implementation and improvement of community mobilization with the improvement of community mobilization with the implementation of the HSEP is expected to enhance the implementation of the HSEP is expected to enhance the effectiveness TLCP.effectiveness TLCP.

• 5.2.5. Medical Services5.2.5. Medical Services• Medical Services is one of the components in Medical Services is one of the components in
essential health service packageessential health service package• The goal of Medical Services is to:The goal of Medical Services is to:• improve quality of health service and utilization by improve quality of health service and utilization by
the population through reorganizing the health the population through reorganizing the health service delivery system into 4-tier systemservice delivery system into 4-tier system
• strengthen the decentralized management to strengthen the decentralized management to ensure full community participationensure full community participation
• develop and implement essential health service develop and implement essential health service package and referral systempackage and referral system
• Develop health facility standards and staff and Develop health facility standards and staff and equip the health facilities accordingly.equip the health facilities accordingly.

In line with this, there has been significant In line with this, there has been significant transformation of the old six-tier health delivery transformation of the old six-tier health delivery system into the new four-tier system spearheaded system into the new four-tier system spearheaded by the establishment of PHCUs (which is being by the establishment of PHCUs (which is being revised and a proposal to use a 3 tier system is revised and a proposal to use a 3 tier system is underway). A complete set of national standards for underway). A complete set of national standards for health posts, health centers and district hospitals health posts, health centers and district hospitals have been prepared, endorsed, published and have been prepared, endorsed, published and distributed to regions. These standards contain distributed to regions. These standards contain specifications for the building design, lists of specifications for the building design, lists of equipment and furniture, the scope of service, equipment and furniture, the scope of service, detailed information on the cadres of staff required, detailed information on the cadres of staff required, and drug lists for each level. Essential health and drug lists for each level. Essential health service package document has been finalized and service package document has been finalized and referral system guideline has been drafted.referral system guideline has been drafted.

• The Civil Service Reform Program (CSRP), which is The Civil Service Reform Program (CSRP), which is being introduced into all public health institutions, is being introduced into all public health institutions, is also showing improvements in the quality of health also showing improvements in the quality of health care. For instance, introduction of the CSRP and care. For instance, introduction of the CSRP and implementation of the Business Process implementation of the Business Process Reengineering in St. Paul Specialized Hospital, Reengineering in St. Paul Specialized Hospital, Adama Hospital and Assella Hospital has shown Adama Hospital and Assella Hospital has shown improvements in terms of reducing the waiting time improvements in terms of reducing the waiting time and friendly environment.and friendly environment.
• Furthermore, health service utilization rate has Furthermore, health service utilization rate has increased from 0.25 in 1996/97 to 0.27 in 2000/01 increased from 0.25 in 1996/97 to 0.27 in 2000/01 and subsequently to 0.36 in EFY 2003/04. and subsequently to 0.36 in EFY 2003/04. Opportunities and options for curative services Opportunities and options for curative services including inpatient care have also improved with the including inpatient care have also improved with the increasing number of private clinics and hospitals increasing number of private clinics and hospitals especially in urban areas.especially in urban areas.
• The challenges with regard to medical service are The challenges with regard to medical service are delayed development of the essential package of delayed development of the essential package of services and referral system guidelines; delayed services and referral system guidelines; delayed revision of coverage calculation system; shortage of revision of coverage calculation system; shortage of diagnosis and treatment protocols; poor drug diagnosis and treatment protocols; poor drug management system; and poor human resource management system; and poor human resource management and unsatisfactory professional ethics. management and unsatisfactory professional ethics. Therefore, the future planning should properly Therefore, the future planning should properly address these areas in order to improve the quality address these areas in order to improve the quality of care and ensure adequate utilization of the health of care and ensure adequate utilization of the health service by the public.service by the public.
• 5.2.6. Hygiene and Environmental Health5.2.6. Hygiene and Environmental Health• A) Objectives of Hygiene and Environmental A) Objectives of Hygiene and Environmental
HealthHealth• Hygiene and environmental health is one of the Hygiene and environmental health is one of the
components in HSEP and the objective of this components in HSEP and the objective of this subcomponent is to:subcomponent is to:
• Increase the coverage of hygiene and environmental health services of Increase the coverage of hygiene and environmental health services of the population.the population.
• Increasing access to toilet facilities from 10 % to 17%, for which the Increasing access to toilet facilities from 10 % to 17%, for which the achievement was 29 % in 2003/04.achievement was 29 % in 2003/04.
• Increase access to safe water which has also improved from 23.1% in Increase access to safe water which has also improved from 23.1% in 1997/98 to 35.9% in 2003/04; while access to sanitation increased from 1997/98 to 35.9% in 2003/04; while access to sanitation increased from 12.5% to 29%.12.5% to 29%.
• Some of the implemented activities are:Some of the implemented activities are:• Public Health Proclamation was issued in 2000Public Health Proclamation was issued in 2000• Public Health Regulation has been prepared and submitted for Public Health Regulation has been prepared and submitted for
endorsement.endorsement.• Forty-seven technical guidelines, leaflets, and posters and related Forty-seven technical guidelines, leaflets, and posters and related
teaching aids on various issues of hygiene and environmental health teaching aids on various issues of hygiene and environmental health were also produced and distributed to health facilities.were also produced and distributed to health facilities.
• Based on the Public Health Proclamation, regions have endorsed Based on the Public Health Proclamation, regions have endorsed Environmental Health Regulation.Environmental Health Regulation.
• National Sanitation Strategy that supports the implementation of MDGs National Sanitation Strategy that supports the implementation of MDGs is prepared in collaboration with the World Bank.is prepared in collaboration with the World Bank.
• Water Quality monitoring by the public sector has reached 44 %. In Water Quality monitoring by the public sector has reached 44 %. In collaboration with EHNRI, MoWR,collaboration with EHNRI, MoWR,
• Regional Water and Health Bureaus, WHO and UNICEF, Rapid National Regional Water and Health Bureaus, WHO and UNICEF, Rapid National Water Quality Assessment is underway.Water Quality Assessment is underway.
• Some packages that suit pastoralist communities have been prepared.Some packages that suit pastoralist communities have been prepared.• To support food-processing plants to produce safe food and be To support food-processing plants to produce safe food and be
competitive in local and international market, ten food-processing plants competitive in local and international market, ten food-processing plants from dairy, meat, fruit and vegetable, flour and edible oil have been from dairy, meat, fruit and vegetable, flour and edible oil have been selected and started implementing HACCP with support from UNIDO. selected and started implementing HACCP with support from UNIDO. Public Health Microbiology of EHNRI has been equipped at a cost of Birr Public Health Microbiology of EHNRI has been equipped at a cost of Birr 1.2 million. Controls and inspection of imported food has shown 24 % 1.2 million. Controls and inspection of imported food has shown 24 % increment in 2003/04 as compared to the 2002/03.increment in 2003/04 as compared to the 2002/03.
• The 75 % achievement in latrine overage of SNNPR in a year time The 75 % achievement in latrine overage of SNNPR in a year time through mobilization of communities and administrative staff at all through mobilization of communities and administrative staff at all regional levels could be sited as a best practice.regional levels could be sited as a best practice.
• The following are major challenges encountered during the The following are major challenges encountered during the implementation of the program:implementation of the program:

– The service has not reached the majority of rural population and in The service has not reached the majority of rural population and in some regions it is limited to urban areas focusing only on some regions it is limited to urban areas focusing only on inspection of catering establishments.inspection of catering establishments.
– Data on sanitation coverage are scanty and variedData on sanitation coverage are scanty and varied– Low performance in the inspection of solid waste disposal (76%) Low performance in the inspection of solid waste disposal (76%)
and control of water sources quality (44%) in 2003/04.and control of water sources quality (44%) in 2003/04.– Contribution of environmental health services in prevention and Contribution of environmental health services in prevention and
control of major diseases such as malaria, TB and diarrhea control of major diseases such as malaria, TB and diarrhea diseases in children is not realized and remained un-integrated into diseases in children is not realized and remained un-integrated into these programs.these programs.
– Hygiene education and promotional works lack systematic Hygiene education and promotional works lack systematic approaches.approaches.
– There is low level of leadership and attention for environmental There is low level of leadership and attention for environmental health services from regional health bureaus to Woreda Health health services from regional health bureaus to Woreda Health Offices. Except for salary, there is no earmarked budget for Offices. Except for salary, there is no earmarked budget for environmental health in several regions and virtually non-existence environmental health in several regions and virtually non-existence at health facility level. Environmental Health is abolished from the at health facility level. Environmental Health is abolished from the organizational structure in one region and downgraded in others.organizational structure in one region and downgraded in others.
– There is lack of career structure for sanitarians resulting in poor There is lack of career structure for sanitarians resulting in poor commitment to their job.commitment to their job.

• B) Access to servicesB) Access to services• To improve healthcare service accessibility, health To improve healthcare service accessibility, health
facility construction and expansions are underway. facility construction and expansions are underway. This will expand the network of health posts and This will expand the network of health posts and health centers, while at the same time ensur¬ing health centers, while at the same time ensur¬ing that they are adequately equipped.that they are adequately equipped.
• One strategy in this component is to implement the One strategy in this component is to implement the accelerated expansion of Primary Care services by accelerated expansion of Primary Care services by constructing new health posts and health centers constructing new health posts and health centers and upgrading health stations to health centers. A and upgrading health stations to health centers. A related key activity for Woreda Health Offices is to related key activity for Woreda Health Offices is to supervise the construction, equipping and furnishing supervise the construction, equipping and furnishing of new health posts and new and upgraded health of new health posts and new and upgraded health centers.centers.

• To reach HSDP III targetsTo reach HSDP III targets::• 13,635 health posts and 3,200 health centers are needed.13,635 health posts and 3,200 health centers are needed.• These facilities must be staffed with 30,000 health extension workers These facilities must be staffed with 30,000 health extension workers
and 5,000 health officersand 5,000 health officers• Facilities also need to produce accurate information about their work Facilities also need to produce accurate information about their work
through a Health Management Information System. Woreda and through a Health Management Information System. Woreda and regional health offices/bureaus provide a vital role in supporting these regional health offices/bureaus provide a vital role in supporting these facilities.facilities.
• 5.2: Trends in increase of selected categories of Health Human 5.2: Trends in increase of selected categories of Health Human Resource in Ethiopia duringResource in Ethiopia during
• HSDP I and II as compared to 1989 E.C.HSDP I and II as compared to 1989 E.C.• Human ResourcesHuman Resources• CategoryCategory• Average Number of yearly graduatesAverage Number of yearly graduates• Difference at 1997 as compared to 1989 Before HSDPDifference at 1997 as compared to 1989 Before HSDP• 19891989• HSDP IHSDP I• 1990-19941990-1994• HSDP IIHSDP II• 1995-19971995-1997

• All physicians 244 205 387 59% increaseAll physicians 244 205 387 59% increase• Specialist physicians 68 63 127 87% increaseSpecialist physicians 68 63 127 87% increase• General practitioners 176 142 260 48% increaseGeneral practitioners 176 142 260 48% increase• Public health officers 46 137 251 45% increasePublic health officers 46 137 251 45% increase• Nurses (except midwifes) 683 667 2601 81% Nurses (except midwifes) 683 667 2601 81%
increaseincrease• Midwifes (Senior) 90 50 75 17% decreaseMidwifes (Senior) 90 50 75 17% decrease• Pharmacists 32 34 59 81% increasePharmacists 32 34 59 81% increase• Laboratory technician 190 214 382 101% increaseLaboratory technician 190 214 382 101% increase• 5.3: Human Resource Development5.3: Human Resource Development
• State the objectives for human resource developmentState the objectives for human resource development
• Identify major challenges to human resource developmentIdentify major challenges to human resource development

• 5.3.1 Introduction5.3.1 Introduction• The major objective of the human resource development The major objective of the human resource development
sub-component is to train and supply qualified health sub-component is to train and supply qualified health workers. The specific objectives are to:workers. The specific objectives are to:
• supply skilled manpower in adequate number to new health supply skilled manpower in adequate number to new health facilitiesfacilities
• improve the capacity of the existing health manpower improve the capacity of the existing health manpower working at various levelsworking at various levels
• initiate and strengthen continuing education and in-service initiate and strengthen continuing education and in-service trainingtraining
• review and improve the curricula of some categories of review and improve the curricula of some categories of health workershealth workers
• rationalize the categories of personnelrationalize the categories of personnel• In order to meet these objectives, the training capacity of In order to meet these objectives, the training capacity of
teaching institutes was increased and strengthened.teaching institutes was increased and strengthened.

• For instance, two already existing MOE For instance, two already existing MOE institutions with health worker training institutions with health worker training programmes (Alemaya andprogrammes (Alemaya and
• Dilla) started operating diploma and degree Dilla) started operating diploma and degree level training programmes in 1990 EFY. New level training programmes in 1990 EFY. New training programmes and schools under training programmes and schools under RHBs were started in Arbaminch, Gambella, RHBs were started in Arbaminch, Gambella, Jijiga, Borena and Benishangul Gumuz; a Jijiga, Borena and Benishangul Gumuz; a number of training institutions were expanded number of training institutions were expanded and rehabilitated; training materials were and rehabilitated; training materials were provided to training institutions; teachers were provided to training institutions; teachers were provided with pedagogic training; and several provided with pedagogic training; and several training curricula were revised.training curricula were revised.

• Health Human Resource Development Plan was Health Human Resource Development Plan was developed with projection of the required human developed with projection of the required human resource by category and strategies of improving the resource by category and strategies of improving the quality of training and human resource management. quality of training and human resource management. The number of graduating health human resource The number of graduating health human resource and availability of all categories of health and availability of all categories of health professionals has also improved over time, the most professionals has also improved over time, the most remarkable improvement being in health officers and remarkable improvement being in health officers and nurses (see table 2.2 and 2.3).nurses (see table 2.2 and 2.3).
• Moreover, the achievement in the training of primary Moreover, the achievement in the training of primary health care workers was 133% and overall, the health care workers was 133% and overall, the number of health workers of all categories trained in number of health workers of all categories trained in 2003/04 was 2,876, which shows an increase by 2003/04 was 2,876, which shows an increase by nearly 64 % as compared to the 2002/03 (1,758).nearly 64 % as compared to the 2002/03 (1,758).

• The major challenges in relation to human resource The major challenges in relation to human resource development are:development are:
• Poor deployment and retention of all health professionalsPoor deployment and retention of all health professionals• Poor human resource managementPoor human resource management• Challenges in areas of training of midwivesChallenges in areas of training of midwives• Poor quality of training due to frequent changes in the Poor quality of training due to frequent changes in the
modality of trainingmodality of training• Lack of national exam to assess the traineesLack of national exam to assess the trainees• Shortage of budget, staff and training materials for RTCsShortage of budget, staff and training materials for RTCs• Irregularities of continuing educations and on the job trainingIrregularities of continuing educations and on the job training• Absence of clear guideline on deployment and transfers of Absence of clear guideline on deployment and transfers of
health professionals at national and inter-regional levels in health professionals at national and inter-regional levels in order to avoid the subsequent illicit behavior impacting staff order to avoid the subsequent illicit behavior impacting staff moralemorale

• 5.3: The ratio of health workforce to population 5.3: The ratio of health workforce to population before and during HSDP I and II as compared to before and during HSDP I and II as compared to 1989 E.C.1989 E.C.
• Human Resources CategoryHuman Resources Category• Availability to populationAvailability to population• Before HSDP 1989 End HSDP I 1994 HSDP IIBefore HSDP 1989 End HSDP I 1994 HSDP II• TotalTotal• No.No.• Ratio to populationRatio to population• TotalTotal• No.No.• Ratio to populationRatio to population• TotalTotal• No.No.• Ratio to populationRatio to population
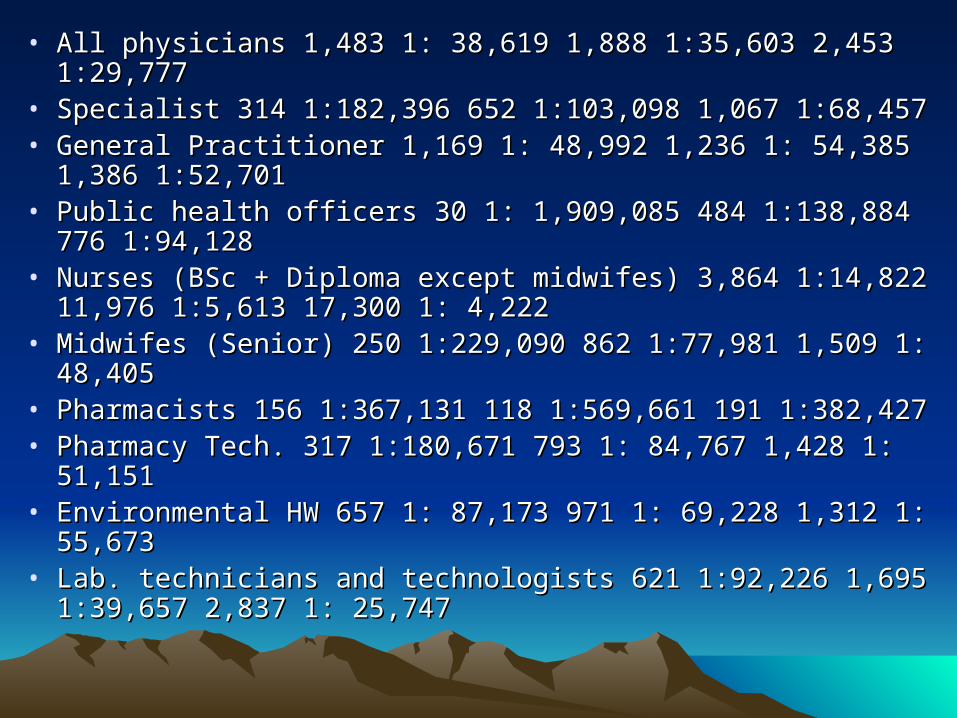
• All physicians 1,483 1: 38,619 1,888 1:35,603 2,453 1:29,777All physicians 1,483 1: 38,619 1,888 1:35,603 2,453 1:29,777• Specialist 314 1:182,396 652 1:103,098 1,067 1:68,457Specialist 314 1:182,396 652 1:103,098 1,067 1:68,457• General Practitioner 1,169 1: 48,992 1,236 1: 54,385 1,386 General Practitioner 1,169 1: 48,992 1,236 1: 54,385 1,386
1:52,7011:52,701• Public health officers 30 1: 1,909,085 484 1:138,884 776 Public health officers 30 1: 1,909,085 484 1:138,884 776
1:94,1281:94,128• Nurses (BSc + Diploma except midwifes) 3,864 1:14,822 Nurses (BSc + Diploma except midwifes) 3,864 1:14,822
11,976 1:5,613 17,300 1: 4,22211,976 1:5,613 17,300 1: 4,222• Midwifes (Senior) 250 1:229,090 862 1:77,981 1,509 1: Midwifes (Senior) 250 1:229,090 862 1:77,981 1,509 1:
48,40548,405• Pharmacists 156 1:367,131 118 1:569,661 191 1:382,427Pharmacists 156 1:367,131 118 1:569,661 191 1:382,427• Pharmacy Tech. 317 1:180,671 793 1: 84,767 1,428 1: Pharmacy Tech. 317 1:180,671 793 1: 84,767 1,428 1:
51,15151,151• Environmental HW 657 1: 87,173 971 1: 69,228 1,312 1: Environmental HW 657 1: 87,173 971 1: 69,228 1,312 1:
55,67355,673• Lab. technicians and technologists 621 1:92,226 1,695 Lab. technicians and technologists 621 1:92,226 1,695
1:39,657 2,837 1: 25,7471:39,657 2,837 1: 25,747

• 5.4: Pharmaceutical Service5.4: Pharmaceutical Service– Describe the Ethiopian drug system.Describe the Ethiopian drug system.– Identify an updated list of essential drugIdentify an updated list of essential drug– Identify challenges in pharmaceutical servicesIdentify challenges in pharmaceutical services
• 5.4.1 Pharmaceutical Services5.4.1 Pharmaceutical Services• The objective of the pharmaceutical The objective of the pharmaceutical
services sub-component is to ensure a services sub-component is to ensure a regular and adequate supply of effective, regular and adequate supply of effective, safe and affordable essential drugs, medical safe and affordable essential drugs, medical supplies and equipment in the public and supplies and equipment in the public and the private sector and ensuring their rational the private sector and ensuring their rational use. The Drug Administration and Control use. The Drug Administration and Control Authority (DACA) and PharmaceuticalAuthority (DACA) and Pharmaceutical
• Administration and Supply Services (PASS) of the Federal Administration and Supply Services (PASS) of the Federal Ministry of Health are the two responsible bodies in the Ministry of Health are the two responsible bodies in the pharmaceutical sector. DACA is responsible for the overall pharmaceutical sector. DACA is responsible for the overall policy implementation and administration of the sector while policy implementation and administration of the sector while PASS is responsible for the procurement and supply of PASS is responsible for the procurement and supply of medical equipments and drugs to health institutions.medical equipments and drugs to health institutions.
• DACA has concluded the total revision of National Drug DACA has concluded the total revision of National Drug Policy (NDP) and the subsequent development of the master Policy (NDP) and the subsequent development of the master plan in 1996-98. The 1987 National Essential Drug List has plan in 1996-98. The 1987 National Essential Drug List has been revised and is ready for printing.been revised and is ready for printing.
• In addition, two studies entitled “Assessment of the In addition, two studies entitled “Assessment of the Pharmaceutical Sector in Ethiopia (FDRE/WHO, 2003)” and Pharmaceutical Sector in Ethiopia (FDRE/WHO, 2003)” and the “Drug Supply and Use in Ethiopia (HCF Secretariat, the “Drug Supply and Use in Ethiopia (HCF Secretariat, 2002)” have been published. One of the most important 2002)” have been published. One of the most important recommendations of these studies is institutional recommendations of these studies is institutional strengthening including the availability of qualified strengthening including the availability of qualified pharmacists.pharmacists.

The local production of pharmaceuticals and medical The local production of pharmaceuticals and medical supplies has increased consistently. By the end of supplies has increased consistently. By the end of 2003, three of the 13 pharmaceutical manufacturers 2003, three of the 13 pharmaceutical manufacturers have received DACA’s licenses for export. The have received DACA’s licenses for export. The number of importers has also increased from 49 in number of importers has also increased from 49 in 2001/02 to 70 in 2003/04. Except for the drug shops 2001/02 to 70 in 2003/04. Except for the drug shops that show increment from 250 to 381, the number of that show increment from 250 to 381, the number of pharmacies has decreased from 304 to 276 and pharmacies has decreased from 304 to 276 and rural drug vendors from 1950 to 1787 for the period rural drug vendors from 1950 to 1787 for the period 2000-2004 (1992-97EFY). Drug formulary and 2000-2004 (1992-97EFY). Drug formulary and standard treatment for different levels of health standard treatment for different levels of health facilities have also been developed. In general, the facilities have also been developed. In general, the availability of drugs in the health facilities has availability of drugs in the health facilities has improved.improved.

• With regard to pharmaceutical human resource,With regard to pharmaceutical human resource,• The number of diploma schools for druggists and pharmacy The number of diploma schools for druggists and pharmacy
technicians has increasedtechnicians has increased• A school of pharmacy opened in Jimma University in 1994 A school of pharmacy opened in Jimma University in 1994
EFY at a degree level, and in the same year the school of EFY at a degree level, and in the same year the school of Pharmacy in AAU started two postgraduate courses.Pharmacy in AAU started two postgraduate courses.
• Several trainings have been conducted on different topics Several trainings have been conducted on different topics and guidelines were producedand guidelines were produced
• A drug information bulletin is being published regularly.A drug information bulletin is being published regularly.• The national availability of essential key drugs (based on a The national availability of essential key drugs (based on a
survey result published in 2003) was:survey result published in 2003) was:• 75% for public facilities, with an 8% general average for 75% for public facilities, with an 8% general average for
presence of expired drugspresence of expired drugs• 85% for regional drug stores, with a 2% general average for 85% for regional drug stores, with a 2% general average for
presence of expired drugspresence of expired drugs• 95% for private retail drug outlets with a 3% general average 95% for private retail drug outlets with a 3% general average
for presence of expired drugsfor presence of expired drugs

• The challenges encountered are:The challenges encountered are:• High attrition rate of pharmaceutical personnel to the private sector.High attrition rate of pharmaceutical personnel to the private sector.• Weakness in the drug management, monitoring and evaluation systemWeakness in the drug management, monitoring and evaluation system• Weakness in the implementation of proclamation and some elements of Weakness in the implementation of proclamation and some elements of
NDPNDP• Low budget allocation to drugsLow budget allocation to drugs• Lack of proper stock management at health facilities as revealed by lack Lack of proper stock management at health facilities as revealed by lack
of stock control toolsof stock control tools• Lack of linkage between the drug registration process with inspection of Lack of linkage between the drug registration process with inspection of
manufacturing sites abroadmanufacturing sites abroad• Inadequate in-service training of health workers and shortage of stores.Inadequate in-service training of health workers and shortage of stores.• Therefore, the future direction should be:Therefore, the future direction should be:• strengthening the overall drug management system,strengthening the overall drug management system,• improving the implementation of policy/proclamations in order to achieve improving the implementation of policy/proclamations in order to achieve
the objectives set under the pharmaceutical componentthe objectives set under the pharmaceutical component• Revision of some aspects of the National Drug Policy (NDP) as indicated Revision of some aspects of the National Drug Policy (NDP) as indicated
by DACAby DACA• Strengthening the medical equipment maintenance system.Strengthening the medical equipment maintenance system.
5.5: Information, Education and Communication (IEC) and 5.5: Information, Education and Communication (IEC) and HealthHealth
• Information Management System (HMIS)Information Management System (HMIS)• List two objectives of Information, Education and List two objectives of Information, Education and
Communication sub componentCommunication sub component• List the objectives of Health Information Management List the objectives of Health Information Management
System (HMIS) sub componentSystem (HMIS) sub component• List the enabling factors for implementation of HMISList the enabling factors for implementation of HMIS• State major challenges for implementation of HMISState major challenges for implementation of HMIS5.5.1. Information, Education and Communication (IEC)5.5.1. Information, Education and Communication (IEC)• The objective of the IEC sub-component is to support the The objective of the IEC sub-component is to support the
development and implementation of a national IEC plan and development and implementation of a national IEC plan and strategy whose goals include:strategy whose goals include:
• Improve health KAP (knowledge, attitude, practice) about Improve health KAP (knowledge, attitude, practice) about personal and environmental hygiene and common illnesses personal and environmental hygiene and common illnesses and their causesand their causes

• Promote community support for preventive and Promote community support for preventive and promotive health services through educating and promotive health services through educating and influencing planners, policy makers, managers, influencing planners, policy makers, managers, women groups and potential collaboratorswomen groups and potential collaborators
• The major constraints to the implementation of The major constraints to the implementation of IEC/BCC (behavioral change communication) are:IEC/BCC (behavioral change communication) are:
• The delay in developing behavioral change The delay in developing behavioral change communication strategies for national and regional communication strategies for national and regional levels focusing on:levels focusing on:– youth - HIV/AIDS, reproductive health, personalyouth - HIV/AIDS, reproductive health, personal– married couples- family planning, safe motherhood, married couples- family planning, safe motherhood,
nutritionnutrition– health workers - interpersonal communication and health workers - interpersonal communication and
counselingcounseling

• Inadequate technical capacity of staff at all levels of the Inadequate technical capacity of staff at all levels of the health system;health system;
• Inadequate budgetary allocation for IECInadequate budgetary allocation for IEC• Poor coordination of the many players both within the Poor coordination of the many players both within the
government and NGOs on IECgovernment and NGOs on IEC• Inadequate quality monitoring system for IECInadequate quality monitoring system for IEC• Inadequate capacity and ineffective system for Inadequate capacity and ineffective system for
planning, implementing, monitoring and evaluation ofplanning, implementing, monitoring and evaluation of
• IEC/BCC activities at all levels of the health IEC/BCC activities at all levels of the health system leading to ineffectiveness of IEC/BCC system leading to ineffectiveness of IEC/BCC efforts to serve as vehicles through which efforts to serve as vehicles through which behavioral change can be effected.behavioral change can be effected.

• 5.5.2. Health Information Management System 5.5.2. Health Information Management System (HMIS)(HMIS)
• Management information system (MIS): is a system Management information system (MIS): is a system designed by an organization to collect and report designed by an organization to collect and report information on a program and which allows information on a program and which allows managers to plan, monitor and evaluate the managers to plan, monitor and evaluate the operations and the performance of the programoperations and the performance of the program
• A Health management Information System (HMIS) A Health management Information System (HMIS) is a management information system that is directed is a management information system that is directed towards health.towards health.
• The major objective of this subcomponent is to:The major objective of this subcomponent is to:– improve knowledge and skills in the areas of policy improve knowledge and skills in the areas of policy
formulation, planning and budgeting, financial formulation, planning and budgeting, financial management, programme implementation and M&E for management, programme implementation and M&E for staff of FMOH, regions and woredasstaff of FMOH, regions and woredas
– Enhance community involvement in the management of Enhance community involvement in the management of health facilities and community based health health facilities and community based health interventions.interventions.

• Health management is implemented by:Health management is implemented by:• Appointment of health mangers with appropriate skillsAppointment of health mangers with appropriate skills• Establishment of management boards, health councils, etc at Establishment of management boards, health councils, etc at
all levelsall levels• Revision of Programme Implementation Manual (PIM).Revision of Programme Implementation Manual (PIM).• Staffing of woreda health offices for the effective Staffing of woreda health offices for the effective
implementation of decentralized health system.implementation of decentralized health system.• Hospital management boards have also been established in Hospital management boards have also been established in
federal and some regional hospitals as part of hospital reform federal and some regional hospitals as part of hospital reform activities.activities.
• Several regions carry out planned supervisory visits, and Several regions carry out planned supervisory visits, and have developed supervision manuals that are available to have developed supervision manuals that are available to health management staff at the zonal, woreda and facility health management staff at the zonal, woreda and facility levels.levels.
• Result Oriented Performance Evaluation System (ROPES) Result Oriented Performance Evaluation System (ROPES) that has been initiated in some regionsthat has been initiated in some regions
• The objectives of HMIS are to:The objectives of HMIS are to:• establish/ strengthen HMIS at all levels of health establish/ strengthen HMIS at all levels of health
service delivery systemservice delivery system• establish HMIS units at all levels (FMOH, RHB, establish HMIS units at all levels (FMOH, RHB,
woreda health offices and HF levels)woreda health offices and HF levels)• Establish/strengthen the database at FMOH, RHBs, Establish/strengthen the database at FMOH, RHBs,
woreda and health facilities.woreda and health facilities.• HMIS is implemented by:HMIS is implemented by:• Reducing the number of reporting formats from 25 Reducing the number of reporting formats from 25
to 12 and efforts are also being made to establish to 12 and efforts are also being made to establish networking between FOMH and RHBs.networking between FOMH and RHBs.
• A national HMIS advisory committee (NAC) has A national HMIS advisory committee (NAC) has been established with representation from different been established with representation from different stakeholders. The NAC is established to facilitate stakeholders. The NAC is established to facilitate the development of a national policy and strategy the development of a national policy and strategy onon
• HMIS and M&E. term of reference (TOR) and plan of HMIS and M&E. term of reference (TOR) and plan of action for NAC and for integrated HMIS, M&E and action for NAC and for integrated HMIS, M&E and Information Communication Technology (ICT) Information Communication Technology (ICT) application in one package has also been application in one package has also been completed.completed.
• FMOH and some regions are publishing the annual FMOH and some regions are publishing the annual Health and Health related Indicators.Health and Health related Indicators.
• Networking through email has been implemented in Networking through email has been implemented in 30 Woredas in Tigray. SNNPR RHB has also 30 Woredas in Tigray. SNNPR RHB has also adopted a generic reporting system, produced adopted a generic reporting system, produced guideline, trained staff at all levels and instituted a guideline, trained staff at all levels and instituted a computerized data system. Most of the regions have computerized data system. Most of the regions have adopted reporting systems on major health adopted reporting systems on major health indicators and health sector activities based on indicators and health sector activities based on formats developed jointly by the FMOH and the formats developed jointly by the FMOH and the regions.regions.

• Challenges faced in relation to HMIS are:Challenges faced in relation to HMIS are:• Lack of coordinated effort and leadershipLack of coordinated effort and leadership• Lack of strategy and policy, shortage of skilled Lack of strategy and policy, shortage of skilled
human resource and lack of guideline.human resource and lack of guideline.• Timeliness and completeness of HMIS Timeliness and completeness of HMIS
reporting remains poor, and such delays reporting remains poor, and such delays contribute to the failure (at all levels) to use contribute to the failure (at all levels) to use data as the basis for informed decision-data as the basis for informed decision-making in planning and management.making in planning and management.
• Parallel reporting mechanisms persist with Parallel reporting mechanisms persist with programmatic and donor-supported initiatives programmatic and donor-supported initiatives resulting in multiple reporting formats and an resulting in multiple reporting formats and an increased administrative workloadincreased administrative workload

• 5.6: Monitoring and Evaluation (M&E) and 5.6: Monitoring and Evaluation (M&E) and Healthcare FinancingHealthcare Financing
– Define Monitoring and evaluationDefine Monitoring and evaluation– State prerequisite for monitoring and evaluation State prerequisite for monitoring and evaluation
implementationimplementation– State the objectives of Health care financing sub State the objectives of Health care financing sub
componentcomponent– Identify the budget source for health care Identify the budget source for health care
financing in Ethiopiafinancing in Ethiopia

• 5.6.1. Monitoring and Evaluation (M&E)5.6.1. Monitoring and Evaluation (M&E)• Definition:Definition:• Monitoring and evaluationMonitoring and evaluation• Monitoring is the systematic and continuous Monitoring is the systematic and continuous
assessment of the progress of a piece of work over assessment of the progress of a piece of work over time.time.
• An evaluation is the assessment at one point in An evaluation is the assessment at one point in time of the impact of a piece of work and the extent time of the impact of a piece of work and the extent to which the stated objectives have been achieved.to which the stated objectives have been achieved.
• The major objective of the M&E component is to The major objective of the M&E component is to strengthen the M&E system at federal and regional strengthen the M&E system at federal and regional levels and establish a system in all woredas. The levels and establish a system in all woredas. The specific objectives were to:specific objectives were to:

• Develop/strengthen a M&E system that functions at Develop/strengthen a M&E system that functions at regional and woreda levels,regional and woreda levels,
• Standardize M&E guidelines, harmonize Standardize M&E guidelines, harmonize supervision guidelines for RHBs and woreda health supervision guidelines for RHBs and woreda health officesoffices
• Regularly monitor progress and achievements of Regularly monitor progress and achievements of HSDP components as a whole and improvements HSDP components as a whole and improvements in service delivery, quality of care and financial in service delivery, quality of care and financial performanceperformance
• Evaluate the impact, effectiveness and cost-Evaluate the impact, effectiveness and cost-effectiveness of HSDP II components.effectiveness of HSDP II components.
• Monitoring and Evaluation is implemented by:Monitoring and Evaluation is implemented by:• The establishment of joint steering committees, at The establishment of joint steering committees, at
both central and regional levels, to oversee both central and regional levels, to oversee implementation,implementation,
• Regular reporting by regions and FMOH Regular reporting by regions and FMOH departmentsdepartments

• 5.6.2. Healthcare Financing5.6.2. Healthcare Financing• A) Source of financing for the health care A) Source of financing for the health care
delivery system in Ethiopiadelivery system in Ethiopia• Financing the formal Health care delivery system is Financing the formal Health care delivery system is
highly dependent on government tax revenue (more highly dependent on government tax revenue (more than 60%), followed by external assistance than 60%), followed by external assistance (bilateral, multi-lateral, UN Agencies) which the later (bilateral, multi-lateral, UN Agencies) which the later grew over the years from 25% in the 1960s to grew over the years from 25% in the 1960s to around 35% to date.around 35% to date.
• The central government is hoping to increase the The central government is hoping to increase the share of external support to health to at least 40% or share of external support to health to at least 40% or more for the effective implementation of the MDG-more for the effective implementation of the MDG-based HSDP III.based HSDP III.
• Other sources of health care financing are less Other sources of health care financing are less significant (user charges, insurance schemes, significant (user charges, insurance schemes, charities, the private sector…etc)charities, the private sector…etc)

• Looking back, the Ethiopian Dollar value of health Looking back, the Ethiopian Dollar value of health expenditure between 1940 to 1943 averaged about expenditure between 1940 to 1943 averaged about
• Million and between 1944 to 1946 about 3.56 Million and between 1944 to 1946 about 3.56 million.million.
• By 1953, 3.4% of the government’s Budget was By 1953, 3.4% of the government’s Budget was devoted to public health.devoted to public health.
• Total health expenditure in 1965-66 averaged to Total health expenditure in 1965-66 averaged to some Birr 77 million (USD 30.0 million). This some Birr 77 million (USD 30.0 million). This expenditure included foreign aid support, expenditure included foreign aid support, expenditure on medical school, the Gondar Public expenditure on medical school, the Gondar Public Health College, private medical practice, and the Health College, private medical practice, and the traditional practitioners.traditional practitioners.
• For the same years, the average annual health For the same years, the average annual health budget including health represented about 5% of budget including health represented about 5% of the totalthe total

• Government budget, averaging about USD Government budget, averaging about USD 0.37 per capita on health care. This was one 0.37 per capita on health care. This was one of the lowest per capita expenditure even by of the lowest per capita expenditure even by the standard of many African countries at the the standard of many African countries at the time.time.
• Total government budget in the 2003-04 Total government budget in the 2003-04 reached to an average of about 1.3 Billion reached to an average of about 1.3 Billion Birr per year. A significant amount of external Birr per year. A significant amount of external support has been mobilized, perhaps support has been mobilized, perhaps equivalent to government allocation, over the equivalent to government allocation, over the last three years for special programs such as last three years for special programs such as HIV/AIDS and other priority areas.HIV/AIDS and other priority areas.

• B) The Healthcare Financing StrategyB) The Healthcare Financing Strategy• The objectives of the Health Care Financing The objectives of the Health Care Financing
(HCF) component are to:(HCF) component are to:• Mobilize increased resources to the Mobilize increased resources to the
health sector, which implies:health sector, which implies:• local retention of revenuelocal retention of revenue• cost–sharingcost–sharing• reduced resource leakage from high waiverreduced resource leakage from high waiver• expand special pharmaciesexpand special pharmacies• user-fees revision and risk-sharing.user-fees revision and risk-sharing.
– Promote efficient allocation of resources and Promote efficient allocation of resources and develop a sustainable health care financing develop a sustainable health care financing system.system.

• To implement the above objectives, the To implement the above objectives, the following steps have been taken:following steps have been taken:
• Background studies have been conductedBackground studies have been conducted• Complimentary reforms have been closely monitoredComplimentary reforms have been closely monitored• Reform implementation strategy/action plan has been Reform implementation strategy/action plan has been
designeddesigned• A study on National Health Accounts (NHA) was also A study on National Health Accounts (NHA) was also
conducted using the 1995/96 EFY data.conducted using the 1995/96 EFY data.• Local training in health care financing and Local training in health care financing and
management, outsourcing, and hospital management management, outsourcing, and hospital management efficiency were done.efficiency were done.
• HCF strategy orientation workshops were conducted in HCF strategy orientation workshops were conducted in all regions and over 1,100 people were sensitizedall regions and over 1,100 people were sensitized

• Establishment of private practitioners/providers Establishment of private practitioners/providers association, facilitated by Ministry of Health, is association, facilitated by Ministry of Health, is encouraging the involvement of the private sector in encouraging the involvement of the private sector in the realization of the Health Care Financing Strategy.the realization of the Health Care Financing Strategy.
• The draft Health Service Delivery, Administration and The draft Health Service Delivery, Administration and Management Proclamation and five regulations (fee Management Proclamation and five regulations (fee waiver and exemption, hospital management board, waiver and exemption, hospital management board, out-sourcing of non-clinical services, fee retention at out-sourcing of non-clinical services, fee retention at facility level and establishing private wings in facility level and establishing private wings in government hospitals) have been completed. The government hospitals) have been completed. The Proclamation and the regulations will soon be Proclamation and the regulations will soon be presented to Parliament for endorsement.presented to Parliament for endorsement.

• UNIT VI: HEALTHCARE SYSTEMUNIT VI: HEALTHCARE SYSTEM• REGULATIONREGULATION• IntroductionIntroduction• In the previous units of the module we have In the previous units of the module we have
seen the historical development of health care seen the historical development of health care delivery system in Ethiopia, Structures and delivery system in Ethiopia, Structures and component, Health service programs. And in component, Health service programs. And in this unit we will see the health system this unit we will see the health system regulation that includes health related regulation that includes health related legislation, and facts about accreditation, legislation, and facts about accreditation, licensing, certification and historical back licensing, certification and historical back ground of professional association. Also the ground of professional association. Also the unit includes Health information policies and unit includes Health information policies and proceduresprocedures

• Unit OutlineUnit Outline
• 1. Healthcare System Regulation1. Healthcare System Regulation
• 1.1 Major health related legislations1.1 Major health related legislations
• 1.2 Regulation of Credentialing Health 1.2 Regulation of Credentialing Health ManpowerManpower
• AccreditationAccreditation
• CertificationCertification
• LicensureLicensure
• 1.3 professional associations1.3 professional associations
• 2. Health Information Systems Policies 2. Health Information Systems Policies and Proceduresand Procedures
• 6.1: 6.1: Healthcare System RegulationsHealthcare System Regulations
• At the end of this lesson, the students At the end of this lesson, the students should be able toshould be able to::
• Identify health legislationsIdentify health legislations
• State proclamations related to healthState proclamations related to health
• Discuss differences among licensing, Discuss differences among licensing, certification and accreditationcertification and accreditation
• Identify the responsible body for accreditation, Identify the responsible body for accreditation, certification and licensurecertification and licensure
• Describe professional associations and the Describe professional associations and the purpose they serve6purpose they serve6

• 6.1.1. Major Health Related Legislations6.1.1. Major Health Related Legislations• Some of the major health related legislations are:Some of the major health related legislations are:• The first health decrees were vaccination against The first health decrees were vaccination against
smallpox by Emperors Yohannes and Menelik II, smallpox by Emperors Yohannes and Menelik II, during the smallpox epidemic in 1886.during the smallpox epidemic in 1886.
• However, modern medical legislation could be However, modern medical legislation could be traced back to the coronation of Emperor traced back to the coronation of Emperor Haileselassie I in 1930.Haileselassie I in 1930.
• On July 18, 1930 a law was passed to regulate the On July 18, 1930 a law was passed to regulate the practice of doctors, dentists, pharmacists, midwives practice of doctors, dentists, pharmacists, midwives and veterinarians. The law specified that no one and veterinarians. The law specified that no one could practice these professions without a relevant could practice these professions without a relevant Diploma.Diploma.
• Formal recognition of Traditional Medicine was Formal recognition of Traditional Medicine was given in 1942 (proc. 27). This was reaffirmed in given in 1942 (proc. 27). This was reaffirmed in 1943 and 1948 (proc. 100) as part of the medical 1943 and 1948 (proc. 100) as part of the medical registration proclamation.registration proclamation.

• Between 1941and1950 some 27 Public Health Between 1941and1950 some 27 Public Health enactments were made available, some of them enactments were made available, some of them were:were:– Public Health Proclamation Negarit Gazeta (NG 26, 1942, Public Health Proclamation Negarit Gazeta (NG 26, 1942,
5-6)5-6)– Medical Registration proc. (NG 27, 1942, 6-7)Medical Registration proc. (NG 27, 1942, 6-7)– Pharmacists and druggists Proc. (NG. 34, 1943, 38-39).Pharmacists and druggists Proc. (NG. 34, 1943, 38-39).– Proclamation to systematize and regulate Missionary Proclamation to systematize and regulate Missionary
health activities (May 28, 1945)health activities (May 28, 1945)– Public Health Proclamation (NG 91, 1947, 66-68)Public Health Proclamation (NG 91, 1947, 66-68)– Medical Practitioners Registration Proclamation (NG 100, Medical Practitioners Registration Proclamation (NG 100,
1948, 1-3)1948, 1-3)– Establishment of the Ministry of Public Health, 1948Establishment of the Ministry of Public Health, 1948– Decree on Health tax (NG 20th, No. 11, 1960).Decree on Health tax (NG 20th, No. 11, 1960).
• Pharmacy regulation (NG 288/1964)Pharmacy regulation (NG 288/1964)

– National Research Institute of Health Established (NG National Research Institute of Health Established (NG 271/1985)271/1985)
– Establishment of Ethiopian Pharmaceutical Manufacturing Establishment of Ethiopian Pharmaceutical Manufacturing Factory NG 167/1994Factory NG 167/1994
– Council of Minister of regulation established regulation no Council of Minister of regulation established regulation no (NG 174/1994) to provide for licensing and supervision of (NG 174/1994) to provide for licensing and supervision of Health service Institution.Health service Institution.
– Establishment of the Pharmaceutical and Medical Establishment of the Pharmaceutical and Medical supplies import and wholesome sale enterprise(NG supplies import and wholesome sale enterprise(NG 176/1994)176/1994)
– Nutrition Research Institute Established under council of Nutrition Research Institute Established under council of ministry of regulation( NG 4/1996)ministry of regulation( NG 4/1996)
– Establishment of Health Education Center NG 40/1998Establishment of Health Education Center NG 40/1998– Establishment of Ethiopian Health Professional Council Establishment of Ethiopian Health Professional Council
(NG 76/2002(NG 76/2002

• 6.1.2. Regulation of Credentialing Health 6.1.2. Regulation of Credentialing Health ManpowerManpower
• In requiring compliance with a well-developed In requiring compliance with a well-developed set of quality standards, the processes of set of quality standards, the processes of accreditation licensure and certification accreditation licensure and certification provide a means of evaluating and provide a means of evaluating and determining not only technical performance, determining not only technical performance, but provide facilities and caregivers with but provide facilities and caregivers with important information on practices that important information on practices that improve the delivery of care. In fact, improve the delivery of care. In fact, accreditation and certification act as public accreditation and certification act as public “seals of approval” of the technical practices “seals of approval” of the technical practices delivered by health care facilities or delivered by health care facilities or personnel, respectively.personnel, respectively.

• The regulation of credentialing health manpower The regulation of credentialing health manpower occurs in three forms:occurs in three forms:
• Accreditation of educational programsAccreditation of educational programs• Certification of personnel by the professionCertification of personnel by the profession• Licensure of personnel by a government agency. Licensure of personnel by a government agency.
(Table 6.1 depicts the differences between these (Table 6.1 depicts the differences between these three forms.)three forms.)
• Characteristics Licensing Certification Characteristics Licensing Certification AccreditationAccreditation
• Applied to Healthcare personnel Healthcare Applied to Healthcare personnel Healthcare personnel Educational institutespersonnel Educational institutes
• Granting body Government agency Peer Granting body Government agency Peer organization or Government agencyorganization or Government agency
• Required for Entry into practice Professional status Required for Entry into practice Professional status Professional statusProfessional status
• PurposePurpose

• Restricts entry into field to personnel who can’t Restricts entry into field to personnel who can’t meet the standardmeet the standard
• Recognized qualification to practice at higher levelRecognized qualification to practice at higher level• Public assurance of desired level of quality of carePublic assurance of desired level of quality of care• Duration Permanent Permanent or fixed term Fixed Duration Permanent Permanent or fixed term Fixed
termterm• Indicates high quality No Yes YesIndicates high quality No Yes Yes• Performance based No Sometimes YesPerformance based No Sometimes Yes• Administration Simple Moderate ComplexAdministration Simple Moderate Complex• Renewal Automatic (possible exam) Continuing Renewal Automatic (possible exam) Continuing
education (possible exam) Complete reinspectioneducation (possible exam) Complete reinspection

• A) AccreditationA) Accreditation• Accreditation refers to a process of quality control and Accreditation refers to a process of quality control and
assurance whereby, as a result of inspection or assessment, assurance whereby, as a result of inspection or assessment, an institution or its programmes are recognized as meeting an institution or its programmes are recognized as meeting minimum standards (Adelman, 1992). In most developing minimum standards (Adelman, 1992). In most developing and developed countries, health science education training and developed countries, health science education training institutions are controlled by the national health rather than institutions are controlled by the national health rather than educational authorities. However in Ethiopia the responsibility educational authorities. However in Ethiopia the responsibility designated to MOH encompasses the accreditation of health designated to MOH encompasses the accreditation of health facilities (e.g. Hospitals, Health Centers, Health Post, etc.) facilities (e.g. Hospitals, Health Centers, Health Post, etc.) licensing of practitioners and specialty certification while licensing of practitioners and specialty certification while institutional and program accreditation is determined by a institutional and program accreditation is determined by a semiautonomous body: Higher Education Relevance Quality semiautonomous body: Higher Education Relevance Quality Agency (HERQA). The MOE established HERQA as a sector Agency (HERQA). The MOE established HERQA as a sector support unit through the Higher Education Proclamation (No. support unit through the Higher Education Proclamation (No. 351/2003). It is directly accountable to the MOE.351/2003). It is directly accountable to the MOE.

• Purpose of Accrediting Educational Purpose of Accrediting Educational Institutions:Institutions:
• Establishing criteria for professional Establishing criteria for professional certification and licensure;certification and licensure;
• Assisting prospective students in identifying Assisting prospective students in identifying acceptable programs;acceptable programs;
• Creating goals for self-improvement and Creating goals for self-improvement and stimulating higher standards among stimulating higher standards among institutions; andinstitutions; and
• Helping to identify institutions and programs Helping to identify institutions and programs for the investment of public and private funds for the investment of public and private funds and providing bases for determining eligibility and providing bases for determining eligibility for governmental assistance.for governmental assistance.

• 6.1 characteristic differences between licensing, 6.1 characteristic differences between licensing, certification and accreditationcertification and accreditation
• B) CertificationB) Certification• Certification is essentially synonymous with Certification is essentially synonymous with
accreditation, except that certification is often accreditation, except that certification is often applied to individuals (such as certifying a medical applied to individuals (such as certifying a medical specialist), whereas accreditation is applied to specialist), whereas accreditation is applied to institutions or programs (such as accrediting a institutions or programs (such as accrediting a medical education program). It is recognized as an medical education program). It is recognized as an important and beneficial component of career important and beneficial component of career development for providers as it consist of the development for providers as it consist of the completion of a training program in different health completion of a training program in different health science professions. Certification enables the public science professions. Certification enables the public to identify those practitioners who have met to identify those practitioners who have met standards of training and experiences set above the standards of training and experiences set above the level required for licensure.level required for licensure.

• In developed countries such as the U.K. and In developed countries such as the U.K. and Australia, national medical councils control Australia, national medical councils control primary certification indirectly through the primary certification indirectly through the process of accrediting the medical school process of accrediting the medical school curriculum. While in the U.S. and Canada, curriculum. While in the U.S. and Canada, national examinations following academic national examinations following academic requirements play a major role in primary requirements play a major role in primary certification (Hafez 1997).certification (Hafez 1997).
• Regardless of either approach, there is Regardless of either approach, there is common ground in terms of certification being common ground in terms of certification being assessed and determined by non assessed and determined by non governmental bodies.governmental bodies.

Primary certification in Ethiopia is mandatory, although Primary certification in Ethiopia is mandatory, although it does not guarantee employment. Examinations it does not guarantee employment. Examinations are conducted at the national level by the MOE, of are conducted at the national level by the MOE, of which health professionals have to score at least which health professionals have to score at least 60% on the qualifying exam to be certified and 60% on the qualifying exam to be certified and registered as professional in a specified health field. registered as professional in a specified health field. Specialty certification is conducted by the MoH. Specialty certification is conducted by the MoH. However, both areas are lacking as certifying bodies However, both areas are lacking as certifying bodies are outside of the influence of professional societies/ are outside of the influence of professional societies/ organizations and assessment of competency organizations and assessment of competency through examination following graduation is not through examination following graduation is not being applied. Additionally, issues of recertification being applied. Additionally, issues of recertification and Certifying medical education to date have not and Certifying medical education to date have not been explored.been explored.
• C) LicensureC) Licensure• Licensure is a regulation of health manpower by a Licensure is a regulation of health manpower by a
government agency that verifies that health government agency that verifies that health providers meet the basic minimum standards of providers meet the basic minimum standards of competency to perform their work safely and competency to perform their work safely and effectively. As licensing functions as a work permit, it effectively. As licensing functions as a work permit, it is mandatory for institutional or independent is mandatory for institutional or independent practices in public /private/nongovernmental practices in public /private/nongovernmental organizations. Upon certification of personnel by the organizations. Upon certification of personnel by the profession, a professional may be registered for a profession, a professional may be registered for a licensure.licensure.
• In 2007 the MOH designated Regional Health In 2007 the MOH designated Regional Health Bureaus the authority to conduct licensing for all Bureaus the authority to conduct licensing for all certificate and diploma level health professionals. certificate and diploma level health professionals. Currently licensing at these levels is being Currently licensing at these levels is being conducted in 5 different regions.conducted in 5 different regions.

• It is the wish of the MOH that all regions It is the wish of the MOH that all regions provide periodic licensure for any certificate or provide periodic licensure for any certificate or diploma level health practitioner to practice diploma level health practitioner to practice within their specific region upon being within their specific region upon being certified, competent and that there is demand.certified, competent and that there is demand.
• The licensing of degree level and above The licensing of degree level and above remains the responsibility of the MoH as the remains the responsibility of the MoH as the equitable distribution of high level health equitable distribution of high level health professionals remains pertinent.professionals remains pertinent.

• 6.1.3. Professional Associations6.1.3. Professional Associations
• The purposes of professional associations are The purposes of professional associations are many, but to site a few, they are:many, but to site a few, they are:
• To devise peer review systemsTo devise peer review systems
• To participate in the setting of professional To participate in the setting of professional standards and provide continuing education in standards and provide continuing education in their respective fieldstheir respective fields
• To serve as referral points in policy and To serve as referral points in policy and development issues.development issues.
• A number of professional associations are in A number of professional associations are in existence in Ethiopia, to cite a few:existence in Ethiopia, to cite a few:

A) Ethiopian Nurses Association (ENA):A) Ethiopian Nurses Association (ENA): established in July 1952, it is the oldest and established in July 1952, it is the oldest and pioneer professional association in Ethiopia. pioneer professional association in Ethiopia. Its Objectives are:Its Objectives are:
• To improve Nursing service to the benefit of To improve Nursing service to the benefit of the society, standing for the right of Nurse and the society, standing for the right of Nurse and ClientsClients
• Advance Nursing Education, practice, Advance Nursing Education, practice, management and research to ensure quality management and research to ensure quality Nursing care to the people of EthiopiaNursing care to the people of Ethiopia
• Promote positive practice environment in the Promote positive practice environment in the work placework place

• B) Ethiopian Traditional Medicine B) Ethiopian Traditional Medicine Practitioners Association: established in Practitioners Association: established in 1991, its objectives are:1991, its objectives are:
• To provide a forum for exchange of ideas and To provide a forum for exchange of ideas and experiences among traditional medicine experiences among traditional medicine practitionerspractitioners

C) Ethiopian Medical Association (EMA): established in C) Ethiopian Medical Association (EMA): established in July 1969, its objectives are:July 1969, its objectives are:
• To promote the science and art of medicine and the To promote the science and art of medicine and the improvement of public healthimprovement of public health
• To keep a high standards of professional ethics and etiquetteTo keep a high standards of professional ethics and etiquette• To promote the professional excellence of its members in To promote the professional excellence of its members in
preventive and curative medicine and medical researchpreventive and curative medicine and medical research• To promote and maintain intellectual and professional To promote and maintain intellectual and professional
freedomfreedom• To provide professional and technical advice to the Ministry To provide professional and technical advice to the Ministry
of Health and other concerned organizationsof Health and other concerned organizations• To initiate and maintain professional linkage with similar To initiate and maintain professional linkage with similar
associations within and outside Ethiopiaassociations within and outside Ethiopia• To provide a forum for the exchange of professional ideas, To provide a forum for the exchange of professional ideas,
knowledge and experienceknowledge and experience• To encourage and support the establishment of specialized To encourage and support the establishment of specialized
societies in medicinesocieties in medicine• To monitor the quality of medical services rendered to the To monitor the quality of medical services rendered to the
publicpublic
• D) Ethiopian Pharmaceutical Association (EPA): D) Ethiopian Pharmaceutical Association (EPA): established in 1974, its objectives are:established in 1974, its objectives are:
• To promote the pharmaceutical professionTo promote the pharmaceutical profession• To promote the rights of its membersTo promote the rights of its members• To provide a forum for exchange of ideas and To provide a forum for exchange of ideas and
experiences among professionalsexperiences among professionals• To work with similar associations for the To work with similar associations for the
improvement of the health servicesimprovement of the health services• To encourage and assist research and development To encourage and assist research and development
programs in the fieldprograms in the field• To ensure an acceptable standard of the profession To ensure an acceptable standard of the profession
in Ethiopiain Ethiopia• To maintain the honor and ethics of the professionTo maintain the honor and ethics of the profession

• E) Ethiopian Public Health Association E) Ethiopian Public Health Association (EPHA): established in August 1989, its (EPHA): established in August 1989, its objectives are:objectives are:
• To bring together professionals to promote To bring together professionals to promote public health sciencepublic health science
• To review and recommend issues related to To review and recommend issues related to health policies, planning, training and health policies, planning, training and managementmanagement
• To promote the professional interest of its To promote the professional interest of its membersmembers
• To advance research in public healthTo advance research in public health
• To disseminate information on public healthTo disseminate information on public health

F) Ethiopian Dental Professionals F) Ethiopian Dental Professionals Association: established in February 1992, Association: established in February 1992, its objectives are:its objectives are:
• To promote dental professionTo promote dental profession• To formulate forums for exchange of ideas To formulate forums for exchange of ideas
among professionals on the global scientific among professionals on the global scientific progress of dentistry.progress of dentistry.
• To keep high standard of professional ethics To keep high standard of professional ethics and etiquette of Ethiopian dental and etiquette of Ethiopian dental professionalsprofessionals
• To safe guard the interests of its membersTo safe guard the interests of its members• To provide professional and technical advice To provide professional and technical advice
to health institutionsto health institutions

• G) Ethiopian Society of Obstetricians and G) Ethiopian Society of Obstetricians and Gynecologists (ESOG): established in March Gynecologists (ESOG): established in March 1992, its objectives are:1992, its objectives are:
• To ensure a high standard of obstetrical and To ensure a high standard of obstetrical and gynecological practicesgynecological practices
• To play an advisory role in the training of obstetrics To play an advisory role in the training of obstetrics and gynecologyand gynecology
• To protect and safeguard the professional interest of To protect and safeguard the professional interest of membersmembers
• To promote friendship and exchange ideas among To promote friendship and exchange ideas among professionalsprofessionals
• To initiate and maintain professional linkages with To initiate and maintain professional linkages with similar societies within and outside Ethiopiasimilar societies within and outside Ethiopia

• H) Radiological Society of Ethiopia: H) Radiological Society of Ethiopia: established in October 1994, its objectives established in October 1994, its objectives are:are:
• To ensure highest possible standard of To ensure highest possible standard of professional competenceprofessional competence
• To serve as an advisory body in the fieldTo serve as an advisory body in the field
• To protect and safeguard professional rights To protect and safeguard professional rights and interests of its membersand interests of its members
• To foster fellowship among members and To foster fellowship among members and other allied professionalsother allied professionals

• 6.2: Health Information Systems Policies 6.2: Health Information Systems Policies and Proceduresand Procedures
• 6.2.1. Introduction6.2.1. Introduction
• Delivering healthcare services to the Delivering healthcare services to the population is dependent on information for population is dependent on information for proper planning. To have a properly proper planning. To have a properly functioning Health Management Information functioning Health Management Information System (HMIS), there must be policies and System (HMIS), there must be policies and procedures which are adequately enforced.procedures which are adequately enforced.

• 6.2.2. HIS Policies and Procedures6.2.2. HIS Policies and Procedures• Legal, regulatory and planning context of health Legal, regulatory and planning context of health
information is a key resource for effective Health Information information is a key resource for effective Health Information System (HIS). It enables the establishment of mechanisms System (HIS). It enables the establishment of mechanisms to ensure data availability, exchange and quality.to ensure data availability, exchange and quality.
• Legal and policy guidance is needed to elaborate Legal and policy guidance is needed to elaborate specifications for access, to protect confidentiality, etcspecifications for access, to protect confidentiality, etc
• In Ethiopia, there is legislation providing the framework for In Ethiopia, there is legislation providing the framework for health information covering specific components, such as health information covering specific components, such as notifiable diseases, private sector data, confidentiality, notifiable diseases, private sector data, confidentiality, fundamental principles of official statistics, etc. With regard fundamental principles of official statistics, etc. With regard to vital statistics, starting from the 1960 Civil Code of to vital statistics, starting from the 1960 Civil Code of Ethiopia, the country has declared different legislations at Ethiopia, the country has declared different legislations at different times to implement the legal and official registration different times to implement the legal and official registration of births and deaths .However, no significant progress has of births and deaths .However, no significant progress has ever been made to put this in to action.ever been made to put this in to action.

• Currently, Ethiopia is in the stage of publicizing the Currently, Ethiopia is in the stage of publicizing the registration law, creating organizational and registration law, creating organizational and administrative structure and establishing local administrative structure and establishing local registration offices and training of registrars. registration offices and training of registrars. Ethiopia does not have a regular system for Ethiopia does not have a regular system for monitoring of the performance of HIS. The National monitoring of the performance of HIS. The National Advisory Committee (NAC) of the HMIS is in charge Advisory Committee (NAC) of the HMIS is in charge of coordinating the health information system of coordinating the health information system although it has a limited mandate and resource to although it has a limited mandate and resource to run the activity on a regular basis.run the activity on a regular basis.
• NAC was initially founded in 2005 with an NAC was initially founded in 2005 with an objective of assisting in the review of the existing objective of assisting in the review of the existing HMIS and M&E system, development of a HMIS and M&E system, development of a comprehensive HMIS and M&E strategy as an comprehensive HMIS and M&E strategy as an implementation tool for monitoring and evaluation of implementation tool for monitoring and evaluation of HSDP III and beyond.HSDP III and beyond.

Ethiopia has limited capacity in core health Ethiopia has limited capacity in core health information sciences to meet health information information sciences to meet health information needs. There is a functional central HIS unit in the needs. There is a functional central HIS unit in the Ministry of Health which plays a significant role in Ministry of Health which plays a significant role in coordinating, strengthening and maintaining the coordinating, strengthening and maintaining the national HIS, including the ongoing HMIS reform. national HIS, including the ongoing HMIS reform. However, it lacks adequate resources to effectively However, it lacks adequate resources to effectively maintain and upgrade the status of HIS to a level maintain and upgrade the status of HIS to a level that meets the health information requirements of that meets the health information requirements of the country. The problem progressively increases the country. The problem progressively increases as we move down to the Woreda health offices. To as we move down to the Woreda health offices. To make things worse, at all levels of the health make things worse, at all levels of the health system, the professional mix is poor and the attrition system, the professional mix is poor and the attrition rate is very high, which calls for major intervention rate is very high, which calls for major intervention in the area of HIS capacity building activities.in the area of HIS capacity building activities.
• 6.2.3. Health Information Related Initiatives6.2.3. Health Information Related Initiatives• The HMIS related initiatives are best understood in The HMIS related initiatives are best understood in
light of the overall objectives of the Health light of the overall objectives of the Health Management Information System, which are:Management Information System, which are:
• Develop and implement a comprehensive and Develop and implement a comprehensive and standardized national HMIS and ensure the use of standardized national HMIS and ensure the use of information for evidence based planning and information for evidence based planning and management of health services.management of health services.
• To review and strengthen the existing HMIS at To review and strengthen the existing HMIS at federal, regional, woreda, health facility and federal, regional, woreda, health facility and community levels and ensure use of health community levels and ensure use of health information for decision-making at all levels.information for decision-making at all levels.
• To achieve 80% completeness and timely To achieve 80% completeness and timely submission of routine health and administrative submission of routine health and administrative reports.reports.
• Achieve 75 % of evidence based planning.Achieve 75 % of evidence based planning.
• The strategy for implementation of HMIS The strategy for implementation of HMIS objectives is:objectives is:
• Institutionalize HMIS at all levels.Institutionalize HMIS at all levels.• Build capacity of health workers to analyze, Build capacity of health workers to analyze,
interpret and use health information for making interpret and use health information for making decisions.decisions.
• Introduce appropriate HMIS technology at all levels Introduce appropriate HMIS technology at all levels of the health system in collaboration with the of the health system in collaboration with the concerned bodies such as the National ICT concerned bodies such as the National ICT Authority.Authority.
• Define the minimum standard of inputs required for Define the minimum standard of inputs required for HMIS at different levels of the health system.HMIS at different levels of the health system.
• Initiate and sustain regular programme review and Initiate and sustain regular programme review and feedback system.feedback system.
• The breakdown of the plan is detailed according to The breakdown of the plan is detailed according to what activities are carried out by the various levels what activities are carried out by the various levels in the healthcare system. These being:in the healthcare system. These being:

• A) The key activities at the Woreda Health Offices level A) The key activities at the Woreda Health Offices level are:are:
• Establishment of HMIS posts and assignment of appropriate Establishment of HMIS posts and assignment of appropriate personnel in the organizational structure of woreda health personnel in the organizational structure of woreda health office and health institutions as per the national standard.office and health institutions as per the national standard.
• Determination of the qualification requirements, job Determination of the qualification requirements, job descriptions, career path, and incentive package standards descriptions, career path, and incentive package standards for personnel working on HMIS.for personnel working on HMIS.
• Ensure the proper reporting and feedback mechanism is laid Ensure the proper reporting and feedback mechanism is laid out beginning form the health extension workers to the HMIS out beginning form the health extension workers to the HMIS personnelpersonnel
• Provide the necessary health and administrative reports to Provide the necessary health and administrative reports to the RHBs as per the guideline.the RHBs as per the guideline.
• Allocate funds for HMIS and provide the necessary facilities Allocate funds for HMIS and provide the necessary facilities for the HMIS units/personnelfor the HMIS units/personnel
• Implement and monitor the pilot HMIS in collaboration with Implement and monitor the pilot HMIS in collaboration with the RHBs.the RHBs.
• Collaborate on the expansion of the geographic information Collaborate on the expansion of the geographic information system and woreda connectivity.system and woreda connectivity.

• B) Key Activities at the Regional Health Bureaus Level:B) Key Activities at the Regional Health Bureaus Level:• Adapt and implement qualification requirements, job Adapt and implement qualification requirements, job
descriptions, career path and incentive packages for descriptions, career path and incentive packages for personnel working on HMIS at different levels of the health personnel working on HMIS at different levels of the health system.system.
• Adapt and implement National HMIS Strategy, manuals and Adapt and implement National HMIS Strategy, manuals and standards developed at national level.standards developed at national level.
• Conduct regular on-the-job training to HMIS focal personnel, Conduct regular on-the-job training to HMIS focal personnel, programme managers and health workers.programme managers and health workers.
• Equip HMIS units at all levels.Equip HMIS units at all levels.• Implement HMIS on pilot basis in collaboration with the Implement HMIS on pilot basis in collaboration with the
FMOH.FMOH.• Collaborate on the establishment of electronic network from Collaborate on the establishment of electronic network from
federal to woreda level as part of implementation of HMIS.federal to woreda level as part of implementation of HMIS.• Initiate and sustain the development of Health and Health Initiate and sustain the development of Health and Health
Related Indicators in the regions.Related Indicators in the regions.• Advocate the allocation of adequate funds for implementation Advocate the allocation of adequate funds for implementation
of National HMIS in woredas.of National HMIS in woredas.

C) Key Activities at the Federal Ministry of Health C) Key Activities at the Federal Ministry of Health Level are:Level are:– Assign a multidisciplinary team at Planning and Assign a multidisciplinary team at Planning and
Programming Department /MOH and provide theProgramming Department /MOH and provide the– necessary facility so that it will be able to spearhead the necessary facility so that it will be able to spearhead the
development and implementation of HMIS at national development and implementation of HMIS at national level.level.
– Develop and popularize the National HMIS Strategy and Develop and popularize the National HMIS Strategy and user-friendly manuals.user-friendly manuals.
– Develop and popularize qualification requirements, job Develop and popularize qualification requirements, job descriptions, and career path and incentive packages for descriptions, and career path and incentive packages for personnel working on HMIS at different levels of the health personnel working on HMIS at different levels of the health system.system.
– Standardize HMIS indicators; harmonize the reporting Standardize HMIS indicators; harmonize the reporting system and collect gender disaggregated data.system and collect gender disaggregated data.
– Develop, adapt and implement HMIS user-friendly Develop, adapt and implement HMIS user-friendly guidelines and revise International Classification ofguidelines and revise International Classification of
– Disease ICD coding system.Disease ICD coding system.

– Initiate pre-service training on HMIS in health Initiate pre-service training on HMIS in health professional training institutions.professional training institutions.
– Implement HMIS on pilot basis before nationwide Implement HMIS on pilot basis before nationwide replication.replication.
– Conduct system analysis for the application of Conduct system analysis for the application of ICT to HMIS, pre test and implement the ICT to HMIS, pre test and implement the application andapplication and
– expand geographic information system.expand geographic information system.– Mobilize funds for implementation of National Mobilize funds for implementation of National
HMIS.HMIS.– Monitor the implementation of program review Monitor the implementation of program review
and research recommendations through HMIS.and research recommendations through HMIS.– Publish Health and Health Related Indictors Publish Health and Health Related Indictors
bulletin annually.bulletin annually.

UNIT VII: HEALTHCARE SERVICE PLANNINGUNIT VII: HEALTHCARE SERVICE PLANNING7.1.1 Introduction7.1.1 Introduction: definitions of key terms: definitions of key termsA) What Is Planning?A) What Is Planning?• A plan is defined as a map, a preparation, or as A plan is defined as a map, a preparation, or as
an arrangement. Planning defines where one wants an arrangement. Planning defines where one wants to go, how to get there and the timetable for the to go, how to get there and the timetable for the journey. Planning can also identify the journey’s journey. Planning can also identify the journey’s milestones. Complete planning sets out indicators milestones. Complete planning sets out indicators for tracking progress and ways to measure if the trip for tracking progress and ways to measure if the trip was worth the investment.was worth the investment.
• Planning is future oriented process of Planning is future oriented process of determining a direction, setting goals, and taking determining a direction, setting goals, and taking actions to reach those goals. Planning is all about actions to reach those goals. Planning is all about making changes and is basic management function making changes and is basic management function that is essential to the success of all levels of an that is essential to the success of all levels of an organization.organization.

B) What Is Health Planning?B) What Is Health Planning?
• Health planning is a process to produce Health planning is a process to produce health. It does this by creating an actionable health. It does this by creating an actionable link between needs and resources. Its nature link between needs and resources. Its nature and scope will depend upon the:and scope will depend upon the:
• Time allowableTime allowable
• Assessing needAssessing need
• Resources available to support the processResources available to support the process
• Broader political and social environment.Broader political and social environment.

7.1.2 Health Service Planning7.1.2 Health Service Planning
Healthcare service planning is a core activity of Healthcare service planning is a core activity of public health professionals and managers. It is not public health professionals and managers. It is not as such a linear process, but a continuous as such a linear process, but a continuous improvement process. It involves gathering data, improvement process. It involves gathering data, translating it into useful information, and using that translating it into useful information, and using that information to make decisions. A generalized model information to make decisions. A generalized model includes the following stages:includes the following stages:
• Needs assessmentNeeds assessment• setting goals and objectivessetting goals and objectives• developing interventionsdeveloping interventions• implementing the interventionsimplementing the interventions• evaluating the resultsevaluating the results

• Charting a course, navigating and keeping a travel log are all Charting a course, navigating and keeping a travel log are all parts of a good planning process. Broad elements of planning parts of a good planning process. Broad elements of planning are:are:
• identifying a vision and goalsidentifying a vision and goals• undertaking strategic planningundertaking strategic planning• evaluationevaluation• The Health Planning Process follows the same basic steps The Health Planning Process follows the same basic steps
any planning process follows. In the health planning process any planning process follows. In the health planning process the following factors must be taken into consideration in each the following factors must be taken into consideration in each planning cycle:planning cycle:
• the definition of what constitutes health, and what are the the definition of what constitutes health, and what are the new definition of society’s health goalsnew definition of society’s health goals
• integration of new technologies that are available to create, integration of new technologies that are available to create, restore, or support healthrestore, or support health
• emerging unforeseen health conditions (e.g. rapidly emerging unforeseen health conditions (e.g. rapidly spreading infectious diseases)spreading infectious diseases)
• changing economic conditionschanging economic conditions• correction of past oversightscorrection of past oversights

• The planning processThe planning process• The planning process has 7 basic steps, best depicted in The planning process has 7 basic steps, best depicted in
the following diagramthe following diagram• Step One: Surveying the Environment/Situation AnalysisStep One: Surveying the Environment/Situation Analysis• This often involves extensive information gathering to This often involves extensive information gathering to
determine the health or illness profiles and experiences of the determine the health or illness profiles and experiences of the population of interest. It is meant to identify the current state population of interest. It is meant to identify the current state of the issue under consideration.of the issue under consideration.
• Step Two: Setting Directions/Setting GoalsStep Two: Setting Directions/Setting Goals• This involves setting goals and objectives, and it also This involves setting goals and objectives, and it also
involves establishing the standards against which current involves establishing the standards against which current health/illness profiles, or current organizational or system health/illness profiles, or current organizational or system performance will be compared. This step is meant to identify performance will be compared. This step is meant to identify the desirable future state (expressed as outcomes if possible)the desirable future state (expressed as outcomes if possible)

• Step Three: Problems and ChallengesStep Three: Problems and Challenges• This involves identifying and quantifying the This involves identifying and quantifying the
difference between what is and what ought to difference between what is and what ought to be.be.
• Step Four: Range of SolutionsStep Four: Range of Solutions• This involves identifying the range of solutions This involves identifying the range of solutions
to each identified problem or challenge. This to each identified problem or challenge. This step should also include assessing each step should also include assessing each possible solution in terms of its feasibility, cost possible solution in terms of its feasibility, cost and effectiveness. So alternate solutions can and effectiveness. So alternate solutions can be compared with each other. This step often be compared with each other. This step often requires significant creativity, since no off-the-requires significant creativity, since no off-the-shelf solutions may be available for some shelf solutions may be available for some problems and challenges.problems and challenges.
• Step Five: Best Solution(s)Step Five: Best Solution(s)
• This step involves a choice of the solution, or This step involves a choice of the solution, or set of solutions, that should be implemented set of solutions, that should be implemented to address the problems or challenges to address the problems or challenges identified in step three. The choice may need identified in step three. The choice may need to take into account financial, political and to take into account financial, political and other limitations.other limitations.
• Step Six: ImplementationStep Six: Implementation
• This step involves implementation of the This step involves implementation of the chosen solutions, and often begins with chosen solutions, and often begins with development of an implementation plan.development of an implementation plan.
• Step Seven: EvaluationStep Seven: Evaluation• This step involves evaluation of the results of This step involves evaluation of the results of
implementation to determine whether the implementation to determine whether the implemented solutions are effective in achieving implemented solutions are effective in achieving their goals. It also involves evaluating the their goals. It also involves evaluating the environment to see if it has changed, thereby environment to see if it has changed, thereby rendering the solutions less effective, more effective rendering the solutions less effective, more effective or irrelevant. This step may begin with development or irrelevant. This step may begin with development of an evaluation plan well before evaluation actually of an evaluation plan well before evaluation actually takes place. It may also involve development of takes place. It may also involve development of ongoing monitoring methods to be used to ongoing monitoring methods to be used to continuously identify and assess the intended and continuously identify and assess the intended and unintended consequences of implementation unintended consequences of implementation actions.actions.
• 7.1.3 Strategies and Approaches used in Health Service 7.1.3 Strategies and Approaches used in Health Service PlanningPlanning
• There are various types of health planning, and the There are various types of health planning, and the approaches used are:approaches used are:
• Strategic planning and,Strategic planning and,• Operational planningOperational planning• A) Strategic PlanningA) Strategic Planning• A strategic planning process is used when there is a A strategic planning process is used when there is a
broad and open question to be answered, and many paths broad and open question to be answered, and many paths are on the table - for example, identifying the desired model are on the table - for example, identifying the desired model for delivery of children’s health services in rural settings and for delivery of children’s health services in rural settings and determining how to move to that model. Usually a strategic determining how to move to that model. Usually a strategic planning process assumes a new look at an issue, and an planning process assumes a new look at an issue, and an outcome that will take time to put in place but will exist for a outcome that will take time to put in place but will exist for a period longer than one funding cycle. Generally speaking it is period longer than one funding cycle. Generally speaking it is assumed that a strategic plan will need to be revised or assumed that a strategic plan will need to be revised or redone when the context in which the service exists changes redone when the context in which the service exists changes markedly. A change in context could relate to challenges to markedly. A change in context could relate to challenges to sustainability, opportunities to expand, or newly identified sustainability, opportunities to expand, or newly identified best practices that should be incorporated into the plan.best practices that should be incorporated into the plan.

• A basic guideline for planning is that a vision A basic guideline for planning is that a vision should be renewed every three to five years should be renewed every three to five years and the strategic directions emanating from and the strategic directions emanating from that vision also re-evaluated, perhaps yearly. that vision also re-evaluated, perhaps yearly. A strategic planning exercise will include:A strategic planning exercise will include:
• Strategic goals and directions,Strategic goals and directions,• Specific implementation or operational Specific implementation or operational
planning components.planning components.• For example in establishing a new local For example in establishing a new local
system of children’s health services, specific system of children’s health services, specific budgets, service expectations, timetables and budgets, service expectations, timetables and human resource models may be designed by human resource models may be designed by the strategic planning group, for hand-off to the strategic planning group, for hand-off to providers. In particular it outlines:providers. In particular it outlines:
– Priority issues in the health authorityPriority issues in the health authority– Critical challenges to population health and service Critical challenges to population health and service
delivery in the regiondelivery in the region– Goals and strategic themes that will guide service deliveryGoals and strategic themes that will guide service delivery– Strategic directions by sector and by geographic area.Strategic directions by sector and by geographic area.
• Within any strategic planning exercise, the following Within any strategic planning exercise, the following activities will occur:activities will occur:
• A visioning exerciseA visioning exercise• Creating mission and goalsCreating mission and goals• Establishing objectivesEstablishing objectives• Establishing strategic directionsEstablishing strategic directions• Developing a framework to establish and monitor Developing a framework to establish and monitor
success – a balanced scorecard approach for success – a balanced scorecard approach for instanceinstance
• Creating an implementation plan/timetableCreating an implementation plan/timetable

• Although originally developed for the corporate Although originally developed for the corporate sector, the balanced scorecard has become popular sector, the balanced scorecard has become popular within the health sector as a tool for both planning within the health sector as a tool for both planning and monitoring.and monitoring.
• Strategic planning processes should be supported Strategic planning processes should be supported by:by:
• Use of data, both quantitative and qualitativeUse of data, both quantitative and qualitative• Consultation with stakeholders (related to all parts Consultation with stakeholders (related to all parts
of the process, from visioning to data interpretation of the process, from visioning to data interpretation and crafting recommendations)and crafting recommendations)
• Application of project management and facilitation Application of project management and facilitation tools, which may include activities such as SWOT tools, which may include activities such as SWOT (strengths, weaknesses, opportunities and threats) (strengths, weaknesses, opportunities and threats) analysis, mind-mapping and strategic alignment analysis, mind-mapping and strategic alignment modelsmodels
• Monitoring and evaluation protocols.Monitoring and evaluation protocols.

• The best tools for strategic planning are often the The best tools for strategic planning are often the ones that the person leading the planning is most ones that the person leading the planning is most familiar with and has used successfully in previous familiar with and has used successfully in previous initiatives. One of the tools commonly used is initiatives. One of the tools commonly used is SWOT analysisSWOT analysis
SWOT Analysis:SWOT Analysis:• This is an outline of strengths, weaknesses, This is an outline of strengths, weaknesses,
opportunities of, and threats to, the organization. It opportunities of, and threats to, the organization. It is usually done at the start of a strategic planning is usually done at the start of a strategic planning exercise in a group setting to identify all factors in exercise in a group setting to identify all factors in each area.each area.
• The factors are usually organized in a table of four The factors are usually organized in a table of four quadrants so participants in the planning exercise quadrants so participants in the planning exercise can visually (and easily) see the context for the can visually (and easily) see the context for the planning.planning.

• Strengths: include factors like staff Strengths: include factors like staff capabilities, effective management capabilities, effective management processes, competitive advantage and processes, competitive advantage and unique programs or products.unique programs or products.
• Weaknesses: include factors like gaps in staff Weaknesses: include factors like gaps in staff skills, financial problems and inadequate skills, financial problems and inadequate information systems.information systems.
• Opportunities: include factors like global Opportunities: include factors like global influences, new policy developments, influences, new policy developments, partnerships and research.partnerships and research.
• Threats: include factors like market demand, Threats: include factors like market demand, loss of key staff and political effects, illiteracy, loss of key staff and political effects, illiteracy, poverty, weak intersectoral collaborationpoverty, weak intersectoral collaboration

B) Operational PlanningB) Operational Planning• An operational planning process starts from a point An operational planning process starts from a point
of a specific objective, for example to increase the of a specific objective, for example to increase the number of clients served at the Health Posts, and number of clients served at the Health Posts, and focuses on the range of opportunities within that focuses on the range of opportunities within that delivery framework.delivery framework.
• Operational planning will include:Operational planning will include:• Statement of purpose/deliverables/target to be Statement of purpose/deliverables/target to be
achieved/success indicatorsachieved/success indicators• Use of available and relevant data and informationUse of available and relevant data and information• Stakeholder engagement (who needs to fund, Stakeholder engagement (who needs to fund,
deliver expanded services?)deliver expanded services?)• Selection of priority action approach (new program Selection of priority action approach (new program
design)design)• Development of an implementation timetable and Development of an implementation timetable and
budget.budget.

• Operational planning processes may be supported Operational planning processes may be supported by activities or tools similar to those for strategic by activities or tools similar to those for strategic planning but with a tighter question applied to these planning but with a tighter question applied to these activities. Included in operational planning could be activities. Included in operational planning could be use of an activity hierarchy model and a program use of an activity hierarchy model and a program logic model. A tool commonly used is a Logic logic model. A tool commonly used is a Logic Model.Model.
• This model creates a diagram of the program and This model creates a diagram of the program and allows the effects of a proposed change to be allows the effects of a proposed change to be determined. It is very helpful for program planning determined. It is very helpful for program planning and implementation monitoring. A logic model and implementation monitoring. A logic model depicts action by describing what the program is depicts action by describing what the program is and what it will do – the sequence of events that and what it will do – the sequence of events that links program investments to results. The model has links program investments to results. The model has the following six components:the following six components:
• Situation: Problem or issue that the program is to Situation: Problem or issue that the program is to address sits within a setting or situation from which address sits within a setting or situation from which priorities are setpriorities are set
• Inputs: resources, contributions and investments Inputs: resources, contributions and investments that are made in response to the situation. Inputs that are made in response to the situation. Inputs lead to outputlead to output
• Outputs: activities, services, events, and products Outputs: activities, services, events, and products that reach people and users. Outputs lead to that reach people and users. Outputs lead to outcomeoutcome
• Outcomes: results or changes for individuals, Outcomes: results or changes for individuals, groups, agencies, communities or systemsgroups, agencies, communities or systems
• Assumptions: beliefs we have about the program, Assumptions: beliefs we have about the program, the people, the environment and the way we think the people, the environment and the way we think the program is going to workthe program is going to work
• External factors: environment in which the program External factors: environment in which the program exists includes a variety of external factors that exists includes a variety of external factors that interact with and influence the program action.interact with and influence the program action.
7.2: Resource Identification7.2: Resource Identification1. At the end of this lesson the learners should 1. At the end of this lesson the learners should
be able to identify information systems to be be able to identify information systems to be used for resource identificationused for resource identification
7.2.1. Introduction to Classification (and 7.2.1. Introduction to Classification (and Identification) of ResourceIdentification) of Resource
• In the planning process resource In the planning process resource identification is one of the critical success identification is one of the critical success factors. Resources can be classified as:factors. Resources can be classified as:
• FacilitiesFacilities• EquipmentEquipment• Human resourceHuman resource• Finance/fundsFinance/funds

• The commonly cited resources are the three The commonly cited resources are the three Ms and a T, that is,Ms and a T, that is,
• MoneyMoney• MaterialsMaterials• Manpower (human power)Manpower (human power)• TimeTime• When assessing and identify resources the When assessing and identify resources the
use of information systems becomes crucial. use of information systems becomes crucial. The commonly used information systems are:The commonly used information systems are:– Human Resource Information System (HRIS)Human Resource Information System (HRIS)– Logistics Management Information System (LMIS)Logistics Management Information System (LMIS)– Financial Management Information System Financial Management Information System
(FMIS)(FMIS)

A) HRIS (Human Resources Information Systems)A) HRIS (Human Resources Information Systems)• Human Resources Management (HRM) is the Human Resources Management (HRM) is the
attraction, selection, retention, development, and attraction, selection, retention, development, and utilization of labor resource in order to achieve both utilization of labor resource in order to achieve both individual and organizational objectives. HRIS is an individual and organizational objectives. HRIS is an integration of HRM and Information Systems (IS). integration of HRM and Information Systems (IS). HRIS helps HR managers perform HR functions in a HRIS helps HR managers perform HR functions in a more effective and systematic way using more effective and systematic way using technology. It is the system used to acquire, store, technology. It is the system used to acquire, store, manipulate, analyze, retrieve, and distribute manipulate, analyze, retrieve, and distribute pertinent information regarding an organization’s pertinent information regarding an organization’s human resources.human resources.
• A strong human resources information system gives A strong human resources information system gives health care leaders the data they need to quickly health care leaders the data they need to quickly answer the key policy and management questions answer the key policy and management questions affecting healthcare service delivery. HRIS affecting healthcare service delivery. HRIS strengthening process includes:strengthening process includes:
• Building local HRIS leadershipBuilding local HRIS leadership• Strengthening infrastructureStrengthening infrastructure• Developing HRIS software solutionsDeveloping HRIS software solutions• Effectively using and analyzing dataEffectively using and analyzing data• Ensuring that users can support and improve the Ensuring that users can support and improve the
system themselves.system themselves.Benefits of HRIS:Benefits of HRIS:• HRIS has showed many benefits to the HR HRIS has showed many benefits to the HR
operations. A few of them can be detailed as:operations. A few of them can be detailed as:• Faster information process,Faster information process,• Greater information accuracy,Greater information accuracy,• Improved planning and program developmentImproved planning and program development• Enhanced employee communicationsEnhanced employee communications
B) LMIS (Logistics Management Information B) LMIS (Logistics Management Information System)System)
• Designing an effective and sustainable supply Designing an effective and sustainable supply chain system for drugs and other commodities chain system for drugs and other commodities is important and can be complex. A correctly is important and can be complex. A correctly run distribution system should also keep run distribution system should also keep drugs in good condition, rationalize drug drugs in good condition, rationalize drug storage points, use transport as efficiently as storage points, use transport as efficiently as possible, reduce theft and fraud and provide possible, reduce theft and fraud and provide information for forecasting needs. This information for forecasting needs. This requires a good management of the system requires a good management of the system along with a simple but well-designed along with a simple but well-designed information system in place.information system in place.

C) FMIS (Finance and Materials Management C) FMIS (Finance and Materials Management Information Systems)Information Systems)
• Finance and Materials Management Finance and Materials Management Information Systems (FMIS) comprises of Information Systems (FMIS) comprises of applications that support core health agency applications that support core health agency financial management, including general financial management, including general ledger, assets and materials management.ledger, assets and materials management.
• FMIS will modernize and standardize FMIS will modernize and standardize business processes and reporting associated business processes and reporting associated with finance and materials management. with finance and materials management. FMIS will provide health agencies with robust FMIS will provide health agencies with robust and capable, industry standard tools that will and capable, industry standard tools that will appropriately support the management of appropriately support the management of complex health agency settingscomplex health agency settings

The core functionality of FMIS includes:The core functionality of FMIS includes:• General ledgerGeneral ledger• BudgetingBudgeting• Accounts payableAccounts payable• Accounts receivableAccounts receivable• Trust accountingTrust accounting• Assets managementAssets management• Equipment hireEquipment hire• Materials managementMaterials management• ProcurementProcurement• Cash receiptingCash receipting• On-line invoice submissionOn-line invoice submission• ExpensesExpenses

The benefits of FMIS are:The benefits of FMIS are:
• Additional control over expenditure - enforce Additional control over expenditure - enforce financial delegationsfinancial delegations
• Substantial cleanup of supplier dataSubstantial cleanup of supplier data
• Online procurement - timely, increased controlOnline procurement - timely, increased control
• Move to EFT payment and cheque printingMove to EFT payment and cheque printing
• Flexibility of reportingFlexibility of reporting
• Stock managementStock management
• Workflow support and controls.Workflow support and controls.

• A) GlossaryA) Glossary• Accreditation:Accreditation: to certify that an individual, to certify that an individual,
organization, educational institution, etc., organization, educational institution, etc., meets and maintains suitable standards.meets and maintains suitable standards.
• Allied health professionalAllied health professional: a person who is : a person who is not a physician, nurse, or pharmacist, and not a physician, nurse, or pharmacist, and who works in the health field. An allied health who works in the health field. An allied health professional may, for example, be a dietitian, professional may, for example, be a dietitian, an emergency medical technician, or an aidean emergency medical technician, or an aide
• Ambulatory care:Ambulatory care: medical services that may medical services that may include diagnosis, treatment, and include diagnosis, treatment, and rehabilitation, that are provided on an rehabilitation, that are provided on an outpatient (nonhospitalized) basis.outpatient (nonhospitalized) basis.

• Ancillary servicesAncillary services: Hospital services other than room and : Hospital services other than room and boardboard
• Business Process Reengineering (BPRBusiness Process Reengineering (BPR): a fundamental ): a fundamental rethinking and radical redesign of business processes to rethinking and radical redesign of business processes to achieve dramatic improvements in critical contemporary achieve dramatic improvements in critical contemporary measures of performance such as cost, quality service, and measures of performance such as cost, quality service, and speed. Also known as Business Process Improvementspeed. Also known as Business Process Improvement
• Catchments area:Catchments area: the geographical area from which a the geographical area from which a school takes its students, or the area from which a hospital school takes its students, or the area from which a hospital services its patientsservices its patients
• Elective SurgeryElective Surgery: surgery that is subject to choice (election). : surgery that is subject to choice (election). The patient or doctor may make the choice.The patient or doctor may make the choice.
• Emergency roomEmergency room: a part of a hospital that takes care of sick : a part of a hospital that takes care of sick or injured people who need immediate attentionor injured people who need immediate attention

• Equity in healthEquity in health: is the absence of systematic disparities in : is the absence of systematic disparities in health (or in the major social determinants of health) health (or in the major social determinants of health) between social groups who have different levels of between social groups who have different levels of underlying social advantage/disadvantage—that is, different underlying social advantage/disadvantage—that is, different positions in a social hierarchy.positions in a social hierarchy.
• Goal:Goal: a broad statement describing a desired future a broad statement describing a desired future condition or achievement without being specific about how condition or achievement without being specific about how much and when.much and when.
• Health education:Health education: education that increases the awareness education that increases the awareness and favorably influences the attitudes and knowledge and favorably influences the attitudes and knowledge relating to the improvement of health on a personal or relating to the improvement of health on a personal or community basiscommunity basis
• Health PolicyHealth Policy: is a legal document which contains decisions : is a legal document which contains decisions usually developed by government policy makers for usually developed by government policy makers for determining present and future objectives pertaining to the determining present and future objectives pertaining to the healthcare system.healthcare system.
• Health postHealth post: one of the satellite facilities in the Primary : one of the satellite facilities in the Primary Health Care UnitHealth Care Unit

Health stationsHealth stations: the smallest health units in the : the smallest health units in the conventional Health Service structure and are conventional Health Service structure and are staffed with 1-3 health assistants.staffed with 1-3 health assistants.
HealthHealth: is a state of physical, mental and social well-: is a state of physical, mental and social well-being. It involves more than just the absence of being. It involves more than just the absence of disease or infirmity. This definition was ratified disease or infirmity. This definition was ratified during the first World Health Assembly and has not during the first World Health Assembly and has not been modified since 1948.been modified since 1948.
Healthcare delivery system: aHealthcare delivery system: a term without specific term without specific definition, referring to all the facilities and services, definition, referring to all the facilities and services, along with methods for financing them, through along with methods for financing them, through which health care is provided to the population.which health care is provided to the population.
HealthcareHealthcare: the prevention, treatment, and : the prevention, treatment, and management of illness and the preservation of management of illness and the preservation of mental and physical well-being through the services mental and physical well-being through the services offered by the medical and allied health professions.offered by the medical and allied health professions.

• According to the World Health Organization, health According to the World Health Organization, health care embraces all the goods and services designed care embraces all the goods and services designed to promote health, including “preventive, curative to promote health, including “preventive, curative and palliative interventions, whether directed to and palliative interventions, whether directed to individuals or to populations”individuals or to populations”
• Higher clinicHigher clinic: staffed at least by a general medical : staffed at least by a general medical practitioner, a specialist and assisted by various practitioner, a specialist and assisted by various specialists serve for general outpatient clinics. For specialists serve for general outpatient clinics. For emergency and delivery this clinic has up to 5 beds.emergency and delivery this clinic has up to 5 beds.
• HospitalHospital: an establishment with at least 25 beds : an establishment with at least 25 beds that provides general medical care round the clock. that provides general medical care round the clock. It is at least equipped with basic laboratory, X-ray It is at least equipped with basic laboratory, X-ray and basic treatment facilities. It is staffed with at and basic treatment facilities. It is staffed with at least one medical practitioner.least one medical practitioner.

• HouseholdHousehold: a single person living alone or a group : a single person living alone or a group voluntarily living together, having common housekeeping voluntarily living together, having common housekeeping arrangements for supplying basic living needs, such as arrangements for supplying basic living needs, such as principal meals. The group may consist of related or principal meals. The group may consist of related or unrelated persons.unrelated persons.
• IndicatorsIndicators: established measures used to determine how : established measures used to determine how well an organization is meeting its customers’ needs as well well an organization is meeting its customers’ needs as well as other operational and financial performance expectations.as other operational and financial performance expectations.
• Infant mortality rate (IMR): the ratio of the number of deaths Infant mortality rate (IMR): the ratio of the number of deaths under one year of age occurring in a given year to the under one year of age occurring in a given year to the number of births in the same year. Also used in a more number of births in the same year. Also used in a more rigorous sense to mean the number of deaths that would rigorous sense to mean the number of deaths that would occur under one year of age in a life table with a radix of occur under one year of age in a life table with a radix of 1,000.1,000.
• Infant mortality: the probability of dying between birth and Infant mortality: the probability of dying between birth and age one per 1000 live births in a given year.age one per 1000 live births in a given year.

• InformaticsInformatics: an emerging term that is used : an emerging term that is used to cover information along with its to cover information along with its management, particularly by computer. management, particularly by computer. Usually the field involved is used along with Usually the field involved is used along with “informatics”, e.g., “medical informatics.”“informatics”, e.g., “medical informatics.”
• Inpatient admission: admission to an Inpatient admission: admission to an institution that provides lodging and institution that provides lodging and continuous nursing services.continuous nursing services.
• In-patientIn-patient: a patient who is admitted and : a patient who is admitted and occupies bed in a health institution for occupies bed in a health institution for diagnosis and/or treatment.diagnosis and/or treatment.

• LeprosariumLeprosarium: leprosy hospital, a hospital for : leprosy hospital, a hospital for the treatment of patients with leprosythe treatment of patients with leprosy
• LicensureLicensure: the state or condition of having a : the state or condition of having a license granted by official or legal authority to license granted by official or legal authority to perform medical acts and procedures not perform medical acts and procedures not permitted by persons without such a license. permitted by persons without such a license. It is also the approval of a drug or medical It is also the approval of a drug or medical procedure by official or legal authority for use procedure by official or legal authority for use in the practice of medicine.in the practice of medicine.
• Life Expectancy at Birth: the average number Life Expectancy at Birth: the average number of years a newborn infant can expect to live of years a newborn infant can expect to live under current mortality levels.under current mortality levels.
• Live birthLive birth: the complete expulsion or extraction : the complete expulsion or extraction from its mother of conception, irrespective of the from its mother of conception, irrespective of the duration of pregnancy, which after such separation duration of pregnancy, which after such separation shows any evidence of life.shows any evidence of life.
• Lower clinicLower clinic: Staffed at least by a health assistant : Staffed at least by a health assistant or a nurse and serve for general outpatient clinic.or a nurse and serve for general outpatient clinic.
• Maternal mortality rate (MMR): a measure of a Maternal mortality rate (MMR): a measure of a woman’s risk of dying from causes associated with woman’s risk of dying from causes associated with pregnancy.pregnancy.
• Medium ClinicMedium Clinic: staffed at least by health officer or : staffed at least by health officer or general medical practitioner and serve for general general medical practitioner and serve for general medical services.medical services.

• MorbidityMorbidity: the extent of illness, injury or disability in : the extent of illness, injury or disability in a population.a population.
• OrganizationOrganization: a collection of people working : a collection of people working together in a planned deliberate social structure to together in a planned deliberate social structure to achieve a common goal.achieve a common goal.
• Organizational StructureOrganizational Structure: the structure and/or : the structure and/or hierarchy of an organization and how its component hierarchy of an organization and how its component parts work together to achieve common goals.parts work together to achieve common goals.
• Out-patientOut-patient: a patient who receive ambulatory care : a patient who receive ambulatory care (examination and treatment) without being admitted (examination and treatment) without being admitted or occupying a bed.or occupying a bed.
• Postnatal visitsPostnatal visits: women attended, at least once : women attended, at least once during postpartum (42 days after delivery), by during postpartum (42 days after delivery), by health professional including HEW’s for reasons health professional including HEW’s for reasons relating to post partum.relating to post partum.
• Potential health service coveragePotential health service coverage: the : the population covered in percentage based on population covered in percentage based on the existing health centers and health stations the existing health centers and health stations in catchments’ area.in catchments’ area.
• ProcessProcess: what happens between the start : what happens between the start and end points. It includes all the activities and end points. It includes all the activities performed by each department, group, or performed by each department, group, or person who are involved in the process. person who are involved in the process. Activities are the major “works” that transform Activities are the major “works” that transform an input into an outputan input into an output

• Public healthPublic health: is the science and art of preventing : is the science and art of preventing disease, prolonging life and promoting health disease, prolonging life and promoting health through the organized efforts and informed choices through the organized efforts and informed choices of society, organizations, public and private, of society, organizations, public and private, communities and individuals. It is concerned with communities and individuals. It is concerned with threats to the overall health of a community based threats to the overall health of a community based on population health analysis. The population in on population health analysis. The population in question can be as small as a handful of people or question can be as small as a handful of people or as large as all the inhabitants of several continents. as large as all the inhabitants of several continents. Public health is also a branch of preventive Public health is also a branch of preventive medicine, a medical specialty. Specialization in medicine, a medical specialty. Specialization in public health also occurs in nursing, nutrition, law, public health also occurs in nursing, nutrition, law, and other disciplines.and other disciplines.
• Rate of national increase: the difference between Rate of national increase: the difference between the births and deaths occurring during a given the births and deaths occurring during a given period divided by the number person-year lived by period divided by the number person-year lived by the population duringthe population during
• Risk BehaviorRisk Behavior: engaging in behavior that is harmful : engaging in behavior that is harmful or dangerous to oneselfor dangerous to oneself
• Strategic PlanningStrategic Planning: the process by which an : the process by which an organizations, public health or otherwise, envisions organizations, public health or otherwise, envisions its future and develops strategies, goals, objectives, its future and develops strategies, goals, objectives, and action plans to achieve that future.and action plans to achieve that future.
• System: a completely functioning process System: a completely functioning process dependent upon many parts to create results where dependent upon many parts to create results where each part has a central purpose that is linked to the each part has a central purpose that is linked to the global goal of the entire system and achievement of global goal of the entire system and achievement of that goal is contingent upon the interaction of the that goal is contingent upon the interaction of the parts.parts.
• Total fertility rate (TFRTotal fertility rate (TFR): the average number of ): the average number of children that would be born per woman of all women children that would be born per woman of all women lived to end of their childbearing years and born lived to end of their childbearing years and born children according to a given set of age specific children according to a given set of age specific fertility rates.fertility rates.

• Under-five mortalityUnder-five mortality: the probability of dying : the probability of dying between birth and age five per 1000 live births in a between birth and age five per 1000 live births in a given year.given year.
• Vital eventsVital events: births, deaths, marriages and : births, deaths, marriages and divorcesdivorces
• B) Business Process Reengineering (BPR) B) Business Process Reengineering (BPR) CORNER PAGECORNER PAGE
• BPR – about FMOHBPR – about FMOH• The Government of Federal Democratic Republic of The Government of Federal Democratic Republic of
Ethiopia has embarked country wide reform Ethiopia has embarked country wide reform initiative aimed at bringing effectiveness and initiative aimed at bringing effectiveness and efficiency in the execution of business practices to efficiency in the execution of business practices to achieve dramatic improvement in critical, achieve dramatic improvement in critical, contemporary measures of performance such as contemporary measures of performance such as cost, quality, service and speed.cost, quality, service and speed.

In line with this, the Federal Ministry of Health In line with this, the Federal Ministry of Health (FMoH) and agencies under the Ministry have (FMoH) and agencies under the Ministry have made strong commitment to fundamentally made strong commitment to fundamentally rethink, radically redesign and fully rethink, radically redesign and fully decentralize the health care, health decentralize the health care, health professionals, health facilities and health professionals, health facilities and health related products regulatory systems with the related products regulatory systems with the intension of satisfying customers/stakeholders intension of satisfying customers/stakeholders needs and expectations and to fulfil sectoral needs and expectations and to fulfil sectoral visions/missions.visions/missions.

The BPR principles are:The BPR principles are:• Organize around outcome not function and Organize around outcome not function and
departmentsdepartments• Provide a single point of contact for customers and Provide a single point of contact for customers and
supplierssuppliers• Bring downstream information upstreamBring downstream information upstream• Capture information once at the source and share it Capture information once at the source and share it
widelywidely• Substitute parallel for sequential processSubstitute parallel for sequential process• Maintain a continuous flow of the main sequenceMaintain a continuous flow of the main sequence• Identify and eliminate non-value adding stepsIdentify and eliminate non-value adding steps• Use triage, not a one-size-fits-all strategyUse triage, not a one-size-fits-all strategy

Based on these principles, the FMoH has Based on these principles, the FMoH has made extensive analysis of the current made extensive analysis of the current work activities, health care practices and work activities, health care practices and overall organizational structure in order to overall organizational structure in order to identify its strengths, weaknesses, identify its strengths, weaknesses, opportunities, and threats. Consequently, opportunities, and threats. Consequently, various departmental functions have various departmental functions have been merged and/or categorized under 8 been merged and/or categorized under 8 core processes and 4 support processes.core processes and 4 support processes.

• The core processes are:The core processes are:• Health Care DeliveryHealth Care Delivery
• Policy, Planning & Monitoring and Policy, Planning & Monitoring and EvaluationEvaluation
• Health Infrastructure Expansion and Health Infrastructure Expansion and RehabilitationRehabilitation
• Financial Resource Mobilization and Health Financial Resource Mobilization and Health InsuranceInsurance
• Research and Technology TransferResearch and Technology Transfer
• Public Health Emergency ManagementPublic Health Emergency Management
• Pharmaceutical Fund and Supply Pharmaceutical Fund and Supply ManagementManagement
• Health and Health Related Regulatory Health and Health Related Regulatory ServicesServices

The support processes are:The support processes are:• Human Resource ManagementHuman Resource Management
• Finance and ProcurementFinance and Procurement
• Legal OfficeLegal Office
• Public RelationPublic Relation


