preschool screening for social and emotional …ceica.cognitrom.ro/files/file/screening-ul...
TRANSCRIPT

Cognition, Brain, Behavior. An Interdisciplinary Journal Copyright © 2009 Romanian Association for Cognitive Science. All rights reserved. ISSN: 1224-8398 Volume XIII, No. 2 (June), 121-146
PRESCHOOL SCREENING FOR SOCIAL AND EMOTIONAL COMPETENCIES –
DEVELOPMENT AND PSYCHOMETRIC PROPERTIES
Catrinel A. ŞTEFAN * 1 , Anca BĂLAJ2, Mihaela PORUMB2, Monica ALBU2, Mircea MICLEA1, 2
1 Department of Psychology, Babeş-Bolyai University, Cluj-Napoca, Romania 2 Cognitrom, LTD, Cluj-Napoca, Romania
ABSTRACT Age-appropriate screening for preschool children is important for early detection of developmental delays. Emotional and social competencies have been established as predictors of mental health, as well as school readiness. We developed two screening scales, for parents and teachers corresponding to three age groups: 2.5-4 years-old, 4-5 years-old, and 5-7.5 years-old respectively. Approximately 150 children from each age group took part in this study. The statistical analysis showed that the internal consistency (α-Cronbach) was high with values over 0.80. Likewise, the test-retest coefficients (after 3 months) indicated values over 0.70. For the assessment of the content validity we correlated the screening scores with Social Skills Rating System (SSRS). We also established the concurrent and predictive validity with measurements of behavior problems (internalizing and externalizing disorders) and school performance. All the above mentioned data show that these screening scales are relevant for predicting children’s mental health problems and school readiness. KEYWORDS: screening, preschool, emotional and social competence, school
readiness, behavior problems.
* Corresponding author: E-mail: [email protected]

C. A. Ştefan, A. Bălaj, M. Porumb, M. Albu, M. Miclea
Cognition, Brain, Behavior. An Interdisciplinary Journal 13 (2009) 121-146
122
An increasingly important trend in the assessment of preschool children is the emphasis placed on developing screening instruments. Screening is a rapid, low-cost evaluation method, which allows gathering information about the need for in-depth assessment (Squires, Pottersi, & Bricker, 1999, as cited in Denham, 2003). Screening, as opposed to diagnosis instruments, is used for determining children’s risk status, not for identifying specific disorders (Gredler, 1997; Pianta & McCoy, 1997). In other words, screening is a preliminary step in diagnosis. Those children identified to be at risk undergo further testing in order to establish diagnosis (Hill, Lochman, Coie, Greenberg, & The Conduct Problems Prevention Research Group, 2004; Korkman, Jaakkola, Pesonen, & Turunen, 2004). The assessment of mental health and school adjustment predictors are important for a few reasons: 1) identifying children who lack age-appropriate skills (at risk children); 2) obtaining relevant information for diagnosis; 3) developing individualized preventive interventions; and 4) evaluating prevention programs for children within this age group (Barry & Lochman, 2003).
According to the latest statistical data in the U.S., up to 10% of preschool children may suffer from symptoms of mental health problems, which could develop in time into a mental health disorder (Health Resources and Services Administration, 2007). About 50% of the children who develop emotional and behavioral problems are likely to drop out from school (HRSA, 2007). Moreover, recent research emphasized that abilities related to school performance develop during the preschool period and manifest a continuous evolution. About 80% of the variance of the school performance at the end of 4th grade could be predicted at the beginning of the first school year [(U.S. Department of Education Early Childhood Longitudinal Study (ECLS), as cited in Ionescu & Benga, 2006], a fact which shows how important is to determine by assessment, during the preschool period, a child’s ability to adapt to school demands. Furthermore, it is obvious that early detection and intervention on a child’s disability reduces social and economic costs in a significant manner, and increases the efficacy of the intervention.
Taking into account these data, it becomes clear that monitoring children’s developmental trend by systematic assessment and early intervention, may have positive long-term effects for their mental health as well as for school adjustment. Caveats in preschool screening practices Preschool children’s screening is not yet a widely used assessment method. Specifically, in Romania, there is a complete lack of screening tools and most decisions about children’s school readiness are made by parents relying on common sense rather than on a rigorous assessment of their child’s abilities. The same lack of systematic assessment can be encountered in the case of referrals for mental health problems. Many children are deprived of early intervention because most of these problems remain undiagnosed, and sometimes, they become of concern only when children are unable to adapt to school requirements and

C. A. Ştefan, A. Bălaj, M. Porumb, M. Albu, M. Miclea
Cognition, Brain, Behavior. An Interdisciplinary Journal 13 (2009) 121-146
123
teachers complain about their behavior. Besides the need for screening instruments in Romania, there are some shortcomings of existing screenings which shall be discussed below.
Screening instruments have been criticized for lacking appropriate psychometric properties, and most importantly for their low ability in predicting child academic and mental health outcomes (Gredler, 1997). A number of meta-analytical reviews have found mixed data on the screening measurements’ predictive validity, generally covering up to 36% of the variance in child outcomes (Carlton & Winsler, 1999; La Paro & Pianta, 2001). These findings encourage mistrust regarding the use of such instruments to delay kindergarten entry (Datar, 2006; Downer & Pianta, 2006; Mantzicopoulos & Neuharth-Prittchett, 1998). Studies on school readiness have consistently shown that children identified as “unready”, i. e., lacking necessary abilities to adapt to school demands, made minimum gains in their acquired competencies after spending an additional year in preschool. Moreover, studies have consistently failed to show that children benefited from later enrollment, and even suggested that in some cases these practices are associated with increased risk for behavioral problems (Bryd, Weitzman, & Auinger, 1997). In the case of the Romanian education system there are no evaluation methods that guide later enrollment. Usually parents make a decision when their children are 6, whether they should spend another year in preschool or go to school. In either case, children are expected to perform well based on their attendance of preschool activities. In both cases, screening instruments should be taken into consideration foremost as means of detecting early signs of problems and as a basis for proceeding in preventive interventions (Barry & Lochman, 2003).
A key element of developing adequate screening instruments is choosing the best predictor for academic achievement. A widely accepted view was that cognitive abilities are the best predictors for academic performance (Snow, 2006). Recent research on school readiness reflected that both emotional and social competencies mediate between cognitive abilities and academic performance (Trentacosta & Izard, 2007). That is, at similar levels of cognitive abilities children with well-developed emotional and social competencies are more likely to perform well in most tasks related to academic performance. Although these are well known facts, social competence measures have been less used in screening research although they are in fact an important source for delaying school enrollment, as well as referrals for mental health problems (Crooks & Peters, 2005; Linares, Rosbruch, Stern, Edwards, Walker, Abikoff et al., 2005). Also, as emotional competence is positively correlated with children’s social competencies (Denham, Mason, Caverly, Schmidt, Hackney, Caswell, et al., 2001; Halberstadt, Denham, & Dunsmore, 2001), screening for both of these abilities is important for detecting children at risk. Moreover, most of the assessment instruments do not treat emotional and social competencies as different constructs, but rather as an umbrella concept for social-emotional competence.

C. A. Ştefan, A. Bălaj, M. Porumb, M. Albu, M. Miclea
Cognition, Brain, Behavior. An Interdisciplinary Journal 13 (2009) 121-146
124
Another issue is associated with the type of measured school outcome. The most commonly used criterion are standardized tests, often exhibiting low to moderate correlations with screening measurements (Tramontana, Hooper, & Selzer, 1988). Another set of outcome measurements is represented by the nontest type, i.e., school grades, teacher ratings of academic achievement or referrals for special education services (McCoy & Pianta, 1997; Strong Scott & Delgado, 2003). These recent trends place a greater emphasis on identifying ecologically valid means of measuring academic performance in children. Achievement on standardized tests can be constrained to performance in a particular moment and may not accurately reflect children’s abilities, while average grades or teacher ratings take into account their behavior over longer periods of time and allow inter-individual comparisons.
Screening instruments should take into account a multi-rater perspective. Several instruments for young children have different versions for teachers and parents (Gresham & Elliott, 1990; Kotler & McMahon, 2002). It is believed that parents and teachers have access to different perspectives on children’s behavior (Achenbach, Dumenci, & Rescorla, 2003), both critical in drawing accurate conclusions. Teachers have the opportunity of observing the children in classrooms and are able to identify a wide range of behavioral, emotional, and learning-related problems in the context of comparisons between children, while parents observe their children in daily interactions in the household (Huffman & Nichols, 2004). Models using a multi-informant perspective have proven better predictors of children’s academic difficulties (Crooks & Peters, 2005).
Frequently, children’s unstable behavior patterns represent a challenge in testing young participants. Some researchers certified that many of the problems exhibited at a certain age may be ephemeral. Poor motor performance (Huffman & Nichols, 2004) or low social skills (Arsenio, Cooperman, & Lover, 2003) at the age of 3 may only reflect a temporary delay in a certain skill acquisition, not a school readiness problem. A way to control this problem is by developing a continuous and flexible assessment tool, sensitive to changes over time (Hirsh-Pasek, Kochanoff, Newcombe, & de Villiers, 2005). As a consequence, we developed three sets of screening items for each age group (2.5-4 years, 4-5 years and 5-7.5 years), as well as items targeting specific behavioral milestones in order to be sensitive to age-related differences. Emotional competence Emotional competence has been defined as the ability to be self-efficient in dealing with emotion eliciting situations in order to ensure adaptation to the social context (Buckley, Storino, & Saarni, 2003; Saarni, 2001). Three dimensions of emotional competence have been identified: emotion understanding, emotional expressiveness, and emotion regulation (Denham, 2006; Halberstadt, Denham, & Dunsmore, 2001). Deficient emotional competencies have been linked to poor

C. A. Ştefan, A. Bălaj, M. Porumb, M. Albu, M. Miclea
Cognition, Brain, Behavior. An Interdisciplinary Journal 13 (2009) 121-146
125
academic skills (Blair, 2002; Trentacosta & Izard, 2007). For example, children with poor emotional regulation skills have problems in focusing and shifting attention, which is a central ability for performance in academic tasks (Hill, Degnan, Calkins, & Keane, 2006). Lack of age-appropriate emotional competencies has been predictive of both internalizing and externalizing problems (Denham, Workman, Cole, Weissbrod, Kendziora & Zahn-Waxler, 2000; Gross & John, 2003). Emotion understanding consists of two main abilities: a receptive and an expressive one. The receptive component refers to the ability to identify emotions based on their labels, while the expressive component taps into their ability to name emotions based on non-verbal cues (Denham, 2006). Erroneous interpretations of affective messages are detrimental to children’s adaptation in social contexts and can be harmful to a child’s ability to maintain and develop friendships (Denham, 2007). Also, children with difficulties in interpreting affective messages are more likely to resort to aggressive strategies in dealing with conflict situations (Dunn & Cutting, 1999), and therefore have heightened risk for mental health problems, especially externalizing disorders (Denham, Blair, Schmidt, Blair, DeMulder, & Caal, 2002; Denham et al., 2001).
Emotion understanding in preschoolers develops from a basic level of ability to distinguish between positive or “good”, and negative or “bad” emotions at the age of 3, to more complex skills (Widen & Russell, 2002). By the time they are 5 most children should be able to correctly name four emotions: happiness, sadness, fear, and anger (Widen & Russell, 2002). Gradually by the age of 6-7, children are able to recognize the so called “social emotions” such as pride and shame, and emotions such as disgust and surprise (Widen & Russell, 2002; Widen & Russell, 2003).
Emotional expressiveness is central to sending affective messages (Denham, 2007). Emotional expressiveness refers to the ability to convey emotional messages in a socially accepted manner. Thus, children exhibiting negative emotional expressiveness, namely anger are less likely to be perceived positively by their peers and teachers (Sebanc, 2003). Children’s negative emotional expressiveness has been predictive of peer rejection and low levels of perceived social skills in teachers’ ratings of social competence (Sebanc, 2003). Emotional expressiveness also refers to being able to manage emotions. Children gradually learn that sending an emotional message can be appropriate in certain contexts, but not in others (Banerjee, 1997). For example, it is preferable to smile even when the gift received is not what the children hoped for, or look sad instead of laughing when parents or teachers are unhappy with their behavior. Preschool children’s ability to exert control over their emotional expression, especially negative emotions such as anger has been consistently linked to prosocial behaviors (Cole, Martin, & Dennis, 2004; Eisenberg, Sadovsky, Spinrad, Fabes, Losoya, Valiente,

C. A. Ştefan, A. Bălaj, M. Porumb, M. Albu, M. Miclea
Cognition, Brain, Behavior. An Interdisciplinary Journal 13 (2009) 121-146
126
et al., 2005). Three-year-old children usually express the emotions they feel. A possible consequence of this phenomenon is that children are more likely to exhibit aggressive strategies in order to deal with social conflict situations (Arsenio et al., 2000). In time, children internalize rules for emotion expression and gradually learn that masking emotions helps them adapt to adults’ expectations (Garner, 1999). Emotion regulation was defined as the processes involved in “evaluating, monitoring and modifying emotional reactions […] in order to accomplish one’s goals” (Thompson, 1994; as cited in Stansbury & Sigman, 2000). Emotion regulation abilities are considered fundamental for school readiness (Blair, 2002). These abilities are to a large extent related to attention focusing and shifting abilities, which are predictive of children’s school readiness (Posner & Rothbart, 2000; Spinrad, Eisenberg, Harris, Hanish, Fabes, Kupanoff, et al., 2004). Moreover, children with adequate regulatory abilities are more likely to exhibit positive emotional expressiveness, which is in turn related to prosocial behaviors, empathy, and positive problem-solving strategies in conflict situations (Calkins & Fox, 2002; Eisenberg, Fabes, Guthrie, & Reiser, 2000; Eisenberg, Guthrie, Murphy, Shepard, Cumberland, & Carlo, 1999). Consequently, children with adequate regulatory abilities proved to be less prone to mental health disorders (Calkins & Dedmon, 2000; Eisenberg et al., 2005; Gilliom, Shaw, Beck, Schonberg, & Lukon, 2002). During the preschool period, children’s strategies change from reliance on adult assistance to gradually becoming able to deal on their own with emotionally arousing stimuli (Stansbury & Sigman, 2000). Most of the strategies listed below are acquired from earlier developmental stages, many 3- and 4-year-old children dealing with emotion eliciting situations use either comforting strategies such as being held in the arms, being hugged by an adult, or self-soothing such as thumb sucking. Another category is instrumental strategies such as avoidance or visually inspecting a temporarily inaccessible item (Stansbury & Sigman, 2000). These strategies have been identified in experimental paradigms in which children are asked to make a choice between a smaller, but immediate reward versus a larger, delayed one. By the time they are 4-years-old, most children rely on attention shifting strategies, which are aimed at distracting attention from the stimuli producing the negative emotion. Usually attention shifting strategies are initially guided by parents, while after the age of 5 children implement these strategies on their own. Also, 6-year-old children begin to use to a certain extent cognitive reappraisal strategies learned from their parents. For example, a child might say that he/she does not want to eat candy, because then he/she will have to go to the dentist (Stansbury & Sigman, 2000).

C. A. Ştefan, A. Bălaj, M. Porumb, M. Albu, M. Miclea
Cognition, Brain, Behavior. An Interdisciplinary Journal 13 (2009) 121-146
127
Social competence Social competence is rather difficult to define. In an attempt to review the main definitions given to social competence, Gimpel and Merrell (1998) proposed that social competence refers to the ability to manifest socially acceptable behaviors with positive outcomes, which allow people to achieve their goals (Mendez, McDermott, & Fantuzzo, 2002). From a conceptual point of view, there is a difference between social competence and social skills. Social competence refers to the evaluative component of social behaviors, and includes social skills which are specific behaviors enacted in order to adapt to a specific social context (Sheridan, Hungelmann, & Poppenga Maughan, 1999).
Although there is extensive research on social competence, there were only few attempts to derive taxonomies for these skills (Gimpel & Merrell, 1998). However, the most widely cited social competencies are compliance to rules, interpersonal skills, and prosocial behaviors (Gimpel & Merrell, 1998). Children with poor social competence have difficulties in developing and maintaining relationships and are frequently rejected by peers. As a consequence, they either become more aggressive, a predictor of externalizing problems, or they develop depressive symptoms, which pose risks for internalizing problems (Brotman, Gouley, Chesir-Teran, Dennis, Klein, & Shrout, 2005; Engels, Finkenauer, Meeus, & Dekovic, 2001). Also, children who are rejected by their peers and are less popular show more problems in adjusting to school (Caldarella & Merrell, 1997; Fabes, Martin, Hanish, Anders, & Madden-Derdich, 2003). Compliance to rules is considered one of the main developmental tasks of preschool children (Wilburn, 2000). Most of the behaviors needed in order to maintain acceptable social interactions are driven by children’s ability to comply with rules or follow directions (Kotler & McMahon, 2002). Children with difficulties in following rules have low abilities in staying on task, which in turn is associated with poor academic performance (Kochanska, 2002; Kochanska, Tjebkes, & Forman, 1998). Lack of compliance is considered adaptive to a certain extent, because non-compliance can be a strategy which children use in order to assert their autonomy in relation to adults (Wahler, 1997). Passive non-compliance, ignoring a request, and negativity, refusing to do something, gradually decline during preschool (Kuczinsky & Kochanska, 1990). By the age of five, children are more compliant and learn to use verbal strategies in order to question or negotiate rule compliance (Lee, Belfiore, Scheeler, Hua, & Smith, 2004). Children who exhibit high levels of non-compliance are rejected by their peers and consequently have low social skills (Lee, Belfiore, & Gormley, 2008; Lee et al., 2004), which puts them at risk for developing externalizing problems (Kochanska, 2002; Kochanska & Murray, 2000).

C. A. Ştefan, A. Bălaj, M. Porumb, M. Albu, M. Miclea
Cognition, Brain, Behavior. An Interdisciplinary Journal 13 (2009) 121-146
128
Interpersonal skills reflect children’s ability to properly interact with other children and adults. Such interpersonal skills can be best evaluated in play settings where children establish friendships (Blankemeyer, Flannery, & Vaszonyi, 2002; Mendez, Fantuzzo, & Cicchetti, 2002). Children’s interpersonal skills develop with age, as their play patterns become more complex and sophisticated, ranging from parallel play to complex interactions in small groups of children (Vaughn, Colvin, Azria, Caya, & Krzysik, 2001). The patterns of child play are quite informative regarding their popularity (Coplan et al., 2004; Vaughn et al., 2001). Children with poor friendship skills are rejected by their peers and as a consequence lack the opportunity to develop their social skills (Gagnon & Nagle, 2004). These children are at risk for developing both internalizing and externalizing disorders (Brotman et al., 2005). Three-year-old children usually exhibit the so-called pretend play. At this age most children engage in isolated or parallel play. Isolated play means that the child plays by himself, while taking on different roles in a story (e.g., he can be the captain of the ship or a member of the crew) (Wilburn, 2000). Parallel play means that although the children are in each other’s proximity, they don’t in fact play the same game. Also, 3-year old begin to interact with other children in groups of two, usually same-sex peers (Fabes et al., 2003). Children’s ability to maintain interactions in larger groups evolves in time. Most 5-year old children participate in cooperative play. That means children exchange ideas over how they should continue a play scenario, and even attribute roles to children involved (Wilburn, 2000). Cooperative play stems from children’s understanding of reciprocity as the basis of building and maintaining friendships. Prosocial behaviors include a wide range of voluntary actions, which are directed at other people’s benefit (Krueger, Hicks, & McGrue, 2001). Behaviors that fall under this category are sharing toys and other objects, turn-taking, giving and asking for help (Warnes, Sheridan, Geske, & Warnes, 2005). Children manifest prosocial behaviors to the extent to which adults encourage and remind them how they should act in certain situations (Zanolli, Paden, & Cox, 1997). Children low on prosocial behavior are rejected by their peers, are often aggressive and exhibit behaviors which put them at risk for externalizing disorders (Hastings, Zahn-Waxler, Robinson, Usher, & Bridges, 2000; Sebanc, 2003).
Sharing toys can be a difficult task for some young children, and it is usually learned like most prosocial behaviors through adult modeling and prompting (Laible, Carlo, Torquati, & Ontai, 2004). Until the age of 5 most children need to be reminded to share toys, help or wait for their turn during a game. Later, once these rules are internalized, most children tend to exhibit these behaviors without adult prompting (Strayer & Roberts, 2004).

C. A. Ştefan, A. Bălaj, M. Porumb, M. Albu, M. Miclea
Cognition, Brain, Behavior. An Interdisciplinary Journal 13 (2009) 121-146
129
OBJECTIVES Our goal was to develop age-appropriate screening scales for assessing emotional and social development in preschool children. We took into consideration the dimensions of the above mentioned emotional and social competencies and age relevant developmental milestones. As a result we generated three versions of the screening scales corresponding to three age groups: 2.5-4 years, 4-5 years, and 5-7.5 years. The two types of scales of the screening instrument were user-friendly and took 10 minutes to complete. This is in accordance with the need to develop feasible instruments easy to administer and to score (DiStefano & Kamphaus, 2007; Smith, McCarthy, & Anderson, 2000). We also developed two versions for each age group, a form for parents and another form for teachers in order to obtain information from a multi-method, multi-informant perspective.
The present study investigates the psychometric properties of two screening scales, namely several methodological criteria such as reliability, factor structure and validity. Our goal was to develop an easy to administer instrument, covering relevant behaviors in order to identify preschool children at risk for academic failure and mental health problems. METHOD Participants. The total number of preschool children included in this study were N = 824. The sample characteristics for each age group: number of children, sex distribution and parental level of education are described below (Table 1). The sample was recruited taking into consideration the geographical areas in Romania, as well as representative urban (57.2%) and rural (42.8%) population distribution according to the latest census data showing that urban population represents 56.3% of the total preschool population.
Table 1 Distribution of participants according to age group, sex, and parental level of education Age group Number of
participants (N)
Sex Parental level of education Boys Girls Up to 8th
grade High school Higher
education 2.5-4 years N = 258 45.7% 54.3% 6.7% 43.3% 49.3% 4-5 years N = 256 43.8% 56.2% 4.8% 42.1% 50.1% 5-7.5 years N = 310 50.3% 49.7% 4.6% 41.6% 52.4%
One validation study, concerning predictive validity was done on a different sample than the one described above. The sample consisted of 30 children aged between 5.8 years and 6.9 years. Of these 12 were boys and 18 were girls.

C. A. Ştefan, A. Bălaj, M. Porumb, M. Albu, M. Miclea
Cognition, Brain, Behavior. An Interdisciplinary Journal 13 (2009) 121-146
130
Scale construction. The scales underwent the following stages: 1) Relying on the literature about child development we identified a few theoretical constructs for emotional competence (emotion understanding, emotional expressiveness, and emotion regulation) and social competence (compliance to rules, interpersonal skills, and prosocial behaviors). 2) An initial pool of items was generated based on a survey of the recent literature, other evaluation instruments used by teachers in preschool, as well as a thorough investigation of curricular objectives set for each age level. The item collection was developed based on age-appropriate milestones. 3) These items were subjected to evaluation by a group of 8 experts in developmental psychology, cognitive psychology, and psychodiagnostic, each holding at least a M.A. in Psychology. The group evaluated the items according to the dimension measured (emotional/social competence), wording, and relevance of the described behavior. 4) The remaining items were further evaluated by 36 preschool teachers and 32 parents, who were asked to complete the scales and make recommendations on how the items were phrased, as well as regarding the difficulties met in understanding their content. A small proportion of items were rephrased. 5) In the final stage, an item analysis was performed on the three versions of the screening completed by 123 preschool teachers and 123 parents. Frequencies for each item were processed in order to determine which respondents tend to answer similarly (have low discriminative power) and which show bimodal distributions (items can be interpreted in more than one way). A number of 5 items from the emotional competence screening and 4 items from the social competence screening were dropped after this analysis. The final versions of the screening scales were further evaluated and are presented in detail below. Instruments a. Screening Scales Emotion Competence Screening Emotion Competence Screening for Preschoolers – Parent Form (SCE-P, Ages 2.5-4.0). The Emotion Competence Scale consists of 11 items measuring Emotion Understanding (e.g., “The child says about himself/herself that he/she is happy or angry”; “The child says about others that they are happy or angry”), Emotion Expression (e.g., “The child expresses joy when receiving a gift”; “The child is sad when something bad happens to a family member”), and Emotion Regulation (e.g., “The child calms down easily after he/she was upset”; “The child plays with another toy when he/she does not have access to a particular toy”). The answers to these items were coded on a 5-point Likert scale, where 1 = almost never and 5 = almost always. All items were scored directly. The total score on this scale was obtained by summing the scores for each item of the scale.

C. A. Ştefan, A. Bălaj, M. Porumb, M. Albu, M. Miclea
Cognition, Brain, Behavior. An Interdisciplinary Journal 13 (2009) 121-146
131
Emotion Competence Screening for Preschoolers – Parent Form (SCE-P, Ages 4.0-5.0). This scale contains 14 items measuring Emotion Understanding (e.g., The child recognizes that others feel happy, angry, sad, or afraid”; “The child expresses context appropriate emotions”), Emotion Expression (e.g., “When scolded or praised, the child expresses the adequate emotion”; “The child imitates cartoon or story characters”), and Emotion Regulation (e.g., “The child shows patience until receiving attention or a reward”; “The child is able to stay calm even in situations he/she does not know how to solve the problem”). The answers to these items were coded on a 5-point Likert scale, where 1 = almost never and 5 = almost always. All items were scored directly. The total score on this scale was obtained by summing the scores for each item of the scale. Emotion Competence Screening for Preschoolers – Parent Form (SCE-P, Ages 5.0-7.5). This scale is made up of 17 items measuring Emotion Understanding (e.g., “The child observes emotion expressions of others and behaves adequately”; “The child says about others that they feel happy, angry, sad, or afraid”), Emotion Expression (e.g., “The child is sad when something bad happens to a family member”; “When scolded or praised, the child expresses the adequate emotion”), and Emotion Regulation (e.g., “The child waits his turn without being told”; “The child asks for help from adults in order to deal with his/her emotions”). The answers to these items were coded on a 5-point Likert scale, where 1 = almost never and 5 = almost always. All items were scored directly. The total score on this scale was obtained by summing the scores for each item of the scale. Emotion Competence Screening for Preschoolers – Teacher Form (SCE-E Ages 4.0-5.0). This scale contains 10 items measuring Emotion Understanding (e.g., “The child recognizes that others feel happy, angry, sad, or afraid”; “The child expresses context appropriate emotions”), Emotion Expression (e.g., “When scolded or praised, the child expresses the adequate emotion”; “The child laughs when playing with other children”), and Emotion Regulation (e.g., “The child only cries when he/she has reason to do so”; “The child is able to stay calm even in situations he/she does not know how to solve”). The items were coded on a 5-point Likert scale, where 1 = never and 5 = always. All items were scored directly. The total score on this scale was obtained by summing the scores for each item of the scale. Emotion Competence Screening for Preschoolers – Teacher Form (SCE-E, Ages 2.5-4.0). The Emotion Competence Scale consists of 10 items assessing Emotion Understanding (e.g., “The child is able to make a distinction between positive and negative feelings”; “The child says about others that they feel happy or angry”), Emotion Expression (e.g., “The child expresses joy when receiving a gift or a reward”; “The child imitates cartoon or story characters”), and Emotion Regulation (e.g., “The child is able to sit and wait for a story to be finished”; “The child plays

C. A. Ştefan, A. Bălaj, M. Porumb, M. Albu, M. Miclea
Cognition, Brain, Behavior. An Interdisciplinary Journal 13 (2009) 121-146
132
with another toy when he/she does not have access to that toy”). The items were coded on a 5-point Likert scale, where 1 = almost never and 5 = almost always. All items were scored directly. The total score on this scale was obtained by summing the scores for each item of the scale. Emotion Competence Screening for Preschoolers – Teacher Form (SCE-E, Ages 5.0-7.5). The Emotion Competence Scale consists of 18 items assessing Emotion Understanding (e.g., “The child recognizes emotions such as shame, pride or disgust”; “The child says about others that they are happy, angry, sad, or afraid”), Emotion Expression (e.g., “The child verbally encourages classmates”; “When scolded or praised, the child expresses the adequate emotion”), and Emotion Regulation (e.g., “The child waits his/her turn without being told”; “The child perseveres on a task even if it is challenging”). The items were coded on a 5-point Likert scale, where 1 = never and 5 = always. All items were scored directly. The total score on this scale was obtained by summing the scores for each item of the scale. Social Competence Screening Social Competence Screening for Preschoolers – Parent Form (SCS-P, Ages 2.5-4.0). This scale contains 10 items measuring Compliance to Rules (e.g., “The child stops an activity on request”; “The child answers adequately to your requests”), Interpersonal Skills (e.g. “The child acts friendly with unfamiliar children”; “The child invites other children to play”), and Prosocial Behavior (e.g., “The child shares his/her toys with other children when told”; “The child asks for help when he does not know how to do something”). Responses on each item were coded on a 5-point Likert scale, where 1 = almost never and 5 = almost always. All items were scored directly. The total score on this scale was obtained by summing the scores for each item of the scale. Social Competence Screening for Preschoolers – Parent Form (SCS-P, Ages 4.0-5.0). The Social Competence Scale consists of 12 items assessing Compliance to Rules (e.g., “The child easily accepts changes in game rules”, “The child is compliant to game rules”), Interpersonal Skills (e.g., “The child cooperates with other children during play”; “The child invites other children to play together”), and Prosocial Behavior (e.g., “The child shares his/her toys without being told”, “The child offers to help others if you tell him/her”). Items were coded on a 5-point Likert scale, where 1 = almost never, and 5 = almost always. All items were scored directly. The total score on this scale was obtained by summing the scores for each item of the scale. Social Competence Screening for Preschoolers – Parent Form (SCS-P, Ages 5.0-7.5). For this age category, the Social Competence scale consists of 22 items

C. A. Ştefan, A. Bălaj, M. Porumb, M. Albu, M. Miclea
Cognition, Brain, Behavior. An Interdisciplinary Journal 13 (2009) 121-146
133
measuring Compliance to Rules (e.g., “The child understands the consequences of not following rules”; “The child puts away his toys without being reminded”), Interpersonal Skills (e.g., “The child speaks about his/her friends from preschool”, “The child is able to identify solutions to his/her problems with partial assistance from you”), and Prosocial Behavior (e.g., “The child takes care of other children’s toys”; “The child shares his/her toys with other children without being told”). Responses on each item of the scale were coded on a 5-point Likert scale, where 1 = almost never and 5 = almost always. All items were scored directly. The total score on this scale was obtained by summing the scores for each item of the scale. Social Competence Screening for Preschoolers – Teacher Form (SCS-E, Ages 2.5-4.0). The Social Competence Scale consists of 14 items measuring Compliance to Rules (e.g., “The child stops speaking when asked by you”; “The child answers adequately on request”), Interpersonal (e.g., “The child plays in small groups of two-three children”; “The child imagines during play that he/she is somebody else”), and Prosocial Behavior (e.g., “The child shares his/her toys with other children when told”; “The child asks for your help to end fights with other children”). Responses for each item were coded on a 5-point Likert scale, where 1 = almost never and 5 = almost always. All items were scored directly. The total score on this scale was obtained by summing the scores for each item of the scale. Social Competence Screening for Preschoolers – Teacher Form (SCS-E, Ages 4.0-5.0). For this age group the scale is made up of 15 items assessing Compliance to Rules (e.g., “The child easily accepts changes in game rules”, “The child follows your rules during tasks”), Interpersonal Skills (e.g., “The child plays with more than three children at once”; “The child invites other children to play together”), and Prosocial Behavior (e.g., “The child shares his/her toys without being told”, “The child takes care of other children’s toys”). Responses for each item were coded on a 5-point Likert scale, where 1 = almost never and 5 = almost always. All items were scored directly. The total score on this scale was obtained by summing the scores for each item of the scale. Social Competence Screening for Preschoolers – Teacher Form (SCS-E, Ages 5.0-7.5). For the last age category the instrument consists of 24 items measuring Compliance to Rules (e.g., “The child understands the consequences of not following rules”; “The child puts away his/her toys without being reminded”), Interpersonal Skills (e.g., “The child is able to join a group without interrupting the game”, “The child remains engaged in group activities for at least fifteen minutes”), and Prosocial Behavior (e.g., “The child takes care of other children’s toys”; “The child says he/she is sorry for doing something wrong when you ask him/her”). Responses for each item were coded on a 5-point Likert scale, where 1 = almost never and 5 = almost always. All items were scored directly. The total score on this scale was obtained by summing the scores for each item of the scale.

C. A. Ştefan, A. Bălaj, M. Porumb, M. Albu, M. Miclea
Cognition, Brain, Behavior. An Interdisciplinary Journal 13 (2009) 121-146
134
b. Validation instruments Social Skills Rating System-Preschool Version Social Skills Rating System (Parent Form). The Social Skills Rating System (SSRS) – Parent Form (Gresham & Elliott, 1990) consists of two summary scales Social Skills and Behavior Problems. The Social Skills scale is comprised of four 10-item subscales: Cooperation (e.g., “Helps you with household tasks without being asked”; “Puts away toys or other household property”), Assertion (e.g., “Joins group activities without being told”; “Received criticism well”), Responsibility (e.g., “Politely refuses unreasonable requests from others”, “Asks permission before using another family member property”), and Self-control (e.g., “Controls temper in conflict situations with you”, “Ends disagreements with you calmly”). Each item is rated 3-point Likert scale, measuring the frequency of a specific behavior, where 0 = never and 2 = very often. The Problem Behavior summary scale consists of two subscales: Externalizing Problems consisting of 6 items (e.g., “Argues with others”, “Disturbs ongoing activities”), and Internalizing Problems consisting of 4 items (e.g., “Says nobody likes him”, “Shows anxiety about being in a group of children”). Both subscales are rated on a 3-point Likert scale, where 0 = never and 2 = very often. Scores obtained for every scale completed are summed and allow computation of raw scores for the basic scales as well as for the summary scales. Social Skills Rating System (Teacher Form). The Social Skills Rating System – Teacher Form (Gresham & Elliott, 1990) consists of two summary scales Social Skills and Behavior Problems. The Social Skills scale includes three 10-item subscales measuring Cooperation (e.g., “Attempts classroom tasks before asking for your help”; “Finishes class assignments within time limits”), Assertion (e.g., “Makes friends easily”; “Volunteers to help peers with classroom tasks”), and Self-control (e.g., “Compromises in conflict situations with peers”; “Receives criticism well”). Each item is rated 3-point Likert scale, measuring the frequency of a specific behavior, where 0 = never and 2 = very often. The Problem Behavior summary scale consists of 6 items measuring Externalizing (e.g., “Has temper tantrums”; “Disobeys rules and requests”), and 4 items evaluating Internalizing disorders (e.g., “Says nobody likes him or her”; “Shows anxiety about being in a group of children”). The items are rated on a 3-point Likert scale, where 0 = never and 2 = very often. Scores obtained for every scale completed are summed and allow computation of raw scores for the basic scales as well as for the summary scales. Procedure. The Screening norms for the screening were obtained using the sample described above. The parents and teachers completed the screening according to the child’s age group. They were also asked to complete the SSRS teacher and parent form. Another group of 30 children were included in the predictive

C. A. Ştefan, A. Bălaj, M. Porumb, M. Albu, M. Miclea
Cognition, Brain, Behavior. An Interdisciplinary Journal 13 (2009) 121-146
135
validation study. For them, screening-based evaluations were done in the year before going to school. Teachers also rated these children for their overall performance in school tasks (letter and digit recognition, drawing, vocabulary, etc.). Teachers were asked to rate the children in three performance groups: “first 5”, “average”, and “last 5”. One year later, the school teachers were asked to make similar evaluations the same children. RESULTS Reliability Internal consistency. The internal consistency of the two scales consistency was computed using α-Cronbach. The α values ranged between .80 and .93 for the SCE-P and SCE-E, and between .89 and .95 for the SCS-P and SCS-E (Table 2). Table 2 Internal consistency (α-Cronbach) for the SCE and SCS parent and teacher form
Teacher version Parent version SCE-E 2.5-4 SCE-E 4-5 SCE-E 5-7.5 SCE-P 2.5-4 SCE-P 4-5 SCE-P 5-7.5
.84 .88 .93 .80 .85 .88 SCS-E 2.5-4 SCS-E 4-5 SCS-E 5-7.5 SCS-P 2.5-4 SCS-P 4-5 SCS-P 5-7.5
.89 .91 .95 .89 .85 .92
Test-retest reliability. Test-retest reliability was measured for both teacher and parent forms of the SCE and SCS for the 5-7.5 age group at a 3 month interval. Test-retest coefficients were in the .72- .83 range (Table 3). Table 3 Test-retest correlations for the SCE and SCS parent and teacher forms for the 5-7.5 age category at T1 and T2 (after 3 months)
SCE-E 5-7.5 (T2)
SCE-P 5-7.5 (T2)
SCS-E 5-7.5 (T2)
SCS-P 5-7.5 (T2)
SCE-E 5-7.5 (T1)
.83*
SCE-P 5-7.5 (T1)
- .72*
SCS-E 5-7.5 (T1)
- - .76*
SCS-P 5-7.5 (T1)
- - - .74*
* p < .05

C. A. Ştefan, A. Bălaj, M. Porumb, M. Albu, M. Miclea
Cognition, Brain, Behavior. An Interdisciplinary Journal 13 (2009) 121-146
136
Inter-rater reliability. Inter-rater reliability was processed between the two informant sources: parents and teachers for each age group. The parent and teacher form of the SCE ranged from .15 (2.5-4 years), to .36 (4-5 years), and .14 (5-7.5 years), while for the SCS varied from .14, .32, and .31, respectively. All correlation coefficients were significant at p < .05, and they were in the range of low agreement. Construct validity Factor structure. For determining the factor structure of our scales we used expert evaluations. A group of eight experts in developmental psychology, cognitive psychology, and psychodiagnostic, each having at least a M.A. in Psychology, evaluated the items according to the dimensions measured (emotional/social competence). The items for which seven out of eight experts agreed on were kept while the others were dropped. Convergent validity. Convergent validity was assessed by establishing the relationship between the two screening measures and similar constructs. For the convergent validity of the SCE (both forms), we chose the Self-control scale form SSRS as its items reflect the use of emotion knowledge and emotion regulation strategies in social interactions. The correlation coefficients were processed separately for both parent and teacher versions. Pearson correlation coefficients varied in the medium range (Table 4). Table 4 Convergent validity of the SCE-E and SCE-P with scores obtained on the Self-Regulation Scale (SSRS) of the parent and teacher forms SCE-E 2.5-4 SCE-E 4-5 SCE-E 5-7.5 Self-Regulation (SSRS-Teacher Form)
.52** .50** .63**
SCE-P 2.5-4 SCE-P 4-5 SCE-P 5-7.5 Self-Regulation (SSRS-Parent Form)
.39** .40** .59**
** p < .01
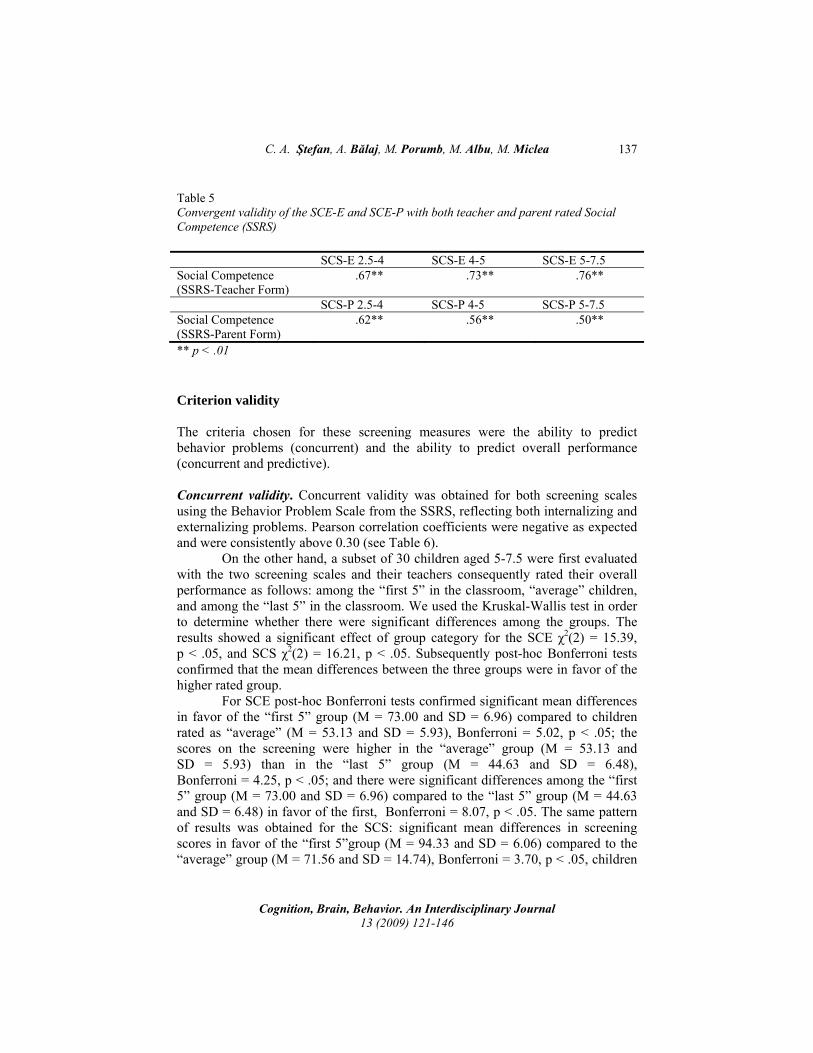
For the SCS version we calculated the correlations between the scores of the screening and a total score of Social Competence of SSRS, both teacher and parent forms. Correlations coefficients were above .50 (Table 5).
C. A. Ştefan, A. Bălaj, M. Porumb, M. Albu, M. Miclea
Cognition, Brain, Behavior. An Interdisciplinary Journal 13 (2009) 121-146
137
Table 5 Convergent validity of the SCE-E and SCE-P with both teacher and parent rated Social Competence (SSRS) SCS-E 2.5-4 SCS-E 4-5 SCS-E 5-7.5 Social Competence (SSRS-Teacher Form)
.67** .73** .76**
SCS-P 2.5-4 SCS-P 4-5 SCS-P 5-7.5 Social Competence (SSRS-Parent Form)
.62** .56** .50**
** p < .01 Criterion validity
The criteria chosen for these screening measures were the ability to predict behavior problems (concurrent) and the ability to predict overall performance (concurrent and predictive). Concurrent validity. Concurrent validity was obtained for both screening scales using the Behavior Problem Scale from the SSRS, reflecting both internalizing and externalizing problems. Pearson correlation coefficients were negative as expected and were consistently above 0.30 (see Table 6).
On the other hand, a subset of 30 children aged 5-7.5 were first evaluated with the two screening scales and their teachers consequently rated their overall performance as follows: among the “first 5” in the classroom, “average” children, and among the “last 5” in the classroom. We used the Kruskal-Wallis test in order to determine whether there were significant differences among the groups. The results showed a significant effect of group category for the SCE χ2(2) = 15.39, p < .05, and SCS χ2(2) = 16.21, p < .05. Subsequently post-hoc Bonferroni tests confirmed that the mean differences between the three groups were in favor of the higher rated group.
For SCE post-hoc Bonferroni tests confirmed significant mean differences in favor of the “first 5” group (M = 73.00 and SD = 6.96) compared to children rated as “average” (M = 53.13 and SD = 5.93), Bonferroni = 5.02, p < .05; the scores on the screening were higher in the “average” group (M = 53.13 and SD = 5.93) than in the “last 5” group (M = 44.63 and SD = 6.48), Bonferroni = 4.25, p < .05; and there were significant differences among the “first 5” group (M = 73.00 and SD = 6.96) compared to the “last 5” group (M = 44.63 and SD = 6.48) in favor of the first, Bonferroni = 8.07, p < .05. The same pattern of results was obtained for the SCS: significant mean differences in screening scores in favor of the “first 5”group (M = 94.33 and SD = 6.06) compared to the “average” group (M = 71.56 and SD = 14.74), Bonferroni = 3.70, p < .05, children

C. A. Ştefan, A. Bălaj, M. Porumb, M. Albu, M. Miclea
Cognition, Brain, Behavior. An Interdisciplinary Journal 13 (2009) 121-146
138
rated as “average” (M = 71.56 and SD = 14.74) had significantly higher scores than those in the “last 5” category (M = 54.13 and SD = 12.11), Bonferroni = 5.79, p <.05, and also significant differences among screening scores in favor of the children rated as “top 5” (M = 94.33 and SD = 6.06) compared to those rated in the “last 5” category (M = 54.13 and SD = 12.11), Bonferroni = 7.24, p < .05.
Table 6 SCE and SCS concurrent validity for mental health problems
SCE-E 2.5-4
SCE-E 4-5
SCE-E 5-7.5
SCS-E 2.5-4
SCS-E 4-5
SCS-E 5-7.5
Behavior Problems (Teacher)
- .41** - .36** - .37** - .51** - .31** - .40**
SCE-P 2.5-4
SCE-P 4-5
SCE-P 5-7.5
SCS-P 2.5-4
SCS-P 4-5 SCS-P 5-7.5
Behavior Problems (Parent)
- .33** - .31** - .46** - .42** - .30** - .42**
** p < .01 Predictive validity. The predictive validity of our screening was established on a subset of 30 children from the 5-7.5 age category. They were assessed using the screening during their last year in kindergarten and were later evaluated by their teacher in the 1st grade. Teachers were asked to classify the children in their classroom in three overall school performance categories: among the “first 5” in the classroom, “average” children, and among the “last 5” in the classroom. The Kruskal-Wallis test was used in order to determine whether there are differences in emotion competence screening scores between the three groups of children. Post-hoc Bonferroni tests were used to determine mean differences between the groups. The results yielded a significant group effect χ2 (2) = 21.61, p < .05. Post-hoc Bonferroni tests showed that children rated among the “first 5” (M = 82.83 and SD = 8.11) had significantly higher scores compared to those rated as “average” (M = 63.00 and SD = 8.59), Bonferroni = 5.44, p < .05; children rated as “average” (M = 63.00 and SD = 8.59) had significantly higher scores than those in the “last 5” (M = 48.25 and SD = 7.59), Bonferroni = 2.62, p < .05; and also significant differences among screening scores in favor of the children rated as “top 5” (M = 82.83 and SD = 8.11) compared to those rated in the “last 5” category (M = 48.25 and SD = 7.59), Bonferroni = 7.78, p < .05. The same procedure was used in order to determine the predictive validity of the social competence screening. The Kruskal-Wallis test showed a significant group effect χ2(2) = 20.97, p < .05, and subsequent Bonferroni tests confirmed significant differences between the three groups in the expected directions. The children’s screening scores were significantly higher in the “first 5” category (M = 108.17 and SD = 13.28)

C. A. Ştefan, A. Bălaj, M. Porumb, M. Albu, M. Miclea
Cognition, Brain, Behavior. An Interdisciplinary Journal 13 (2009) 121-146
139
compared to those classified as “average” (M = 86.13 and SD = 9.79), Bonferroni = 5.13, p<.05; children rated as “average” (M = 86.13 and SD = 9.79) had significantly higher scores than those in the “last 5” (M = 61.88 and SD = 9.60), Bonferroni = 3.09, p < .05; and children from the “first 5” category (M = 108.17 and SD = 13.28) has significantly higher screening scores than those in the “last 5” category (M = 61.88 and SD = 9.60), Bonferroni = 8.13, p < .05. DISCUSSION First, we will discuss reliability indices. The internal consistency showed that all the scales have high internal consistency. Also, test-retest coefficients show good stability of the scales over time. Inter-rater reliability coefficients were low. This result is in accordance with the fact that in many cases children’s behaviors at home and in school are inconsistent and this is the reason for adopting a multi-informant and a multi-method approach. A meta-analysis showed that inter-rater reliability for instruments evaluating preschool children’s behavior are in the medium range, more precisely between 0.30-0.50 (Achenbach et al., 2002). As it can be seen in our results, inter-rater reliability is around 0.30 only for screening measures for the 5.0-7.5 age group. It is possible that with age, contextual incongruence in children’s behaviors is less likely to be observed. Another possible explanation is that in some cases parents tend to show bias in evaluating their own children or have little opportunities of comparing them to other children in the same age category. On the other hand, teachers can use their observations from the classroom and make comparisons between children that can prove to be more accurate (Huffman & Nichols, 2004). Our aim was to use a multiple-informant strategy of assessment which we believe to be effective in establishing a behavior pattern and a trend in skill acquisition. In our view, it is not so important to match the evaluations, as to integrate information from both parent and teacher perspective (Crooks & Peters, 2005). Construct validity was assessed using the SSRS Parent and Teacher forms. In order to assess construct validity for the SCE-P and SCE-E, we chose the Self-Regulation subscale from the SSRS. This scale includes items which reflect children’s ability to use emotion regulation abilities in social interactions. Our choice was largely determined by the fact that the existing scales usually measure social-emotional competencies as a unitary construct. One of the aims of this screening was to make a clear distinction between these two competencies. The Pearson product-moment correlations for the SCE-E and SCE-P were in the medium range, which is satisfactory taking into account that the two constructs are not entirely similar. On the other hand, the Social Competence Scale from the SSRS Parent and Teacher forms were positively correlated with the SCS-P, and SCS-E respectively. Pearson coefficients were ranging from medium to high,

C. A. Ştefan, A. Bălaj, M. Porumb, M. Albu, M. Miclea
Cognition, Brain, Behavior. An Interdisciplinary Journal 13 (2009) 121-146
140
especially for the SCS-E. These data showed that our scales measure similar constructs as other instruments. Concurrent validity was determined for two types of criteria: behavior problems and teacher ratings of child performance in school tasks. Pearson correlations between the SCS-P and SCS-E and the Behavior Problem Scale from the SSRS Parent and Teacher versions were medium negative correlations. These data show good predictive validity of our screening measures for mental health symptoms specific to both internalizing and externalizing problems, which is one of the aims of our instrument.
In order to determine the screening’s capacity to accurately predict school readiness, we used an ecologically valid strategy: teacher ratings of child overall performance. Teachers are more likely to observe and make comparisons between children’s performance on similar tasks (McCoy & Pianta, 1997; Strong Scott & Delgado, 2003). The results yielded significant differences between screening scores obtained by children included in three overall performance categories: “first 5”, “average”, and “last 5”. All differences were in the expected direction, meaning that the highest scores on the screening were obtained by the children rated among the “top 5”, followed by those of the children rated as “average”, while the lowest scores were obtained by those rated as “last 5”. These results also indicated that screening for emotional and social competencies is a good predictor of a child performance on school tasks. We only obtained data regarding this type of performance for the 5-7.5 age group, because at this time most of the children are supposed to exhibit behaviors predictive for their ability to adequately perform in school. Also, teacher evaluations of such performance would have been premature as preschool activities for children under the age of 5 are less oriented to preparing them to deal with school tasks. We also wanted to see to what extent preschool measurements of social and emotional competence made by teachers during the last year in preschool were predictive of their school performance in the 1st grade. The data show that both average scores of children on the SCE-E and SCS-E were the highest in the “first 5” category and decreased as a function of group classification. These data show that children’s school success can be predicted by emotional and social competencies screening in preschool. Furthermore, it seems that these data are in accordance with more recent paradigms in school readiness research that place a greater emphasis on the fact that emotional and social competencies mediate the impact of cognitive abilities on school performance (Blair, 2002; Snow, 2006). For example, children with well developed emotional regulation strategies are able to focus and shift their attention over longer periods of time (Hill, Degnan, Calkins, & Keane, 2006). On the other hand, children that score high on instruments of peer acceptance and other instruments of social competence are more likely to adapt to school environment and develop long-term positive attitudes towards school and are less likely to drop out (Caldarella & Merrell, 1997).

C. A. Ştefan, A. Bălaj, M. Porumb, M. Albu, M. Miclea
Cognition, Brain, Behavior. An Interdisciplinary Journal 13 (2009) 121-146
141
CONCLUSIONS Our first aim was to develop a user-friendly, easy to administer screening instrument, integrating parent and teacher evaluations. Furthermore, we used developmental milestones for three age groups in order to accurately assess children’s abilities longitudinally, taking into account the way these competencies change according to the child age. Initial stages of instrument development were followed by research on validity. Inter-item and test-retest reliability were consistently good. However, low correlations on inter-rater reliability should be a result of the fact that our instrument evaluates these competencies in different settings. Children’s behavior is known to be inconsistent at this age, teacher and parent ratings often mirroring different aspects of child behavior (Huffman & Nichols, 2004). Also, these inconsistencies as shown by Achenbach et al. (2002) tend to diminish in 10-11 year-old children, teacher and parent ratings becoming more similar. Validity evaluation showed that both parent and teacher versions of the SCE and SCS measure similar constructs as other similar instruments. Criterion validity coefficients are important for a screening instrument largely because they should be able to predict a child’s risk status. As stated, our goals were twofold: being able to predict behavior problems and difficulties in adapting to school demands. Our measures showed good predictive capacity for measures of internalizing and externalizing problems. Overall performance in school tasks was evaluated concurrently and predictively. In both cases, as expected, emotional and social competence screening proved reliable in determining children’s performance. To sum up, the SCE and SCS parent and teacher forms for each age group show good psychometric properties. Based on these properties, we developed norms for the Romanian population of preschool children. However, there is a need to further evaluate these instruments, especially by further validation studies. Also, a shortcoming of this research is the fact that we did not obtain data on specificity and sensitivity indices. These data will be gathered in an upcoming study. However, results obtained on predictive validity are encouraging to take this next logical step. The practical implications of our research are most relevant for mental health practitioners especially those working as school psychologists. To our knowledge this is the first attempt to develop a screening instrument in Romania that is able to predict mental health problems and possible school readiness problems based on a child’s emotional and social skills development. It would be essential to change existing practices largely based on common sense, when it comes to 1st grade enrollment, with sound, empirically tested instruments. We believe that a consistent longitudinal evaluation of children is needed in order to prevent mental health problems and school maladjustment. As a consequence, the

C. A. Ştefan, A. Bălaj, M. Porumb, M. Albu, M. Miclea
Cognition, Brain, Behavior. An Interdisciplinary Journal 13 (2009) 121-146
142
aim of screening is not simply labelling children as deficient in acquiring certain abilities, but rather promoting an early detection and intervention in such cases. ACKNOWLEDGMENTS
The authors would like to express their gratitude to Dr. Oana Benga and Dr. Thea Ionescu from Babeş-Bolyai University for allowing us to use as reference their work on a Behavior Checklist for preschoolers, and for their valuable input on item selection. REFERENCES Achenbach, T. M., Dumenci, L., & Rescorla, L. A. (2002). Ten-year comparisons of
problems and competencies for national samples of youth. Journal of Emotional and Behavioral Disorders, 10, 194-203.
Arsenio, W. F., Cooperman, S., & Lover, A. (2000). Affective predictors of prescholers’ aggression and peer acceptance: Direct and indirect effects. Developmental Psychology, 36, 438-448.
Banerjee, M. (1997). Hidden emotions: Preschoolers’ knowledge of appearance-reality and emotion display rules. Social Cognition, 15, 107-132.
Barry, T., & Lochman, J. (2003). Social skills-assessment. In: T. Ollendick & C. Schroeder (Eds.), Encyclopedia of Clinical Child and Pediatric Psychology (pp. 629-631). Kluwer Academic/Plenum Publishers.
Blair, C. (2002). School readiness – integrating cognition and emotion in a neurobiological conceptualization of children's functioning at school entry. American Psychologist, 57, 111-127.
Blankemeyer, M., Flannery, D. J., & Vazsonyi, A. T. (2002). The role of aggression and social competence in children’s perceptions of the child-teacher relationship. Psychology in the Schools, 39, 293-304.
Brotman, L. M., Gouley, K. K., Chesir-Teran, D., Dennis, T., Klein, R. G., & Shrout, P. (2005). Prevention for preschoolers at high risk for conduct problems: Immediate outcomes on parenting practices and child social competence. Journal of Clinical Child and Adolescent Psychology, 34, 724-734.
Bryd, R., Weitzman, M., & Auinger, P. (1997). Increased behavior problems associated with delayed school entry and delayed school progress. Pediatrics, 100, 654-661.
Buckley, M., Storino, M., & Saarni, C. (2003). Promoting emotional competence in children and adolescents: Implications for school psychologists. School Psychology Quarterly, 18, 177-191.
Caldarella, P., & Merrell, K. W. (1997). Common dimensions of social skills of children and adolescents: A taxomomy of positive behaviors. School Psychology Review, 26, 264-278.
Calkins, S. D., & Fox, N. A. (2002). Self-regulatory processes in early personality development: A multilevel approach to the study of childhood social withdrawal and aggression. Development and Psychopathology, 14, 477-498.
Carlton, M. P., & Winsler, A. (1999). School readiness: The need for a paradigm shift. School Psychology Review, 28, 338-352.

C. A. Ştefan, A. Bălaj, M. Porumb, M. Albu, M. Miclea
Cognition, Brain, Behavior. An Interdisciplinary Journal 13 (2009) 121-146
143
Cole, P. M., Martin, S. E., & Dennis, T. A. (2004). Emotion regulation as a scientific construct: Methodological challenges and directions for child development research. Child Development, 75, 317-333.
Crooks, C. V., & Peters, R. D. (2005). Predicting academic difficulties: Does a complex, multidimensional model outperform a unidimensional teacher rating scale? Canadian Journal of Behavioural Science, 37, 170-180.
Cutting, A. L., & Dunn, J. (2006). Conversations with siblings and with friends: Links between relationship quality and social understanding. British Journal of Developmental Psychology, 24, 73-87.
Datar, A. (2006). Does delaying kindergarten entrance give children a head start. Economics of Education Review, 25, 43-62.
Denham, S. (2007). Dealing with feelings: how children negotiate the worlds of emotions and social relationships. Cognition, Brain, Behavior, 11, 1-48.
Denham, S., Mason, T., Caverly, S., Schmidt, M., Hackney, R., Caswell, C., & DeMulder, E. (2001). Preschoolers at play: Co-socializers of emotional and social competence. International Journal of Behavioral Development, 25, 90-101.
Denham, S., Workman, E., Cole, P., Weissbrod, C., Kendziora, K., & Zahn-Waxler, C. (2000). Prevention of externalizing behavior problems from early to middle childhood: The role of parental socialization and emotion expression. Development and Psychopathology, 12, 23-45.
Denham, S. A. (2006). Social-emotional competence as support for school readiness: What is it and how do we assess it? Early Education and Development, 17, 57-89.
Denham, S. A., Blair, K. A., Schmidt, M. S., Blair, K., DeMulder, E., & Caal, S. (2002). Preschool understanding of emotions: Contributions to classroom anger and aggression. Journal of Child Psychology and Psychiatry, 43, 901-916.
DiStefano, C. A., & Kamphaus, R. W. (2007). Development and validation of a behavioral screener for preschool-age children. Journal of Emotional and Behavioral Disorders, 15, 93-102.
Downer, J. T., & Pianta, R. C. (2006). Academic and cognitive functioning in the first grade: Associations with earlier home and child care predictors with concurrent home and classroom experiences. School Psychology Review, 35, 11-30.
Eisenberg, N., Fabes, R. A., Guthrie, I. K., & Reiser, M. (2000). Dispositional emotionality and regulation: Their role in predicting quality of social functioning. Journal of Personality and Social Psychology, 78, 136-157.
Eisenberg, N., Guthrie, I. K., Murphy, B. C., Shepard, S. A., Cumberland, A., & Carlo, G. (1999). Consistency and development of prosocial dispositions: A longitudinal study. Child Development, 70, 1360-1372.
Eisenberg, N., Sadovsky, A., Spinrad, T. L., Fabes, R. A., Losoya, S. H., Valiente, C., Reiser, M., Cumberland, A., & Shepard, S. A. (2005). The relations of problem behavior status to children’s negative emotionality, effortful control, and impulsivity: concurrent relations and prediction of change. Developmental Psychology, 42, 193-211.
Engels, C. M. E., Finkenauer, C., Meeus, W., & Dekovic, M. (2001). Parental attachment and adolescents’s emotional adjustment: Associations with social skills and relational competence. Journal of Counseling Psychology, 48, 428-439.

C. A. Ştefan, A. Bălaj, M. Porumb, M. Albu, M. Miclea
Cognition, Brain, Behavior. An Interdisciplinary Journal 13 (2009) 121-146
144
Fabes, R. A., Martin, C. L., Hanish, L. D., Anders, M. C., & Madden-Derdich, D. A. (2003). Early school competence: The roles of sex-segregated play and effortful control. Developmental Psychology, 39, 848-858.
Garner, P. W. (1999). Continuity in emotion knowledge from preschool to middle-childhood and relation to emotion socialization. Motivation and Emotion, 23, 247-266.
Gilliom, M., Shaw, D. S., Beck, J. E., Schonberg, M. A., & Lukon, J. L. (2002). Anger regulation in disadvantaged preschool boys: Strategies, antecedents, and the development of self-control. Developmental Psychology, 38, 222-235.
Gimpel, G. A., & Merrell, K. W. (1998). On the nature and value of social skills. In: G.A. Gimpel & K.W. Merrell (Eds.), Social skills of children and adolescents: conceptualization, assessment, treatment (pp. 1-28). Lawrence Erlbaum Associates, Mahwah, NJ.
Gredler, G. R. (1997). Issues in early childhood screening assessment. Psychology in the Schools, 34, 99-106.
Gresham, F. M., & Elliott, S. N. (1990). Social Skills Rating System manual. American Guidance Services, Circle Pines, MN.
Halberstadt, A. G., Denham, S. A., & Dunsmore, J. C. (2001). Affective social competence. Social Development, 10, 10-20.
Hastings, P. D., Zahn-Waxler, C., Robinson, J., Usher, B., & Bridges, D. (2000). The development of concern for others in children with behavior problems. Developmental Psychology, 36, 531-546.
Health Resources and Services Administration. (2007). Child Health USA 2007. Retreived February 10th, 2009, from http://www.mchb.hrsa.gov/mchirc/chusa/.
Hill, A. L., Degnan, K. A., Calkins, S. A., & Keane, S. P. (2006). Profiles of externalizing behavior problems for boys and girls across preschool: The roles of emotion regulation and inattention. Developmental Psychology, 42, 913-928.
Hill, A. L., Degnan, K. A., Calkins, S. A., & Keane, S. P. (2006). Profiles of externalizing behavior problems for boys and girls across preschool: The roles of emotion regulation and inattention. Developmental Psychology, 42, 913-928.
Hill, L. G., Lochman, J. E., Coie, J. D., Greenberg, M. T., & The Conduct Problems Prevention Research Group (2004). Effectiveness of early screening for externalizing problems: Issues of screening accuracy and utility. Journal of Consulting and Clinical Psychology, 72, 809-820.
Hirsh-Pasek, K., Kochanoff, A., Newcombe, N. S., & de Villiers, J. (2005). Using scientific knowledge to inform preschool assessment: making the case for “empirical validity”. Social Policy Report, 19, 3-19.
Huffman, L. C., & Nichols, M. (2004). Early detection of young children’s mental health problems in primary care settings. In R. Delcarmen-Wiggins & A. Carter (Eds.), Handbook of Infant, Toddler, and Preschool Mental Health Assessment (467-490). Oxford University Press, NY.
Ionescu, T., & Benga, O. (2007). Reconceptualizing early education on scientific grounds: School readiness in focus. Cognition, Brain, Behavior, 9, 49-65.
Kochanska, G. (2002). Commited compliance, moral self, and internalization: A mediational model. Developmental Psychology, 38, 339-351.

C. A. Ştefan, A. Bălaj, M. Porumb, M. Albu, M. Miclea
Cognition, Brain, Behavior. An Interdisciplinary Journal 13 (2009) 121-146
145
Kochanska, G., Tjebkes, T. L., & Forman, D. R. (1998). Children’s emerging regulation of conduct: Restraint, compliance, and internalization from infancy to the second year. Child Development, 69, 1378–1389.
Korkman, M., Jaakkola, M., Pesonen, A.-E., & Turunen, M-M. (2004). Screening of developmental disorders in five-year-olds using the FTF (Five to Fifteen) questionnaire: A validation study. European Child & Adolescent Psychiatry (Supplement 3), 13, 31-38.
Kotler, J. C., & McMahon, R. J. (2002). Differentiating between anxious, aggressive, and socially competent children: validation of the Social Competence and Behavior Evaluation – 30 (Parent version). Behavior Research and Therapy, 40, 947-959.
Krueger, R. F., Hicks, B. M., & McGue, M. (2001). Altruism and antisocial behavior: Independent tendencies, unique personality correlates, distinct etiologies. Psychological Science, 12, 397-402.
Kuczinski, L., & Kochanska, G. (1990). Development of children’s non-compliance strategies from toddlerhood to age 5. Developmental Psychology, 26, 398-408.
La Paro, K. M., & Pianta, R.C . (2001). Predicting children’s competence in the early school years: A meta-analytic review. Review of Educational Research, 70, 443-484.
Laible, D, Carlo, G., Torquati, J., & Ontai, L. (2004). Children’s perception of family relationships as assessed in a doll story completion task: Links to parenting, social competence and externalizing behavior. Social Development, 13, 551-569.
Lee, D. L., Belfiore, P. J., & Gormley, S. (2008). Riding the wave: creating a momentum of school success. Teaching Exceptional Children, 40, 65-70.
Lee, D. L., Belfiore, P. J., Scheeler, M. C., Hua, Y., & Smith, R. (2004). Behavioral momentum in academics: Using embedded high-p sequence to increase academic productivity. Psychology in the Schools, 41, 789-801.
Lemerise, A. E., & Arsenio, C. R. (2000). An integrated model of emotion processes and cognition in social information processing. Child Development, 71, 107-118.
Linares, L. O., Rosbruch, N., Stern, M. B., Edwards, M. E., Walker, G., Abikoff, H. B., & Alvir, J. M. I. (2005). Developing cognitive-social-emotional competencies to enhance academic learning. Psychology in the Schools, 42, 405-418.
Mantzicopoulos, P. Y., & Neuharth-Pritchett, S. (1998). Transitional first-grade referrals: An analysis of school-related factors and children’s characteristics. Journal of Educational Psychology, 90, 122-133.
Mendez, J.L., Fantuzzo, J., & Cicchetti, D. (2002). Profiles of social competence among low-income African American preschool children. Child Development, 73, 1085-1100.
Pianta, R. C., & McCoy, S. J. (1997). The first day of school: The predictive validity of early school screening. Journal of Applied Developmental Psychology, 18, 1-22
Posner, M. I., & Rothbart, M. K. (2000). Developing mechanisms of self-regulation. Development and Psychopathology, 12, 427-441.
Saarni, C. (2001). The continuity dilemma in emotional competence. Psychological Inquiry, 12, 94-96.
Sebanc, A. M. (2003). The friendship features of preschool children: Links with porsocial behavior and aggression. Social Development, 12, 249-268.

C. A. Ştefan, A. Bălaj, M. Porumb, M. Albu, M. Miclea
Cognition, Brain, Behavior. An Interdisciplinary Journal 13 (2009) 121-146
146
Sheridan, S. M., Hungelman, A., & Poppenga-Maughan, D. (1999). A contextualized framework for social skills assessment, intervention, and generalization. School Psychology Review, 28, 84-103.
Smith, G. T., McCarthy, D. M., & Anderson, K. G. (2000). On the sins of short-form development. Psychological Assessment, 12, 102-111.
Snow, K. L. (2006) Measuring school readiness: Conceptual and practical considerations. Early Education and Development, 17, 7–41.
Spinrad, T. L., Eisenberg, N., Harris, E., Hanish, L., Fabes, R.A., Kupanoff, K., Ringwald, S., & Holmes, J. (2004). The relation of children's everyday nonsocial peer play behavior to their emotionality, regulation, and social functioning. Developmental Psychology, 40, 67-80.
Stansbury, K., & Sigman, M. (2000). Responses of preschoolers in two frustrating episodes: Emergence of complex strategies for emotion regulation. Journal of Genetic Psychology, 161, 182-202.
Strayer, J., & Roberts, W. (2004). Children’a anger, emotional expressiveness, and empathy: relations with parent’s empathy, emotional expressiveness and parenting practices. Social Development, 13, 229-254.
Strong Scott, M., & Delgado, C. F. (2003). Using educational placement in third grade to select and validate a preschool screening measure. Psychology in the Schools, 40, 565-582.
Tramontana, M. G., Hooper, S. R., & Selzer, S. C. (1988). Research on the preschool prediction of later academic achievement: A review. Developmental Review, 8, 89-146.
Trentacosta, C. J., & Izard, C. E. (2007). Kindergarten children's emotion competence as a predictor of their academic competence in first grade. Emotion, 7, 77-88.
Vaughn, B. E., Colvin, T. N., Azria, M. R., Caya, L., & Krzysik, L. (2001). Dyadic analyses of friendship in a sample of preschool-age children attending Head Start: Correspondence between measures and implications of social competence. Child Development, 72, 862-878.
Wahler, R. G. (1997). On the origins of children’s compliance and opposition: Family context, reinforcement, and rules. Journal of Child and Family Studies, 6, 191-208.
Warnes, E. D., Sheridan, S. M., Geske, J., & Warnes, W. A. (2005). A contextual approach to the assessment of social skills: Identifying meaningful behaviors for social competence. Psychology in the Schools, 42, 173-187.
Widen, S. C., & Russell, J. A. (2002). Gender and preschoolers’ perception of emotion. Merrill-Palmer Quarterly, 48, 248–262.
Widen, S. C., & Russell, J. A. (2003). A closer look at preschoolers’ freely produced labels for facial expressions. Developmental Psychology, 39, 114–128.
Wilburn, R. E. (2000). Understanding the preschooler. Peter Lang, NJ. Zanolli, K. M., Paden, P., & Cox, K. (1997). Teaching prosocial behavior to typically
developing toddlers. Journal of Behavioral Education, 7, 373-391.