preprocedural coronary ct angiography significantly improves success rates of pci for chronic total...
TRANSCRIPT

ORIGINAL PAPER
Preprocedural coronary CT angiography significantly improvessuccess rates of PCI for chronic total occlusion
Andreas Rolf • Gerald S. Werner • Annika Schuhback • Johannes Rixe • Helge Mollmann •
Holger M. Nef • Constantin Gundermann • Christoph Liebetrau • Gabriele A. Krombach •
Christian W. Hamm • Stephan Achenbach
Received: 1 March 2013 / Accepted: 14 June 2013
� Springer Science+Business Media Dordrecht 2013
Abstract Chronic total occlusions of coronary arteries
occur in about 20 % of patients with suspected coronary
artery disease and are more frequent with increasing age.
The success rate of interventions is lower (55–80 %)
compared to conventional lesions ([90 %). Coronary CT
angiography (coronary CTA) provides information about
the occluded segment, which cannot be obtained from
invasive angiograms (XA). We therefore hypothesized that
preprocedural coronary CTA may improve success rates of
percutaneous coronary intervention (PCI) for coronary
arteries (CTO). 30 patients with chronic total coronary
artery occlusions (mean age 73 years, 26 men) and pre-
dicted high complexity were imaged by coronary CTA
prior to PCI for CTO. CT data sets were acquired with a 64
detector row dual source scanner and retrograde ECG
gating, 0.6 mm collimation and z-flying focal spot,
yielding isovoxel spatial resolution of about 0.4 mm.
Based on the CT data sets, established complexity criteria
for CTO (Euro CTO club, Di Mario et al. in EuroInter-
vention 3(1):30–43, 2007) were evaluated and compared to
invasive coronary angiography. Three-dimensional vol-
ume-rendered images of the occluded coronary artery were
displayed in the catheterization lab during PCI to guide the
advancement of the wire. PCI success, defined as the
ability to advance the guide wire into the distal lumen with
thrombolysis in myocardial infarction III flow was com-
pared to 43 controls without coronary CTA using propen-
sity score matching based on established criteria of
procedural success. The course of the occluded segments
was visualized by coronary CTA in all cases. Calcification,
lesion length, stump morphology and presence of side
branches were underestimated by invasive angiograms
when compared to coronary CTA. PCI success rate in 30
patients who underwent pre-procedural CTA was signifi-
cantly higher than in patients without prior coronary CTA
[unmatched: CT 90 % (27/30) vs. no CT 63 % (27/43),
p = 0.009; matched: CT 88 % (22/25) vs. no CT 64 % (16/
25) p = 0.03]. Through information not readily seen on
invasive coronary angiography, coronary CTA can signif-
icantly enhance success rates of PCI for CTO.
Keywords Coronary computed tomography angiography �Chronic total occlusion � PCI
Introduction
Chronic total occlusions of coronary arteries (CTO) occur
in about 20 % of patients with known or suspected coro-
nary artery disease [1], are more frequent in the right
coronary artery (RCA), and increase with advancing
A. Rolf (&) � H. Mollmann � H. M. Nef � C. Gundermann �C. Liebetrau � C. W. Hamm
Department of Cardiology, Kerckhoff Heart Center,
Benekestrasse 2-8, 61231 Bad Nauheim, Germany
e-mail: [email protected]; [email protected]
A. Rolf � J. Rixe � H. Mollmann � H. M. Nef � C. W. Hamm
Department of Cardiology, University of Giessen, Klinikstr. 33,
35392 Giessen, Germany
G. S. Werner
Department of Cardiology, Klinikum Darmstadt, Grafenstr. 9,
64283 Darmstadt, Germany
A. Schuhback � S. Achenbach
Department of Cardiology, University of Erlangen,
Ulmenweg 18, 91054 Erlangen, Germany
G. A. Krombach
Department of Radiology, University of Giessen, Klinikstr. 33,
35392 Giessen, Germany
123
Int J Cardiovasc Imaging
DOI 10.1007/s10554-013-0258-y

patient age [2, 3]. The definition of CTO is an obstruction
of a native coronary artery for at least 3 months showing
no ante grade blood flow as assessed by coronary angiog-
raphy [thrombolysis in myocardial infarction (TIMI) grade
0] [3–5]. Revascularization of CTOs through percutaneous
coronary intervention (PCI) is challenging. Reported suc-
cess rates are between 55 % and 80 % [3, 6–10]. In com-
parison, the success rate for PCI of coronary artery stenoses
is more than 90 % [11]. However, patients benefit from
successful CTO recanalization through reduced long-term
cardiac mortality and decreased need for coronary artery
bypass surgery [12]. The most common cause for PCI
failure is the inability to successfully pass a guidewire
across the occluded segment [8]. Many predictors for PCI
failure have been identified, such as length of the occluded
segment, severe calcification, tortuosity of the occlusion,
stump morphology, distal vessel opacity, presence of
sidebranches and presence of bridging collaterals [7, 8, 13–
15]. The Euro CTO club has defined categorical com-
plexity criteria by which to estimate the expected proce-
dural success (compare Table 1 [5]). The success rate of
procedures can be expected as high as 90 % with pre-
dominantly favourable characteristics but may drop to 60
% in view of several unfavourable characteristics [5].
Even after crossing the proximal cap, further advance-
ment of the guidewire is challenging as the course of the
vessel is not known and the intraluminal position of the
wire cannot be verified.
Coronary computed tomography angiography (coronary
CTA) has been suggested to provide useful information for
procedure planning and prediction of procedure success
[16–21]. One hallmark of coronary CTA is the ability to
visualize the complete course of the occluded segment of
the vessel. This additional information can help to control
the guidewire position during advancement through the
lesion.
We therefore hypothesized that CT may provide useful
additional information beyond invasive coronary angiog-
raphy for CTO procedures. First we determined differences
in CTO classification by CT and invasive angiography and
in a second step, we analysed whether making volume-
rendered coronary CTA images available in the catheteri-
zation laboratory during the CTO procedure might increase
success rates of the procedure.
Patients and methods
Patients and ethics
Between December 2008 and December 2009 30 patients
were referred to our institution to undergo coronary CT
angiography prior to elective interventional recanalization
of a chronic total occlusion at Darmstadt Community
Hospital. Patients were referred because of the expected
high complexity of the intervention, 10 of them had failed
attempts at other institutions. All patients had symptomatic
angina despite optimal medical treatment, the majority of
patients had either undergone exercise testing or had
inducible ischemia on SPECT or cardiac MRI. Viability
diagnostics were available for some patients, those who
had not undergone viability testing had no regional wall
motion abnormalities on echo. All patients had diagnostic
quality of their scans and were therefore included in this
retrospective, explorative analysis. In order to match these
patients with a control cohort, we also included 43 patients
in the study who underwent PCI for CTO at the same
institution who had a similar complexity, but without prior
coronary CTA. A chronic total coronary occlusion was
defined as the presence of TIMI 0 flow within the occluded
segment and occlusion duration C3 month.
The study was approved by the ethics committee of the
University of Giessen.
Coronary CTA
All patients were examined using a dual source CT system
(Somatom Definition�, Siemens Healthcare, Forchheim,
Germany). The CTA was performed 2 ± 0.2 days prior to
the intervention. After placing an 18-G intravenous cath-
eter into an antecubital vein, and placing the ECG
Table 1 Euro CTO club complexity criteria
Simple Complex
Vessel diameter (mm) [3.0 \3.0
Occlusion length (mm) \20 [20
Calcium occluded segment None to moderate Severe
Tortuosity occluded segment Minimal to
moderate
Severe
Occlusion stump Tapered Blunt or
absent
Distal vessel opacification Good to excellent Poor
Distal vessel disease Absent or
moderate
Severe
Tandem/multiple occlusions No Yes
Tortuosity proximal to
occlusion
Minimal to
moderate
Severe
Disease of the proximal
segment
Absent or
Moderate
Severe
Expected guiding catheter
support
Good Poor
Ostial location No Yes
Previous attempts No Yes
Renal insufficiency Yes No
Expected patient tolerance Good Poor
Int J Cardiovasc Imaging
123
electrodes in standard position, all patients received 0.8 mg
of glycerole trinitrate sublingually immediately before the
scan. To achieve sufficient heart rate control patients were
administered between 5 and 15 mg of metroprolol i.v., with
a target heart rate below 65/min. Initially a topogram and
an unenhanced CT acquisition for calcification scoring
(64 9 0.6 collimation, variable pitch of 0.2–0.43,
depending on heart rate, reconstructed slice thickness
3.0 mm, reconstruction kernel B35f, respectively) were
obtained. A test bolus approach was performed determin-
ing the contrast agent transit time (10 ml of iopamidole,
containing 370 mg iodine/ml, followed by 50 ml of iso-
tonic saline, both at 6 ml/s). CT angiography was then
performed after injection of 80–120 ml of contrast agent at
6 ml/s, followed by 50 ml of saline. The exact amount of
contrast agent to be injected was calculated by the expected
duration of CT data acquisition and thus varied between
different patients. Data acquisition was performed from the
level of the tracheal bifurcation to the diaphragm in cranio-
caudal direction using a detector collimation of
32 9 0.6 mm and slice acquisition 64 9 0.6 mm by means
of a z-flying focal spot. Gantry rotation time was 330 ms
and pitch was 0.2–0.43. Tube current was adapted auto-
matically to each patient’s weight using CareDose 4D�
automatic exposure control and a reference tube current of
320 mAs. Tube voltage was 120 kV for both tubes, and the
ECG pulsing window was fixed to 35–70 % of the RR
interval for all patients.
Image data were reconstructed with a slice thickness of
0.75 mm and increment of 0.3 mm using a single RR-
interval reconstruction approach, resulting in a temporal
resolution of 83 ms. For synchronization of data recon-
struction with the ECG signal, retrospective gating was
performed. Image reconstructions were rendered in 5 %
increments from 35 to 70 % of the RR cycle and for each
patient, the data set with least motion was identified and
used for further processing and analysis.
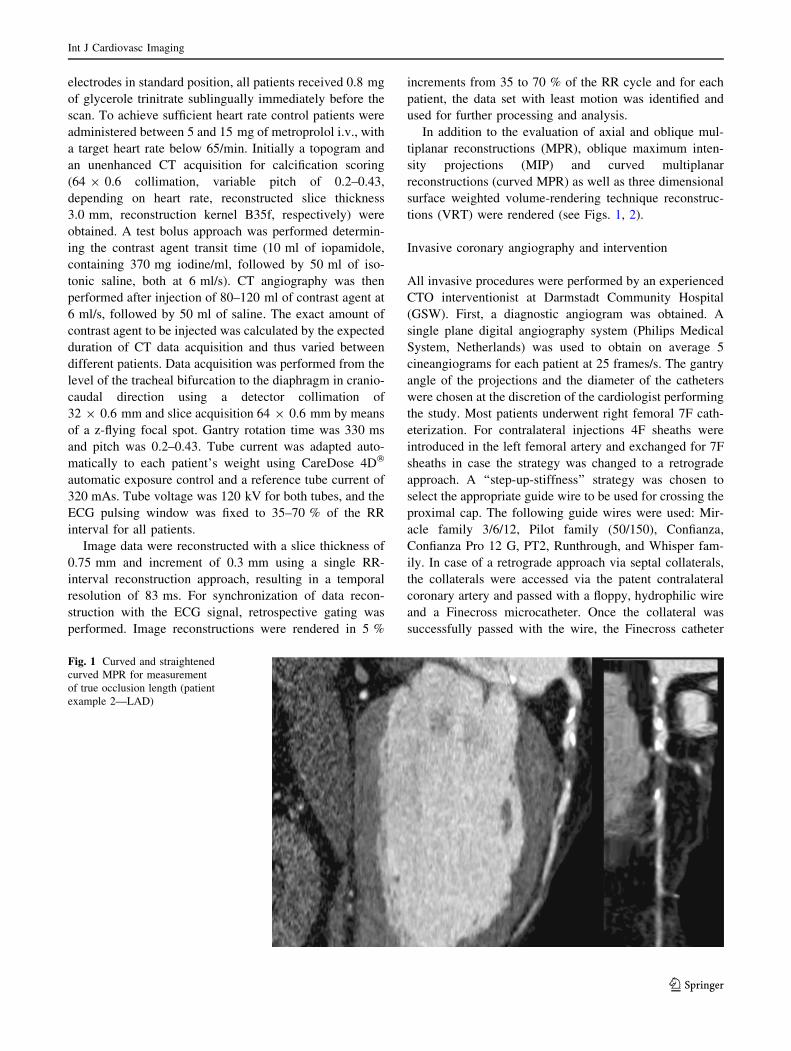
In addition to the evaluation of axial and oblique mul-
tiplanar reconstructions (MPR), oblique maximum inten-
sity projections (MIP) and curved multiplanar
reconstructions (curved MPR) as well as three dimensional
surface weighted volume-rendering technique reconstruc-
tions (VRT) were rendered (see Figs. 1, 2).
Invasive coronary angiography and intervention
All invasive procedures were performed by an experienced
CTO interventionist at Darmstadt Community Hospital
(GSW). First, a diagnostic angiogram was obtained. A
single plane digital angiography system (Philips Medical
System, Netherlands) was used to obtain on average 5
cineangiograms for each patient at 25 frames/s. The gantry
angle of the projections and the diameter of the catheters
were chosen at the discretion of the cardiologist performing
the study. Most patients underwent right femoral 7F cath-
eterization. For contralateral injections 4F sheaths were
introduced in the left femoral artery and exchanged for 7F
sheaths in case the strategy was changed to a retrograde
approach. A ‘‘step-up-stiffness’’ strategy was chosen to
select the appropriate guide wire to be used for crossing the
proximal cap. The following guide wires were used: Mir-
acle family 3/6/12, Pilot family (50/150), Confianza,
Confianza Pro 12 G, PT2, Runthrough, and Whisper fam-
ily. In case of a retrograde approach via septal collaterals,
the collaterals were accessed via the patent contralateral
coronary artery and passed with a floppy, hydrophilic wire
and a Finecross microcatheter. Once the collateral was
successfully passed with the wire, the Finecross catheter
Fig. 1 Curved and straightened
curved MPR for measurement
of true occlusion length (patient
example 2—LAD)
Int J Cardiovasc Imaging
123

was exchanged for an over-the-wire (OTW) balloon. Low-
pressure dilation of the collateral was achieved with a
1.25–1.5 mm OTW balloon to enable the penetration of a
balloon to the segment distal to the CTO. Penetration of the
distal CTO cap, initially with a soft wire and subsequently
with increasingly stiff wires, was then attempted. Wire
penetration was supported by the OTW balloon catheter.
Once the distal CTO cap had been penetrated, the wire was
advanced as far as possible and a distal channel was created
by repetitive balloon inflations. Next, an attempt was made
to cross the proximal CTO cap and the middle portion of
the CTO. The wire was then advanced to the created distal
channel and finally to the distal true lumen. In case the first
wire had penetrated the false lumen a second guide wire
would sometimes be used to follow another course to the
true lumen (parallel wire technique).
Both groups were treated according to the same inter-
ventional strategy.
Procedural success of the intervention was defined as the
ability to cross the lesion with the guide wire and advance
the guide wire into the distal true lumen, with subsequent
dilatation and stent placement with final TIMI3 flow.
To guide the procedure in the catheterization lab, 3D-
rendered VRT reconstructions of the occluded vessels were
projected in the catheterization suite. Orientations were
automatically aligned with the angulation of the c-arm.
Image processing and analysis
Processing of the coronary cineangiograms was performed
on an offline workstation and all metric measures were
calibrated against the diameter of the diagnostic or guide
catheter. Qualitative assessments were performed visually
by two experienced observers blinded to the treatment
group in consensus reading. For each patient, standardized
complexity criteria defined by the Euro CTO club (com-
pare Table 1 [5]) were measured and recorded. The com-
plexity criteria are categorical with two or three tiers in
each variable. Patients were stratified into each category of
each variable in consensus reading of two experienced
physicians familiar with both CT images and cineangio-
grams blinded for the corresponding measurement of the
CTA/cineangiogram respectively. There was no clear cut
off between categories. In case of calcification for example
lesions were rated not calcified, moderately calcified or
severely calcified. Depending on the category of each
variable the lesion was rated as complex or not complex.
The processing of the coronary CTA images was per-
formed on a dedicated workstation (syngo� workplace,
Siemens Medical Solutions, Forchheim, Germany). Vessel
and lumen diameters were measured in orthogonal pro-
jections on the curved MPR images and segment lengths
were measured on curved MPR images to yield the true
length of the occlusion. Qualitative assessments were
performed by two experienced observers. All lesions were
categorized according to the complexity criteria of the Euro
CTO club.
Propensity score matching and statistical analysis
To match patients between those who underwent CT and
those who did not, we chose 8 variables, which had been
Fig. 2 Invasive coronary angiogram of the RCA and corresponding VRT image shows that the true course of the RCA is much longer than the
invasive angiogram suggests
Int J Cardiovasc Imaging
123

shown to predict procedural success and with special rel-
evance to CT imaging: visibility of the occluded segments
(for example through microchannels in case of angiograms
or by CT), degree of calcification, occlusion length (as
categorical variable (B20 or [20 mm), tortuosity of the
occluded segment (as categorical variable (minimal, mod-
erate, severe), stump morphology (as categorical variable
(tapered, blunt, absent), opacity of the distal vessel seg-
ment, presence of side branches and ostial/non ostial
lesion. Also compare Table 1.
We performed nearest neighbour matching without
replacement and a caliper of 0.2. We used standardized
differences to report the baseline balance of the matched
variables. Differences between the two groups regarding
the complexity criteria were tested for statistical signifi-
cance using student’s t test for paired variables, Wilcoxon
signed rank test for non independent variables and
McNemar’s test, where appropriate depending on the scale
of the variable [22]. Additionally, multivariate logistic
regression analysis was performed to investigate the effect
that preprocedural coronary CTA has on procedural suc-
cess. Vessel course visibility, calcification, occlusion
length, tortuosity, stump morphology, distal vessel opacity,
presence of ostial lesions and sidebranches were included
in the model, as they had been identified as predictive of
procedural success in prior publications [7, 8, 13–16, 18].
Results are presented as odds ratios and 95 % confidence
intervals. A p value of B0.05 was considered statistically
significant. All computations were made using STATA11
(StataCorp LP, College Station, Texas, USA), propensity
score matching was performed with the psmatch2 proce-
dure by Leuven and Sianesi [23] balance testing of stan-
dardized differences was performed with the pstest
procedure by the same authors.
Results
The mean heart rate during coronary CT angiography was
61 ± 11 bpm and the mean dose length product of coro-
nary CT angiography was 640.7 ± 256.5, corresponding to
an estimated effective dose of 10.9 ± 4.2 mSv. In all 30
patients who underwent coronary CT angiography, data
sets were considered fully diagnostic and were included in
the analysis. Baseline characteristics of the patients are
displayed in Table 2.
The overall safety of the procedure was very good.
Creatinine levels increased significantly after the procedure
but not clinicially relevant (1.05 ± 0.22 vs.
1.15 ± 0.25 mg/dl, p = 0.001). However there was no
significant difference in postprocedural creatinine levels
between groups (1.18 ± 0.22 mg/dl CTA group vs.
1.12 ± 0.23 mg/dl no prior CTA group, p = 0.21). Three
patients had dissections (CTA group 2, no prior CTA 1
patients) all three could be covered by stents. 3 patients had
minor bleeding complications at the access site (CTA
group 1, without prior CTA 2 patients), there was one
major bleeding complication necessitating one blood
transfuion in the group without prior CTA. One temporary
acute kidney injury was documented in the CTA group,
maximum creatinine was 2.2 mg/dl, which returned to
normal at demission. There was one tamponade docu-
mented in the group without prior CTA, which could be
drained by pericardiocentesis without residual complica-
tions. The overall p for procedural complications was 0.6.
The course of the occluded segment was visible in all of
the 30 coronary CTA data sets but only in 8 of the 30
invasive coronary angiograms (p = 0.0001). The occlusion
length appeared to be significantly shorter on XA angio-
grams than in the projection-free measurements on the
curved MPR CT images (coronary CTA 30.2 ± 3.7 mm
vs. XA 21.9 ± 3.3 mm, p = 0.00001). There was no sig-
nificant difference in the measurements of the proximal
vessel diameter (coronary CTA 2.4 ± 0.25 mm vs. XA
2.3 ± 0.1 mm, p = 0.7289). The degree of calcification
(none to moderate vs. severe) was estimated to be signifi-
cantly smaller on XA angiograms compared to coronary
CTA (coronary CTA 8 of 30 complex calcifications, XA 2
of 30 complex calcifications, p = 0.004). There was a
trend towards more unfavourable stump morphology (blunt
or absent vs. tapered stump) by coronary CTA (coronary
CTA 17 complex morphologies, XA 11 complex mor-
phologies, p = 0.08). The presence of side branches was
correctly detected in a larger number of patients using
coronary CTA (coronary CTA 12 sidebranches, XA 6
sidebranches, p = 0.04). No statistically relevant differ-
ences were found for distal opacification (good or excellent
vs. poor) (coronary CTA 1 complex morphologies, XA 4
complex morphologies, p = 0.76), distal disease (absent or
moderate vs. severe) (coronary CTA 4 complex morphol-
ogies, XA 1 complex morphology, p = 0.07), presence of
multiple or tandem occlusions (coronary CTA 4 complex
morphologies, XA 4 complex morphologies, p = 1.0),
proximal tortuosity (minimal to moderate vs. severe)
(coronary CTA 2 complex morphologies, XA 7 complex
morphologies, p = 0.2), disease of the proximal segment
(absent or moderate vs. severe) (coronary CTA 9 complex
morphologies, XA 3 complex morphologies, p = 0.401) or
the identification of ostial lesions (coronary CTA 2 com-
plex morphologies, XA 2 complex morphologies,
p = 1.00) between coronary CTA and XA angiograms.
The additional burden of ionizing radiation by coronary
CTA was 10.8 ± 0.4 mSv and 73.2 ± 7.2 ml of contrast
agent had been administered for the coronary CTA.
After propensity matching, 25 patients in each group
remained for further analysis. 5 patients in the CT group
Int J Cardiovasc Imaging
123

were not eligible for matching because they were outside
the caliper of 0.2. Matching variables were well balanced
between the two groups (compare Table 3). The recom-
mended bias B10 % was met in all but two variables. A
significant bias remained with respect to vessel tortuosity,
which was in favour of the coronary CTA group (21.1 %).
Both in direct and in matched comparison, the inter-
ventional success rate was significantly higher in the group
of patients which had undergone pre-interventional coro-
nary CTA [unmatched: CT group 90 % (27/30) vs. no CT
group 63 % (27/43)], p = 0.009; matched: CT group 88 %
(22/25) vs. no CT group 64 % (16/25), p = 0.03]. Multi-
variate analysis on all 73 patients identified prior CT
as only independent predictor of procedural success
(coefficient 1.7 (0.087–3.23) p = 0.039. Four of the 27
successful recanalizations in the coronary CTA group were
achieved using a retrograde approach, while only two ret-
rograde approaches had been made in the group without
coronary CTA (p = 0.39).
The total procedure time was comparable between the
CTA- versus invasive coronary angiography groups
(107.7 ± 53.7 vs. 98.6 ± 35.2, p = 0.419). Similarly,
there were no significant differences in procedural time
among patients with successful versus unsuccessful PCI of
CTO (102.2 ± 43.6 vs. 102.8 ± 45, p = 0.957).
There was a trend to higher procedural doses of inon-
izing radiation in the coronary CTA group as compared to
patients without CT (18.9 ± 0.9 vs. 13.9 ± 0.5 mSv,
p = 0.09). There wasalso a trend towards more extensive
use of procedural contrast in the coronary CTA group
(287.7 ± 22.5 vs. 242.3 ± 13.4 ml, p = 0.08).
Discussion
Several publications have speculated about the effect of
preprocedural coronary CTA on the success rate of CTO
interventions and its role for the future. While some CT
parameters have been shown to predict procedural out-
come, there are some concerns regarding the radiation dose
that comes along with the additional CT imaging study [20,
24, 25]. Hence, it is necessary to clarify whether using CT
prior to attempted interventional CTO recanalization
results in clinical benefits. Kaneda et al. compared success
rates of procedures with and without prior coronary CTA
and found the success rate in the CT group to be higher
than that in the group without prior CT. However they did
not match both cohorts and did not use hypothesis testing.
From the early era of CTO interventions till today
several parameters have been identified as independent
predictors of procedural success by multivariate regression
analysis: occlusion length, calcification of the proximal
cap, stump morphology, tortuosity of the vessel and pres-
ence of a side branch as well as bridging collaterals and a
prior failed attempt [13, 14, 26–29]. All factors have been
accounted for in this analysis apart from bridging collat-
erals and failed attempts. The presence of bridging collat-
erals reflects the duration of the CTO and was therefore
found to be predictive of success. Since the duration of the
CTO did not differ in both groups we omitted this factor.
Previous attempts (predictive of failure) had almost
exclusively been made in the coronary CTA group (10
previous attempts vs. 1), therefore matching based on this
variable was not possible. But since 10 failed previous
attempts in the coronary CTA group were in favour of the
control cohort we thought it justified to perform matching
irrespective of this variable.
Table 2 Baseline characteristics
Number of patients Preprocedural
CT
Without
preprocedural
CT
p value
30 42
Clinical
Age (± SD) 63.3 (12) 62.5 (9.9) 0.75
Sex male 26 (87) 33 (76) 0.29
CCS Class I 6 (20) 3 (7) 0.15
CCS Class II 15 (50) 29 (67)
CCS Class III/IV 9 (30) 11 (26)
Inducible Ischemia 24 (80) 26 (60) 0.12
Viability positive (rest
not tested, echo
normal)
17 (56) 24 (55) 0.94
Risk factors
Smoker 20 (66) 20 (46) 0.09
Diabetes 4 (13) 14 (32) 0.06
Hyperlipemia 18 (60) 29 (67) 0.51
Hypertension 25 (83) 33 (77) 0.49
Body mass index (±SD) 27.6 (4.2) 26.8 (4.4) 0.4
Angiographic/procedural
History of myocardial
infarction month
(±SD)
44.1 (55.4) 39.2 (36.8) 0.78
Prior attempt at CTO 10 (33)** 1 (2)** 0.0001
Retrograde approach 5 (17) 6 (43) 0.75
Number of diseased
vessels
0.82
1 3 (10) 5 (11)
2 14 (46) 15 (34)
3 13 (43) 18 (42)
CTO vessel 0.59
Left anterior
descending artery
6 (20) 5 (11)
Circumflex artery 8 (26) 15 (34)
Right coronary artery 16 (53) 22 (51)
** Significant at 0.001 level
Int J Cardiovasc Imaging
123

Thus both groups had very similar baseline likelihoods
of procedural success and the greater success rate can
confidently be attributed to the additional information
yielded by coronary CTA.
We found, that among these factors calcification, lesion
length and stump morphology as well as presence of
sidebranches were underestimated by invasive angiograms.
These findings add to our hypothesis, that coronary CTA
yields additional information that assists in choosing the
right revascularization strategy and thus can help increas-
ing the success rates.
The most difficult issue in CTO interventions is to track
the right course through the lesion, beginning with the
proximal stump morphology and the crossing of the cap
over navigating the right way through the lesion to pene-
trating the distal cap.
It was possible to visualize the true and complete course
of the occluded vessel in all cases, by aligning the 3D
Dataset orientation to the orientation of the C-arm it was
possible to verify the right direction of the guidewire.
Figure 2 illustrates that the invasive angiogram can be
quite misleading when compared to the VRT image from
coronary CTA.
Interestingly the CT guided procedures tended to be
slightly longer and used higher dosages of the contrast
agent. We can only speculate about the reason but this is
probably due to more frequent rechecking of the guidewire
position in accordance with 3D VRT Dataset. This supports
our theory that the higher success rate is largely due to
better guidewire steering through the lesion.
In the present study we found significantly higher suc-
cess rates within the CT group in two well-matched
cohorts, yielding a success rate of 88 versus 64 %. To our
best knowledge this is the first study to make a direct
comparison between two treatment groups based on pro-
pensity score matching which is considered to be the gold
standard for matched pair analyses. The matching variables
were thoroughly chosen and well balanced between the
groups, which is paramount to this analysis. To avoid a
selection bias, we chose 8 variables for the propensity score
matching.
These findings are in good agreement with results of
Otsuka et al. [17] who also found, that 3D VRT images
helped to find optimal projection angles with least fore-
shortening and additional information about sidebranches
and lesion length. Similar results were found by Yokoyama
et al. [19] who found severely bent CTO segments in 13 %
of patients, which were not readily visible on invasive
angiograms.
Our data suggest, that success rates of PCI for CTO can
be improved by use of preprocedural coronary CTA. This
effect can be attributed to better vessel tracking on the
coronary CTA images within the occluded segment and to
the improved estimation of the complexity criteria.
Study limitations
This study is limited by the relatively small number of
patients, however we were able to perform thorough
Table 3 Covariate balance
Variable Sample Mean %Reduct t test
Treated Control %Bias Bias t p [ t
Visibility Unmatched 0.26667 0.09302 45.7 2.00 0.050
Matched 0.08333 0.125 -11 76 -0.46 0.645
Length (cat) Unmatched 0.5 0.53488 -6.9 -0.29 0.773
Matched 0.5 0.45833 8.2 -19.4 0.28 0.778
Calcification Unmatched 0.4 0.2093 32.3 1.37 0.175
Matched 0.29167 0.29167 0.0 100 0.00 1.000
Tortuosity Unmatched 0.53333 0.48837 7.6 0.31 0.757
Matched 0.54167 0.66667 -21.1 -178.0 -0.71 0.484
Stump morphology Unmatched 0.46667 0.69767 -32.0 -1.32 0.192
Matched 0.58333 0.54167 5.8 82.0 0.21 0.835
Distal opacity Unmatched 0.6 0.81395 -27.6 -1.15 0.256
Matched 0.625 0.66667 -5.4 80.5 -0.19 0.851
Ostial lesion Unmatched 0.06667 0.16279 -30.1 -1.22 0.225
Matched 0.08333 0.08333 0.0 100 0.00 1.000
Sidebranch Unmatched 0.2 0.32558 -28.4 -1.18 0.242
Matched 0.20833 0.20833 0.0 100 0.00 1.000
Int J Cardiovasc Imaging
123

matching of the coronary CTA and control cohort and
found a significant impact of coronary CTA on the success
rate of revascularization.
Conclusion
In this retrosepective propensity score matched analysis we
could demonstrate a significantly higher success rate of
CTO recanalization procedures with additional coronary
CTA. These results warrant a prospective, randomized
study comparing procedures with and without prior coro-
nary CTA to confirm our results.
Conflict of interest None.
References
1. Fefer P, Knudtson ML, Cheema AN, Galbraith PD, Osherov AB,
Yalonetsky S et al (2012) Current perspectives on coronary
chronic total occlusions: the canadian multicenter chronic total
occlusions registry. J Am Coll Cardiol 59(11):991–997
2. Cohen HA, Williams DO, Holmes DR Jr, Selzer F, Kip KE,
Johnston JM et al (2003) Impact of age on procedural and 1-year
outcome in percutaneous transluminal coronary angioplasty: a
report from the NHLBI Dynamic Registry. Am Heart J
146(3):513–519
3. Hoe J (2009) CT coronary angiography of chronic total occlu-
sions of the coronary arteries: how to recognize and evaluate and
usefulness for planning percutaneous coronary interventions. Int J
Cardiovasc Imaging 25(Suppl 1):43–54
4. Stone GW, Kandzari DE, Mehran R, Colombo A, Schwartz RS,
Bailey S et al (2005) Percutaneous recanalization of chronically
occluded coronary arteries: a consensus document: part I. Circ
Cardiovasc Imaging. 112(15):2364–2372
5. DiMario C, Werner G, Sianos G, Galassi A, Buttner J, Dudek D
et al (2007) European perspective in the recanalisation of Chronic
Total Occlusions (CTO): consensus document from the EuroCTO
Club. EuroIntervention 3:30–43
6. Suero JA, Marso SP, Jones PG, Laster SB, Huber KC, Giorgi LV
et al (2001) Procedural outcomes and long-term survival among
patients undergoing percutaneous coronary intervention of a
chronic total occlusion in native coronary arteries: a 20-year
experience. J Am Coll Cardiol 38(2):409–414
7. Olivari Z, Rubartelli P, Piscione F, Ettori F, Fontanelli A, Sa-
lemme L et al (2003) Immediate results and one-year clinical
outcome after percutaneous coronary interventions in chronic
total occlusions: data from a multicenter, prospective, observa-
tional study (TOAST-GISE). J Am Coll Cardiol 41(10):1672–
1678
8. Stone GW, Reifart NJ, Moussa I, Hoye A, Cox DA, Colombo A
et al (2005) Percutaneous recanalization of chronically occluded
coronary arteries: a consensus document: part II. Circ Cardiovasc
Imaging 112(16):2530–2537
9. Mehran R, Claessen BE, Godino C, Dangas GD, Obunai K,
Kanwal S et al (2011) Long-term outcome of percutaneous cor-
onary intervention for chronic total occlusions. JACC Cardiovasc
Interv 4(9):952–961
10. Galassi AR, Tomasello SD, Reifart N, Werner GS, Sianos G,
Bonnier H et al (2011) In-hospital outcomes of percutaneous
coronary intervention in patients with chronic total occlusion:
insights from the ERCTO (European Registry of Chronic Total
Occlusion) registry. EuroIntervention 7(4):472–479
11. Soon KH, Selvanayagam JB, Cox N, Kelly AM, Bell KW, Lim
YL (2007) Percutaneous revascularization of chronic total
occlusions: review of the role of invasive and non-invasive
imaging modalities. Int J Cardiol 116(1):1–6
12. Joyal D, Afilalo J, Rinfret S (2010) Effectiveness of recanaliza-
tion of chronic total occlusions: a systematic review and meta-
analysis. Am Heart J 160(1):179–187
13. Noguchi T, Miyazaki MS, Morii I, Daikoku S, Goto Y, Nonogi H
(2000) Percutaneous transluminal coronary angioplasty of
chronic total occlusions. Determinants of primary success and
long-term clinical outcome. Catheter Cardiovasc Interv
49(3):258–264
14. Tan KH, Sulke N, Taub NA, Watts E, Karani S, Sowton E
(1993) Determinants of success of coronary angioplasty in
patients with a chronic total occlusion: a multiple logistic
regression model to improve selection of patients. Br Heart J
70(2):126–131
15. Di Mario C, Werner GS, Sianos G, Galassi AR, Buttner J, Dudek
D et al (2007) European perspective in the recanalisation of
Chronic Total Occlusions (CTO): consensus document from the
EuroCTO Club. EuroIntervention 3(1):30–43
16. Mollet NR, Hoye A, Lemos PA, Cademartiri F, Sianos G,
McFadden EP et al (2005) Value of preprocedure multislice
computed tomographic coronary angiography to predict the out-
come of percutaneous recanalization of chronic total occlusions.
Am J Cardiol 95(2):240–243
17. Otsuka M, Sugahara S, Umeda K, Nakamura M, Nakamura A,
Bonkohara Y et al (2008) Utility of multislice computed
tomography as a strategic tool for complex percutaneous coro-
nary intervention. Int J Cardiovasc Imaging 24(2):201–210
18. Kaneda H, Saito S, Shiono T, Miyashita Y, Takahashi S, Domae
H (2007) Sixty-four-slice computed tomography-facilitated per-
cutaneous coronary intervention for chronic total occlusion. Int J
Cardiol 115(1):130–132
19. Yokoyama N, Yamamoto Y, Suzuki S, Suzuki M, Konno K,
Kozuma K et al (2006) Impact of 16-slice computed tomography
in percutaneous coronary intervention of chronic total occlusions.
Catheter Cardiovasc Interv 68(1):1–7
20. Garcia–Garcia HM, van Mieghem CA, Gonzalo N, Meijboom
WB, Weustink AC, Onuma Y et al (2009) Computed tomography
in total coronary occlusions (CTTO registry): radiation exposure
and predictors of successful percutaneous intervention. EuroIn-
tervention 4(5):607–616
21. Soon KH, Cox N, Wong A, Chaitowitz I, Macgregor L, Santos
PT et al (2007) CT coronary angiography predicts the outcome of
percutaneous coronary intervention of chronic total occlusion.
J Interv Cardiol 20(5):359–366
22. Austin PC (2008) A critical appraisal of propensity-score
matching in the medical literature between 1996 and 2003. Stat
Med 27(12):2037–2049
23. Leuven E, Sianesi B (2010) PSMATCH2: stata module to per-
form full Mahalanobis and propensity score matching, common
support graphing and covariate imbalance testing. 4.0.4. Nov
2010 ed2003
24. Schwartz RS, Cardiac CTA (2008) three-dimensions, and the
chronic total occlusion: a window to the future. Catheter Car-
diovasc Interv 71(6):790–791
25. Hecht HS (2008) Applications of multislice coronary computed
tomographic angiography to percutaneous coronary intervention:
how did we ever do without it? Catheter Cardiovasc Interv
71(4):490–503
26. Puma JA, Sketch MH Jr, Tcheng JE, Harrington RA, Phillips HR,
Stack RS et al (1995) Percutaneous revascularization of chronic
coronary occlusions: an overview. J Am Coll Cardiol 26(1):1–11
Int J Cardiovasc Imaging
123

27. Dong S, Smorgick Y, Nahir M, Lotan C, Mosseri M, Nassar H
et al (2005) Predictors for successful angioplasty of chronic
totally occluded coronary arteries. J Interv Cardiol 18(1):1–7
28. Morino Y, Abe M, Morimoto T, Kimura T, Hayashi Y, Mura-
matsu T et al (2011) Predicting successful guidewire crossing
through chronic total occlusion of native coronary lesions within
30 minutes: the J-CTO (Multicenter CTO Registry in Japan)
score as a difficulty grading and time assessment tool. JACC
Cardiovasc Interv 4(2):213–221
29. Tomasello SD, Costanzo L, Campisano MB, Barrano G, Ca-
podanno D, Tamburino C et al (2011) Does occlusion duration
influence procedural and clinical outcome of patients who
underwent percutaneous coronary intervention for chronic total
occlusion? J Interv Cardiol 24(3):223–231
Int J Cardiovasc Imaging
123