preparing for npts: learning from the past and preparing for the future
DESCRIPTION
Preparing for NPTs: Learning from the Past and Preparing for the Future. Anthony Lombardo, PhD July 27, 2011. Biomedical Approaches to HIV Prevention. Vaccines Microbicides Pre-exposure Prophylaxis (PrEP) Post-exposure Prophylaxis (PEP) - PowerPoint PPT PresentationTRANSCRIPT

Preparing for NPTs: Learning from the Past and Preparing for
the Future
Anthony Lombardo, PhD
July 27, 2011

Biomedical Approaches to HIV Prevention Vaccines Microbicides Pre-exposure Prophylaxis (PrEP) Post-exposure Prophylaxis (PEP)
Socio-Behavioural Issues of New Biomedical HIV Prevention Technologies Anthony Lombardo, January 2011, CATIE http://bit.ly/npt_sb
Partial Efficacy and the Uptake of New Biomedical HIV Prevention Technologies Anthony Lombardo, January 2011, CATIE http://bit.ly/npt_pe

Agenda Utilizing the technologies
Awareness Access Acceptability Adherence
Key socio-behavioural considerations Understanding risk Risk compensation Context of use Stigma
NPTs and the landscape of HIV prevention

Biomedical Prevention: Benefits Potential impact
Greater reach than behavioural interventions “Easier” to implement
Empowerment Women Men
But what are the “real life” challenges?
Importance of Social Science in Understanding NPTs and their Use Need to understand why people use
technologies – and why they don’t As with any other technology
Condoms, HAART
Need to understand how NPTs may change risk behaviour
Need to address these issues to support individuals’ use of the technologies
(Imrie et al., 2007; Kippax, 2008; Rosengarten et al., 2008)

Awareness of NPTs Awareness is key to uptake/use
Awareness of the technologies tends to vary by technology and population PEP: MSM, tends to be below 60% PEP: HIV+ women in London clinic, 80% had not
heard of PEP PrEP: MSM, approximately 20 – 25%
Awareness improved by campaigns

Acceptability of NPTs NPTs overall
Tend to be seen as acceptable…but a number of important considerations for acceptability: Efficacy of NPT at preventing HIV Side effects caused by NPT Cost of NPT
Microbicides Generally found acceptable by women, but concerns
about: Physical characteristics of the microbicide
Leakage, time of use, contraceptive properties Delivery method
Gels, rings, tablets Similar concerns about rectal microbicides, for both men and
women

Partial Efficacy Condoms &
microbicides

Partial Efficacy Condoms and Microbicides
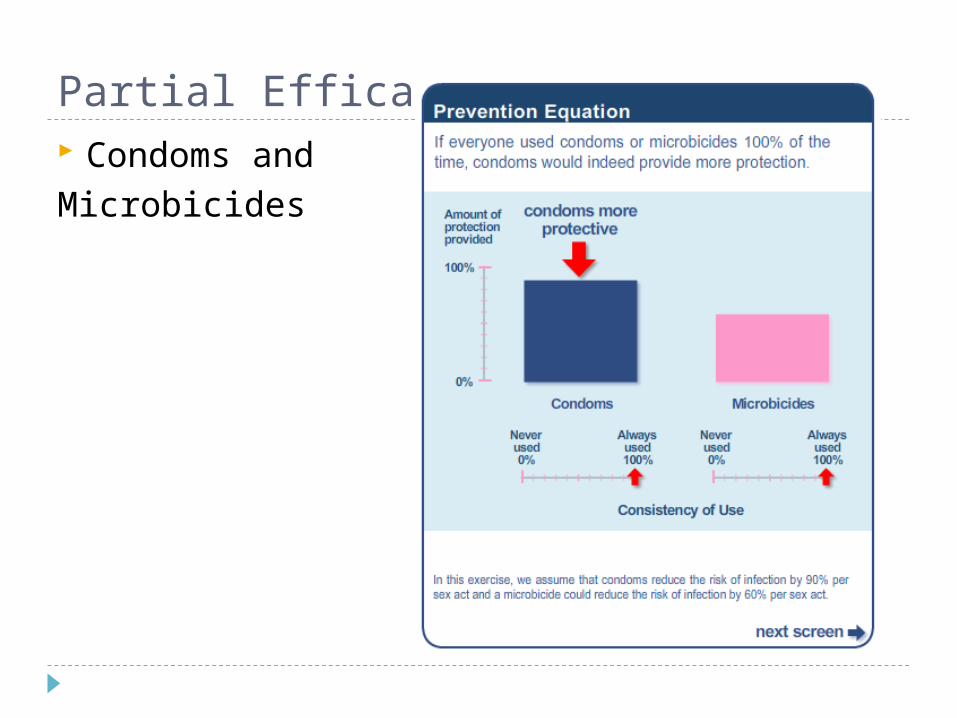
Partial Efficacy Condoms and Microbicides

Acceptability of NPTs Gender/power relations play a role
Women’s use of microbicides in context of relationships
NPTs may be most acceptable to those most at risk for HIV infection NPT studies suggest people with higher sexual risk
more likely to use or be interested in using NPTs

Access to NPTs Access to NPTs impacted by individual and
structural factors Testing
Knowledge of HIV status Availability
Technologies themselves Someone who can prescribe them
Timely access e.g., clinic hours, clinician awareness, awareness of risk
Cost

Access to NPTs Disparities impact access to NPTs
Race, gender, socio-economic status Similar to disparities in access to HAART
Concurrent HIV risk behaviours may impact access e.g., drug use: stigma, social exclusion, housing
instability, health care system access (Krüsi et al., 2010)

Adherence to NPTs HAART adherence as guide Barriers and motivators at individual and
structural levels Fear of disclosure, depression, forgetting to take
medications, scheduling Stigma, social isolation, social networks
Side effects may be significant barrier HIV-negative people may not tolerate side effects
Adherence rates iPrEX trial: 2,499 HIV- MSM, 95% adherence CAPRISA 004 trial: 72% of sex acts (past 30 days)
covered by two doses of gel 40% of 889 women had less than 50% adherence

Key Socio-Behavioural Issues Understandings of Risk Risk Compensation Gender, Agency and Empowerment

Understandings of Risk How individuals think about their own “risk”
behaviour will impact use of technologies How do people decide if they have been at risk,
and therefore attempt to access an NPT? Understandings of risk influenced at numerous
levels Individual: decisions about the “safety” of a sexual
partner or a sexual act e.g., serosorting, strategic positioning
Community: setting the “criteria” for what makes a safe partner or a safe sexual act

Understandings of Risk People at risk for HIV may not realize that
they are, and may not access NPTs PEP
Sayer et al. (2008): MSM in Brighton, UK Men accessed PEP because of “unusual” or “rare” sexual
encounters Sex with a casual partner deemed ‘unsafe’, sex at a certain type
of venue, sex under the influence Schechter et al. (2004): Brazilian MSM
Top reasons for not using PEP: sex with steady partner and encounters considered ‘low risk’
Vaccine Low perceived risk for HIV associated with less uptake of
potential vaccine, among diverse populations Newman, et al., 2008; Ravert & Zimet, 2009; Rhodes &
Hergenrather, 2002; Rudy et al., 2005; Salazar et al., 2005

Understandings of Risk People may think they are at greater risk than
they actually are, leading to potential misuse of NPTs
The “worried well” Poynten et al. (2007): PEP requests in an Australian
cohort, 1998-2004 “relatively large number” of requests unnecessary because
HIV status of partner in the exposure known in only about 1/3 of cases
Pinkerton et al. (1998) Priority of PEP: partners of HIV+ people; receptive anal
intercourse; likely HIV+ partner; extenuating circumstances (violent sex, partner with other STDs)
“provision of PEP to individuals with low-risk of exposures would diminish overall cost-effectiveness of the program”
Ethics?
Risk Compensation People may increase their risk behaviour
because of the perceived protection from NPTs
Evidence is mixed But evidence is also “early”
Few NPTs in real-world application

Risk Compensation PrEP
Early evidence does not suggest an increase in risk behaviour iPrEX trial: no evidence of risk compensation Ghanaian PrEP trial showed no increase in risk behaviour
among women in the trial (Guest et al., 2008) Californian studies of MSM show under 10% of men would be
less safe with efficacious PrEP (AIDS Partnership California, 2009; Al-Tayyib et al., 2009)
Intentions to use PrEP not associated with HIV risk factors (Mimiaga et al, 2009)
Reports of ‘off-label’ use of ARVs for PEP/PrEP among MSM concerning (Mansergh et al., 2010) Compromising preventive and treatment aspects of ARVs Reliance on unproven technologies (Kellerman et al., 2006)

Risk Compensation Microbicides
Little direct evidence, but some suggestion of an inclination towards increased risk behaviour CAPRISA 004: no evidence of risk compensation Possible decreasing condom use with highly effective
microbicide (Thurman et al., 2009) Belief in protection of microbicide in clinical trial,
despite warnings about unknown efficacy (Mantell et al., 2006)
MSM use of dangerous/unproven rectal microbicides, such as nonoxynol-9 (Carballo-Diéguez et al., 2007; Mansergh et al., 2003)

Risk Compensation Vaccine
Trials show mixed evidence of risk compensation Early San Francisco trials showed increase in insertive
unprotected anal intercourse among participants (Chesney et al., 1997)
Other trials have found no increase in risk behaviours among participants (Bartholow et al., 2005; Lampinen et al., 2005; van Griensven et al., 2004)
Hypothetical vaccine studies suggest potential increase in risk behaviour Concerns that “others” would increase their risk
behaviour (Salazar et al., 2005; Webb et al., 1999) Individuals themselves suggesting they would increase
risk behaviour with efficacious HIV vaccine (Barrington et al., 2008; Crosby et al., 2006; Newman et al., 2009)

Risk Compensation Definitive statements about the impact of
NPTs on risk behaviour are not possible at present Available evidence has some shortcomings…
Must account for the role of risk reduction counseling in controlled NPT trials, which may not reflect “real life”
Studies of hypothetical use and/or risk compensation may not reflect “real life”
Promotion of NPTs must account for the possibility of risk compensation
NPTs will not provide protection against other STIs

Gender, Agency and Empowerment NPTs may offer choice for people – especially
women – who cannot control men’s use of condoms
Use of NPTs still impacted by gender inequalities and power relations Severy et al. (2005): microbicide acceptability in
context Individual-level
Beliefs about susceptibility to HIV impact use Relationship-level
New relationships vs. established ones; difficulties in bringing the subject up with partner; male partner views on microbicides
Socio-cultural level Gender/economic inequalities mean women’s dependence on
men; cultural norms about intravaginal practices
Gender, Agency and Empowerment Female-controlled prevention options may
have unintended consequences (Koo et al., 2005; Mantell et al., 2006; Woodsong, 2004) Repercussions if secretive use is discovered Discontinuation of condoms with women’s
microbicide use Emphasis on women’s responsibility for sexual
health, rather than shared responsibility NPTs can empower other groups with
difficulties in sexual negotiation

NPTs and Landscape of HIV Prevention Combination prevention
NPTs alone are not enough NPTs will likely not be 100% effective Behavioural strategies still necessary
Need to go “beyond the individual” NPTs used by individuals, but within a broader
context Use of NPTs needs to be understood from different
levels in which it will be used Individual, community, society
(Cohen et al., 2008; Padian et al., 2008; Vermund et al., 2009)

NPTs in ContextIndividual Relationship/
CommunitySociety
(Social, Political, Economic)
Awareness Social relations Social networks Mass media
Marketing strategies
Acceptability Others’ evaluations of microbicides
Agency to negotiate microbicide use
Side effects
Norms about NPTs in social networks
Meanings of sex and drug use
Power relations in sexual encounters
Gender inequality Social constructions of
masculinity Social constructions of
sexuality
Access Subjective risk calculations based on the type of partner or risk event
Barriers to HIV testing Barriers to timely
treatment Barriers to health care
access generally
Norms about “risk” and “safety” in social networks
Stigma about testing; HIV diagnosis; accessing NPTs
Availability of NPTs in local setting
Availability of NPTs NPT distribution
policies Public health care
coverage of NPTs Medical culture
surrounding NPTs Racial and gender
disparitiesAdherence Influence of
relationship partner Negotiation skills Cost of treatments Convenience of
treatments
Social support networks
Stigma
Availability of NPTs Public health care
coverage of NPTs

Implementing NPTs Connected and complementary services
Risk reduction counseling STI screening Hepatitis vaccinations Counseling Ongoing HIV-status monitoring
e.g., PrEP: side effects; HIV infection; increases in risk behaviour
(Clauson, 2009; Paxton et al., 2007; Pozniak, 2004)

Messaging and Marketing NPTs Emphasizing benefits and limitations of NPTs Address/discourage risk compensation Culturally- and gender-appropriate Communicating partial effectiveness
How to encourage uptake with technologies that are not 100% protective…and discourage risk compensation?
Utilize social theory to increase uptake of messages Use particular health behaviour change models
e.g., health belief model, stages of change, etc. But must still account for contextual issues(Access Working Group; Cassell et al., 2006; Eaton &
Kalichman, 2007; Global HIV Prevention Working Group, 2006; Nodin et al., 2008)
Messaging and Marketing NPTs Framing approaches
Downplaying focus on HIV prevention PEP as ‘morning after pill,’ PrEP as ‘birth control’ Microbicide as sexual enhancement rather than
HIV prevention Caution of unintended consequences
“Female-controlled” marketing may alienate men Marketing to high-risk groups may stigmatize the
NPT and reduce access Marketing a product to be used covertly?
(Access Working Group; Cassell et al., 2006; Eaton & Kalichman, 2007; Global HIV Prevention Working Group,
2006; Nodin et al., 2008)

Messaging and Marketing NPTs Whom to message?
Individual users Mass media
Social networks Partners, friends, families
Health care practitioners How are people talking about NPTs?
“Education” may not be the complete answer How people talk about NPTs may have a big
impact on how if and/or how they are used e.g., controversy over MMR (measles, mumps, rubella)
vaccinations Require grounding in local understandings
Need formative research

In Conclusion… NPTs must be understood within a broader
context Many issues involved in NPT access and use
depending on factors beyond the individual Messaging/marketing NPTs must account for
this broader context Risk compensation must be monitored,
especially in real-world application Behavioural approaches should not be
abandoned for biomedical interventions

HIV Prevention: The Bigger Picture
What does all of this mean for HIV prevention? Need to acknowledge shortcomings of three
different approaches Behavioural
Lack of coverage Biomedical
Science and uptake Structural
Difficult to implement Difficult to evaluate
Prevention needs to encompass all three levels

Readings & ResourcesBrooks, R. A., Etzel, M., Klosinski, L. E., Leibowitz, A. A., Sawires, S., Szekeres, G., et al. (in press). Male circumcision and HIV prevention:
Looking to the future. AIDS Behav.Cassell, M. M., Halperin, D. T., Shelton, J. D., & Stanton, D. (2006). Risk compensation: The Achilles' heel of innovations in HIV
prevention? BMJ, 332, 605-607.Global Campaign for Microbicides. (2009). Trials Watch: Microbicides late clinical development. Available:
www.global-campaign.org/download.htmGuinot, D., Ho, M. T., Poynten, I. M., McAllister, J., Pierce, A., Pell, C., et al. (2009). Cost-effectiveness of HIV nonoccupational post-
exposure prophylaxis in Australia. HIV Med, 10(4), 199-208.Gupta, G. R., Parkhurst, J. O., Ogden, J. A., Aggleton, P., & Mahal, A. (2008). Structural approaches to HIV prevention. Lancet, 372, 764-
775.Hanenberg, R. S., Rojanapithayakorn, W., Kunasol, P., & Sokal, D. C. (1994). Impact of Thailand’s HIV-control programme as indicated by
the decline of sexually transmitted diseases. Lancet, 344(8917), 243-245.Millett, G. A., Flores, S. A., Marks, G., Reed, J. B., & Herbst, J. H. (2008). Circumcision status and risk of HIV and sexually transmitted
infections among men who have sex with men: A meta-analysis. JAMA, 300(14), 1674-1684.Moore, J. P., Klasse, P. J., Dolan, M. J., & Ahuja, S. K. (2008). AIDS/HIV. A STEP into darkness or light? Science, 320, 753-755.Okwundu, C. I., & Okoromah, C. A. (2009). Antiretroviral pre-exposure prophylaxis (PrEP) for preventing HIV in high-risk individuals.
Cochrane Database Syst Rev, 1, CD007189.Padian, N. S., Buve, A., Balkus, J., Serwadda, D., & Cates, W., Jr. (2008). Biomedical interventions to prevent HIV infection: Evidence,
challenges, and way forward. Lancet, 372, 585-599.Rerks-Ngarm, S., Pitisuttithum, P., Nitayaphan, S., Kaewkungwal, J., Chiu, J., Paris, R., et al. (2009). Vaccination with ALVAC and AIDSVAX
to prevent HIV-1 infection in Thailand. N Engl J Med, 361(23), 2209-2220.Robertson M., Mehrotra D., Fitzgerald D., et al. (2008, February). Efficacy results from the STEP study (Merck V520 Protocol 023/HVTN
502): A phase II test-of-concept trial of the MRKAd5 HIV-1 Gag/Pol/Nef trivalent vaccine. 15th Conference on Retroviruses and Opportunistic Infections, Boston, MA.
Rotheram-Borus, M. J., Swendeman, D., & Chovnick, G. (2009). The past, present, and future of HIV prevention: Integrating behavioral, biomedical, and structural intervention strategies for the next generation of HIV prevention. Annu Rev Clin Psychol, 5, 143-167.
Turner, A. N., Morrison, C. S., Padian, N. S., Kaufman, J. S., Salata, R. A., Chipato, T., et al. (2007). Men's circumcision status and women's risk of HIV acquisition in Zimbabwe and Uganda. AIDS, 21(13), 1779-1789.
Weiss, H. A., Halperin, D., Bailey, R. C., Hayes, R. J., Schmid, G., & Hankins, C. A. (2008). Male circumcision for HIV prevention: From evidence to action? AIDS, 22(5), 567-574.
Williams, B. G., Lloyd-Smith, J. O., Gouws, E., Hankins, C., Getz, W. M., Hargrove, J., et al. (2006). The potential impact of male circumcision on HIV in sub-Saharan Africa. PLoS Med, 3(7), e262.
World Health Organization. (2009). Towards universal access: Progress report (Key Messages). Switzerland, WHO HIV/AIDS Department.

ReferencesAccess Working Group. (n.d.). Preparing for Microbicide Access and Use. Microbicide Initiative,
Rockefeller Foundation. Retrieved from http://www.global-campaign.org/clientfiles/rep6_preparing.pdfAIDS Partnership California. (2009). Pre-Exposure Prophylaxis and HIV Prevention: Assessing Community
Needs and Preparedness in California.Al-Tayyib, A., Voetsch, A. C., Thrun, M. W., Herbst, J. H., Carey, J. W., DiNenno, E., & Smith, D. K. (2009).
Knowledge and attitudes about PrEP for HIV prevention among men who have sex with men. Presented at the 2009 National HIV Prevention Conference, Atlanta, GA.
Barrington, C., Moreno, L., & Kerrigan, D. (2008). Perceived influence of an HIV vaccine on sexual-risk behaviour in the Dominican Republic. Culture, Health & Sexuality, 10(4), 391-401. doi:10.1080/13691050801898877
Bartholow, B. N., Buchbinder, S., Celum, C., Goli, V., Koblin, B., Para, M., Marmor, M., et al. (2005). HIV sexual risk behavior over 36 months of follow-up in the world's first HIV vaccine efficacy trial. Journal of Acquired Immune Deficiency Syndromes, 39(1), 90-101.
Carballo-Diéguez, A., Bauermeister, J. A., Ventuneac, A., Dolezal, C., Balan, I., & Remien, R. H. (2007). The Use of Rectal Douches among HIV-uninfected and Infected Men who Have Unprotected Receptive Anal Intercourse: Implications for Rectal Microbicides. AIDS and Behavior, 12(6), 860-866. doi:10.1007/s10461-007-9301-0
Chesney, M. A., Chambers, D. B., & Kahn, J. O. (1997). Risk behavior for HIV infection in participants in preventive HIV vaccine trials: a cautionary note. Journal of Acquired Immune Deficiency Syndromes, 16(4), 266-271.
Clauson, K. A., Polen, H. H., Joseph, S. A., & Zapantis, A. (2009). Role of the pharmacist in pre-exposure chemoprophylaxis (PrEP) therapy for HIV prevention. Pharmacy Practice (Internet), 7(1), 11-18.
Cohen, M. S., Kaleebu, P., & Coates, T. (2008). Prevention of the sexual transmission of HIV-1: preparing for success. Journal of the International AIDS Society, 11, 4. doi:10.1186/1758-2652-11-4
Crosby, R. A., & Holtgrave, D. R. (2006). Will sexual risk behaviour increase after being vaccinated for AIDS? International Journal of STD & AIDS, 17(3), 180-184.
Eaton, L. A., & Kalichman, S. C. (2007). Risk compensation in HIV prevention: implications for vaccines, microbicides, and other biomedical HIV prevention technologies. Current HIV/AIDS Reports, 4(4), 165–172.
Global HIV Prevention Working Group. (2006). New Approaches to HIV Prevention: Accelerating Research and Ensuring Future Access. Global HIV Prevention Working Group. Retrieved from http://www.globalhivprevention.org/pdfs/New%20Prevention%20Approaches.pdf

Referencesvan Griensven, F., Keawkungwal, J., Tappero, J. W., Sangkum, U., Pitisuttithum, P., Vanichseni, S.,
Suntharasamai, P., et al. (2004). Lack of increased HIV risk behavior among injection drug users participating in the AIDSVAX (R) B/E HIV vaccine trial in Bangkok, Thailand. AIDS, 18, 295-301.
Guest, G., Shattuck, D., Johnson, L., Akumatey, B., Kekawo Clarke, E. E., Chen, P. L., & MacQueen, K. M. (2008). Changes in sexual risk behavior among participants in a PrEP HIV prevention trial. Sexually Transmitted Diseases, 35(12), 1002-1008.
Imrie, J., Elford, J., Kippax, S., & Hart, G. J. (2007). Biomedical HIV prevention—and social science. Lancet, 370, 10–11.
Kellerman, S. E., Hutchinson, A. B., Begley, E. B., Boyett, B. C., Clark, H. A., & Sullivan, P. (2006). Knowledge and use of HIV pre-exposure prophylaxis among attendees of minority gay pride events, 2004. Journal of Acquired Immune Deficiency Syndromes, 43(3), 376-377.
Kippax, S. (2008). Understanding and integrating the structural and biomedical determinants of HIV infection: a way forward for prevention. Current Opinion in HIV and AIDS, 3(4), 489-494.
Koo, H. P., Woodsong, C., Dalberth, B. T., Viswanathan, M., & Simons-Rudolph, A. (2005). Context of Acceptability of Topical Microbicides: Sexual Relationships. Journal of Social Issues, 61(1), 67-93. doi:10.1111/j.0022-4537.2005.00394.x
Krüsi, A., Wood, E., Montaner, J., & Kerr, T. (2010). Social and structural determinants of HAART access and adherence among injection drug users. International Journal of Drug Policy, 21, 4-9.
Lampinen, T. M., Chan, K., Remis, R. S., Merid, M. F., Rusch, M., Vincelette, J., Logue, K., et al. (2005). Sexual risk behaviour of Canadian participants in the first efficacy trial of a preventive HIV-1 vaccine. Canadian Medical Association Journal, 172(4), 479-483.
Lunding, S., Katzenstein, T. L., Kronborg, G., Lindberg, J. Å., Jensen, J., Nielsen, H. I., Pedersen, C., et al. (2010). The Danish PEP Registry: Experience With the Use of Postexposure Prophylaxis (PEP) Following Sexual Exposure to HIV From 1998 to 2006. Sexually Transmitted Diseases, 37(1), 49-52. doi:10.1097/OLQ.0b013e3181b6f284
Mansergh, G., Marks, G., Rader, M., Colfax, G. N., & Buchbinder, S. (2003). Rectal use of nonoxynol-9 among men who have sex with men. AIDS, 17, 905-909.
Mansergh, G., Colfax, G., McKirnan, D., Koblin, B., Flores, S., Hudson, S., & Project MIX Study Group. (2010). Use and Sharing of Antiretroviral Medications for Pre- and Post-exposure Prophylaxis to Prevent Sexual Transmission of HIV among High-risk, Substance-using Men Who Have Sex with Men in 4 US Cities. Presented at the 17th Conference on Retroviruses and Opportunistic Infections, San Francisco, CA.
Mantell, J. E., Dworkin, S. L., Exner, T. M., Hoffman, S., Smit, J. A., & Susser, I. (2006). The promises and limitations of female-initiated methods of HIV/STI protection. Social Science & Medicine, 63(8), 1998–2009.
Mantell, J. E., Morar, N. S., Myer, L., & Ramjee, G. (2006). "We Have Our Protector": Misperceptions of Protection Against HIV Among Participants in a Microbicide Efficacy Trial. American Journal of Public Health, 96(6), 1073-1077. doi:10.2105/AJPH.2004.047514

ReferencesMartin, J. N., Roland, M. E., Neilands, T. B., Krone, M. R., Bamberger, J. D., Kohn, R. P., Chesney, M. A., et
al. (2004). Use of postexposure prophylaxis against HIV infection following sexual exposure does not lead to increases in high-risk behavior. AIDS, 18(5), 787.
Mimiaga, M. J., Case, P., Johnson, C. V., Safren, S. A., & Mayer, K. H. (2009). Preexposure Antiretroviral Prophylaxis Attitudes in High-Risk Boston Area Men Who Report Having Sex With Men: Limited Knowledge and Experience but Potential for Increased Utilization After Education. Journal of Acquired Immune Deficiency Syndromes, 50(1), 77-83. doi:10.1097/QAI.0b013e31818d5a27
Newman, P. A., Duan, N., Kakinami, L., & Roberts, K. (2008). What can HIV vaccine trials teach us about future HIV vaccine dissemination? Vaccine, 26(20), 2528–2536.
Newman, P. A., Lee, S., Duan, N., Rudy, E., Nakazono, T. K., Boscardin, J., Kakinami, L., et al. (2009). Preventive HIV Vaccine Acceptability and Behavioral Risk Compensation among a Random Sample of High-Risk Adults in Los Angeles (LA VOICES). Health Services Research, 44(6), 2167-2179. doi:10.1111/j.1475-6773.2009.01039.x
Nodin, N., Carballo-Diéguez, A., Ventuneac, A. M., Balan, I. C., & Remien, R. (2008). Knowledge and acceptability of alternative HIV prevention bio-medical products among MSM who bareback. AIDS Care, 20(1), 106-115. doi:10.1080/09540120701449096
Padian, N. S., Buvé, A., Balkus, J., Serwadda, D., & Cates, W. (2008). Biomedical interventions to prevent HIV infection: evidence, challenges, and way forward. Lancet, 372, 585-599.
Paxton, L. A., Hope, T., & Jaffe, H. W. (2007). Pre-exposure prophylaxis for HIV infection: what if it works? Lancet, 370(9581), 89–93.
Pinkerton, S. D., Holtgrave, D. R., & Bloom, F. R. (1998). Cost-effectiveness of post-exposure prophylaxis following sexual exposure to HIV. AIDS, 12(9), 1067-1078.
Poynten, I., Smith, D., Kaldor, J., & Grulich, A. (2007). The public health impact of widespread availability of nonoccupational postexposure prophylaxis against HIV. HIV Medicine, 8, 374-381.
Pozniak, A. (2004). Post-exposure prophylaxis for sexual exposure to HIV. Current Opinion in Infectious Diseases, 17(1), 39-40.
Rhodes, S. D., & Hergenrather, K. C. (2002). Exploring hepatitis B vaccination acceptance among young men who have sex with men: Facilitators and barriers. Preventive Medicine, 35, 128-134.
Roedling, S., Reeves, I., Copas, A. J., Beattie, A., Edwards, S. G., Fisher, M., & Benn, P. (2008). Changes in the provision of post-exposure prophylaxis for HIV after sexual exposure following introduction of guidelines and publicity campaigns. International Journal of STD & AIDS, 19(4), 241-242.

ReferencesRosengarten, M., Michael, M., Mykhalovskiy, E., & Imrie, J. (2008). The challenges of technological innovation in HIV.
Lancet, 372, 356–357.
Rudy, E. T., Newman, P. A., Duan, N., Kelly, E. M., Roberts, K. J., & Seiden, D. S. (2005). HIV vaccine acceptability among women at risk: Perceived barriers and facilitators to future HIV vaccine uptake. AIDS Education and Prevention, 17(3), 253-267.
Russell D. Ravert, & Gregory D. Zimet. (2009). College student invulnerability beliefs and HIV vaccine acceptability. American Journal of Health Behavior, 33(4), 391-399.
Salazar, L. F., Holtgrave, D., Crosby, R. A., Frew, P., & Peterson, J. L. (2005). Issues related to gay and bisexual men's acceptance of a future AIDS vaccine. International Journal of STD & AIDS, 16(8), 546-548.
Sayer, C., Fisher, M., Nixon, E., Nambiar, K., Richardson, D., Perry, N., & Llewellyn, C. (2008). Will I? Won't I? Why do men who have sex with men present for post-exposure prophylaxis for sexual exposures? Sexually Transmitted Infections, 85(3), 206-211. doi:10.1136/sti.2008.033662
Schechter, M., do Lago, R. F., Mendelsohn, A. B., Moreira, R. I., Moulton, L. H., & Harrison, L. H. (2004). Behavioral impact, acceptability, and HIV incidence among homosexual men with access to postexposure chemoprophylaxis for HIV. Journal of Acquired Immune Deficiency Syndromes, 35(5), 519-525.
Severy, L. J., Tolley, E., Woodsong, C., & Guest, G. (2005). A Framework for Examining the Sustained Acceptability of Microbicides. AIDS and Behavior, 9(1), 121-131. doi:10.1007/s10461-005-1687-y
Shoptaw, S., Rotheram-Fuller, E., Landovitz, R. J., Wang, J., Moe, A., Kanouse, D. E., & Reback, C. (2008). Non-occupational post exposure prophylaxis as a biobehavioral HIV-prevention intervention. AIDS Care, 20(3), 376-381. doi:10.1080/09540120701660353
Sonder, G. J. B., van den Hoek, A., Regez, R. M., Brinkman, K., Prins, J. M., Mulder, J., Veenstra, J., et al. (2006). Trends in HIV Postexposure Prophylaxis Prescription and Compliance After Sexual Exposure in Amsterdam, 2000-2004. Sexually Transmitted Diseases, 34(5), 288-293. doi:10.1097/01.olq.0000237838.43716.ee
Thurman, A. R., Holden, A. E. C., Shain, R. N., Perdue, S., & Piper, J. M. (2009). Effect of Acculturation on the Acceptability of Potential Microbicides and Sexual Risk-Taking. Sexually Transmitted Diseases, 36(6), 387-394. doi:10.1097/OLQ.0b013e318198d90c
Vermund, S. H., Allen, K. L., & Karim, Q. A. (2009). HIV-prevention science at a crossroads: advances in reducing sexual risk. Current Opinion in HIV and AIDS, 4(4), 266-273.
Waldo, C. R., Stall, R. D., & Coates, T. J. (2000). Is offering post-exposure prevention for sexual exposures to HIV related to sexual risk behavior in gay men? AIDS, 14(8), 1035.
Webb, P. M., Zimet, G. D., Mays, R., & Fortenberry, J. D. (1999). HIV immunization: acceptability and anticipated effects on sexual behavior among adolescents. Journal of Adolescent Health, 25(5), 320–322.
Woodsong, C. (2004). Covert use of topical microbicides: Implications for acceptability and use. Perspectives on Sexual and Reproductive Health, 36(3), 127-131.