preoperative preparation of patients for thoracic surgery
TRANSCRIPT


CONTENTS
Preface xiRichard I. Whyte
Smoking Cessation: Techniques and Potential Benefits 189Tomasz M. Ziedalski and Stephen J. Ruoss
Tobacco smoking significantly increases the risk of perioperative and postoperative com-plications. Observational evidence suggests that preoperative smoking cessation maydecrease the risk of certain complications. Smoking cessation programs that employbehavioral and cognitive therapy and pharmacotherapy have been used successfully inmany situations and should be used to discourage smoking preoperatively. Further eval-uation of the effectiveness of particular types of interventions is needed to clarify the bestapproach to smoking cessation for surgical patients.
Preoperative Patient Education in Thoracic Surgery 195 Richard I. Whyte and Patricia D. Grant
This article describes the role of preoperative teaching in thoracic surgery. Preoperativepatient teaching may take many forms and is offered to patients across many venues andformats. The goal of patient teaching is to improve patients’ understanding of their dis-ease process and the operation that they are about to experience with the goal of enlist-ing their active participation in the healing process. The additional goal of obtaininginformed consent is not only codified in law, but also has become an ingrained compo-nent to the current physician-patient relationship. The preoperative teaching process isbest approached as a team effort, and multiple modalities often must be used so that thepatient becomes a knowledgeable and willing member of the team.
The Value of Preoperative Pulmonary Rehabilitation 203Shanon T. Takaoka and Ann B. Weinacker
Although pulmonary rehabilitation is potentially beneficial before any surgery, it hasbeen applied and studied primarily in the setting of major thoracic surgical procedures,including lung volume reduction surgery, lung transplantation, and lung resection. Thisarticle defines the essential elements of pulmonary rehabilitation, outlines the prerequi-sites for enrollment, and discusses its current role in the setting of anticipated thoracicsurgery. Pulmonary rehabilitation seems to be a cost-effective, benign intervention withno adverse effects and should remain an essential component of patient managementbefore lung transplantation, lung volume reduction surgery, lung resection, and poten-tially any other elective thoracic surgical procedure.
PREOPERATIVE PREPARATION OF PATIENTS FOR THORACIC SURGERY
VOLUME 15 • NUMBER 2 • MAY 2005 v

Informed Consent: Ethical and Legal Aspects 213Carole A. Klove, Sarah J. DiBoise, Betty Pang, and William C. Yarbrough
The doctrine of informed consent serves the dual function of promoting the beneficence,benevolence, and nonmalfeasance of the physician and the autonomy, bodily integrity,and self-determination of the patient. Conflict arises when a patient’s individual libertyrights clash with a physician’s medical conclusions formed in the patient’s perceivedbest interest. This article explores the ethical and legal nuances of the doctrine ofinformed consent in an attempt to empower the provider with a deeper understandingof the physician’s rights and responsibilities in obtaining a true informed consent.
Fast-Tracking: Eliminating Roadblocks to Successful Early Discharge 221Jules Lin and Mark D. Iannettoni
This article describes common obstacles to successful early discharge that face many thoracic surgeons despite technically successful procedures; these obstacles includeinadequate pain control, prolonged air leaks, and social issues. With continually increas-ing health care costs and limited resources, identifying the factors that affect length ofstay has taken on new importance. Potential solutions that also maintain the quality ofpatient care are discussed and include the use of minimally invasive techniques, opti-mizing pain control, early mobilization, discharge planning, patient education, and thedevelopment of clinical pathways.
Perioperative Antibiotics: When, Why? 229Mark S. Allen
The use of prophylactic antibiotics in general thoracic surgery is well established. Thisarticle explains the rationale for modern-day surgical wound infection prophylaxis, thewhy and the when. Various arguments about the use of antibiotics to prevent empyemaand pneumonia after a thoracic operation also are presented.
Pulmonary Embolism Prophylaxis: Evidence for Utility in Thoracic Surgery 237Dean M. Donahue
Patients requiring thoracotomy for the treatment of malignancy are at risk for develop-ing a pulmonary embolism. Few data exist on effective prophylaxis techniques in thisspecific patient population, yet effective strategies can be inferred from other major sur-gical procedures to reduce the risk of this potentially life-threatening complication.
Management of the Anticoagulated Patient 243Mark H. Meissner and Riyad Karmy-Jones
Patients who are to undergo surgery may be anticoagulated for therapeutic reasons(eg, deep venous thrombosis, valve replacement, lytic therapy) or because of comorbidconditions (eg, renal or hepatic failure). In addition, the proposed operative interventionmay be elective or urgent. The approach to managing the coagulation status is criticallyaffected by the circumstances and requires a basic understanding of the risks involved ofbleeding and correcting the underlying pathophysiology. This article reviews the indica-tions, pharmacology, and complications of common anticoagulation therapies (includinglaboratory and clinical assessment) in the surgical patient.
vi CONTENTS
Preoperative Cardiac Evaluation: Mechanisms, Assessment, and Reduction of Risk 263Euan A. Ashley and Randall H. Vagelos
Considerable uncertainty exists as to when it is appropriate to investigate cardiac disease ina preoperative thoracic patient and which tools are best suited to the task. Common diseaseorigins, commonality of symptoms, and coexistent disease all serve to make accurate diag-nosis and effective risk prediction difficult. Interventions known to reduce risk and savelives are few. This article explores the basis for anesthetic risk in cardiovascular and pul-monary disease. Common disease mechanisms and the utility of tools available to assess riskare discussed. Risk reduction also is discussed, and recommendations specific to the pre-operative cardiac evaluation of the thoracic surgery patient are offered.
Preoperative Preparation for Esophageal Surgery 277Jessica Scott Donington
Esophageal surgeries can be placed into two broad categories: anatomic modificationsfor benign esophageal disorders and resections for carcinomas. The clinical setting andscope of intervention are different for these two groups, as is the preoperative prepara-tion. The goal of preoperative evaluation for benign esophageal disease is to make anaccurate and complete diagnosis; the tools for this include barium esophagogram,endoscopy, pH monitoring, and manometry. The preoperative concerns for esophagealresection for cancer involve accurate staging of the cancer, using CT, positron emissiontomography, and endoscopic ultrasound, and complete physiologic evaluation of thepatient to determine his or her ability to withstand a large operation.
Preoperative Preparation of the Patient with Myasthenia Gravis 287Kemp H. Kernstine
The morbidity and mortality of patients with myasthenia gravis undergoing thymectomycan be substantial. The surgeon must have a thorough knowledge of the evaluation andtests necessary to confirm a diagnosis and should not rely totally on the neurologist’sassessment. Through partnership with the neurologist, the ideal means of medical andsurgical management can be achieved.
Preoperative Pulmonary Evaluation of the Thoracic Surgical Patient 297Aditya K. Kaza and John D. Mitchell
Surgery remains the mainstay of therapy for early-stage non-small lung cancer. Manypatients have poor underlying pulmonary function, in large part resulting from long-termtobacco abuse. It is the responsibility of the thoracic surgeon to assess accurately the pul-monary function of a potentially operable patient at the time of the preoperative evaluation.This assessment provides an objective risk profile associated with the planned pulmonaryresection for the patient and family, minimizes morbidity and mortality, and in some casesleads the surgeon to recommend alternative therapies. This article provides a systematicapproach to the pulmonary evaluation of the thoracic surgical patient.
The Preoperative Anesthesia Evaluation 305Clifford A. Schmiesing and Jay B. Brodsky
Timely and thorough preoperative assessment is a cornerstone of excellent patientoutcomes and efficient use of medical resources. This article focuses on the importantelements of the preoperative anesthetic assessment of a patient presenting for thoracic
CONTENTS vii

surgery. Areas of shared concern between the surgeon and anesthesiologist areemphasized. Cardiovascular risk assessment and preoperative management are high-lighted because cardiorespiratory complications are the major causes of morbidityafter thoracic surgery. Practical and simple strategies for common preoperative issues,including medications and diagnostic testing, are provided, and the benefits of a com-prehensive anesthesia preoperative assessment are discussed.
Index 317
viii CONTENTS

FORTHCOMING ISSUES
August 2005
New Treatments for Gastroesophageal Reflux DiseaseClaude Deschamps, MD, Guest Editor
November 2005
Ethics in Thoracic SurgeryRobert M. Sade, MD, Guest Editor
RECENT ISSUES
February 2005
Advances in Anesthesia and Pain ManagementJerome M. Klafta, MD, Guest Editor
November 2004
MesotheliomaDavid J. Sugarbaker, MD, andMichael Y. Chang, MD, Guest Editors
August 2004
Quality of Life After Thoracic SurgeryAnthony P.C. Yim, MD, Guest Editor
May 2004
Aggressive Surgery for Lung Cancer Valerie W. Rusch, MD, Guest Editor
THE CLINICS ARE NOW AVAILABLE ONLINE!
Access your subscription at:http://www.theclinics.com

Thorac Surg
Preface
Preoperative Preparation of Patients for Thoracic Surgery
Richard I. Whyte, MD
Guest Editor
The preoperative preparation of patients for tho-
racic surgery is complex and involves individuals
from diverse subspecialties within the field of
medicine. This issue of the Thoracic Surgery Clinics
focuses on these interrelationships through contri-
butions from the fields of nursing, law, pulmonary
medicine, cardiology, and anesthesia, in addition to
thoracic surgery. Although several of the authors
are from Stanford University, I have attempted to
provide some diversity in both geographical location
and specialty training in the selection of authors for
this issue.
Because thoracic surgery encompasses a wide
range of pathologic entities, I have attempted to cover
ground that is common to many patients and disease
processes (anesthetic concerns, preoperative teaching,
legal issues of informed consent, smoking cessation,
preoperative cardiac evaluation, antibiotic and deep
venous thrombosis prophylaxis), as well as more
1547-4127/05/$ – see front matter D 2005 Elsevier Inc. All rights
doi:10.1016/j.thorsurg.2005.03.008
specific issues such as pulmonary rehabilitation, my-
asthenia gravis, esophageal surgery, and fast-tracking
in lung surgery.
I would like to thank the authors who contri-
buted to this issue, because they contributed consider-
able amounts of time in preparing these manuscripts.
I would also like to thank Dr. Mark Ferguson
for giving me the opportunity to put this piece
of collaborative work together. I hope that the
readers find it interesting and valuable, and I
would be happy to receive any feedback on any
of the contributions.
Richard I. Whyte, MD
Department of Cardiothoracic Surgery
Stanford University Medical Center
300 Pasteur Dr, CVRB 205
Stanford, CA 94305, USA
E-mail address: [email protected]
Clin 15 (2005) xi
reserved.
thoracic.theclinics.com
Thorac Surg Clin
Smoking Cessation: Techniques and Potential Benefits
Tomasz M. Ziedalski, MD, Stephen J. Ruoss, MD*
Division of Pulmonary and Critical Care Medicine, Stanford University School of Medicine, 300 Pasteur Drive,
H3143, Stanford, CA 94305, USA
Cigarette smoking is the leading preventable
cause of death in the United States and is responsible
for 20% of all deaths, or more than 400,000 deaths
annually [1]. The potential health benefits of smoking
cessation are substantial. Smoking cessation reduces
the risk and slows the progression of already estab-
lished smoking-related lung disease and increases life
expectancy, even when smokers stop smoking after
age 65 years or after the development of a tobacco-
related disease [2].
Each year, 10% of the general population may
undergo surgery with general anesthesia. Although
complications rates vary with the type of surgery per-
formed and the patient’s underlying health status,
pulmonary and cardiovascular complications occur in
10% of the cases [3]. Because smokers have a sixfold
increase in intraoperative and postoperative complica-
tions, efforts directed at reducing smoking prevalence
in prospective surgical patients might be beneficial
in reducing perioperative medical problems [4].
Effects of cigarette smoke
Smoking has multiple effects on the pulmonary
and cardiovascular systems and on wound healing.
In a large retrospective study, specific respiratory
events, such as reintubation, laryngospasm, broncho-
1547-4127/05/$ – see front matter D 2005 Elsevier Inc. All rights
doi:10.1016/j.thorsurg.2005.02.003
The authors have no relationship with any commercial
company that has a direct financial interest in the subject
matter of this article. No funding support was received for
this article.
* Corresponding author.
E-mail address: [email protected] (S.J. Ruoss).
spasm, aspiration, hypoventilation, and hypoxemia,
were significantly increased among smokers, with
the relative risks of 1.8 in all smokers, 2.3 in young
(16–39 years old) smokers, and 6.3 in obese young
smokers [5]. The relative risk of perioperative bron-
chospasm was 25.7 in young smokers with chronic
bronchitis [5].
Smoking causes increased mucus production and
damage to the tracheal cilia, leading to decreased
mucus clearance [6]. The combination of decreased
mucus clearance and tobacco smoke–induced im-
pairment of immune function may lead to an in-
creased risk of pulmonary infections [7,8].
Surgery itself is associated with reduced pul-
monary function. This reduced function is observed
predominantly in thoracic and abdominal surgery,
in which atelectasis and diaphragmatic dysfunction
lead to significant reduction in vital capacity and
functional residual capacity [9]. Pulmonary function
impairment is further accentuated among smokers.
Smoking cessation can result in improvement in
maximal expiratory flow rates and closing volumes
[10,11].
Smoking has many effects on cardiac and vascular
function. Short-term effects of smoking are secondary
to increased amounts of carbon monoxide and nico-
tine in the serum. The binding of carbon monoxide to
hemoglobin can reduce the oxygen availability to
peripheral tissues by 12% [7]. It changes the structure
of the hemoglobin molecules, shifting the oxygen-
hemoglobin curve to the left, further reducing oxygen
availability. Carboxyhemoglobin levels of 6% have
been shown to increase significantly the risk of ven-
tricular arrhythmias among patients with coronary
artery disease [12]. By stimulating the stress re-
sponse to surgery, nicotine together with carbon mon-
15 (2005) 189 – 194
reserved.
thoracic.theclinics.com

ziedalski & ruoss190
oxide creates an oxygen availability and consump-
tion imbalance.
Nicotine affects coronary vascular resistance and
blood flow. The effects of nicotine on coronary blood
flow include indirect vasodilatory effects by mecha-
nisms related to the increased cardiac work and direct
coronary vasoconstrictor effects [13,14]. The effects
of nicotine replacement therapy on oxygen consump-
tion are not well understood [15].
The association between cigarette smoking and
delayed wound healing is well recognized in clinical
practice, but controlled studies are limited [16–18].
Although the mechanisms are not established, the
effects of the toxic constituents of cigarette smoke,
such as nicotine, carbon monoxide, and hydrogen
cyanide, are potential mechanisms by which smoking
may impair wound repair. Nicotine’s vasoconstrictor
properties may reduce nutritional blood flow to the
skin, resulting in tissue ischemia and impaired
healing of injured tissue. Nicotine increases plate-
let adhesiveness, potentially increasing the risk of
thrombotic microvascular occlusion and tissue ische-
mia. Carbon monoxide and hydrogen cyanide can
contribute further to tissue hypoxemia and inadequate
healing [17]. In addition, the synthesis of subcuta-
neous collagen in smokers is impeded, indicating an
impaired wound healing process [19].
Smoking cessation in the preoperative period
The potential dangers of operative complications
resulting from smoking have been recognized since
the 1940s. In 1944, Morton [20] stated: ‘‘. . . the
morbidity rate for smokers taking more than 10 ciga-
rettes a day is 6 times that for non-smokers . . . it isadvisable for smokers to stop or reduce their smoking
as a precaution against pulmonary complications.’’
Whether preoperative smoking cessation can
reduce the incidence of perioperative and postop-
erative complications is not established. In an un-
controlled observational study of 200 consecutive
patients undergoing elective coronary artery bypass
graft surgery, an association between preoperative
smoking cessation and postoperative pulmonary
morbidity was examined [21]. Postoperative pulmo-
nary complications occurred in one third of the ac-
tive smokers. Patients who had stopped smoking for
2 months or less had a pulmonary complication rate
almost four times that of patients who had stopped for
more than 2 months (57.1% versus 14.5%). Patients
who had stopped smoking for more than 6 months
had rates similar to patients who had never smoked
(11.1% and 11.9%). Preoperative pulmonary dys-
function, increased pack-years of smoking, and
prolonged surgical time were independently and sta-
tistically significantly associated with postoperative
pulmonary morbidity.
This landmark study suggests that smoking ces-
sation should occur at least 8 weeks before surgery
to maximize the reduction of postoperative respira-
tory complications [21]. In addition, because smok-
ing-induced reduction in lung function and the
impairment of immune function may be significantly
reversed by 6 to 8 weeks of abstinence, smoking
cessation interventions are likely to be more benefi-
cial when offered at least 6 weeks before surgery
rather than in the immediate preoperative period
[11,22]. Such timely interventions may be difficult
to achieve unless there is a partnership between sur-
geons and referring physicians. Currently, no ran-
domized trials have assessed the role of preoperative
smoking cessation on perioperative and postoperative
outcomes. A Cochrane review assessed the evidence
for an effect of preoperative smoking intervention on
smoking cessation in the postoperative period and
longer term and on the incidence of postoperative
complications [23]. Although no randomized, con-
trolled data exist for the role of preoperative smoking
cessation, some limited studies have attempted to
answer this question.
A prospective nonrandomized trial designed to
evaluate the effectiveness of written preoperative
advice to stop smoking before admission for elective
surgery showed that such advice was ineffective in
persuading patients to stop smoking. Fifteen percent
of all patients continued to smoke within 1 hour of
surgery, but there was a reduction in the amount of
tobacco consumed [24].
Another small study evaluated a smoking cessa-
tion program, implemented by a nurse in surgical
preadmission clinics [25]. Sixty smokers were ran-
domized into two groups. When attending the pre-
operative clinic, patients in the treatment group
received educational interventions and self-assess-
ment questionnaires relating to smoking cessation,
whereas patients in the control group received routine
information. There was a significant increase in posi-
tive behavior on admission to the hospital in the
treatment group (80% stopped or reduced smoking)
compared with the control group (50% stopped or
reduced smoking), particularly in patients who did
not intend to reduce or stop before admission. Pa-
tients described the approach of the nurse and a leaf-
let devised for the study as the most helpful aspects
of the program. The lack of blinding in this study
limits the applicability of the data, but the approach
to smoking cessation warrants more investigation.

smoking cessation 191
Although it is desirable that smoking cessation
should occur in the preoperative period, it is unclear
if this is the most suitable time for most patients.
Patients may be more likely to comply with smoking
cessation advice during the time of an acute illness
because the possibility of reducing perceived vulnera-
bility to postoperative complications could promote
patient motivation to quit or reduce smoking before
operation. Interventions such as consulting and phar-
macotherapy help patients to stop smoking in mul-
tiple settings and should work in the perioperative
period. Although some patients tend to be more ner-
vous about smoking cessation before surgery because
they might feel that they need to smoke to deal with
the stress of impending surgery, a successful preop-
erative smoking intervention potentially could reduce
perioperative complications and lead to long-term
health gains.
Smoking cessation during the perioperative period
In a prospective, randomized trial of patients
with a diagnosis of cancer who were hospitalized
for a surgical procedure, a one-time, inpatient, nurse-
managed, minimal smoking cessation intervention
was assessed for effectiveness on smoking cessation
[26]. On hospital admission, 64% of the intervention
group and 71% of the usual care group reported their
intention to quit smoking. At 6 weeks postinterven-
tion, only 21% of the intervention group and 14% of
the usual care group were abstinent from smoking.
More than 90% of the intervention group members
who resumed smoking did so within the first week
of discharge. Additional contact before discharge or
within the first few days after discharge may be
necessary to reinforce strategies for remaining absti-
nent [26].
A Veterans Affairs Medical Center randomized,
controlled trial of 324 patients hospitalized for non-
cardiac surgery assessed the effectiveness of an in-
tervention during that hospitalization. Of patients,
52% were randomized into an intervention group
consisting of a multicomponent intervention designed
to increase self-efficacy and coping skills that in-
cluded face-to-face in-hospital counseling, viewing
a smoking cessation videotape, self-help literature,
nicotine replacement therapy, and 3 months of tele-
phone follow-up. The remaining 48% of patients
received self-help literature and brief counseling
lasting 10 minutes. Serum or saliva cotinine levels
were measured to confirm self-reported smoking ces-
sation. At 12 months of follow-up, the self-reported
quit rate was 27% among the intervention group and
13% among the comparison group (relative risk 2.1;
95% confidence interval 1.2–3.5; P < .01). Based on
biochemical confirmation, 15% of the intervention
group compared with 8% of the comparison group
were not smoking at 12 months (relative risk 2; 95%
confidence interval 1–3.9; P = .04) [27].
In another study designed to examine the effect of
a nurse-delivered smoking cessation intervention on
short-term smoking abstinence among hospitalized
postoperative patients, 80 patients were prospectively
randomized. The intervention consisted of three
structured smoking cessation sessions during hos-
pitalization, followed by phone calls once a week
for 5 weeks after discharge. Of the experimental
group, 37.8% of patients were abstinent compared
with 25.6% in the usual care group. Abstinence rates
of experimental group patients from cardiovascular
(40%) and oncology (64.3%) units were higher than
that of general surgery (13.3%) patients. Regardless
of group assignment, 100% of cardiovascular and
oncology patients abstained during hospitalization
compared with only 10.7% of general surgery pa-
tients [28].
A systematic review of all trials of behavioral,
pharmacologic, or multicomponent interventions de-
signed to help hospitalized patients with smoking
cessation showed that intensive intervention con-
sisting of inpatient contact with at least 1 month of
follow-up was associated with significantly higher
cessation rates (odds ratio 1.82; 95% confidence in-
terval, 1.49–2.22) [29]. Any contact during hospitali-
zation with a minimal follow-up failed to show any
significant effect on abstinence.
Therapeutic approaches to smoking cessation
Currently, more than 23% of United States adults
smoke cigarettes, and 70% of smokers report a desire
to quit [30]. Smoking should be viewed as a chronic
disease that requires a long-term management strat-
egy, rather than a quick and easy treatment [31].
Fewer than 10% of smokers who attempt to quit on
their own are successful over the long-term. Smokers
who seek professional help are more successful
[2,31]. The main obstacle to quitting is the addictive
nature of nicotine.
Counseling and pharmacotherapy are effective in
smoking cessation, but the combination of the two
achieves the best results [31,32]. Randomized, con-
trolled trials have shown that a physician’s advice to
stop tobacco smoking increased the rates of cessation
by 30% [32]. Formal counseling sessions, even brief
ones lasting less than 3 minutes, are more effective

ziedalski & ruoss192
than simple advice. Counseling can be performed in a
group setting and usually employs cognitive behav-
ioral methods with which smokers learn to identify
behavioral clues and learn how to cope with stress
and manage symptoms of nicotine withdrawal. Pa-
tients also develop the skills necessary to prevent
relapse [2].
Many pharmacologic approaches are available for
smoking cessation. Nicotine replacement with gum, a
transdermal patch, a nasal spray, and a vapor inhaler
all have shown efficacy in randomized, double-blind
placebo trials and are associated with a doubling
of the long-term (1-year) rates of abstinence [32,33].
The pharmacokinetic properties of the available
nicotine formulations differ, with the patch providing
a stable, fixed dose of nicotine over 16 or 24 hours,
whereas the other formulations have a more rapid
onset and a shorter duration of action.
The goal of nicotine replacement therapy is to
relieve the craving for nicotine and the symptoms of
nicotine withdrawal. One randomized, controlled trial
directly compared the four nicotine replacement
products [34]. Although the efficacy of each product
was similar at week 12 of follow-up, the rates of
compliance varied, being highest for the patch, inter-
mediate for the gum, and lowest for the vapor inhaler
and the nasal spray. Different nicotine replacement
products can be combined safely, and combining the
nicotine patch with gum, inhaler, or nasal spray was
more efficacious than the use of any of these products
alone [32,35]. Nicotine replacement therapy is gen-
erally safe in patients with cardiovascular disease
[36,37]. Although it has not been studied in patients
with unstable angina or recent myocardial infarction,
the risks of nicotine replacement should be lower than
in cigarette smoking [2,15]. In smokers with high
Table 1
Pharmacologic therapy for smoking cessation
Nicotine replacement therapy Product name
Transdermal patch Nicoderm
Nicotrol
Nicotine gum Nicorette
Nasal spray Nicotrol NS
Inhaler Nicotrol Inhaler
Nonnicotine therapy
Bupropion Zyban
Wellbutrin SR
Nortriptyline Aventyl
Pamelor
Clonidine Catapres
nicotine dependence, higher levels of nicotine
replacement may be necessary. This replacement
can be achieved by multiple patches and sometimes
additional amounts of polacrilex gum, nasal spray, or
nicotine inhaler [38,39]. Although specific nicotine
receptor antagonists are not yet available commer-
cially, the role of these agents is under investigation
[40,41].
Besides nicotine replacement therapy, other phar-
macotherapy has been explored (Table 1). The best-
studied and most widely used agent is bupropion.
This antidepressant with dopaminergic and norad-
renergic activity is an effective agent for smoking
cessation and is related to a doubling of smoking ces-
sation rates compared with placebo treatment [32,33].
A randomized, placebo-controlled trial directly com-
pared bupropion alone or in combination with the
nicotine patch [42]. Bupropion produced a signifi-
cantly higher rate of abstinence at 1 year than ei-
ther the nicotine patch or placebo. Treatment with
bupropion and the nicotine patch did not lead to sig-
nificantly higher cessation rates compared with treat-
ment with bupropion alone. The role of combination
therapy warrants further investigation.
Nortriptyline, an antidepressant with noradrener-
gic activity, 75 to 100 mg daily given for 3 months,
starting 10 to 28 days before quitting, was shown to
be efficacious in small trials [43,44]. Several other
antidepressants have been used in smoking cessation,
including doxepin, imipramine, fluoxetine, and ven-
lafaxine. These agents warrant further investigation.
Clonidine, an a-noradrenergic agonist that sup-
presses sympathetic activity, is used most frequently
as an antihypertensive agent. It has been shown to
decrease the symptoms of nicotine withdrawal and
has been effective for smoking cessation [32]. Meca-
Dose Duration of therapy
7, 14, 21 mg patch for 24 h 8 wk
15 mg patch for 16 h 8 wk
2- and 4-mg pieces 8–12 wk
1 piece per hour
0.5 mg per spray 3–6 mo
1–2 doses per hour
4 mg per cartridge 3–6 mo
6–16 cartridges per day
150 mg per for 3 days, then 7–12 wk
150 mg twice a day
75–100 mg/d 12 wk
0.1–0.3 mg twice a day 3–10 wk

smoking cessation 193
mylamine (Inversine), an antihypertensive drug with
nicotine receptor antagonist activity, suppresses
nicotine withdrawal syndrome and increases smoking
cessation rates when administered with a nicotine
replacement therapy [45,46].
Because many smokers report missing the sensory
aspect of smoking, sensory replacement therapy
has been used. Inhalers containing ascorbic or citric
acid had modest increased rates of short-term cessa-
tion [47,48].
Summary
Smokers have a significantly greater risk of
complications during and after operations. Cigarette
smoke has significant effects on cardiac function, cir-
culation, and respiratory function. Preliminary studies
suggest that smoking cessation for a minimum of 6 to
8 weeks before surgery is required to reduce the peri-
operative and postoperative risks of smoking. Smok-
ing cessation programs that employ advice, support
groups, nicotine replacement therapy, or some anti-
depressants have been used successfully in many
situations and should be used to discourage smoking
preoperatively. Further research is needed, however,
to clarify the best approach to smoking cessation for
surgical patients.
References
[1] Tobacco use—United States, 1900–1999. MMWR
Morb Mortal Wkly Rep 1999;48:986–93.
[2] Rigotti NA. Clinical practice: treatment of tobacco
use and dependence. N Engl J Med 2002;346:506–12.
[3] Pedersen T. Complications and death following anaes-
thesia: a prospective study with special reference to the
influence of patient-, anaesthesia-, and surgery-related
risk factors. Dan Med Bull 1994;41:319–31.
[4] Bluman LG, Mosca L, Newman N, Simon DG.
Preoperative smoking habits and postoperative pulmo-
nary complications. Chest 1998;113:883–9.
[5] Schwilk B, Bothner U, Schraag S, Georgieff M.
Perioperative respiratory events in smokers and non-
smokers undergoing general anaesthesia. Acta Anaes-
thesiol Scand 1997;41:348–55.
[6] Lourenco RV, Klimek MF, Borowski CJ. Deposition
and clearance of 2 micron particles in the tracheobron-
chial tree of normal subjects—smokers and non-
smokers. J Clin Invest 1971;50:1411–20.
[7] Pearce AC, Jones RM. Smoking and anesthesia:
preoperative abstinence and perioperative morbidity.
Anesthesiology 1984;61:576–84.
[8] Cohen S, Tyrrell DA, Russell MA, Jarvis MJ, Smith
AP. Smoking, alcohol consumption, and susceptibility
to the common cold. Am J Public Health 1993;83:
1277–83.
[9] Jenkins SC, Soutar SA, Forsyth A, Keates JR,
Moxham J. Lung function after coronary artery surgery
using the internal mammary artery and the saphenous
vein. Thorax 1989;44:209–11.
[10] Bode FR, Dosman J, Martin RR, Macklem PT.
Reversibility of pulmonary function abnormalities in
smokers: a prospective study of early diagnostic tests
of small airways disease. Am J Med 1975;59:43–52.
[11] Buist AS, Sexton GJ, Nagy JM, Ross BB. The effect of
smoking cessation and modification on lung function.
Am Rev Respir Dis 1976;114:115–22.
[12] Sheps DS, Herbst MC, Hinderliter AL, et al. Produc-
tion of arrhythmias by elevated carboxyhemoglobin
in patients with coronary artery disease. Ann Intern
Med 1990;113:343–51.
[13] Kaijser L, Berglund B. Effect of nicotine on coronary
blood-flow in man. Clin Physiol 1985;5:541–52.
[14] Roth GM, Shick RM. The effects of smoking on the
peripheral circulation. Dis Chest 1960;37:203–10.
[15] Benowitz NL, Gourlay SG. Cardiovascular toxicity of
nicotine: implications for nicotine replacement therapy.
J Am Coll Cardiol 1997;29:1422–31.
[16] Haverstock BD, Mandracchia VJ. Cigarette smoking
and bone healing: implications in foot and ankle
surgery. J Foot Ankle Surg 1998;37:69–78.
[17] Silverstein P. Smoking and wound healing. Am J Med
1992;93:22S–4S.
[18] Sorensen LT, Jorgensen T, Kirkeby LT, Skovdal J,
Vennits B, Wille-Jorgensen P. Smoking and alcohol
abuse are major risk factors for anastomotic leakage in
colorectal surgery. Br J Surg 1999;86:927–31.
[19] Jorgensen LN, Kallehave F, Christensen E, Siana JE,
Gottrup F. Less collagen production in smokers.
Surgery 1998;123:450–5.
[20] Morton H. Tobacco smoking and pulmonary compli-
cations after operation. Lancet 1944;243:368–70.
[21] Warner MA, Offord KP, Warner ME, Lennon RL,
Conover MA, Jansson-Schumacher U. Role of pre-
operative cessation of smoking and other factors in
postoperative pulmonary complications: a blinded pro-
spective study of coronary artery bypass patients. Mayo
Clin Proc 1989;64:609–16.
[22] Beckers S, Camu F. The anesthetic risk of tobacco
smoking. Acta Anaesthesiol Belg 1991;42:45–56.
[23] Moller A, Villebron N, Pedersen T. Interventions for
preoperative smoking cessation (Cochrane Review).
In: The Cochrane Library, Issue 3, 2004.
[24] Munday IT, Desai PM, Marshall CA, Jones RM,
Phillips ML, Rosen M. The effectiveness of pre-opera-
tive advice to stop smoking: a prospective controlled
trial. Anaesthesia 1993;48:816–8.
[25] Haddock J, Burrows C. The role of the nurse in health
promotion: an evaluation of a smoking cessation
programme in surgical pre-admission clinics. J Adv
Nurs 1997;26:1098–110.
[26] Griebel B, Wewers ME, Baker CA. The effectiveness
of a nurse-managed minimal smoking-cessation inter-

ziedalski & ruoss194
vention among hospitalized patients with cancer. Oncol
Nurs Forum 1998;25:897–902.
[27] Simon JA, Solkowitz SN, Carmody TP, Browner WS.
Smoking cessation after surgery: a randomized trial.
Arch Intern Med 1997;157:1371–6.
[28] Wewers ME, Bowen JM, Stanislaw AE, Desimone
VB. A nurse-delivered smoking cessation intervention
among hospitalized postoperative patients—influence
of a smoking-related diagnosis: a pilot study. Heart
Lung 1994;23:151–6.
[29] Munafo M, Rigotti N, Lancaster T, Stead L, Murphy
M. Interventions for smoking cessation in hospitalised
patients: a systematic review. Thorax 2001;56:656–63.
[30] The health benefits of smoking cessation: a report of
the Surgeon General (DHHS publication no. [CDC]
90-8416). Washington, DC7 Department of Health
and Human Services; 1990.
[31] A clinical practice guideline for treating tobacco use
and dependence: A US Public Health Service report.
The Tobacco Use and Dependence Clinical Practice
Guideline Panel, Staff, and Consortium Representa-
tives. JAMA 2000;283:3244–54.
[32] Lancaster T, Stead L, Silagy C, Sowden A. Effective-
ness of interventions to help people stop smoking:
findings from the Cochrane Library. BMJ 2000;321:
355–8.
[33] Hughes JR, Goldstein MG, Hurt RD, Shiffman S.
Recent advances in the pharmacotherapy of smoking.
JAMA 1999;281:72–6.
[34] Hajek P, West R, Foulds J, Nilsson F, Burrows S,
Meadow A. Randomized comparative trial of nicotine
polacrilex, a transdermal patch, nasal spray, and an
inhaler. Arch Intern Med 1999;159:2033–8.
[35] Bohadana A, Nilsson F, Rasmussen T, Martinet Y.
Nicotine inhaler and nicotine patch as a combination
therapy for smoking cessation: a randomized, double-
blind, placebo-controlled trial. Arch Intern Med 2000;
160:3128–34.
[36] Nicotine replacement therapy for patients with coro-
nary artery disease. Working Group for the Study of
Transdermal Nicotine in Patients with Coronary artery
disease. Arch Intern Med 1994;154:989–95.
[37] Joseph AM, Norman SM, Ferry LH, et al. The safety
of transdermal nicotine as an aid to smoking cessation
in patients with cardiac disease. N Engl J Med 1996;
335:1792–8.
[38] Sachs DP, Benowitz NL. Individualizing medical
treatment for tobacco dependence. Eur Respir J 1996;
9:629–31.
[39] Lillington GA, Leonard CT, Sachs DP. Smoking ces-
sation: techniques and benefits. Clin Chest Med 2000;
21:199–208.
[40] Brauer LH, Behm FM, Westman EC, Patel P, Rose
JE. Naltrexone blockade of nicotine effects in ciga-
rette smokers. Psychopharmacology (Berl) 1999;143:
339–46.
[41] Watkins SS, Epping-Jordan MP, Koob GF, Markou A.
Blockade of nicotine self-administration with nicotinic
antagonists in rats. Pharmacol Biochem Behav 1999;
62:743–51.
[42] Jorenby DE, Leischow SJ, Nides MA, et al. A con-
trolled trial of sustained-release bupropion, a nicotine
patch, or both for smoking cessation. N Engl J Med
1999;340:685–91.
[43] Prochazka AV, Weaver MJ, Keller RT, Fryer GE,
Licari PA, Lofaso D. A randomized trial of nortripty-
line for smoking cessation. Arch Intern Med 1998;
158:2035–9.
[44] Hall SM, Reus VI, Munoz RF, et al. Nortriptyline
and cognitive-behavioral therapy in the treatment
of cigarette smoking. Arch Gen Psychiatry 1998;55:
683–90.
[45] Rose JE, Behm FM, Westman EC, Levin ED, Stein
RM, Ripka GV. Mecamylamine combined with nico-
tine skin patch facilitates smoking cessation beyond
nicotine patch treatment alone. Clin Pharmacol Ther
1994;56:86–99.
[46] Rose JE, Behm FM, Westman EC. Acute effects of
nicotine and mecamylamine on tobacco withdrawal
symptoms, cigarette reward and ad lib smoking.
Pharmacol Biochem Behav 2001;68:187–97.
[47] Levin ED, Behm F, Carnahan E, LeClair R, Shipley R,
Rose JE. Clinical trials using ascorbic acid aerosol
to aid smoking cessation. Drug Alcohol Depend 1993;
33:211–23.
[48] Behm F, Schur C, Levin ED, et al. Clinical evaluation
of a citric acid inhaler for smoking cessation. Drug
Alcohol Depend 1993;31:131–8.

Thorac Surg Clin
Preoperative Patient Education in Thoracic Surgery
Richard I. Whyte, MDa,*, Patricia D. Grant, RNb
aDepartment of Cardiothoracic Surgery, Stanford University Medical Center, CVRB 205, 300 Pasteur Drive,
Stanford, CA 94305, USAbThoracic Surgery Service, Stanford University Medical Center, 300 Pasteur Drive, Stanford, CA 94305, USA
Optimal outcome after thoracic surgery, as with
any type of surgery, involves the coordinated activity
of many individuals, including the patient, surgeon,
anesthesiologist, nurses, resident physicians, respira-
tory therapists, and a host of other participants. The
phrase coordinated activity implies that each partici-
pant has knowledge of his or her role and expecta-
tions. For the patient, who is generally uneducated
in the course of the surgical process, this learning
process involves the preoperative and postoperative
period. Through the process of preoperative teaching,
the patient understands his or her role in the overall
process and how he (or she) can facilitate or delay
recovery. This article describes the role of preopera-
tive teaching in thoracic surgery. The focus is not on
the surgeon’s role, but rather the role of the greater
surgical team, which frequently involves nurses,
medical assistants, resident physicians, nurse practi-
tioners, and anesthesiologists.
Because most patients are new to the thoracic
surgical process, the amount of information may be
overwhelming—particularly when patients are con-
fronted with a new diagnosis of malignancy or when
they have no advance knowledge of the magnitude or
risks of the planned surgery. As such, important
concepts often are presented more than once or in
more than one way. Material that the surgeon covers
in the initial consultation often needs to be reinforced
at a subsequent preoperative visit or even again on
the day of surgery.
In the authors’ practice, a recommendation for
surgery often is given at the time of the initial
1547-4127/05/$ – see front matter D 2005 Elsevier Inc. All rights
doi:10.1016/j.thorsurg.2005.02.002
* Corresponding author.
E-mail address: [email protected] (R.I. Whyte).
consultation. Sufficient time is allocated for the sur-
geon to describe the operation and its risks, benefits,
and alternatives. Questions are encouraged, but often
the patient cannot assimilate all of the information
and formulate appropriate questions. Questions often
arise in the following days, as the patient has had time
to digest the information, process it, and assimilate it
on intellectual and emotional levels. If a recommen-
dation for surgery is offered at the initial consultation,
the clinical nurse specialist spends additional time
with the patient interpreting and reinforcing what the
surgeon said, answering questions, and providing a
contact telephone number for subsequent questions.
Patients often have a separate visit a few days be-
fore surgery. At that time, the planned operation is
reviewed again with the patient, and additional ques-
tions are answered. Patients also are seen in a pre-
operative anesthesia clinic by a physician or an
anesthetic nurse practitioner. In this setting, informa-
tion flows two ways: The anesthesia service performs
a preoperative anesthesia assessment, and the patient
has an opportunity to learn more about the planned
anesthesia and postoperative pain issues. The final
opportunity for preoperative teaching is by the
perioperative nurses who, in doing their own pre-
operative patient assessment, answer any remaining
questions and deal with remaining concerns.
Content of preoperative teaching
The content of preoperative teaching should
include all significant issues related to a particular
patient’s operation. For the purposes of discussion,
the content can be separated into two groups: issues
15 (2005) 195 – 201
reserved.
thoracic.theclinics.com

whyte & grant196
related to surgery (or thoracic surgery) in general and
issues related to a specific operation.
General preoperative education
At the initial consultation, the surgeon usually
provides an explanation of the proposed procedure.
Retention of this information is highly variable and
depends on the rapport between the surgeon and
patient; the surgeon’s willingness to provide infor-
mation; and the patient’s curiosity, emotional state of
mind, intelligence, and knowledge base. An intellec-
tually sophisticated patient with a background in the
medical sciences who presents to the office with an
Internet printout of all the latest lung cancer clinical
trials is likely to be handled differently than a poorly
educated patient who has done no background
investigations. Similarly the emotional state of the
patient must be taken into account because it is likely
that an emotionally upset patient hearing the diag-
nosis of ‘‘cancer’’ for the first time may have less
retention than someone who is being provided a sec-
ond opinion or someone who is seeing the surgeon
after a course of preoperative chemotherapy.
At the conclusion of the preoperative process, all
patients need to have some retained understanding of
the planned procedure, why it is being recommended,
what its risks are, whether there are alternatives, and
how their active participation in the surgical process
can make a difference in recovery. Although this
information is generally covered, at some level, by
the surgeon, the surgical nurse often has to review it
with the patient and focus on areas where retention
was inadequate.
Respiratory hygiene
Many of the common complications after tho-
racic surgery—atelectasis, pneumonia, and pulmo-
nary embolism—are pulmonary in nature. Although
pulmonary embolism cannot be prevented through
improvement in pulmonary hygiene, atelectasis and
pneumonia can be prevented through active patient
involvement. Coughing, deep breathing, using an
incentive spirometer, walking, sitting to eat, and
performing other seemingly minor activities all can
contribute to improved pulmonary hygiene and a
decreased incidence of postoperative pneumonia.
Although coughing per se is painful and controver-
sial in terms of its ability to prevent pneumonia,
avoidance of sputum retention is desired. Patients
can be taught to splint the operative side to mini-
mize pain with coughing. Deep breathing can open
collapsed alveoli and prevent overt atelectasis. Walk-
ing and use of an incentive spirometer aim for the
same goals—improved aeration of the lungs and
avoidance of alveolar and segmental collapse. Eat-
ing in bed should be avoided because the often
semirecumbent posture predisposes to aspiration
and regurgitation.
Although all of these respiratory hygiene mea-
sures can be addressed in the postoperative period, it
is best to address these concepts initially in the pre-
operative period. Setting expectations is important,
and in the postoperative period, when the patient’s
sensorium may be clouded by pain and narcotics,
learning is suboptimal. Teaching proper use of an
incentive spirometer is far more effective preopera-
tively than postoperatively when inhalation is com-
promised by pain. When patients are taught how to
use this device preoperatively, they have a relevant
basis from which to compare their postoperative
inspiratory effort and function. Convincing patients
that they can do much better is difficult if they have
never seen the device until the evening after surgery.
Pain
One of the most frightening things for patients
facing surgery is the expectation of pain. Other
frightening concepts include loss of personal control
and death. Because death is usually unlikely, and loss
of control is unavoidable, the expectation of pain
often becomes a major source of anxiety. In the pre-
operative period, the anxiety surrounding pain, rather
than the pain itself, is the problem. Effective pre-
operative teaching can allay these fears, reduce the
anxiety, and provide a framework for realistic expec-
tations regarding postoperative pain [1,2].
A discussion of narcotic analgesics, patient-
controlled analgesia, nonsteroidal analgesics, and epi-
dural anesthesia (continuous, intermittent, and patient
controlled) is appropriate. Side effects, including
nausea, gastrointestinal dysfunction, and the potential
for a lack of efficacy, should be discussed. The goal
of postoperative analgesia also should be discussed.
Patients should not expect to be oblivious to the fact
that they just had surgery, but the goal of post-
operative analgesia should be pain control that pro-
vides patients with an ability to function and interact
with their environment effectively.
Family members should be cautioned that patient-
controlled analgesia is for patients, not family mem-
bers, to control. Family members also should be
cautioned that narcotics may have undesirable side

preoperative patient education 197
effects, such as somnolence, respiratory depression,
dysphoria, disorientation, and even delirium. Family
members should be advised that these side effects
generally resolve quickly after discontinuation of
narcotics, and that the physicians and nurses need
to be made aware if these side effects occur.
Patients should be advised that postoperative early
ambulation is desirable. The upright posture has
many advantages in terms of pulmonary function,
although multiple attachments such as chest tubes,
urinary catheters, epidural catheters, and infusion
pumps often make ambulation difficult. Effective
preoperative counseling sets the expectations, which
can be reinforced in the postoperative period.
Smoking cessation
In thoracic surgical practice, many of the rele-
vant diseases, particularly lung cancer and emphy-
sema, are smoking related. Although many patients
have quit smoking by the time they come to the
thoracic surgeon, others continue to smoke because
the addictive qualities of nicotine outweigh the
intellectual knowledge that smoking is harmful.
Faced with an upcoming operation, the patient may
use smoking as a method of coping with anxiety and
fear. Patients should be counseled vigorously, how-
ever, to stop smoking in preparation for surgery.
Cigarette smoking impairs the mucociliary clearance
mechanisms of the tracheobronchial tree and may
predispose to postoperative pulmonary complications.
The optimal time for smoking cessation is unclear,
and one article even suggested an increase in peri-
operative pulmonary complications when smoking
cessation occurred immediately before surgery [3,4].
Most surgeons encourage patients to stop smoking
in preparation for thoracic surgery. Whether surgery
should be denied to patients who continue to smoke
is controversial. Every effort should be made pre-
operatively to persuade the patient to stop smoking.
Diet and nutrition
Preoperative patient education should cover nu-
tritional issues routinely but is particularly important
in two classes of patients: (1) patients who have
recently experienced a significant weight loss and
(2) patients who are to undergo preoperative chemo-
therapy or radiation therapy. The first group includes
many patients with esophageal cancer in whom
dysphagia or odynophagia have limited their oral
intake and resulted in a long-standing caloric defi-
ciency. Although significant weight loss is common
in patients with metastatic disease, such patients
frequently are identified through preoperative staging
tests and often do not come to the attention of the
surgeon. The second group involves patients who
ideally should be seen by the surgeon before the
neoadjuvant therapy is started. In these patients,
nutritional deficiencies can be expected and conse-
quently preempted. Patient questions regarding nutri-
tional supplementation (including herbal or other
nontraditional forms of treatment) often arise at this
time and can be dealt with appropriately.
Wound care and drains
Although most thoracic surgery patients require
little or no postdischarge wound care, the preopera-
tive visit is a reasonable time to raise this issue. Pa-
tients often have negative expectations about wound
care and often are pleasantly surprised to learn that
care is usually minimal. Occasionally, patients are
discharged home with tubes or drains still in place.
Because percutaneous tubes and drains are an integral
part of modern surgical care and their use has become
ubiquitous, health care providers may become numb
to their invasiveness and the patient’s sense of a loss
of personal image. Patients should be taught about the
uses and benefits of percutaneous tubes and drains as
early as possible. In years past, patients routinely
were kept in the hospital until all drains and tubes
were out: mastectomy patients stayed in the hospital,
on intravenous antibiotics, until the Jackson-Pratt
drains were removed. Now, as a result of ‘‘best prac-
tice’’ analysis, evidence-based medicine, and changes
in reimbursement policies, practices have changed,
and patients are taught that it is acceptable to go
home with a small drain.
Postdischarge social issues
Although it may seem premature to enter into a
discussion of postdischarge psychosocial issues in the
preoperative phase, such a discussion is not inappro-
priate. Postdischarge issues, such as family involve-
ment in postoperative convalescence, job-related
concerns, and expectations regarding physical limi-
tations, including appetite, sleep irregularity, and sex-
ual function, can be broached in the preoperative
period and brought up again in more detail later.
Issues that potentially may delay discharge from the
hospital may become apparent in these discussions
(which are frequently left to the nursing staff), and it
is helpful to address these issues early so that they do
not become problems later. In dealing with the patient

whyte & grant198
and family, cultural sensitivity and family dynamics
may play crucial roles in effecting a smooth post-
operative recovery.
Contact numbers
Part of the preoperative teaching process is to
effect seamless communication between the patient
and the surgeon. Because many surgeons delegate
much of the preoperative teaching to resident phy-
sicians, nurses, and other nonphysician staff, it is
crucial to provide patients with a reliable method of
contacting the surgeon or his or her designee. Pa-
tient satisfaction has an increasing role in deter-
mining where patients go for their care, and one of
the simplest methods for improving patient satisfac-
tion is providing them with a reliable conduit to the
surgeon and his or her staff.
Procedure-specific teaching
In addition to the more general areas discussed
earlier, each patient needs teaching directed toward
the specific operation he or she is to undergo. Infor-
mation that needs to be covered at this stage includes
the size and location of the incision, the general
outline of the operation, the expected postoperative
physiologic state or deterioration from baseline, and
a general overview of the risks of complications or
death. Several common examples are detailed next.
Pulmonary resection (lobectomy/pneumonectomy)
In addition to providing information regarding in-
cision length and position, morbidity, mortality,
and other issues described previously, patients under-
going thoracotomy for pulmonary resection should
receive counseling on postthoracotomy pain and
the potential for decreases in pulmonary reserve.
Thoracotomy incisions are notoriously painful, and
although early postoperative pain can be managed
effectively by modern analgesic techniques, the late
issues of ongoing narcotic use and the incumbent
gastrointestinal side effects should be discussed
proactively. From the standpoint of loss of pulmo-
nary reserve, patients with marginal preoperative
lung function should be advised that they are likely
to have less exercise capacity and that nasal oxygen
therapy may be necessary on a short-term basis. In
the authors’ practice, patients who would be expected
to require supplemental oxygen on a long-term basis
rarely are offered surgery. Patients undergoing
pneumonectomy are at particular risk for symptom-
atic decreases in exercise capacity and should be
counseled accordingly.
Thoracoscopy
Patients scheduled for thoracoscopy, particularly
limited procedures such as lung biopsy, sympathec-
tomy, and pleural biopsy, often can be discharged the
day after surgery. Reports of outpatient thoracoscopy
have appeared in the literature, but the presence of a
chest tube often dictates an overnight stay [5]. Pa-
tients should be advised that the chest tube probably
will be removed on the morning after surgery, and
that issues such as pain, nausea, and general fatigue
will be managed on an outpatient basis.
Esophagectomy patients need to be forewarned
about early satiety and the possibility of dumping
syndrome. The presence of tubes and drains, which
are second nature to the surgeon, are not second na-
ture to the patient. The idea of having a chest tube can
be frightening to some patients. Drains, wound care,
and jejunostomy tubes, all of which are common
to thoracic surgery practice, are foreign to medically
naive patients. Clinicians must be cognizant of pa-
tients’ naivete and address it through good preopera-
tive teaching.
Patients need to have some concept of the risks
of the planned procedure. Although some patients
do not want to face these considerations, the doc-
trine of informed consent is an integral part of the
medical system. The surgeon and members of his or
her team need to balance the patient’s desire for in-
formation (or lack thereof), the need to provide a basis
for informed consent, and the undesirable outcome of
fostering fear and anxiety. In general, at a minimum,
a description of common complications, a qualitative
assessment of morbidity and mortality, and an invi-
tation to go into greater detail should be offered.
Lung volume reduction surgery (and other operations
in patients with severe emphysema)
The major specific issue to address in patients
with severe emphysema is prolonged air leaks. Dis-
cussion of other complications, such as pain control,
risks of pneumonia, and the potential for postopera-
tive mechanical ventilation, should not be omitted,
but prolonged air leaks with the ongoing need for
chest tube drainage specifically should be mentioned.
Techniques such as the use of reinforcing strips for
surgical staplers and surgical glue can be discussed,
although these patients often stay in the hospital for
prolonged periods simply because of the need for
ongoing pleural drainage. Use of one-way valves and
the possibility of being discharged home with a chest
tube in place can be discussed in the preoperative

preoperative patient education 199
phase of care—not as a likely outcome, but so that it
is not such a foreign concept if it needs to come up
again later.
Esophagectomy
Esophagectomy is one of the larger operations
that thoracic surgeons perform regularly. It is asso-
ciated with significant short-term and long term
morbidity and consequently warrants special atten-
tion in a discussion of preoperative teaching. From
the patient’s perspective, esophagectomy generally
is seen in the context of a diagnosis of cancer that
carries an unusually poor long-term outlook. The
operation generally involves two incisions and is as-
sociated with the possibilities of death, a stay in the
ICU, chest tubes, feeding tubes, and other daunting
obstacles. The ‘‘tradeoff’’ is that patients often start
with severe dysphagia (in contrast to lung cancer
patients who are generally asymptomatic) and end
having a much improved quality of swallowing.
For these patients, specific preoperative teaching
issues should include the surgical risks (bleeding,
infection, anastomotic leak, hoarseness [in the case of
a cervical anastomosis], and the risk of perioperative
and operative mortality—1–5% in various series). To
counterbalance these negatives, relief of dysphagia
and the possibility of cure can be raised. The post-
operative issues of early satiety, dumping, and regur-
gitation (the risks of which vary depending on the
planned operative approach) all should be discussed,
although it should be made clear that the degree of
these symptoms and their duration have a wide range.
Photodynamic therapy
Photodynamic therapy is a technique of ablating
obstructing tumors of the major bronchi or esopha-
gus (and now approved for the ablation of columnar-
lined esophageal mucosa) that has the undesirable
side effect of prolonged cutaneous photosensitivity.
The only governmentally approved and commer-
cially available photosensitizing agent in the United
States, Photofrin, is associated with a 6-week period
of photosensitivity, during which time patients
should avoid direct sunlight and wear protective
clothes when outside (eg, gloves, wide-brimmed hat,
long sleeves, long pants). Failure to be compliant
may result in a severe sunburn-like reaction, even to
the point of blistering. It is helpful to council pa-
tients repeatedly on these restrictions and to use a
combination of verbal direction, written material,
and a take-home video. Despite all of these modali-
ties, some patients are noncompliant, but because
the photosensitivity reaction develops quickly, they
rarely repeat their indiscretions.
Transplantation
On review of the literature on preoperative
teaching of patients for thoracic surgery, it is found
that the greatest amount of effort has gone into car-
diac surgery (not a topic of this article) and trans-
plantation [6–8]. One reason is that the preoperative
assessment of patients for transplantation is far
more complicated than it is for most other tho-
racic surgical patients. The other reason is that, for
most transplant patients, the transplant itself is just
the start of a transforming process that results in
lifelong involvement with the transplant center, the
ongoing use of multiple medications, and the need
for periodic physiologic and pathologic assessment
of the outcome (eg, pulmonary function tests, bron-
choscopy with biopsy). The preoperative evaluation
of transplant patients attempts to identify patients with
the greatest chance of benefiting from receiving a
scarce resource (donor organs) and involves a rigor-
ous medical screening and evaluation and a thorough
psychosocial evaluation. Drug or alcohol abuse,
destructive behavior, noncompliance, and lack of
social supports all argue against offering such pa-
tients donor organs. This preoperative assessment
frequently involves psychologists (or psychiatrists)
and social workers in addition to the more ‘‘nuclear’’
team of the surgeon, transplant pulmonologist, and
the rest of the transplant team. Given the complexity
and lifelong duration of the transplant process, it is
not surprising that the preoperative assessment and
teaching processes are more involved.
Research protocols
In addition to providing excellent patient care,
academic medical centers have the added responsi-
bilities of teaching and conducting research. For the
thoracic surgeon, clinical trials provide a mechanism
for improving the outcome of future patients with
lung cancer, esophageal cancer, and end-stage lung
disease. In many academic medical centers, clinical
trial nurses play a vital role in identifying patients for
clinical trials and in educating patients about these
trials. These discussions involve the nature of the
trial, inclusion and exclusion criteria, study design
(randomized/prospective versus open-label/historical
control), and risks and potential benefits associated
with the specific trial in question. Compared with
physician investigators, clinical trial nurses often
have more time to spend with the patients, may be
less perceived as having a vested interest in the out-
come of the trial, and may be more open to questions
than the physician investigator. The downside is that
the nurses may have a less detailed knowledge of

whyte & grant200
the trial (eg, pharmacology, pathophysiology, surgical
anatomy). Consequently, physician backup to these
clinical trial nurses must be available.
Preoperative teaching tools
Verbal instruction
Verbal instruction is the cornerstone tool to pre-
operative teaching, and whoever conveys information
verbally must be cognizant of the recipient’s intellec-
tual level, interest in acquiring the information, at-
tention span, and emotional ability to handle the
information. Multiple factors, such as language bar-
riers, learning disabilities, and cultural barriers, can
impair this knowledge transfer, and other strategies,
including repetition, provision of written material,
interpreters, and drawings, may be necessary. It is
often surprising to find that patients, after what was
thought to be a thorough preoperative discussion,
continue to have basic questions that they are reluc-
tant to discuss with the surgeon and that are asked to
the preoperative nurse or other staff only after the
surgeon has left.
Written material
Complementing verbal instruction and direction is
the dissemination of written material. Nonprofit orga-
nizations have a variety of patient education materials
available at relatively low cost. The American Cancer
Society has a telephone hotline for information that
can be sent to patients free of charge. The information
covers general cancer care and preparation for sur-
gery, including topics such as ‘‘what questions to ask
the doctor’’ and ‘‘what are the risks and side effects
of surgery.’’ The American Lung Association has a
large amount of free and low-cost written material
on smoking cessation and lung health, including pul-
monary function testing, bronchoscopy, lung cancer,
and lung transplantation. Lastly, information packets
for commonly performed operations can be bought
or made ‘‘in house’’; the latter has the advantage
of providing information specific to the institution
and surgeons.
Manufacturers of commercial products often pro-
vide free product-specific patient education packets
or booklets. One example is Axcan Pharmaceuticals,
which supplies patient education material on photo-
dynamic therapy for lung and esophageal cancer and
Barrett’s esophagus. Another example is Denver Bio-
medical, which provides written information and a
patient video on its PleurX pleural catheter. Other
companies, such as Bristol-Myers-Squibb Oncology
and Aventis Pharmaceuticals, supply product-specific
and disease-specific patient information and more
general cancer care information on topics such
as nutrition and exercise in the form of books
and pamphlets.
Web-based material
Much of the information described in this article,
in addition to a wealth of additional information, is
also available online. The American Cancer Society
and the American Lung Association have extensive
websites with large amounts of patient-oriented infor-
mation. In addition, for cancer patients, the National
Cancer Institute provides a detailed and user-friendly
website (www.cancer.gov) with a wealth of material
aimed at the patient level. The University of Pennsyl-
vania (www.oncolink.upenn.edu) also provides an
outstanding patient-centered website that is relatively
free of institutional and commercial bias. Addi-
tional patient-oriented information on clinical trials
is available through the Coalition of National Cancer
Cooperative Groups (www.cancertrialshelp.org).
Numerous pharmaceutical company websites also
offer disease-specific information on disease preven-
tion, diagnosis, causes, and treatment. With the ubiq-
uity of Web access, the authors caution patients that
information obtained on the Web can be highly bi-
ased, poorly referenced, and even self-serving and
promotional in nature, but that reputable sources can
provide valuable insights into their disease and the
treatment options that are available to them.
Audiovisual material
Another opportunity for teaching includes provi-
sion of audiovisual material. Axcan Pharmaceuti-
cals, the supplier of Photofrin, has created a video
detailing the risks of photosensitivity and how to
avoid such side effects. Diagrams and models also
may be used. Commercially available lung models
can help the surgeon or clinical nurse specialist ex-
plain the concepts of bronchopulmonary segments,
lobectomy, and wedge resection. Diagrams, which
can be hand-drawn or commercially obtained, can
be used to explain anatomic concepts. Lastly, use of
the patient’s own radiographs can be an excellent
teaching method, and patients generally pay a great
deal of attention to their own radiographs. It takes

preoperative patient education 201
relatively little time to explain the basics of a CT
scan, and patients are often surprised that what
is a ‘‘lung nodule’’ to one physician is a ‘‘worri-
some mass’’ to another. Such teaching methods are
particularly helpful when patients are to be followed
radiographically for an indeterminate pulmonary
nodule. As the saying goes, ‘‘a picture is worth a
thousand words,’’ and 1 or 2 minutes spent with a real
radiograph can take the place of and be more
satisfying than a lengthy description of the films.
Summary
Preoperative patient teaching may take many
forms and is offered to patients across many venues
and formats. The goal of patient teaching is to im-
prove patients’ understanding of their disease process
and the operation that they are about to experience
with the goal of enlisting their active participation in
the healing process. The additional goal of obtaining
informed consent is not only codified in law, but also
has become an ingrained component to the current
physician-patient relationship. The preoperative
teaching process is best approached as a team effort,
and multiple modalities often must be used so that the
patient becomes a knowledgeable and willing mem-
ber of the team.
References
[1] Smeltzer SC, Bare BG. Preoperative nursing manage-
ment. In: Smeltzer SC, Bare BG, editors. Brunner
and Suddarth’s textbook of medical surgical nursing.
10th edition. Philadelphia7 Lippincott Williams &
Wilkins; 2004. p. 399–416.
[2] Miro J, Raich RM. Effects of a brief and economical
intervention in preparing patients for surgery: does
coping style matter? Pain 1999;83:471–5.
[3] Bluman LG, Mosca L, Newman N, Simon DG.
Preoperative smoking habits and postoperative pulmo-
nary complications. Chest 1998;113:883–9.
[4] Ratner PA, Johnson JL, Richardson CG, et al. Efficacy
of a smoking-cessation intervention for elective-surgical
patients. Res Nurs Health 2004;27:148–61.
[5] Chang AC, Yee J, Orringer MB, Iannettoni MD.
Diagnostic thoracoscopic lung biopsy: an outpatient
experience. Ann Thorac Surg 2002;74:1942–6.
[6] Shuldham CM, Fleming S, Goodman H. The impact of
pre-operative education on recovery following coronary
artery bypass surgery: a randomized controlled clinical
trial. Eur Heart J 2002;23:666–74.
[7] Hobbs FD. Does pre-operative education of patients
improve outcomes? The impact of pre-operative educa-
tion on recovery following coronary artery bypass
surgery: a randomized controlled clinical trial. Eur
Heart J 2002;23:600–1.
[8] Bahruth AJ. What every patient should know. . .pretransplantation and posttransplantation. Crit Care
Nurs Q 2004;27:31–60.

Thorac Surg Clin
The Value of Preoperative Pulmonary Rehabilitation
Shanon T. Takaoka, MD, Ann B. Weinacker, MD*
Department of Medicine, Division of Pulmonary and Critical Care Medicine, Stanford University, 300 Pasteur Drive,
#H3142, Stanford, CA 94305-5236, USA
For many decades, pulmonary rehabilitation has
served as an integral, although relatively unheralded,
component of the medical and surgical manage-
ment of chronic lung diseases. Its value has become
more apparent in recent years with the increasing
prevalence of chronic obstructive pulmonary disease
(COPD) and the renewed interest in lung volume
reduction surgery (LVRS) as a viable surgical option
for selected patients with COPD [1]. Although exist-
ing data primarily support its use in COPD, pulmo-
nary rehabilitation also has been applied with some
success to patients with other chronic lung diseases,
such as cystic fibrosis, interstitial lung disease, and
neuromuscular conditions, and in patients awaiting
lung transplantation or lung resection [2]. Partici-
pation in perioperative pulmonary rehabilitation is
encouraged and often required for patients under-
going such surgeries, with the goals of optimizing
quality of life, functional capacity, and overall sur-
gical outcomes. Although pulmonary rehabilitation
is potentially beneficial before any surgery, it has
been applied and studied primarily in the setting of
major thoracic surgical procedures, including LVRS,
lung transplantation, and lung resection. This article
defines the essential elements of pulmonary rehabili-
tation, outlines the prerequisites for enrollment, and
discusses its current role in the setting of anticipated
thoracic surgery.
1547-4127/05/$ – see front matter D 2005 Elsevier Inc. All rights
doi:10.1016/j.thorsurg.2005.02.001
* Corresponding author.
E-mail address: [email protected] (A.B. Weinacker).
Background
Although the fundamental tenets of pulmonary
rehabilitation were elucidated in the 1970s, they were
not put into widespread practice until more recently.
Subsequently the data from numerous studies have
supported unequivocally the utility of pulmonary re-
habilitation in improving symptoms of underlying
disease, functional capacity, and quality of life, par-
ticularly in patients with COPD [3]. Pulmonary re-
habilitation has been defined as ‘‘a multidimensional
continuum of services directed to persons with pul-
monary disease and their families, usually by an in-
terdisciplinary team of specialists, with the goal of
achieving and maintaining the individual’s maximum
level of independence and functioning in the com-
munity’’ [4]. This definition emphasizes the key
elements of program individualization, family in-
volvement, and a multidisciplinary approach. The
participation of physicians, nurses, respiratory thera-
pists, physical therapists, occupational therapists, die-
titians, and psychologists maximizes surgical benefit
and prepares patients and their families to cope with
the psychosocial stressors of surgery.
Role of preoperative pulmonary rehabilitation
Goals and proposed benefits
The primary goal of pulmonary rehabilitation is
to facilitate the patient’s return to independent func-
tion at the highest possible level (Table 1). To achieve
this goal, concurrent goals are to relieve symptoms
(mainly dyspnea), decrease disability associated with
15 (2005) 203 – 211
reserved.
thoracic.theclinics.com

Table 1
General and surgery-specific goals of pulmonary rehabili-
tation with the anticipated long-term benefits
Goals Benefits
General
Decrease dyspnea
Decrease symptom-related
disability
Optimized functional
status
Enhanced quality
Improve patient compliance of life
Decreased health
care usage
Optimize underlying lung
disease and coexisting
medical conditions
Increase cardiopulmonary
conditioning
Improve nutritional status
Surgery-specific
Improve airway clearance
and diaphragmatic function
Improved tolerance
of surgery
Increase patient tolerance of
symptoms while waiting for
donor organ
Decreased postoperative
complications
Identify compliant patients/
good surgical candidates
takaoka & weinacker204
symptoms, and empower patients to understand and
manage better their disease processes [5]. Likewise,
pulmonary rehabilitation can lead to optimization of
medical therapy, improvement in nutritional status,
and better cardiopulmonary conditioning [6]. Coex-
isting medical conditions, such as infection and
hypoxemia, also should be prevented and managed
in the setting of pulmonary rehabilitation [7]. Ulti-
mately, pulmonary rehabilitation should culminate in
a better overall quality of life, increased participation
in physical and social activities, and decreased health
care use. Data from numerous controlled trials have
shown a decrease in the lengths of hospital stays and
the total number of hospitalizations after rehabilita-
tion and a trend toward fewer visits to the emergency
department or physician’s office [3]. Although pul-
monary rehabilitation has been shown to improve
significantly symptom control, functional status, and
quality of life, most studies have shown no improve-
ment in lung function itself.
In the preoperative setting, the overall goal of
pulmonary rehabilitation is to maximize the advan-
tages derived from the planned surgery. In addition
to the aforementioned benefits, other proposed but
unproven benefits for surgical patients include im-
proved tolerance of the surgical procedure, increased
ability to clear secretions, and decreased work of
breathing as a result of improvement in diaphrag-
matic function [8]. These benefits should decrease
postoperative complication rates; improve postopera-
tive adherence to exercise regimens; and, in the set-
ting of lung transplantation, improve tolerance of the
time spent waiting for an appropriate organ donor.
Some patients may derive so much benefit from re-
habilitation in terms of improved functional status
and quality of life that surgery can be reconsidered or
postponed [2]. Rehabilitation can serve the valuable
purpose of further distinguishing appropriate candi-
dates for surgery. Patients who are too debilitated or
too noncompliant to complete a preoperative rehabili-
tation program are unlikely to have good surgical
outcomes, and consideration of alternative therapeu-
tic options may be indicated [9].
Setting
Pulmonary rehabilitation has been implemented
with remarkable success in the inpatient setting, for-
mal outpatient setting, and home setting. The choice
of setting for an individual patient depends on physi-
cal and psychosocial status, program accessibility, fi-
nancial considerations, and patient preference [3]. For
significantly debilitated patients, home-based reha-
bilitation is preferred, whereas patients with stable
disease, relatively good functional status, and the
ability to travel conveniently are good candidates for
formal outpatient therapy. A study comparing formal
outpatient pulmonary rehabilitation with home-based
therapy in COPD patients indicated that although
improvements in exercise capacity were observed in
both treatment groups compared with controls, the
improvements were sustained for a longer time in the
home-based group. This observed trend was likely
due to the fact that patients participating in home-
based pulmonary rehabilitation tend to continue the
exercise regimens after completion of the prescribed
programs [10].
Benefits related to specific surgical procedures
Lung volume reduction surgery
As the incidence of COPD continues to increase,
LVRS is an increasingly more attractive measure in
the palliation of severe emphysema (Table 2). Given
the established benefit seen in emphysema patients
who participate in pulmonary rehabilitation, it has
become standard practice to require patients awaiting
LVRS to complete a preoperative rehabilitation pro-
gram. In the landmark study by the National Em-
physema Treatment Trial Research Group, all patients
were required to complete 6 to 10 weeks of formal
pulmonary rehabilitation before they could be
randomized to undergo LVRS or continued medical

Table 2
Primary surgical procedures using preoperative pulmonary rehabilitation, proposed benefits based on available studies, and the
strength of the supporting data
Surgery Proposed benefits Data strength
LVRS Improve health-related quality of life, improved
functionality and exercise capacity [11–13,41]
Few or small randomized controlled trials,
many observational studies
Lung transplantation Improved functional status, exercise tolerance,
and quality of life [14–18]
Few or small randomized controlled trials,
many observational studies
Lung resection Increased inspiratory muscle strength and
improved preoperative lung function [19,42]
Few or small randomized controlled or
observational trials
Other high-risk surgery
(ie, CABG,
upper abdominal)
Improved preoperative lung function, decreased
rate of postoperative pulmonary complications,
fewer radiographic abnormalities [20,21]
Few or small randomized controlled or
observational trials
Abbreviations: CABG, coronary artery bypass graft; LVRS, lung volume reduction surgery.
preoperative pulmonary rehabilitation 205
therapy [11]. The combination of pulmonary rehabili-
tation and bilateral LVRS can improve health-related
quality of life significantly. In one study [12], each
intervention contributed differently; the pulmonary
rehabilitation component had the greatest effect
on patients’ perceptions of their physical limitations
secondary to illness, and LVRS more significantly
improved actual physical and social function and
vitality. These findings suggest a complementary
relationship between pulmonary rehabilitation and
LVRS, resulting in greater overall patient benefit
when they are implemented together.
A similar study compared pulmonary rehabilita-
tion with LVRS in 200 patients with severe COPD.
After completing an 8-week rehabilitation course,
patients were randomized to receive either continued
rehabilitation for an additional 3 months or LVRS.
Evaluation of all patients before randomization
showed that the initial rehabilitation program resulted
in a trend toward a longer 6-minute walk distance
(285 ± 96 m versus 269 ± 91 m; P = .14) and a
significant increase in total maximal exercise time
(7.4 ± 2.1 min versus 5.8 ± 1.7 min; P < .001) [13].
Consistent with other studies, however, there was no
improvement in pulmonary function test results after
completion of rehabilitation. The patients who
continued to participate in pulmonary rehabilitation
showed a trend toward higher maximal oxygen con-
sumption and a significant improvement in quality-
of-life indicators. It is unclear, however, whether
these effects have any impact on morbidity and mor-
tality after LVRS. Further studies comparing pulmo-
nary rehabilitation plus LVRS with LVRS alone are
needed to establish definitively the value of preopera-
tive rehabilitation.
Lung transplantation
Enrollment in pulmonary rehabilitation before
lung transplantation is encouraged in many centers
because patients selected for transplantation are often
severely physically deconditioned. Attendance by
lung transplant candidates at pulmonary rehabilitation
programs has been shown to be greater than 80%; this
is likely a reflection of the rate of referral and the
selection of compliant patients [14]. The data sup-
porting the efficacy and benefit of pretransplant re-
habilitation largely comprise uncontrolled studies,
however, which are limited further by small sample
sizes, widely varying program intensities and dura-
tions, and lack of standardized outcome measures.
Four of these studies showed a trend toward im-
provement in functional capacity after rehabilitation,
as represented by improved 6-minute walk distances
in patients with various causes of end-stage lung
disease awaiting either single-lung or double-lung
transplantation [15–18]. The largest of these studies
divided 110 patients into five groups based on the
underlying lung disease and the type of lung trans-
plant planned (single or double). Three of the five
groups experienced significant increases in mean
6-minute walk distances before transplantation, indi-
cating that preoperative pulmonary rehabilitation in
the lung transplant population can result in increased
exercise tolerance. Although the data are limited,
and the effect on surgical outcome has yet to be es-
tablished, pulmonary rehabilitation before lung trans-
plant does seem to improve safely functional status
and patient well-being.
Lung resection
Lung cancer is a major cause of mortality, and
with smoking as the primary risk factor, many
patients undergoing lung resection have associated
COPD. Minimal data exist, however, regarding
pulmonary rehabilitation before lung resection. This
fact may be due in part to the relatively brief time
between cancer diagnosis and surgery, which does
not allow for significant patient participation in

takaoka & weinacker206
rehabilitation. In one of the few existing studies to
date, Weiner et al [19] randomized 32 patients with
COPD undergoing resection for primary lung neo-
plasm to receive either incentive spirometry and in-
spiratory muscle training for 2 weeks before lung
resection or no training at all. The investigators found
that inspiratory muscle strength, as measured by the
maximum inspiratory pressure at residual volume,
increased significantly in the training group, but
remained unchanged in the group that received no
training [19]. The relevance of these data on clinical
outcomes has not yet been established; however, the
data suggest a potential beneficial impact of rehabili-
tation activities on patient lung mechanics.
Other high-risk surgical procedures
Although preoperative pulmonary rehabilitation
has been studied primarily in association with major
lung-related surgeries, two small prospective studies
have shown that patients randomized to undergo 2 to
4 weeks of short-term pulmonary rehabilitation be-
fore coronary artery bypass graft surgery had signifi-
cantly better lung function (ie, peak expiratory flow
rate, inspiratory capacity, gas exchange) postopera-
tively than patients who did not undergo rehabilita-
tion, although the risk of postoperative pulmonary
complications was not consistently reduced [20,21].
These studies were small, however, and have not
been validated.
Another randomized controlled study of 81 pa-
tients examined the efficacy of pulmonary reha-
bilitation in preventing postoperative pulmonary
complications after upper abdominal surgery. Al-
though not clinically significant, the rehabilitation
group had a lower incidence of postoperative pul-
monary complications (7.5% versus 19.5%; P = 0.11)
and significantly fewer radiographic alterations (15%
versus 39%; P = .01) than the control group [22].
Patient selection for pulmonary rehabilitation
Inclusion criteria
Essentially any patient with stable chronic lung
disease who experiences significant symptoms that
diminish functional status or quality of life is an
appropriate candidate to consider for pulmonary re-
habilitation [5]. The magnitude of spirometric abnor-
malities seems to correlate poorly with levels of
dyspnea or functional capacity and is a poor indicator
of eligibility for pulmonary rehabilitation [23]. An
important prerequisite is the patient’s motivation to
participate in the various program elements, which
can be rigorous and demanding. Although advanced
age previously was thought to be a factor prohib-
iting enrollment in pulmonary rehabilitation, it is now
thought that patients of all ages who meet the other
inclusion criteria are eligible to participate. Because
elderly patients often have comorbidities that impair
their musculoskeletal, sensory, and cognitive abilities
(eg, arthritis, decreased visual acuity, dementia), they
are likely to derive considerable benefit from super-
vised exercise programs, nutritional education, and
training in medication administration techniques [24].
It is debated whether smoking cessation should be
a prerequisite or a goal of pulmonary rehabilitation.
Some authors argue that patients who are unable to
quit smoking lack the necessary motivation to be
successful participants in rehabilitation. The educa-
tional and behavioral modification elements of pul-
monary rehabilitation programs have the potential,
however, to be powerful adjuncts to ongoing smoking
cessation efforts. It has been proposed that non-
smokers and smokers who are enrolled in smoking
cessation programs should be deemed good candi-
dates for pulmonary rehabilitation [23].
Exclusion criteria
The only absolute contraindication to enrollment
in pulmonary rehabilitation is a lack of compliance as
shown by prior experience with the patient during the
course of medical treatment or an expressed unwill-
ingness to participate in the program [24]. As men-
tioned previously, active smoking is not a criterion
for exclusion if the patient shows a commitment to
quitting by participating in a smoking cessation pro-
gram in conjunction with pulmonary rehabilitation.
Severe functional disability also is not an absolute
contraindication [23] because patients still may derive
benefit from the exercise program and the adjunctive
educational components. Other comorbidities, par-
ticularly if unstable or symptomatic, that either would
endanger the patient or would interfere with the re-
habilitative process are relative contraindications to
participation; every effort to identify and optimize
treatment of coexisting diseases should be made be-
fore referral for pulmonary rehabilitation. Examples
of these diseases include recent myocardial infarc-
tion, unstable angina, severe pulmonary hyperten-
sion, advanced arthritis, disruptive behaviors, or
significant learning disabilities [3]. Additional exclu-
sion criteria are specific to the individual surgical
procedures, such as age limitations for lung trans-
plantation or specific spirometric parameters for lung
resection. Patients who are denied surgery based on
prohibitive but potentially reversible factors may be-

preoperative pulmonary rehabilitation 207
come better surgical candidates after completion of
a rehabilitation program. Pulmonary rehabilitation
can be an important and efficacious alternative for
patients who are deemed poor operative candidates.
Preoperative pulmonary evaluation
Major pulmonary complications, including pneu-
monia, atelectasis, bronchospasm, and respiratory
failure, are significant causes of postoperative mor-
bidity and mortality. Identification of procedure-
related and patient-related risk factors predisposing
to development of postoperative pulmonary compli-
cations is an essential component of the preoperative
evaluation. Procedure-related risk factors include the
surgical site, with thoracic and upper abdominal sur-
geries incurring the highest risk; duration of surgery;
and type of anesthesia (regional versus general) [25].
Various patient-specific risk factors also have been
identified and are discussed in more detail next. Some
of these risk factors are potentially modifiable with
early identification and initiation of appropriate mea-
sures, including pulmonary rehabilitation.
Patient-related risk factors
The most important risk factor for postoperative
pulmonary complications in the setting of thoracic
surgery is the severity of underlying lung disease.
Historically, specific thresholds for forced expiratory
volume in 1 second (FEV1), forced vital capacity, and
vital capacity were proposed as predictors of high
surgical risk. The literature and clinical experience
have since proven, however, that patients with severe
underlying lung impairment can undergo thoracic
surgery safely, and the previously identified thresh-
olds are not absolute. Currently, marginal surgical
patients are defined as having at least three of the fol-
lowing five pulmonary function abnormalities: FEV1
less than 1.2 L, maximum voluntary ventilation 35%
or less of predicted normal values, mid-expiratory
flow (forced expiratory flow 25–75%) of 0.6 to 1 L/s,
diffusing capacity 35% or less of predicted normal
values, and hypercapnia (Paco2 >45 mm Hg) [26]. In
LVRS, preoperative hypercapnia greater than 45 mm
Hg is strongly predictive of increased postoperative
mortality [27].
Cigarette smoking is an established risk factor for
postoperative complications, especially when the
smoking history exceeds 20 pack-years or if the
patient has smoked within 8 weeks of surgery.
Although the magnitude of this risk has not been
clearly delineated, smokers seem to be at greater risk
for significant postoperative hypoxemia, pneumonia,
delayed extubations, and increased ICU admissions
[28,29]. Additional risk factors for postoperative pul-
monary complications include general health status as
represented by American Society of Anesthesiolo-
gists classification greater than 2 (ie, having more
than mild systemic disease) [30], decreased exercise
capacity as indicated by a maximal oxygen con-
sumption less than 10 mL/kg/min, oxygen desatura-
tion during exercise, inability to climb more than one
flight of stairs, or 6-minute walk distance less than
200 feet before or after rehabilitation [31]. Although
obesity and advanced age have been identified previ-
ously as risk factors, the available data are conflict-
ing, and neither factor is considered independently
to prohibit surgical intervention.
Relevant preoperative testing
After a thorough history and physical examina-
tion, the preoperative pulmonary evaluation before
thoracic surgery usually proceeds in three stages.
Stage I includes measurement of spirometry, diffus-
ing capacity, and arterial blood gases to establish the
baseline severity of underlying lung disease. Stage II
testing uses a quantitative split-function ventilation-
perfusion scan to assess the function of each lung
independently. In patients with marginal lung func-
tion who are anticipating significant lung resec-
tion (primarily pneumonectomy or lobectomy), split
ventilation-perfusion scans facilitate calculation of
the predicted postoperative FEV1. Typically a post-
operative FEV1 less than 0.8 L or less than 35% of
predicted normal values indicates excessive surgical
risk and inoperable disease [26]. Stage III evaluation
is undertaken for patients with a marginal predicted
postoperative FEV1 and comprises primarily various
modes of exercise testing, including stair climbing,
timed walk test, exercise oximetry, and incremental
or submaximal cycle ergometry with the goal of
estimating or measuring maximal oxygen consump-
tion to risk stratify the patient [32]. Generally the
ability to climb higher than 14 m [33], 6-minute walk
distances greater than 700 ft, oxygen saturations 92%
or greater at rest and with exertion on exercise
oximetry, and a maximal oxygen consumption greater
than 15 mL/kg/min are indicators of good surgical
outcome [34]. Conversely, patients who climb less
than 12 m [33], have 6-minute walk distances less
than 500 ft, have oxygen saturations less than 90%
at rest or desaturate by more than 5% with exertion,
and have a maximal oxygen consumption less than
10 mL/kg/min are poor surgical candidates with
increased risk for postoperative pulmonary compli-

Box 1. Prerehabilitation assessment
Complete history and physical examination
Assess dyspnea and health-relatedquality of life
Cognitive evaluation
Mini-Mental Status ExaminationBaseline spirometryPulse oximetry or arterial blood gasCardiopulmonary testing
Determine baseline exercise capacity
Identify cardiac comorbidity orexercise-induced hypoxemia
Formulate exercise prescriptionNutritional assessmentPsychosocial evaluation
Assess support system, coexistingdepression or anxiety, copingand self-care skills
takaoka & weinacker208
cations [33]. Marginal patients are patients with
values intermediate to these criteria.
Table 3
Essential components and associated recommendations for a
multidisciplinary pulmonary rehabilitation program
Intervention Current recommendations
Exercise 20–30 min at least 3–5 times/wk
of muscle group–specific activity,
including aerobic, flexibility, and
strength training, targeting
improvement in dyspnea
Upper and lower
extremity
Ventilatory muscle
training
Use in patients refractory to other
forms of exercise (data conflicting)
Education Medication administration and
compliance, oxygen therapy,
symptom management, breathing
control techniques, nutrition,
energy conservation techniques,
respiratory and chest/airway
clearance methods
Psychosocial/behavior
modification
Smoking cessation, stress
management and coping skills,
end-of-life planning,
sexuality, self-management skills
Outcomes assessment Monitor domains of dyspnea,
health-related quality of life, and
exercise tolerance before, during,
and after rehabilitation
Initial prerehabilitation assessment
Before participation in a pulmonary rehabilitation
program, patients should undergo a formal evaluation
of their physical, mental, emotional, and social status
(Box 1). This assessment is important to ensure a
patient is an appropriate candidate for rehabilitation,
to identify any special areas of need the patient
may have, and to establish a baseline for comparison
with future assessments. An objective measurement
of dyspnea and health-related quality of life using
any one of a variety of rating scales or questionnaires
should be performed. Evaluation of the patient’s
cognitive function (most commonly done with the
Mini-Mental Status Examination) and educational
level also should be included to determine the
patient’s baseline capacities and to identify any
special needs or goals. Nutritional status should be
assessed because patients with severe COPD often
have changes in body weight, body composition, and
eating habits that all can affect exercise performance
negatively and increase mortality, independent of un-
derlying lung function [35]. Finally, patients should
undergo a full psychosocial assessment to evaluate
the level of social and family support, any coexisting
anxiety or depression, and patient coping and self-
care skills [5].
Essential components of pulmonary rehabilitation
Exercise training
Exercise training is a fundamental component
of any pulmonary rehabilitation program (Table 3)
and is the only element with strong support from
the literature. Although there are extensive variations
between programs with respect to exercise mode,
frequency, duration, and intensity, a reasonable ap-
proach uses the patient’s baseline activity level, re-
sults of exercise testing, and unique needs or goals
to determine the initial training regimen. Exercises
in flexibility, aerobic activities, and strength training
should be included. The desired frequency is initially
three to five times per week, increasing to daily, with
a minimum duration of 20 to 30 minutes including
periods of rest as needed. Minimal exercise intensity
is to 50% of maximal oxygen consumption or is
targeted to patient tolerance and gradually increased
[5]. Although heart rate is the traditional target pa-
rameter during exercise, dyspnea ratings are pref-
erable in this setting [36] because most patients with
chronic lung disease are limited by breathlessness,
breathing mechanics, and oxygen desaturation rather
than hemodynamic disturbances. Supplemental oxy-

preoperative pulmonary rehabilitation 209
gen should be used when necessary to maintain an
oxygen saturation 90% or greater during exercise.
Substantial evidence from controlled and uncon-
trolled studies indicates that specific lower extremity
training consistently leads to improvement in exercise
tolerance, particularly in tasks involving those muscle
groups. Typical training modes include walking,
treadmill exercises, stair climbing, and stationary
bicycle. Although the studies are limited by variations
in exercise prescription, there is general agreement
that lower extremity conditioning leads to significant
improvement in various outcome measures, most
notably in timed walk tests [6]. Although the data
for upper extremity exercise are less robust, arm
training usually is included in pulmonary rehabilita-
tion programs for several reasons. First, activities
involving primarily the upper extremities, which in-
clude many essential activities of daily living, seem
to have a higher ventilatory demand and are associ-
ated with more symptoms of dyspnea than are lower
extremity tasks. Second, the shoulder girdle elevates
the rib cage when the arms are anchored and can assist
in ventilation, decreasing the work of breathing during
a particular activity. Third, there is moderate evidence
suggesting that upper extremity exercises decrease
patient dyspnea and increase functional capacity. Up-
per extremity conditioning usually incorporates arm
ergometry or resistance exercises using 1- to 2-kg
weights or gravity [5].
Ventilatory muscle training, including sustained
hyperpnea and inspiratory resistance breathing, has
been proposed as an effective means of improving
respiratory muscle function, decreasing dyspnea and
increasing exercise tolerance. The current data are
largely conflicting, however, and do not support the
routine use of ventilatory muscle training in pul-
monary rehabilitation, although it may be employed
in specific patients who are refractory to optimal
therapy [6].
The benefit obtained with any type of training is
conferred largely to the muscles that undergo targeted
exercise (ie, 6-minute walk distance is improved with
leg but not arm training). Although some cross bene-
fit is seen, training should attempt to parallel the de-
sired outcome as much as possible. Some degree of
training reversibility occurs, and the conditioning
effects are maintained only as long as the activity is
continued [3]. The optimal duration and intensity of
postrehabilitation exercise have not been elucidated.
Chest physiotherapy
Chest physiotherapy, including postural drainage,
chest percussion, and flutter valve use, is applied
primarily to patients with purulent lung disease
(ie, cystic fibrosis, bronchiectasis, chronic bronchi-
tis). The goals of chest physiotherapy are to improve
ventilation and exercise tolerance and to decrease the
work of breathing [37]. Although chest physiotherapy
has been studied mainly in the postoperative setting,
limited data suggest that perioperative chest physio-
therapy may lead to fewer pulmonary complications
after surgery [38].
Education
Although poorly effective when used alone,
educational intervention is an essential component
of pulmonary rehabilitation and encompasses a
wide array of pertinent topics, including the proper
administration of medications (technique, compli-
ance, schedule, and side effects), use of supplemental
oxygen, nutritional support, strategies to relieve
dyspnea, pulmonary anatomy and physiology, and
the pathophysiology of COPD. Patients learn meth-
ods of energy conservation and work simplification,
which ultimately allow them to perform activities of
daily living more easily, and enable them to divert
energy toward other less essential tasks. They also are
taught breathing control techniques, such as pursed-
lip and diaphragmatic breathing [39]. Pursed-lip
breathing is performed by inhaling through the nose
and exhaling against partially closed lips. This
breathing technique theoretically reduces respiratory
rate, arterial carbon dioxide, and minute ventilation,
while increasing arterial oxygen tension, oxygen
saturation, and tidal volume. Diaphragmatic breath-
ing relies on the conscious expansion of the abdomi-
nal wall during inspiration to augment diaphragmatic
mechanical efficiency and reduce dyspnea. Data are
conflicting for both techniques, and some studies
show increased dyspnea using these techniques. In
the case of diaphragmatic breathing, there may be
decreased mechanical efficiency and increased work
of breathing [6].
Psychosocial support
Despite a lack of strong evidence supporting
psychosocial interventions, they are integral to a
multidisciplinary rehabilitation effort. Many patients
with chronic, disabling lung disease have concurrent
mood and thought disturbances, including anxiety,
depression, low self-esteem, poor body image, and
social withdrawal. These problems often are accen-
tuated in the preoperative setting because patients
often are dealing with a recent diagnosis of cancer,
are anxious about an upcoming surgery, or are

takaoka & weinacker210
waiting on the transplant list. As part of a compre-
hensive pulmonary rehabilitation program, patients
learn a variety of relaxation and coping techniques.
They are encouraged to discuss concerns regarding
intimacy and relationships with family and friends
and receive emotional support to do so.
Outcomes assessment
Outcomes monitoring is an essential aspect of
any rehabilitation program to assess patient response
and progress over time. There are three recommended
domains for outcomes monitoring: dyspnea, health-
related quality of life, and exercise tolerance [40].
Dyspnea is classified as either functional (limiting
performance of specific activities) or exertional and
is quantified with a patient-reported severity scale.
Health-related quality of life refers to a patient’s sat-
isfaction or happiness with life in the health domain.
Most rehabilitation programs use disease-specific
questionnaires, such as the Chronic Respiratory
Disease questionnaire or the St. George’s Respiratory
questionnaire, to monitor health-related quality of life
to predict outcomes after pulmonary rehabilitation
[6]. Exercise tolerance typically is monitored by ei-
ther a 6-minute walk or a submaximal or maximal
exercise test. Although less objective and more in-
fluenced by patient effort and motivation than a
submaximal or maximal exercise test, the 6-minute
walk test is a sensitive measure of response to reha-
bilitation and is simple and inexpensive [33]. Other
outcomes to assess include nutritional status, smok-
ing cessation, medication use and compliance, and
changes in anxiety or depression.
Summary
Although data are limited for preoperative pul-
monary rehabilitation, benefit can be inferred largely
from studies done on COPD and pulmonary rehabili-
tation because of the similarity of patient populations.
Although underlying lung function is unchanged, pa-
tients who undergo preoperative pulmonary rehabili-
tation seem to experience an enhanced quality of life
and increased functional capacity. Likewise, multi-
disciplinary rehabilitation programs can result in bet-
ter patient compliance with medications and smoking
cessation and decreased use of various health care re-
sources. Although pulmonary rehabilitation works to
benefit patients anticipating surgery, it also represents
a valuable treatment alternative to patients who are
poor surgical candidates. Pulmonary rehabilitation
seems to be a cost-effective, benign intervention with
no adverse effects and should remain an essential
component of patient management before lung trans-
plantation, LVRS, lung resection, and potentially any
other elective thoracic surgical procedure.
References
[1] National Emphysema Treatment Trial Research Group.
A randomized trial comparing lung-volume-reduction
surgery with medical therapy for severe emphysema.
N Engl J Med 2003;348:2059–73.
[2] Fishman AP, editor. Pulmonary rehabilitation: lung bi-
ology in health and disease, vol. 91. New York7Marcel
Dekker; 1996.
[3] American Thoracic Society. Pulmonary rehabilita-
tion—1999. Am J Respir Crit Care Med 1999;159:
1666–82.
[4] Fishman AP. Pulmonary rehabilitation research. Am J
Respir Crit Care Med 1994;149:825–33.
[5] Mahler DA. Pulmonary rehabilitation. Chest 1998;
113(4):263–8.
[6] Ries AL, Carlin BW, Carrieri-Kohlman V, et al.
Pulmonary rehabilitation: Joint ACCP/AACVPR evi-
dence-based guidelines. Chest 1997;112:1363–96.
[7] American Thoracic Society. Pulmonary rehabilitation.
Am Rev Respir Dis 1981;124:663–6.
[8] Cahalin LP. Preoperative and postoperative condition-
ing for lung transplantation and volume-reduction
surgery. Crit Care Nurs Clin N Am 1996;8:305–22.
[9] Palmer SM, Tapson VF. Pulmonary rehabilitation in
the surgical patient. Respir Care Clin 1998;4:71–83.
[10] Strijbos JH, Postma DS, Van Altena R, Gimeno F,
Koeter GH. A comparison between an outpatient
hospital-based pulmonary rehabilitation program and
a home-care pulmonary rehabilitation program in
patients with COPD. Chest 1996;109:366–72.
[11] National Emphysema Treatment Trial Research Group.
A randomized trial comparing lung-volume-reduction
surgey with medical therapy for severe emphysema. N
Engl J Med 2003;348:2059–73.
[12] Moy ML, Ingenito EP, Mentzer SJ, Evans RB, Reilly
JJ. Health-related quality of life improves following
pulmonary rehabilitation and lung volume reduction
surgery. Chest 1999;115:383–9.
[13] Criner GJ, Cordova FC, Furukawa S, et al. Prospective
randomized trial comparing bilateral lung volume
reduction surgery to pulmonary rehabilitation in severe
chronic obstructive pulmonary disease. Am J Respir
Crit Care Med 1999;160:2018–27.
[14] Craven JL, Bright J, Dear CL. Psychiatric, psychoso-
cial, and rehabilitative aspects of lung transplantation.
Clin Chest Med 1990;11:247–57.
[15] Dear CL, Grossman RF, Mauer JR. Preoperative
evaluation of patients awaiting lung transplant. Chest
1988;94(1):30S.

preoperative pulmonary rehabilitation 211
[16] Dear CL, Thomas J, Kesten S, Mauer JR. Impact of
preoperative pulmonary rehabilitation on the cystic
fibrosis lung transplant recipients [abstract]. Am J
Respir Crit Care Med 1994;149:A733.
[17] Biggar D, Trulock E, Patterson G, Cooper J. Compari-
sons of functional results of single versus bilateral lung
transplantation in COPD patients through three years
[abstract]. Am J Respir Crit Care Med 1994;149:A740.
[18] Biggar D, Trulock E, Patterson G, Cooper J. Medium
term results of pulmonary rehabilitation prior to lung
transplantation [abstract]. Am Rev Respir Dis 1993;
147:A333.
[19] Weiner P, Man A, Weiner M, et al. The effect of
incentive spirometry and inspiratory muscle training on
pulmonary function after lung resection. J Thorac
Cardiovasc Surg 1997;113:552–7.
[20] Rajendran AJ, Pandurangi UM, Murali R, Gomathi S,
Vijayan VK, Cherian KM. Preoperative short-term
pulmonary rehabilitation for patients of chronic ob-
structive pulmonary disease undergoing coronary artery
bypass graft surgery. Indian Heart J 1998;50:531–4.
[21] Weiner P, Zeidan F, Zamir D, et al. Prophylactic
inspiratory muscle training in patients undergoing
coronary artery bypass graft. World J Surg 1998;22:
427–31.
[22] Chumillas S, Ponce JL, Delgado F, Viciano V, Matue
M. Prevention of postoperative pulmonary complica-
tions through respiratory rehabilitation: a controlled
clinical study. Arch Phys Med Rehabil 1998;79:5–9.
[23] ZuWallack RL. Selection criteria and outcome assess-
ment in pulmonary rehabilitation. Mondaldi Arch
Chest Dis 1998;53:429–37.
[24] Ambrosino N, Foglio K. Selection criteria for pulmo-
nary rehabilitation. Respir Med 1996;90:317–22.
[25] Mohr DN, Lavender RC. Preoperative pulmonary
evaluation. Postgrad Med 1996;100:241–56.
[26] Burke JR, Duarte IG, Thourani VH, Miller JI. Pre-
operative risk assessment for marginal patients requir-
ing pulmonary resection. Ann Thorac Surg 2003;76:
1767–73.
[27] Szekely LA, Oelberg DA, Wright C, et al. Preoperative
predictors of operative morbidity and mortality in
COPD patients undergoing bilateral lung volume
reduction surgery. Chest 1997;111:550–8.
[28] Bluman LG, Mosca L, Newman N, Simon DG.
Preoperative smoking habits and postoperative pulmo-
nary complications. Chest 1998;113:883–9.
[29] Moller AM, Maaloe R, Pedersen T. Postoperative
intensive care admittance: the role of tobacco smoking.
Acta Anaesthesiol Scand 2001;45:345–8.
[30] Kroenke K, Lawrence VA, Theroux JF, et al. Operative
risk in patients with severe obstructive pulmonary
disease. Arch Intern Med 1992;152:967–71.
[31] Cordova FC, Criner GJ. Surgery for chronic obstruc-
tive pulmonary disease: the place for lung volume
reduction and transplantation. Curr Opin Pulm Med
2001;7:93–104.
[32] Datta D, Lahiri B. Preoperative evaluation of patients
undergoing lung resection surgery. Chest 2003;123:
2096–103.
[33] Brunelli A, Monteverde M, Al Refai M. Stair climbing
as a predictor of cardiopulmonary complications after
pulmonary lobectomy in the elderly. Ann Thorac Surg
2003;77:266–70.
[34] Burke JR, Duarte IG, Thourani VH, Miller JI.
Preoperative risk assessment for marginal patients re-
quiring pulmonary resection. Ann Thorac Surg 2003;
76:1767–73.
[35] Gray-Donald K, Gibbons L, Shapiro SH, Macklem PT,
Martin JG. Nutritional status and mortality in chronic
obstructive pulmonary disease. Am J Respir Crit Care
Med 1996;153:961–6.
[36] Horowitz MB, Littenberg B, Mahler DA. Dyspnea
ratings for prescribing exercise intensity in patients
with COPD. Chest 1996;109:1169–75.
[37] Certo C. Chest physical therapy. In: Hodgkin J,
Connors GL, Bell CW, editors. Pulmonary rehabilita-
tion: guidelines to success. 2nd edition. Philadelphia7
JB Lippincott Company; 1993. p. 232–3.
[38] Pashkow P, Ades PA, Emery CF, et al (Outcomes
Committee of the AACVPR). Outcome measurement
in cardiac and pulmonary rehabilitation. J Cardiopulm
Rehabil 1995;15:394–405.
[39] Tiep BL. Disease management of COPD with pulmo-
nary rehabilitation. Chest 1997;112:1630–56.
[40] De Torres JP, Pinto-Plata V, Ingenito E, et al. Power of
outcome measurements to detect clinically significant
changes in pulmonary rehabilitation of patients with
COPD. Chest 2002;121:1092–8.
[41] Cooper JD, Trulock EP, Triantafillou AN, et al.
Bilateral pneumonectomy (volume reduction) for
chronic obstructive pulmonary disease. J Thorac
Cardiovasc Surg 1995;109:106–16.
[42] Wilson DJ. Pulmonary rehabilitation exercise program
for high-risk thoracic surgical patients. Chest Surg Clin
N Am 1997;7:697–706.
Thorac Surg Clin
Informed Consent: Ethical and Legal Aspects
Carole A. Klove, RN, JDa,*, Sarah J. DiBoise, JDa, Betty Pang, JDb,
William C. Yarbrough, BAa
aStanford Hospital and Clinics and Lucile Packard Children’s Hospital, 300 Pasteur Drive, Stanford, CA 94305, USAbStanford University School of Medicine, 300 Pasteur Drive, Stanford, CA 94305, USA
Obtaining informed consent is only one of many
requirements necessary to any medical or surgical
procedure. In contrast to other checkbox items, ob-
taining patient consent, more specifically informed
consent, requires a progressive dialog between the
patient and physician—one in which the patient de-
velops an understanding of the procedure and its
risks and consequences, while the physician learns
about and manages the patient’s expectations.
Informed consent provides an opportunity for both
parties to engage in a meaningful discussion, ulti-
mately leading to a patient’s voluntary and informed
decision. In general, this process fulfills physicians’
ethical responsibilities and their legal duties to inform
patients fully of the diagnosis, prognosis, nature of
the procedure, risks and benefits associated with the
medical intervention, and any alternative treatments
that may exist.
If physicians fail to obtain informed consent,
what legal liability do they have? Originally, failure
to obtain consent was treated in the courts as the
intentional tort of battery [1]. Battery is best defined
as ‘‘an act that was intended to cause, and does cause,
an offensive contact with or unconsented touching of
or trauma upon the body of another’’ [2]. A plaintiff
suing under the theory of battery merely had to prove
that he or she had undergone an unconsented touch-
ing to prevail. The plaintiff needed to prove that
he or she was provided with inaccurate or mislead-
ing information as to the nature of the procedure or
its consequences.
1547-4127/05/$ – see front matter D 2005 Elsevier Inc. All rights
doi:10.1016/j.thorsurg.2005.02.005
* Corresponding author.
E-mail address: [email protected] (C.A. Klove).
Slowly over time, this theory of recovery gave
way to the present-day negligence theory in all
but one state (Pennsylvania) [3,4]. Although battery
still may constitute a theoretical basis for recovery
for medical malpractice, modern health care delivery
lends itself more readily to negligence as a basis of
recovery. To prevail on a theory of negligence, the
plaintiff (injured patient) must establish by a pre-
ponderance of the evidence (>50% likelihood) the
following four elements: (1) the physician owed a
duty to the patient to obtain his or her informed
consent, (2) the physician breached that duty, (3) the
physician’s breach directly and proximately caused
the patient’s injury, and (4) the patient suffered com-
pensable harm. This final element is crucial in that
an inability to show harm in a case of professional
negligence (malpractice) leaves the plaintiff without
the damages portion of his or her complaint and
with no right to recovery. Familiarity with the origins
of the informed consent doctrine and an awareness
of the salient issues surrounding current standards of
informed consent provide physicians with a greater
appreciation of the moral underpinnings and practical
application of this legal doctrine.
Development of the informed consent doctrine
‘‘Law pervades medicine because ethics pervades
medicine’’ [5]. In the health care domain, the law is
often perceived to be a restrictive intrusion on physi-
cian autonomy, and informed consent is yet another
legal doctrine that attempts to shift the focus of
medical decisions from the physician to the ultimate
15 (2005) 213 – 219
reserved.
thoracic.theclinics.com

klove et al214
risk bearer—the patient. The doctrine provides
another source of potential conflict between parties
who traditionally have been in a trusting relationship.
In Schloendorff v Society of New York Hospital,
[6] Justice Cordozo stated: ‘‘Every human being of
adult years and sound mind has a right to determine
what shall be done with his own body; and a surgeon
who performs an operation without his patient’s
consent, commits an assault, for which he is liable
in damages’’ [7]. The physician is bound by a pro-
fessional oath, an ethical code of conduct, and statu-
tory and case law always to act in the best interest of
the patient. In the process, patients receive valuable
input and guidance from a well-educated and knowl-
edgeable advocate and become equipped with the
information necessary to weigh the risks and benefits
for themselves and to proceed with or refuse treat-
ment [8]. The competent rendering of treatment by
physicians and disclosure of information are not the
sole measures of their duty to the patient. Physicians
maintain the additional duty of respecting the
patient’s right to follow or ignore their recommenda-
tions, even if they ultimately disagree with the
patient’s choice.
Physician’s legal duty: materiality
The legal duty of physicians to obtain consent for
treatment has its earliest roots in English law. The
first decision can be traced to the 1767 case of Slater
v Baker and Stapleton [9], in which the court es-
tablished the custom of obtaining consent from the
patient before surgery and assessing legal liability
when that custom was not followed. The Slater court
did not allow, however, for nuances as to whether or
not consent was indeed obtained; consent either
existed or it did not.
This concept of consent did not change until 1914
in Schloendorff v Society of New York Hospital [10].
In this case, the patient consented to an exploratory
surgery that led to the discovery and subsequent
removal of a fibroid tumor. The patient later de-
veloped a gangrenous infection requiring the removal
of several fingers. The court held that the patient
voluntarily consented only to the exploratory surgery
and not to the removal of the tumor and, by violating
the narrow consent given, ‘‘the ministers of healing
whom it [New York Hospital] has selected have
proved unfaithful to their trust’’ [11].
Schloendorff underscored the necessity of volun-
tary approval of a proposed procedure. Despite an
acknowledgment of the need for consent and narrow-
ing the doctrine’s application only to the specific
procedure, the consent doctrine was not fully fleshed
out—to require the physician to inform the patient
fully of relevant, material information that would
guide such a decision. Although far from today’s
model of informed consent, the court in Schloendorff
moved closer toward today’s concept of the patient as
the autonomous decision maker in the process of
electing to undergo a surgical procedure. Consent
given freely but without proper information is mean-
ingless. In 1957, the California Court of Appeals
in Salgo v Leland Stanford Jr. University Board of
Trustees directly addressed this issue.
The Salgo [12] case proved to be the defining
moment in an entirely different doctrine—informed
consent. The case involved the use of translumbar
aortography to determine the degree of blockage in
the descending aorta. The procedure required the
insertion of a large-bore needle into the aorta ap-
proximately 3 to 4 inches away from the patient’s
midline and spinal cord. After the surgery, the patient
was left paralyzed. The appeals court reversed on the
grounds that the trial court had misapplied the res
ipsa loquitur doctrine—a legal doctrine in which
negligence is inferred from injury—in a medical mal-
practice case. Remanding the case, the court stated:
‘‘[a] physician violates his duty to his patient and
subjects himself to liability if he withholds any facts
which are necessary to form the basis of an intelligent
consent by the patient to the proposed treatment’’
[13]. This conditioning of freedom of choice on the
disclosure of ‘‘material’’ information provided the
backbone of the informed consent model today.
Building on the decision in Salgo, two cases
decided in 1960 more clearly defined the affirmative
duty of a physician to disclose by describing the
information that was crucial to impart to the patient.
In Mitchell [14], the patient suffered several fractured
vertebrae while undergoing insulin and electroshock
therapy for schizophrenia. In Natanson [15], the
patient’s radiation therapy for breast cancer inflicted
severe damage to the muscle, skin, and bone beneath
her left arm. Mitchell set forth the simple directive
that risk of collateral damage must be disclosed, and
Natanson established the elements of informed
consent that are fully in force today: disclosure of
the nature of the ailment, nature of the proposed
treatment, consequences of that procedure, probabil-
ity of success, alternative treatments, and the risk of
unfortunate results.
A patient can make an informed decision only
after receiving and assimilating all relevant facts. The
physician must select that information that is ‘‘mate-
rial’’ to the patient. Commonly accepted elements of
a physician’s professional duty of disclosure include

1 Any physician who treats a patient shall inform the
atient about the availability of all alternate, viable medical
odes of treatment and about the benefits and risks of these
eatments. The physician’s duty to inform the patient under
is section does not require disclosure of: (1) Information
eyond what a reasonably well-qualified physician in a
imilar medical classification would know; (2) detailed
chnical information that in all probability a patient would
ot understand; (3) risks apparent or known to the patient;
) extremely remote possibilities that might falsely or
etrimentally alarm the patient; (5) information in emergen-
ies where failure to provide treatment would be more
armful to the patient than treatment; (6) information in
ases where the patient is incapable of consenting.
informed consent 215
diagnosis, prognosis, nature of the procedure, pur-
pose of the procedure, risks and benefits of the prof-
fered treatment, and alternative treatment options
(including nontreatment choices). Rooted in the basic
tenets of bodily integrity and individual autonomy, it
can be confusing to the physician to determine the
level of detail that a particular patient would find
material. Some light may be shed by reviewing what
courts have determined to be material generally and
in specific situations.
The present embodiment of the informed consent
doctrine was enumerated in 1972 [16]. In Canterbury
v Spence, the federal appeals court for the District
of Columbia reviewed a directed verdict in favor of
the physicians against a patient who had agreed to a
surgery to alleviate back pain and, as a consequence
of a postsurgery fall, became paralyzed. According
to the court, the central issue was an inadequate
disclosure by the physicians of risks and alternatives
of the surgical procedure. In deciding Canterbury, the
court provided guidance on the legal disclosure duty
of the physician. Recognizing the great disparity of
knowledge between patients and physicians and the
potential for abuse of patient rights, the court held
that ‘‘[t]o the physician, whose training enables a
self-satisfying evaluation, the answer may seem
clear, but it is the prerogative of the patient, not the
physician, to determine for himself the direction in
which his interests seem to lie’’ [17]. The Canterbury
court made clear that ‘‘[a] physician is under a duty to
treat his patient skillfully but proficiency in diagnosis
and therapy is not the full measure of his responsi-
bility’’ [18]. In determining that the proficient ad-
ministration of experienced care is not the sole gauge
of a physician’s competency, the court found that even
a task completed successfully could constitute mal-
practice if achieved without informed approval from
the patient.
The California Supreme Court also has recognized
this duty and extended it to include providing in-
formation relevant to the prevention of disease [19].
In Truman, the court was reluctant to find that the
patient’s family had no recourse when Truman’s phy-
sician, in failing to recommend annual pap smears,
prevented his patient from receiving a simple di-
agnostic procedure that may have led to earlier
treatment of her cervical cancer and saved her life.
The physician’s negligence in failing to recommend
a procedure that was standard practice within the
medical community negated his patient’s informed
choice. Relying on an earlier California case [20],
the Truman court reiterated the patient’s inherent
right to exercise control over [his or her] own body.
To be effective, the patient’s consent must be self-
determined and informed. In this case, the patient,
never having been empowered with material infor-
mation on which to base an informed decision, ex-
ercised neither element of consent.
Materiality, or relevance of information, is the
crucial factor in determining what facts and informa-
tion the physician must convey to the patient. Neither
the physician who overwhelms the patient with an
exhaustive list of procedures, consequences, benefits,
risks, and alternatives nor the physician who fails to
mention important facts has achieved his or her
purpose. What information is material? That is, what
must a physician include, and what may he or she
omit? The court in Arato [21], relying on the rea-
soning in Salgo and Natanson that ‘‘each patient
presents a separate problem’’ [22], found that mate-
riality is subjectively determined for a given patient
with a specific diagnosis, yet objectively determined
in that the physician must consider what a reasonable
person in the patient’s position would want to know
to make an informed decision. The Arato court held
that the physician is under no duty to disclose infor-
mation material to the patient’s nonmedical interests.
In this case, statistical life expectancy was found to
fall outside of medical interests and outside the pro-
tection of the doctrine of informed consent.
In a case involving a Wisconsin surgeon accused
of failure to obtain informed consent before a pro-
cedure to clip a cerebral aneurysm, the court greatly
expanded the surgeon’s duty of proper disclosure
[23]. In Kokemoor, the court found that in providing
information to the patient, the physician failed to
disclose his experience with the procedure and his
rate of success compared with other physicians and
failed to offer a tertiary care facility with more ex-
perienced physicians. The Wisconsin Supreme Court
extended the doctrine of informed consent and found
that all of these items were material [24].1 As stated
p
m
tr
th
b
s
te
n
(4
d
c
h
c

klove et al216
in Canterbury, these material facts are of the sort
‘‘demanding a communication’’ [25] by the physician
and, according to Kokemoor, ‘‘a physician of good
standing would have made the plaintiff aware of the
alternative of lower risk surgery with a different,
more experienced surgeon in a better-equipped
facility’’ [26].
Finally, in Moore [27], the California Supreme
Court held that treating physicians must disclose any
research or economic interests to patients as part of
the informed consent process. The court’s concern
was based in maintaining the integrity of a physi-
cian’s professional judgment in recommending medi-
cal procedures to patients. The court stated, ‘‘. . . aphysician who is seeking a patient’s consent for a
medical procedure must, to satisfy his fiduciary duty
and to obtain the patient’s informed consent, disclose
personal interests unrelated to the patient’s health,
whether research or economic, that may affect his
medical judgment’’ [28].
The above-described cases are a testament to a
variable concept of what constitutes material infor-
mation and what does not. Uniform measures of
materiality, aside from the large concepts in Natanson
or Canterbury, remain largely amorphous. Pragmati-
cally a physician’s duty is measured differently in
different jurisdictions. The standards as to what con-
stitutes material information generally fall into one of
three categories: physician-based disclosure, patient-
based disclosure, and a mixed or hybrid standard.
Although familiarity with the practices of other ju-
risdictions is not strictly required, it is recommended
that physicians have a general knowledge of the
standard set forth in their state of practice.
The physician-based standard is premised on the
notion that physicians encompass certain expert
knowledge that uniquely enables them to determine
what material information to impart to a patient de-
ciding whether or not to undergo a medical proce-
dure. This standard is an objective standard in that the
physician has a legal duty to disclose any information
that a reasonable physician in the same or similar
circumstances would provide to the patient for the
purpose of obtaining consent. This standard is the
most widely adopted and is the rule in roughly half
of all states.2 The primary advantage of a physician-
2 Alabama, Arizona, Arkansas, Colorado, Delaware,
Idaho, Illinois, Indiana, Kansas, Kentucky, Maine, Michi-
gan, Missouri, Montana, Nebraska, Nevada, New Hamp-
shire, New York, North Carolina, North Dakota, South
Carolina, Tennessee, Vermont, Virginia, and Wyoming.
based standard is that it enables the most knowl-
edgeable party to determine the materiality of the
information disclosed; this is also the chief criticism
because the physician’s determinations bear little
‘‘personal’’ responsibility and potentially deprive
the patient of the capability of making a truly in-
formed choice. Other disadvantages include the lack
of established customs in new procedures, discrep-
ancies between patient and physician’s concepts
of materiality, and the exact definition of a ‘‘reason-
able physician.’’
In contrast to the physician-based standard, the
patient-based standard requires the physician to
disclose any information that a reasonable patient
would consider material to a decision concerning his
or her medical treatment [29]. Nineteen states and the
District of Columbia have adopted the reasonable
patient standard.3 The basic premise is that the patient
who ultimately bears the consequences should deter-
mine what information is relevant in making his or
her decision. The patient-based standard is based on a
hypothetical ‘‘reasonable patient,’’ however, and the
physician is left with the problem of subjectively
determining what is important to a particular patient.
The physician-based standard affords the physician a
more objective standard shaped by formal education,
professional custom, and experience.
Finally, states adopting standards with elements
of patient-based and physician-based standards are
described as applying a hybrid standard. Six states
fall into this category: four by statute and two by case
law [30]. In states applying this standard, the
physician may be held to the standard of what the
reasonable physician would disclose in combination
with what the reasonable patient would desire to
know in making an autonomous choice.
Causation
In addition to showing that the physician owed a
duty to the patient and the physician breached that
duty, the plaintiff must prove that he or she was
injured and that the negligence of the practitioner was
a direct and proximate cause of the injury. The issue
of causation is a combination of two issues. First,
3 Alaska, Connecticut, Georgia, Hawaii, Iowa, Louisi-
ana, Maryland, Massachusetts, Minnesota, Mississippi, New
Jersey, Ohio, Oklahoma, Pennsylvania, Rhode Island, South
Dakota, Washington, West Virginia, and Wisconsin.

informed consent 217
decision causation [31] stipulates that had the physi-
cian completely disclosed all of the material infor-
mation, the patient would have chosen differently,
and injury would not have occurred. Second, treat-
ment or injury causation [31] is framed with respect
to the treatment rendered: The injury would have
never occurred but for the physician failing to ex-
ercise reasonable care. The latter concept does not
depend on hindsight and lends itself more readily
to proof and the judicial process.
Damages
Patients must show that they suffered actual
damages from the injury directly caused by the
physician’s failure to disclose material information.
Even if the patient suffered an injury, if that injury
caused no harm that could be remedied by a court
of law, the patient cannot recover under the negli-
gence theory.
Practical aspects
Aside from ethical and legal aspects, several prac-
tical aspects deserve attention. Patient competence to
comprehend a material disclosure is of great concern
to the physician in evaluating the patient’s decision-
making capacity. The determination that a patient is
incompetent to render a legally and medically cog-
nizable decision alters the health care dynamic.
The patient, traditionally a partner in the decision-
making process, may have his or her decision-making
capacity greatly limited. Medical decisions, previ-
ously the sole province of the patient, move to a third
party—a relative, a guardian, or a court appointed
guardian ad litem. The doctrine of informed consent
and all of its requirements still apply, however; the
decision normally reserved for the patient to make
simply is shifted to a surrogate with the mental ca-
pacity to make that determination.
Competence, as it relates to medical decision
making in informed consent, depends on a patient’s
individual capacity. Capacity, as defined by North-
ern, is the ‘‘mental ability to make a rational decision,
which includes the ability to perceive, appreciate all
relevant facts and to reach a rational judgment upon
such facts’’ [32]. Determinations of capacity have
been made in cases involving sexual consent [33],
entrance into contract [34], right to marry [35], exe-
cution of a will [36], ability to donate organs [37],
right to vote [38], and ability to stand trial [39].
Capacity in one context may be insufficient in an-
other, however. The manner in which competence is
evaluated, be it in a judicial hearing, a statutory pro-
vision, or a medical determination, is as varied as the
fields in which it is applied.
In most situations, a minor child is deemed to lack
sufficient capacity to arrive at a medical decision. Yet,
depending on the level of independence and maturity,
age, and the nature of the procedure, certain minors
have a statutory right to consent to the medical
intervention themselves; this generally does not apply
to a minor’s consent to surgery. A parent or guardian
would then act in the role of the child to determine
an appropriate and acceptable decision and give a
substituted informed consent.
The form in which patients receive informa-
tion and the complexity of the information used in
obtaining consent greatly influence a patient’s com-
prehension. Studies of patients’ recollection of infor-
mation gathered in the early stages of the consent
process indicate that patients receiving written infor-
mation, as opposed to verbal information, had greater
recall and recognition after surgery [40,41]. Com-
plexity of information within the consent form and
the patient’s reading ability or language proficiency
seem to have a further impact on comprehension [42].
Some researchers have suggested preconsent testing
of comprehension capacity in cases in which there are
questions as to the involvedness of the subject matter
or the mental ability of the patient [43].
Exceptions to obtaining informed consent
Informed consent is not required in all situations.
As with all rights, in certain situations, a patient’s
right to make a medical decision may be overridden.
In cases of emergency and patient waiver, the deci-
sion rests with the physician. In rare cases, a patient’s
decision may be overridden by the physician’s thera-
peutic privilege.
In cases of emergency, in which informed consent
cannot function properly because of the immediacy of
the situation, informed consent is excused. Where
time is of the essence, death or serious bodily injury
may result from inaction, and the treating physician
has no prior knowledge of the patient’s desire to
refuse the specific treatment administered, informed
consent is presumed, and medical intervention may
be undertaken without liability. In addition, a com-
petent patient holding the right to consent may waive
such rights and defer to the medical decision-making

klove et al218
power of the physician. In each circumstance, the
physician is acting as a surrogate for the patient.
Finally, the doctrine of therapeutic privilege al-
lows the physician to determine that disclosure of
information, although material, would actually harm
the patient. Owing to a strong paternalistic flavor,
therapeutic privilege often finds itself at odds with
informed consent and likewise has fallen out of favor.
Regardless of sound judgment or good intentions,
therapeutic privilege carries with it a measurable
cautionary note: Use sparingly and always document.
If any doubt exists as to whether or not to disclose
certain information, physicians should always err on
the conservative side and disclose.
Summary
The legal doctrine of informed consent looms
large over the medical profession with many interest
groups trying to expand and narrow the doctrine,
including patient rights advocates, managed care or-
ganizations, government agencies, and accreditation
organizations. The legal profession itself has taken no
small part in defining the doctrine. No physician
today is practicing without the daily influence of law
on his or her practice of medicine. The doctrine of
informed consent, with all of its ambiguities and
difficulties, has established a medical duty on the
physician to make a reasonable attempt to unite the
goals of the patient and the physician. Ultimately,
physicians gain from the knowledge that their
wisdom and skill has fostered a decision that is ame-
nable to the patient. The patient gains from a fa-
cilitated decision that truly reflects that individual’s
self-determined will. As a result, both parties enjoy
a newly formed partnership and the return of some-
thing that has long been taken for granted—trust in
the physician-patient relationship.
References
[1] Mohr v Williams, 95 Minn 261 (1905).
[2] Proffitt v Ricci, 463 A.2d 514, 517 (1983).
[3] Warren BJ. Pennsylvania medical informed con-
sent law: a call to protect patient autonomy rights by
abandoning the battery approach. 38 Duq L. Rev
917 (2000).
[4] Kottkamp NA. Finding clarity in a gray opinion:
a critique of Pennsylvania informed consent doctrine.
61 U. Pitt. L. Rev 241 (1999).
[5] Scott C. Why law pervades medicine: an essay on the
ethics in health care. 14 ND J.L. Ethics & Pub Pol’y
245, 245 (2000).
[6] Schloendorff v Society of New York Hospital, 105
N.E. 92 (1914).
[7] Schloendorff v Society of New York Hospital, 105
N.E. 93 (1914).
[8] Washington v Harper, 494 US 210 (1990).
[9] Berg JW, Appelbaum PS, Lidz CW, et al. The legal
requirements for disclosure and consent: history
and current status. In: Berg JW, Appelbaum PS, Lidz
CW, et al, editors. Informed consent: legal theory and
clinical practice. New York7 Oxford University Press;
2001. p. 42.
[10] Schloendorff, 105 N.E. 92 (1914).
[11] Schloendorff, 105 N.E. 95 (1914).
[12] Salgo v Leland Stanford Jr. University Board of
Trustees, 317 P.2d 170 (1957).
[13] Salgo v Leland Stanford Jr. University Board of
Trustees, 317 P.2d 181 (1957).
[14] Mitchell v Robinson, 334 S.W.2d 11 (1960).
[15] Natanson v Kline, 350 P.2d 1093 (1960).
[16] Canterbury v Spence, 464 F.2d 772 (D.C. Cir. 1972).
[17] Canterbury v Spence, 464 F.2d 781 (D.C. Cir. 1972).
[18] Canterbury v Spence, 464 F.2d 781 (D.C. Cir. 1972).
[19] Truman v Thomas, 611 P.2d 902 (1980).
[20] Cobbs v Grant, 8 Cal.3d 229 (1972).
[21] Arato v Avedon, 858 P.2d 598 (1993).
[22] Salgo v Leland Stanford Jr. University Board of
Trustees, 317 P.2d 170, 181 (1957), Natanson v Kline,
350 P.2d 1093, 1104 (1960).
[23] Johson v Kokemoor, 545 N.W. 2d 495 (1996).
[24] Wis. Stat. x 448.30.
[25] Canterbury v Spence, 464 F.2d 772, 787 (D.C.
Cir. 1972).
[26] Johson v Kokemoor, 545 N.W. 2d 495, 510 (1996).
[27] Moore v Regents of University of California, 51 Cal.
3d 120 (1990).
[28] Moore v Regents of University of California, 51 Cal.3d
120, 131–132(1990).
[29] Alaska Stat x 09.55.556.
[30] California (Cobbs v Grant, 8 Cal.3d 229 (1972)),
Florida (Fla Stat Ann x766.103), New Mexico (Gerety
v Demers, 589 P.2d 180 (1978)), Oregon (Ore Rev Stat
x 677.097), Texas (Tex. Civ Prac. & Rem. Code x74.101), and Utah (Utah Code Ann x 78–14–5).
[31] Berg JW, Appelbaum PS, Lidz CW, et al. Legal rules
for recovery. In: Berg JW, Appelbaum PS, Lidz CW,
et al, editors. Informed consent: legal theory and
clinical practice. New York7 Oxford University Press;
2001. p. 137–40.
[32] State of Tennessee, Dept. of Human Services v North-
ern, 563 S.W.2d 197, 209 (1978).
[33] Propes v State, 68 Ga. App. 418 (1942).
[34] Equipto Div Aurora Equip. Co. v Yarmouth, 1996
Wash. App. LEXIS 569 (1997).
[35] Johnson v Johnson, 214 Minn. 462 (1943).
[36] Estate of McKasson v Hamric, 70 Ark. App. 507 (2000).
[37] Curran v Bosze, 141 Ill. 2d 473 (1990).
[38] Pitts v Black, 608 F. Supp. 696 (1984).

informed consent 219
[39] Virgin Islands v Gumbs, 42 V.I. 79 (2000).
[40] Layton S. Informed consent in oral and maxillofacial
surgery: a study of the value of written warnings.
Br J Oral Maxillofac Surg 1994;32:34–6.
[41] Askew G. Informed consent: can we educate patients?
J R Coll Edinb 1990;35:308–10.
[42] Philipson SJ. Informed consent for research: a study
to evaluate readability and processability to affect
change. J Invest Med 1995;43:459–67.
[43] Mayberry MK. Towards better informed consent in
endoscopy: a study of information and consent pro-
cesses in gastroscopy and flexible sigmoidoscopy.
Eur J Gastroenterol Hepatol 2001;13:1467–76.

Thorac Surg Clin
Fast-Tracking: Eliminating Roadblocks to Successful
Early Discharge
Jules Lin, MDa, Mark D. Iannettoni, MD, MBAb,*
aDepartment of Surgery, Section of Thoracic Surgery, Office of Surgery Education, University of Michigan Medical Center,
TC 2207/0342, 1500 East Medical Center Drive, Ann Arbor, MI 48109, USAbDepartment of Cardiothoracic Surgery, University of Iowa Hospitals and Clinics, 200 Hawkins Drive, Room 1602-JCP,
Iowa City, IA 52242, USA
Ever-increasing health care costs and limited
medical resources have driven health care organiza-
tions to focus on key components of these costs, such
as the hospital length of stay (LOS). This article
summarizes some common obstacles to successful
early discharge that affect thoracic surgical patients.
Some authors also have identified criteria to predict
which patients are more likely to have a prolonged
LOS to anticipate better the needs of these high-risk
patients. Potential solutions to overcome these
obstacles are discussed in hopes of increasing the
rate of successful early discharge. The involvement
of thoracic surgeons in this process is essential to en-
sure that the quality of patient care is maintained and
perhaps even improved.
Although there are multiple reports on the deter-
minants for delayed discharge after chest surgery,
most describe series of cardiac surgical patients.
Several more recent series describe factors involved
in general thoracic surgery, however. In a prospective
study of 130 patients undergoing major pulmonary
resection, Irshad et al [1] identified factors associated
with a hospital stay greater than 6 days (Box 1). The
most frequent medical reasons for a delayed dis-
charge were persistent air leaks (12.3% of patients),
1547-4127/05/$ – see front matter D 2005 Elsevier Inc. All rights
doi:10.1016/j.thorsurg.2005.01.007
This article was supported by NIH T32 Surgical
Oncology Research Training Program CA009672-13.
* Corresponding author.
E-mail address: [email protected]
(M.D. Iannettoni).
pulmonary infections (6.1%), and atrial fibrillation
(5.1%), which increased the LOS by 13.1, 9.6, and
2.4 days. Cardinale, et al [2] found a 12% incidence
of atrial fibrillation after pulmonary resection for
lung cancer, but found no difference in LOS. Wright
et al [3] reported the most common reasons for failure
of early discharge were inadequate pain control and
persistent air leaks. Discharge delays after esopha-
gectomy also are due to pain control and respiratory
issues, in addition to concerns regarding anastomotic
healing and an enteral diet [4].
Although the mean medically required LOS was
6.9 days in the series reported by Irshad et al [1], the
average LOS was 7.35 days, suggesting additional
social obstacles to early discharge. The most common
cause was inadequate home support, which was found
in 10.2% of patients. Convalescent facilities were
unavailable in 7.1% of cases. Social factors resulted
in an increase of 44 hospital days per 100 patients.
Nonmedical factors were associated with age older
than 75, female gender, and a cancer diagnosis.
Preoperative interventions
Smoking cessation
Many patients presenting with lung cancer con-
tinue to smoke at the time of initial assessment for
pulmonary resection and are at an increased risk for
postoperative complications. Warner et al [5] showed
that smoking cessation more than 8 weeks before
15 (2005) 221 – 228
reserved.
thoracic.theclinics.com

Box 1. Common reasons for failure ofearly discharge
Medical factors
Inadequate pain controlPersistent air leakPulmonary infectionsAtrial arrhythmiaSevere nauseaFever
Social factors
Inadequate home supportUnavailability of convalescent facilities
lin & iannettoni222
coronary artery bypass decreased the risk of pulmo-
nary complications to that of nonsmokers, whereas
patients who quit less than 8 weeks preoperatively
showed no advantage. Studies have shown that even
1 to 2 minutes of advice results in 5% of pa-
tients quitting smoking, which increases with the
use of supplemental pamphlets [6]. Nicotine replace-
ment doubles cessation rates and can be combined
with bupropion.
Preoperative education
Patients should be instructed on the use of the
incentive spirometer and an exercise program if
appropriate. Thorens [7] reported that therapy ini-
tiated before surgery was more effective in reducing
pulmonary complications than therapy begun post-
operatively (47% compared with 27%). The expected
hospital course and discharge plans also should be
outlined clearly for patients and their families along
with a discussion of possible complications. In a pa-
tient satisfaction survey, Wright et al [3] found that
after proper education and instruction, most patients
were comfortable with an earlier discharge.
Intraoperative techniques
Muscle-sparing thoracotomy
Owing to the morbidity associated with a standard
posterolateral thoracotomy incision, alternative ap-
proaches have been developed. A muscle-sparing
thoracotomy preserves the latissimus dorsi and
serratus anterior muscles. Alkcali et al [8] performed
a prospective, randomized trial of 60 patients and
found that there was significantly less postoperative
pain in the muscle-sparing group, but that pulmonary
function and LOS were not significantly different. A
more recent report by de Lima and Carvalho [9]
found, however, that using a muscle-sparing thora-
cotomy contributed to a decrease in hospital stay. The
vertical axillary thoracotomy is another alternative
approach and may offer improved cosmesis and pre-
servation of shoulder girdle function.
Video-assisted thoracic surgery
Compared with thoracotomy, video-assisted tho-
racic surgery (VATS) decreases the amount of chest
wall trauma and postoperative pain. Although a
standard posterolateral thoracotomy may require an
incision 30 to 40 cm long, biopsies can be performed
through three 1-cm ports, and a VATS lobectomy is
performed using a 5- to 8-cm incision. The forced
expiratory volume at 1 second (FEV1), a measure of
pulmonary function, decreases approximately 30%
after a thoracotomy versus 15% in patients under-
going VATS [10]. There also is indirect evidence that
VATS may improve postoperative immune function
by reducing the body’s inflammatory response [11].
VATS is associated with a decreased LOS and an
earlier return to normal activities [12].
Thoracoscopic lung biopsy was evaluated as an
outpatient procedure in 62 patients at the University
of Michigan [13]. Chest tubes were removed in the
recovery room as long as there were no air leaks
and the chest radiograph did not reveal a pneumo-
thorax. Using these criteria, 72.5% of patients were
discharged on the same day of their operation with
an oral analgesic, and only 5% were admitted for
longer than 3 days. There was no operative mortality;
one patient required readmission for a pneumothorax.
Preventza et al [14] found that VATS wedge resection
could be performed with an overnight admission in
87% of patients in a retrospective review of 37 cases,
and that hospital charges were nearly half of that for
a thoracotomy.
Minimally invasive surgical techniques also can
be applied to pulmonary lobectomy and esophagec-
tomy. DePaula et al [15] performed laparoscopic
transhiatal esophagectomy in a series of 11 patients,
although there were no clear decreases in morbidity
or mortality. Nguyen et al [16] used a combined
laparoscopic and thoracoscopic approach for im-
proved visibility. Comparing a minimally invasive
series with historical open transthoracic and trans-
hiatal controls, these authors reported decreased use
of the ICU, blood loss, operating times, and LOS.

fast-tracking 223
Postoperative care
Pain control
Wright et al [3] identified inadequate pain control
as the most frequent reason for not being discharged
by the target date. Postoperative pain also is an
important factor affecting pulmonary function after
thoracotomy, and effective analgesia is crucial in
minimizing pulmonary complications. Intermittent
dosing of narcotics leads to widely varying levels
with inadequate pain control at the trough and depres-
sion of respiratory drive and the patient’s sensorium
at peak levels and can contribute to inactivity, nausea,
and hypotension. Patients with chronic obstructive
pulmonary disease also may be more susceptible to
the respiratory effects of narcotics. Modern analgesic
methods including patient-controlled analgesia, epi-
dural catheters, and regional intercostal nerve blocks
can improve patient comfort greatly and consequently
may lead to better pulmonary function in the post-
operative period.
Thoracic epidural analgesia has been used increas-
ingly in thoracic surgery and has been found to im-
prove vital capacity and functional residual capacity
by decreasing pain, leading to a reduced risk of pul-
monary complications [17]. de Lima and Carvalho
[9] reported that the use of epidural analgesia also
contributed to a decrease in the LOS. Berrisford et al
[18] found that intercostal nerve block with bupiva-
caine resulted in a postoperative FEV1 40% higher
than placebo, and Richardson et al [19] reported
similar results with preservation of postoperative
pulmonary function in patients treated with preinci-
sional pain prophylaxis and postoperative, continuous
intercostal nerve block. In a comparison of lumbar
epidural analgesia and a continuous intercostal
nerve block in 20 patients, no significant differences
were found in pain relief, oxygen saturation, or
pulmonary function [20]. Nausea was less frequent
in the intercostal block group, however, and vomit-
ing, pruritus, and urinary retention occurred only in
the patients with epidural analgesia. Other alterna-
tives include perioperative ketorolac, infiltration of
the incision with local anesthetic, and intercostal
nerve cryoanalgesia.
Persistent air leaks
Prolonged air leaks are a major determinant of
LOS and were identified by Wright et al [3] as the
second most common reason for failure to be dis-
charged by the target date. Rice and Kirby [21] found
that air leaks contributed an average of 5.6 extra days
to the hospital stay. Air leaks tend to occur at suture
lines, in areas of extensive dissection, and especially
in emphysematous lungs. The risk can be decreased
with meticulous operative technique. Patients at
high risk have been treated with various procedures
in the hopes of decreasing the incidence of air leaks,
such as buttressing the staple line with bovine peri-
cardium, pleural tenting, pneumoperitoneum, pleural
decortication, crushing the phrenic nerve, pleural
partition, and muscle flap transposition with varying
degrees of success.
Robinson and Preksto [22] described a series of
48 patients in which pleural tenting was performed
in 20 cases. They found a shorter duration of air leak
of 1.6 days versus 3.9 days, a shorter chest tube du-
ration of 4 days versus 6.6 days, less drainage, and
a decreased LOS of 6.4 days versus 8.6 days.
When an air leak has developed, some surgeons
believe that placing chest tubes to water seal may be
more effective than continuous suction. Cerfolio et al
[23] randomized 140 patients to water seal or suction
on postoperative day (POD) 2. Air leaks resolved in
67% of patients on water seal by POD 3. All of the
patients who did not resolve had leaks greater than
4/7 on an air leak meter. Only 1 of 15 patients (7%)
on suction sealed their air leak by POD 3. Based on
these results, air leaks greater than 4/7 are unlikely to
resolve on water seal, may lead to pneumothorax,
and should be treated with a Heimlich valve as an
outpatient. Cerfolio et al [23] concluded that water
seal is more effective than continuous suction in re-
solving air leaks, although the issue is controversial.
Wain et al [24] described using a bioresorbable
polyethylene glycol–based sealant in 172 random-
ized patients to prevent postoperative air leaks. A
significantly higher percentage of treated patients
were found to be free of air leaks, and there was a
trend toward earlier chest tube removal and decreased
LOS. Porte et al [25] also applied a prophylactic
synthetic sealant and found the percentage of pa-
tients free from air leaks on POD 3 and POD 4 was
higher; however, LOS was not significantly differ-
ent, and four patients developed empyema from in-
fected sealant.
Some authors have advocated outpatient treatment
of air leaks. Use of the Heimlich valve, a small-
caliber tube with a flutter valve, has been shown to
shorten the average LOS after various procedures
[26]. Careful monitoring and follow-up through a
well-coordinated clinic are required. Ponn et al [27]
described a series of 176 patients in which chest
tubes were managed on an outpatient basis, saving
1263 hospital days. The failure rate was 2% for

lin & iannettoni224
postresection air leaks with no mortality or life-
threatening events. McKenna et al [26] also described
the ambulatory management of prolonged air leaks in
25 patients using the Heimlich valve. Chest tubes
were removed an average of 7.7 days after discharge,
decreasing the mean hospital LOS by 46%.
Pulmonary infections
Patients undergoing pulmonary resection are at an
increased risk for respiratory complications because
of a higher incidence of chronic pulmonary disease;
postoperative diaphragmatic dysfunction; decreased
lung volumes; and impaired cough, mucociliary func-
tion, and gas exchange. Respiratory complications
often lead to a prolonged hospital LOS, increased
mortality, and higher costs. Long-term smoking is
the most important risk factor for lung carcinoma, and
Garibaldi et al [28] found that a smoking history was
a significant risk factor for postoperative pneumonia,
highlighting the importance of smoking cessation.
Postoperatively, pulmonary function is affected by
pain, diaphragmatic dysfunction, decreased respira-
tory effort, and lying supine for prolonged periods—
all of which can cause atelectasis and predispose to
pneumonia. In addition to aggressive pain control
and minimally invasive approaches, techniques have
been developed to improve atelectasis postopera-
tively, including cough and deep breathing exercises,
incentive spirometry, intermittent positive-pressure
breathing, and constant positive airway pressure.
Although these methods have not been assessed in
patients specifically undergoing lung resection, pro-
spective studies have been performed after upper
abdominal surgery. Morran et al [29] studied 102 pa-
tients in a randomized trial and found that pneumonia
was significantly reduced after routine postoperative
chest physiotherapy. Celli et al [30] prospectively
evaluated 172 randomized patients and found that
prophylactic regimens significantly reduced pulmo-
nary complications. In addition, a trend was seen
toward a decreased LOS, which was significant in the
incentive spirometry group.
Patients who are intubated in the ICU are at
the highest risk for nosocomial pneumonia. London
et al [31] noted a significant decrease in the incidence
of pneumonia using a prospective protocol that in-
cluded early extubation, and Tovar et al [32] recom-
mended extubation in the operating room when
possible. Early ambulation improves pulmonary
function, and Kamel et al [33] found that time to
ambulation was an independent predictor of the
development of pneumonia and a prolonged LOS.
Social factors
Although medical complications had the most
significant effect on delayed discharge, social factors
also were significant according to Irshad et al [1].
Extensive preoperative education is essential so that
patients and their families clearly understand the
expected postoperative course and possible compli-
cations. Early and proactive discharge planning also
should be initiated during preoperative planning.
Clinic nurses should identify high-risk individuals
who require referral to a case manager. Home support
and caregivers should be identified early, and if the
expected need for a convalescent facility is high,
arrangements should be made to assist in the efficient
transfer of care for the patient’s rehabilitation and
recovery. Postoperatively, restoration of the patient’s
mobility allows a return to independence and self-
sufficiency. At each step, the patient should be given
verbal and written instructions. In addition, a crucial
but often overlooked aspect of successful early
discharge is close, active follow-up with either phone
calls or office visits.
Clinical pathways
Although many of the above-described strategies
are being used individually, there is a large amount
of variation depending on the surgeon and the medi-
cal center. Rosen et al [34] reported that 75% of all
variability in LOS across hospitals is unexplained by
complications and mortality, and that a major reason
for this variability is differences in efficiency. Clinical
pathways (Table 1) have been devised to optimize
care and to help standardize clinical practice by
making all caregivers aware of the expected sequence
of events as patients proceed from a state of illness to
one of wellness. Patient progress in terms of pain
control, diet, and activity level is tracked and
documented, allowing earlier recognition of compli-
cations and intervention. Standard order sheets and
protocols help to reduce errors, and pathways should
be designed with variance codes to identify factors
leading to a prolonged hospital stay to improve future
efficiency. In addition, in academic medical centers,
pathways can help new residents quickly learn the
pattern of care as they rotate from month to month on
different clinical services. Clinical pathways have
been found to improve outcomes in the treatment of
a variety of diseases and have been reported to re-
duce LOS and hospital costs in cardiac surgery [35].
Although numerous studies have evaluated the
use of clinical pathways in thoracic surgery, most

Table 1
Sample clinical pathway for elective pulmonary resection*
Preop Day of operation POD 1 POD 2 POD 3–4
Education Expected course,
possible complications
Review pathway Review pathway,
discharge plans
Review pathway,
discharge plans
Discharge instructions
Interventions Smoking cessation Muscle-sparing
thoracotomy or
VATS, extubate
in OR, transfer to
floor if stable
d/c central line,
wean O2, place
chest tube to
water seal
d/c epidural,
Foley 8 h later,
1st chest tube if
no air leak
d/c 2nd chest tube if
no air leak and output
< 400 mL/d, if air leak
use Heimlich valve
Assessment History and physical Monitor chest
tube output,
cardiac rhythm
O2 saturation O2 saturation Adequate oxygenation,
pain control
Tests Preop labs, PFTs Labs prn, CXR Labs prn, CXR Labs prn, CXR Labs prn, CXR
Activity Exercise program
if appropriate
Ambulate with
assistance
Ambulate, PT
consult prn
Ambulate Ambulate
Medications Nicotine patch prn Preop antibiotics,
epidural, incentive
spirometer
Inhalers, chest PT,
antiemetics prn, d/c
antibiotics
Oral pain
medication prn
Oral pain
medication prn
Nutrition NPO after midnight Evening after OR
full liquids
Resume preop diet
Discharge
planning
Identify patients
for case manager
Confirm home
support
Identify the need
for rehabilitation or
home O2
Set up close follow-up
Abbreviations: CXR, chest x-ray; d/c, discontinue; labs, laboratory tests; NPO, nothing per mouth; OR, operating room;
PFTs, pulmonary function tests; POD, postoperative day; preop, preoperative; prn, as needed; PT, physical therapy; VATS,
video-assisted thoracic surgery.
* Clinical pathways are general guidelines, and variances in individual patient needs and responses are to be expected.
fast-tracking 225
have used historical controls, and the results of these
studies must be considered with caution until pro-
spectively controlled trials are performed. Although
Pearson et al [36] found that LOS decreased 7% for
thoracic procedures after the institution of a clinical
pathway, similar decreases were seen in neighboring
centers without clinical pathways. These authors
believed that the decrease in LOS seen may be due
to competitive pressures or patient selection bias.
Wright et al [3] evaluated the course of 284 pa-
tients undergoing lobectomy and found a decrease in
the LOS from 10.6 to 7.5 days and hospital costs
from $16,063 to $14,792 after the implementation
of a clinical pathway encouraging early discontinua-
tion of antibiotics, removal of chest tubes and epi-
dural catheters, and an aggressive protocol to treat
nausea. Of patients, 68% were discharged by the
target LOS of 7 days. Readmissions and mortality
were not significantly different.
Cerfolio et al [37] evaluated 500 patients who
underwent pulmonary resection using a clinical path-
way. Of patients, 96% were extubated in the operating
room, and 76% did not require admission to the ICU.
Patients with significant comorbidities or instability
were admitted to the ICU for an average of 1 day.
Epidural catheters and chest tubes were removed on
POD 2 if there was no air leak, and drainage was less
than 400 mL/d. The median day of discharge was
POD 4, and patient satisfaction was 91%.
Tovar et al [32] evaluated 10 patients who under-
went major lung resections with cryolysis of the
intercostal nerves and followed a clinical pathway
including extubation in the operating room, dis-
continuation of the Foley catheter and intravenous
fluids on discharge from the recovery room, and
transfer to an intermediate care unit where oxygen
was weaned and an oral diet and ambulation were
started. Chest tubes were removed when there was no
air leak the evening after the operation. Patients were
discharged when they were ambulating indepen-
dently, oxygenation was adequate, and pain was con-
trolled on oral medication. Eight patients were
discharged on the morning of POD 1 and two pa-
tients on POD 2. There were no readmissions, and
the investigators concluded that most patients can
be managed with a 1-day hospital stay after a major
pulmonary resection. In a second study, Tovar [38]
found that 70- and 80-year-old patients also could be
treated with a similar accelerated recovery program
with an average LOS of 1 day.

Fig. 1. The rate of postoperative recovery is significantly
associated (P = .0013) with the overall number of identified
risk factors. OP, day of operation. (From Ueda K, Kaneda Y,
Sakano H, Tanaka T, Li T, Hamano K. Obstacles for short-
ening hospitalization after video-assisted pulmonary resec-
tion for lung cancer. Ann Thorac Surg 2003;76:1816–20;
with permission from the Society of Thoracic Surgeons.)
lin & iannettoni226
Zehr et al [4] described the use of clinical path-
ways for esophagectomy and pulmonary resection. In
the esophagectomy pathway, patients were managed
in the ICU for 24 to 36 hours with overnight in-
tubation. Pain was controlled with epidural analgesia,
and central lines, cervical drains, and Foley catheters
were discontinued on POD 2. Enteral feedings were
started on POD 3 and advanced to 30 mL/h over
2 days. A video esophagram was performed on POD
5 or 6. Under the pathway, LOS decreased from
13.6 to 9.5 days. In the pulmonary resection pathway,
patients were extubated in the operating room with a
12- to 24-hour ICU stay. Pain was controlled with an
epidural catheter, and chest tubes were removed on
POD 3 or 4. The LOS decreased from 8 to 6.4 days.
Nomori et al [39] advocated the early removal
of chest tubes and oxygen support and found in
130 lung cancer patients that earlier removal resulted
in significantly less impairment of the 6-minute walk
distance 1 week postoperatively at 88.8% versus
81.5% of baseline. The clinical pathway encouraged
chest tube removal on POD 1 if there was no air leak
and output was less than 400 mL/d and discontinua-
tion of oxygen support if saturations were greater
than 90%. Only one patient required thoracentesis
after discharge. These authors concluded that chest
tubes and oxygen support restrict mobility and in-
crease patient discomfort and that removal allows
earlier ambulation and recovery of respiratory func-
tion and muscle strength.
Ueda et al [40] described the use of a clinical
pathway to manage patients after video-assisted pul-
monary resections in 40 patients with suspected lung
cancer in a prospective series. Recovery was consid-
ered complete when patients progressed through the
seven steps of the pathway, and the mean recovery
time was 3.7 days. Ueda et al [40] identified six
factors related to a prolonged hospital recovery, in-
cluding age greater than 65, breathlessness, radio-
graphic evidence of emphysema, poor performance
status, preoperative partial pressure of oxygen less
than 80 mm Hg, and a predicted postoperative FEV1
less than 60%. The number of risk factors was
significantly associated with the length of recovery,
and 100% of patients with no risk factors, 68% with
one to three risk factors, and 22% with four to six
risk factors recovered by POD 3 (Fig. 1).
For practitioners contemplating implementation of
clinical pathways, the pathways must be developed
with input from all members of the patient care team,
including surgeons, anesthesiologists, nurses, physi-
cal therapists, and social workers. Involving the care
team in the development process serves to educate the
hospital staff and encourages interest in improving
patient care and efficiency. A thorough review of the
literature should be performed to ensure that path-
ways are based on the best evidence available, with
the understanding that these guidelines can evolve as
more evidence becomes available. If equally valid
alternatives are presented, both can be included as
options in the pathway. Postdischarge patient satis-
faction surveys also are important as the pathways are
continually refined. In addition, it is important to
recognize that standardized clinical pathways are
guidelines intended to streamline patient care, while
improving quality and reducing errors, rather than
rigid protocols; many patients have unique needs
that cannot be managed by a uniform pathway.
Summary
With continually increasing health care costs and
limited medical resources, there has been increasing
focus on shortening hospital stays. Many medical and
nonmedical reasons can lead to a delay in hospital
discharge after thoracic surgery despite technically
successful procedures; common obstacles include
inadequate pain control, prolonged air leaks, and
social issues. Preoperative patient education, mini-
mally invasive surgical techniques, aggressive pain
control, and early resumption of physical activity and
discontinuation of chest tubes and catheters are im-
portant in successful early discharge. Although many
fast-tracking 227
of these components can be combined in clinical
pathways to optimize care with the input of various
members of the patient care team, the thoracic sur-
geon must reassess outcomes constantly to ensure the
maintenance of the quality of care.
References
[1] Irshad K, Feldman LS, Chu VF, Dorval JF, Baslalm G,
Morin JE. Causes of increased length of hospitalization
on a general thoracic surgery service: a prospective
observational study. Can J Surg 2002;45:264–8.
[2] Cardinale D, Martinoni A, Cipolla CM, et al. Atrial
fibrillation after operation for lung cancer: clinical
and prognostic significance. Ann Thorac Surg 1999;
68:1827–31.
[3] Wright CD, Wain JC, Grillo HC, Moncure AC,
Macaluso SM, Mathisen DJ. Pulmonary lobectomy
patient care pathway: a model to control cost and
maintain quality. Ann Thorac Surg 1997;64:299–302.
[4] Zehr KJ, Dawson PB, Yang SC, Heitmiller RF.
Standardized clinical care pathways for major thoracic
cases reduce hospital costs. Ann Thorac Surg 1998;66:
914–9.
[5] Warner MA, Divertie MB, Tinker JH. Preoperative
cessation of smoking and pulmonary complications in
coronary artery bypass patients. Anesthesiology 1984;
60:380–3.
[6] Fisher Jr EB, Rost K. Smoking cessation: a practi-
cal guide for the physician. Clin Chest Med 1986;7:
551–65.
[7] Thorens L. Postoperative pulmonary complications:
observations on their prevention by means of physio-
therapy. Acta Chir Scand 1954;107:194.
[8] Akcali Y, Demir H, Tezcan B. The effect of stan-
dard posterolateral versus muscle-sparing thoracotomy
on multiple parameters. Ann Thorac Surg 2003;76:
1050–4.
[9] de Lima NF, Carvalho AL. [Early discharge following
major thoracic surgery: identification of related fac-
tors]. Rev Port Pneumol 2003;9:205–13.
[10] Kaseda S, Aoki T, Hangai N, Shimizu K. Better
pulmonary function and prognosis with video-assisted
thoracic surgery than with thoracotomy. Ann Thorac
Surg 2000;70:1644–6.
[11] Leaver HA, Craig SR, Yap PL, Walker WS. Lympho-
cyte responses following open and minimally invasive
thoracic surgery. Eur J Clin Invest 2000;30:230–8.
[12] Nakajima J, Takamoto S, Kohno T, Ohtsuka T. Costs
of videothoracoscopic surgery versus open resection
for patients with of lung carcinoma. Cancer 2000;
89(11 Suppl):2497–501.
[13] Chang AC, Yee J, Orringer MB, Iannettoni MD.
Diagnostic thoracoscopic lung biopsy: an outpatient
experience. Ann Thorac Surg 2002;74:1942–7.
[14] Preventza O, Hui HZ, Hramiec J. Fast track video-
assisted thoracic surgery. Am Surg 2002;68:309–11.
[15] DePaula AL, Hashiba K, Ferreira EA, de Paula RA,
Grecco E. Laparoscopic transhiatal esophagectomy
with esophagogastroplasty. Surg Laparosc Endosc
1995;5:1–5.
[16] Nguyen NT, Schauer P, Luketich JD. Minimally
invasive esophagectomy for Barrett’s esophagus with
high-grade dysplasia. Surgery 2000;127:284–90.
[17] Wahba WM, Don HF, Craig DB. Post-operative epi-
dural analgesia: effects on lung volumes. Can Anaesth
Soc J 1975;22:519–27.
[18] Berrisford RG, Sabanathan SS, Mearns AJ, Bickford-
Smith PJ. Pulmonary complications after lung resec-
tion: the effect of continuous extrapleural intercostal
nerve block. Eur J Cardiothorac Surg 1990;4:407–11.
[19] Richardson J, Sabanathan S, Mearns AJ, Evans CS,
Bembridge J, Fairbrass M. Efficacy of pre-emptive
analgesia and continuous extrapleural intercostal
nerve block on post-thoracotomy pain and pulmo-
nary mechanics. J Cardiovasc Surg (Torino) 1994;35:
219–28.
[20] Richardson J, Sabanathan S, Eng J, et al. Continuous
intercostal nerve block versus epidural morphine for
postthoracotomy analgesia. Ann Thorac Surg 1993;
55:377–80.
[21] Rice TW, Kirby TJ. Prolonged air leak. Chest Surg
Clin N Am 1992;2:803–11.
[22] Robinson LA, Preksto D. Pleural tenting during upper
lobectomy decreases chest tube time and total hospi-
talization days. J Thorac Cardiovasc Surg 1998;115:
319–27.
[23] Cerfolio RJ, Bass C, Katholi CR. Prospective random-
ized trial compares suction versus water seal for air
leaks. Ann Thorac Surg 2001;71:1613–7.
[24] Wain JC, Kaiser LR, Johnstone DW, et al. Trial of a
novel synthetic sealant in preventing air leaks after
lung resection. Ann Thorac Surg 2001;71:1623–9.
[25] Porte HL, Jany T, Akkad R, et al. Randomized
controlled trial of a synthetic sealant for preventing
alveolar air leaks after lobectomy. Ann Thorac Surg
2001;71:1618–22.
[26] McKenna Jr RJ, Fischel RJ, Brenner M, Gelb AF. Use
of the Heimlich valve to shorten hospital stay after
lung reduction surgery for emphysema. Ann Thorac
Surg 1996;61:1115–7.
[27] Ponn RB, Silverman HJ, Federico JA. Outpatient
chest tube management. Ann Thorac Surg 1997;64:
1437–40.
[28] Garibaldi RA, Britt MR, Coleman ML, Reading JC,
Pace NL. Risk factors for postoperative pneumonia.
Am J Med 1981;70:677–80.
[29] Morran CG, Finlay IG, Mathieson M, McKay AJ,
Wilson N, McArdle CS. Randomized controlled trial
of physiotherapy for postoperative pulmonary compli-
cations. Br J Anaesth 1983;55:1113–7.
[30] Celli BR, Rodriguez KS, Snider GL. A controlled trial
of intermittent positive pressure breathing, incentive
spirometry, and deep breathing exercises in prevent-
ing pulmonary complications after abdominal surgery.
Am Rev Respir Dis 1984;130:12–5.
lin & iannettoni228
[31] London MJ, Shroyer AL, Jernigan V, et al. Fast-track
cardiac surgery in a Department of Veterans Affairs
patient population. Ann Thorac Surg 1997;64:134–41.
[32] Tovar EA, Roethe RA, Weissig MD, Lloyd RE, Patel
GR. One-day admission for lung lobectomy: an in-
cidental result of a clinical pathway. Ann Thorac Surg
1998;65:803–6.
[33] Kamel HK, Iqbal MA, Mogallapu R, Maas D,
Hoffmann RG. Time to ambulation after hip fracture
surgery: relation to hospitalization outcomes. J Ger-
ontol A Biol Sci Med Sci 2003;58:1042–5.
[34] Rosen AB, Humphries JO, Muhlbaier LH, Kiefe CI,
Kresowik T, Peterson ED. Effect of clinical factors
on length of stay after coronary artery bypass sur-
gery: results of the cooperative cardiovascular project.
Am Heart J 1999;138(1 Pt 1):69–77.
[35] Engelman RM, Rousou JA, Flack 3rd JE, et al. Fast-
track recovery of the coronary bypass patient. Ann
Thorac Surg 1994;58:1742–6.
[36] Pearson SD, Kleefield SF, Soukop JR, Cook EF, Lee
TH. Critical pathways intervention to reduce length of
hospital stay. Am J Med 2001;110:175–80.
[37] Cerfolio RJ, Pickens A, Bass C, Katholi C. Fast-
tracking pulmonary resections. J Thorac Cardiovasc
Surg 2001;122:318–24.
[38] Tovar EA. One-day admission for major lung resec-
tions in septuagenarians and octogenarians: a compa-
rative study with a younger cohort. Eur J Cardiothorac
Surg 2001;20:449–54.
[39] Nomori H, Horio H, Suemasu K. Early removal of
chest drainage tubes and oxygen support after a
lobectomy for lung cancer facilitates earlier recovery
of the 6-minute walking distance. Surg Today 2001;
31:395–9.
[40] Ueda K, Kaneda Y, Sakano H, Tanaka T, Li TS,
Hamano K. Obstacles for shortening hospitalization
after video-assisted pulmonary resection for lung
cancer. Ann Thorac Surg 2003;76:1816–20.

Thorac Surg Clin
Perioperative Antibiotics: When, Why?
Mark S. Allen, MDa,b,*
aDivision of General Thoracic Surgery, Mayo Clinic, 200 First Street, SW Rochester, MN 55905, USAbDepartment of Surgery, Mayo Medical School, Rochester, MN 55905, USA
Before Joseph Lister’s principle of antisepsis,
surgery commonly led to postoperative fevers, com-
monly known as ‘‘irrative fever,’’ followed by infec-
tion, drainage, ‘‘laudable pus,’’ sepsis, and death.
Since the introduction of antisepsis, surgery has pro-
gressed to an endeavor that prolongs and improves
life. About 27 million operations are performed each
year in the United States. Surgical site infections (SSI)
are the third most common nosocomial infection [1].
About two thirds of SSI develop in the surgical inci-
sion. In 1980, Cruse and Foord [2] estimated that
SSI increased hospital stay by 10 days and increased
costs by $2000, and a 1992 analysis revealed each
SSI increased costs more than $3000 and hospital
stay by 7.3 days [3]. Prevention of life-threatening
and costly SSI is important.
A variety of techniques should be considered to
decrease SSI, including recommendations for preop-
erative, intraoperative, and postoperative practices
that may reduce the risk of an infection. Careful sur-
gical technique with avoidance of unnecessary tissue
destruction is probably the most important factor in
decreasing the incidence of postoperative infections.
The use of perioperative antibiotics should be seen as
an adjunct to meticulous technique and proper
procedures. Perioperative antibiotics are thought to
decrease wound infections and may decrease other
SSI in general thoracic surgery, such as empyema and
postoperative pneumonias.
1547-4127/05/$ – see front matter D 2005 Elsevier Inc. All rights
doi:10.1016/j.thorsurg.2005.01.005
* Division of General Thoracic Surgery, Mayo Clinic,
200 First Street, SW Rochester, MN 55905.
E-mail address: [email protected]
The use of prophylactic antibiotics in general
thoracic surgery is well established. This article ex-
plains the rationale for modern-day surgical wound
infection prophylaxis, the why and the when. Various
arguments about the use of antibiotics to prevent
empyema and pneumonia after a thoracic operation
also are presented. The evidence supporting the use
of antibiotic prophylaxis for general thoracic surgical
procedures is overwhelming; however, despite nu-
merous well-done randomized trials, controversy still
exists as to when to stop the antibiotics, which agent
to use, and whether or not the use of antibiotics de-
creases wound infections only or wound infections
and deeper infections, such as pneumonia or em-
pyema (Table 1).
Prophylactic antibiotics were proposed by Eriksen
et al [4,5] in 1954, before any randomized study
had proven their efficacy. Kvale et al [6] reported the
first randomized study to examine the question in
1977. At that time, there was disagreement between
surgeons, who believed perioperative antibiotics
decreased infectious complications, and internists,
who believed perioperative antibiotics did not de-
crease infectious complications but increased resis-
tant organisms. The study by Kvale et al [6] was
the first randomized study on perioperative anti-
biotics for lung surgery since the introduction of
perioperative antibiotics. At Kvale’s institution, the
infection rate was 25% for all thoracic surgery
procedures, which the authors found unacceptable.
They conducted a randomized, prospective, double-
blind study from March 1974 to December 1975.
They gave cefazolin (Kefzol), 500 mg intramuscu-
larly on call and every 6 hours postoperatively until
orally tolerated, then cephalexin (Keflex), 500 mg
15 (2005) 229 – 235
reserved.
thoracic.theclinics.com

Table 1
Randomized studies concerning prophylactic antibiotics
Primary author Year Type of trial Agent(s) used
No.
patients
Wound
infection Pneumonia Empyema
Kvale [6] 1977 Prospective,
randomized,
double-blind
Cefazolin vs placebo 77 Significant
reduction
Significant
reduction
Significant
reduction
Truesdale [7] 1979 Prospective,
randomized,
double-blind
Cefazolin vs placebo 57 NSD NSD NSD
Cameron [8] 1981 Prospective,
randomized
Cephalothin vs placebo 171 NSD NSD NSD
Ilves [9] 1981 Prospective,
randomized,
double-blind
Cephalothin vs placebo 211 Significant
reduction
NSD NSD
Frimodt-
Moller [10]
1982 Prospective,
randomized,
double-blind
Penicillin G vs placebo 101 Significant
reduction
NSD NSD
Tarkka [13] 1987 Prospective,
randomized
Doxycycline
vs cefuroxime
120 NSD NSD NSD
Aznar [14] 1991 Prospective,
randomized,
double-blind
Cefazolin vs placebo 127 Significant
reduction
NSD Significant
reduction
Olak [11] 1991 Prospective,
randomized,
double-blind
Cefazolin 1 vs 6 doses 199 NSD NSD NSD
Krasnik [15] 1991 Prospective,
randomized,
double-blind
Penicillin G
vs Cefuroxime
94 NSD NSD NSD
Wertzel [12] 1992 Prospective,
randomized,
double-blind
Ampicillin/sulbactam
1 vs 3 doses
60 NSD NSD NSD
Frey [16] 1993 Prospective,
randomized
Cefuroxime vs placebo 200 NSD NSD NSD
Bernard [17] 1994 Prospective,
randomized,
double-blind
Cefuroxime vs placebo 203 NSD Chest x-ray
more often
normal
Significant
reduction
Boldt [18] 1999 Prospective,
randomized
Ampicillin/sulbactam
vs cefazolin
120 Not stated Significant
reduction
Not stated
Turna [19] 2003 Prospective,
randomized,
double-blind
Cefuroxime vs cefepime 102 NSD NSD NSD
Abbreviation: NSD, no significant difference.
allen230
orally every 6 hours for a total of 5 days, or placebo.
The vials were identical, so neither the staff nor the
patient knew who received antibiotics versus placebo.
Patients with prior chest infections, patients with
known allergies, patients who had received anti-
biotics within 1 week of surgery, and patients who
had refused informed consent were not eligible.
Specific protocols for postoperative management
and definitions of wound infection, pneumonia, and
empyema were established prospectively. The inves-
tigators randomized 77 patients undergoing pulmo-
nary surgery. Of the control group, 17 of 34 (50%)
developed ‘‘infection,’’ although 50% of these re-
ceived no further treatment. Only 8 of 43 (19%) of
the treated group developed infection (P = .005).
Kvale et al [6] concluded that ‘‘the routine use of
perioperative antibiotics is indicated to prevent post-
operative infections in pulmonary resection.’’
The results of the Kvale trial were challenged by
a subsequent randomized, prospective, double-blind
trial by Truesdale et al [7] in 1979. This group
randomized 57 patients undergoing pulmonary resec-

perioperative antibiotics 231
tion. They used cefazolin, 1 g intramuscularly on
admittance to the operating room, followed by cepha-
lothin (Keflin), 2 g intravenously every 6 hours for
48 hours, starting immediately after surgery, versus
placebo. The vials of antibiotic and placebo were
identical so that patients and physicians did not
know which patients were receiving antibiotics and
which were receiving placebo. In this study, 5 of
29 (17.2%) placebo patients and 5 of 28 (17.8%)
treated patients developed a postoperative infection
(P = not significant). Complications of prophylaxis
occurred in 17.2% (31 of 57) of placebo patients and
64.4% of treated patients and included hypersensi-
tivity reactions in 2, drug fever in 9, phlebitis in 14,
and increased blood urea nitrogen and liver function
tests in 8. Truesdale et al [7] concluded that pro-
phylactic antibiotics for pulmonary resection did not
outweigh the benefits and should not be employed.
This view was supported further by a larger
randomized trial by Cameron et al [8] from Johns
Hopkins Medical Center. They randomized 171 pa-
tients undergoing pulmonary resection to cephalo-
thin, 2 g intravenously the evening before surgery,
at 6:00 a.m. the morning of surgery, during the
operation, and 6 hours after surgery, or placebo (no
antibiotics). The hospital stay was 15.5 days for the
antibiotic group and 15.7 days for the placebo group.
There was no difference in the number of post-
operative fevers. The number of ‘‘septic complica-
tions’’ in the antibiotic group was 22 versus 26 in the
nonantibiotic group. Even when infections were
broken down into pneumonia, empyema, and wound
infection, there were no differences. The authors did
not give the actual numbers of wound infections, so it
is unknown if a trend was evident. They did find that
when postoperative infections occurred in the anti-
biotic group, they were often from gram-negative
organisms that were resistant to cephalothin. They
recommended that patients not receive prophylactic
antibiotics before pulmonary surgery.
Several months after Cameron’s study, the results
from an even larger study from the Toronto general
thoracic surgical group was published [9]. Ilves et al
[9] randomized 211 patients undergoing a pulmonary
or esophageal operation to receive either placebo or
cephalothin, 2 g intravenously at the induction of
anesthesia and 2 g intravenously 4 hours later. During
the study, neither the patients nor the staff knew
which group the patients were in. The surgical prepa-
ration, procedure, and postoperative care were stan-
dardized. The investigators found that 7 patients of
118 (5.9%) in the treatment group developed a wound
infection versus 22 of 93 (23.7%) in the placebo
group (P < .05). There also was a reduction in the
incidence of postoperative pulmonary infections and
empyemas, but the difference did not reach statistical
significance. The investigators were unable to detect
a difference in the bacteriology of the infections
between the two groups. Ilves et al [9] stated their
policy is to ‘‘employ prophylactic perioperative
antibiotic coverage in clean-contaminated major
thoracic cases.’’
A similar result was reported from Denmark by
Frimodt-Moller et al [10] in1982.Theycomparedpeni-
cillin G prophylaxis with placebo in a randomized,
double-blind, controlled prospective trial. The inves-
tigators used penicillin G at a dose of 5 million IU
intravenously immediately before surgery and every
6 hours after surgery for five doses. They random-
ized 94 patients: 45 in the penicillin G group and 47
in the placebo group. There were nine (19.1%)
wound infections in the placebo group versus two
(4.4%) in the prophylactic group (P = .03). There
was no difference in the number of empyemas or
lower respiratory tract infections between the two
groups. Frimodt-Moller et al [10] also showed a sig-
nificant reduction in the length of hospitalization
(3 days) with penicillin G prophylaxis, a highly cost-
efficient finding.
These two major positive studies seem to contra-
dict the study done by Cameron et al [8]. Perhaps the
wound infection rate was already so low at Johns
Hopkins that the study was underpowered to show a
significant difference. Whatever the reason, most
surgeons believed the positive findings of the Ilves
and Frimoldt-Moller studies and discounted the
negative findings of the Cameron study. Even though
most surgeons had been using prophylactic anti-
biotics for general thoracic surgical operations before
the publication of these studies, these findings con-
firmed what they empirically thought to be fact.
The question of whether to give a single dose or
prolonged postoperative prophylaxis was examined
in a randomized study by Olak et al [11], in which
they randomized 208 patients to one dose of cefazolin
(1 g intravenously at the induction of anesthesia) or
the induction dose of cefazolin plus five doses every
8 hours after surgery. They found no difference in the
number of wound infections, pneumonias, or empy-
emas between the two groups and concluded that
there was no benefit to prolonging the antibiotic
prophylaxis after the operation concluded.
Additional confirmation for use of only a single
dose comes from a randomized study done in Ger-
many by Wertzel et al [12]. This group randomized
60 patients undergoing pulmonary resection to re-
ceive ampicillin/sulbactam (Unasyn), either 3 g at
induction or 3 g at induction and two further doses at

allen232
8-hour intervals. They found no difference in the
incidence of wound infection or any other infections.
They did report about a 30% incidence of bronchitis
and pneumonia, but stated that, ‘‘whether PX
[prophylactic antibiotics] is reducing these complica-
tions cannot be answered by our study’’ [12].
With confirmation that prophylactic antibiotics
reduce wound infection rates and that a short course
is effective, interest was turned to studying ways of
decreasing the rate of pneumonia and empyema after
general thoracic surgical operations by employing
prophylactic antibiotics directed at respiratory flora.
In 1987, Tarkka et al [13] published a prospective,
randomized trial from Finland to determine if cefu-
roxime (Zinacef), an agent effective against the
common skin flora Staphylococcus aureus and the
respiratory pathogen Haemophilus influenzae, would
reduce the rates of wound infection and pneumonia
and empyema. They randomized 120 patients to
receive either their usual prophylactic antibiotic,
doximycin, 200 mg orally the day before surgery,
100 mg intravenously during the operation, and
100 mg orally every day for 3 days, or cefuroxime,
1.5 g during anesthesia induction and 0.75 g every
8 hours times three after surgery. The two groups
were comparable in all categories. They found a
significantly lower rate of minor lower respiratory
tract infections in the cefuroxime group, but no dif-
ference in the rate of pneumonia or empyema. Tarkka
et al [13] hypothesized that the bactericidal effects
of cefuroxime may account for the difference.
Aznar et al [14] tried to determine if cefazolin
alone would decrease the rates of empyema and
pneumonia. They randomized 143 patients and, after
excluding 16 patients, were left with 127 patients
(57 in the placebo group and 70 in the cefazolin group).
Cefazolin, 1 g intravenously one half hour before
surgery, was used. There was no significant differ-
ence in the demographics or operations performed
between the two groups. A marked difference in
wound infection (14% versus 1.5%) was shown, but
no statistically significant benefit for empyema (14%
versus 7%) or pneumonia (8.8% versus 4.3%) in the
placebo versus cefazolin group. Aznar et al [14] con-
cluded, as others had, that a preoperative dose of
prophylactic antibiotics decreased wound infection
rates but not the risk of pneumonia or empyema.
In the same year as Aznar’s study, 1991, Krasnik
et al [15] reported a randomized double-blind study
to examine if cefuroxime was better than penicillin G
in preventing empyema and pneumonia as the study
by Tarkka et al [13] had done. The medications were
started just before surgery and repeated every 8 hours
after surgery. Krasnik et al [15] analyzed 94 patients
(48 in the penicillin G group and 46 in the cefuroxime
group). They also found no difference in the rate of
pneumonia or empyema between the two groups and
concluded they still prefer penicillin G for prophy-
lactic antibiotics for pulmonary surgery.
A positive finding from the use of cefuroxime was
reported in a German trial [16]. Frey et al [16] com-
pared no antibiotics with one dose of cefuroxime,
1.5 g intravenously at the induction of anesthesia.
They found fewer wound infections and fewer pa-
tients with ‘‘pronounced infiltration’’ on daily chest
x-rays in the cefuroxime group. Also, the number of
patients requiring additional antibiotics was less in
the treated group compared with the placebo group.
The use of a control group with no antibiotics makes
interpretation of this study difficult.
Another positive study using cefuroxime was
published in 1994 [17]. Bernard et al [17] randomized
203 patients undergoing a general thoracic surgical
procedure. All patients received an induction dose of
cefuroxime, 1.5 g intravenously, and a second dose
2 hours later. Patients were then randomized to
cefuroxime, 1.5 g intravenously every 6 hours for
48 hours, or placebo. The investigators found a
marked reduction in the incidence of empyema: 6%
in the treatment group versus 15.6% in the placebo
group (P = .03). This finding is undoubtedly related
to the fact that seven patients in the placebo group
developed bronchial fistulas, whereas only two in the
treatment group developed fistulas. The development
of fistulas is thought to be unrelated to an infection,
but rather related to local factors at the bronchial
closure. Postoperative chest x-rays were more often
normal in the treatment group, but there was no
difference in the number of patients who developed
purulent expectorations and atelectasis associated
with a temperature greater than 38�C. No information
is given about length of stay for these patients.
Bernard et al [17] concluded, perhaps mistakenly, that
‘‘48-hour antibiotic prophylaxis regime decreases the
rate of deep infectious complications.’’
In another randomized trial that showed effective-
ness in reducing pneumonia, Boldt et al [18]
compared a single injection of cefazolin, 2 g intrave-
nously, with ampicillin/sulbactam, 1.5 g intrave-
nously. They also studied the microbiologic tracheal
aspirates of the two groups and found all the bacteria
were susceptible to the prophylaxis in the ampicillin/
sulbactam group, whereas 8 of 25 patients in the
cefazolin-only group had resistant organisms. They
found fewer bronchopulmonary infections in the
ampicillin/sulbactam group. The group given cefazo-
lin stayed in the ICU longer and incurred higher costs
than the ampicillin/sulbactam group.

Box 1. Centers for Disease Control andPrevention recommendations to reducesurgical site infections
Preoperative
1. When possible, identify and treatall existing infections
2. Do not remove hair preoperativelyat or around the incision, unless itinterferes with the operation
3. If hair is removed, remove it imme-diately before the operation, pref-erably with electric clippers
4. Control serum blood glucose levelsin all diabetic patients
5. Encourage tobacco cessation6. Do not withhold necessary blood
products7. Require patients to shower or
bathe with an antiseptic agent onat least the night before surgery
8. Thoroughly wash and clean at andaround the incision site to removegross contamination before per-forming antiseptic skin preparation
9. Use an appropriate antiseptic agentfor skin preparation
10. Apply preoperative antiseptic skinpreparation in concentric circlesmoving toward the periphery
11. Keep preoperative hospital stay asshort as possible
12. No recommendation to wean ste-roids, enhancenutrition, applymupi-rocin to nares, or enhance woundspace oxygenation
Intraoperative
Surgical team1. Keep nails short and do not wear
artificial nails2. Perform preoperative surgical scrub
for 2–5 minutes3. Obtain appropriate cultures from, and
exclude from duty, surgical personnelwho have draining skin lesions untilinfection has been ruled out or per-sonnel have received adequate ther-apy and infection has resolved
4. Wear a surgical mask that coversthe mouth and nose
5. Wear a cap or hood to cover fullyhair on the head and face
6. Use surgical gowns and drapes thatare effective barriers when wet
Ventilation1. Maintain positive-pressure ventila-
tion in the operating room with re-spect to the corridors and adjacentareas
2. Maintain a minimum of 15 airchanges per hour, of which at least3 should be fresh air
3. Filter all air through the appropriatefilters
4. Introduce all air at the ceiling andexhaust near the floor
5. Do not use UV radiation in the op-erating room to prevent SSI
6. Keep operating doors closed exceptas needed
7. Limit the number of personnel enter-ing the operating room to necessarypersonnel
Postoperative
1. Protect incision with a sterile dress-ing for 24–48 hours
2. Wash hands before and after dress-ing changes and any contact withthe surgical site
3. When an incision’s dressing must bechanged, use sterile technique
4. Educate the patient and family re-garding proper incision care, symp-toms of SSI, and the need to reportsuch symptoms
5. No recommendation on the need tokeep incision covered after 48 hoursor on the appropriate time to showeror bathe with an uncovered incision
Adapted from Mangram A, Horan T,Peason M, Silver L, Jarvis W. Guidelinefor prevention of surgical site infection,1999. Infect Control Hosp Epidemiol1999;20:247–78; with permission.
perioperative antibiotics 233

allen234
A more recent randomized trial comes from Tur-
key, where Turna et al [19] hypothesized that using a
third-generation cephalosporin may have greater
activity against gram-negative pathogens and reduce
the rate of postoperative pneumonias. They random-
ized 104 patients to receive either cephalexin, 1.5 g
intravenously 1 hour before surgery and every
12 hours for 48 hours postoperatively, or cefepime
(Maxipime), 1 g intravenously for 24 hours after sur-
gery. The study was powered to find a 30% difference
in the 40% infection rate in the investigators’ de-
partment. In contrast to the prior studies, these inves-
tigators found no difference in the infection rates
between the two groups, and the third-generation
cephalosporin was more expensive.
Even with these well-done randomized, double-
blind control trials, the use of prophylactic antibi-
otics to reduce the rate of pneumonia or empyema
remains controversial. At present, there are con-
flicting results in the literature, and the use of pro-
phylactic antibiotics is nonuniform throughout
thoracic surgery.
Highlighting the consequence of these conflicting
data is a 1990 study by LoCicero [20], in which he
surveyed 408 thoracic surgeons about their practice
of prophylactic antibiotic usage. A quarter of the
surgeons were from a university practice, and almost
three quarters were in a private practice. About half of
the respondents had been in practice for 5 to 15 years.
Prophylactic antibiotics were given in only 80.9%
of patients undergoing pulmonary resection, despite
the overwhelming evidence of effectiveness presented
earlier in this article. The percentage of use was
worse for esophageal operations (77.7%), open lung
biopsies (51%), or other thoracic procedures (52%).
The most commonly used drugs were cephalosporin
(54.4%) and late-generation cephalosporin (30.1%).
Almost all surgeons who gave prophylactic anti-
biotics gave them before the skin incision. The length
of administration also varied. In pulmonary resec-
tions, antibiotics were given for 1 day in 17%, 2 days
in 40.3%, 3 days in 21%, and greater than 3 days in
15.9%. For esophageal operations, the use tended to
be longer—for 2 days in 30%, 3 days in 18.9%, and
greater than 3 days in 38.3%.
The current guidelines for prevention of SSI are
available online (http://www.cdc.gov/ncidod/hip/ssi/
ssi.pdf). This document is a comprehensive descrip-
tion of procedures and techniques to minimize SSI.
Included is an excellent description about antimicro-
bial prophylaxis for all surgical procedures. It
emphasizes that prophylactic antibiotics are not an
attempt to sterilize tissues, but rather to reduce the
burden ‘‘to a level that cannot overwhelm host de-
fenses.’’ Four principles are outlined to maximize the
effectiveness of antimicrobial prophylaxis:
1. Use prophylaxis based on clinical trials.
2. Use a safe, inexpensive agent that is bacteri-
cidal for most contaminants (S. aureus for gen-
eral thoracic surgery).
3. Establish serum levels at the time of incision
(give on call to operating room).
4. Maintain levels during operation, and discon-
tinue ‘‘at most’’ a few hours after inci-
sion closure.
Also included in this document is a variety of
procedures and techniques related to skin preparation,
operating room environment, and medical personnel
hygiene to reduce SSI (Box 1). Given all the
recommendations, the best method of reducing
infection remains meticulous technique and attention
to detail.
References
[1] Mangram A, Horan T, Peason M, Silver L, Jarvis W.
Guideline for prevention of surgical site infection,
1999. Infect Control Hosp Epidemiol 1999;20:247–78.
[2] Cruse P, Foord R. The epidemiology of wound infec-
tion: a 10-year prospective study of 62,939 wounds.
Surg Clin North Am 1980;60:27–40.
[3] Poulsen KB, Bremmelgaard A, Sorenson AI, et al.
Estimated costs of postoperative wound infections. A
case-control study marginal hospital and social security
costs. Epidemiol Infect 1994;113:283–95.
[4] Eriksen K, Hansen J, Lund F. Postoperative infection
in surgery of the lung: prophylaxis with high level
systemic penicillin therapy. Acta Chir Scand 1954;107:
460–5.
[5] Eriksen K, Hansen J. Prophylactic use of antibiotics in
surgery of the lung. Acta Chir Scand 1964;128:651–8.
[6] Kvale P, Ranga V, Kopacz M, Cox F, Magalligan D,
Davila J. Pulmonary resection. South Med J 1977;
70(Suppl 1):64–9.
[7] Truesdale R, D’Alessandri R, Manuel V, Diacoff G,
Kluge R. Antimicrobial vs placebo prophylaxis in
noncardiac thoracic surgery. JAMA 1979;241:1254–6.
[8] Cameron J, Imbembo A, Keiffer R, Spray S, Baker R.
Prospective clinical trial of antibiotics for pulmonary
resection. Surg Gynecol Obstet 1981;152:156–8.
[9] Ilves R, Cooper J, Todd T, Pearson F. Prospective,
randomized, double-blind study using prophylactic
cephalothin for major, elective, general thoracic op-
erations. J Thorac Cardiovasc Surg 1981;81:813–7.
[10] Frimodt-Moller N, Ostri P, Pedersen I, Poulsen S.
Antibiotic prophylaxis in pulmonary surgery: a double-
blind study of penicillin versus placebo. Ann Surg
1982;195:444–50.

perioperative antibiotics 235
[11] Olak J, Jeyasingham K, Forrester-Wood C, Hutter J,
Al-Seerah M, Brown E. Randomized trial of one-dose
versus six-dose cefazolin prophylaxis in elective gen-
eral thoracic surgery. Ann Thorac Surg 1991;51:956–8.
[12] Wertzel H, Swoboda L, Joos-Wurtemberger A, Frank
U, Hasse J. Perioperative antibiotic prophylaxis in gen-
eral thoracic surgery. Thorac Cardiovasc Surg 1992;40:
326–9.
[13] Tarkka M, Pokela R, Lepojarvi M, Nissinen J, Karkola
P. Infection prophylaxis in pulmonary surgery: a ran-
domized prospective study. Ann Thorac Surg 1987;44:
508–13.
[14] Aznar R, Mateu M, Miro J, et al. Antibiotic prophy-
laxis in non-cardiac thoracic surgery: cefazolin versus
placebo. Eur J Cardiothorac Surg 1991;5:515–8.
[15] Krasnik M, Thiss J, Frimodt-Moller N. Antibiotic
prophylaxis in non-cardiac thoracic surgery: a double
blind study of penicillin vs. cefuroxime. Scand J Thorac
Cardiovasc Surg 1991;25:73–6.
[16] Frey D, Reichmann A-K, Mauch H, Kaiser D. ‘‘Single-
shot’’ antibiotikaprophylaxe in der thoraxchirurgie:
Senkung der postopertiven infektionstrate. Infection
1993;21(Suppl):35–44.
[17] Bernard A, Pillett M, Goudet P, Viard H. Antibiotic
prophylaxis in pulmonary surgery a prospective
randomized double-blind trial of flash cefuroxime
versus forty-eight-hour cefuroxime. J Thorac Cardio-
vasc Surg 1994;107:896–900.
[18] Bolt J, Piper S, Uphus D, Fussle R, Hempelmann G.
Preoperative microbiologic screening and antibiotic
prophylaxis in pulmonary resection operations. Ann
Thorac Surg 1999;68:208–11.
[19] Turna A, Kutlu C, Ozalp T, Karamustafaoglu A,
Mulazimoglu L, Bedirhan M. Antibiotic prophylaxis
in elective thoracic surgery: cefuroxime versus cefe-
pime. Thorac Cardiovasc Surg 2003;51:84–8.
[20] LoCicero J. Prophylactic antibiotic usage in cardio-
thoracic surgery. Chest 1990;98:719–23.
Thorac Surg Clin
Pulmonary Embolism Prophylaxis: Evidence for Utility in
Thoracic Surgery
Dean M. Donahue, MDa,b,*
aDivision of Thoracic Surgery, Harvard Medical School, Boston, MA 02114, USAbDivision of Thoracic Surgery, BLK1570, Massachusetts General Hospital, 55 Fruit Street, Boston, MA 02114, USA
The clinical presentation of pulmonary embolism
(PE) is a spectrum that ranges from asymptomatic
small emboli to a life-threatening condition with
profound cardiogenic shock. Most patients with PE
have deep vein thrombosis (DVT) that is clinically
not apparent. In a study by Girard et al [1], 82% of
venography-proven pulmonary emboli had ultra-
sound evidence of DVT; however, only 42% of these
patients had clinical signs or symptoms suggesting
DVT. Because most patients at risk for PE have
no clinical warning signs, an effective prophylaxis
against PE must be targeted at preventing DVT.
Despite the widespread concern for postoperative
PE, there has been little written regarding the in-
cidence of PE in patients undergoing thoracotomy
for lung resection. To date, there has been only
one prospective study of thoracic surgical patients
examining the incidence of PE [2]. In this study,
postoperative thromboembolism occurred in 19%
of patients (including 5% with pulmonary emboli).
Guidelines from the Seventh American College of
Chest Physicians Conference on Antithrombotic and
Thrombotic Therapy were published in 2004, but
these did not address prophylaxis recommendations
specific to thoracic surgical procedures [3]. Patients
undergoing major thoracic surgical procedures fre-
quently have several risk factors for developing
DVT, including older age, malignancy, and smoking
1547-4127/05/$ – see front matter D 2005 Elsevier Inc. All rights
doi:10.1016/j.thorsurg.2005.01.003
* Division of Thoracic Surgery, BLK1570, Massachu-
setts General Hospital, 55 Fruit Street, Boston, MA 02114.
E-mail address: [email protected]
(Box 1). Because these risk factors are thought to be
cumulative [4], an effective strategy for thrombopro-
phylaxis is an important component of postopera-
tive care.
Risk factors in thoracic surgical patients
Possibly the greatest risk factor for developing
PE is the necessity of undergoing a major surgical
procedure. Patients undergoing major surgery have an
approximately sixfold increase in risk of PE [3]. The
risk varies depending on the type of procedure per-
formed; most series identify a neurosurgical proce-
dure involving the brain or meninges as having the
highest incidence of symptomatic PE (approximately
6%) [5]. Orthopedic surgical procedures involving
hip or knee arthroplasty have an approximately 3%
incidence of PE, but there are few published data on
PE in patients undergoing thoracotomy. In a series of
337 patients undergoing pulmonary resection without
any prophylaxis against DVT, there was a 2.1% inci-
dence of clinically apparent PE [6]. When pneumatic
compression devices were used in the next 362 pa-
tients, the incidence of PE fell to zero.
The presence of cancer increases the risk of PE
by sixfold [7]. Cancer patients undergoing surgery
have twice the risk of developing DVT and a three-
fold increase in risk of a fatal PE compared with
patients without cancer [8,9]. The presence of malig-
nancy also is associated with a diminished response
to thromboprophylaxis [9]. A retrospective review of
autopsies performed in major US teaching hospitals
showed that 25% of patients dying with lung cancer
15 (2005) 237 – 242
reserved.
thoracic.theclinics.com

Box 1. Risk factors for venousthromboembolism
Acquired
Surgery or hospitalization with immobilityTraumaMalignancyPrevious or family history of PE or DVTAgePregnancy, oral contraceptive use,
or hormone replacement therapyCongestive heart failureChronic renal diseaseHypertensionLupus anticoagulant (antiphospholipid
antibody syndrome)ObesitySmokingImmobility, including prolonged air travelIndwelling venous foreign bodiesThoracic outlet obstruction
(Paget-Schroetter syndrome)Hyperhomocysteinemia
Inherited
Factor V Leiden mutationProthrombin gene mutationAntithrombin III deficiencyProtein C deficiencyProtein S deficiency
0
200
400
600
800
1000
1200
0-14
20-2
430
-34
40-4
450
-54
60-6
4
age (years)
Inci
den
ce (
per
100
,000
)
Fig. 1. Increasing risk of pulmonary thromboembolic events wit
Petterson TM, O’Fallon WM, Melton 3rd LJ. Trends in the inc
a 25-year population-based study. Arch Intern Med 1998;158:585
donahue238
had PE. In half of these patients, PE was the cause of
death [10].
Other features common to thoracic surgical pa-
tients, such as advancing age and smoking, increase
the risk of PE. Advancing age has been well estab-
lished as a risk factor for PE, including patients
undergoing surgical procedures. The risk has been
shown to rise exponentially with age (Fig. 1) be-
ginning at age 40 [11–13].
Although there have been several case reports
of PE after thoracic surgical procedures, there are
only three large published series. Ziomek et al [2]
published the only prospective series. They per-
formed preoperative venous duplex scanning of the
lower extremities and ventilation-perfusion scans in
77 patients, including 65 patients with cancer. Neither
subcutaneous heparin nor compression devices were
routinely employed; early ambulation/mobilization
was the only routine DVT prophylaxis. In this series,
there were four cases of DVT and one PE identified
preoperatively—all in patients who had prior surgery
within 1 year. After thoracotomy and pulmonary
resection, there was a 14% incidence of DVT and a
6% incidence of PE. The PE was identified at a mean
4.5 days after surgery (range 2–6 days). In 27% of
patients developing DVT, PE also was identified. The
one postoperative death in the series was due to PE.
Risk factors for the development of DVT included
cancer (compared with patients with benign pulmo-
nary disease), primary lung cancer (compared with
metastatic disease to the lung), adenocarcinoma
(compared with other cell types), and advancing age.
Kalweit et al [14] reported a series of 1735 patients
undergoing pulmonary resection for malignancy.
Prophylaxis against PE included intravenous heparin
70-7
480
-84
males
females
h age. (Adapted from Silverstein MD, Heit JA, Mohr DN,
idence of deep vein thrombosis and pulmonary embolism:
–93; with permission.)

Box 2. Options for thromboprophylaxis
Mechanical
Early ambulationGraduated compression stockingsIntermittent pneumatic compression
deviceInferior vena cava filter
Pharmacologic
Heparin
Unfractionated
Low-molecular-weightEnoxaparinDalteparinTinzaparin
Warfarin
pulmonary embolism prophylaxis 239
beginning on the first postoperative day. When
ambulatory, patients were changed to subcutaneous
heparin injections three times a day. Compression
stockings were placed on patients with varicose veins
or a prior history of DVT. In this series, the incidence
of massive PE was 1.6%, with 23 confirmed and
4 clinically suspected cases. Twenty-five of these
patients died, resulting in an overall PE-related
mortality of 1.4%. The postoperative mortality in
the series was 7.2%, with PE accounting for 20% of
the deaths. No data were provided on the over-
all incidence of DVT or nonlethal PE. Autopsies
performed on 20 of these cases revealed 19 patients
with a central embolism and 1 patient with peripheral
emboli. In half of the cases, DVT was found at
autopsy. Nearly all of the patients dying from PE had
their event occur between 13 hours and 4 days after
their operation. In half of these patients, the lethal PE
occurred within the first 48 hours after surgery; this
may reflect the delay in initiating thromboprophy-
laxis until the first postoperative day.
Direct thrombin inhibitorsLepirudin
Bivalirudin
Argatroban
Desirudin
MelagatranDirect factor Xa inhibitors
FondaparinuxActivated protein CTissue factor pathway inhibitorNematode anticoagulant peptide c2
Prophylaxis against pulmonary embolism
The methods available to reduce the risk of DVT
and PE are outlined in Box 2. Options for thrombo-
prophylaxis can be divided into mechanical and
pharmacologic methods.
Mechanical thromboprophylaxis
Mechanical means of reducing the risk of PE
include early ambulation, graduated compression
stockings, intermittent pneumatic compression (IPC)
devices, and inferior vena cava filters. These modali-
ties are particularly useful in patients in whom
the risk of bleeding reduces or prevents the use
of anticoagulants.
Early ambulation has reduced significantly the
incidence of ultrasound-documented and symptom-
atic PE in patients undergoing total hip arthroplasty
[15]. After a minor surgical procedure, early ambu-
lation is adequate prophylaxis for patients younger
than 40 years old with no additional risk factors. It is
useful only as an adjunct in prophylaxis for post-
operative thoracic surgical patients.
Elastic stockings or graduated compression stock-
ings were first shown to be effective in PE prevention
in 1952 [16]. Properly fitting stockings are estimated
to produce a 60% reduction in the relative risk of PE
in general surgical patients [17]. Improperly applied
or fitted stockings may result in a tourniquet effect
that reduces venous flow and increases the risk of PE
[18]. Properly fitted stockings should be placed
before the induction of anesthesia and worn through-
out the hospitalization. Although there are no con-
trolled studies of postoperative outpatient use, it is
reasonable to continue use of the stockings in patients
with limited mobility. Caution also needs to be taken
in patients with peripheral arterial disease to avoid
soft tissue injury [19,20]. If stockings are used, the
underlying skin should be checked frequently.
It is assumed that IPC devices reduce the risk of
PE by improving venous blood flow and reducing
stasis, although there is debate regarding the role of
IPC devices in activating local plasminogen and
subsequent fibrinolysis [21,22]. The reduction in
PE risk has been shown to be most pronounced in
individuals with a body mass index of less than
25 kg/m2 [23]. These devices are safe and have few
drawbacks; however, their efficacy depends on near-
continuous use in nonambulatory patients. IPC de-
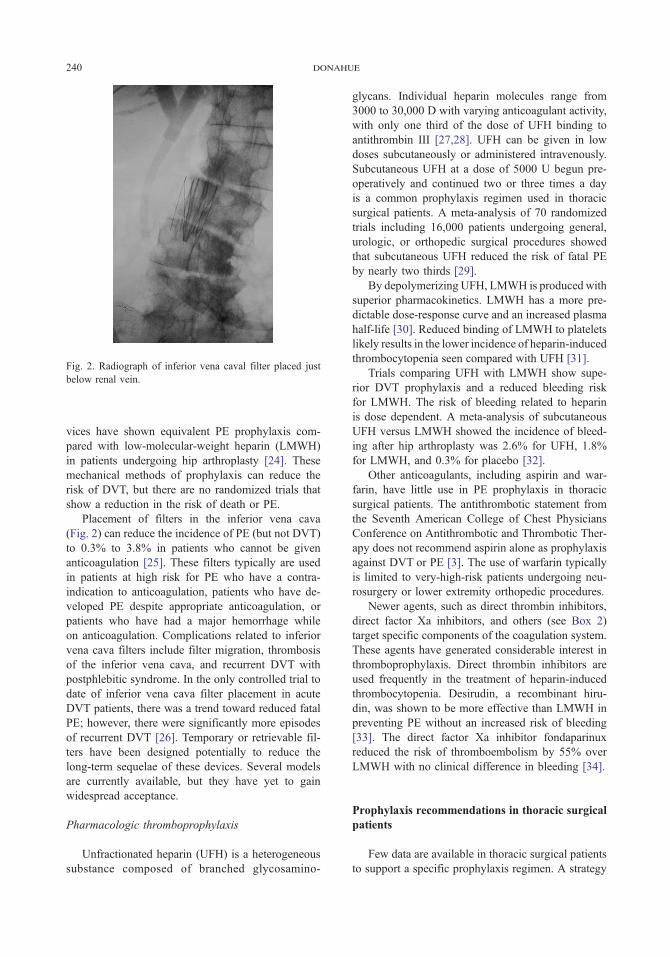
Fig. 2. Radiograph of inferior vena caval filter placed just
below renal vein.
donahue240
vices have shown equivalent PE prophylaxis com-
pared with low-molecular-weight heparin (LMWH)
in patients undergoing hip arthroplasty [24]. These
mechanical methods of prophylaxis can reduce the
risk of DVT, but there are no randomized trials that
show a reduction in the risk of death or PE.
Placement of filters in the inferior vena cava
(Fig. 2) can reduce the incidence of PE (but not DVT)
to 0.3% to 3.8% in patients who cannot be given
anticoagulation [25]. These filters typically are used
in patients at high risk for PE who have a contra-
indication to anticoagulation, patients who have de-
veloped PE despite appropriate anticoagulation, or
patients who have had a major hemorrhage while
on anticoagulation. Complications related to inferior
vena cava filters include filter migration, thrombosis
of the inferior vena cava, and recurrent DVT with
postphlebitic syndrome. In the only controlled trial to
date of inferior vena cava filter placement in acute
DVT patients, there was a trend toward reduced fatal
PE; however, there were significantly more episodes
of recurrent DVT [26]. Temporary or retrievable fil-
ters have been designed potentially to reduce the
long-term sequelae of these devices. Several models
are currently available, but they have yet to gain
widespread acceptance.
Pharmacologic thromboprophylaxis
Unfractionated heparin (UFH) is a heterogeneous
substance composed of branched glycosamino-
glycans. Individual heparin molecules range from
3000 to 30,000 D with varying anticoagulant activity,
with only one third of the dose of UFH binding to
antithrombin III [27,28]. UFH can be given in low
doses subcutaneously or administered intravenously.
Subcutaneous UFH at a dose of 5000 U begun pre-
operatively and continued two or three times a day
is a common prophylaxis regimen used in thoracic
surgical patients. A meta-analysis of 70 randomized
trials including 16,000 patients undergoing general,
urologic, or orthopedic surgical procedures showed
that subcutaneous UFH reduced the risk of fatal PE
by nearly two thirds [29].
By depolymerizing UFH, LMWH is produced with
superior pharmacokinetics. LMWH has a more pre-
dictable dose-response curve and an increased plasma
half-life [30]. Reduced binding of LMWH to platelets
likely results in the lower incidence of heparin-induced
thrombocytopenia seen compared with UFH [31].
Trials comparing UFH with LMWH show supe-
rior DVT prophylaxis and a reduced bleeding risk
for LMWH. The risk of bleeding related to heparin
is dose dependent. A meta-analysis of subcutaneous
UFH versus LMWH showed the incidence of bleed-
ing after hip arthroplasty was 2.6% for UFH, 1.8%
for LMWH, and 0.3% for placebo [32].
Other anticoagulants, including aspirin and war-
farin, have little use in PE prophylaxis in thoracic
surgical patients. The antithrombotic statement from
the Seventh American College of Chest Physicians
Conference on Antithrombotic and Thrombotic Ther-
apy does not recommend aspirin alone as prophylaxis
against DVT or PE [3]. The use of warfarin typically
is limited to very-high-risk patients undergoing neu-
rosurgery or lower extremity orthopedic procedures.
Newer agents, such as direct thrombin inhibitors,
direct factor Xa inhibitors, and others (see Box 2)
target specific components of the coagulation system.
These agents have generated considerable interest in
thromboprophylaxis. Direct thrombin inhibitors are
used frequently in the treatment of heparin-induced
thrombocytopenia. Desirudin, a recombinant hiru-
din, was shown to be more effective than LMWH in
preventing PE without an increased risk of bleeding
[33]. The direct factor Xa inhibitor fondaparinux
reduced the risk of thromboembolism by 55% over
LMWH with no clinical difference in bleeding [34].
Prophylaxis recommendations in thoracic surgical
patients
Few data are available in thoracic surgical patients
to support a specific prophylaxis regimen. A strategy

pulmonary embolism prophylaxis 241
can be developed based on data inferred from nu-
merous trials of patients undergoing other major
surgical procedures. These recommendations are
outlined in Table 1.
For prophylaxis against PE to be effective, it must
be initiated as soon as the risk of DVT begins. There
is little risk to applying properly fitted graduated
compression stockings. These stockings should be
placed preoperatively and continued until the patient
is consistently ambulating. IPC devices should be
placed and activated before the induction of anes-
thesia, when the period of immobility begins.
Pharmacologic prophylaxis should be used in
addition to mechanical measures in patients under-
going thoracotomy. Patients age 40 to 60 with no
additional risk factors undergoing surgery for benign
disease can receive subcutaneous UFH twice daily
or LMWH daily. A higher risk group includes any
patient older than 60 and any patient with cancer or a
prior DVT. This group should receive UFH three
times a day or LMWH at a dose of 3400 U or more
Table 1
Risk stratification for thromboembolism
Risk group % Fatal PE Prophylaxis
Low risk < 0.01 Early ambulation
Minor surgery, age < 40
Moderate risk 0.1–0.4 Subcutaneous
UFH bid
Minor surgery,
risk factors present
LMWH �3400 U qd
Major surgery, age < 60,
no risk factors
IPC or GCS
High risk 0.4–1 Subcutaneous
UFH tid
Major surgery, age > 60,
no risk factors
LMWH >
3400 U qd
Major surgery, age < 60,
single risk factor
IPC
Highest risk 0.2–5 LMWH >
3400 U qd
Patients with multiple
risk factors
Fondaparinux
Major trauma patients UFH or
LMWH plus
Spinal cord injury IPC and GCS
Abbreviations: GCS, graduated compression stockings; IPC,
intermittent pneumatic compression (device); LMWH, low-
molecular-weight heparin; UFH, unfractionated heparin.
Modified from Geerts WH, Pineo GF, Heit JA, et al.
Prevention of venous thromboembolism: the Seventh ACCP
Conference on Antithrombotic and Thrombolytic Therapy.
Chest 2004;126(3 Suppl):338S–400S.
daily. The highest risk group—anyone with more
than one risk factor—would receive this regimen plus
an IPC device and compression stockings.
References
[1] Girard P, Musset D, Parent F, Maitre S, Phlippoteau C,
Simonneau G. High prevalence of detectable deep
venous thrombosis in patients with acute pulmonary
embolism. Chest 1999;116:903–8.
[2] Ziomek S, Read RC, Tobler HG, et al. Thromboembo-
lism in patients undergoing thoracotomy. Ann Thorac
Surg 1993;56:223–6.
[3] Geerts WH, Pineo GF, Heit JA, et al. Prevention of
venous thromboembolism: the Seventh ACCP Confer-
ence on Antithrombotic and Thrombolytic Therapy.
Chest 2004;126(3 Suppl):338S–400S.
[4] Rosendaal FR. Venous thrombosis: a multicausal
disease. Lancet 1999;353:1167–73.
[5] White RH, Romano PS, Zhou H. A population-based
comparison of the 3-month incidence of thrombo-
embolism after major elective/urgent surgery. Thromb
Haemost 2001;86:2255–64.
[6] Nagahiro I, Andou A, Aoe M, Sano Y, Date H,
Shimizu N. Intermittent pneumatic compression is
effective in preventing symptomatic pulmonary embo-
lism after thoracic surgery. Surg Today 2004;34:6–10.
[7] Heit JA, Silverstein MD, Mohr DN, et al. Risk factors
for deep vein thrombosis and pulmonary embolism:
a population-based case-control study. Arch Intern
Med 2000;160:809–15.
[8] White RH, Zhou H, Romano PS. Incidence of symp-
tomatic venous thromboembolism after different elec-
tive or urgent surgical procedures. Thromb Haemost
2003;90:446–55.
[9] Gallus AS. Prevention of post-operative deep leg vein
thrombosis in patients with cancer. Thromb Haemost
1997;78:126–32.
[10] Ziomek S, Palmer H, Fink L, et al. Pulmonary embo-
lism and lung cancer: a postmortem study of 482 pa-
tients. Chest 1992;102:119S.
[11] Heit JA, Silverstein MD, Mohr DN, et al. The epi-
demiology of venous thromboembolism in the com-
munity. Thromb Haemost 2001;86:452–63.
[12] Silverstein MD, Heit JA, Mohr DN, Petterson TM,
O’Fallon WM, Melton 3rd LJ. Trends in the incidence
of deep vein thrombosis and pulmonary embolism:
a 25-year population-based study. Arch Intern Med
1998;158:585–93.
[13] Heit JA, Melton III LJ, Lohse CM, et al. Incidence
of venous thromboembolism in hospitalized patients
vs community residents. Mayo Clin Proc 2001;76:
1102–10.
[14] Kalweit G, Huwer H, Volkmer I, Petzold T, Gams E.
Pulmonary embolism: a frequent cause of acute fatality
after lung resection. Eur J Cardiothorac Surg 1996;
10:242–7.

donahue242
[15] Beuhler KO, D’Lima DD, Colwell Jr CW, Otis SM,
Walker RH. Venous thromboembolic disease after
hybrid hip arthroplasty with negative duplex screening.
Clin Orthop 1999;361:168–77.
[16] Wilkins R, Mixter G, Stanton J, Litter J. Elastic
stockings in the prevention of pulmonary embolism:
a preliminary report. N Engl J Med 1952;246:360–4.
[17] Jeffrey PC, Nicolaides AN. Graduated compression
stockings in the prevention of postoperative deep vein
thrombosis. Br J Surg 1990;77:380–3.
[18] Best AJ, Williams S, Crozier A, Bhatt R, Gregg PJ,
Hui AC. Graded compression stockings in elective
orthopaedic surgery: an assessment of the in vivo per-
formance of commercially available stockings in
patients having hip and knee arthroplasty. J Bone Joint
Surg Br 2000;82:116–8.
[19] Dismuke SE, Wagner EH. Pulmonary embolism as a
cause of death: the changing mortality in hospitalized
patients. JAMA 1986;255:2039–42.
[20] Anderson Jr FA, Wheeler HB, Goldberg RJ, et al.
A population-based perspective of the hospital inci-
dence and cause-fatality rtes of deep vein thrombosis
and pulmonary embolism. The Worcester DVT Study.
Arch Intern Med 1991;151:933–8.
[21] Allenby F, Boardman L, Pflugg JJ, Calnan JS. Effects
of external pneumatic intermittent compression on
fibrinolysis in man. Lancet 1973;2:1412–4.
[22] Calhan MA, Hanna DJ, Wiley LA, Cox DK, Killewich
LA. External pneumatic compression and fibrinolysis
in abdominal surgery. J Vasc Surg 2000;32:537–43.
[23] White RH, Gettner S, Newman JM, Trauner KB,
Romano PS. Predictors of rehospitalization for symp-
tomatic venous thromboembolism after total hip
arthroplasty. N Engl J Med 2000;343:1758–64.
[24] Warwick D, Harrison J, Glew D, Mitchelmore A,
Peters TJ, Donovan J. Comparison of the use of a foot
pump with the use of low-molecular-weight heparin for
the prevention of deep-vein thrombosis after total hip
replacement: a prospective, randomized trial. J Bone
Joint Surg Am 1998;80:1158–66.
[25] Streiff MB. Vena caval filters: a comprehensive re-
view. Blood 2000;95:3669–77.
[26] Decousus H, Leizorovicz A, Parent F, et al. A clinical
trial of vena caval filters in the prevention of
pulmonary embolism in patients with proximal deep-
vein thrombosis. Prevention du Pisque d’Embolie Pul-
monaire par Interruption Cave Study Group. N Engl J
Med 1998;338:409–15.
[27] Lam LH, Silbert JE, Rosenberg RD. The separation
of active and inactive forms of heparin. Biochem Bio-
phys Res Commun 1976;69:570–7.
[28] Anderson LO, Barrowcliffe TW, Holmer E, et al.
Anticoagulant properties of heparin fractionated by
affinity chromatography on matrix-bound antithrombin
III and by gel filtration. Thromb Res 1976;9:575–83.
[29] Collins R, Scrimgeour A, Yusuf S, Peto R. Reduction
in fatal pulmonary embolism and venous thrombosis
by perioperative administration of subcutaneous hepa-
rin: overview of results of randomized trials in gen-
eral, orthopedic, and urologic surgery. N Engl J Med
1988;318:1162–73.
[30] Weitz JI. Low-molecular-weight heparins. N Engl J
Med 1997;337:688–98.
[31] Warkentin TE, Levine MN, Hirsh J, et al. Heparin-
induced thrombocytopenia in patients treated with low-
molecular-weight heparin or unfractionated heparin.
N Engl J Med 1995;332:1330–5.
[32] Imperiale TF, Speroff T. A meta-analysis of methods
to prevent venous thromboembolism following total
hip replacement. JAMA 1994;271:1780–5.
[33] Eriksson BI, Wille-Jorgensen P, Kalebo P, et al. A
comparison of recombinant hiruden with a low-
molecular-weight heparin to prevent thromboembolic
complications after total hip replacement. N Engl J
Med 1997;337:1329–35.
[34] Turpie AGG. Overview of the clinical results of pen-
tasaccharide in major orthopedic surgery. Haemato-
logica 2001;86(Suppl 11):59–62.
Thorac Surg Clin
Management of the Anticoagulated Patient
Mark H. Meissner, MDa,b, Riyad Karmy-Jones, MDb,c,*
aDepartment of Vascular Surgery, University of Washington School of Medicine, Harborview Medical Center,
325 9th Avenue, Seattle, WA, 98195, USAbDepartment of Interventional Radiology, University of Washington School of Medicine, Harborview Medical Center,
325 9th Avenue, Seattle, WA, 98195, USAcDepartment of Cardiothoracic Surgery, University of Washington School of Medicine, Harborview Medical Center,
325 9th Avenue, Seattle, WA, 98195, USA
Patients who are to undergo surgery may be anti-
coagulated for therapeutic reasons (eg, deep venous
thrombosis [DVT], valve replacement, lytic therapy)
or because of comorbid conditions (eg, renal or he-
patic failure). In addition, the proposed operative in-
tervention may be elective or urgent. The approach to
managing the coagulation status is critically affected
by the circumstances and requires a basic understand-
ing of the risks involved of bleeding and correcting
the underlying pathophysiology. This article reviews
the indications, pharmacology, and complications of
common anticoagulation therapies (including labora-
tory and clinical assessment) in the surgical patient.
Coagulation system
Normal hemostasis requires the complex inter-
action of platelets; the endothelium; and more than
100 procoagulant, inhibitory, and fibrinolytic proteins
(Fig. 1). Primary hemostasis results in the immediate
formation of a platelet plug at the site of vascular
injury. The generation of thrombin (factor IIa), the
key effector enzyme of coagulation, and the conver-
sion of soluble fibrinogen to insoluble fibrin result
in the stabilization of the platelet plug by a secondary
1547-4127/05/$ – see front matter D 2005 Elsevier Inc. All rights
doi:10.1016/j.thorsurg.2005.01.006
* Corresponding author. Department of Surgery, Box
359796, Harborview Medical Center, 325 9th Avenue,
Seattle, WA 98195.
E-mail address: [email protected] (R. Karmy-Jones).
organized fibrin thrombus on the surface of acti-
vated platelets.
Coagulation is initiated either by mechanical in-
jury or cytokine-induced activation of endothelial
cells and monocytes. In either case, tissue factor, a
single-chain receptor for factor VII, is exposed as a
membrane protein. This pathway, also known as the
extrinsic pathway, is the most important physiologic
pathway for initiation of coagulation in response to
injury. Exposed tissue factor binds inactive factor VII
and activated factor VIIa, a small amount of which
circulates in blood. The tissue factor:VIIa complex
autoactivates factor VII and activates factors IX and X
[1,2]. Feedback amplification occurs as factor VII
bound to tissue factor is activated by factors VIIa,
IXa, and Xa.
Subsequent formation of the prothrombinase
complex, composed of phospholipid bound pro-
thrombin (factor II), factor Xa, and its factor Va
cofactor, results in the generation of thrombin from
prothrombin. There seems to be a threshold response
in which a certain level of initiating procoagulant
stimulus (VIIa– tissue factor) is required to produce
effective thrombin generation [3,4]. When this thresh-
old is reached, the amount of thrombin generated is
independent of the initiating stimulus. Thrombin
activates factors V, VIII, and XI, which cause feed-
back amplification through further activation of
factor IX. The thrombin-mediated conversion of
pro-cofactors V and VIII is particularly important
because the active cofactors serve to assemble the
prothrombinase and tenase complexes. Thrombin-
15 (2005) 243 – 262
reserved.
thoracic.theclinics.com
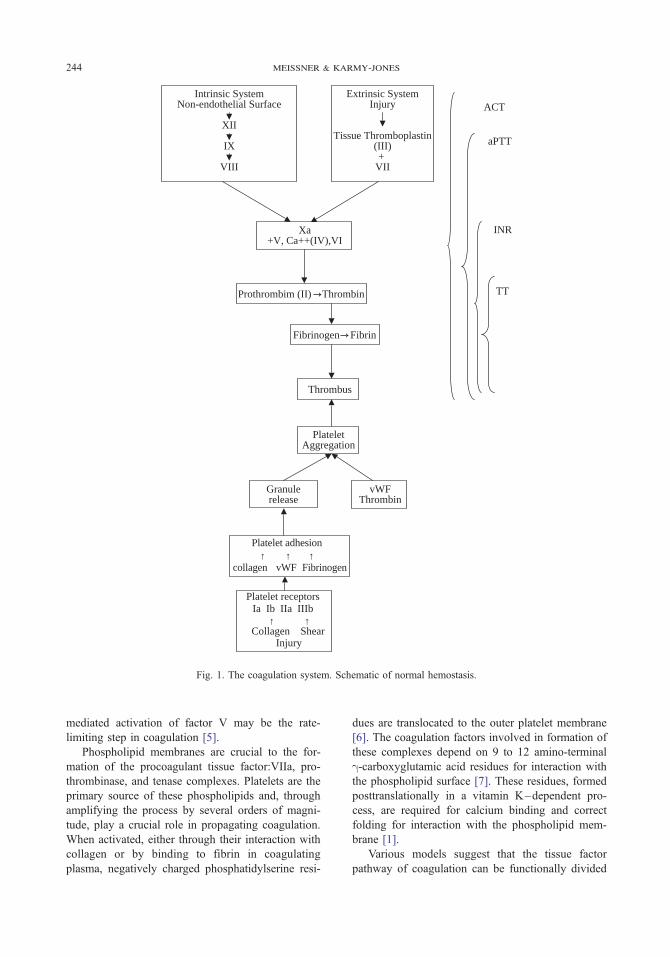
aPTT
INR
TT
Intrinsic SystemNon-endothelial Surface
XII
IX
VIII
Xa+V, Ca++(IV),VI
Prothrombim (II) Thrombin
Fibrinogen Fibrin
Thrombus
PlateletAggregation
Granulerelease
vWFThrombin
Platelet adhesion
collagen vWF Fibrinogen
Platelet receptorsIa Ib IIa IIIb
Collagen ShearInjury
Extrinsic SystemInjury
Tissue Thromboplastin(III)+
VII
ACT
↑ ↑ ↑
↑ ↑
Fig. 1. The coagulation system. Schematic of normal hemostasis.
meissner & karmy-jones244
mediated activation of factor V may be the rate-
limiting step in coagulation [5].
Phospholipid membranes are crucial to the for-
mation of the procoagulant tissue factor:VIIa, pro-
thrombinase, and tenase complexes. Platelets are the
primary source of these phospholipids and, through
amplifying the process by several orders of magni-
tude, play a crucial role in propagating coagulation.
When activated, either through their interaction with
collagen or by binding to fibrin in coagulating
plasma, negatively charged phosphatidylserine resi-
dues are translocated to the outer platelet membrane
[6]. The coagulation factors involved in formation of
these complexes depend on 9 to 12 amino-terminal
g-carboxyglutamic acid residues for interaction with
the phospholipid surface [7]. These residues, formed
posttranslationally in a vitamin K–dependent pro-
cess, are required for calcium binding and correct
folding for interaction with the phospholipid mem-
brane [1].
Various models suggest that the tissue factor
pathway of coagulation can be functionally divided

Table 1
Antithrombotic agents
Mechanism
of action
Currently
approved agents
Anticoagulants IIa / Xa inhibitors Unfractionated
heparin
Xa > IIa inhibitors Low-molecular-
weight heparins
Xa inhibitors Fondaparinux
IIa inhibitors Lepirudin
Bivalirudin
Argatroban
Tissue factor
pathway inhibitors
IXa inhibitors
Vitamin K
antagonists
Warfarin
Antiplatelet
agents
Cyclooxygenase
inhibitors
Aspirin
Phosphodiesterase
inhibitors
Dipyridamole
ADP antagonists Ticlopidine
Clopidogrel
GP IIb/IIIa
antagonists
Abciximab
Tirofiban
Eptifibatide
management of the anticoagulated patient 245
into two phases. During the initiation phase, nano-
molar amounts of thrombin and femtomolar to
picomolar quantities of factors VIIa, IXa, Xa, and
XIa are generated [8]. Most importantly, this phase
leads to quantitative activation of the Va and VIIIa
cofactors. The prothrombin time (PT) and activated
partial thromboplastin time (aPTT) measure only
the initiation phase of coagulation. The propagation
phase is characterized by explosive prothrombin acti-
vation and thrombin generation. This phase is largely
driven by the tenase complex–mediated activation
of factor X [8]. Most of the major congenital
deficiencies and clinically effective anticoagulants
have their major effect during the propagation phase.
The efficacy of most anticoagulants depends on their
ability to inhibit thrombin after formation of the
initial fibrin-platelet clot.
The physiologic importance of the intrinsic co-
agulation pathway, through which coagulation is
initiated by a combination of factor XII, high-
molecular-weight kininogen, prekallikrein, and fac-
tor XI, is unclear. The less important role of the
intrinsic pathway is suggested by the observation that
few deficiencies of the intrinsic pathway are asso-
ciated with bleeding. Thrombin-induced activation of
factor XIa is likely important in the propagation of
coagulation, however, generating sufficient factor IXa
to prevent severe bleeding, after the tissue factor
pathway has been terminated by its natural inhibitors
[2,4,6,7].
Negative regulators of coagulation include tissue
factor pathway inhibitor, which regulates the initia-
tion phase of coagulation, and the antithrombin (AT)
and the protein C systems, which regulate the propa-
gation phase. A tissue factor pathway inhibitor:Xa
complex binds VIIa– tissue factor to form an inactive
complex, limiting the initiation phase but allowing
sustained activation through factors VIIIa, IXa, and
XIa [3,4,7,9]. The protein C system is initiated by
the interaction of thrombin with endothelial bound
thrombomodulin. Undergoing a conformational
change, the thrombomodulin-bound thrombin loses
its activity toward fibrinogen and factors V, VIII, and
XIII and activates the vitamin K–dependent zy-
mogen protein C [7]. Activated protein C, together
with its protein S cofactor, cleaves phospholipid
bound factors VIIIa and Va. AT, a serine protease
inhibitor, is present in significant molar excess to its
target proteases and inhibits factors IIa, VIIa, IXa,
Xa, XIa, and XIIa. In contrast to the protein C
pathway, AT acts as a scavenger and preferentially
inhibits circulating, rather than membrane bound,
factors IIa and Xa. Thrombin bound to fibrin clot is
relatively protected from the action of AT. These
pathways function synergistically to limit more
effectively the response to tissue factor than any
single mechanism alone. The combination of tissue
factor pathway inhibitor and AT is 70-fold more
potent than either inhibitor alone.
Therapeutic anticoagulation
A variety of anticoagulation agents are currently
available, each with unique and at times comple-
mentary mechanisms depending on which part of the
coagulation cascade they primarily affect (Table 1).
Antiplatelet agents
Platelets play a significant role in many cardio-
vascular disorders and are an attractive target for
reducing long-term morbidity and mortality. Cur-
rently approved antiplatelet agents, used either as an
adjunct to vascular interventions or to reduce car-
diovascular morbidity, include aspirin; the adenosine
diphosphate (ADP) antagonists clopidogrel and ticlo-
pidine; and the glycoprotein (GP) IIb/IIIa antagonists
abciximab, eptifibatide, and tirofiban. Numerous trials

meissner & karmy-jones246
have established that antiplatelet therapy reduces the
risk of myocardial infarction (MI) and stroke by one
third and vascular death by one sixth among patients
with ischemic coronary or cerebrovascular disease
[10,11]. A meta-analysis of several randomized trials
including patients with vascular disease suggests a
25% reduction in the odds of sustaining an important
vascular event (stroke, MI, or vascular death) with the
use of antiplatelet agents [12]. The widespread use
of antiplatelet agents may account partially for the
reduction in mortality in patients with peripheral vas-
cular disease.
Aspirin has been the most widely studied anti-
platelet agent. It acts to inactivate permanently the
cyclooxygenase (COX) activity of prostaglandin H
synthase-1 and synthase 2 (COX-1 and COX-2) by
acetylation of the COX site in the enzymatic domain.
These isozymes catalyze the first step leading from
arachidonic acid to thromboxane A2, which induces
platelet aggregation and vasoconstriction, and pros-
taglandin I2, which inhibits platelet aggregation and
causes vasodilation. Aspirin undergoes extensive
first-pass hepatic metabolism to salicylate, a weak
reversible COX inhibitor. Despite its short half-life
(15–20 minutes), once-daily dosing is able to in-
hibit platelet thromboxane A2 production completely
through irreversible inhibition of COX-1 and has
proved equally effective in low (50–100 mg/d) and
high (900–1500 mg/d) doses [11]. In contrast, endo-
thelial prostaglandin I2 production is derived from
COX-1 and COX-2 activity, COX-2-dependent syn-
thesis being relatively aspirin resistant [13]. Never-
theless, even low doses of aspirin given over the
long-term reduce basal and stimulated prostacyclin
production [14]. Although the clinical relevance of
reduced prostacyclin production is controversial, use
of the lowest effective dose may maximize efficacy
and minimize toxicity. Aspirin has other effects at
high doses, including an anti-inflammatory action
and suppression of plasma coagulation, but it is
doubtful that these effects are as clinically relevant as
suppression of platelet thromboxane A2 production.
Because the mean life span of circulating platelets is
10 days, approximately 50% of platelets remain
functional 5 to 6 days after treatment.
The clinical role of dipyridamole, an inhibitor of
cyclic nucleotide phosphodiesterase that increases
cyclic adenosine monophosphate levels within plate-
lets, is controversial [15]. Although its efficacy
remains in doubt, more recent studies have suggested
a benefit in patients with prior stroke or transient
ischemic attacks compared with aspirin alone [13].
Ticlopidine and clopidogrel are thienopyridine
derivatives that selectively inhibit ADP-induced
platelet aggregation through permanent alteration of
a postulated ADP receptor. Both can be considered
prodrugs, being hepatically metabolized to an active
transient metabolite, and are considered to act through
similar mechanisms [15,16]. Both drugs increase the
bleeding time, with a maximal effect after 5 to 6 days
of oral administration. At least some trials have
suggested that the antiplatelet effect of ticlopidine
may delayed for 2 weeks, making ticlopidine a sub-
optimal agent when immediate antiplatelet effects
are required.
Clopidogrel is six times more potent and has a
better safety profile than ticlopidine and may be more
effective than aspirin among patients with symp-
tomatic peripheral arterial disease. Clopidogrel is
rapidly hepatically metabolized to an active platelet
inhibitor with a short half-life. Similar to aspirin, the
active metabolite of clopidogrel is thought to alter
platelet function permanently, with cumulative inhi-
bition on repeated daily dosing. At doses of 50 to
100 mg, clopidogrel requires 4 to 7 days to reach a
steady state of 50% to 60% inhibition of ADP-
induced platelet aggregation. Loading doses of the
drug (300 mg) result in much more rapid inhibition,
however [13]. Approximately 7 days are required for
platelet function to return to normal after cumulative
doses are stopped. The bleeding risk associated with
clopidogrel is approximately equivalent to that of
aspirin, although aspirin is more likely to cause gas-
trointestinal bleeding [17].
Aspirin and the thienopyridines target only
thromboxane A2 and ADP-mediated platelet aggre-
gation, leaving the action of other agonists intact.
It is now recognized that the integrin aIIbb3 (GPIIb/
IIIa) is the final common pathway of platelet ag-
gregation and that receptor antagonists are potent
inhibitors of platelet aggregation [13]. Expression
of the GPIIb/IIIa integrin mediates fibrinogen bind-
ing to platelets through the Arg-Gly-Asp (RGD)
and Arg-Gly-Asp-Ser (RGDS) amino acid sequences
of fibrinogen, von Willebrand factor, and fibronec-
tin [15]. Many GPIIb/IIIa inhibitors have been
developed, including monoclonal antibodies, pep-
tides containing the RGD sequence, and RGD
mimetics. The monoclonal antibodies, such as ab-
ciximab (ReoPro,) are noncompetitive antagonists,
whereas the peptides and peptidomimetics are com-
petitive inhibitors [18]. In addition to their anti-
platelet effects, these agents diminish thrombin
generation through reduced phosphatidylserine
exposure and factor V binding [6]. For unclear
reasons, antibody antagonists of GPIIb/IIIa are better
inhibitors of thrombin generation than are the pep-
tide inhibitors.

management of the anticoagulated patient 247
Indirect thrombin inhibitors
Unfractionated heparin
Compounds that inhibit thrombin by potentiat-
ing the action of AT, such as unfractionated heparin
(UFH) and low-molecular-weight heparin (LMWH),
are known as indirect thrombin inhibitors. Although
the use of bovine products has declined with the ap-
pearance of bovine spongiform encephalopathy, UFH
is prepared from tissue extracts of porcine intestine
or bovine lung [19]. Commercially available products
are a heterogeneous mixture of glycosaminoglycans.
Pharmacology and mechanism of action. Heparin
acts primarily to catalyze the antithrombin (AT)-
mediated inhibition of thrombin (factor IIa) and
factors IXa, Xa, IXa, and XIIa; the greatest clinical
effect is on factors IIa and Xa. In the absence of a
catalyst, either endothelial heparan sulfates or exoge-
nous heparin, AT inactivates thrombin and factor
Xa at a low basal rate. Heparin binding to AT causes
a 9000-fold and 17,000-fold increase in inhibi-
tory activity against thrombin and factor Xa [20].
Neither UFH nor LMWH is able to inactivate
phospholipid-bound factor Xa or fibrin-bound throm-
bin. Fibrin-bound thrombin is protected from the
action of AT by formation of heparin/thrombin/
fibrin complexes that render it inaccessible to AT-
bound heparin.
The structure and size of the individual heparin
chains determine their ability to catalyze inhibition of
thrombin and factor Xa. The catalytic effect of
heparin depends on the binding of a unique penta-
saccharide sequence to a specific site on AT, pro-
ducing a conformational change that exposes its
reactive center. This pentasaccharide sequence is
present in only 20% to 50% of UFH chains and even
fewer LMWH chains [19]. AT-mediated inactivation
of factor Xa requires only the presence of the appro-
priate pentasaccharide sequence, whereas binding
to factor IIa further requires a flanking chain 15 to
16 saccharide units in length and containing a second
domain that electrostatically attracts the AT reactive
site [19,21]. Heparin chains must have a minimum
molecular weight of approximately 5400 D for
thrombin binding [22,23]. Anti–factor IIa activity
increases with the size of the heparin molecule, while
anti– factor Xa activity remains stable [5]. The anti–
factor Xa and anti– factor IIa activity of UFH is
approximately equal. The effect of heparin on the
aPTT primarily reflects its anti– factor IIa, rather than
anti– factor Xa, activity. Oligosaccharide chain length
also is an important determinant of clearance; longer
chains—chains with greater anti–factor IIa activity
and influencing the aPTT—are cleared more rapidly
than shorter chains [24].
UFH and LMWH also have anticoagulant proper-
ties independent of AT. Both agents cause the release
of tissue factor pathway inhibitor from the vascular
endothelium, leading to inhibition of factor X acti-
vation and subsequent thrombin generation. These
drugs also enhance activated protein C inactivation of
factor V, but not factor Va, in an AT-independent
manner. Such an effect could downregulate thrombin
production by decreasing the amount of membrane-
bound factor V capable of conversion to factor Va
and blocking the factor V/Va site with inactive fac-
tor V [25]. UFH also causes the release of platelet
factor 4 from activated platelets. Finally, heparin has
several biologic effects unrelated to its anticoagulant
action, including osteoblast suppression/osteoclast
activation associated with osteopenia, inhibition of
vascular smooth muscle cell proliferation, and
increased vascular permeability. Heparin also binds,
stabilizes, and potentiates the activities of several
growth factors and cell adhesion glycoproteins [26].
In addition to its specific binding to AT, heparin
also binds nonspecifically to several plasma proteins,
endothelial cells, and macrophages [24]. Many
heparin-binding proteins, such as vitronectin and
fibronectin, are acute-phase reactants, contributing
to the variable anticoagulant effect of heparin [27].
Binding to platelet factor 4 and multimers of von
Willebrand factor may be particularly important
because this clears higher molecular weight chains
from the circulation, renders them ineffective as anti-
coagulants, and lowers the effective heparin concen-
tration at sites of vascular injury [28,29]. The platelet
factor 4/heparin complexes are also one of the
antigens responsible for heparin-induced thrombocy-
topenia (HIT). Nonspecific protein binding signifi-
cantly affects the clearance of heparin, resulting in
a bioavailability of only about 30% and causing
variability in dose response and heparin resistance
in some patients [22,30].
UFH is cleared from the plasma in two phases—
a rapid, saturable phase secondary to endothelial and
macrophage binding and slower, unsaturable renal
clearance. The clearance of therapeutic doses of
heparin is dose related. The half-life of heparin in-
creases from 30 minutes after an intravenous bolus
of 25 U/kg to 60 minutes after a dose of 100 U/kg.
At therapeutic doses, the half-life of plasma heparin
activity is 63 ± 19 minutes, whereas that of the
heparin-induced change in aPTT is 84 ± 71.5 minutes
[31]. It is now realized, however, that heparin also has
some postdrug effects, such as the release of tissue

meissner & karmy-jones248
factor pathway inhibitor, whic may not follow the
pharmacokinetics of the drug.
Dose and administration. Heparin may be admin-
istered by continuous intravenous, intermittent intra-
venous, or intermittent subcutaneous injection.
Continuous intravenous administration is most com-
monly used; trials evaluating the safety and efficacy
of intermittent subcutaneous injection often have
been contradictory [32]. Although heparin is a large,
highly anionic molecule that is poorly absorbed from
the gastrointestinal tract, carrier molecules that
increase passive intestinal absorption and enable oral
administration also have been developed [33,34].
Heparin is measured in terms of the US Pharma-
copoeia unit, defined as the amount of heparin
causing 1 mL of sheep blood to half-clot when kept
at 20�C for 1 hour. Because UFH is a heterogeneous
mixture of compounds with variable biologic activity,
however, absolute dosages are irrelevant to its toxic
and therapeutic effects. The anticoagulant response
varies among patients, and the use of UFH requires
laboratory monitoring, most often using the aPTT.
Differences in anticoagulant response are due to
individual differences in the clearance of heparin
and in the aPTT response to a given amount of hepa-
rin. For the treatment of venous thromboembolism
(VTE), a therapeutic aPTT range of 1.5 to 2.5 times
the control value was previously recommended.
Ratios near the lower end of this target range are
associated with subtherapeutic heparin levels, how-
ever [35]. The responsiveness of different aPTT
reagents to heparin varies, and there is no equivalent
to the international normalized ratio (INR) used to
adjust for variability in PT reagents. The use of a
fixed therapeutic range for the aPTT is no longer
acceptable, and current recommendations are that
heparin dose be adjusted to achieve an aPTT
equivalent to a heparin level of 0.2 to 0.4 U/mL
measured by protamine titration [35,36]. Although at
least some data suggest that the aPTT response is
poorly related to the therapeutic outcome in VTE and
MI [24], the aPTT should be checked 6 hours after an
intravenous bolus dose and approximately 3 hours
after a subcutaneous dose of UFH. Heparin can be a
difficult drug to titrate, and failure to achieve a
therapeutic aPTT is among the most common errors
associated with use of the drug. Although some
authors have suggested that failure to achieve a thera-
peutic aPTT within the first 24 hours is associated
with a substantially higher risk of recurrent VTE,
others have found no difference in 3-month recur-
rence rates among patients achieving (5.3–7%) or
not achieving (6.3–7.8%) a therapeutic aPTT within
24 hours if initial heparin doses exceed 30,000 U/24 h
[36,37]. Monitoring anti– factor Xa levels is an
alternative in patients with lupus anticoagulant or
factor XII deficiency, in whom the aPTT may be
unreliable [22].
For the treatment of VTE, most more recent
studies have used an initial heparin bolus dose of
5000 U followed by a starting infusion rate of
30,000 to 35,000 U/24 h [36]. Weight-based nomo-
grams have been shown to outperform other
approaches to UFH administration, however, increas-
ing the aPTT above the therapeutic threshold more
rapidly, better estimating eventual heparin require-
ments, and requiring fewer dosage adjustments [38].
Current consensus recommendations for VTE include
initial treatment with 80 U/kg of heparin intra-
venously followed by a maintenance infusion of
18 U/kg with subsequent dosage adjustment to
maintain an aPTT in the therapeutic range [24,28].
Nomograms for VTE have incorporated a higher
dose than for unstable angina because the bleeding
risk is higher among patients receiving thrombolytic
therapy or GP IIb/IIIa antagonists. Variability in labo-
ratory reagents requires, however, that the appro-
priate therapeutic range and dosage adjustments be
locally determined.
Because of their rapid onset of action, UFH and
LMWH are currently the anticoagulants of choice
when immediate anticoagulation is required. Estab-
lished indications for UFH include the prevention and
treatment of VTE; periprocedural use in cardiac
surgery, vascular surgery, and coronary angioplasty;
as an adjunct to coronary stents; and in the treatment
of disseminated intravascular coagulation. The only
randomized trial comparing initial anticoagulation
with heparin versus no anticoagulation in the treat-
ment of VTE was stopped after enrolling only
35 patients because of the high mortality and recur-
rence rate in the untreated group [39]. Among the
19 patients randomized to no treatment, 5 died, and
5 others had nonfatal recurrent pulmonary embolism,
compared with 1 death and no recurrences in the
16 treated patients. A 5-day course of intravenous
UFH, when followed by oral anticoagulation, has
been shown to be sufficient for the treatment of VTE.
The incidence of recurrent thromboembolism during
or within 1 week of heparin therapy is 1.4% [40].
UFH administered in a dose of 5000 U subcutane-
ously every 8 to 12 hours also has been shown to be
effective in the prevention of VTE in general surgery
patients and seriously ill medical patients [24]. UFH
usually is combined with antiplatelet agents (aspirin
or GPIIb/IIIa inhibitors) or thrombolytic agents in
the treatment of acute coronary syndromes.

management of the anticoagulated patient 249
Complications. Bleeding is the most common
complication associated with anticoagulant therapy.
The risk of major bleeding associated with UFH and
LMWH has been reported to be 0% to 7% and 0%
to 3% [41]. Others have noted major bleeding in 4%
to 6% of patients treated with UFH [32,40], with fatal
bleeding in 1% to 2% of patients with major bleeding
[42]. Although approximately half of patients with a
major bleeding event have a supratherapeutic aPTT
within 24 hours of hemorrhage [40], the aPTT is
poorly predictive of bleeding complications. In con-
trast, 24-hour heparin dose per m2 body surface
area is significantly related to bleeding. The aPTT
independent bleeding risk associated with heparin
may be due to its other effects, such as those on
platelet function. Most major bleeding episodes
during treatment for VTE have been noted to occur
near the end of initial heparin treatment when the INR
is approaching the therapeutic range [40]. A body
surface area 2 m2 or less (odds ratio 2.3, confidence
interval 1.2–4.4) and malignancy (odds ratio 2.4,
confidence interval 1.1–4.9) are independent risk
factors for bleeding while receiving parenteral anti-
coagulants [42].
Other risks associated with UFH include elevated
liver function tests, HIT, and osteopenia with long-
term administration. Increased plasma levels of liver
enzymes have been reported in 18% to 89% of
patients receiving heparin and are seen in association
with LMWH [43].
Based on etiology and the risk of complications,
HIT often is divided into types I and II [44]. Type I
HIT derives from the intrinsic proaggregatory ef-
fect of heparin and is generally asymptomatic,
characterized by a decrease in platelet count within
the first 3 days of therapy and rarely associated
with platelet counts less than 100,000/mL [44]. The
platelet count often returns to the normal range
despite continued heparin therapy. Type II HIT is
the most common drug-induced, immune-mediated
thrombocytopenia, occurring in 1% to 3% of patients
receiving heparin for more than 5 days [45,46].
Thrombocytopenia results from antibodies directed
against multimolecular complexes of platelet fac-
tor 4 and heparin chains longer than 12 to 14 sac-
charide units. The heparin/platelet factor 4/IgG
complex binds to platelet Fc receptors, causing
antibody-mediated platelet activation and inducing
platelet-derived procoagulant microparticles. The
antibody also may bind similar epitopes on endothe-
lial cells, potentially resulting in immune-mediated
endothelial injury [44,46]. Heparin antibodies have
been noted in 40% of patients undergoing cardiac
surgery [47].
Early manifestations of type II HIT include a
decrease in platelet count of greater than 50%,
often to less than 100,000/mL, and skin lesions at
injection sites. Thrombocytopenia is usually first
seen after 5 to 10 days of heparin therapy, but can
be seen within hours in previously exposed pa-
tients. Manifestations can occur after heparin is
administered in any dose by any route, but are ob-
served most frequently in patients receiving hepa-
rin as postoperative prophylaxis. In one series of
127 patients with HIT, 73.2% were receiving hepa-
rin for prophylactic indications [45]. Several labo-
ratory tests for HIT have been developed. Platelet-
associated IgG is almost always elevated but has low
specificity. The 14C-serotonin platelet release assay to
detect heparin-dependent IgG antibodies is sensitive
and specific (>90%) for HIT, but results are not
immediately available. Commonly accepted diagnos-
tic criteria for HIT include (1) a decline in platelet
count to less than 150,000/mL 5 or more days after
beginning heparin and (2) a positive platelet14C-
serotonin release assay.
In contrast to other immune-mediated thrombo-
cytopenias, type II HIT is associated with a high risk
of thrombosis. Arterial or venous thrombosis may
develop in 50% to 75% of patients, and the mortality
rate is 25% to 30% [24,48]. HIT is recognized before
the occurrence of a thrombotic event in only half
of patients [45]. Although some investigators have
reported arterial events to be more common, others
have reported a 4.3:1 ratio of venous to arterial events
[45]. Arterial thrombi usually consist primarily
of platelets, giving rise to the description ‘‘white
clot syndrome.’’
If platelet counts fall precipitously or reach levels
of less than 100,000/mL, heparin should be stopped
and alternative anticoagulants, such as lepirudin or
argatroban, used until the patient is therapeutic on
warfarin. For patients with asymptomatic HIT, the
30-day cumulative thrombosis rate is 52.8% [45].
Because thrombosis may occur even after withdrawal
of heparin, even asymptomatic patients should be
therapeutically anticoagulated with alternative agents
until the platelet count has normalized [24]. Other
authors have suggested that asymptomatic patients be
treated until the HIT antibody can no longer be
detected [48]. Because there is a high incidence of
cross-reactivity with heparin-dependent antibodies,
LMWH should not be used in patients with type II
HIT. Occasional reports of venous gangrene associ-
ated with decreased protein C levels suggest that
warfarin, without an alternative parenteral anticoagu-
lant, should not be used as initial monotherapy for
acute HIT [22,24,44].

meissner & karmy-jones250
Low-molecular-weight heparin
LMWH was specifically developed to provide an
agent that was more specific than heparin, separating
its anti– factor IIa and anti–factor Xa activity, with
the potential benefit of reducing the hemorrhagic side
effects [19]. LMWH is derived from the chemical or
enzymatic depolymerization of UFH to produce a
heterogeneous mixture of species with mean molecu-
lar weights of 4500 to 5000 D. The methods of
depolymerization and species produced differ sub-
stantially between LMWH preparations. By defini-
tion, LMWH has a mean molecular weight of less
than 8000 D with at least 60% of all molecules
having a molecular weight of less than 8000 D. In
contrast, 30% of the components of UFH are low-
molecular-weight chains.
The biologic difference between UFH and the
LMWH arises from their predominant inactivation of
factor Xa and reduced cellular and protein binding.
Because of their shorter chain length, most LMWH
species are unable to form the ternary complex
required for the inactivation of thrombin, although
they retain their ability to inactivate factor Xa.
Among the eight LMWH species approved for use
in the world (four in the United States), the anti–
factor Xa–to–anti– factor IIa ratio varies between
1.5 and 4 compared with 1 for UFH [19,24]. Because
the affinity of heparin for plasma proteins depends on
chain length, LMWH has substantially reduced pro-
tein binding. Because of reduced binding to cells and
plasma proteins, LMWH is primarily renally cleared
and has less interaction with macrophages, platelets,
and osteoblasts. Corresponding clinical advantages
of LMWH include 90% to 100% bioavailability, al-
lowing once-daily or twice-daily subcutaneous injec-
tion; a more predictable dose-response, which permits
weight-based dosing without the need for laboratory
monitoring; a longer half-life; and less risk of
osteopenia and HIT. Because of the high incidence
of cross-reactivity, however, LMWH should not be
substituted for UFH in patients with HIT. Although
early animal studies suggested LMWH may have a
wider therapeutic window and lower risk of bleeding,
this has not been confirmed clinically, and there are
no significant differences in bleeding rates between
UFH and LMWH [5,49].
Because the aPTT primarily reflects anti–factor
IIa activity, it is not useful for monitoring the anti-
coagulant activity of LMWH. Monitoring is unneces-
sary in most patients, however, and usually is
considered only in clinical situations in which the
dosage is poorly defined or difficult to predict. The
potency of LMWH is measured most often by chro-
mogenic assays for anti– factor Xa activity. For
twice-daily administration in the treatment of DVT,
anti– factor Xa levels of 0.6 to 1 IU/mL measured
4 hours after a subcutaneous dose seem to be
adequate. Monitoring of anti–factor Xa levels may
be appropriate in children and pregnant women,
obese patients (>110 kg), and patients with renal
failure. Possibly because plasma assays measure only
the ability to inactive free factor Xa rather than that
within the prothrombinase complex, the relationship
between anti– factor Xa activity and in vivo efficacy
or complications is poor. In the treatment of DVT,
the degree of thrombus regression after 10 days of
LMWH seems weakly related to anti– factor Xa
levels, however.
Depending on the preparation and indication,
LMWH can be administered subcutaneously once
or twice daily based on total body weight. Established
indications for LMWH include the prophylaxis and
treatment of VTE and the early treatment of unstable
angina. Compared with UFH, the use of LMWH in
the treatment of unstable angina or non–Q wave MI
is associated with a 15% to 20% relative risk re-
duction in MI or death during the first 7 to 14 days,
although this benefit is not sustained in the long-term
[24]. Other benefits of LMWH are either unclear
(in combination with thrombolysis in the treatment
of Q wave MI) or doubtful (prevention of restenosis
after coronary angioplasty).
Factor Xa inhibitors
Factor Xa may be a particularly suitable target for
directed anticoagulants because it is located at the
convergence of the intrinsic and extrinsic pathways
and is higher in the coagulation cascade than other
potential targets. Specific inhibitors of factor Xa
that are currently available or in clinical trials include
various pentasaccharide derivatives. In contrast to
heparin and LMWH, these drugs are homogeneous
synthetic agents with isolated pharmacologic targets,
selectively inhibiting factor Xa without a correspond-
ing effect on factor IIa. The pentasaccharide sequence
corresponds to the minimal binding sequence on the
heparin chain required for interaction with AT. These
agents indirectly inhibit the activity of factor Xa
through AT and, in contrast to heparin, do not prolong
the aPTT.
Fondaparinux (Arixtra) is a synthetic pentasac-
charide that reversibly binds the heparin-binding site
of AT, increasing its anti– factor Xa activity more
than 270-fold [50]. Because it interacts only with the
heparin-binding site, the drug is ineffective against
thrombin but has high anti– factor Xa activity. Free

management of the anticoagulated patient 251
factor Xa rather than factor Xa bound in the
prothrombinase complex seems to be the primary
target of the drug [29]. Because the agent inhibits
thrombin generation, but not thrombin itself, the
thrombin-mediated amplification loops are preserved,
and these agents do not compromise thrombin or
ADP-induced platelet aggregation. There is, however,
some experimental evidence that in the presence of
fondaparinux, AT also is able to inhibit factor VIIa
bound to tissue factor [51].
A terminal methyl group prevents nonspecific
binding to plasma proteins, giving fondaparinux
a predictable pharmacologic response [52,53]. No
changes in the pharmacokinetic properties of the drug
have been noted with concomitant administration
of aspirin, warfarin, and some nonsteroidal anti-
inflammatory drugs. In contrast to UFH, fondapa-
rinux is relatively insensitive to platelet-derived
heparin neutralizing proteins. Limited data suggest
that fondaparinux does not form complexes with
platelet factor 4 and does not cross-react with
antibodies from patients with type II HIT [54]. The
drug is 100% available after subcutaneous injection
with an elimination half-life of about 17 hours,
allowing once-daily subcutaneous administration in
a fixed dose without monitoring. Because the drug
is not metabolized and is primarily renally excreted,
precautions may be necessary in patients with re-
nal dysfunction.
Fondaparinux currently is approved for major
orthopedic prophylaxis. In a meta-analysis of
7344 patients undergoing hip replacement, major
knee surgery, or surgery for hip fracture, fondapa-
rinux, 2.5 mg once daily started postoperatively,
reduced the odds of VTE by 55.2% compared with
enoxaparin (6.8% versus 13.7%) [55]. Major bleed-
ing events were more common among patients
receiving fondaparinux (2.7% versus 1.7%), however.
Compared with placebo after an initial 7-day course
of fondaparinux in patients undergoing hip fracture
surgery, extended prophylaxis for 21 days reduced
the incidence of VTE at 4 weeks from 35% to 1.4%
[53]. In the treatment of acute DVT, early results of
phase II and III trials suggest that fondaparinux at a
dose of 7.5 mg once daily is comparable in safety and
efficacy to initial treatment with LMWH [50,53].
Early phase II studies also have shown fondaparinux
to be at least equal to UFH as an adjunct to coronary
thrombolysis and angioplasty [52,53].
The half-lives of pentasaccharide derivatives
depend on their binding affinity for AT, the concen-
tration of AT, and the elimination half-life of AT.
Pentasaccharide analogues differing in their binding
affinity to AT and half-life have been developed.
These include an O-methylated, O-sulfated pentasac-
charide with an affinity for AT 34-fold times higher
than that of fondaparinux [56]. The half-life of
this drug is prolonged to 61.9 hours in nonhuman
primates and 80 hours in humans. Idraparinux is
a long-acting anti– factor Xa pentasaccharide in
phase III clinical trials for the treatment of VTE.
The drug can be administered as a weekly subcuta-
neous dose. Phase III studies evaluating the efficacy
of idraparinux in VTE and atrial fibrillation are in
progress or planned [53].
Warfarin
Pharmacology and mechanism of action
The vitamin K antagonists are currently the
most widely used oral anticoagulants. Vitamin K–
dependent coagulation proteins include factors II,
VII, IX, and X and proteins C and S. All except
protein S are synthesized exclusively in the liver. In
all cases, the g-carboxyglutamate residues function
to accelerate thrombin formation by binding calcium
ions, causing the protein to undergo a conformational
change that exposes the platelet phospholipid-binding
domain. Vitamin K–dependent proteins also are in-
volved in other regulatory processes, including bone
metabolism and vascular wall homeostasis, and the
vitamin K antagonists interfere with physiologic pro-
cesses other than the processes related to coagulation.
The vitamin K antagonists are derived from
4-hydroxycoumarin and include warfarin, phenpro-
coumon, and acenocoumarol. All act through the
enzyme, KO reductase, which is responsible for gen-
eration of the active form of vitamin K, the hydro-
quinone KH2. A deficiency of KH2 causes production
of partially carboxylated and decarboxylated proteins
with decreased procoagulant activity. Warfarin is the
most widely used vitamin K antagonist and is the
11th most frequently prescribed drug in the United
States [57]. It is a racemic mixture of R and S enan-
tiomers that are differentially metabolized; S-warfarin
is approximately three times more potent. Warfarin
circulates bound to plasma proteins and has a half-life
of 36 to 42 hours.
The anticoagulant effect of warfarin is notoriously
variable and is influenced by factors affecting the
metabolism of warfarin; dietary and gastrointestinal
factors influencing the availability and absorption
of vitamin K1; and factors, such as acute illness,
that alter the synthesis and metabolism of vitamin K–
dependent procoagulants. A reduced response to
warfarin may occur in patients with a diet high in
green vegetables or receiving vitamin K supplements,

meissner & karmy-jones252
whereas the effect may be potentiated in patients
receiving intravenous antibiotics or with fat mal-
absorption. Given the diversity of drug interactions,
more frequent monitoring of the INR is warranted
when new medications are added or withdrawn.
Genetic factors also may play a role in the anti-
coagulant response to warfarin. Hereditary resistance
to warfarin has been reported, with affected patients
requiring 2.6 mg/kg/d of warfarin [58]. These patients
require high plasma levels of warfarin for adequate
anticoagulation, but have otherwise normal warfarin
pharmacokinetics. Conversely, genetic heterogeneity
for cytochrome P-450 CYP2C9, the enzyme respon-
sible for converting S-warfarin to its inactive
hydroxyl forms, is associated with decreased dose
requirements. Patients with a low warfarin dose
requirement (<1.5 mg/day) are six times more likely
to have a variant CYP2C9 allele associated with
impaired S-warfarin metabolism [59]. These individ-
uals have been noted to have more problems on in-
duction of warfarin therapy and a 3.7-fold higher rate
of major bleeding complications.
The anticoagulant effect of warfarin most com-
monly is measured using the PT, which is sensitive to
reductions in three of the four vitamin K–dependent
procoagulants (factors II, VII, and X). Thromboplas-
tin reagents used in the PT assay vary in their
responsiveness to the anticoagulant effects of war-
farin, which in the past led to clinically important
differences in recommended oral anticoagulant doses;
this has largely been rectified by standardizing
thromboplastins according to their international sen-
sitivity index (ISI), which measures the responsive-
ness of a given thromboplastin to a reduction in
vitamin K–dependent factors in comparison to a
reference standard. The effect of warfarin-induced
anticoagulation is now standardized by converting the
PT measured with local thromboplastin reagents to an
INR, calculated as [24]:
INR ¼ patient PT=mean normal PTð ÞISI
Some evidence suggests that the anticoagulant effects
of warfarin, as measured by the PT, are disassociated
from the antithrombotic effects during the induction
of treatment. This observation arises from the fact
that prolongation of the PT early after initiating
warfarin primarily reflects reductions in factor VII,
which has the shortest half-life. The antithrombotic
effect is more closely related to the level of
prothrombin, however, which has a half-life of
96 hours compared with 6 to 24 hours for factors
VII and IX. The delayed reduction in prothrombin
levels is the basis for overlapping heparin and
warfarin treatment.
Dose and administration
Randomized clinical trials have established the
effectiveness of warfarin for the primary and sec-
ondary prevention of VTE; for the prevention of
embolism in patients with prosthetic heart valves
or atrial fibrillation; for the prevention of stroke,
recurrent MI, and death in patients with anterior MI;
for the prevention of anterior MI in patients with
peripheral vascular disease; and for the prevention of
MI in high-risk men [24]. Other commonly recog-
nized indications include rheumatic mitral valve
disease, mitral valve prolapse, mitral annular calcifi-
cation, nonrheumatic mitral regurgitation, mobile
aortic atheromas or plaques greater than 4 mm in
size, and systemic thromboembolism of unknown
etiology. One large randomized trial has shown oral
anticoagulants to be more effective than aspirin in
preventing thrombosis of infrainguinal vein, but not
prosthetic, grafts [60].
Although there is limited evidence that an INR of
1.3 to 2.0 may reduce myocardial ischemic events
when used as primary prevention in men without
ischemic heart disease, the therapeutic effect of war-
farin is significantly reduced at INR values less than
2 [24]. A moderate intensity of anticoagulation (INR
2.0–3.0) is appropriate for most indications. Excep-
tions requiring more intense anticoagulation include
some types of mechanical prosthetic heart valves and
some patients with antiphospholipid antibody syn-
drome. Limited evidence suggests an improved out-
come in patients with antiphospholipid antibodies
who are anticoagulated to an INR of 2.5 to 3.5.
The appropriate initial warfarin dose is contro-
versial, although initiating warfarin at a dose of 5 mg,
rather than with a loading dose of 10 mg, is often
recommended. As noted earlier, the antithrombotic
effect of warfarin is most closely related to pro-
thrombin levels, which are equivalently reduced by
a 5- or 10-mg dose [24]. A therapeutic INR usually
can be achieved within 4 to 5 days after initiating
warfarin at 5 mg/d. Adverse effects of loading doses
of warfarin include a more rapid reduction in
protein C and a higher risk of overanticoagulation.
Higher initial doses should be avoided in patients at
risk of bleeding or with a known deficiency of
protein C or S, in whom the risk of skin necrosis is
higher [61]. Although parenteral anticoagulants can
be avoided when instituting anticoagulation for
chronic atrial fibrillation, heparin should be adminis-
tered simultaneously for 4 to 5 days, until the INR is
in the therapeutic range on two measurements at least

management of the anticoagulated patient 253
24 hours apart, if urgent anticoagulation is required
for the treatment of thromboembolic disease. Simul-
taneous initiation of heparin and warfarin is safe
and not associated with more frequent recurrence or
hemorrhage [61]. Several studies have shown that
the use of adjuvants such as computer-driven pro-
tocols and nomograms can improve the initiation
and maintenance of anticoagulation with vitamin K
antagonists [61].
Complications
Although effective in preventing thrombosis,
warfarin has a narrow therapeutic window. Several
factors, including widespread adoption of the INR,
decreased intensity of anticoagulation, and the orga-
nization of anticoagulation clinics, have increased the
safety of long-term oral anticoagulation; however,
bleeding remains the most important associated
complication and is closely related to the intensity
of anticoagulation. Clinical trials have established
that the bleeding risk increases as the INR is in-
creased from 2.0 to 3.0 to 3.0 to 4.5 and rises expo-
nentially as the INR increases to greater than 5.0 [24].
Total time in the therapeutic range also is an
important determinant of bleeding risk and anti-
coagulant efficacy. Risk factors for bleeding include
a history of hemorrhage, previous stroke, and
comorbid conditions such as renal insufficiency or
hypertension. The independent risk of bleeding
associated with age is controversial, but at least some
data suggest that elderly patients can be anticoagu-
lated safely if closely monitored in the setting of
an anticoagulation clinic. The overall rate of major
bleeding during a 3-month course of warfarin to
maintain an INR of 2.0 to 3.0 is 3% or less [41].
Various clinical trials have reported major bleeding
rates between 0.5 and 4.2 per 100 patients; cohort
studies have reported higher rates of 1.2 to 7 episodes
per 100 patients [61]. The risk of bleeding is
increased when high-intensity warfarin (INR 3.0–
4.5) is used in combination with aspirin [24].
Increased rates of minor bleeding also have been
reported with lower intensity regimens, however.
Nonhemorrhagic adverse effects of warfarin
include an associated embryopathy and warfarin-
induced skin necrosis. Oral anticoagulants cross
the placenta and are associated with a characteristic
embryopathy, CNS deficits, and increased rates of
fetal death. The coumarin derivatives interfere with
calcium deposition, causing irregular deposition in
areas that are not normally calcified, and approxi-
mately 30% of infants born to mothers taking these
drugs have serious bone defects. Although the
incidence of embryopathy is highest during the first
6 to 12 weeks of gestation, fetal bleeding and
death may occur throughout pregnancy. Although
warfarin is contraindicated during pregnancy, it can
be administered safely to nursing mothers [24].
Warfarin-induced skin necrosis is a rare complication
associated with large loading doses of warfarin and
presumably occurs when the introduction of warfarin
causes a more rapid reduction in protein C levels than
in the other vitamin K–dependent procoagulants. The
incidence is estimated to be between 1:100 and
1:10,000, and it is more common in women with a
predilection for the breast, thighs, and buttocks [62].
Patients with deficiencies of the protein C pathway
may be particularly susceptible to skin necrosis,
although this complication also may occur in non-
deficient individuals. Introducing warfarin gradually
while the patient is receiving therapeutic doses of
parenteral anticoagulants can minimize the potential
for this complication.
Direct thrombin inhibitors
Thrombin has multiple roles in coagulation,
including conversion of fibrinogen to fibrin, ampli-
fication of the coagulation cascade, and activation of
platelets. Given its central role in coagulation and
cardiovascular disease, the treatment of many throm-
botic disorders is directed toward blocking the action
of thrombin. Heparin historically has been used as a
primary treatment of such disorders, although it has
several limitations, including extensive protein bind-
ing and an inability to inactivate platelet-bound factor
Xa and fibrin-bound thrombin.
This last consideration may be particularly impor-
tant. The thrombin molecule contains three binding
sites, including the catalytic site responsible for
the cleavage of substrates (active site), a substrate
recognition site that also functions as the binding site
for the AT component of the heparin-AT complex
(exosite 1), and a heparin binding domain (exosite 2)
[27,30]. Heparin bound to exosite 2 bridges more
fibrin onto thrombin and renders the heparin/fibrin/
thrombin complex inaccessible to inhibition by AT
[27]. Such fibrin-bound thrombin serves as a reser-
voir of thrombogenic activity capable of converting
factors V and VIII to their active form, generating
fibrin from fibrinogen, activating factor XIII, and
attenuating fibrinolysis [23]. Bound thrombin also
continues to activate platelets through thromboxane
A2–independent mechanisms that are not inhibited
by aspirin [63]. Platelet-bound factor Xa is similarly
resistant to inactivation by the heparin/AT complex,

meissner & karmy-jones254
serving as a source of further thrombin generation
[23]. Drugs such as heparin incompletely attenuate
the thrombotic process, a potentially important con-
cern at sites of arterial injury.
The direct thrombin inhibitors offer several poten-
tial advantages over heparin. These agents act inde-
pendently of AT, either blocking the active site or
preventing interaction with its substrates. Several
direct thrombin inhibitors have been developed and
can be classified as being natural substrate analogues,
recombinant derivatives, or synthetic inhibitors; as
being directed against the active site or exosites; and
as being reversible or irreversible inhibitors. Three
parenteral direct thrombin inhibitors—lepirudin,
bivalirudin, and argatroban—are currently available,
and oral direct thrombin inhibitors, such as ximela-
gatran, are on the immediate horizon. Lepirudin and
argatroban are approved for the treatment of HIT,
and bivalirudin is approved as an adjunct to coronary
angioplasty. These agents typically can be monitored
with the aPTT.
Fibrin binding does not compromise agents
directed against the active site. Although inhibitors
that also bind exosite 1 compete with fibrin, the
fibrin-thrombin interaction is of low affinity in the
absence of heparin. The lower molecular weight
thrombin inhibitors are more effective against fibrin-
bound thrombin, presumably because of better
diffusion into the thrombus. In addition to inhibiting
the action of thrombin on fibrinogen, the direct
thrombin inhibitors block amplification of coagula-
tion through activation of factors V and VIII and
fibrin stabilization by factor XIII [48]. These agents
do not bind plasma proteins and result in a more
predictable dose-response than heparin. Additionally,
in contrast to heparin, these drugs are not neutralized
by platelet factor 4 and multimers of von Willebrand
factor, large quantities of which may be present at
sites of arterial plaque rupture. Finally, the direct
thrombin inhibitors do not promote the platelet
release reactions and inactivate thrombin-induced
platelet activation [64]. The combined ability to in-
hibit fibrin-bound thrombin without inducing platelet
aggregation may be particularly important in the
management of acute coronary syndromes. In a meta-
analysis including 35,970 patients, the use of direct
thrombin inhibitors in the setting of acute coronary
syndromes was associated with 15% reduction in
death or MI compared with heparin [63]. It was
estimated that 125 patients would need to be treated
with a direct thrombin inhibitor to avoid one event.
Although not currently supported by any data, simi-
lar concerns may exist in a patient with peripheral
vascular disease.
Despite similar advantages, there are potentially
important differences in the anticoagulant profiles
of the direct thrombin inhibitors, and they should
not be regarded as pharmacologically equivalent.
These agents vary in their specificity, and at least
some are capable of inhibiting other serine prote-
ases. Additionally, the theoretical observation that
some of these drugs, particularly the tripeptide deri-
vatives, may interfere with fibrinolysis is of un-
known significance.
Hirudin derivatives
Hirudin, a 65–amino acid polypeptide derived
from salivary extracts of the medicinal leech (Hirudo
medicinalis), is the prototype direct thrombin inhibi-
tor. Various recombinant derivatives of hirudin have
been developed. Lepirudin is a recombinant deriva-
tive of hirudin lacking a sulfated tyrosine at residue
63 and is known as a desulfatohirudin or deshirudin.
A long-acting polyethylene glycol–complexed hi-
rudin derivative (PEG-hirudin) also has been devel-
oped and evaluated in phase II trials [63]. Native
and recombinant hirudins form an essentially irre-
versible 1:1 complex with the active site and exo-
site, although the deshirudins have a 10-fold lower
affinity for thrombin [23,27]. Although most direct
thrombin inhibitors have a predictable anticoagulant
response, hirudin’s narrow therapeutic window man-
dates monitoring.
Lepirudin has a half-life of 1.3 hours, is renally
excreted, and can be monitored using the aPTT.
An initial bolus infusion of 0.4 mg/kg followed by a
continuous infusion of 0.15 mg/kg/h with subsequent
adjustments to maintain the aPTT between 1.5 and
2.5 times baseline has been recommended [22].
Because it is renally cleared, strict dosage adjustment
in renal failure is required. Lepirudin is approved for
the treatment of HIT. Clinical trials also have shown
hirudin to be at least as safe and effective as heparin
in the management of unstable angina, as an adjunct
to thrombolytic therapy, and in the prophylaxis and
treatment of VTE [27]. Concern remains, however,
that hirudin’s narrow therapeutic window may limit
its application in acute coronary syndromes, where
high doses are often required, and bleeding rates may
be higher [23,63,65].
Hirulogs
The hirulogs inhibit thrombin by binding to the
catalytic site and the anion binding exosite. Bivali-
rudin (Angiomax), currently approved for the man-
agement of acute coronary syndromes, is a 20–amino

management of the anticoagulated patient 255
acid synthetic analogue of hirudin. In contrast to
hirudin, inhibition by bivalirudin is reversed by
cleavage of the amino terminus by thrombin, freeing
the active site and leaving only the low-affinity inter-
action between the carboxyterminus and exosite 1.
Because it is a reversible inhibitor, bivalirudin may
have a wider therapeutic window than hirudin.
Bivalirudin has a half-life of 25 minutes and is elimi-
nated by renal clearance and proteolytic cleavage.
Clearance is reduced in patients with renal insuffi-
ciency. Although bivalirudin causes dose-dependent
increases in the activated clotting time, aPTT, INR,
and thrombin time, point-of-care monitoring with the
activated clotting time is the most often used. For
percutaneous coronary intervention, dose adjustment
to maintain an activated clotting time of 350 seconds
or greater has been recommended [30].
Small molecule direct thrombin inhibitors
Small molecule direct thrombin inhibitors also
have been developed. These include many tripeptide
derivatives or peptidomimetic compounds, such as
argatroban, melagatran, efegatran, inogatran, and
napsagatran. Most small molecule direct thrombin
inhibitors are characterized by a strongly basic group
interacting with the active site of thrombin, have low
oral bioavailability, have short plasma half-lives and
are hepatically metabolized. All produce predictable
anticoagulation measurable by common coagulation
assays with minimal drug interactions. Plasma levels
and anticoagulant response tend to be linearly related
to dose with little intraindividual variation. Because
of interactions, however, the PT/INR cannot be used
to monitor the introduction of oral vitamin K
antagonists while receiving parenteral direct thrombin
inhibitors. Similar to UFH, a coagulation rebound
phenomenon has been observed with parenteral direct
thrombin inhibitors. Compared with other direct
thrombin inhibitors used in the treatment of acute
coronary syndromes, the univalent inhibitors are
associated with a borderline increased risk of MI
and lower rates of major bleeding [63].
Of the parenteral small molecule direct thrombin
inhibitors, argatroban (Acova) is the only agent that
is currently approved by the US Food and Drug
Administration. Argatroban is an arginine derivative
that functions as a reversible, competitive inhibitor at
the catalytic site of thrombin. In contrast to heparin,
argatroban does not cause release of tissue factor
pathway inhibitor, a factor that may contribute to its
predictability and relatively low incidence of bleed-
ing. It has a half-life of 30 to 45 minutes and is
hepatically metabolized by hydroxylation and aroma-
tization of the 3-methyltetrahydroquinolone ring with
subsequent biliary excretion [22,27,66]. Hepatic
insufficiency is associated with a fourfold decrease
in the total clearance of argatroban and a twofold to
threefold increase in half-life [66,67]. In contrast to
the other available direct thrombin inhibitors, the
clearance and half-life of argatroban are independent
of renal function. The anticoagulant effect of arga-
troban is predictable with a low coefficient of
variability between healthy subjects. The response
is dose dependent, however, and requires monitoring
with either the aPTT or activated clotting time.
Ximelagatran (H 376/95) is the orally available
prodrug of melagatran, a dipeptide direct thrombin
inhibitor. The prodrug is 170 times more lipophilic
than melagatran, allowing oral administration and
absorption [68]. In contrast to other small molecule
inhibitors, ximelagatran has an oral bioavailability of
18% to 24% with minimal protein binding and low
variability in plasma levels [67,68]. Ximelagatran is
biotransformed to melagatran after oral administra-
tion and competitively and reversibly binds to the
active site of thrombin. Active melagatran is cleared
by the kidneys with a half-life of 3 hours. It can
be administered twice daily and has a predictable
pharmacokinetic effect that is not influenced by age,
gender, or weight, requiring no monitoring. The drug
has no relevant interactions with food or drugs
metabolized by cytochrome P-450.
Several clinical trials evaluating the safety and
efficacy of ximelagatran in VTE and atrial fibrillation
are currently under way or have been reported. Com-
pared with dalteparin (5000 IU once daily), the com-
bination of subcutaneous melagatran (3 mg twice
daily) started preoperatively and oral ximelagatran
(24 mg twice daily) postoperatively reduced the fre-
quency of VTE in orthopedic patients from 28.2% to
15.1%, although the frequency of excessive bleeding
was higher (5% versus 2.4%) [69]. Ximelagatran in a
dose of 24 mg twice daily also has shown efficacy
comparable to that of enoxaparin in preventing
VTE after total knee replacement [70]. In contrast,
ximelagatran at a dose of 36 mg twice daily was
significantly more effective than warfarin in reducing
the incidence of VTE and death (20.3% versus
27.6%) in patients undergoing total knee replacement
[71]. No increased bleeding was observed in patients
receiving 36 mg of ximelagatran twice daily.
Ximelagatran also has shown promise in the
extended treatment of a first episode of VTE. After
completion of a 6-month course of anticoagulation,
ximelagatran (24 mg twice daily) reduced the inci-
dence of recurrent thromboembolism from 12.6% to
2.8% at 18 months [61]. There was no increased

meissner & karmy-jones256
bleeding among patients receiving ximelagatran,
although increased transaminase levels were more
frequent (6.4% versus 1.2%) than in patients receiv-
ing placebo. Ximelagatran also has shown promise in
the prevention of stroke in patients with nonvalvular
atrial fibrillation, and clinical trials evaluating the
utility of this approach are in progress [72]. Com-
pared with aspirin alone in patients with acute
coronary syndromes, ximelagatran and aspirin for
6 months significantly reduced the incidence of
death, nonfatal MI, and severe recurrent ischemia
from 16.3% to 12.7% [73]. Such extended treatment
may provide effective secondary prophylaxis and
protect against rebound events after UFH or LMWH
is discontinued. The incidence of major bleeding did
not differ between groups, although elevated trans-
aminase levels were more common among patients
receiving ximelagatran. Transaminase elevation seems
to be dose related, to occur within 2 to 6 months of
treatment, and to be asymptomatic. Other phase II
trials have noted a 4.3% incidence of self-limited
transaminase elevation [72]. Given the limitations of
warfarin, it is anticipated that these drugs will replace
vitamin K antagonists in the long-term treatment of
atrial fibrillation and VTE.
Reversing the action of anticoagulants
Heparin and low-molecular-weight heparin
The anticoagulant effect of UFH can be reversed
by the administration of protamine, a cationic heparin
binding protein. Protamine is administered in a
neutralizing dose of 1 mg per 100 U of UFH. The
60-minute half-life of heparin must be considered in
calculating the protamine dose. Risks of protamine
administration include bradycardia and hypotension,
which can be reduced by slow administration, and
allergic reactions associated with previous exposure,
including protamine-containing insulin, vasectomy,
and fish allergies. Although protamine is effective in
reversing heparin’s anti – factor IIa activity and
reducing the aPTT, it binds less well to shorter
heparin chains and only partially neutralizes anti–
factor Xa activity. Protamine sulfate can be used in
patients with clinical bleeding while receiving
LMWH, but is less effective than with UFH. Standard
doses of protamine have been shown to reverse
acutely only 42% of the factor Xa activity and 92%
of the anti– factor IIa activity after a subcutaneous
dose of tinzaparin [74]. As a result of the subcuta-
neous depot, however, there is a gradual return of
anti– factor IIa and anti– factor Xa activities.
Warfarin
There are three approaches to correcting a supra-
therapeutic INR: discontinuation of warfarin, admin-
istration of vitamin K1, and infusion of fresh frozen
plasma (FFP) or prothrombin concentrate. All of
these approaches have disadvantages, including
slow reversal and transient warfarin resistance for
vitamin K and the risk of viral transmission for the
plasma-derived products. The appropriate approach
to an individual patient depends on the INR, the
presence of bleeding, and the need for invasive
procedures. The risk of bleeding is significantly
increased at an INR greater than 4.0 to 5.0, and in
a nonbleeding patient, the INR optimally should be
corrected below this range but not into the subthera-
peutic range. Oral vitamin K significantly reduces
the INR within 24 hours. Low-dose (0.5–2.5 mg)
intravenous vitamin K also is effective, although
higher doses (� 10 mg) are associated with temporary
warfarin resistance on reintroducing oral anticoagu-
lants [75]. Although occasionally associated with
anaphylaxis, intravenous administration of small
doses (0.5 mg) of vitamin K1 to excessively anti-
coagulated patients reduces the INR to less than
5.5 within 24 hours without causing excessive delay
when reinstituting anticoagulation [76].
Current recommendations include lowering or
omitting a dose in patients with an INR less than
5.0 and no bleeding. For nonbleeding patients with
an INR greater than 5.0 but less than 9.0, with-
holding one or two doses with or without adminis-
tering 1 to 2.5 mg of oral vitamin K is acceptable.
For patients with an INR greater than 9.0, 3 to 5 mg
of oral vitamin K1 reduces the INR within 24 to
48 hours. For patients with serious bleeding, FFP or
prothrombin concentrate should be administered in
conjunction with 10 mg of vitamin K1 by slow
intravenous infusion.
Management of a patient undergoing surgery or
other invasive procedure requires special attention.
The anticoagulant effects of warfarin require sev-
eral days to recede after the drug is stopped and
several days to become therapeutic after restarting
the drug. Most patients require about 4 days to
reach an INR less than 1.5 after warfarin is stopped.
For patients at low risk for bleeding, reducing
the INR to 1.3 to 1.5 before invasive procedures is
acceptable. Postoperative intravenous heparin ther-
apy has been estimated to cause major bleeding in
3% of patients; approximately 3% of these epi-
sodes are fatal or disabling [77]. It is currently
recommended that the management of antico-
agulated patients undergoing invasive procedures

management of the anticoagulated patient 257
be guided by the underlying risks of thrombosis
and bleeding.
For VTE, preoperative therapeutic UFH or LMWH
is warranted when the INR is less than 2.0 in patients
with an event within 1 month of surgery, whereas
postoperative therapeutic anticoagulation is appro-
priate for patients with an event within the preceding
3 months. For arterial thromboembolism, preopera-
tive therapeutic anticoagulation with UFH or LMWH
is recommended only for patients undergoing surgery
within 1 month of an event. Postoperative heparin
anticoagulation should be considered in such patients
only if the risk of bleeding is low. Bridging therapy
has not been recommended for patients with me-
chanical heart valves or nonvalvular atrial fibrillation
without a history of arterial embolism. For patients
with a low risk of thrombosis, such as patients with a
remote (>3 months) history of DVT or atrial fibril-
lation without stroke, warfarin can be discontinued
preoperatively, the procedure performed with ap-
propriate postoperative prophylaxis when the INR
has returned to normal, and warfarin restarted.
For intermediate-risk patients, warfarin should be
discontinued approximately 4 days preoperatively,
the procedure performed when the INR normalizes,
and the patient covered perioperatively beginning
2 days before surgery with low-dose UFH or LMWH.
For patients with a high risk of thrombosis, such
as patients with recent DVT, prosthetic mitral valves,
or older mechanical valves, warfarin should be
discontinued approximately 4 days preoperatively
and the patient bridged with full-dose UFH or
LMWH as the INR falls below the therapeutic range
approximately 2 days preoperatively. The risk of
thromboembolism exceeds that of bleeding in pa-
tients undergoing dental procedures, and warfarin
need not be discontinued in patients at low risk
for bleeding.
Table 2
Typical laboratory patterns of coagulopathy
Platelets Bleeding time aP
Warfarin N N N
Heparin N N "Thrombocytopenia # N–" N
vWD N " N
Liver failure N Variable "Hemophilia N N "Fibrinolysis N N "Abbreviations: aPTT, activated partial thromboplastin time; FDP, fib
N, normal; TT, thrombin time; vWD, von Willebrand disease.
Newer anticoagulants
No effective reversal agents exist for many of
the newer anticoagulants. There is no specific
antidote for the pentasaccharide derivative factor Xa
inhibitors, although limited data suggest that recom-
binant factor VIIa normalizes the thrombin generation
time in healthy volunteers [53]. Protamine does not
reverse the effects of the direct thrombin inhibitors.
Potential thrombin inhibitor antagonists, including
desmopressin, factor VIIa, factor VIII, and activated
prothrombin complex (Feiba), have been suggested
[48]. Most of the direct thrombin inhibitors have a
half-life of only 30 to 45 minutes in normal indi-
viduals. Although lepirudin should not be used in
patients with renal insufficiency, accidental over-
dosage in these patients can be managed with dialysis
using a polymethylmethylacrylate membrane [27].
Bivalirudin is also approximately 25% cleared by
hemodialysis [30].
Assessment of bleeding potential
One single test rarely can truly assess the risk
of bleeding or define the etiology of a coagulopathy.
A comprehensive approach, combining clinical sce-
nario and laboratory tests, is required and can be com-
plex and confusing (Table 2). Owings and Gosselin
[78] provided a comprehensive review of this topic.
The approach varies depending on whether in the
preoperative or postoperative phase and whether or
not there is active bleeding.
Clinical assessment
The primary assessment should begin with
the history and physical examination. Simple ques-
TT INR TT Fibrinogen FDP
–" " N N 0
N–" " N 0
N N N 0
N N N 0
" N–" " 0
N N N 0
" " N–# "rin degradation product; INR, international normalized ratio;

meissner & karmy-jones258
tions about bleeding history, such as easy bruising,
frequent nosebleeds, family history of bleeding
disorders, and medications, may direct a specific
evaluation. Physical assessment includes observing
bruising, telangiectasias, conjunctival hemorrhages,
or purpura. Attention to temperature is important,
particularly in the ICU or trauma setting. Patients
with body temperatures 35�C or lower should be
actively rewarmed. In some settings, such as major
trauma, operative intervention may have to be
stopped to allow time for resuscitation and rewarm-
ing, correcting diffuse bleeding. Hypothermic co-
agulopathy may not be associated with abnormal
aPTT or INR because these tests usually are per-
formed at 37�C, correcting the inhibition of coagu-
lation. Hemodilution can occur if greater than 10 U
of packed red blood cells are given in a short time
without plasma replacement.
Laboratory assessment
Normal activated partial thromboplastin time and
normal international normalized ratio
Patients who exhibit persistent bleeding despite
having normal aPTT and INR often have disordered
platelet activity, owing to either low numbers or
function. A platelet disorder may be suspected by a
prolonged bleeding time, reduced platelet count, or
tests of platelet function. Patients who are to undergo
major surgery require at least a platelet count greater
than 20,000/mm3 [78]. In general, the authors prefer
to maintain counts greater than 50,000/mm3 before
lung resection thoracotomy for at least 48 hours or
until chest drains are discontinued. This preference is
not based on any solid evidence, however, and varies
significantly from case to base, depending on the
sense of the risk of bleeding. Decreased platelet count
can be secondary to immune disorders (eg, HIT,
thrombocytopenia purpuras, antibiotic reactions) or
acquired conditions (eg, disseminated intravascular
coagulopathy [DIC], dilutional coagulopathy, myelo-
dysplastic syndromes). Clinically significant bleeding
can occur when platelet counts decrease to less than
10,000/mm3, and patients in whom even minor
bleeding would be catastrophic (eg, following neuro-
surgical procedures) should have platelet counts
maintained at greater than 20,000/mm3. Other tests
of platelet number or function are available. The
bleeding time is considered inaccurate because nor-
mal results are seen in half of patients with congenital
thrombocytopenia [79]. Other rapid tests, such as the
Sonoclot or Thromboelastogram, are available and
can be useful in studying platelet function and
number separately.
Platelet dysfunction may be anticipated by a his-
tory of medication. Aspirin, as noted earlier, causes
an irreversible dysfunction that lasts the lifetime of
the platelet, or approximately 10 days. Patients who
are to undergo elective surgery should stop aspirin at
least 7 days before surgery; patients requiring urgent
operation, depending on the complexity of the
procedure, can be treated by platelet transfusion.
Acquired disorders include renal failure, which can
be managed by desmopressin. Hereditary conditions,
of which von Willebrand disease is the most
common, also should be considered. von Willebrand
disease has three forms: type I (reduced concen-
tration), type II (dysfunctional), and type III (absent).
Desmopressin also can be used, although in some
forms (type IIb) it is contraindicated. Cryoprecipitate
can be helpful. Deficits in von Willebrand factor
function also are seen in patients with renal failure.
Preoperatively, in elective surgery patients, manage-
ment can include dialysis (to reduce the level of
uremia) and an infusion of 0.3 to 0.4 mg/kg of
desmopressin 1 hour before surgery. Desmopressin
has a half-life of 55 minutes and can be repeated
every 12 hours, although after two doses resistance
can be seen in some cases [80]. Probably the most
common scenario in which platelet dysfunction is
encountered in thoracic surgery is after cardiopulmo-
nary bypass. Minimizing pump suction, the return of
salvaged blood using heparin-bonded circuits seems
to be beneficial in reducing the risk of bleeding,
thrombotic complications, and inflammatory cascade–
mediated complications.
Prolonged activated partial thromboplastin time and
normal international normalized ratio
The most common cause of a prolonged aPTT is
heparin administration. Management, as discussed
earlier, can include simply withholding heparin or
administering (carefully) protamine sulfate. FFP does
not correct the effect of heparin, and because heparin
acts by potentiating AT, which is present in FFP, this
may accentuate the anticoagulation activity of hepa-
rin. In some thrombotic states, FFP is administered
with heparin specifically for this purpose. FFP, by
binding the agent, reverses the effect of direct
thrombin inhibitors. Hereditory deficiencies of factors
VIII, IX, and XI (hemophilia A, B, and C) usually
do not manifest with abnormal coagulation parame-
ters until factor activity levels decrease to less than
40%. Management includes transfusion of FFP, cryo-
precipitate, or specific factor replenishment. FFP
contains 1 U/mL of factor VIII; cryoprecipitate, 5 to
10 U/mL; and factor VIII concentrate, 25 U/mL. The
half-life is 8 to 12 hours. One recommended approach

management of the anticoagulated patient 259
has been to transfuse to levels as close to 100% as
possible immediately before operation, then maintain
levels greater than 40% until sutures and drains are
removed [81]. Recombinant factor VII (rVIIa) also
has been used for factor VIII and factor IX deficiency.
von Willebrand disease also may be associated
with prolonged aPTT and can be confirmed by
studies of platelet function or measurement of cir-
culating levels. Management has been discussed in
the previous section.
Increased international normalized ratio and normal
activated partial thromboplastin time
The two most common etiologies of increased
INR and normal aPTT are liver failure and warfarin
administration. Correction of the latter has been
discussed. In the former, FFP administration is the
mainstay of treatment, unless the disease is so far
advanced that a DIC state exists, in which case
cryoprecipitate is often required, as is desmopressin
and platelet transfusion.
Increased international normalized ratio and
increased activated partial thromboplastin time
The causes of increased INR and increased
aPTT are often multifactorial. It is important, par-
ticularly in patients without bleeding or who have no
reason to have a bleeding tendency, to ensure that the
laboratory tests were done correctly (eg, inadequate
volume of blood). Hemodilution and nephrotic syn-
drome result in a loss of coagulation factors. DIC
represents a consumption of factors, and D-dimer
levels greater than 2000 ng/mL support the diagnosis.
DIC can be mild, moderate, or severe (Table 3). At
the most advanced stage, DIC bleeding is a result
of consumption of factors and excessive fibrinolysis.
Initial management includes addressing the under-
Table 3
Phases of disseminated intravascular coagulation
Phase 1 No obvious clinical manifestations
Routine laboratory screening normal
Directed tests (eg, prothrombin fragments)
may reveal thrombin generation
Phase 2 Bleeding from wounds, IV sites
aPTT, INR", fibrinogen#, FDP +
Phase 3 Multiple organ dysfunction syndrome
Diffuse bleeding
aPTT, INR"", fibrinogen, FDP##Abbreviations: aPTT, activated partial thromboplastin time;
FDP, fibrin degradation product; INR, international normal-
ized ratio.
lying cause and correcting hypothermia. Subsequent
treatment is administration of FFP, cryoprecipitate,
calcium, and platelets, until bleeding stops, and
aPTT and INR normalize [78]. If fibrinogen is less
than 100 mg/dL, cryoprecipitate is probably the
more effective vehicle for replenishment. Alternative
approaches have attempted to use heparin to inhibit
clotting, allowing restoration of clotting factors, or
antifribrinolytics, such as aminocaproic acid. In
trauma patients, with uncontrollable nonsurgical
bleeding, with or without hypothermia, rVIIa has
been studied with some success [82].
Hypercoagulable states and venous
thromboembolism
The bulk of this article has addressed issues
relating primarily to hypocoagulable states. Hyper-
coagulability states are important to recognize, if only
because of the risk of VTE and graft occlusion. In
addition, the inflammatory response to surgery may
increase the risk of thrombosis. Acquired conditions
that predispose to VTE in particular are trauma,
cancer, and immobility. Other acquired conditions
include diverse syndromes, such as the previously
discussed HIT and lupus anticoagulant. Congenital
deficiencies in coagulation include AT III, plas-
minogen, proteins C and S, and overall such defects
may be present in 20% of cases of recurrent VTE
[80]. Acute VTE associated in the setting of con-
genital protein C or protein S deficiency should be
treated with heparin. Long-term therapy can be based
on warfarin, with the aforementioned caution re-
garding slow institution of therapy in patients with
protein C deficiency.
Summary
Excessive bleeding or thrombosis is a preeminent
concern for all surgeons. Patients may be at risk
because of medical therapy, underlying disease, or
complications related to both. An understanding of
the coagulation cascade—mechanisms and tests of
function—permits a rational, if not always complete,
basis for a plan of therapy. Newer anticoagulation
medications are changing how thrombotic complica-
tions, such a VTE or graft occlusion, are treated or
prevented. This entire area is undergoing rapid
evolution, and the approaches that have been standard
for decades soon will be supplanted. Ultimately,
however, the most important assessment is made at
the bedside by the clinician.
meissner & karmy-jones260
References
[1] Dahlback B. Blood coagulation. Lancet 2000;355:
1627–32.
[2] Bachman F. Plasminogen-plasmin enzyme system.
In: Colman RW, Hirsh J, Marder VJ, Clowes AW,
George JN, editors. Hemostasis and thrombosis:
basic principles and clinical practice. Philadelphia7
Lippincott Williams & Wilkins; 2001. p. 275–320.
[3] Butenas S, van’t Veer C, Mann KG. ‘‘Normal’’
thrombin generation. Blood 1999;94:2169–78.
[4] van’t Veer C, Mann KG. Regulation of tissue factor
initiated thrombin generation by the stoichiometric
inhibitors tissue factor pathway inhibitor, antithrom-
bin-III, and heparin cofactor-II. J Biol Chem 1997;
272:4367–77.
[5] Morris TA. Heparin and low molecular weight heparin:
background and pharmacology. Clin Chest Med 2003;
24:39–47.
[6] Heemskerk JW, Bevers EM, Lindhout T. Platelet acti-
vation and blood coagulation. Thromb Haemost 2002;
88:186–93.
[7] Davie EW. Biochemical and molecular aspects of the
coagulation cascade. Thromb Haemost 1995;74:1–6.
[8] Butenas S, van’t Veer C, Cawthern K, Brummel KE,
Mann KG. Models of blood coagulation. Blood Coagul
Fibrinolysis 2000;11(Suppl 1):S9–13.
[9] Broze GJ. Tissue factor pathway inhibitor. Thromb
Haemost 1995;74:90–3.
[10] Collaborative overview of randomised trials of anti-
platelet therapy: I. prevention of death, myocardial
infarction, and stroke by prolonged antiplatelet therapy
in various categories of patients. Antiplatelet Trialists’
Collaboration. BMJ 1994;308:81–106.
[11] Patrono C, Coller B, Dalen JE, et al. Platelet-active
drugs: the relationships among dose, effectiveness, and
side effects. Chest 1998;114(5 Suppl):470S–88S.
[12] Secondary prevention of vascular disease by prolonged
antiplatelet treatment. Antiplatelet Trialists’ Collabo-
ration. BMJ (Clin Res Educ) 1988;296:320–31.
[13] Patrono C, Coller B, Dalen JE, et al. Platelet-active
drugs: the relationships among dose, effectiveness, and
side effects. Chest 2001;119(1 Suppl):39S–63S.
[14] Clarke RJ, Mayo G, Price P, FitzGerald GA. Suppres-
sion of thromboxane A2 but not of systemic prostacy-
clin by controlled-release aspirin. N Engl J Med 1991;
325:1137–41.
[15] Verstraete M, Zoldhelyi P. Novel antithrombotic drugs
in development. Drugs 1995;49:856–84.
[16] Savi P, Pereillo JM, Uzabiaga MF, et al. Identification
and biological activity of the active metabolite of
clopidogrel. Thromb Haemost 2000;84:891–6.
[17] Kaufman JS, O’Connor TZ, Zhang JH, et al. Random-
ized controlled trial of clopidogrel plus aspirin to
prevent hemodialysis access graft thrombosis. J Am
Soc Nephrol 2003;14:2313–21.
[18] Ferguson JJ, Zaqqa M. Platelet glycoprotein IIb/IIIa
receptor antagonists: current concepts and future direc-
tions. Drugs 1999;58:965–82.
[19] Linhardt RJ, Gunay NS. Production and chemical
processing of low molecular weight heparins. Semin
Thromb Hemost 1999;25(Suppl 3):5–16.
[20] Whisstock JC, Pike RN, Jin L, et al. Conformational
changes in serpins: II. the mechanism of activation
of antithrombin by heparin. J Mol Biol 2000;301(5):
1287–305.
[21] Gallus AS, Lee LH, Coghlan DW. New aspects of
the blood coagulation cascade, anticoagulants and vein
thrombosis in Asia. Ann Acad Med Singapore 2002;
31:685–96.
[22] Billett HH. Direct and indirect antithrombins: heparins,
low molecular weight heparins, heparinoids, and
hirudin. Clin Geriatr Med 2001;17:15–29.
[23] Bates SM, Weitz JI. Direct thrombin inhibitors for
treatment of arterial thrombosis: potential differences
between bivalirudin and hirudin. Am J Cardiol 1998;
82:12P–8P.
[24] Ansell J, Hirsh J, Dalen J, et al. Managing oral anti-
coagulant therapy. Chest 2001;119(1 Suppl):22S–38S.
[25] Petaja J, Fernandez JA, Gruber A, Griffin JH. Anti-
coagulant synergism of heparin and activated protein C
in vitro: role of a novel anticoagulant mechanism of
heparin, enhancement of inactivation of factor V by
activated protein C. J Clin Invest 1997;99:2655–63.
[26] Fuller K, Chambers TJ, Gallagher AC. Heparin aug-
ments osteoclast resorption-stimulating activity in
serum. J Cell Physiol 1991;147:208–14.
[27] Weitz JI, Crowther M. Direct thrombin inhibitors.
Thromb Res 2002;106:V275–84.
[28] Hyers TM, Agnelli G, Hull RD, et al. Antithrombotic
therapy for venous thromboembolic disease. Chest
2001;119(1 Suppl):176S–93S.
[29] Beguin S, Choay J, Hemker HC. The action of a
synthetic pentasaccharide on thrombin generation in
whole plasma. Thromb Haemost 1989;61:397–401.
[30] Wiggins BS, Spinler S, Wittkowsky AK, Stringer KA.
Bivalirudin: a direct thrombin inhibitor for percuta-
neous transluminal coronary angioplasty. Pharmaco-
therapy 2002;22:1007–18.
[31] Hirsh J, van Aken WG, Gallus AS, Dollery CT, Cade
WL, Yung WL. Heparin kinetics in venous thrombosis
and pulmonary embolism. Circulation 1976;53:691–5.
[32] Hommes DW, Bura A, Mazzolai L, Buller HR, ten
Cate JW. Subcutaneous heparin compared with con-
tinuous intravenous heparin administration in the initial
treatment of deep vein thrombosis: a meta-analysis.
Ann Intern Med 1992;116:279–84.
[33] Baughman RA, Kapoor SC, Agarwal RK, Kisicki J,
Catella-Lawson F, FitzGerald GA. Oral delivery of
anticoagulant doses of heparin: a randomized, double-
blind, controlled study in humans. Circulation 1998;
98:1610–5.
[34] Money SR, York JW. Development of oral heparin
therapy for prophylaxis and treatment of deep venous
thrombosis. Cardiovasc Surg 2001;9:211–8.
[35] Brill-Edwards P, Ginsberg JS, Johnston M, Hirsh J.
Establishing a therapeutic range for heparin therapy.
Ann Intern Med 1993;119:104–9.

management of the anticoagulated patient 261
[36] Anand S, Ginsberg JS, Kearon C, Gent M, Hirsh J. The
relation between the activated partial thromboplastin
time response and recurrence in patients with venous
thrombosis treated with continuous intravenous hepa-
rin. Arch Intern Med 1996;156:1677–81.
[37] Anand SS, Bates S, Ginsberg JS, et al. Recurrent
venous thrombosis and heparin therapy: an evaluation
of the importance of early activated partial thrombo-
plastin times. Arch Intern Med 1999;159:2029–32.
[38] Raschke R, Reilly B, Guidry J, Fontana J, Srinivas S.
The weight-based heparin dosing nomogram compared
with a ‘‘standard care’’ nomogram: A randomized
controlled trial. Ann Intern Med 1993;119:874–81.
[39] Barritt DW, Jordan SC. Anticoagulant drugs in the
treatment of pulmonary embolism: a controlled trial.
Lancet 1960;1:1309–12.
[40] Zidane M, Schram MT, Planken EW, et al. Frequency
of major hemorrhage in patients treated with unfrac-
tionated intravenous heparin for deep venous throm-
bosis or pulmonary embolism: a study in routine
clinical practice. Arch Intern Med 2000;160:2369–73.
[41] Levine MN, Raskob G, Landefeld S, Kearon C.
Hemorrhagic complications of anticoagulant treatment.
Chest 2001;119(1 Suppl):108S–21S.
[42] Wester JP, de Valk HW, Nieuwenhuis HK, et al. Risk
factors for bleeding during treatment of acute venous
thromboembolism. Thromb Haemost 1996;76:682–8.
[43] Reiter M, Bucek RA, Koca N, Heger J, Minar E.
Idraparinux and liver enzymes: observations from the
PERSIST trial. Blood Coagul Fibrinolysis 2003;14:
61–5.
[44] Gupta AK, Kovacs MJ, Sauder DN. Heparin-induced
thrombocytopenia. Ann Pharmacother 1998;32:55–9.
[45] Warkentin TE, Kelton JG. A 14-year study of
heparin-induced thrombocytopenia. Am J Med 1996;
101:502–7.
[46] Greinacher A, Potzsch B, Amiral J, Dummel V,
Eichner A, Mueller-Eckhardt C. Heparin-associated
thrombocytopenia: isolation of the antibody and char-
acterization of a multimolecular PF4-heparin com-
plex as the major antigen. Thromb Haemost 1994;71:
247–51.
[47] Spiess B, Warkentin T, Francis J, Koster A. Advances
in the understanding and treatment of heparin-induced
thrombocytopenia in patients undergoing cardiac sur-
gery. Clin Adv Hematol Oncol 2003;August:3–11.
[48] Fareed J, Callas D, Hoppensteadt DA, Lewis BE, Bick
RL, Walenga JM. Antithrombin agents as anticoagu-
lants and antithrombotics: implications in drug devel-
opment. Semin Hematol 1999;36(1 Suppl 1):42–56.
[49] Dolovich LR, Ginsberg JS, Douketis JD, Holbrook
G, Cheah G. A meta-analysis comparing low-
molecular weight heparins with unfractionated heparin
in the treatment of venous thromboembolism. Arch
Intern Med 2000;160:181–8.
[50] Wolf B, Nichols DM, Duncan JL. Safety of a single
duplex scan to exclude deep venous thrombosis. Br J
Surg 2000;87:1525–8.
[51] Lormeau JC, Herault JP, Herbert JM. Antithrombin-
mediated inhibition of factor VIIa-tissue factor com-
plex by the synthetic pentasaccharide representing the
heparin binding site to antithrombin. Thromb Haemost
1996;76:5–8.
[52] Petitou M, Duchaussoy P, Herbert JM, et al. The
synthetic pentasaccharide fondaparinux: first in the
class of antithrombotic agents that selectively inhibit
coagulation factor Xa. Semin Thromb Hemost 2002;
28:393–402.
[53] Koopman MM, Buller HR. Short- and long-acting
synthetic pentasaccharides. J Intern Med 2003;254:
335–42.
[54] Amiral J, Lormeau JC, Marfaing-Koka A, et al.
Absence of cross-reactivity of SR90107A/ORG31540
pentasaccharide with antibodies to heparin-PF4 com-
plexes developed in heparin-induced thrombocytope-
nia. Blood Coagul Fibrinolysis 1997;8:114–7.
[55] Turpie AG, Bauer KA, Eriksson BI, Lassen MR.
Fondaparinux vs enoxaparin for the prevention of
venous thromboembolism in major orthopedic surgery:
a meta-analysis of 4 randomized double-blind studies.
Arch Intern Med 2002;162:1833–40.
[56] Herbert JM, Herault JP, Bernat A, et al. Biochemical
and pharmacological properties of SANORG 34006, a
potent and long-acting synthetic pentasaccharide.
Blood 1998;91:4197–205.
[57] Shapiro SS. Treating thrombosis in the 21st century. N
Engl J Med 2003;349:1762–4.
[58] Alving BM, Strickler MP, Knight RD, Barr CF,
Berenberg JL, Peck CC. Hereditary warfarin resis-
tance: investigation of a rare phenomenon. Arch
Intern Med 1985;145:499–501.
[59] Aithal GP, Day CP, Kesteven PJ, Daly AK. Associa-
tion of polymorphisms in the cytochrome P450
CYP2C9 with warfarin dose requirement and risk of
bleeding complications. Lancet 1999;353:717–9.
[60] Treatment of proximal deep vein thrombosis with a
novel synthetic compound (SR90107A/ORG31540)
with pure anti-factor Xa activity: a phase II evaluation.
The Rembrandt Investigators. Circulation 2000;102:
2726–31.
[61] Schulman S. Clinical practice: care of patients receiv-
ing long-term anticoagulant therapy. N Engl J Med
2003;349(7):675–83.
[62] Sallah S, Abdallah JM, Gagnon GA. Recurrent
warfarin-induced skin necrosis in kindreds with
protein S deficiency. Haemostasis 1998;28:25–30.
[63] Direct thrombin inhibitors in acute coronary syn-
dromes: principal results of a meta-analysis based on
individual patients’ data. Lancet 2002;359:294–302.
[64] Matsuo T, Koide M, Kario K. Development
of argatroban, a direct thrombin inhibitor, and its
clinical application. Semin Thromb Hemost 1997;23:
517–22.
[65] Kong DF, Topol EJ, Bittl JA, et al. Clinical outcomes
of bivalirudin for ischemic heart disease. Circulation
1999;100:2049–53.
[66] Swan SK, Hursting MJ. The pharmacokinetics and
pharmacodynamics of argatroban: effects of age, gen-
meissner & karmy-jones262
der, and hepatic or renal dysfunction. Pharmacotherapy
2000;20:318–29.
[67] Hauptmann J. Pharmacokinetics of an emerging new
class of anticoagulant/antithrombotic drugs: a review
of small-molecule thrombin inhibitors. Eur J Clin
Pharmacol 2002;57:751–8.
[68] Gustafsson D, Nystrom J, Carlsson S, et al. The direct
thrombin inhibitor melagatran and its oral prodrug H
376/95: intestinal absorption properties, biochemical
and pharmacodynamic effects. Thromb Res 2001;101:
171–81.
[69] Eriksson BI, Bergqvist D, Kalebo P, et al. Ximelagatran
and melagatran compared with dalteparin for preven-
tion of venous thromboembolism after total hip or knee
replacement: the METHRO II randomised trial. Lancet
2002;360:1441–7.
[70] Geerts WH, Heit JA, Clagett GP, et al. Prevention
of venous thromboembolism. Chest 2001;119(Suppl):
132S–75S.
[71] Francis CW, Berkowitz SD, Comp PC, et al. Compari-
son of ximelagatran with warfarin for the prevention of
venous thromboembolism after total knee replacement.
N Engl J Med 2003;349:1703–12.
[72] Petersen P, Grind M, Adler J. Ximelagatran versus
warfarin for stroke prevention in patients with non-
valvular atrial fibrillation. SPORTIF II: a dose-guiding,
tolerability, and safety study. J Am Coll Cardiol 2003;
41:1445–51.
[73] Wallentin L, Wilcox RG, Weaver WD, et al. Oral
ximelagatran for secondary prophylaxis after myocar-
dial infarction: the ESTEEM randomised controlled
trial. Lancet 2003;362:789–97.
[74] Holst J, Bergvist D, Garre K, Nielsen H, Hedner U,
Ostergaard PB. Protamine neutralization of intravenous
and subcutaneous low-molecular-weight heparin (tin-
zaparin, Logiparin): an experimental investigation in
healthy volunteers. Blood Coagul Fibrinolysis 1994;5:
795–803.
[75] Fan J, Armitstead JA, Adams AG, Davis GA. A
retrospective evaluation of vitamin K1 therapy to
reverse the anticoagulant effect of warfarin. Pharma-
cotherapy 2003;23:1245–50.
[76] Shetty HG, Backhouse G, Bentley DP, Routledge
PA. Effective reversal of warfarin-induced excessive
anticoagulation with low dose vitamin K1. Thromb
Haemost 1992;67:13–5.
[77] Douketis JD, Kearon C, Bates S, Duku EK, Ginsberg
JS. Risk of fatal pulmonary embolism in patients with
treated venous thromboembolism. JAMA 1998;279:
458–62.
[78] Owings JT, Gosselin RC. Bleeding and transfusion.
In: Souba WW, Fink MP, Jurkovich GJ, Kaiser L,
Pearce WH, Pemberton JD, editors. American College
of Surgeons: principles and practice. New York7
WebMD Inc; 2004. p. 5–65.
[79] Lind SE. The bleeding time does not predict surgical
bleeding. Blood 1991;77:2547–52.
[80] Dyke CD, Sobel M. The management of coagulation
problems in the surgical patient. Adv Surg 1991;24:
229–57.
[81] Kreiger JN, Hilgartner MW, Redo SF. Surgery in
patients with congenital disorders of blood coagula-
tion. Ann Surg 1977;185:290–4.
[82] Eikelbloom JW, Bird R, Blythe D, et al. Recombinant
activated factor VII for the treatment of life-threatening
haemorrhage. Blood Coagul Fibrinolysis 2003;14:
713–7.
Thorac Surg Clin
Preoperative Cardiac Evaluation: Mechanisms, Assessment,
and Reduction of Risk
Euan A. Ashley, MRCP, DPhil*, Randall H. Vagelos, MD*
Division of Cardiology, Stanford University School of Medicine, Falk CVRB, 300 Pasteur Drive, Stanford, CA 94305, USA
In the management of cardiovascular and pulmo-
nary disease, the paths of cardiologists and thoracic
surgeons inevitably cross. Interdependence of blood
oxygenation and tissue perfusion means that rarely
does a disease of one system exist in isolation. Al-
though widely acknowledged, however, considerable
uncertainty exists as to when it is appropriate to in-
vestigate cardiac disease in a preoperative thoracic
patient and which tools are best suited to the task.
Common disease origins, commonality of symptoms,
and coexistent disease all serve to make accurate
diagnosis and effective risk prediction difficult. In
addition, interventions known to reduce risk and
save lives are few. This article explores the basis for
anesthetic risk in cardiovascular and pulmonary
disease. Common disease mechanisms and the utility
of tools available to assess risk are discussed. Risk
reduction also is discussed, and recommendations
specific to the preoperative cardiac evaluation of the
thoracic surgery patient are offered.
Procedures
In the United States, and for the purposes of
this article, thoracic surgery is distinguished from
cardiac surgery by the exclusion of procedures in-
volving the heart and proximal vascular tree, includ-
ing the coronary arteries and thoracic aorta, but
excluding the pericardium. The most common pro-
1547-4127/05/$ – see front matter D 2005 Elsevier Inc. All rights
doi:10.1016/j.thorsurg.2005.01.004
* Corresponding authors.
E-mail addresses: [email protected] (E.A. Ashley),
[email protected] (R.H. Vagelos).
cedure in the database of the Society for Thoracic
Surgeons is wedge resection, representing 16% of all
submitted procedures (Table 1) [1]. During the data
collection period, lobectomy constituted 14.5% of
procedures, and esophagectomy constituted 4.5%;
pleurodesis and decortication constituted 5% of pro-
cedures. Endoscopic procedures made up 13%, of
which mediastinoscopy accounted for 7.4%, flexible
bronchoscopy accounted for 4.5%, and esophagos-
copy accounted for 1.2%. The 30-day mortality of
the patients in this database was around 5%, a figure
that emphasizes the high risk of thoracic surgery and
the comorbidity of the patients.
Noncardiac surgery and the cardiovascular
system
To understand fully the value of preoperative car-
diac evaluation, it is helpful to define what exactly it
is about surgery that increases the risk of cardiac
morbidity (Box 1).
Effects of surgery on the cardiovascular system
Although anesthesiologists have many tools at
their disposal with which to control pain, a degree of
nociception and associated autonomic reflex is inevi-
table in response to surgical ‘‘injury.’’ Pain fibers
relay in the brainstem, where reflex sympathetic out-
flow results in augmentation of circulating catechol-
amines and the classic ‘‘fight-or-flight’’ response:
tachycardia, hypertension, cardiac inotropy, vasodila-
tion of skin and skeletal muscle, and vasoconstriction
of intestinal arterioles. These stressors are com-
15 (2005) 263 – 275
reserved.
thoracic.theclinics.com

Table 1
Thoracic surgery procedures*
Procedure %
Lobectomy 14.5
Wedge resection, single 9.5
Mediastinoscopy 7.4
Wedge resection, multiple 6.5
Esophagectomy 4.8
Pleurodesis 2.7
Decortication 2.3
Segmentectomy 1.9
Tracheostomy 1.8
Mediastinal mass resection 1.7
Pericardial window 1.6
Chest wall repair 1.5
Chest wall resection 1.5
Open pleural drainage 1.4
Thymectomy 1.1
* Thoracic surgery procedures submitted to the General
Thoracic Surgery Database; January 2002–June 2003. The
Society of Thoracic Surgeons, 6633 North Saint Clair Street,
Suite 2320, Chicago, IL, USA 60611–3658.
Box 1. Sources of cardiac risk
Nociception and stress increaseendogenous sympathetic nervoussystem activity.
Death of cells leads to release ofintracellular contents—increasedserum potassium and circulatingprotein load.
Death of cells leads to increases incirculating inflammatory mediators.
Anesthetic induction can be associatedwith vasodilation and negativeinotropy.
Succinylcholine can increase serumpotassium.
Narcotic agents inhibit sympatheticreflexes in patients dependent onsympathetic tone.
Volatile agents are cardiodepressantand vasodilatory.
Volatile agents cause coronary dilation,which may lead to coronary steal.
Some volatile agents (halothane)sensitize the myocardium tocatecholamines.
Some volatile agents (desflurane) in-crease myocardial oxygen demand.
ashley & vagelos264
pounded further by blood loss, fluid shift, and meta-
bolic compromise. The ‘‘surgical’’ death of cells
leads to release of intracellular contents and increases
in the plasma levels of intracellular proteins and ions
with a negative transmembrane gradient (eg, potas-
sium). Easily tolerated by a healthy heart, these
metabolic and energetic derangements challenge the
diseased heart and may precipitate ischemia or
decompensated function.
Although sympathetic outflow can be largely
controlled during the procedure, patients with pre-
existing heart failure, who are dependent on sym-
pathetic tone, represent an important exception.
Reducing endogenous sympathetic drive in a popu-
lation with chronic remodeling of the adrenergic
system could lead to decompensation for lack of
circulating catecholamines.
Cardiac effects of general anesthesia
In addition to effects specific to the surgery it-
self, additional cardiovascular challenge is associated
with general anesthesia. Most agents are negative ino-
tropes and vasodilators.
Induction agents
Agents for anesthetic induction, such as propofol,
decrease arterial pressure mainly through vasodila-
tion, whereas barbiturates, such as thiopental, are
negatively inotropic [2]. In contrast, etomidate and
ketamine are minimally cardiodepressant, and the
latter can increase heart rate and blood pressure
through activation of the sympathetic nervous sys-
tem [3].
Neuromuscular blockade
Newer neuromuscular blocking drugs generally
have few cardiovascular side effects. Succinylcho-
line, commonly used because of its rapid onset, can
produce unpredictable changes in heart rate and
increases serum potassium concentration by approx-
imately 0.5 mEq/L. Pancuronium increases blood
pressure and heart rate by blocking muscarinic ace-
tylcholine receptors in the sinoatrial node, increases
sympathetic activity via antimuscarinic actions, and
inhibits reuptake of catecholamines.
Narcotic-based anesthetics
Narcotic-based anesthetics have little direct effect
on myocardial contractility or vasomotor tone, but
attenuate sympathetically mediated cardiovascular
reflexes in response to pain. Although this feature
makes them highly attractive agents for anesthesia in
cardiac patients, narcotic-based anesthetics are less
suitable for patients chronically dependent on en-

preoperative cardiac evaluation 265
dogenous sympathetic tone, in whom the withdrawal
of these reflexes may cause profound hemodynamic
change. In addition, synthetic narcotics are po-
tently vagotonic.
Volatile anesthetics
Volatile anesthetics, such as isoflurane, are used
for maintenance of general anesthesia and produce
varying degrees of vasodilation and negative ino-
tropy, a result of sympathetic nervous system in-
hibition. The negative inotropy includes impaired
diastolic relaxation, which may cause increased end-
diastolic pressures. One volatile agent, desflurane,
has a biphasic effect on sympathetic tone, increasing
activity at lower doses and inhibiting activity at
higher doses [4]. In relation to the coronary circu-
lation, effects of volatile agents are varied. Some
vasodilate coronary arteries, contributing, at least in
theory, to coronary ‘‘steal’’ (vasodilation in the pres-
ence of hemodynamically significant stenoses causes
ischemia by decreasing the coronary perfusion pres-
sure through the distal collateral network). Some
agents, such as halothane, sensitize the myocardium
to catecholamine-induced dysrhythmias, an effect
compounded by hypercapnia.
Manifestations
The combined effects of surgery and anesthesia
are complex, but relate mostly to a balance between
sympathetic nervous system activity (positive ino-
tropy, net increase in vascular resistance) and the
abrogation of these effects directly or indirectly by
anesthesia. These phenomena increase risk in three
ways. First, the negative inotropy of anesthesia may
contribute to decompensated ventricular function and
pulmonary edema, which increases sympathetic
drive. Second, increasing the workload of the heart
may induce ischemia through stable obstructive
coronary disease (low flow but no acute syndrome,
analogous to stable angina). This ischemia amplifies
the risk of arrhythmia already provided by increased
circulating catecholamines and the increased sensi-
tivity to them caused by some anesthetics. Third,
surgery is associated with unstable coronary syn-
dromes and myocardial infarction (MI), most of
which occur in the postoperative, rather than intra-
operative, period.
Non–Q wave, troponin-positive MI and ST
elevation MI occur early in the postoperative period
(8–24 hours) [5–8]. In one study of 185 patients
undergoing major vascular surgery, non–ST eleva-
tion infarction followed periods of prolonged silent
ischemia (50% of perioperative MIs were silent in
another study [8]). This silent ischemia was preceded
by periods of modest tachycardia (typically 90–
100 beats/min) providing a potential early warning
sign and, possibly, a mechanism [7,9]. The presence
of a spectrum of acute syndromes was confirmed
in a postmortem study, in which postoperative MIs
clustered into two groups: patients with no plaque
rupture who tended to present early in days 1 to 3 and
patients with plaque rupture who presented in an even
distribution from days 1 to 12 [10]. Some authors
have suggested different mechanisms are implied in
these two groups [5], although the evidence for this
implication is sparse.
The pathophysiologic basis of postoperative acute
coronary syndromes is not clear. One hypothesis is
that prolonged intraoperative sympathetic overactiva-
tion with hypercontractility and increased blood pres-
sure causes greater intracoronary mechanical forces,
which makes coronary plaques more likely to rupture
(‘‘mechanical’’ hypothesis). Another is that circulat-
ing inflammatory factors released in response to inci-
sion and cautery ‘‘sensitize’’ plaques from the
intraluminal side (‘‘inflammatory’’ hypothesis). Sup-
port for the latter hypothesis comes from the growing
consensus that acute coronary syndromes reflect
activation of at least one branch of, and perhaps the
whole, coronary tree [11,12]. In addition, because
most ischemia is silent and occurs 8 to 24 hours after
the procedure, either the effect takes some time to
build (consistent with the inflammatory hypothesis),
or there is another effect relating to anesthetic re-
covery, for which the most likely candidate is un-
controlled pain causing sympathetic activation and
increased blood pressure (consistent with the
mechanical hypothesis). The reality almost certainly
lies in between with contributions from both of these
mechanisms. There is increasing interest in measur-
ing (and abrogating) inflammatory mediators in
cardiovascular disease generally, although this has
not met with universal success [13].
Risk of cardiac disease in the pulmonary patient
It has been known for some time that chronic
obstructive pulmonary disease (COPD) is an impor-
tant risk marker for atherosclerosis. Even modest
reductions in forced expiratory volume in 1 second
(FEV1) result in large increases in hazard ratios for
ischemic heart disease independent of age, cigarette
smoking, diastolic blood pressure, cholesterol con-
centration, body mass index, and social class [14].
These authors found that FEV1 was equivalent to
cholesterol in predicting ischemic risk. In another

ashley & vagelos266
study [15], severe airflow obstruction almost doubled
the chances of ECG evidence of MI. Although classic
mechanisms of pulmonary hypertension and right
ventricular failure (cor pulmonale) provide a link with
severe pulmonary disease, a relationship with earlier
stage COPD has been less explored. Such early
disease can affect the heart, however, at least in the
form of right axis deviation on the 12-lead ECG [16].
In relation to pathogenesis, Sin and Man [15]
suggested that low-level inflammation originating in
the airways can become systemic and trigger parallel
inflammatory changes in coronary arteries. These
authors showed that patients with highly elevated
C-reactive protein and moderate or severe airflow
obstruction had an infarction injury score higher than
groups without airflow obstruction or groups with
low C-reactive protein, suggesting an additive effect
of these factors on the severity of cardiac injury
after MI. A link with systemic inflammation also is
supported by studies discussing the importance of
systemic inflammation in the prediction [17] and
pathogenesis [18] of heart disease and human [19]
and animal studies [20] showing that particulate air
pollution contributes to the progression of athero-
sclerosis and vulnerability of plaques to rupture.
A second link between pulmonary and cardiovas-
cular disease is provided by the use of inhaled
b-agonist drugs, such as albuterol. In one case-controlstudy [21], compared with subjects who did not fill a
b-agonist prescription, subjects who had filled one
b-agonist prescription in the 3 months before their
index date had an elevated estimated risk of MI,
suggesting a direct effect of inhaled b-agonists on the
processes of plaque erosion and rupture. There was no
dose-response relationship between b-agonist use andrisk. Not all investigators have found such a connec-
tion, however. Ferguson et al [22] performed a pooled
analysis of cardiovascular safety data from salmeterol
use and found no increased risk of cardiovascular
adverse events compared with placebo. There were no
clinically significant differences in heart rate, ectopy,
or 24-hour ECG monitoring between the salmeterol
group and the placebo group [22].
Regardless of the effect of inhaled b-agonists,there is evidence of abnormal endogenous sympa-
thetic tone in COPD patients. Volterrani et al [23]
studied heart rate variability in patients with COPD
and age-matched controls at rest and during vagal and
sympathetic maneuvers. Patients with COPD showed
a depressed global heart rate variability and in par-
ticular a depressed heart rate variability response to
sympathetic and vagal stimuli. More recently, Heindl
et al [24] found that microneurography of the pero-
neal nerve, a surrogate for sympathetic system acti-
vation, was higher in COPD patients with hypoxemia
compared with healthy subjects. On administration
of oxygen, activation decreased only in the COPD
patients, providing direct evidence of baseline sym-
pathetic activation in patients with chronic respiratory
failure. Other authors have found similar results [25].
Assessment of perioperative risk
Surgical risk comprises a combination of factors
relating to the procedure and the patient. The
American Heart Association rates thoracic surgery
as intermediate risk, defined as an estimated risk rate
of less than 5% (consistent with an estimated overall
mortality of approximately 5% [1]). Data relating
specifically to the cardiovascular risk of thoracic sur-
gery are limited, however; most investigators assess-
ing cardiac risk in noncardiac surgery have studied
patients undergoing major vascular surgery.
Risk relating to the surgical patient has been
studied by many investigators and considered by
consensus panels [26]. One problem, already men-
tioned earlier, is that there is currently no test, im-
aging or otherwise, which adequately identifies
‘‘rupture-prone’’ plaques or individuals. It is chal-
lenging to attempt to predict which patients are likely
to have an acute coronary syndrome and which are
likely to have only ischemia with stable obstruction.
Traditional two-dimensional coronary catheterization
is an excellent technique to measure luminal diame-
ter, but vascular remodeling means that encroachment
is a late phenomenon, and studies have shown that
luminal diameter bears little relation [27] (or perhaps
even an inverse relation [28,29]) to likelihood of
plaque rupture. Although some authors have hypothe-
sized that patients might fall into a rupture-prone and
a rupture-resistant group, direct evidence for this is
currently lacking.
Despite this uncertainty and the emerging para-
digm shift, the approach to predicting risk is clear:
measure relevant factors to the best of current ability,
document outcome, and enter the results into a multi-
variate risk prediction model. The issue of workup
bias always is confounding (patients who are judged
by current local criteria to have increased risk have
some intervention, altering that risk); however, the
analysis is still informative.
Guidelines
There have been at least 10 multivariate models
published analyzing risk in noncardiac surgery.

STEP 1 Need fornoncardiac surgery
Coronary revascularizationwithin 5 yr?
Operatingroom
Recurrentsymptomsor signs?
Recent coronary angiogramor stress test?
Intermediate clinicalpredictors†
Intermediate clinical predictors† Intermediate Clinical Predictors†
Major Clinical Predictors**
Minor Clinical Predictors ‡
Minor or noclinical predictors ‡
Minor or no clinical predictors ‡
Operatingroom
Operatingroom
Operatingroom
Postoperative riskstratification and risk
factor reduction
Postoperative riskstratification and risk
factor reduction
Postoperative riskstratification and
risk factor management
Go tostep 6
Go tostep 7
Unstable coronarysyndromes
Decompensated CHF
SignificantarrhythmiasSevere valvulardisease
Renal insufficiency
Diabetes mellitus
Prior MIMild angina pectoris
Compensated orprior CHF
Consider coronaryangiography
Subsequent caredictated by findings and
treatment results
Subsequent care*dictated by findings and treatment results
Subsequent care*dictated by findings and treatment results
Consider delayor cancel noncardiac
surgery
Medical managementand risk factormodification
Clinical predictors
Major clinical predictors**
Clinical predictors
Functional capacity
Surgical risk
Noninvasive testing
Invasive testing
Clinical predictors
Functional capacity
Surgical risk
Noninvasive testing
Invasive testing
Recent coronaryevaluation
Low risk
Low risk
High risk
High risk
Emergencysurgery
Favorable result andno change in
symptoms
STEP 2
STEP 3
STEP 4
STEP 6
STEP 8
STEP 8
STEP 7
Yes
Yes
•
•
•
•
••
•
•
•
Abnormal ECGAdvanced age•
•
History of stroke•
Low functionalcapacity
Rhythm otherthan sinus
•
•
Uncontrolled systemichypertension
•
Poor
(<4 METs)
Poor
(<4 METs)
Moderateor
excellent(<4 METs)
Moderateor
excellent(>4 METs)
Lowsurgical riskprocedure
Highsurgical riskprocedure
High surgical risk
procedure
Considercoronary
angiography
Considercoronary
angiography
Noninvasivetesting
Noninvasivetesting
Intermediatesurgical riskprocedure
Intermediateor low
surgical riskprocedure
Yes
No
No
No
Urgent or electivesurgery
Unfavorable result orchange in symptoms
STEP 5
Fig. 1. The American Heart Association/American College of Cardiology algorithm for preoperative screening. CHF, congestive
heart failure; MI, myocardial infarction. (From Eagle KA, Berger PB, Calkins H, et al. ACC/AHA guideline update for
perioperative cardiovascular evaluation for noncardiac surgery—executive summary: a report of the American College of
Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to Update the 1996 Guidelines on
Perioperative Cardiovascular Evaluation for Noncardiac Surgery). Circulation 2002;105:1257–67; with permission.)
preoperative cardiac evaluation 267
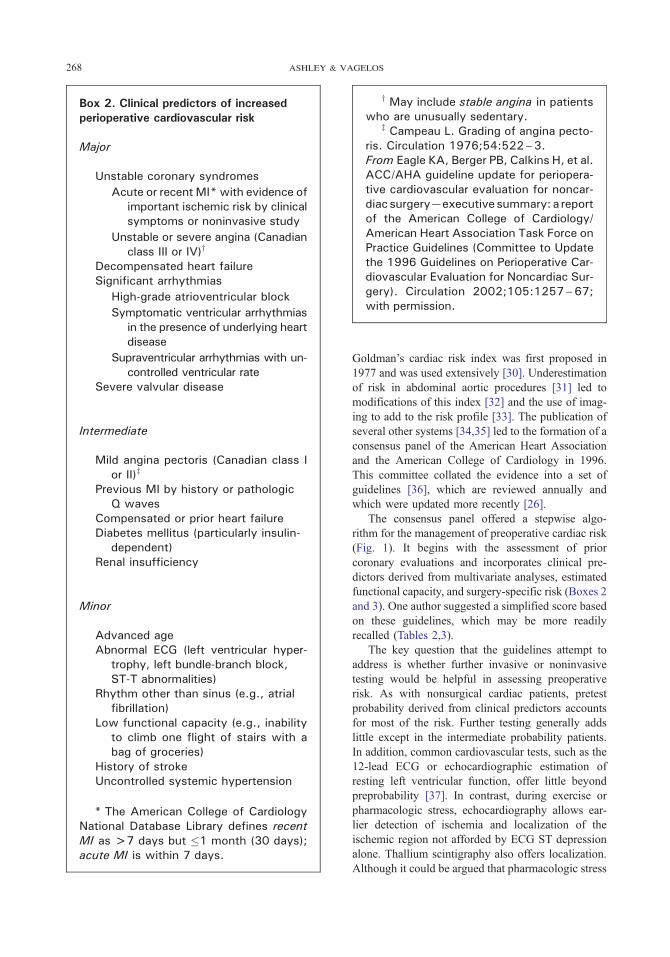
Box 2. Clinical predictors of increasedperioperative cardiovascular risk
Major
Unstable coronary syndromes
Acute or recent MI* with evidence ofimportant ischemic risk by clinicalsymptoms or noninvasive study
Unstable or severe angina (Canadianclass III or IV)y
Decompensated heart failureSignificant arrhythmias
High-grade atrioventricular block
Symptomatic ventricular arrhythmiasin the presence of underlying heartdisease
Supraventricular arrhythmias with un-controlled ventricular rate
Severe valvular disease
Intermediate
Mild angina pectoris (Canadian class Ior II)z
Previous MI by history or pathologicQ waves
Compensated or prior heart failureDiabetes mellitus (particularly insulin-
dependent)Renal insufficiency
Minor
Advanced ageAbnormal ECG (left ventricular hyper-
trophy, left bundle-branch block,ST-T abnormalities)
Rhythm other than sinus (e.g., atrialfibrillation)
Low functional capacity (e.g., inabilityto climb one flight of stairs with abag of groceries)
History of strokeUncontrolled systemic hypertension
* The American College of CardiologyNational Database Library defines recentMI as >7 days but �1 month (30 days);acute MI is within 7 days.
y May include stable angina in patientswho are unusually sedentary.
z Campeau L. Grading of angina pecto-ris. Circulation 1976;54:522–3.From Eagle KA, Berger PB, Calkins H, et al.ACC/AHA guideline update for periopera-tive cardiovascular evaluation for noncar-diac surgery—executive summary: a reportof the American College of Cardiology/American Heart Association Task Force onPractice Guidelines (Committee to Updatethe 1996 Guidelines on Perioperative Car-diovascular Evaluation for Noncardiac Sur-gery). Circulation 2002;105:1257–67;with permission.
ashley & vagelos268
Goldman’s cardiac risk index was first proposed in
1977 and was used extensively [30]. Underestimation
of risk in abdominal aortic procedures [31] led to
modifications of this index [32] and the use of imag-
ing to add to the risk profile [33]. The publication of
several other systems [34,35] led to the formation of a
consensus panel of the American Heart Association
and the American College of Cardiology in 1996.
This committee collated the evidence into a set of
guidelines [36], which are reviewed annually and
which were updated more recently [26].
The consensus panel offered a stepwise algo-
rithm for the management of preoperative cardiac risk
(Fig. 1). It begins with the assessment of prior
coronary evaluations and incorporates clinical pre-
dictors derived from multivariate analyses, estimated
functional capacity, and surgery-specific risk (Boxes 2
and 3). One author suggested a simplified score based
on these guidelines, which may be more readily
recalled (Tables 2,3).
The key question that the guidelines attempt to
address is whether further invasive or noninvasive
testing would be helpful in assessing preoperative
risk. As with nonsurgical cardiac patients, pretest
probability derived from clinical predictors accounts
for most of the risk. Further testing generally adds
little except in the intermediate probability patients.
In addition, common cardiovascular tests, such as the
12-lead ECG or echocardiographic estimation of
resting left ventricular function, offer little beyond
preprobability [37]. In contrast, during exercise or
pharmacologic stress, echocardiography allows ear-
lier detection of ischemia and localization of the
ischemic region not afforded by ECG ST depression
alone. Thallium scintigraphy also offers localization.
Although it could be argued that pharmacologic stress

Table 2
Abbreviated algorithm for assessment of cardiac risk*
Clinical predictors Functional capacity Surgical risk
Major 4 Poor 2 High 2
Intermediate 2 Moderate or 0 Intermediate 1
preoperative cardiac evaluation 269
with a sympathetic agonist, such as dobutamine,
might better mimic the actual stress of surgery, func-
tional capacity has been shown repeatedly to be a
potent predictor of risk in perioperative and general
populations [38–41].
Box 3. Surgery-specific risk* fornoncardiac surgical procedures
High (reported cardiac risk often >5%)
Emergent major operations,particularly in the elderly
Aortic and other major vascular surgeryPeripheral vascular surgeryAnticipated prolonged surgical
procedures associated with largefluid shifts or blood loss or both
Intermediate (reported cardiac riskgenerally <5%)
Carotid endarterectomyHead and neck surgeryIntraperitoneal and intrathoracic surgeryOrthopedic surgeryProstate surgery
Low (reported cardiac risk generally<1%)y
Endoscopic proceduresSuperficial proceduresCataract surgeryBreast surgery
* Combined incidence of cardiac deathand nonfatal MI.
y Do not generally require further pre-operative cardiac testing.From Eagle KA, Berger PB, Calkins H, et al.ACC/AHA guideline update for periopera-tive cardiovascular evaluation for noncar-diac surgery—executive summary: a reportof the American College of Cardiology/American Heart Association Task Force onPractice Guidelines (Committee to Updatethe 1996 Guidelines on Perioperative Car-diovascular Evaluation for Noncardiac Sur-gery). Circulation 2002;105:1257–67;with permission.
better
Minor 0 Low 0
* Each patient gets a point score from each of the three
columns. The total score for the three columns is added. A
point score of �4 suggests the need for further cardiac
evaluation. A patient with �3 points could proceed safely to
the operating room.
From Stinson DK. An abbreviation of the ACC/AHA algo-
rithm for perioperative cardiovascular evaluation for noncar-
diac surgery. Anesth Analg 2003;97:295–6; with permission.
These observations were confirmed by Kertai
et al [42], who performed a meta-analysis of the
prognostic accuracy of different diagnostic tests for
predicting perioperative cardiac risk. They compared
ambulatory ECG, exercise ECG, radionuclide ven-
triculography, myocardial perfusion scintigraphy,
dobutamine stress echocardiography, and dipyrida-
mole stress echocardiography and found that dobuta-
mine stress echocardiography had the optimal
combination of sensitivity (85%) and specificity
(70%) for predicting postprocedure events. In the
statistical model, significant differences were found,
however, only between dobutamine stress echocar-
diography and perfusion scintigraphy (odds ratio 5.5).
Assessing risk in thoracic surgery populations
Although none of the major risk prediction studies
were performed in a thoracic surgery population,
several issues specific to this population warrant
discussion. Although echocardiography offers advan-
tages over ECG in the detection of ischemia and
the assessment of valvular and ventricular function,
chronic lung disease can make quality images dif-
ficult to acquire. One solution is dobutamine stress
MR imaging [43]. Dobutamine stress MR imaging
has not been studied in a perioperative population,
but MR imaging has advantages in accuracy and
reliability over echocardiography [44] and is particu-
larly advantageous in patients with suboptimal
echocardiographic image quality (Fig. 2) [45].
Exercise intolerance is nonspecific, and in patients
with chronic lung disease, it can be unclear whether
reduced functional capacity relates to a modifiable
cardiovascular cause or a less modifiable pulmonary
cause. To approach this problem, there has been
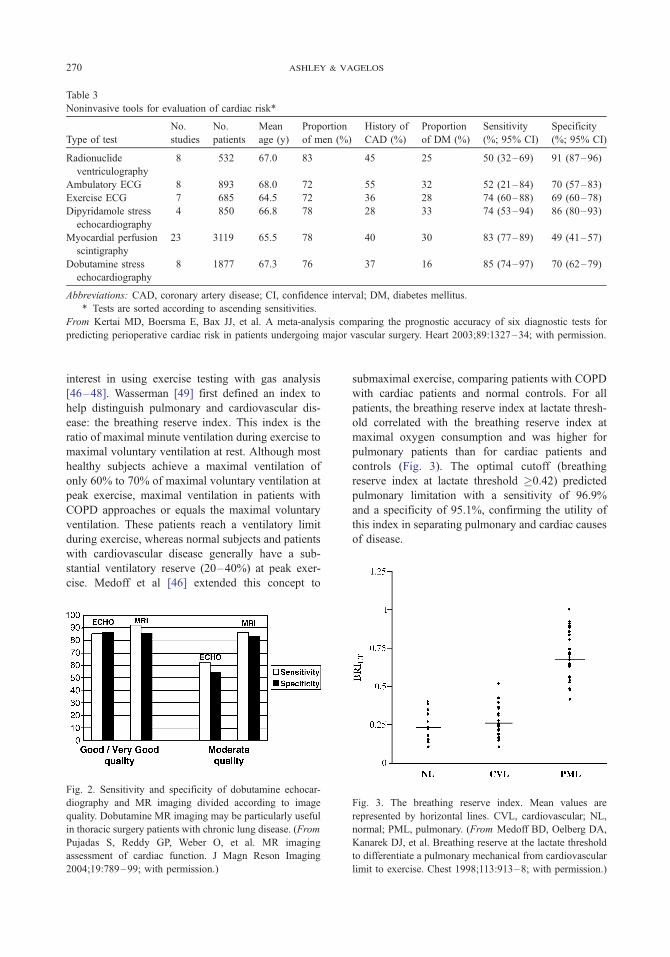
Table 3
Noninvasive tools for evaluation of cardiac risk*
Type of test
No.
studies
No.
patients
Mean
age (y)
Proportion
of men (%)
History of
CAD (%)
Proportion
of DM (%)
Sensitivity
(%; 95% CI)
Specificity
(%; 95% CI)
Radionuclide
ventriculography
8 532 67.0 83 45 25 50 (32–69) 91 (87–96)
Ambulatory ECG 8 893 68.0 72 55 32 52 (21–84) 70 (57–83)
Exercise ECG 7 685 64.5 72 36 28 74 (60–88) 69 (60–78)
Dipyridamole stress
echocardiography
4 850 66.8 78 28 33 74 (53–94) 86 (80–93)
Myocardial perfusion
scintigraphy
23 3119 65.5 78 40 30 83 (77–89) 49 (41–57)
Dobutamine stress
echocardiography
8 1877 67.3 76 37 16 85 (74–97) 70 (62–79)
Abbreviations: CAD, coronary artery disease; CI, confidence interval; DM, diabetes mellitus.
* Tests are sorted according to ascending sensitivities.
From Kertai MD, Boersma E, Bax JJ, et al. A meta-analysis comparing the prognostic accuracy of six diagnostic tests for
predicting perioperative cardiac risk in patients undergoing major vascular surgery. Heart 2003;89:1327–34; with permission.
ashley & vagelos270
interest in using exercise testing with gas analysis
[46–48]. Wasserman [49] first defined an index to
help distinguish pulmonary and cardiovascular dis-
ease: the breathing reserve index. This index is the
ratio of maximal minute ventilation during exercise to
maximal voluntary ventilation at rest. Although most
healthy subjects achieve a maximal ventilation of
only 60% to 70% of maximal voluntary ventilation at
peak exercise, maximal ventilation in patients with
COPD approaches or equals the maximal voluntary
ventilation. These patients reach a ventilatory limit
during exercise, whereas normal subjects and patients
with cardiovascular disease generally have a sub-
stantial ventilatory reserve (20–40%) at peak exer-
cise. Medoff et al [46] extended this concept to
Fig. 2. Sensitivity and specificity of dobutamine echocar-
diography and MR imaging divided according to image
quality. Dobutamine MR imaging may be particularly useful
in thoracic surgery patients with chronic lung disease. (From
Pujadas S, Reddy GP, Weber O, et al. MR imaging
assessment of cardiac function. J Magn Reson Imaging
2004;19:789–99; with permission.)
submaximal exercise, comparing patients with COPD
with cardiac patients and normal controls. For all
patients, the breathing reserve index at lactate thresh-
old correlated with the breathing reserve index at
maximal oxygen consumption and was higher for
pulmonary patients than for cardiac patients and
controls (Fig. 3). The optimal cutoff (breathing
reserve index at lactate threshold �0.42) predicted
pulmonary limitation with a sensitivity of 96.9%
and a specificity of 95.1%, confirming the utility of
this index in separating pulmonary and cardiac causes
of disease.
Fig. 3. The breathing reserve index. Mean values are
represented by horizontal lines. CVL, cardiovascular; NL,
normal; PML, pulmonary. (From Medoff BD, Oelberg DA,
Kanarek DJ, et al. Breathing reserve at the lactate threshold
to differentiate a pulmonary mechanical from cardiovascular
limit to exercise. Chest 1998;113:913–8; with permission.)
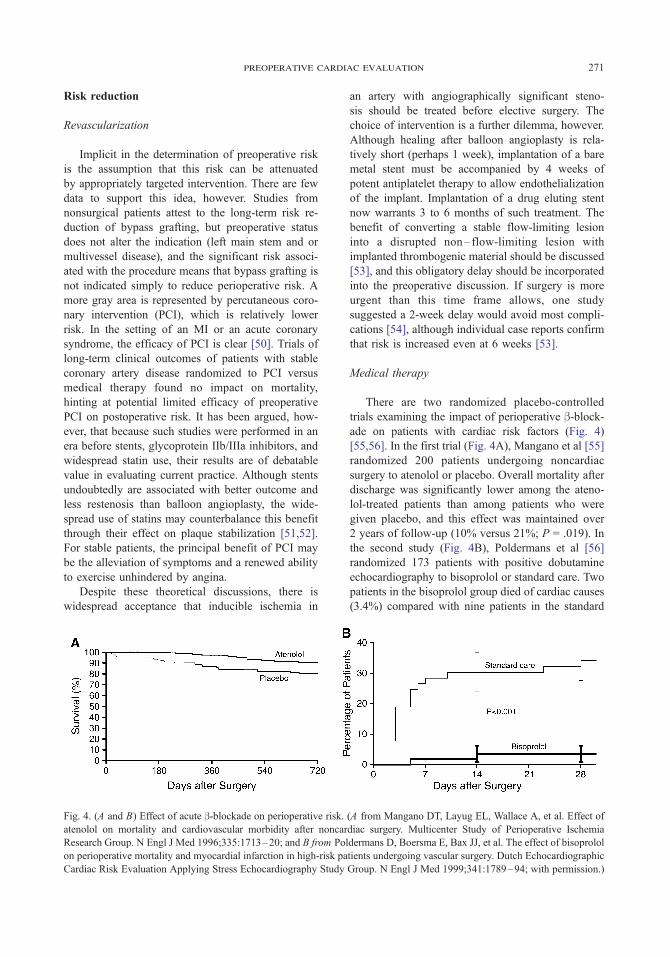
preoperative cardiac evaluation 271
Risk reduction
Revascularization
Implicit in the determination of preoperative risk
is the assumption that this risk can be attenuated
by appropriately targeted intervention. There are few
data to support this idea, however. Studies from
nonsurgical patients attest to the long-term risk re-
duction of bypass grafting, but preoperative status
does not alter the indication (left main stem and or
multivessel disease), and the significant risk associ-
ated with the procedure means that bypass grafting is
not indicated simply to reduce perioperative risk. A
more gray area is represented by percutaneous coro-
nary intervention (PCI), which is relatively lower
risk. In the setting of an MI or an acute coronary
syndrome, the efficacy of PCI is clear [50]. Trials of
long-term clinical outcomes of patients with stable
coronary artery disease randomized to PCI versus
medical therapy found no impact on mortality,
hinting at potential limited efficacy of preoperative
PCI on postoperative risk. It has been argued, how-
ever, that because such studies were performed in an
era before stents, glycoprotein IIb/IIIa inhibitors, and
widespread statin use, their results are of debatable
value in evaluating current practice. Although stents
undoubtedly are associated with better outcome and
less restenosis than balloon angioplasty, the wide-
spread use of statins may counterbalance this benefit
through their effect on plaque stabilization [51,52].
For stable patients, the principal benefit of PCI may
be the alleviation of symptoms and a renewed ability
to exercise unhindered by angina.
Despite these theoretical discussions, there is
widespread acceptance that inducible ischemia in
Fig. 4. (A and B) Effect of acute b-blockade on perioperative risk.
atenolol on mortality and cardiovascular morbidity after noncar
Research Group. N Engl J Med 1996;335:1713–20; and B from Pol
on perioperative mortality and myocardial infarction in high-risk pa
Cardiac Risk Evaluation Applying Stress Echocardiography Study
an artery with angiographically significant steno-
sis should be treated before elective surgery. The
choice of intervention is a further dilemma, however.
Although healing after balloon angioplasty is rela-
tively short (perhaps 1 week), implantation of a bare
metal stent must be accompanied by 4 weeks of
potent antiplatelet therapy to allow endothelialization
of the implant. Implantation of a drug eluting stent
now warrants 3 to 6 months of such treatment. The
benefit of converting a stable flow-limiting lesion
into a disrupted non– flow-limiting lesion with
implanted thrombogenic material should be discussed
[53], and this obligatory delay should be incorporated
into the preoperative discussion. If surgery is more
urgent than this time frame allows, one study
suggested a 2-week delay would avoid most compli-
cations [54], although individual case reports confirm
that risk is increased even at 6 weeks [53].
Medical therapy
There are two randomized placebo-controlled
trials examining the impact of perioperative b-block-ade on patients with cardiac risk factors (Fig. 4)
[55,56]. In the first trial (Fig. 4A), Mangano et al [55]
randomized 200 patients undergoing noncardiac
surgery to atenolol or placebo. Overall mortality after
discharge was significantly lower among the ateno-
lol-treated patients than among patients who were
given placebo, and this effect was maintained over
2 years of follow-up (10% versus 21%; P = .019). In
the second study (Fig. 4B), Poldermans et al [56]
randomized 173 patients with positive dobutamine
echocardiography to bisoprolol or standard care. Two
patients in the bisoprolol group died of cardiac causes
(3.4%) compared with nine patients in the standard
(A from Mangano DT, Layug EL, Wallace A, et al. Effect of
diac surgery. Multicenter Study of Perioperative Ischemia
dermans D, Boersma E, Bax JJ, et al. The effect of bisoprolol
tients undergoing vascular surgery. Dutch Echocardiographic
Group. N Engl J Med 1999;341:1789–94; with permission.)

ashley & vagelos272
care group (17%; P = .02). This pattern also was seen
in nonfatal MI, which occurred in nine patients in the
standard care group (17%) and in no patients in
the bisoprolol group (P < .001). The fact that these
trials achieved statistical significance with only a
few patients suggests a potent protective effect for
b-blockade in postoperative cardiac risk, something
that may have been predicted from the earlier dis-
cussion of pathophysiology.
Although these trials represent the best current
evidence for effective intervention, they say nothing
about the risk of the increasing number of cardiac
patients who are already on b-blockers. Foex et al
reviewed the literature to identify studies examining
the relationship between long-term b-blockade and
adverse perioperative outcome [57]. Of 18 studies
identified, none showed a protective effect of long-
term b-blockade. Cumulative odds ratios calculated
for the likelihood of MI, cardiac death, and major
cardiac complications showed that patients receiving
long-term b-blocker therapy were more likely to have
an MI. Although it seems logical that this finding
relates to the use of b-blockers in a higher risk group
(patients with known hypertension or coronary artery
disease), the populations in the acute studies also
were at high risk, which may have accentuated the
benefits of acute b-blockade. Matching patients for
risk to test this hypothesis would not be ethical,
but the upregulation of b-receptors in long-term
b-blockade provides one explanation and suggests
there may be benefit from additional b-blockade in
the perioperative period.
It could be argued that the applicability of
b-blocker studies to thoracic surgery patients is
limited by the presence of COPD, which traditionally
is held to preclude the use of these medications. More
recent studies have shown that there is little or no
downside to the use of cardioselective b-blockade in
COPD patients [58]. Cardioselective b-blockersproduced no significant change in FEV1 or respira-
tory symptoms compared with placebo and did not
significantly affect the FEV1 treatment response to
b2-agonists in the meta-analysis by Salpeter et al [59].
Even nonselective b-blockers, such as carvedilol,
have been shown to be tolerated well by COPD
patients who have no significant reversible airflow
limitation (patients with asthma tolerated carvedilol
poorly). Finally, Gottlieb et al showed that overall
risk is similarly reduced in COPD patients as in the
general population: Mortality was 40% lower in the
COPD subgroup with b-blockade [60].
For patients with known intolerance of b-blockers,alternative possibilities exist. Four studies have
suggested beneficial effects of the centrally acting
a2-agonists clonidine or mivazerol in reducing post-
operative cardiac events. The mechanism seems to
relate to central sympatholysis, although the inhibi-
tion does not extend to the hypothalamic-pituitary-
adrenal axis [61].
The effects of calcium channel blockers on
perioperative cardiac risk were assessed in a meta-
analysis by Wijeysundera and Beattie [62]. Eleven
studies encompassing 1007 patients were included in
an analysis showing that calcium channel blockers
significantly reduced ischemia and supraventricular
tachycardia and exhibited a trend toward reduction
in death and MI. Most of the benefit seemed to relate
to the use of diltiazem, emphasizing the role of con-
trolling heart rate in postoperative risk (the mechani-
cal hypothesis). In a meta-analysis, Stevens et al [63]
did not corroborate these positive effects of calcium
channel blockers. The earlier study suggests, how-
ever, that a tighter focus on rate-limiting calcium
blockers might yield clearer results.
Two studies have shed light on the protective role
of HMG-CoA reductase inhibitors (statins) in post-
operative risk. Poldermans et al [64] conducted a
case-control study among 2816 patients who under-
went major vascular surgery and found that statin
therapy was significantly less common in cases than
in controls (8% versus 25%; P < .001). Lindenauer
et al [65] performed a retrospective cohort study of
780,591 patients and found that treatment with lipid-
lowering agents was associated with lower crude
mortality (2.13% versus 3.05%; P < .001), and that
this effect remained after adjustment for propensity.
Although clearly arguing for a randomized controlled
trial, reports such as the Heart Protection Study [66]
mean that patients with demonstrable risk increas-
ingly will be on these lifesaving medications.
Summary
The changing paradigm in cardiovascular disease
in which atherosclerotic lesions exist in a spectrum of
stable to unstable, the lack of a perfect prediction
tool, and the paucity of randomized controlled data
on appropriate intervention make protection of car-
diac patients undergoing thoracic surgery challeng-
ing. Nociception-related sympathetic drive combines
with inflammatory stimuli and the cardiodepressant
effects of anesthesia to create a window of maximum
risk in the early postoperative period (8–24 hours),
and although multivariate models have shown that a
combination of surgery-specific risk, patient-specific
cardiovascular history, and estimated functional
capacity best determine the need for further inves-

preoperative cardiac evaluation 273
tigation, the optimal choice of investigation is
unclear. Exercise or dobutamine stress echocardiog-
raphy provide the best validated investigations, and in
the case of poor images, dobutamine MR imaging is
increasingly used. When disease is found, medical
and interventional options are available. PCI is often
used, but the risk of converting a stable flow-limiting
lesion into a less stable non–flow-limiting lesion
must be considered, along with a delay for anti-
platelet therapy and endothelialization of the stent.
Alternatively, medical protection with acute b-block-ade or a2-agonists reduces risk (although b-blockadeoften is avoided in chronic lung disease, even
nonselective agents are safe in patients with non–
airways reactive COPD). In addition, it is likely
that statin use reduces risk, probably by stabilizing
plaques, but patients with cardiac risk are increas-
ingly likely to be taking this medication already.
The assessment and management of cardiac risk in
the perioperative thoracic surgery patient is challeng-
ing. With focused, rational, and individually tailored
management; tight monitoring of postoperative pain;
and a close working relationship between the surgeon,
anesthesiologist, and cardiologist, patient care can be
optimized, and risk can be effectively controlled.
References
[1] The Society of Thoracic Surgeons. General thoracic
surgery procedure database. Chicago, IL7 The Society
of Thoracic Surgeons; 2004.
[2] Gelissen HP, Epema AH, Henning RH, et al. Inotropic
effects of propofol, thiopental, midazolam, etomidate,
and ketamine on isolated human atrial muscle. Anes-
thesiology 1996;84:397–403.
[3] Kawakubo A, Fujigaki T, Uresino H, et al. Compara-
tive effects of etomidate, ketamine, propofol, and fen-
tanyl on myocardial contractility in dogs. J Anesth
1999;13:77–82.
[4] Pac-Soo CK, Ma D, Wang C, et al. Specific actions of
halothane, isoflurane, and desflurane on sympathetic
activity and A delta and C somatosympathetic reflexes
recorded in renal nerves in dogs. Anesthesiology 1999;
91:470–8.
[5] Landesberg G. The pathophysiology of perioperative
myocardial infarction: facts and perspectives. J Car-
diothorac Vasc Anesth 2003;17:90–100.
[6] Badner NH, Knill RL, Brown JE, et al. Myocardial
infarction after noncardiac surgery. Anesthesiology
1998;88:572–8.
[7] Landesberg G, Mosseri M, Zahger D, et al. Myocardial
infarction after vascular surgery: the role of prolonged
stress-induced, ST depression-type ischemia. J Am
Coll Cardiol 2001;37:1839–45.
[8] Landesberg G, Luria MH, Cotev S, et al. Importance of
long-duration postoperative ST-segment depression in
cardiac morbidity after vascular surgery. Lancet 1993;
341:715–9.
[9] Rapp HJ, Rabethge S, Luiz T, et al. Perioperative ST-
segment depression and troponin T release: identifica-
tion of patients with highest risk for myocardial
damage. Acta Anaesthesiol Scand 1999;43:124–9.
[10] Cohen MC, Aretz TH. Histological analysis of
coronary artery lesions in fatal postoperative myocar-
dial infarction. Cardiovasc Pathol 1999;8:133–9.
[11] Naghavi M, Libby P, Falk E, et al. From vulnerable
plaque to vulnerable patient: a call for new definitions
and risk assessment strategies. Part II. Circulation
2003;108:1772–8.
[12] Naghavi M, Libby P, Falk E, et al. From vulnerable
plaque to vulnerable patient: a call for new definitions
and risk assessment strategies. Part I. Circulation 2003;
108:1664–72.
[13] Anker SD, Coats AJ. How to RECOVER from
RENAISSANCE? The significance of the results
of RECOVER, RENAISSANCE, RENEWAL and
ATTACH. Int J Cardiol 2002;86:123–30.
[14] Hole DJ, Watt GC, Davey-Smith G, et al. Impaired
lung function and mortality risk in men and women:
findings from the Renfrew and Paisley prospective
population study. BMJ 1996;313:711–6.
[15] Sin DD, Man SF. Why are patients with chronic
obstructive pulmonary disease at increased risk of
cardiovascular diseases? The potential role of systemic
inflammation in chronic obstructive pulmonary dis-
ease. Circulation 2003;107:1514–9.
[16] Conover M. Understanding electrocardiography.
St Louis7 Mosby; 2002.
[17] Ridker PM, Rifai N, Rose L, et al. Comparison of
C-reactive protein and low-density lipoprotein choles-
terol levels in the prediction of first cardiovascular
events. N Engl J Med 2002;347:1557–65.
[18] Li JJ, Fang CH. C-reactive protein is not only an in-
flammatory marker but also a direct cause of cardio-
vascular diseases. Med Hypoth 2004;62:499–506.
[19] Brook RD, Franklin B, Cascio W, et al. Air pollution
and cardiovascular disease: a statement for healthcare
professionals from the Expert Panel on Population and
Prevention Science of the American Heart Association.
Circulation 2004;109:2655–71.
[20] Suwa T, Hogg JC, Quinlan KB, et al. Particulate air
pollution induces progression of atherosclerosis. J Am
Coll Cardiol 2002;39:935–42.
[21] Au DH, Lemaitre RN, Curtis JR, et al. The risk of
myocardial infarction associated with inhaled beta-
adrenoceptor agonists. Am J Respir Crit Care Med
2000;161:827–30.
[22] Ferguson GT, Funck-Brentano C, Fischer T, et al.
Cardiovascular safety of salmeterol in COPD. Chest
2003;123:1817–24.
[23] Volterrani M, Scalvini S, Mazzuero G, et al. Decreased
heart rate variability in patients with chronic obstruc-
tive pulmonary disease. Chest 1994;106:1432–7.
[24] Heindl S, Lehnert M, Criee CP, et al. Marked sym-
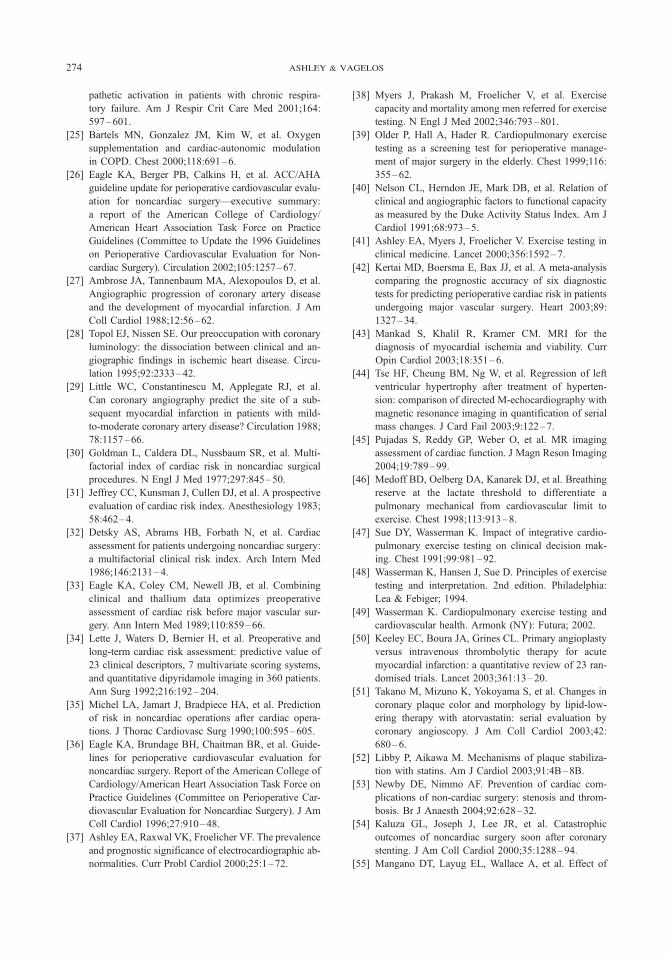
ashley & vagelos274
pathetic activation in patients with chronic respira-
tory failure. Am J Respir Crit Care Med 2001;164:
597–601.
[25] Bartels MN, Gonzalez JM, Kim W, et al. Oxygen
supplementation and cardiac-autonomic modulation
in COPD. Chest 2000;118:691–6.
[26] Eagle KA, Berger PB, Calkins H, et al. ACC/AHA
guideline update for perioperative cardiovascular evalu-
ation for noncardiac surgery—executive summary:
a report of the American College of Cardiology/
American Heart Association Task Force on Practice
Guidelines (Committee to Update the 1996 Guidelines
on Perioperative Cardiovascular Evaluation for Non-
cardiac Surgery). Circulation 2002;105:1257–67.
[27] Ambrose JA, Tannenbaum MA, Alexopoulos D, et al.
Angiographic progression of coronary artery disease
and the development of myocardial infarction. J Am
Coll Cardiol 1988;12:56–62.
[28] Topol EJ, Nissen SE. Our preoccupation with coronary
luminology: the dissociation between clinical and an-
giographic findings in ischemic heart disease. Circu-
lation 1995;92:2333–42.
[29] Little WC, Constantinescu M, Applegate RJ, et al.
Can coronary angiography predict the site of a sub-
sequent myocardial infarction in patients with mild-
to-moderate coronary artery disease? Circulation 1988;
78:1157–66.
[30] Goldman L, Caldera DL, Nussbaum SR, et al. Multi-
factorial index of cardiac risk in noncardiac surgical
procedures. N Engl J Med 1977;297:845–50.
[31] Jeffrey CC, Kunsman J, Cullen DJ, et al. A prospective
evaluation of cardiac risk index. Anesthesiology 1983;
58:462–4.
[32] Detsky AS, Abrams HB, Forbath N, et al. Cardiac
assessment for patients undergoing noncardiac surgery:
a multifactorial clinical risk index. Arch Intern Med
1986;146:2131–4.
[33] Eagle KA, Coley CM, Newell JB, et al. Combining
clinical and thallium data optimizes preoperative
assessment of cardiac risk before major vascular sur-
gery. Ann Intern Med 1989;110:859–66.
[34] Lette J, Waters D, Bernier H, et al. Preoperative and
long-term cardiac risk assessment: predictive value of
23 clinical descriptors, 7 multivariate scoring systems,
and quantitative dipyridamole imaging in 360 patients.
Ann Surg 1992;216:192–204.
[35] Michel LA, Jamart J, Bradpiece HA, et al. Prediction
of risk in noncardiac operations after cardiac opera-
tions. J Thorac Cardiovasc Surg 1990;100:595–605.
[36] Eagle KA, Brundage BH, Chaitman BR, et al. Guide-
lines for perioperative cardiovascular evaluation for
noncardiac surgery. Report of the American College of
Cardiology/American Heart Association Task Force on
Practice Guidelines (Committee on Perioperative Car-
diovascular Evaluation for Noncardiac Surgery). J Am
Coll Cardiol 1996;27:910–48.
[37] Ashley EA, Raxwal VK, Froelicher VF. The prevalence
and prognostic significance of electrocardiographic ab-
normalities. Curr Probl Cardiol 2000;25:1–72.
[38] Myers J, Prakash M, Froelicher V, et al. Exercise
capacity and mortality among men referred for exercise
testing. N Engl J Med 2002;346:793–801.
[39] Older P, Hall A, Hader R. Cardiopulmonary exercise
testing as a screening test for perioperative manage-
ment of major surgery in the elderly. Chest 1999;116:
355–62.
[40] Nelson CL, Herndon JE, Mark DB, et al. Relation of
clinical and angiographic factors to functional capacity
as measured by the Duke Activity Status Index. Am J
Cardiol 1991;68:973–5.
[41] Ashley EA, Myers J, Froelicher V. Exercise testing in
clinical medicine. Lancet 2000;356:1592–7.
[42] Kertai MD, Boersma E, Bax JJ, et al. A meta-analysis
comparing the prognostic accuracy of six diagnostic
tests for predicting perioperative cardiac risk in patients
undergoing major vascular surgery. Heart 2003;89:
1327–34.
[43] Mankad S, Khalil R, Kramer CM. MRI for the
diagnosis of myocardial ischemia and viability. Curr
Opin Cardiol 2003;18:351–6.
[44] Tse HF, Cheung BM, Ng W, et al. Regression of left
ventricular hypertrophy after treatment of hyperten-
sion: comparison of directed M-echocardiography with
magnetic resonance imaging in quantification of serial
mass changes. J Card Fail 2003;9:122–7.
[45] Pujadas S, Reddy GP, Weber O, et al. MR imaging
assessment of cardiac function. J Magn Reson Imaging
2004;19:789–99.
[46] Medoff BD, Oelberg DA, Kanarek DJ, et al. Breathing
reserve at the lactate threshold to differentiate a
pulmonary mechanical from cardiovascular limit to
exercise. Chest 1998;113:913–8.
[47] Sue DY, Wasserman K. Impact of integrative cardio-
pulmonary exercise testing on clinical decision mak-
ing. Chest 1991;99:981–92.
[48] Wasserman K, Hansen J, Sue D. Principles of exercise
testing and interpretation. 2nd edition. Philadelphia7
Lea & Febiger; 1994.
[49] Wasserman K. Cardiopulmonary exercise testing and
cardiovascular health. Armonk (NY)7 Futura; 2002.
[50] Keeley EC, Boura JA, Grines CL. Primary angioplasty
versus intravenous thrombolytic therapy for acute
myocardial infarction: a quantitative review of 23 ran-
domised trials. Lancet 2003;361:13–20.
[51] Takano M, Mizuno K, Yokoyama S, et al. Changes in
coronary plaque color and morphology by lipid-low-
ering therapy with atorvastatin: serial evaluation by
coronary angioscopy. J Am Coll Cardiol 2003;42:
680–6.
[52] Libby P, Aikawa M. Mechanisms of plaque stabiliza-
tion with statins. Am J Cardiol 2003;91:4B–8B.
[53] Newby DE, Nimmo AF. Prevention of cardiac com-
plications of non-cardiac surgery: stenosis and throm-
bosis. Br J Anaesth 2004;92:628–32.
[54] Kaluza GL, Joseph J, Lee JR, et al. Catastrophic
outcomes of noncardiac surgery soon after coronary
stenting. J Am Coll Cardiol 2000;35:1288–94.
[55] Mangano DT, Layug EL, Wallace A, et al. Effect of

preoperative cardiac evaluation 275
atenolol on mortality and cardiovascular morbidity
after noncardiac surgery. Multicenter Study of Peri-
operative Ischemia Research Group. N Engl J Med
1996;335:1713–20.
[56] Poldermans D, Boersma E, Bax JJ, et al. The effect
of bisoprolol on perioperative mortality and myocar-
dial infarction in high-risk patients undergoing vascu-
lar surgery. Dutch Echocardiographic Cardiac Risk
Evaluation Applying Stress Echocardiography Study
Group. N Engl J Med 1999;341:1789–94.
[57] Giles JW, Sear JW, Foex P. Effect of chronic beta-
blockade on perioperative outcome in patients under-
going noncardiac surgery: an analysis of observational
and case control studies. Anaesthesia 2004;59(6):574–83.
[58] Andrus MR, Holloway KP, Clark DB. Use of beta-
blockers in patients with COPD. Ann Pharmacother
2004;38:142–5.
[59] Salpeter SR, Ormiston TM, Salpeter EE, et al.
Cardioselective beta-blockers for chronic obstructive
pulmonary disease: a meta-analysis. Respir Med 2003;
97:1094–101.
[60] Gottlieb SS, McCarter RJ, Vogel RA. Effect of beta-
blockade on mortality among high-risk and low-risk
patients after myocardial infarction. N Engl J Med
1998;339(8):489–97.
[61] Yotsui T. Clonidine premedication prevents sympa-
thetic hyperactivity but does not prevent hypothalamo-
pituitary-adrenocortical responses in patients under-
going laparoscopic cholecystectomy. J Anesth 2001;
15:78–82.
[62] Wijeysundera DN, Beattie WS. Calcium channel
blockers for reducing cardiac morbidity after non-
cardiac surgery: a meta-analysis. Anesth Analg 2003;
97:634–41.
[63] Stevens RD, Burri H, Tramer MR. Pharmacologic
myocardial protection in patients undergoing non-
cardiac surgery: a quantitative systematic review.
Anesth Analg 2003;97:623–33.
[64] Poldermans D, Bax JJ, Kertai MD, et al. Statins are
associated with a reduced incidence of perioperative
mortality in patients undergoing major noncardiac
vascular surgery. Circulation 2003;107:1848–51.
[65] Lindenauer PK, Pekow P, Wang K, et al. Lipid-
lowering therapy and in-hospital mortality following
major noncardiac surgery. JAMA 2004;291:2092–9.
[66] Collins R, Armitage J, Parish S, et al. MRC/BHF
Heart Protection Study of cholesterol-lowering with
simvastatin in 5963 people with diabetes: a ran-
domised placebo-controlled trial. Lancet 2003;361:
2005–16.

Thorac Surg Clin
Preoperative Preparation for Esophageal Surgery
Jessica Scott Donington, MD
Division of Thoracic Surgery, Department of Cardiothoracic Surgery, Stanford University School of Medicine, Falk CVRB,
300 Pasteur Drive, Stanford, CA 94305, USA
Esophageal surgery requires careful attention to
detail to avoid complications and ensure operative
success. Careful preoperative assessment and prepa-
ration is as important as meticulous surgical tech-
nique in ensuring a successful outcome. Most elective
esophageal surgeries can be placed into two broad
groups: resections for cancer and interventions for
benign esophageal conditions, such as gastroesopha-
geal reflux disease (GERD) and esophageal motility
disorders. Although proper preoperative diagnosis
and evaluation are vital to the operative success of
both groups, the patient population, risk factors,
scope of procedure, anticipated outcome, and pre-
operative preparation are different, and they are
addressed separately here.
Preoperative evaluation for benign esophageal
disease
The surgical treatment of benign esophageal
disorders is challenging because it attempts to alter
esophageal anatomy with the goal of improving func-
tion. A successful outcome is assessed by the ability
to provide symptom relief without complication. The
introduction of laparoscopic and thoracoscopic tech-
niques in the 1980s and 1990s has had a significant
impact on the use of surgery for the control of be-
nign esophageal conditions. Less invasive approaches
have altered the attitude of patients and physicians
toward surgical intervention for functional disease of
the esophagus. With the increased use of surgery
comes an increased risk of improper patient selection.
1547-4127/05/$ – see front matter D 2005 Elsevier Inc. All rights
doi:10.1016/j.thorsurg.2005.01.001
E-mail address: [email protected]
Symptoms of esophageal disease, such as dysphagia,
epigastric pain, heartburn, regurgitation, and belch-
ing, are nonspecific and can occur in a variety of
esophageal, gastric, and duodenal disorders [1]. A
precise diagnosis is vital before any surgical inter-
vention for benign esophageal disease.
GERD is the most common benign disorder of the
esophagus and accounts for 75% of benign esopha-
geal disease [2]. Although many of the symptoms
of GERD can be controlled with medication, such an
approach is inadequate to control all symptoms and
prevent complications in many patients. Achalasia is
the most common primary motility disorder of the
esophagus, and similar to GERD, surgical treatment
now is most commonly laparoscopic. Patients with
typical and atypical symptoms of disease should un-
dergo a full battery of clinical tests to confirm the
diagnosis and exclude other causes of symptoms.
Other motility disorders that need to be recognized
or ruled out preoperatively include diffuse esopha-
geal spasm, nutcracker esophagus, hypertensive lower
esophageal sphincter (LES), and nonspecific motility
disorders. An extensive workup also is necessary to
rule out secondary motility disorders of the esopha-
gus, which develop from long-standing disease and
greatly hamper the success of surgery if not identified
before intervention.
Most patients undergoing procedures for benign
esophageal disease are relatively healthy and ambu-
latory. Malnutrition is not a major preoperative con-
cern because most of these patients still can swallow.
Most of these operations now are performed lapa-
roscopically with short hospitalizations and rapid
return to oral intake. The procedures are relatively
well tolerated with low rates of morbidity and mor-
tality. The successful relief of symptoms after these
15 (2005) 277 – 285
reserved.
thoracic.theclinics.com

donington278
operations depends on a precise diagnosis and iden-
tification of patients who are most likely to benefit
from the procedure. The focus of the preoperative
evaluation is on an accurate and precise diagnosis,
rather than cardiopulmonary status of the patient.
Barium esophagogram
Radiographic study of the esophagus is a fun-
damental part of the comprehensive evaluation of
patients with esophageal dysfunction. A barium eso-
phagogram defines esophageal anatomy and provides
some functional assessment of the esophagus. Esopha-
gogram should include examination of the esopha-
geal body and the upper and lower sphincters.
Videotaped swallows can be analyzed in slow motion
for better delineation of functional disorders. Barium
esophagogram should be one of the first diagnostic
tests in patients with dysphagia. It can contribute to
the diagnosis with typical findings such as the ‘‘bird-
beak’’ tapering of the distal esophagus in achalasia
and can exclude quickly anatomic diseases, such as
diverticulum or neoplasm (Fig. 1). The role of radio-
graphic studies in GERD is also to identify anatomic
complications of the disease, such as stricture. Con-
trast esophagography provides information that is
vital in the planning of an antireflux operation, in-
cluding the location of the gastroesophageal junction,
the presence and size of a hiatal hernia, the presence
of an intrathoracic stomach, or the presence of a
shortened esophagus. Any one of these findings may
Fig. 1. Contrast (barium) esophagograms showing achalasia (A),
esophagus (C).
cause the surgeon to alter his or her approach and
consider an open versus a laparoscopic approach or a
thoracic versus an abdominal approach.
Endoscopy with biopsy
Endoscopy should be performed in all patients
with benign esophageal disorders, including GERD,
to exclude or identify esophageal complications. It is
useful to grade the severity of esophagitis, rule out
infectious agents, identify strictures and diverticula,
and establish the size of hiatal hernia. Biopsy speci-
mens should be obtained of any mucosal abnormali-
ties to exclude the presence of Barrett’s esophagus or
malignancy; cultures also should be sent so that yeast
and other infectious agents can be treated preopera-
tively, and strictures can be dilated.
Esophageal manometry
Esophageal manometry is an essential preopera-
tive test in patients undergoing procedures for GERD
or another motility disorder. It is the gold standard for
the assessment of the function of the LES and body
of the esophagus. It allows for the diagnosis of pri-
mary esophageal motility disorders, such as achala-
sia, diffuse esophageal spasm, nutcracker esophagus,
and hypertensive LES. Esophageal manometry can
identify the effects of systemic disorders, such as
scleroderma and diabetes. At manometry, the LES
is described in terms of its position relative to the
diaphragm, length, resting pressure, and relaxation in
esophageal diverticulum (B), and adenocarcinoma of distal

preoperative preparation for esophageal surgery 279
response to swallowing. Esophageal body motility is
described by the amplitude and progression of con-
tractions in response to wet and dry swallows. Im-
paired esophageal motility can lead to delayed
esophageal emptying and prolonged acid exposure
of the esophageal mucosa. Poor esophageal body mo-
tility also has been shown to affect the development
and persistence of reflux-associated respiratory symp-
toms. If esophageal body motility disorders are recog-
nized preoperatively, adjustments to the operative
procedure can be made, including a looser or partial
wrap. Missed motility disorders have a significant
impact on the success of antireflux procedures.
Twenty-four-hour pH monitoring
Twenty-four-hour pH monitoring is probably
the most important test to confirm the diagnosis of
GERD. This test, which has 90% sensitivity in the
diagnosis of GERD, is performed as an outpatient
procedure and requires that proton-pump inhibitors
be stopped for at least 7 days and H2-blockers be
stopped 2 days before testing [3]. Patients are in-
structed to attend to their normal activities and restrict
their diets to foods with pH between 5.0 and 6.0. The
patients keep a careful record of any reflux symptoms
during the study period. The pH monitor measures
the amount of time the esophagus pH is below a
given threshold over a 24-hour period. Most centers
use a pH of 4 as the threshold. If the esophageal
Fig. 2. The primary tumor is defined by the depth of invasion thr
mucosa and submucosa. T2 invades into, but not through, the mu
invades adjacent structures. Lymph nodes are defined by the prese
TW. Clinical staging of esophageal carcinoma: CT, EUS, PET. Ch
mucosa is exposed to a pH of less than 4 for more
than 5% of the testing time, pathologic acid reflux is
present [4]. A positive test is determined by the
amount of time that the distal esophagus is exposed to
a pH less than 4, the number of reflux episodes with
pH less than 4, the number of episodes lasting more
than 5 minutes, and the length of the longest episode
[4]. Patients with alkaline reflux also can have
damage to the esophageal mucosa despite a negative
pH test. In these cases, an intraluminal bile salt probe
can be placed in the esophagus to confirm a diag-
nosis. Although pH studies classically are used to
confirm the diagnosis of GERD, they also have a
distinct pattern in achalasia and other motility
disorders in which there is stasis and fermentation
in the esophagus that leads to lactic acid production
and a consistently low pH through the day.
Summary
Careful preoperative evaluation of esophageal
anatomy and function is key to the successful out-
come of surgical intervention for benign esophageal
disease. The expectation for symptom relief without
complication is high in this patient population. It
is imperative that the anatomy and function of the
esophagus are thoroughly delineated preoperatively
so that the correct diagnosis can be made, and the
correct operation can be performed. Endoscopy, pH
monitoring, manometry, and radiographic studies are
ough the layers of the esophageal wall. T1 is limited to the
scularis propria. T3 extends through the muscularis, and T4
nce (N1) or absence (N0) of metastatic spread. (From Rice
est Surg Clin N Am 2000;10:473; with permission.)
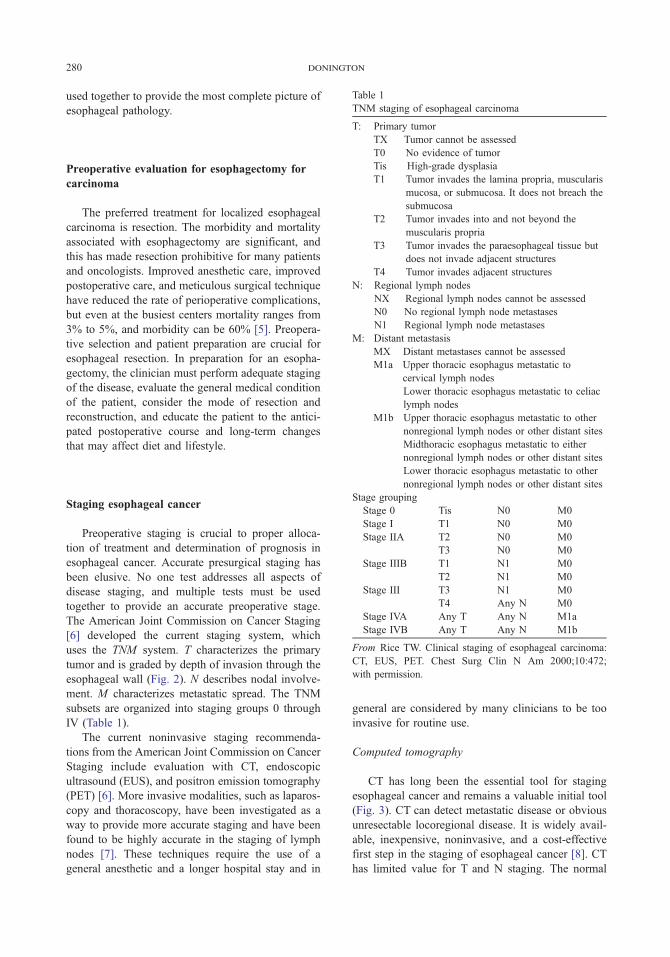
Table 1
TNM staging of esophageal carcinoma
donington280
used together to provide the most complete picture of
esophageal pathology.
T: Primary tumor
TX Tumor cannot be assessed
T0 No evidence of tumor
Tis High-grade dysplasia
T1 Tumor invades the lamina propria, muscularis
mucosa, or submucosa. It does not breach the
submucosa
T2 Tumor invades into and not beyond the
muscularis propria
T3 Tumor invades the paraesophageal tissue but
does not invade adjacent structures
T4 Tumor invades adjacent structures
N: Regional lymph nodes
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastases
N1 Regional lymph node metastases
M: Distant metastasis
MX Distant metastases cannot be assessed
M1a Upper thoracic esophagus metastatic to
cervical lymph nodes
Lower thoracic esophagus metastatic to celiac
lymph nodes
M1b Upper thoracic esophagus metastatic to other
nonregional lymph nodes or other distant sites
Midthoracic esophagus metastatic to either
Preoperative evaluation for esophagectomy for
carcinoma
The preferred treatment for localized esophageal
carcinoma is resection. The morbidity and mortality
associated with esophagectomy are significant, and
this has made resection prohibitive for many patients
and oncologists. Improved anesthetic care, improved
postoperative care, and meticulous surgical technique
have reduced the rate of perioperative complications,
but even at the busiest centers mortality ranges from
3% to 5%, and morbidity can be 60% [5]. Preopera-
tive selection and patient preparation are crucial for
esophageal resection. In preparation for an esopha-
gectomy, the clinician must perform adequate staging
of the disease, evaluate the general medical condition
of the patient, consider the mode of resection and
reconstruction, and educate the patient to the antici-
pated postoperative course and long-term changes
that may affect diet and lifestyle.
nonregional lymph nodes or other distant sitesLower thoracic esophagus metastatic to other
nonregional lymph nodes or other distant sites
Stage grouping
Stage 0 Tis N0 M0
Stage I T1 N0 M0
Stage IIA T2 N0 M0
T3 N0 M0
Stage IIIB T1 N1 M0
T2 N1 M0
Stage III T3 N1 M0
T4 Any N M0
Stage IVA Any T Any N M1a
Stage IVB Any T Any N M1b
From Rice TW. Clinical staging of esophageal carcinoma:
CT, EUS, PET. Chest Surg Clin N Am 2000;10:472;
with permission.
Staging esophageal cancer
Preoperative staging is crucial to proper alloca-
tion of treatment and determination of prognosis in
esophageal cancer. Accurate presurgical staging has
been elusive. No one test addresses all aspects of
disease staging, and multiple tests must be used
together to provide an accurate preoperative stage.
The American Joint Commission on Cancer Staging
[6] developed the current staging system, which
uses the TNM system. T characterizes the primary
tumor and is graded by depth of invasion through the
esophageal wall (Fig. 2). N describes nodal involve-
ment. M characterizes metastatic spread. The TNM
subsets are organized into staging groups 0 through
IV (Table 1).
The current noninvasive staging recommenda-
tions from the American Joint Commission on Cancer
Staging include evaluation with CT, endoscopic
ultrasound (EUS), and positron emission tomography
(PET) [6]. More invasive modalities, such as laparos-
copy and thoracoscopy, have been investigated as a
way to provide more accurate staging and have been
found to be highly accurate in the staging of lymph
nodes [7]. These techniques require the use of a
general anesthetic and a longer hospital stay and in
general are considered by many clinicians to be too
invasive for routine use.
Computed tomography
CT has long been the essential tool for staging
esophageal cancer and remains a valuable initial tool
(Fig. 3). CT can detect metastatic disease or obvious
unresectable locoregional disease. It is widely avail-
able, inexpensive, noninvasive, and a cost-effective
first step in the staging of esophageal cancer [8]. CT
has limited value for T and N staging. The normal

Fig. 3. CT scans showing extensive involvement of the gastric cardia (A), malignant adenopathy along the left gastric artery (B),
and loss of definition of the mediastinal planes (C) in a patient with a large mid-third squamous cell carcinoma of the esophagus.
preoperative preparation for esophageal surgery 281
esophagus is 3 mm thick, and anything greater than
5 mm on CT is considered abnormal [9]. Current CT
technology does not allow detailed visualization of
the esophageal wall and is unable to determine depth
of invasion and cannot distinguish between T1, T2, or
T3 disease. CT has some value in the identification
and exclusion of T4 tumors, particularly when the
clinician can identify a fat plane surrounding the
tumor. CT criteria for invasion of adjacent structures
includes displacement or indentation into the airway
and greater than 90� arc interface with the aorta [10].
CT easily visualizes abnormal lymph nodes in the
paraesophageal and retroperitoneal fat. Lymph nodes
greater than 1 cm in short axis are considered abnor-
mal [6]. The sensitivity of CT for mediastinal lymph-
adenopathy is 34% to 61%, and the sensitivity of CT
in the abdomen is 50% to 76% [11].
CT is useful for the detection of metastatic dis-
ease. The most common sites of metastatic spread
from esophageal cancer are the liver, lung, bone, and
adrenal glands. A CT scan of the chest and upper
abdomen encompasses most of those sites. CT has a
sensitivity of 70% to 80% for detection of liver me-
tastases 2 cm or larger [12]. Its sensitivity decreases
significantly in subcentimeter lesions.
Positron emission tomography
PET uses a radioactively labeled glucose molecule
fluorodeoxyglucose F 18 (FDG) to image tumor tis-
sue. FDG becomes trapped in the glycogen pathway
and accumulates in cells that are metabolically active.
FDG is reported to accumulate in 97% of esophageal
cancers [13]. The availability of PET is becoming
more widespread, and at present its role in the staging
of esophageal cancer is being evaluated in a coop-
erative group setting by the American College of
Surgeons Oncology Group (AOSOG Z0060).
The sensitivity of PET for detecting primary
esophageal tumors is high [13]. The technique is
not able to distinguish esophageal wall layers or
paraesophageal tissue, therefore it has no value
in determining T status. PET also is poor at differ-
entiating regional lymph nodes from the primary
tumor because the uptake from the primary tumor
frequently overwhelms uptake in regional nodes. The

donington282
sensitivity, specificity, and accuracy of PET for loco-
regional lymph nodes are 52%, 94%, and 84% com-
pared with 15%, 97%, and 77% for CT [13]. The
most important role for PET is in screening for distant
metastatic disease. Most studies indicate that PET is
superior to CT in detecting metastases. Sensitivity of
PET is 70% to 75%, and specificity is 90% to 93%
[14]. PET is able to detect metastatic disease that is
occult on CT in 15% to 20% of patients [15].
Endoscopic ultrasound
EUS is a significant advancement in the preopera-
tive evaluation of esophageal cancer. It is currently
the most accurate mode of determining T and N status
of esophageal tumors. EUS combines flexible endos-
copy with high-frequency ultrasound and provides
360� visualization of the layers of the esophageal
wall. The esophageal wall is visualized in five dis-
crete alternating hypoechoic and hyperechoic layers
surrounded by paraesophageal tissues (Fig. 4). The
fourth layer represents the muscularis propria, which
is crucial in differentiating early-stage tumors from
T3 tumors. The accuracy of determination of T status
by EUS is 84% [16], which is far superior to that of
CT. The accuracy of T status determination seems to
vary with the depth of invasion. EUS is most accurate
for T4 tumors (88–100%) and least accurate at
predicting T1 tumors (75–82%) [11]. Frequently the
standard EUS probe cannot be passed through a
malignant stricture, and this significantly impairs the
accuracy of the examination. The inability to pass the
probe is in itself an accurate predictor of a T3 or T4
tumor in 90% of patients [17], but does not allow for
Fig. 4. Esophageal ultrasound of a T3N1 esophageal can-
cer. Arrows indicate penetration of the tumor into the mus-
cularis propria. Arrowhead indicates an enlarged nearby
lymph node.
the evaluation of celiac lymph nodes. Small probes
and safer dilating techniques allow for more complete
studies [18].
EUS also is an excellent tool for the evaluation
of regional lymph nodes in esophageal cancer. Fea-
tures that indicate malignant involvement include size
greater than 1cm, round shape, sharp edges, and a
hypoechoic center [16]. Accuracy of predicting nodal
involvement is nearly 100% when all four character-
istics are present [19]. EUS seems to be more accu-
rate for the diagnosis of celiac nodal involvement
than mediastinal node involvement [20]. The ability
to combine fine-needle aspiration with EUS offers
even greater precision in staging by providing his-
tologic verification of suspicious lymph nodes. The
sensitivity, specificity, and accuracy of EUS and fine-
needle aspiration in detecting celiac lymph node in-
volvement are 98%, 100%, and 98% [21].
EUS does not allow evaluation of distant sites
and has a limited role in the assessment of metastatic
disease. EUS can detect metastatic spread to organs
adjacent to the stomach and esophagus. Metastases
to the left lateral segment of the liver and the retro-
peritoneum can be detected by EUS, and biopsy
specimens can be obtained [12].
Bronchoscopy
Bronchoscopy is an important tool in the evalua-
tion of patients with carcinoma involving the
proximal esophagus and mid-esophagus. Direct
tracheobronchial involvement renders the patient T4
and unresectable. Brushings, washings, and biopsy
samples increase the rate of detection of invasion
compared with visual inspection alone [22].
Patient evaluation
An esophageal resection results in a significant
physiologic insult to the patient, and a patient’s gen-
eral medical condition is a major factor when de-
ciding whether a patient with esophageal cancer can
undergo resection. The mortality from esopha-
gectomy at major centers in the United States has
declined from of 12% in the 1970s to 3% to 7% in the
1990s [23]. Adequate preoperative patient selection
is an important part of that reduction in mortality,
by identifying high-risk patients in whom resection
would be hazardous. Factors to consider in preopera-
tive risk analysis include age, pulmonary function,
cardiac function, and nutritional status.

preoperative preparation for esophageal surgery 283
Age
Age older than 70 has been identified by some
authors as a risk factor for poor outcome after esopha-
gectomy, with cardiopulmonary causes accounting
for most deaths in this age group [24]. More recent
series have not seen an increase in complication rates
in the elderly when properly selected [25], even in
patients who receive induction chemoradiotherapy
[26]. Age is recognized as an independent risk factor
for the development of pulmonary complications
[27], and older patients need a full cardiopulmonary
evaluation preoperatively.
Pulmonary evaluation
Pulmonary complications are among the most
frequent complications after esophagectomy. They
also are among the most devastating complications,
resulting in prolonged hospital stay, increased costs,
and increased hospital mortality. Respiratory failure
is a significant risk factor for death after esophagec-
tomy [28]. The rate of pulmonary complications after
esophagectomy is 29% to 35%, higher than after any
common operation, including a major lung resection
[27]. Reasons cited for this increase include surgery
in two cavities, disruption of lymphatics, disruption
of respiratory muscles, placement of conduit in the
chest, and recurrent laryngeal nerve injury [27]. Pa-
tient factors, including preexisting lung disease,
tobacco and alcohol abuse, and poor performance
status, also contribute to pulmonary complications.
Attempts have been made to identify patients who are
at increased risk for postoperative pulmonary com-
plications after esophagectomy. Aside from age,
overall performance status (Eastern Cooperative
Oncology Group scale) and percent forced expiratory
vital capacity in 1 second have been recognized as
risk factors for pulmonary complications [27]. Be-
cause outcome after esophagectomy is influenced
heavily by pulmonary status, careful preoperative
pulmonary assessment with pulmonary function tests
is mandatory. In addition, high-risk patients may re-
quire arterial blood gas or expired gas analysis during
exercise for appropriate evaluation.
Nutritional evaluation
The most common presenting symptom in pa-
tients with esophageal cancer is dysphagia, a symp-
tom often associated with significant weight loss.
There is a correlation between preoperative values of
prognostic nutritional index and the incidence of
postoperative complications [29]. In addition, there is
a decrease in the rate of resectability in patients with
anorexia [30]. Nutritional supplementation should
be considered in any patient with a greater than
10%weight loss or an abnormally low serum albumin
level [31]. Patients receiving preoperative radiation
and chemotherapy are at increased risk for preopera-
tive malnutrition. For these patients, preopera-
tive nutritional supplementation, through either an
operatively placed jejunal feeding tube or a naso-
enteric tube, should be considered before the start of
therapy to help improve nutritional status before sur-
gical resection.
Cardiac evaluation
After esophagectomy, death resulting from iso-
lated cardiac cause is uncommon, but cardiac events
are recognized as a common cause of morbidity, with
atrial arrhythmias being the most common cardiac
complication [28]. A cardiac history, physical exami-
nation, and ECG are required in all patients. The need
for a more extensive evaluation with echocardio-
graphy or stress evaluation is based on the patient’s
coronary disease risk factors, including advanced age,
tobacco use, diabetes, hypertension, elevated choles-
terol, and presence of peripheral vascular disease.
Mode of resection and reconstruction
Numerous accepted surgical approaches to esopha-
geal resection and reconstruction exist. The most com-
monly used procedures in the United States are the
transthoracic (Ivor Lewis) and transhiatal approaches.
The approach used is individualized based on the
tumor characteristics and location, the surgeon’s pref-
erence, and the patient’s medical needs. A careful
history of previous operations or diseases is needed
before making a decision regarding the approach for
resection and the conduit for reconstruction. Severe
chronic obstructive pulmonary disease or history of
previous thoracotomy or empyema may preclude a
transthoracic approach.
The stomach is the conduit of choice for recon-
struction for most surgeons. The stomach has an
extensive vascular supply, large size (it can reach to
the base of the tongue in most cases), and recon-
struction requires only one anastomosis. In patients
with a history of previous gastric surgery or extensive
tumor extension into the stomach, a secondary plan

donington284
for reconstruction needs to be considered. The colon
is the next most commonly used replacement. If a
colon interposition is anticipated, angiographic and
colonoscopic (or radiographic) evaluation should be
done preoperatively, and the colon should be pre-
pared before surgery. Either right or left colon can be
used. Esophageal reconstruction with the colon
requires three anastomoses, but functional results
are good.
Summary
Careful preoperative assessment is crucial in pa-
tients undergoing esophagectomy. The procedure
carries significant morbidity and mortality, and care-
ful evaluation is vital to minimizing risks. Tumor
stage and the patient’s general medical condition play
equally important roles in determining operability.
Patients with impaired pulmonary, cardiac, or nutri-
tional function need to be identified, and reversible
impairments need to be treated preoperatively. Pre-
operative tumor staging is done with a combination
of tests, which should include CT, PET, and EUS
for best noninvasive staging and more invasive tech-
niques used on an individual basis.
References
[1] Costantini M, Crookes PF, Bremner RM, et al. Value
of physiologic assessment of foregut symptoms in a
surgical practice. Surgery 1993;114:780–6.
[2] Trus TL, Hunter JG. Minimally invasive surgery of the
esophagus and stomach. Am J Surg 1997;173:242–55.
[3] Klaus A, Hinder RA. Gastroesophageal reflux and
esophageal hiatal hernia. In: Kelly KA, Sarr MG,
Hinder RA, editors. Mayo Clinic gastrointestinal sur-
gery. Philadelphia7 WB Saunders; 2004. p. 23–35.
[4] Costantini M, DeMeester TR. Preoperative assessment
of esophageal function. In: Bremner CG, DeMeester
TR, Peracchia A, editors. Modern approach to benign
esophageal disease. St Louis7 Quality Medical Publish-
ing; 1995. p. 17–56.
[5] Swisher SG, Deford L, Merriman KW, et al. Effect of
operative volume on morbidity, mortality, and hospital
use after esophagectomy for cancer. J Thorac Cardio-
vasc Surg 2000;119:1126–32.
[6] Greene FL, Page DL, Fleming ID, et al. Esophagus.
In: Greene FL, Page DL, Fleming ID, et al, editors.
American Joint Committee on Cancer: Cancer Stag-
ing Handbook. New York7 Springer-Verlag; 2002.
p. 101–9.
[7] Krasna MJ, Jiao X. Thoracoscopic and laparoscopic
staging for esophageal cancer. Semin Thorac Cardio-
vasc Surg 2000;12:186–94.
[8] Hadzijahic N, Wallace MB, Hawes RH, et al. CT or
EUS for the initial staging of esophageal cancer? A
cost minimization analysis. Gastrointest Endosc 2000;
52:715–20.
[9] van Overhagen H, Behrendt MD. Diagnosis and
staging of carcinoma of the esophagus and gastro-
esophageal junction, and detection of positive re-
currence, by computed tomography. In: Meyers MA,
editor. Neoplasms of the Digestive Tract: Imaging,
Staging, and Management. Philadelphia7 Lippencott-
Raven; 1998. p. 31–48.
[10] Picus D, Balfe DM, Koehler RE, Roper CL, Owen JW.
Computed tomography in the staging of esophageal
carcinoma. Radiology 1983;146:433–8.
[11] Saunders HS, Wolfman NT, Ott DJ. Esophageal
cancer: Radiologic staging. Radiol Clin North Am
1997;35:281–94.
[12] Rice TW. Clinical staging of esophageal carcinoma:
CT, EUS, and PET. Chest Surg Clin N Am 2000;10:
471–85.
[13] Kim K, Park SJ, Kim BT, Lee KS, Shim YM. Evalu-
ation of lymph node metastases in squamous cell
carcinoma of the esophagus with positron emission
tomography. Ann Thorac Surg 2001;71:290–4.
[14] Luketich JD, Friedman DM, Weigel TL, et al. Evalu-
ation of distant metastases in esophageal cancer:
100 consecutive positron emission tomography scans.
Ann Thorac Surg 1999;68:1133–6.
[15] Flamen P, Lerut A, Van Cutsem E, et al. Utility of
positron emission tomography for the staging of pa-
tients with potentially operable esophageal carcinoma.
J Clin Oncol 2000;18:3202–10.
[16] Rosch T. Endosonographic staging of esophageal can-
cer: a review of literature results. Gastrointest Endosc
Clin N Am 1995;5:537–47.
[17] Van Dam J, Rice TW, Catalano MF, Kirby T, Sivak Jr
MV. High-grade malignant stricture is predictive of
esophageal tumor stage: Risks of endosonographic
evaluation. Cancer 1993;71:2910–7.
[18] Pfau PR, Ginsberg GG, Lew RJ, Faigel DO, Smith DB,
Kochman ML. Esophageal dilation for endosono-
graphic evaluation of malignant esophageal strictures
is safe and effective. Am J Gastroenterol 2000;95:
2813–5.
[19] Catalano MF, Sivak Jr MV, Rice T, Gragg LA, Van
Dam J. Endosonographic features predictive of lymph
node metastasis. Gastrointest Endosc 1994;40:442–6.
[20] Catalano MF, Alcocer E, Chak A, et al. Evaluation of
metastatic celiac axis lymph nodes in patients with
esophageal carcinoma: accuracy of EUS. Gastrointest
Endosc 1999;50:352–6.
[21] Eloubeidi MA, Wallace MB, Reed CE, et al. The utility
of EUS and EUS-guided fine needle aspiration in
detecting celiac lymph node metastasis in patients with
esophageal cancer: a single-center experience. Gastro-
intest Endosc 2001;54:714–9.
[22] Riedel M, Stein HJ, Mounyam L, Lembeck R, Siewert
JR. Extensive sampling improves preoperative bron-
choscopic assessment of airway invasion by supra-
preoperative preparation for esophageal surgery 285
carinal esophageal cancer: a prospective study in 166
patients. Chest 2001;119:1652–60.
[23] Swisher SG, Hunt KK, Holmes EC, Zinner MJ,
McFadden DW. Changes in the surgical management
of esophageal cancer from 1970 to 1993. Am J Surg
1995;169:609–14.
[24] Muehrcke DD, Kaplan DK, Donnelly RJ. Oesopha-
gogastrectomy in patients over 70. Thorax 1989;44:
141–5.
[25] Fontes PR, Nectoux M, Escobar AG, Eilers RJ, Davila
AR. Is age a risk factor for esophagectomy? Int Surg
2001;86:94–6.
[26] Rice D, Correa A, Putnam JB, et al. Induction che-
moradiotherapy prior to esophagectomy in elderly pa-
tients is not associated with increased morbidity.
Presented at the 40th Annual Meeting of the Society
of Thoracic Surgeons. San Antonio, 2004.
[27] Ferguson MK, Durkin AE. Preoperative prediction of
the risk of pulmonary complications after esophagec-
tomy for cancer. J Thorac Cardiovasc Surg 2002;123:
661–9.
[28] Griffin S, Desai J, Charlton M, Townsend E, Fountain
SW. Factors influencing mortality and morbidity fol-
lowing oesophageal resection. Eur J Cardiothorac Surg
1989;3:419–23.
[29] Nozoe T, Kimura Y, Ishida M, Saeki H, Korenaga D,
Sugimachi K. Correlation of pre-operative nutritional
condition with post-operative complications in surgical
treatment for oesophageal carcinoma. Eur J Surg Oncol
2002;28:396–400.
[30] Belghiti J, Langonnet F, Bourstyn E, Fekete F. Surgical
implications of malnutrition and immunodeficiency in
patients with carcinoma of the oesophagus. Br J Surg
1983;70:339–41.
[31] Reed CE. Surgical management of esophageal carci-
noma. Oncologist 1999;4:95–105.
Thorac Surg Clin
Preoperative Preparation of the Patient with
Myasthenia Gravis
Kemp H. Kernstine, MD, PhD
Department of Thoracic Surgery, City of Hope National Medical Center, 1500 East Duarte Road, Suite 2001,
Duarte, CA 91010-3000, USA
The combination of symptoms of myasthenia
gravis (MG) was first described in the latter part of
the 19th century [1]. The role of the thymus in the
pathogenesis of MG was theoretical until the work
of Sauerbruch and Blalock [2]. In 1939, Blalock et al
[3] reported performing a thymectomy in a myas-
thenic woman who had dramatic postoperative symp-
tom improvement. Blalock et al [4] reported their first
myasthenic thymectomy series 2 years later. Several
features, including the timing of surgery from the
time of diagnosis, the age of the patient, and the de-
gree of symptoms and the extent of the thymic resec-
tion, seem to correlate with remission [5]. Residual
tissue (2 g) after thymectomy may perpetuate the
symptoms [6].
The role of thymectomy in the treatment of MG
is not well defined. Identification of an appropriate
patient depends on a variety of characteristics. First,
does the patient have MG? A thorough evaluation of
the classic symptoms of the disease and others that
are in the differential diagnosis should be performed.
Provocative tests may assist in modifying the diag-
nosis; disease classification by symptoms and treating
drugs helps to determine the likelihood of surgical
resection success. Are there comorbid diseases that
might pose a significant obstacle to surgery? Would
thymectomy benefit the patient? These are a few of
the questions that are addressed in this article.
MG is the fatigue of voluntary muscles that
worsens with repetitive or continuous use and im-
1547-4127/05/$ – see front matter D 2005 Elsevier Inc. All rights
doi:10.1016/j.thorsurg.2005.01.002
E-mail address: [email protected]
proves with rest. The symptoms worsen as the day
progresses. The proximal muscle groups are pre-
dominantly affected and usually symmetrically. The
shoulders and upper extremities are more commonly
involved than the lower extremities. Sudden or grad-
ual weakness of the skeletal musculature, even with
minimal exertion, is the classic presentation. Ptosis,
diploplia, and blurring are the presenting symptoms
in nearly 50% of patients, and in 15%, they are the
sole symptoms. Of patients, 85% develop generalized
muscle weakness. In 20%, the bulbar muscles alone
are affected.
The physical examination may show a loss of
smile, facial weakness, and nasal speech. Patients
frequently may sit slumped forward, unable to hold
their head erect. Patients may be febrile and have
rhonchi, rales, and wheezing from the recurrent as-
piration. The gag reflex may be absent. In contrast
to other potential diseases, the pupils in MG should
react to light and accommodation, and the corneal
reflex should be preserved. Placing an ice pack over
the eyelids of myasthenic patients with ptosis tem-
porarily improves the lagging lid. Signs of exoph-
thalmos may represent coexistent thyroid disease.
Limitation of neck flexion and extension may be a
sign of coexistent rheumatoid arthritis. Myasthenic
patients may have associated atrial fibrillation and
signs of heart failure. Provocative testing during the
examination to show weakness with repetitive ac-
tion includes hand grip strength with a dynamometer,
head raising, and arm and leg raising. Stepping up
and down on a footstool may prove difficult as the
exercise is repeated. Patients may have an elevated
white blood cell count, fever, and chest x-ray findings
15 (2005) 287 – 295
reserved.
thoracic.theclinics.com

kernstine288
consistent with pneumonia. A thorough history and
physical examination by the MG surgeon often
provides sufficient information to make the diagnosis
and determine the appropriate test to confirm it. To
assist in grading the disease and following the course
of therapy, Barohn et al [7] developed a quantitative
MG score that has been adopted by the Myasthenia
Gravis Foundation (Table 1).
MG is an autoimmune disease. Nearly 90% of
MG patients test positive for acetylcholine receptor
(ACh-R) antibodies [8]. The serum from affected
patients may be transferred experimentally to and
induces symptoms in test animals. Plasmapheresis
reduces or relieves the symptoms. A complex inter-
action of the thymic myoid cells with the local cyto-
Table 1
Quantitative myasthenia gravis score for disease severity
Test item None Mild
Grade 0 1
Double vision on lateral
gaze right or left
(circle one), seconds
61 11–60
Ptosis
(upward gaze), seconds
61 11–60
Facial muscles Normal lid
closure
Complete, weak,
some resistance
Swallowing 4 oz water
(1⁄2 cup)
Normal Minimal coughing
or throat clearing
Speech after counting aloud
from 1 to 50 (onset
of dysarthria)
None at 50 Dysarthria at 30–4
Right arm outstretched
(90� sitting), seconds240 90–239
Left arm outstretched
(90� sitting), seconds240 90–239
Vital capacity, % predicted �80 65–79
Right-hand grip, kgW
Men �45 15–44
Women �30 10–29
Left-hand grip, kgW
Men �35 15–34
Women �25 10–24
Head lifted
(45� supine), seconds120 30–119
Right leg outstretched
(45� supine), seconds100 31–99
Left leg outstretched
(45� supine), seconds100 31–99
From Barohn RJ, McIntire D, Herbelin L, et al. Reliability test
Acad Sci 1998;841:769–72; with permission.
kine and complement pathways is believed to initiate
and perpetuate the disease [9]. Neither ACh-R anti-
body concentration nor antibody binding seems to
correlate with the severity of the disease or the prog-
nosis. Ultimately, there is a gradual destruction of the
nicotinic postsynaptic motor end plate ACh-R. The
decrease in the number of receptors seems to corre-
late with the severity of disease [10]. Symptoms usu-
ally occur when the amount of receptors is less than
30% of normal [11]. Other abnormalities identified in
the synaptic cleft include a reduction in the end plate
folds and an increase in the distance of the synaptic
cleft. The result is less ACh released with repetitive
stimulation, in essence a ‘‘rundown’’ phenomenon,
and less effect from the ACh released [12]. Drugs,
Moderate Severe Score
2 3
1–10 Spontaneous
1–10 Spontaneous
Complete, without
resistance
Incomplete
Severe coughing/
chocking or nasal
regurgitation
Cannot swallow
(test not attempted)
9 Dysarthria at 10–29 Dysarthria at 9
10–89 0–9
10–89 0–9
50–64 <50
5–14 0–4
5–9 0–4
5–14 0–4
5–9 0–4
1–29 0
1–30 0
1–30 0
Total quantitative
myasthenia gravis
score (range, 0–39)
ing of the quantitative myasthenia gravis score. Ann N Y

Box 1. Myasthenia Gravis Foundationclassification*
I—May have weakness of eye closure
All other muscle strength is normalII—Mild weakness affecting other
than ocular muscles
Alsomay have ocular muscle weak-ness of any severityIIa—Predominantly affecting limb
or axial muscles or bothAlsomay have lesser involve-
ment of oropharyngeal orrespiratorymusclesorboth
III—Moderate weakness affecting otherthan ocular muscles
Alsomay have ocular muscleweak-ness of any severity
IIIa—Predominantly affectinglimb or axial muscles or bothAlso may have lesser
involvement of oropha-ryngeal muscles
IIIb—Predominantly affectingoropharyngeal or respira-tory muscles or both
IV—Severe weakness affecting otherthan ocular muscles
Also may have ocular muscle weak-ness of any severity
IVa—Predominantly affecting limbor axial muscles or bothAlso may have lesser
involvement of oropha-ryngeal muscles
IVb—Predominantly affectingoropharyngeal or respira-tory muscles or both
V—Defined by intubation, with or with-out mechanical ventilation exceptwhen employed in routine postop-erative management. The use of afeeding tube without intubationplaces the patient in class IVb
* It is recommended that the most se-verely affected muscles be employed todefine the patient’s class. The maximumseverity—the most severe pretreatmentstatus determined by this classification—is recommended as a permanent pointof reference.
Data from Appendix: Myasthenia GravisFoundation of America Recommendationsfor Clinical Research Standards. In:Kaminski HJ, editor. Myasthenia Gravisand related disorders. Totowa (NJ): Hu-mana Press; 2003. p. 373–80.
preoperative preparation of mg patient 289
body temperature, and emotions may worsen the
neuromuscular transmission.
The age of presentation is bimodal. The most
typical patients are young women in their 20s and 30s
(mean 26 years). The male-to-female ratio is 1:4, and
for patients younger than 30, it is 1:5. Among older
patients, men are more common. The symptom onset
may be slow or rapid. The prevalence is 1 to 14 per
100,000 [13]. Since the 1980s, the mortality asso-
ciated with MG has decreased. As a result, the num-
ber of living patients has increased. Ten percent of
patients have an additional associated autoimmune
disorder; 4% have thyroid abnormalities, more com-
monly hypothyroidism.
The Myasthenia Gravis Foundation has made
numerous modifications to the Osserman Classifica-
tion (Box 1). The classification provides a means
to evaluate the natural history, assist in developing
a treatment plan, and assist in determining a prog-
nosis. It is not a linear grading system. The examiner
simply determines whether there is presence of
ocular, bulbar, generalized, or proximal muscle weak-
ness and makes a rough subjective assessment of
the severity.
A general understanding of the diagnostic tests
assists in confirming the diagnosis. Before surgery, it
is helpful to have a neurologist who is experienced
in the disease examine the potential surgical patient.
Electromyography (EMG) has been used since 1895.
The ‘‘jolly test’’ repetitively stimulates a peripheral
motor nerve at 2 to 3 Hz while recording the muscle
action potential from two surface electrodes. The test
is considered diagnostic when the height of the mea-
sured action potential decreases by 15% or more
with the repetitive stimulation. Accuracy is optimized
when the symptomatic muscle groups are tested. Fifty
percent of MG patients have false-negative EMG,
especially patients with mild generalized symptoms
or ocular symptoms only. The test is simple to per-
form, but interpretation varies by observer.
Single-fiber EMG or ‘‘jitter test’’ requires an
experienced neurophysiologist and is expensive to
perform. Fine-needle electrodes are placed between
two muscle fibers innervated by a single motor neu-
ron. The variation and the action potential between

Box 2. Differential diagnosis of patientswith myasthenia gravis
Congenital myasthenic syndromesDrug-induced myasthenic syndromes
Penicillamine, organophosphates
Curare
Procainamide
Quinines
Aminoglycosides
MetoclopramideEaton-Lambert syndromeAmyotrophic lateral sclerosisMuscular atrophyHyperthyroidismGraves’ diseaseBotulismProgressive external ophthalmoplegia
(Kearns-Sayre syndrome)Intercranial mass compressing
cranial nervesPsychoneurosis
kernstine290
the two muscle fibers are measured. The test is 95%
sensitive and is best done in patients with generalized
MG. The specificity is 50% because other nerve dis-
orders may produce a false-positive result. This test
typically is used to assess response to therapy.
The Tensilon (edrophonium) test is fairly simple
to perform: 0.1 to 0.2 mg of Tensilon is given in-
travenously initially to determine if symptoms im-
prove. If there is no response, an additional 2 mg of
the drug is administered. If there is no symptom
improvement, 9 mg is given. The onset of action is
usually within 30 seconds and lasts approximately
5 minutes. The gradual increase in edrophonium dose
is meant to avoid a cholinergic crisis. This test is least
sensitive in patients with ocular symptoms only, but
is 95% sensitive in the general MG population.
Observer variability occurs. A test has its maximum
sensitivity when the patient is at his or her weakest.
To evaluate better equivocal or weak test results,
neostigmine (Prostigmin), a cholinesterase inhibitor,
may be given to prolong the response.
The binding, blocking, and modulating antibody
test is a radioimmunoassay using radioactive iodine–
tagged a-bungarotoxin, which binds specifically and
irreversibly to the ACh-R antibody. The test is 80%
to 90% sensitive. The modulating or blocking anti-
bodies are positive in 5% of patients who are binding
antibody negative [14]. The 10% to 20% who are
antibody negative still have a circulating immune
complex that affects the motor nerve end plate and
can cause symptoms on passive transfer of serum
[15]. Among patients with ocular symptoms, 50% are
antibody positive. The test is the most specific of the
tests used, although patients with amyotrophic lateral
sclerosis, biliary cirrhosis, tardive dyskinesia, thyroid-
itis, thymoma without MG, and lupus erythematosus
can have false-positive antibody tests [16]. The
antibody levels do not correlate with the symptoms
or the effectiveness of therapy [17,18]. Anti–striated
muscle antibodies are associated with patients who
have a thymoma [19]. Seronegative patients are more
likely female and more frequently have either ocular
and bulbar symptoms only or severe bulbar, neck,
and respiratory symptoms. As a group, these patients
are less likely to respond to thymectomy [20]. A
relatively rare group of ACh-R antibody–negative
MG patients express antibodies against the muscle
receptor tyrosine kinase [21]. These patients are much
less likely to benefit from thymectomy because they
are less likely to have thymic pathology.
Box 2 lists the other potential diseases that may be
confused with myasthenia gravis. The first, congeni-
tal myasthenic syndrome, is not a single disease, but
rather a group of several rare congenital myasthenic
syndromes associated with weakness in neonates and
infants [22]. Typically, there is a family history of the
abnormality, there is no ACh-R antibody present, and
the Tensilon test is negative. These syndromes
represent a host of synaptic abnormalities that result
in weakness [23].
MG syndrome can develop in a small percentage
(<1%) of patients treated with penicillamine. Fre-
quently the syndrome begins with ocular symptoms
and can progress to generalized myasthenia. The
Tensilon test, EMG, and the ACh-R antibody tests are
positive. Organophosphates, procainamide, quinines,
aminoglycosides, and metoclopramide all can cause
MG-type symptoms. The symptoms usually improve
with discontinuation of the drugs.
Botulism also can result in ocular and bulbar
weakness. In botulism, the pupils do not respond to
light or accommodation. With repeated nerve stimu-
lation, EMG shows an increased response, rather
than the decrease seen with MG.
Brainstem pathology, such as tumors or aneu-
rysms, can cause dysfunction in the cranial nerves.
On physical examination, evaluation of cranial
nerves III through VI may prove beneficial. The loss
of a corneal reflex is not a finding in MG, whereas
it is in brainstem lesions. MRI of the brain and skull
base may be beneficial to differentiate these lesions

preoperative preparation of mg patient 291
from MG. Generalized symptoms of myasthenia re-
duce the likelihood of brainstem pathology.
Kearns-Sayre syndrome is a mitochondrial disor-
der that presents in children as ptosis and ophthalmo-
plegia and may continue to progress to generalized
muscle weakness. There is associated retinal degen-
eration and progressive cerebellar disease. Muscle
biopsy specimens also may help to differentiate this
disease from MG.
Thyroid disease may coexist with MG and may be
difficult to differentiate from it. When exophthalmos
is present, the eye disease is more likely due to
Graves’ disease than MG. The presence of MG
warrants performing thyroid function studies.
Amyotrophic lateral sclerosis can cause progres-
sive muscular weakness, including the bulbar mus-
cles. The peripheral nature of the weakness and the
associated hyperreflexia and Babinski sign can help
to differentiate this disease from MG. Amyotrophic
lateral sclerosis can have a positive Tensilon test and
ACh-R antibody.
Psychoneuroses and depression may simulate or
may appear similar to MG. With psychoneuroses and
depression, the fatigue is greater in the morning, in
contrast to the worsening fatigue through the day with
MG. Provocative testing also may help to differentiate
MG from psychoneuroses and depression.
Eaton-Lambert syndrome may have similar char-
acteristics to MG and is associated with small cell
lung cancer and Hodgkin’s disease in 85% of cases.
Pelvic muscle and truncal weakness is more fre-
quently an early symptom, making it difficult for
patients to stand up out of a chair. Bulbar and ocular
symptoms are rare; however, ptosis may be seen. The
shoulders are less frequently involved with Eaton-
Lambert syndrome. Eaton-Lambert symptoms are
more pronounced in the morning and seem to
improve through the day; there also may be asso-
ciated autonomic abnormalities, such as dry mouth.
EMG shows an increased response rather than the
decreased response in MG. Autoantibodies to the
P/Q-type calcium channels are found in more than
95% of patients with Eaton-Lambert syndrome.
These autoantibodies also may be found in patients
with MG, but are relatively rare (<5% of patients).
After reviewing the history and physical exami-
nation findings and the provocative testing results,
excluding other potential diseases, the degree of dis-
ease or the Myasthenia Gravis Foundation Associa-
tion classification is determined (see Box 2). The
neurologist chooses medication that minimizes the
symptoms with minimal side effects. Cholinesterase
inhibitors or anticholinesterases increase the synaptic
cleft ACh. Prolonged use may enhance the destruc-
tive effect of MG [24,25]. Medications include
neostigmine and pyridostigmine (Mestinon). Pyrido-
stigmine has a longer half-life and usually is started at
60 mg three times per day; it may be increased to
1500 mg/d. After the drug is initiated, most patients
experience symptomatic improvement. The improve-
ment is short-lived, and it is beneficial to have a
second agent to treat the patient in preparation for
surgery. The side effects are diarrhea, rhinorrhea,
nausea, increased salivation and tears, bronchorrhea,
and abdominal pain. Excessive dosing may result in a
cholinergic crisis, which is characterized by myosis,
paralysis, salivation, tearing, bronchorrhea, diaphore-
sis, and wheezing. Progressive weakness associated
with anticholinesterases may be difficult to differen-
tiate from undertreatment or overtreatment of MG in
the postoperative period.
Corticosteroids are used at doses of 50 to 100 mg/d
of prednisone (1–2 mg/kg/d for children). Symp-
toms may worsen significantly 4 to 8 days after
corticosteroids are started, prompting some physi-
cians to admit patients for steroid initiation. Approxi-
mately 3 to 6 weeks are required for symptoms to
improve. When symptom management is optimized
(usually 3–6 months), the dose may be adjusted for
lifelong use. Side effects of steroid use include
cataracts, cushingoid features, aseptic necrosis of the
femoral heads, obesity, psychosis, hypertension, glu-
cose intolerance, osteoporosis, and gastrointestinal
ulceration. Prednisone doses of less than 10 mg/d
may reduce the likelihood of complications before a
median sternotomy is performed, although the pres-
ence of steroids may serve to reduce poststernotomy
complications [26].
Immunosuppressive medications also may be
beneficial and are used in a significant percentage
of patients. Azathioprine (Imuran) is used frequently
to decrease steroid doses or to benefit patients who
are incompletely treated with steroids or unable to
tolerate steroids. More specifically, immunosuppres-
sive therapy attempts to target the T cells. Azathio-
prine most frequently is used lifelong, and its onset
effect takes approximately 3 to 12 months. The dose
is started at 50 mg/d for the first week, then increased
2 to 3 mg/kg/d until the desired effect is achieved.
Nearly half of patients show some improvement.
Approximately 10% of patients have flulike reaction,
and there is associated bone marrow suppression,
nausea, vomiting, and biliary stasis.
Cyclosporine is an alternative immunosuppressive
agent that inhibits interleukin-2 by helper T cell. Cy-
closporine seems to have a more rapid response than
azathioprine; the dose is 5 mg/kg/d. Side effects in-
clude hypertension, hirsutism, and renal dysfunction.

Fig. 1. CT scan of patient who presented with myasthenia
and was found to have a large, malignant thymoma.
kernstine292
Intravenous immunoglobulin improves symptoms
for periods of weeks to months. Patients are given a
daily dose of 400 mg/kg/d intravenously over a 5-day
period. It is generally well tolerated. This medication
may be useful in controlling symptoms in children
with more advanced disease before thymectomy.
Plasmapheresis may be performed removing 1 to
3 L of plasma each session every other day for three
to five sessions. The goal is to achieve the desired
effect after the plasmapheresis has been performed.
The improvement may last several weeks and may
occur in antibody-positive or antibody-negative pa-
tients. Plasmapheresis seems to be significantly effec-
tive in patients with respiratory dysfunction (with
vital capacity <2 L) and patients who may be on a
ventilator [27,28] and is superior to anticholines-
terase medication [29,30]. Patients with advanced
disease who receive preoperative plasma exchange
required less long-term ventilation and shorter ICU
stays [31]. Plasmapheresis may allow the discon-
tinuation of anticholinesterase drugs preoperatively,
reducing the bronchorrhea that is associated with
anticholinesterase drugs.
Other diseases may coexist with MG and should
be screened preoperatively. Associated thyroid dis-
ease may exist in 5% to 10% of MG patients. Pa-
tients may be hypothyroid or hyperthyroid, and the
associated thyroid disease may worsen the symp-
toms of myasthenia. It is recommended that thyroid
function tests be performed routinely before surgi-
cally treating patients with MG. Other autoimmune
diseases include rheumatoid arthritis and systemic
lupus erythematosus; measuring a screening serum
antinuclear antibody and rheumatoid factor may be
beneficial as well.
Thymic hyperplasia is found in 70% and thymic
atrophy in 20% of surgically resected patients [32].
Thymomas are found in approximately 10% to 20%
of patients with MG. These tumors are rare in patients
younger than age 20; the incidence is greatest in older
men. Patients with thymomas are less likely to bene-
fit from thymectomy. In the initial evaluation and
preoperatively, patients should have a screening chest
CT scan for thymoma (Fig. 1), which is approxi-
mately 88% sensitive [33]. There is no evidence that
MRI is superior to CT in screening for thymomas.
Before surgery, assessing the areas of potential
organ dysfunction may be of significant benefit. In-
spiratory and expiratory muscles may be dysfunc-
tional [34,35]. Spirometry may show a normal total
lung capacity, but a low vital capacity with a normal-
to-high residual volume [36]. Patients who are at risk
for prolonged ventilatory support include patients
with advanced disease; a Myasthenia Gravis Founda-
tion classification II or higher (see Box 2); duration of
MG for more than 6 years; history of steroid require-
ment; and a prior history of MG-induced respiratory
insufficiency, vital capacity less than 2.9 L, pyrido-
stigmine dose greater than 750 mg/d 48 hours before
surgery, or maximal expiratory force less than 40 to
50 cm H2O [37–40]. The upper airway may be af-
fected or obstructed by bulbar muscular dysfunction
or potential mediastinal thymic compression from an
anterior thymic mass [41]. There may be a risk of
airway obstruction at the time of intubation. A flow-
volume loop may be beneficial in evaluating these
patients. If this is present, the patient may need to be
intubated using an awake intubation technique of lo-
cal anesthesia and mild sedation.
Patients with MG also may have associated car-
diac dysfunction [42]. They may have conduction de-
fects and arrhythmias, including sinus bradycardia,
premature ventricular contractions, and atrial fibrilla-
tion. There also may be some primary left ventricular
filling dysfunction—a condition that seems to be
more frequent in patients with thymoma [43,44]. A
preoperative ECG and possibly an echocardiogram
may be warranted, particularly if symptoms and signs
of cardiac dysfunction are present.
In preparing a patient for surgery, the goals are
to suppress the immune response, decrease the cir-
culating antibodies, and optimize the neuromuscu-
lar transmission. The anticholinesterase medication
should be minimized over several weeks before sur-
gery to reduce the likelihood for postoperative bron-
chorrhea and rhinorrhea, while maintaining symptom
control. On the morning of surgery, a half dose of
anticholinesterase inhibitor should be given to pa-
tients with mild symptoms, and a full dose should be
given to patients with moderate-to-severe symptoms

preoperative preparation of mg patient 293
[45]. Steroids should be minimized to reduce the
likelihood of postoperative wound healing problems,
infection, and pulmonary complications.
From the anesthetic standpoint, some inhalation
agents should be avoided in MG patients [46,47].
Propofol has been used and does not seem to affect
neuromuscular transmission [48]. Depolarizing mus-
cle relaxants, such as succinylcholine, are less likely
to be effective. Preoperative plasmapheresis may de-
lay significantly the reversal of succinylcholine. The
nondepolarizing agents, such as atracurium, are not
dependent on plasmacholinesterases and are better
agents [49].
The role of thymectomy in the management of
MG is controversial. Although there is long-standing
evidence that the procedure is beneficial, the timing
of surgery and the surgical approach are controver-
sial. Some authors believe that thymectomy is valu-
able as an initial form of therapy because it reduces
the likelihood for long-term sequelae of MG. Other
authors believe that thymectomy should be reserved
for patients who fail medical management or have
excessive medication-related side effects. Thymec-
tomy is rarely, if ever, an emergent procedure. The
procedure has a mortality of less than 1%, although
morbidity may be substantial in the most severely
affected patients; 22% of patients with preoperative
respiratory insufficiency may require long-term me-
chanical ventilation [50].
In a meta-analysis of 21 nonthymomatous MG
cohorts from 1953 to 1998, patients who received
thymectomy were 2.1 times more likely to develop
treatment-free remission, 1.6 times more likely to
become asymptomatic, and 1.7 times more likely to
have improved symptoms compared with patients
who did not undergo surgery [51]. Median sterno-
tomy is the most frequently used approach, but other
techniques, including the transcervical thoracoscopic
and robotic approaches, have been described. The
patient selection for each of these approaches has not
been completely elucidated.
Summary
All patients who are to undergo a thymectomy
should be evaluated thoroughly by a neurologist—
ideally one with special training and interest in the
diagnosis and management of MG. Confirmatory
tests to diagnose MG and other potential diseases
should be reviewed. The antibody test seems to be
most specific, but there are rare cases of other dis-
eases that are ACh-R antibody positive. In 10% of
MG patients, serology is negative, and other tests are
necessary to confirm the diagnosis. All patients
should undergo a contrast-enhanced high-resolution
CT scan with 5- to 8-mm slices because thymoma or
thymic carcinoma may be present. Pulmonary func-
tion tests, including vital capacity, forced expiratory
volume, maximal expiratory force, arterial blood gas,
and a flow-volume loop, should be performed. Exer-
cise testing to evaluate for hypoxia and hypotension
with exercise and ambulation also may be appro-
priate. A thorough assessment for cardiac dysfunc-
tion, including echocardiography, nuclear medicine
studies, or a formal cardiology evaluation, may be
beneficial. Because MG is a complex autoimmune
disease, preoperative blood tests should include thy-
roid function testing, antinuclear antibody, and rheu-
matoid factor in addition to routine preoperative
studies. Plasmapheresis or intravenous immuno-
globulin should be considered for patients with
advanced disease, bulbar symptoms, or poor pulmo-
nary function. Given these guidelines, careful selec-
tion of candidates for surgery should optimize the
long-term results for patients with MG.
References
[1] Morton LT, Moore RJ. A chronology of medicine and
related sciences. Aldershot (UK)7 Scholar Press; 1997.
[2] Talbott JH. A biographical history of medicine, ex-
cerpts and essays on the men and their work. New
York7 Grune & Stratton; 1970.
[3] Blalock A, Mason MF, Morgan HJ, et al. Myasthenia
gravis and tumors of the thymic region. Ann Surg
1939;110:544–61.
[4] Blalock A, Harvey AM, Ford FF, et al. The treatment
of myasthenia gravis by removal of the thymus gland.
JAMA 1941;117:1529–33.
[5] Jaretzki A, Steinglass KM, Sonett JR. Thymectomy in
the management of myasthenia gravis. Semin Neurol
2004;24:49–62.
[6] Jaretzki 3rd A, Penn AS, Younger DS, et al.
‘‘Maximal’’ thymectomy for myasthenia gravis: re-
sults. J Thorac Cardiovasc Surg 1988;95:747–57.
[7] Barohn RJ, McIntire D, Herbelin L, Wolfe GI, Na-
tions S, Bryan WW. Reliability testing of the quanti-
tative myasthenia gravis score. Ann N Y Acad Sci
1998;841:769–72.
[8] Graus YM, DeBaets MH. Myasthenia gravis: an auto-
immune response against the acetylcholine receptor.
Immunol Res 1993;12:78–100.
[9] Milani M, Ostlie N, Wang W, Conti-Fine BM. T cells
and cytokines in the pathogenesis of acquired myas-
thenia gravis. Ann N Y Acad Sci 2003;998:284–307.
[10] Fambrough DM, Drachman DB, Satyamurti S. Neuro-
muscular junction in myasthenia gravis: decreased
acetylcholine receptors. Science 1973;182:293–5.
kernstine294
[11] Paton WDM, Waud DR. The margin of safety of neu-
romuscular transmission. J Physiol (Lond) 1967;191:
59–90.
[12] Woolf AL. Morphology of the myasthenic neuro-
muscular junction. Ann N YAcad Sci 1966;135:35–9.
[13] http://www.myasthenia.org/information/summary.htm.
Accessed November 12, 2004.
[14] Ciafaloni E, Sanders DB. Advances in myasthenia
gravis. Curr Neurol Neurosci Rep 2002;2:89–95.
[15] Drachman DB. Myasthenia gravis. N Engl J Med 1994;
330:1797–810.
[16] Abbott RJ, Holden D, Currie S. False positive anti-
acetylcholine receptor antibodies in motor neurone dis-
ease. Lancet 1986;1:906–7.
[17] Howard Jr FM, Lennon VA, Finley J, Matsumoto J,
Elveback LR. Clinical correlations of antibodies that
bind, block, or modulate human acetylcholine recep-
tors in myasthenia gravis. Ann N Y Acad Sci 1987;
505:526–38.
[18] Olanow CW, Wechsler AS, Roses AD. A prospective
study of thymectomy and serum acetylcholine receptor
antibodies in myasthenia gravis. Ann Surg 1982;196:
113–21.
[19] Lanska DJ. Diagnosis of thymoma in myasthenics
using anti-striated muscle antibodies: predictive value
and gain in diagnostic certainty. Neurology 1991;41:
520–4.
[20] Verma PK, Oger JJ. Seronegative generalized myas-
thenia gravis: low frequency of thymic pathology.
Neurology 1992;42:586–9.
[21] McConville J, Farrugia ME, Beeson D, et al. Detec-
tion and characterization of MuSK antibodies in
seronegative myasthenia gravis. Ann Neurol 2004;55:
580–4.
[22] Harper CM. Congenital myasthenic syndromes. Semin
Neurol 2004;24:111–23.
[23] Engel AG, Ohno K, Sine SM. Congenital myasthenic
syndromes: a diverse array of molecular targets.
J Neurocytol 2003;32:1017–37.
[24] Engel AG, Lambert EH, Santa T. Study of long-term
anticholinesterase therapy: effects on neuro-muscular
transmission and on motor endplate line structure.
Neurology 1973;23:1273–81.
[25] Chang CC, Chen TF, Chuang ST. Influence of
chronic neostigmine treatment on the number of ace-
tylcholine receptors and the release of acetylcholine
from the rat diaphragm. J Physiol (Lond) 1977;230:
613–8.
[26] Zielinski M, Kuzdzal J, Staniec B, et al. Safety for
preoperative use of steroids for transsternal thymec-
tomy in myasthenia gravis. Eur J Cardiothorac Surg
2004;26:407–11.
[27] Gracey DR, Howard Jr FM, Divertie MB. Plasmaphe-
resis in the treatment of ventilator-dependent myasthe-
nia gravis patients: report of four cases. Chest 1984;
85:739–43.
[28] Spence PA, Morin JE, Katz M. Role of plasmapherisis
in preparing myasthenic patients for thymcetomy:
initial results. Can J Surg 1984;27:303–5.
[29] Goti P, Spinelli A, Marconi G, et al. Comparative
effects of plasma exchange and pyridostigmine on
respiratory muscle strength and breathing pattern in
patients with myasthenia gravis. Thorax 1995;50:
1080–6.
[30] Cumming WJK, Hudgson P. The role of plasmaphe-
resis in preparing patients with myasthenia for thy-
mectomy. Muscle Nerve 1986;9:S155–8.
[31] d’Empaire G, Hoaglin DC, Perlo VP, et al. Effect of
prethymectomy plasma exchange on postoperative res-
piratory function in myasthenia gravis. J Thorac Car-
diovasc Surg 1985;89:592–6.
[32] Castleman B. The pathology of the thymus in myas-
thenia gravis. Ann N Y Acad Sci 1966;135:496–503.
[33] Pirronti T, Rinaldi P, Batocchi AP, Evoli A, Di
Schino C, Marano P. Thymic lesions and myasthe-
nia gravis: diagnosis based on mediastinal imaging
and pathological findings. Acta Radiol 2002;43:
380–4.
[34] Mier-Jedrzejowicz AK, Brophy C, Green M. Respira-
tory muscle function in myasthenia gravis. Am Rev
Respir Dis 1988;138:867–73.
[35] Book WJ, Abel M, Eisenkraft JB. Anesthesia and
neuromuscular diseases. Anesth Clin North Am 1996;
14:515–42.
[36] Zulueta JJ, Fanburg BL. Respiratory dysfunction in
myasthenia gravis. Clin Chest Med 1994;15:683–91.
[37] Leventhal SR, Orkin FK, Hirsh RA. Prediction of the
need for postoperative mechanical ventilation in
myasthenia gravis. Anesthesiology 1980;53:26–30.
[38] Eisenkraft JB, Papatestas AE, Kahn CH, et al.
Predicting the need for postoperative mechanical ven-
tilation in myasthenia gravis. Anesthesiology 1986;
65:79–82.
[39] Gracey DR, Divertie MB, Howard FM, et al. Post-
operative respiratory care after transsternal thymec-
tomy in myasthenia gravis: a 3-year experience in
53 patients. Chest 1984;86:67–71.
[40] Younger DS, Braun NMT, Jaretzki III A, Penn AS,
Lovelace AE. Myasthenia gravis: determinants for
independent ventilation after transsternal thymectomy.
Neurology 1984;34:336–40.
[41] Putman MT, Wise RA. Myasthenia gravis and upper
airway obstruction. Chest 1996;109:400–4.
[42] Gibson TC. The heart in myasthenia gravis. Am Heart
J 1975;90:389–96.
[43] Johannessen KA, Mygland A, Gilhus NE, et al. Left
ventricular function in myasthenia gravis. Am J Car-
diol 1992;69:129–32.
[44] Hofstad H, Ohm O-J, Mork SJ, et al. Heart disease
in myasthenia gravis. Acta Neurol Scand 1984;70:
176–84.
[45] Girnar DS, Weinreich AI. Anesthesia for transcervical
thymectomy in myasthenia gravis. Anesth Analg 1976;
55:13–7.
[46] Nissson E, Muller K. Neuromuscular effects of
isoflurane in patients with myasthenia gravis. Acta
Anaesthesiol Scand 1990;34:126–31.
[47] Saitoh Y, Toyooka H, Amaha K. Recoveries of post-

preoperative preparation of mg patient 295
tetanic twitch and train of four responses after ad-
ministration of vecuronium with different inhalation
anesthetics and neurosept anaesthesia. Br J Anaesth
1993;70:402–4.
[48] Book WJ, Abel M, Eisenkraft JB. Anesthesia and neu-
romuscular diseases. Anesth Clin North Am 1996;14:
515–42.
[49] Bell CF, Florence AM, Hunter JM, et al. Atracurium
in the myasthenic patient. Anaesthesia 1984;39:961–8.
[50] Kas J, Kiss D, Simon V, Svastics E, Major L, Szobor A.
Decade-long experience with surgical therapy of myas-
thenia gravis: early complications of 324 transsternal
thymectomies. Ann Thorac Surg 2001;72:1691–7.
[51] Gronseth GS, Barohn RJ. Practice parameter: thy-
mectomy for autoimmune myasthenia gravis (an
evidence-based review): report of the Quality Stan-
dards Subcommittee of the American Academy of
Neurology. Neurology 2000;55:7–15.

Thorac Surg Clin
Preoperative Pulmonary Evaluation of the
Thoracic Surgical Patient
Aditya K. Kaza, MD, John D. Mitchell, MD*
Section of General Thoracic Surgery, Division of Cardiothoracic Surgery, University of Colorado Health Sciences Center,
4200 East 9th Avenue, C-310, Denver, CO 80262, USA
Surgery remains the mainstay of therapy for early-
stage non–small lung cancer, with approximately
45,000 cases of early-stage disease (stages I, II, and
select IIIA) diagnosed annually. Many of these pa-
tients have poor underlying pulmonary function, in
large part resulting from long-term tobacco abuse.
It is the responsibility of the thoracic surgeon to as-
sess accurately the pulmonary function of a poten-
tially operable patient at the time of the preoperative
evaluation. This assessment provides an objective risk
profile associated with the planned pulmonary resec-
tion for the patient and family, minimizes morbidity
and mortality, and in some cases leads the surgeon to
recommend alternative therapies.
General considerations
Several questions should be asked in the general
pulmonary assessment of a patient being considered
for lung resection surgery. Careful appraisal of prior
history and pertinent review of systems (Box 1) often
can predict the objective results obtained in sub-
sequent pulmonary function testing.
Is the patient currently smoking? Active use of
tobacco at the time of surgery predisposes patients to
a variety of postoperative pulmonary complications
[1,2], usually through increased production and
reduced clearance of sputum in the perioperative
1547-4127/05/$ – see front matter D 2005 Elsevier Inc. All rights
doi:10.1016/j.thorsurg.2005.02.004
* Corresponding author.
E-mail address: [email protected]
(J.D. Mitchell).
period. Significant atelectasis, pneumonia, or respi-
ratory insufficiency requiring intubation may result.
Patients should be counseled regarding the benefits
of abstinence from smoking as early as possible
before the procedure. A long prior smoking history
may suggest significant occult parenchymal disease
(chronic obstructive pulmonary disease), but is asso-
ciated with increased risk even in the absence of such
findings [3].
Does the patient have an occupational or travel
history that would predispose him or her to certain
pulmonary disorders? A variety of industrial and
environmental exposures, both organic and inorganic,
can lead to the insidious development of interstitial
lung disease and reduced pulmonary function [4].
Common environmental agents include silica, asbes-
tos, beryllium, and animal/bird products (farmer’s
lung or variants). A history of travel to areas endemic
to certain fungal infections (Coccidioides or Histo-
plasma) also may be relevant.
What is the activity level of the patient? Patients
with suboptimal performance on objective exercise
testing are at increased risk for perioperative cardio-
pulmonary complications [5–8]. In addition, self-
reported poor exercise tolerance has been shown to be
associated reliably with increased postoperative risk
[9]. Pulmonary rehabilitation, although not always
practical, may improve exercise tolerance dramati-
cally and is strongly advocated before lung trans-
plantation or lung volume reduction surgery [10,11].
Does the patient have a history of prior or active
pulmonary infection? A history of recurrent pulmo-
nary infections may suggest impaired mucociliary
clearance, airway obstruction, or localized bronchiec-
15 (2005) 297 – 304
reserved.
thoracic.theclinics.com

Box 1. General considerations in thepulmonary resection candidate
Smoking historyOccupational and travel historyExercise tolerancePrior history of:
Recurrent pulmonary infections
Recognized pulmonary airway/paren-chymal disease
Cardiac disease
Pulmonary or cardiac surgery
kaza & mitchell298
tasis. Successful treatment of active infection before
surgical resection is advised, but not always feasible
in the setting of a postobstructive infectious process.
Is an underlying pulmonary parenchymal disorder
present? The concomitant presence of significant
obstructive, interstitial, or infectious lung disease can
have a major impact on the patient’s functional status
and the conduct of the proposed operation. In addi-
tion, certain pulmonary disorders (particularly inter-
stitial lung disease) may be associated with a poor
prognosis, which may influence the degree of risk a
patient maywish to assume in the perioperative period.
Is cardiac disease present? Many cardiac and
pulmonary disorders have common etiologic factors.
The presence of significant ischemic or valvular heart
disease can have an impact on postoperative pulmo-
nary complications. Preexisting right ventricular
dysfunction has been shown to be a risk factor for
complications after pulmonary resection [12].
Has the patient had prior thoracic surgery? A
prior history of pulmonary resection or significant
intrathoracic procedure can have a significant impact
on the risk profile at the time of subsequent surgery.
Spirometry
Spirometry is a simple, inexpensive, readily
available test and remains the starting point in the
evaluation of a patient for proposed pulmonary
resection. Spirometry should be performed with the
patient in stable condition, with and without the
use of inhaled bronchodilators. A bronchodilator re-
sponse greater than 15% is considered significant and
indicates a component of reactive airways disease.
The forced expiratory volume in 1 second (FEV1)
is the most commonly used parameter from spiro-
metric testing for pulmonary risk assessment. Sev-
eral large studies in the past have suggested FEV1
criteria for safe pulmonary resection, including an
FEV1 greater than 1.5 L for a proposed lobectomy
and greater than 2 L for a pneumonectomy [13–15].
These criteria have been adopted as guidelines by at
least one major thoracic society, with no further
testing needed to ensure operability [16]. The
difficulty with these absolute values is that they do
not take into account size or gender of the particular
patient, producing bias against resection in smaller
individuals. For this reason, most practitioners use
or express measured FEV1 as a percentage of the
predicted value for the patient’s gender, height, and
weight. In this fashion, investigators have suggested
an FEV1 greater than 80% of the predicted value is
associated with a low risk of perioperative complica-
tions after major lung resection, and no further testing
is needed (Fig. 1) [17]. Other parameters investigated
include maximum voluntary ventilation (MVV) and
FEV25–75%, with a MVV less than 40% predicted or
a FEV25–75% of 0.6 to 1 L indicative of a marginal
candidate for lobar resection [18].
Diffusion capacity
The diffusion capacity in the lung for carbon
monoxide (Dlco) was found to be the most
important predictor of mortality and was the sole
predictor of postoperative pulmonary complications
in a retrospective review of 237 patients published by
Ferguson et al [19] in 1988. In this study, a Dlco
less than 60% of predicted was associated with
increased mortality. The importance of Dlco in risk
assessment before lung resection has been substanti-
ated by further reports, with little interplay between
Dlco and either FEV1 or maximum oxygen con-
sumption (Vo2max) [20,21].
Arterial blood gas analysis
The presence of resting hypercapnea, defined as a
Pco2 greater than 45 mm Hg on room air, has long
been described as a relative contraindication to lung
resection [14,18]. Other reports dispute this assertion,
however, and show equivalent outcomes above and
below this value [22–24].
Prediction of postoperative function
Most patients presenting for lung surgery are
likely to have reduced lung function, and it is the
responsibility of the surgeon to ensure adequate
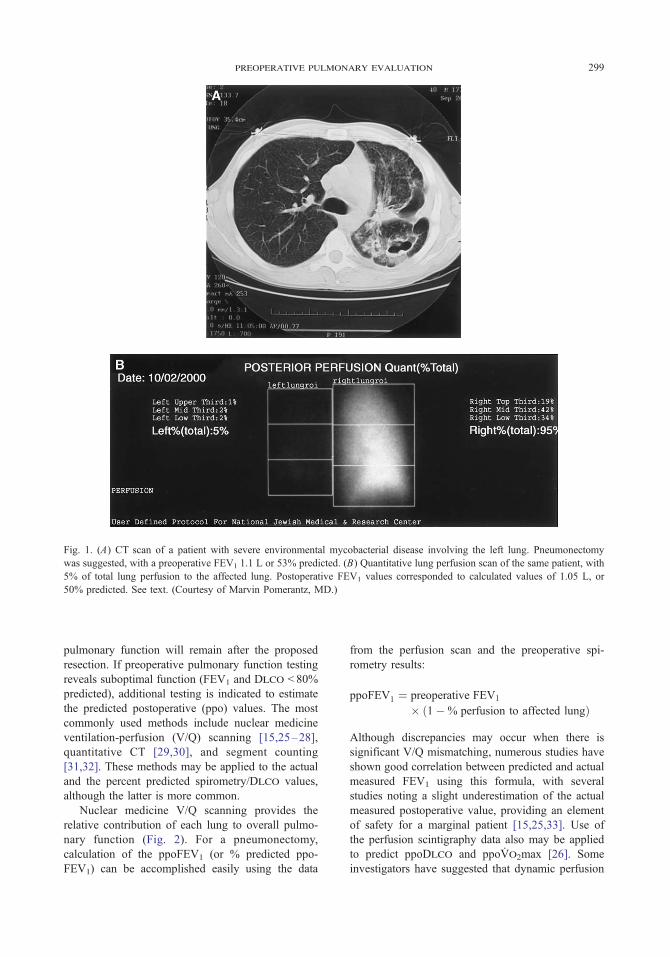
Fig. 1. (A) CT scan of a patient with severe environmental mycobacterial disease involving the left lung. Pneumonectomy
was suggested, with a preoperative FEV1 1.1 L or 53% predicted. (B) Quantitative lung perfusion scan of the same patient, with
5% of total lung perfusion to the affected lung. Postoperative FEV1 values corresponded to calculated values of 1.05 L, or
50% predicted. See text. (Courtesy of Marvin Pomerantz, MD.)
preoperative pulmonary evaluation 299
pulmonary function will remain after the proposed
resection. If preoperative pulmonary function testing
reveals suboptimal function (FEV1 and Dlco < 80%
predicted), additional testing is indicated to estimate
the predicted postoperative (ppo) values. The most
commonly used methods include nuclear medicine
ventilation-perfusion (V/Q) scanning [15,25–28],
quantitative CT [29,30], and segment counting
[31,32]. These methods may be applied to the actual
and the percent predicted spirometry/Dlco values,
although the latter is more common.
Nuclear medicine V/Q scanning provides the
relative contribution of each lung to overall pulmo-
nary function (Fig. 2). For a pneumonectomy,
calculation of the ppoFEV1 (or % predicted ppo-
FEV1) can be accomplished easily using the data
from the perfusion scan and the preoperative spi-
rometry results:
ppoFEV1 ¼ preoperative FEV1
� 1�% perfusion to affected lungð Þ
Although discrepancies may occur when there is
significant V/Q mismatching, numerous studies have
shown good correlation between predicted and actual
measured FEV1 using this formula, with several
studies noting a slight underestimation of the actual
measured postoperative value, providing an element
of safety for a marginal patient [15,25,33]. Use of
the perfusion scintigraphy data also may be applied
to predict ppoDlco and ppoVo2max [26]. Some
investigators have suggested that dynamic perfusion

SpirometryDLCO
FEV1 > 80% predictedDLCO > 80% predicted
Offer Surgery
FEV1 < 80% predictedDLCO < 80% predicted
Estimation ofPostoperative Function
(ppo)* ppoFEV1 >40% predicted ppoDLCO >40-50% predicted
ppoFEV1 <40% predicted ppoDLCO <40-50% predicted
Exercise Study
Defer Surgery
VO2max >15 ml/kg/min
VO2max <15 ml/kg/minppoVO2max >10 ml/kg/min
ppoVO2max <10 ml/kg/min
ProposedLung
Resection
Fig. 2. Algorithm for preoperative pulmonary evaluation. *Estimated with quantitative perfusion scan, CT scan, or seg-
ment counting.
kaza & mitchell300
MR imaging techniques may be a feasible alternative
to V/Q scintigraphy [34].
The perfusion study also may be used to predict
function after lobectomy, as described by Wernly
et al [15]:
ppoFEV1 ¼ preoperative FEV1 � preoperative FEV1
�% perfusion to affected lung
� # resected segments
# segments in affected lung
An alternative method of calculating ppoFEV1 with-
out the use of a quantitative perfusion study involves
simply accounting for the number of resected seg-
ments as a percentage of the total number of segments
in both lungs, as described by Juhl and Frost [31].
With 19 lung segments, each segment accounts for
roughly 5.26% of the overall lung function:
ppoFEV1 ¼ preoperative FEV1
� ð1� ½# segments resected
� 5:26�=100Þ
Simple segment counting obviates the need for
expensive nuclear medicine testing and has been
adopted as the preferred method of calculating
postoperative spirometry values after lobectomy by
at least one major thoracic society [16]. Although
segment counting has been suggested to be as
accurate as V/Q scintigraphy [35], it does not take
into account the functional differences between vary-
ing segments, which may prove important in mar-

preoperative pulmonary evaluation 301
ginal patients with heterogeneous patterns of lung
disease, such as emphysema. Perhaps to account for
this factor, one group suggested adding 250 mL of
volume to the ppoFEV1 calculated by segment count-
ing, to obtain a more reliable estimation of post-
operative function [32].
At least one study has compared scintigraphy,
segment counting, and quantitative CT in predicting
postoperative pulmonary function [36]. In this study,
four parameters were assessed: FEV1, FVC, Dlco,
and Vo2max. Although scintigraphy and CT were
found to be useful, perfusion scintigraphy was noted
to be the most accurate.
Numerous studies have shown ppoFEV1 to be a
predictor of perioperative risk. Historically a cutoff of
ppoFEV1 less than 800 mL was used as a determinant
of unresectability [37]. More recent studies suggest
that morbidity and mortality are significantly in-
creased if the ppoFEV1 is less 40% [22,38–40].
Similarly, ppoDlco has been shown to be strongly
predictive of complications and death when the value
is less than 40% [18,21]. At least one group has
suggested the product of ppoFEV1 and ppoDlco
(predicted postoperative product) less than 1650 may
be an even more sensitive indicator of postoperative
mortality [33].
Exercise testing
Patients considered at high risk for perioperative
complications on the basis of standard spirometry
testing and calculation of postoperative function
should undergo exercise testing. The purpose of ex-
ercise testing is to identify some patients deemed
high risk but still able to tolerate resection with ac-
ceptable morbidity and mortality.
The easiest form of exercise testing is stair
climbing, with the height climbed inversely related
to the frequency of postoperative complications
[41,42]. Investigators have found increased morbid-
ity and mortality when less than 2 flights [43,44],
3 flights [45,46], 12 m [47], or 44 steps [48] are
climbed. One study found the height climbed to be
the sole predictor of morbidity through multivariate
analysis [47]. Others have shown correlation with the
patient’s Vo2max [49].
The 6-minute walk test was modified from the
original 12-minute test and provides objective evi-
dence of the patient’s exercise function [50]. The test,
usually performed in a hallway over a preset distance,
measures the distance a patient can walk quickly on a
hard, flat surface in 6 minutes. The test is self-paced
and does not reflect maximal exercise capacity. Some
investigators believe that because most activities of
daily living are performed in a submaximal exercise
environment, the test is a better assessment of the
patient’s general exercise tolerance. Holden et al [48]
found an achieved distance of greater than 1000 feet
to be associated with improved surgical outcomes
after lung resection. The 6-minute walk test is
commonly used in lung transplantation evaluations
and was used to exclude patients with severely
reduced exercise capacity after pulmonary rehabili-
tation in the National Emphysema Treatment Trial
[10]. A variation of the 6-minute walk test is the
shuttle walk, in which patients ambulate between two
cones placed 10 m apart. The walking speed, paced
by an audio signal, is increased each minute until the
patient is unable to continue. The shuttle walk more
closely correlates with Vo2max, with one study
showing that inability to complete 25 shuttles (250 m
[about 820 ft]) suggested a Vo2max less than 10 mL/
kg/min [51].
Where available, formal cardiopulmonary exer-
cise testing should be pursued when preliminary
spirometry and split function studies suggest the
patient is at increased risk of perioperative compli-
cations. The test usually is performed with incre-
mental work performed on a treadmill or bicycle
ergometer, measuring oxygen saturation and exhaled
gases to determine Vo2, Vo2max, carbon dioxide
output, and minute ventilation. The most commonly
used parameter measured with cardiopulmonary
exercise testing is Vo2max, which denotes a plateau
above which further increases in work do not result in
greater oxygen consumption. This parameter differs
slightly from Vo2peak, which describes the highest
oxygen consumption achieved before symptoms
(fatigue, dyspnea) forced the patient to stop the test.
Such limitations are common in patients with ad-
vanced lung disease.
Several studies have shown patients to be at low
risk for perioperative complications if the preopera-
tive Vo2max is greater than 20 mL/kg/min [52–54],
whereas others use Vo2maxgreater than 15mL/kg/min
as a cutoff for resection [55,56]. A Vo2max less than
10 mL/kg/min is associated with prohibitive morbid-
ity and mortality [17,52,57,58]. Bolliger et al [58]
found a ppoVo2max less than 10 mL/kg/min to cor-
relate with a 100% postoperative mortality.
Exercise oximetry has been suggested to be
helpful in predicting postoperative complications by
some authors [16,59,60] and not by others [61].
Ninan et al [59] found desaturation with exercise
greater than 4% highly predictive of longer ICU stays
and major morbidity.

kaza & mitchell302
Effect of lung volume reduction surgery
Occasionally a patient with a lung mass and poor
pulmonary function may present with functional and
anatomic factors favorable for lung volume reduction
surgery [10]. Because successful lung volume reduc-
tion surgery results in an improvement in FEV1 and
other pulmonary parameters, a combined operation
has been proposed as a strategy to allow safe resec-
tion. The pulmonary mass may reside in the severely
emphysematous part of the lung or may be resected
separately from the lung volume resection. Several
small studies have validated this approach in selected
patients [62,63].
Summary
Fig. 2 is an algorithm for the preoperative
pulmonary evaluation of the lung resection candidate.
Patients should undergo routine spirometry and
diffusion capacity testing. If the FEV1 and Dlco
are greater than 80% predicted, no further study is
needed. When these parameters are less than 80%,
some estimation of postoperative function is likely
needed, taking into account the proposed resection.
Patients with ppoFEV1 or ppoDlco less than 40%
are at increased risk of perioperative complications or
death and should undergo formal exercise testing. A
Vo2max or ppoVo2max less than 10 mL/kg/min is
associated with prohibitive risk for anatomic lung
resection, and alternative treatment modalities should
be considered.
References
[1] Myrdal G, Gustafsson G, Lambe M, Horte LG, Stahle
E. Outcome after lung cancer surgery: factors predict-
ing early mortality and major morbidity. Eur J Cardio-
thorac Surg 2001;20:694–9.
[2] Moores LK. Smoking and postoperative pulmonary
complications: an evidence-based review of the recent
literature. Clin Chest Med 2000;21:139–46.
[3] Wightman J. A prospective survey of the incidence
of postoperative pulmonary complications. Br J Surg
1968;55:85–91.
[4] Schwartz MI, King TE, Raghu G. Approach to the
evaluation and diagnosis of interstitial lung disease.
In: Schwartz MI, King TE, editors. Interstitial lung dis-
ease. Hamilton (Ontario)7 BC Decker; 2003. p. 1–31.
[5] Matsuoka H, Nishio W, Sakamoto T, Harada H, Tsu-
bota N. Prediction of morbidity after lung resection
with risk factors using treadmill exercise test. Eur J
Cardiothorac Surg 2004;26:480–2.
[6] Gerson MC, Hurst JM, Hertzberg VS, et al. Prediction
of cardiac and pulmonary complications related to
elective abdominal and noncardiac thoracic surgery
in geriatric patients. Am J Med 1990;88:101–7.
[7] Epstein S, Faling L, Daly B, Celli B. Predicting
complications after pulmonary resection: preoperative
exercise testing vs a multifactorial cardiopulmonary
risk index. Chest 1993;104:694–700.
[8] Epstein S, Faling L, Daly B, Celli B. Inability to
perform bicycle ergometry predicts increased morbid-
ity and mortality after lung resection. Chest 1995;
107:311–6.
[9] Reilly DF, McNeely MJ, Doerner D, et al. Self-
reported exercise tolerance and the risk of serious
perioperative complications. Arch Intern Med 1999;
159:2185–92.
[10] National Emphysema Treatment Trial Research Group.
A randomized trial comparing lung-volume-reduction
surgery with medical therapy for severe emphysema.
N Engl J Med 2003;348:2059–73.
[11] American Thoracic Society: Statement of pulmonary
rehabilitation-1999. Am J Respir Crit Care Med 1999;
159:1666–82.
[12] Okada M, Okada M, Ishii N, et al. Right ventricular
ejection fraction in the preoperative risk evaluation of
candidates for pulmonary resection. J Thorac Cardio-
vasc Surg 1996;112:364–70.
[13] Boushy SF, Billig DM, North LB, et al. Clinical course
related to preoperative and postoperative pulmonary
function in patients with bronchogenic carcinoma.
Chest 1971;59:383–91.
[14] Miller JI. Physiologic evaluation of pulmonary func-
tion in the candidate for lung resection. J Thorac
Cardiovasc Surg 1993;105:347–51.
[15] Wernly J, DeMeester TR, Kirchner PT, et al. Clinical
value of quantitative ventilation-perfusion lung scans
in the surgical management of bronchogenic carci-
noma. J Thorac Cardiovasc Surg 1980;80:535–43.
[16] British Thoracic Society, Society of Cardiothoracic
Surgeons of Great Britain, Ireland Working Party.
Guidelines on the selection of patients with lung cancer
for surgery. Thorax 2001;56:89–108.
[17] Wyser C, Stulz P, Soler M, et al. Prospective evaluation
of an algorithm for the functional assessment of lung
resection candidates. Am J Respir Crit Care Med 1999;
159:1450–6.
[18] Burke JR, Duarte IG, Thourani VH, Miller J, Joseph I.
Preoperative risk assessment for marginal patients re-
quiring pulmonary resection. Ann Thorac Surg 2003;
76:1767–73.
[19] Ferguson MK, Little L, Rizzo L, et al. Diffusing capac-
ity predicts morbidity and mortality after pulmonary
resection. J Thorac Cardiovasc Surg 1988;96:894–900.
[20] Wang J, Olak J, Ultmann RE, Ferguson MK. Assess-
ment of pulmonary complications after lung resection.
Ann Thorac Surg 1999;67:1444–7.
[21] Ferguson MK, Reeder LB, Mick R. Optimizing se-
lection of patients for major lung resection. J Thorac
Cardiovasc Surg 1995;109:275–83.

preoperative pulmonary evaluation 303
[22] Kearney D, Lee T, Reilly J, DeCamp M, Sugarbaker
D. Assessment of operative risk in patients under-
going lung resection: importance of predicted pulmo-
nary function. Chest 1994;105:753–9.
[23] Stephan F, Boucheseiche S, Hollande J, et al. Pul-
monary complications following lung resection: a com-
prehensive analysis of incidence and possible risk
factors. Chest 2000;118:1263–70.
[24] Harpole Jr DH, Liptay MJ, DeCamp Jr MM, Mentzer
SJ, Swanson SJ, Sugarbaker DJ. Prospective analysis
of pneumonectomy: risk factors for major morbidity
and cardiac dysrhythmias. Ann Thorac Surg 1996;61:
977–82.
[25] Bolliger C, Jordan P, Soler M, et al. Pulmonary
function and exercise capacity after lung resection.
Eur Respir J 1996;9:415–21.
[26] Corris P, Ellis D, Hawkins T, Gibson G. Use of
radionuclide scanning in the preoperative estimation
of pulmonary function after pneumonectomy. Thorax
1987;42:285–91.
[27] Chenuel B, Haouzi P, Olivier P, Marie PY, Chalon B,
Borrelly J. Effect of exercise on lung-perfusion scan-
ning in patients with bronchogenic carcinoma. Eur
Respir J 2002;20:710–6.
[28] Giordano A, Calcagni M, Meduri G, Valente S, Galli
G. Perfusion lung scintigraphy for the prediction of
postlobectomy residual pulmonary function. Chest
1997;111:1542–7.
[29] Wu MT, Chang JM, Chiang AA, et al. Use of
quantitative CT to predict postoperative lung function
in patients with lung cancer. Radiology 1994;191:
257–62.
[30] Wu M-T, Pan H-B, Chiang AA, et al. Prediction of
postoperative lung function in patients with lung
cancer: comparison of quantitative CT with perfu-
sion scintigraphy. AJR Am J Roentgenol 2002;178:
667–72.
[31] Juhl B, Frost N. A comparison between measured and
calculated changes in the lung function after opera-
tion for pulmonary cancer. Acta Anaesthesiol Scand
1975;57(Suppl):39–45.
[32] Zeiher B, Gross T, Kern J, Lanza L, Peterson M.
Predicting postoperative pulmonary function in pa-
tients undergoing lung resection. Chest 1995;108:
68–72.
[33] Pierce R, Copland J, Sharpe K, Barter C. Preoperative
risk evaluation for lung cancer resection: predicted
postoperative product as a predictor of surgical mor-
tality. Am J Respir Crit Care Med 1994;150:947–55.
[34] Ohno Y, Hatabu H, Higashino T, et al. Dynamic
perfusion MRI versus perfusion scintigraphy: predic-
tion of postoperative lung function in patients with
lung cancer. AJR Am J Roentgenol 2004;182:73–8.
[35] Win T, Laroche CM, Groves AM, et al. Use of
quantitative lung scintigraphy to predict postopera-
tive pulmonary function in lung cancer patients under-
going lobectomy. Ann Thorac Surg 2004;78:1215–8.
[36] Bolliger CT, Guckel C, Engel H, et al. Prediction of
functional reserves after lung resection: comparison
between quantitative computed tomography, scintigra-
phy, and anatomy. Respiration (Herrlisheim) 2002;69:
482–9.
[37] Olsen G, Block A, Swenson E, Castle J, Wynne J.
Pulmonary function evaluation of the lung resection
candidate: a prospective study. Am Rev Respir Dis
1975;111:379–87.
[38] Putnam Jr J, Lammermeier D, Colon R, McMurtrey
M, Ali M, Roth J. Predicted pulmonary function and
survival after pneumonectomy for primary lung
carcinoma. Ann Thorac Surg 1990;49:909–14.
[39] Markos J, Mullan BP, Hillman DR, et al. Preoperative
assessment as a predictor of mortality and morbidity
after lung resection. Am Rev Respir Dis 1989;139:
902–10.
[40] Wahi R, McMurtrey M, DeCaro L, et al. Determi-
nants of perioperative morbidity and mortality after
pneumonectomy. Ann Thorac Surg 1989;48:33–7.
[41] Bolton J, Weiman D, Haynes J, Hornung C, Olsen G,
Almond C. Stair climbing as an indicator of pulmo-
nary function. Chest 1987;92:783–8.
[42] Brunelli A, Monteverde M, Al Refai M, Fianchini A.
Stair climbing test as a predictor of cardiopulmonary
complications after pulmonary lobectomy in the
elderly. Ann Thorac Surg 2004;77:266–70.
[43] Van Nostrand D, Kjelsberg M, Humphrey E. Preresec-
tional evaluation of risk from pneumonectomy. Surg
Gynecol Obstet 1968;127:306–12.
[44] Girish M, Trayner Jr E, Dammann O, Pinto-Plata V,
Celli B. Symptom-limited stair climbing as a predic-
tor of postoperative cardiopulmonary complications
after high-risk surgery. Chest 2001;120:1147–51.
[45] Olsen G, Bolton J, Weiman D, Hornung C. Stair
climbing as an exercise test to predict the postopera-
tive complications of lung resection: two years’ expe-
rience. Chest 1991;99:587–90.
[46] Pate P, Tenholder MF, Griffin JP, Eastridge CE,
Weiman DS. Preoperative assessment of the high-risk
patient for lung resection. Ann Thorac Surg 1996;61:
1494–500.
[47] Brunelli A, Al Refai M, Monteverde M, Borri A, Salati
M, Fianchini A. Stair climbing test predicts cardio-
pulmonary complications after lung resection. Chest
2002;121:1106–10.
[48] Holden D, Rice T, Stelmach K, Meeker D. Exercise
testing, 6-min walk, and stair climb in the evaluation
of patients at high risk for pulmonary resection. Chest
1992;102:1774–9.
[49] Pollock M, Roa J, Benditt J, Celli B. Estimation of
ventilatory reserve by stair climbing: a study in patients
with chronic airflow obstruction. Chest 1993;104:
1378–83.
[50] Butland R, Pang J, Gross E, Woodcock A, Geddes D.
Two-, six-, and 12-minute walking tests in respiratory
disease. BMJ 1982;284:1607–8.
[51] Singh S, Morgan M, Hardman A, et al. Comparison
of oxygen uptake during a conventional treadmill test
and the shuttle walking test in chronic airflow limi-
tation. Eur Respir J 1994;7:2016–20.
kaza & mitchell304
[52] Bechard D, Wetstein L. Assessment of exercise oxy-
gen consumption as preoperative criterion for lung
resection. Ann Thorac Surg 1987;44:344–9.
[53] Smith T, Kinasewitz G, Tucker W, et al. Exercise
capacity as a predictor of post-thoracotomy morbidity.
Am Rev Respir Dis 1984;129:730–4.
[54] Bolliger C, Jordan P, Soler M, et al. Exercise capacity
as a predictor of postoperative complications in lung
resection candidates. Am J Respir Crit Care Med 1995;
151:1472–80.
[55] Walsh G, Morice R, Putnam Jr J, et al. Resection of
lung cancer is justified in high-risk patients selected by
exercise oxygen consumption. Ann Thorac Surg 1994;
58:704–10.
[56] Morice R, Peters E, Ryan M, Putnam J, Ali M, Roth J.
Exercise testing in the evaluation of patients at high
risk for complications from lung resection. Chest
1992;101:356–61.
[57] Olsen GN, Weiman DS, Bolton JW, et al. Submaximal
invasive exercise testing and quantitative lung scan-
ning in the evaluation for tolerance of lung resection.
Chest 1989;95:267–73.
[58] Bolliger C, Wyser C, Roser H, Soler M, Perruchoud A.
Lung scanning and exercise testing for the prediction
of postoperative performance in lung resection can-
didates at increased risk for complications. Chest
1995;108:341–8.
[59] Ninan M, Sommers KE, Landreneau RJ, et al. Stan-
dardized exercise oximetry predicts postpneumonec-
tomy outcome. Ann Thorac Surg 1997;64:328–32.
[60] Rao V, Todd TRJ, Kuus A, Buth KJ, Pearson FG.
Exercise oximetry versus spirometry in the assessment
of risk prior to lung resection. Ann Thorac Surg
1995;60:603–8.
[61] Varela G, Cordovilla R, Jimenez MF, Novoa N. Utility
of standardized exercise oximetry to predict cardio-
pulmonary morbidity after lung resection. Eur J
Cardiothorac Surg 2001;19:351–4.
[62] McKenna Jr R, Fischel R, Brenner M, Gelb A. Com-
bined operations for lung volume reduction surgery
and lung cancer. Chest 1996;110:885–8.
[63] Choong CK, Meyers BF, Battafarano RJ, et al. Lung
cancer resection combined with lung volume reduction
in patients with severe emphysema. J Thorac Cardio-
vasc Surg 2004;127:1323–31.

Thorac Surg Clin
The Preoperative Anesthesia Evaluation
Clifford A. Schmiesing, MD*, Jay B. Brodsky, MD
Department of Anesthesia, Stanford University Medical Center, 300 Pasteur Drive, H3524, Stanford, CA 94305, USA
Nowhere is the challenge and importance of the
collaboration of surgeons and anesthesiologists
greater than in thoracic surgery. Most patients facing
major chest surgery for advanced malignancy are
elderly and frequently have serious complications of
lifelong tobacco use. Airway management, lung iso-
lation techniques, and multimodal efforts to manage
respiratory complications and control postoperative
pain are just a few examples of the challenges con-
fronting physicians caring for thoracic surgical pa-
tients. Cardiorespiratory complications are the major
causes of morbidity after thoracic surgery [1].
Delivery of efficient, cost-effective medical care
to increasingly knowledgeable patients presents
another layer of complexity to the task facing sur-
geons and anesthesiologists. Most of the millions of
surgical procedures performed annually in the United
States are on an outpatient or same-day admission
basis. Previously, in the era before use review and
preauthorization requirements, preoperative patient
preparation could occur in the hospital without limits
on the number of consultants and diagnostic tests
obtained. Risk assessment, if it was considered at
all, was limited to ‘‘You know, she may not make it
through surgery.’’ Patients today know more and
expect more and often are active participants in
medical decisions affecting their care. It is now un-
usual to cancel a surgical procedure because the
patient is ‘‘too sick.’’
Many goals of the anesthesia and surgical pre-
operative assessment overlap. Shared goals include
obtaining a complete current and past medical history,
1547-4127/05/$ – see front matter D 2005 Elsevier Inc. All rights
doi:10.1016/j.thorsurg.2005.02.006
* Corresponding author.
E-mail address: [email protected]
(C.A. Schmiesing).
performing a thorough physical examination, and
obtaining and evaluating pertinent diagnostic tests to
assess risk and optimize outcome. Problems such as
postoperative respiratory failure, perioperative myo-
cardial infarction, blood pressure control, coagulopa-
thies, inadequate pain control, and end-of-life issues
concern anesthesiologists and surgeons. Other impor-
tant common goals are obtaining informed consent;
addressing a patient’s questions and concerns; and
educating the patient and family members about the
surgical procedure, anesthesia, and recovery period.
Specific anesthetic concerns include preoperative air-
way assessment, intravenous access, suitability of re-
gional anesthetic techniques, and the patient’s likely
response and tolerance to anesthetic agents.
One key element of the preoperative assessment is
timing. Timely preoperative assessment allows early
identification of potential problems and proactive
planning before surgery. Examples of issues that
can benefit from early detection and intervention in-
clude identification and treatment of exacerbations of
chronic obstructive pulmonary disease; the need to
obtain autologous or designated donor blood dona-
tions; control of hypertension; substance abuse; and
evaluation of new symptoms or conditions, such
as chest pain or arrhythmias. Medication adjustment
may require significant lead-time. Conversion or ces-
sation of anticoagulant regimens typically requires
1 week, and initiation of antihypertensive therapy
may take even longer. Simply obtaining relevant out-
side medical records under the new Health Insurance
Portability and Accountability Act mandates, such as
prior anesthetic records documenting a difficult in-
tubation or intraoperative incident, can require sev-
eral days [2].
Early preoperative assessment also is important
because nobody benefits from avoidable last-minute
15 (2005) 305 – 315
reserved.
thoracic.theclinics.com

Box 1. Anesthesia PreoperativeAssessment Clinic positive outcomes
� Decreased rate of surgical delays andcancellations
� Reduction in preoperative testing andspecialty consultations
� Convenient ‘‘one-stop’’ coordinatedpresurgical preparation for admission,laboratory, and preanesthesiaservices
� Development of clinical pathwaysand protocols to improve efficiencyand quality of care
� Enhanced patient education
Table 1
American Society of Anesthesiologists physical status
classification
Class 1 Healthy patient, no medical problems
Class 2 Mild systemic disease
Class 3 Severe systemic disease, but not incapacitating,
or multiple systemic problems
Class 4 Severe systemic disease that is a constant threat
to life
Class 5 Moribund, not expected to survive 24 h
regardless of operation
schmiesing & brodsky306
surgical cancellations [3]. An inadequate preoperative
evaluation that fails to identify a patient on warfarin
or to discover a history of exertional chest pain in the
holding area minutes before surgery results in loss of
time and resources because of delay or cancellation or
may lead to pressure to proceed despite unresolved
medical issues [4]. Patients may be devastated or
angry when their surgery is cancelled at the last
minute for reasons they can barely comprehend,
especially when it is due to miscommunication
or oversight.
Communication is another important element in
the preoperative assessment. Effective collaboration
between the anesthesiologist and the surgeon is en-
hanced when key information is shared in an open
and timely manner. This is a ‘‘two-way’’ street. When
a potential problem or unresolved issue is identified,
especially one with no simple solution, it benefits the
physicians involved to discuss the matter and develop
a management plan before surgery. No one wants to
be surprised by a problem in the operating room
that was identifiable early on. Examples of issues that
benefit from early preoperative planning include a
patient who refuses blood products, a patient who
requires extensive preoperative medical clearance or
testing, an extremely high-risk patient, an impaired
patient, or a patient with complicating social situa-
tions. Preoperative ‘‘team’’ collaboration can enhance
working relationships and create an atmosphere of
respect and trust between the anesthesiologist and the
surgeon. Everyone, but most importantly the patient,
benefits from this team approach.
Anesthesia preoperative assessments are per-
formed in a variety of settings depending on nu-
merous factors, including patient demographics and
acuity levels and institutional factors such as physi-
cian staffing constraints, surgical volume, and avail-
able facilities. The model effectively implemented at
the authors’ institution and at many other academic
and large medical centers is an Anesthesia Preopera-
tive Assessment Clinic (APEC) [5]. The benefits of
an Anesthesia Preoperative Assessment Clinic are
listed in Box 1.
Beyond the American Society of Anesthesiologists
classification system
An important assumption underlying the preop-
erative assessment is that it can improve outcome
by identifying high-risk patients. The well-known
American Society of Anesthesiologists (ASA) Physi-
cal Status Classification has been used routinely for
decades to stratify patient health status and to
estimate risk (Table 1). Although the ASA Physical
Status Classification remains a useful means to
convey quickly an overall impression of a patient’s
status, it is imprecise and has limited utility. First, the
ASA classification allows considerable leeway in
how patients are classified. A young patient with
controlled hypertension would be classified status
ASA class 2. An elderly patient with poorly con-
trolled hypertension, chronic opiate use and toler-
ance, obesity, and long-standing tobacco abuse also
might be classified ASA class 2, especially if he or
she were asymptomatic. The ASA Physical Status
Classification does not take into account the under-
lying risk of the planned surgical procedure. A patient
classified ASA class 4 with advanced coronary artery
disease (CAD) is at low risk for complications after
cataract removal, but at considerably higher risk
when undergoing an esophagectomy. Lastly, the ASA
classification system is not specific enough to be
useful in making management decisions for individ-
ual patients.
A more useful approach to preoperative risk as-
sessment and management is to consider each of the
patient’s diseases or problems individually and in

Box 2. Preoperative medicationconsiderations
1. Patients should provide a completelist or the actual pill bottles so thatmedications can be administered ac-curately during their hospitalization.
2. Most medications should be contin-ued up to, and including, the day ofsurgery (taken with a small sip ofwater). Notable exceptions include:
a. Oral and injectable diabeticmedications
b. Antiplatelet and anticoagulantmedications
c. Diuretics
d. Dietary supplements, herbs, andmegadose vitamin preparations
3. In most instances, patients can con-tinue opiate analgesics on the dayof surgery without ill effect. Manypatients assume they cannot takepain medications on the day of sur-gery, andappreciate being instructedthey can.
4. The frequency of prn opiate analge-sics should be determined preopera-tively to anticipate opiate toleranceor withdrawal.
5. If an analgesic is discontinued be-fore surgery (eg, ibuprofen), con-sider giving the patient a suitablealternative (eg, celecoxib or acet-aminophen/hydrocodone [Vicodin]).
6. Some patients benefit from a pre-operative anxiolytic (eg, alprazolam)
preoperative anesthesia evaluation 307
aggregate and to consider how each medical con-
dition would affect the patient’s response to anes-
thetic and surgical stresses. Each significant medical
condition should be assessed in terms of its severity
and degree of organ impairment, then the condi-
tion should be optimized to the fullest extent pos-
sible given the constraints and the reality of the
clinical situation. A medical problem may or may not
be significant.
Consider a patient with a history of viral hepatitis.
A distant history of hepatitis A holds no relevance to
an upcoming lobectomy for lung cancer. It carries no
anesthetic or surgical risk, does not require detailed
assessment, and cannot be optimized before surgery.
Hepatitis C, on the other hand, is a chronic destruc-
tive liver disease with a large variation in clinical se-
verity from completely asymptomatic to profoundly
debilitating and life-threatening. Hepatitis C may
have marked physiologic consequences during the
perioperative period, including coagulopathy, en-
cephalopathy, pulmonary and cardiac dysfunction,
fluid imbalances, electrolyte abnormalities, malnutri-
tion, and impaired drug metabolism. It is important to
determine the degree of hepatic impairment caused
by hepatitis C through history, physical examination,
and subsequent focused diagnostic testing, including
hepatic, renal, and coagulation function. Many
patients with long-standing hepatitis C have no
significant abnormalities of coagulation and hepatic
function, whereas others are severely impaired. When
the degree of impairment has been determined, risk
assessment and planning for specific problems can
occur. Examples of planning include drainage of
pleural and peritoneal effusions, preparation and
preoperative administration of blood products,
choices of intraoperative invasive monitoring and
postoperative nursing care, suitability of regional
anesthesia, and fluid management. Individual assess-
ment of specific problems guides testing, planning,
and management. It is more useful than simply
assigning an ASA classification based on a history
of ‘‘hepatitis.’’
for preoperative anxiety orinsomnia.
7. Preprinted instructions with explicitinformation regarding preoperativemedications are helpful to ensurecompliance.
8. With the continual flood of newmedications, it is advisable alwaysto look up unfamiliar medications toavoid medication errors and harmfuldrug interactions.
Preoperative assessment of common medical
conditions
Hypertension
Preoperative hypertension is common [6]. Factors
that can exacerbate hypertension before surgery in-
clude pain, anxiety, and patient confusion about
antihypertensive regimens in the immediate preopera-
tive period. Severe preoperative hypertension is as-

schmiesing & brodsky308
sociated with labile intraoperative blood pressure.
This situation can result in significant hypotension,
increasing the risk of myocardial ischemia and
infarction, cerebral and renal dysfunction, and dys-
rhythmias [6–8]. Patients with renal insufficiency
and congestive heart failure secondary to hyper-
tension should be considered at higher operative risk
[9]. Moderate hypertension (diastolic blood pressure
< 110 mm Hg) did not increase risk, however, in one
study of more than 600 patients undergoing sur-
gery [10].
As a general rule, patients presenting with severe
uncontrolled hypertension (systolic blood pressure
> 200mmHgor diastolic blood pressure > 110mmHg)
should be treated before elective surgery. Treatment
of hypertension usually can be accomplished with-
out cancellation of surgery when identified early
(ie, at least 1 week). The b1-selective b-blockers(atenolol and metoprolol) are effective choices when
antihypertensive therapy must be initiated and no
contraindications to b blockade are present. The
combination of atenolol and an anxiolytic, such
as alprazolam, is effective in treating preoperative
hypertension in a previously untreated patient. Key
points regarding initiation of efforts to control
preoperative hypertension include rapid initiation
and titration of therapy coordinated through an Anes-
thesia Preoperative Assessment Clinic and the pri-
mary care physician or surgeon and close monitoring
and follow-up to ensure safety and effectiveness.
Treatment should be reassessed 1 to 2 days before sur-
gery to avoid the need for a last-minute cancellation.
Patients whose hypertension is well controlled
preoperatively should be instructed to continue their
antihypertensive medications up to and including the
day of surgery. Diuretic medications are an excep-
tion; they should be avoided the day of surgery.
General points regarding preoperative medication
use are provided in Box 2.
Box 3. Lee’s revised cardiac risk index
One point is assigned for each of thefollowing when present:
1. High-risk surgical procedure2. History of ischemic heart disease
(excluding previousrevascularization)
3. History of congestive heart failure4. History of stroke or transient ische-
mic attack5. Preoperative insulin therapy6. Preoperative creatinine >2 mg/dL
Ischemic heart disease and cardiac risk
Perioperative myocardial infarction and cardiac
death remain a major problem [11]. Identification,
risk stratification, preoperative testing, and manage-
ment for each individual patient may be difficult and
complex. These issues become more complex in the
setting of surgery for malignancy, where any benefit
of diagnostic testing and therapeutic interventions
to improve cardiac outcomes may require weeks to
months to complete, but must be weighed against the
risk of delaying potentially curative surgery. Numer-
ous guidelines to help identify high-risk patients
have been published [9,12–16]. Detailed comparison
of these guidelines is beyond the scope of this arti-
cle. One simple approach to risk assessment is dis-
cussed, however.
Patients can be stratified into low-risk, intermedi-
ate-risk, and high-risk groups. Analysis of clinical
variables is the first step in stratification. One useful
assessment tool is the revised cardiac risk index by
Lee et al [16], based on six clinical variables listed in
Box 3. The index is simple to apply using readily
available preoperative data. Patients with fewer than
3 points are generally at low risk, whereas patients
with 3 or more points are at high risk for periopera-
tive cardiac events (Fig. 1). Analysis suggests that
routine use of noninvasive diagnostic testing, includ-
ing myocardial perfusion imaging and dobutamine
stress echocardiography, provides little additional in-
formation beyond that obtained from Lee’s revised
cardiac index, especially in low-risk patients [17].
Functional testing is useful in further stratifying
patients with 3 or more points. Testing of these
high-risk patients can identify a group of extremely
high-risk patients with extensive areas of myocardial
ischemia. This small subset of patients seems to be
at very high risk of serious cardiac complications,
with or without protective perioperative b-blockertherapy [18,19].
The question often arises as to whether coronary
revascularization should be performed before non-
cardiac surgery. Several studies have shown that pa-
tients who have had coronary artery bypass graft
(CABG) procedures in the 5 years before a noncar-
diac operation had fewer cardiac deaths and myo-
cardial infarctions than patients receiving medical
therapy alone [12,20,21]. Based on these findings, the
American College of Cardiologists and the American
Heart Association do not recommend preoperative
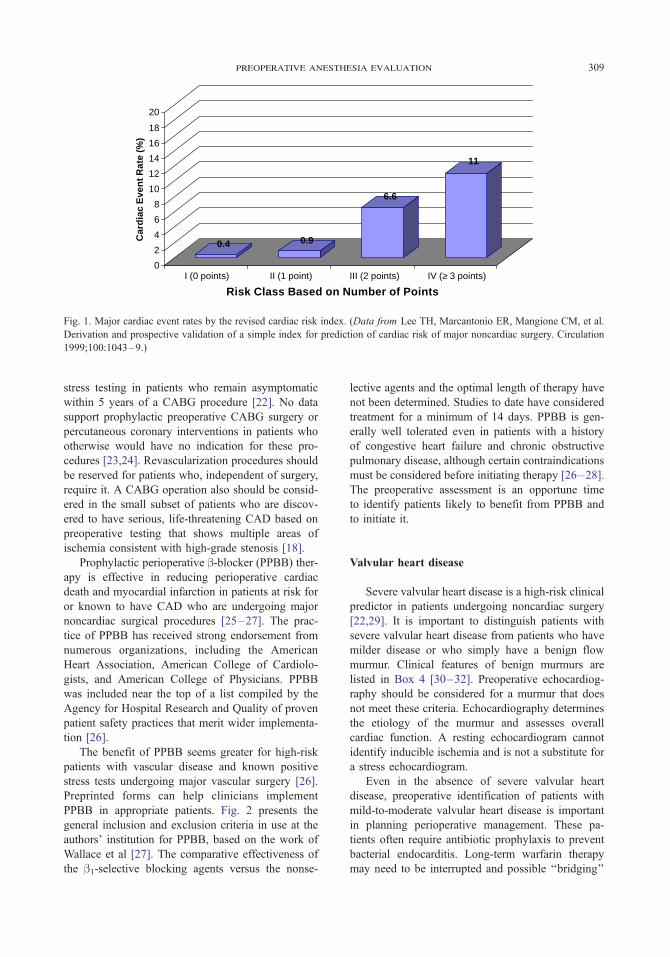
0.4 0.9
6.6
11
0
2
4
6
8
10
12
14
16
18
20
Car
dia
c E
ven
t Rat
e (%
)
I (0 points) II (1 point) III (2 points) IV (≥ 3 points)
Risk Class Based on Number of Points
Fig. 1. Major cardiac event rates by the revised cardiac risk index. (Data from Lee TH, Marcantonio ER, Mangione CM, et al.
Derivation and prospective validation of a simple index for prediction of cardiac risk of major noncardiac surgery. Circulation
1999;100:1043–9.)
preoperative anesthesia evaluation 309
stress testing in patients who remain asymptomatic
within 5 years of a CABG procedure [22]. No data
support prophylactic preoperative CABG surgery or
percutaneous coronary interventions in patients who
otherwise would have no indication for these pro-
cedures [23,24]. Revascularization procedures should
be reserved for patients who, independent of surgery,
require it. A CABG operation also should be consid-
ered in the small subset of patients who are discov-
ered to have serious, life-threatening CAD based on
preoperative testing that shows multiple areas of
ischemia consistent with high-grade stenosis [18].
Prophylactic perioperative b-blocker (PPBB) ther-apy is effective in reducing perioperative cardiac
death and myocardial infarction in patients at risk for
or known to have CAD who are undergoing major
noncardiac surgical procedures [25–27]. The prac-
tice of PPBB has received strong endorsement from
numerous organizations, including the American
Heart Association, American College of Cardiolo-
gists, and American College of Physicians. PPBB
was included near the top of a list compiled by the
Agency for Hospital Research and Quality of proven
patient safety practices that merit wider implementa-
tion [26].
The benefit of PPBB seems greater for high-risk
patients with vascular disease and known positive
stress tests undergoing major vascular surgery [26].
Preprinted forms can help clinicians implement
PPBB in appropriate patients. Fig. 2 presents the
general inclusion and exclusion criteria in use at the
authors’ institution for PPBB, based on the work of
Wallace et al [27]. The comparative effectiveness of
the b1-selective blocking agents versus the nonse-
lective agents and the optimal length of therapy have
not been determined. Studies to date have considered
treatment for a minimum of 14 days. PPBB is gen-
erally well tolerated even in patients with a history
of congestive heart failure and chronic obstructive
pulmonary disease, although certain contraindications
must be considered before initiating therapy [26–28].
The preoperative assessment is an opportune time
to identify patients likely to benefit from PPBB and
to initiate it.
Valvular heart disease
Severe valvular heart disease is a high-risk clinical
predictor in patients undergoing noncardiac surgery
[22,29]. It is important to distinguish patients with
severe valvular heart disease from patients who have
milder disease or who simply have a benign flow
murmur. Clinical features of benign murmurs are
listed in Box 4 [30–32]. Preoperative echocardiog-
raphy should be considered for a murmur that does
not meet these criteria. Echocardiography determines
the etiology of the murmur and assesses overall
cardiac function. A resting echocardiogram cannot
identify inducible ischemia and is not a substitute for
a stress echocardiogram.
Even in the absence of severe valvular heart
disease, preoperative identification of patients with
mild-to-moderate valvular heart disease is important
in planning perioperative management. These pa-
tients often require antibiotic prophylaxis to prevent
bacterial endocarditis. Long-term warfarin therapy
may need to be interrupted and possible ‘‘bridging’’

Stanford University Department of Anesthesia
Prophylactic Perioperative Beta Blockade (PPBB) Considerations
All patients scheduled for major elective non-cardiac surgery requiring general anesthesia and a hospital stay qualify. Patients foremergency surgery, hemodynamically unstable patients, and renal transplant patients need to be assessed individually1 . These guidelinesare intended to provide supplemental information for use with the Prophylactic Perioperative Beta Blockade (PPBB) Protocol order form(15-1797).
Consider PPBB for patients within at least one of the following categories:Known coronary artery disease Any two of the following: age > 65 years,Atherosclerotic vascular disease hypertension, current smoker, hyperlipidemiaDiabetes
Patients within any of the following categories should not receive PPBB:Known sensitivity to beta blockers Second or third degree heart blockAcute congestive heart failure Systolic blood pressure (SBP) < 100 mmHgAcute bronchospasm Heart rate < 60 beats per minute (bpm)Acutely hemodynamically unstable patients
Care must be taken with administration to patients with a history of asthma or COPD.
Drug Choice: Atenolol, bisoprolol and metoprolol may all be used. They are all long-acting, Beta-1 selective and have similar efficacy inthe prevention of death after myocardial infarction. Other beta blockers without intrinsic sympathomimetic effect are probably equivalent,so if a patient is on another beta blocker it is unnecessary to change to a Beta-1 selective drug. However, the dosage should be adjustedto keep the HR < 80 bpm.
How should PPBB be initiated?
Preoperatively: If HR > 60 bpm and SBP > 100 mmHg, then oral dosing with twice daily metoprolol (25-50 mg), or once dailyatenolol (50-100 mg) can be started several days before surgery. Target HR is > 50 and < 70 bpm.
In Holding Area prior to surgery: If HR > 60 bpm and SBP > 100 mmHg, metoprolol 2.5-5.0 mg IV can be given while monitoringHR and BP. For maximal beta blockade, consider additional dose(s) every 10 minutes if HR remains > 70 bpm and SBP > 100mmHg. Target HR is > 50 and < 70 bpm.
During Surgery: If HR >60 bpm and SBP >100 mmHg, metoprolol 2.5-5.0 mg IV every 10 minutes may be given 30 minutes priorto emergence. Target HR for maximal beta blockade is < 70 bpm. Alternatively, esmolol infusion may be titrated to maintain HR <70 during emergence.
PACU or ICU after surgery: If HR > 60 bpm, and SBP > 100 mmHg, metoprolol 2.5-5.0 mg IV may be given while monitoringHR and BP. For maximal beta blockade, consider additional dose(s) every 10 minutes if HR remains > 70 bpm and SBP > 100mmHg. Target HR is > 50 and < 70 bpm. Consider use of PPBB Protocol order form (15-1797).
Postoperative Care: If the patient is to be kept NPO, metoprolol 2.5-10 mg IV every 6 hours dosing should be continued withtarget HR > 50 and < 70 bpm while maintaining SBP > 100 mmHg. When patient is able to take oral medications the patient maybe switched to twice daily oral metoprolol (25-50 mg), or once daily atenolol (50-100 mg) with dosage adjusted to keep HR > 50and < 70 bpm and SBP > 100 mmHg. Consider use of PPBB Protocol order form (15-1797).
PPBB should be continued for at least 7 days postoperatively. Patients with a history of coronary artery disease may benefit fromindefinite beta blockade therapy.
1 These guidelines provide basic recommendations. They are not intended as absolute or standard requirements. Practice guidelines should bemodified based on clinical needs and individual practice to ensure the highest quality of patient care.`
References:
1. Mangano DT, Browner WS, Hollenberg M, Li J, Tateo IM. Long-term cardiac prognosis following noncardiac surgery. The study ofPerioperative Ischemia Research Group [see comments] [Journal Article]. Journal of the American Medical Association (JAMA), July 8,1992 268(2);233-9.
2. Mangano DT, Browner WS, Hollenberg M, London MJ, Tubau JF, Tateo IM, Association of perioperative myocardial ischemia withcardiac morbidity and mortality in men undergoing noncardiac surgery. The Study of Perioperative Ischemia Research Group [seecomments] [Journal Article] New England Journal of Medicine, Dec. 17, 1990, 323(26):1781-8.
3. Mangano DT, Layug EL, Wallace A, Tateo IM, McSPI: Effect of atenolol on mortality and cardiovascular morbidity after noncardiacsurgery. New England Journal of Medicine, 1996. 335:1713-1720.
4. Poldermans D, Boersma E, Jeron J, et al. The effect of bisoprolol on perioperative mortality and myocardial infarction inhigh-risk patients undergoing vascular surgery. New England Journal of Medicine, 1999; 341:1789-94.
5. Wallace A, Layug B, Tateo I, Li J, Hollenberg M, Browner W, Miller D, Mangano D, Group. MR: Prophylactic atenololreduces postoperative myocardial ischemia. Anesthesiology 1998; 88:7-17.
This form is not intended to be a permanent part of the patient's Medical Record.
Fig. 2. Prophylactic perioperative b-blocker therapy inclusion and exclusion criteria.
schmiesing & brodsky310
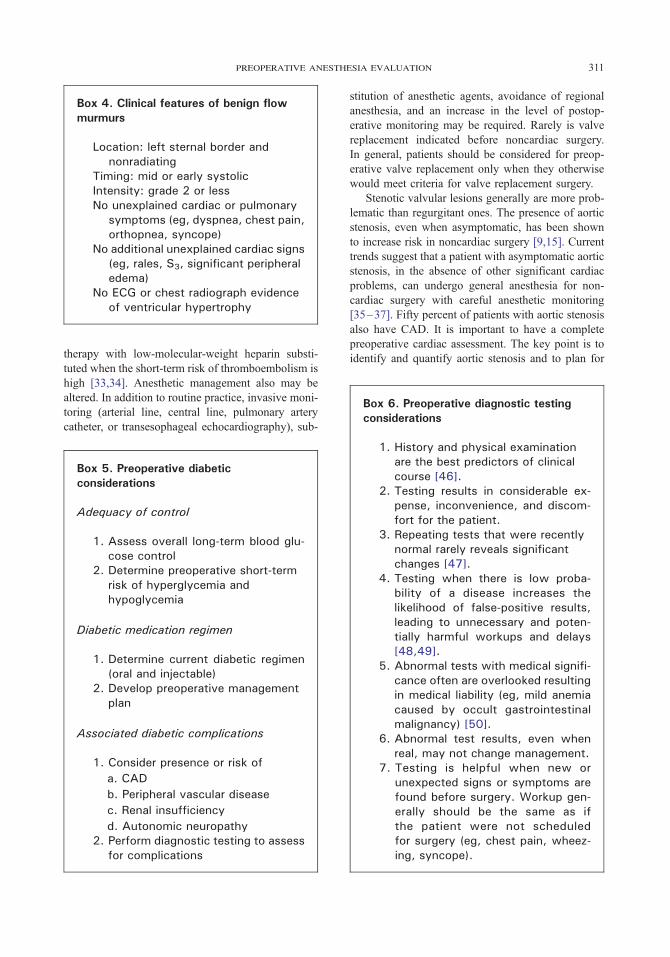
Box 4. Clinical features of benign flowmurmurs
Location: left sternal border andnonradiating
Timing: mid or early systolicIntensity: grade 2 or lessNo unexplained cardiac or pulmonary
symptoms (eg, dyspnea, chest pain,orthopnea, syncope)
No additional unexplained cardiac signs(eg, rales, S3, significant peripheraledema)
No ECG or chest radiograph evidenceof ventricular hypertrophy
Box 6. Preoperative diagnostic testingconsiderations
preoperative anesthesia evaluation 311
therapy with low-molecular-weight heparin substi-
tuted when the short-term risk of thromboembolism is
high [33,34]. Anesthetic management also may be
altered. In addition to routine practice, invasive moni-
toring (arterial line, central line, pulmonary artery
catheter, or transesophageal echocardiography), sub-
Box 5. Preoperative diabeticconsiderations
Adequacy of control
1. Assess overall long-term blood glu-cose control
2. Determine preoperative short-termrisk of hyperglycemia andhypoglycemia
Diabetic medication regimen
1. Determine current diabetic regimen(oral and injectable)
2. Develop preoperative managementplan
Associated diabetic complications
1. Consider presence or risk of
a. CAD
b. Peripheral vascular disease
c. Renal insufficiency
d. Autonomic neuropathy2. Perform diagnostic testing to assess
for complications
stitution of anesthetic agents, avoidance of regional
anesthesia, and an increase in the level of postop-
erative monitoring may be required. Rarely is valve
replacement indicated before noncardiac surgery.
In general, patients should be considered for preop-
erative valve replacement only when they otherwise
would meet criteria for valve replacement surgery.
Stenotic valvular lesions generally are more prob-
lematic than regurgitant ones. The presence of aortic
stenosis, even when asymptomatic, has been shown
to increase risk in noncardiac surgery [9,15]. Current
trends suggest that a patient with asymptomatic aortic
stenosis, in the absence of other significant cardiac
problems, can undergo general anesthesia for non-
cardiac surgery with careful anesthetic monitoring
[35–37]. Fifty percent of patients with aortic stenosis
also have CAD. It is important to have a complete
preoperative cardiac assessment. The key point is to
identify and quantify aortic stenosis and to plan for
1. History and physical examinationare the best predictors of clinicalcourse [46].
2. Testing results in considerable ex-pense, inconvenience, and discom-fort for the patient.
3. Repeating tests that were recentlynormal rarely reveals significantchanges [47].
4. Testing when there is low proba-bility of a disease increases thelikelihood of false-positive results,leading to unnecessary and poten-tially harmful workups and delays[48,49].
5. Abnormal tests with medical signifi-cance often are overlooked resultingin medical liability (eg, mild anemiacaused by occult gastrointestinalmalignancy) [50].
6. Abnormal test results, even whenreal, may not change management.
7. Testing is helpful when new orunexpected signs or symptoms arefound before surgery. Workup gen-erally should be the same as ifthe patient were not scheduledfor surgery (eg, chest pain, wheez-ing, syncope).
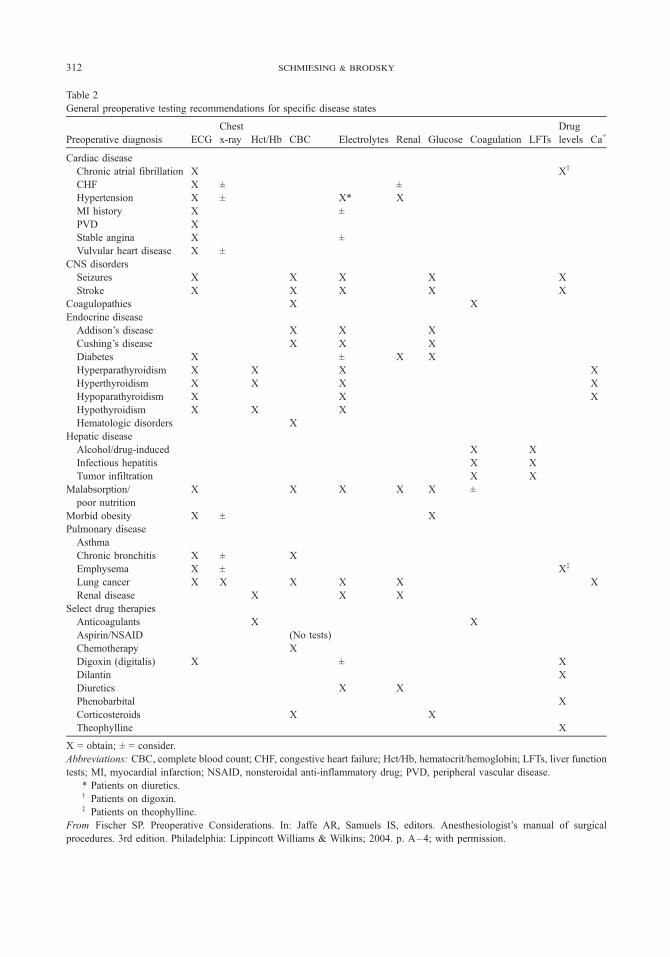
Table 2
General preoperative testing recommendations for specific disease states
Preoperative diagnosis ECG
Chest
x-ray Hct/Hb CBC Electrolytes Renal Glucose Coagulation LFTs
Drug
levels Ca+
Cardiac disease
Chronic atrial fibrillation X Xy
CHF X ± ±
Hypertension X ± X* X
MI history X ±
PVD X
Stable angina X ±
Vulvular heart disease X ±
CNS disorders
Seizures X X X X X
Stroke X X X X X
Coagulopathies X X
Endocrine disease
Addison’s disease X X X
Cushing’s disease X X X
Diabetes X ± X X
Hyperparathyroidism X X X X
Hyperthyroidism X X X X
Hypoparathyroidism X X X
Hypothyroidism X X X
Hematologic disorders X
Hepatic disease
Alcohol/drug-induced X X
Infectious hepatitis X X
Tumor infiltration X X
Malabsorption/
poor nutrition
X X X X X ±
Morbid obesity X ± X
Pulmonary disease
Asthma
Chronic bronchitis X ± X
Emphysema X ± Xz
Lung cancer X X X X X X
Renal disease X X X
Select drug therapies
Anticoagulants X X
Aspirin/NSAID (No tests)
Chemotherapy X
Digoxin (digitalis) X ± X
Dilantin X
Diuretics X X
Phenobarbital X
Corticosteroids X X
Theophylline X
X = obtain; ± = consider.
Abbreviations: CBC, complete blood count; CHF, congestive heart failure; Hct/Hb, hematocrit/hemoglobin; LFTs, liver function
tests; MI, myocardial infarction; NSAID, nonsteroidal anti-inflammatory drug; PVD, peripheral vascular disease.
* Patients on diuretics.y Patients on digoxin.z Patients on theophylline.
From Fischer SP. Preoperative Considerations. In: Jaffe AR, Samuels IS, editors. Anesthesiologist’s manual of surgical
procedures. 3rd edition. Philadelphia: Lippincott Williams & Wilkins; 2004. p. A–4; with permission.
schmiesing & brodsky312

preoperative anesthesia evaluation 313
potential intraoperative problems. Unrecognized se-
vere aortic stenosis may be the cause of major peri-
operative complications.
Mitral stenosis is more difficult to identify by
auscultation than aortic stenosis. Mitral stenosis
presents as a low-pitched diastolic rumble with or
without an opening snap. Symptomatic patients with
mitral stenosis and pulmonary hypertension are at
high risk [38]. Patients with either aortic or mitral
regurgitation who have preserved left ventricular
function are generally at lower risk from anesthe-
sia [39,40].
Diabetes mellitus
Diabetes is the most common endocrine disorder
in surgical patients, affecting approximately 5% of
the North America population [41,42]. Diabetic
patients present numerous issues to be considered
during the preoperative assessment (Box 5). Asso-
ciated CAD is a significant problem and should
always be considered during the preoperative assess-
ment of a diabetic patient. General goals include
avoidance of hyperglycemia and hypoglycemia.
Surgery should be scheduled early in the day. Fast-
ing patients should be cautioned about symptoms of
hypoglycemia and hyperglycemia and advised to
monitor glucose levels at home. Patients should be
given clear instructions about how and when to ad-
just their diabetic regimen.
In general, fasting type 2 diabetics on diet or oral
therapy alone simply may withhold their medications
on the day of surgery. Type 1 and type 2 diabetics
requiring insulin can be managed with a ‘‘sliding
scale’’ on the day of surgery or with a downward
adjustment in their usual insulin regimen, switching
from long-acting to short-acting or intermediate-
acting insulins. Patients on insulin pumps usually
can continue them at their basal rate.
No single formula or conversion scale fits all
clinical situations. It is helpful to enlist the patient’s
experience when deciding how to adjust insulin-
dosing regimens because patients usually have good
insight into their likely responses to changes in their
oral intake and therapy. Simply instructing a patient
who is coming for surgery early in the morning to
take their morning insulin at 5 a.m. is not appropri-
ate if they normally do not take their insulin until
10 a.m. Changes should be conservative; one should
not aim for tight preoperative glycemic control.
Blood glucose levels of 120 to 200 g/dL are generally
well tolerated and safe. Frequent checks of blood
glucose levels at home and after the patient arrives
at the hospital minimize problems.
Preoperative diagnostic testing
In addition to the cardiovascular screening tests
discussed previously, preoperative evaluation before
thoracic surgery often includes a complete assessment
of pulmonary function and reserve. Detailed discus-
sions of appropriate pulmonary testing strategies
before thoracic surgery are presented elsewhere in
this issue. What is considered ‘‘appropriate’’ routine
preoperative testing continues to evolve, more re-
cently taking a path leading to fewer, not more, tests.
There is little evidence to suggest a clear benefit for
most routine testing and much to argue against it
[43–45]. Some factors to consider regarding diag-
nostic testing are presented in Box 6. Often the type
of operation determines the appropriate tests. General
testing guidelines for specific medical conditions
are provided in Table 2 [51].
Summary
Thorough and timely anesthesia preoperative
evaluation is essential for good patient outcomes.
Perioperative care is becoming more complex and
comprehensive, while older and sicker patients are
being considered for major thoracic surgery. In ad-
dition to pulmonary and wound care, prevention of
cardiac complications with b-blocker therapy, mul-
timodal pain control, tighter glycemic control, nutri-
tional support, and prevention of thromboembolism
are important perioperative goals. Early identification
of significant medical and nonmedical issues allows
for complete evaluation and planning and decreases
the likelihood of delays, cancellations, and compli-
cations. Good communication and preparation benefit
everyone. The implementation of an anesthesia pre-
operative assessment program or clinic can help
achieve these important goals.
References
[1] Slinger PD, Johnston MR. Preoperative evaluation of
the thoracic surgery patient. 3rd edition. Philadelphia7
Churchill Livingstone; 2003.
[2] Gostine L. National health information privacy:
regulations under the health Insurance Portability and
Accountability Act. JAMA 2001;285:3015–21.
schmiesing & brodsky314
[3] Pollard JB, Olson L. Early outpatient preoperative
anesthesia assessment: does it help to reduce operating
room cancellations? Anesth Analg 1999;89:502–5.
[4] Singer SJ, Gaba DM, Geppert JJ, Sinaiko AD, Howard
SK, Park KC. The culture of safety: results of an
organization-wide survey in 15 California hospitals.
Qual Saf Health Care 2003;12:112–8.
[5] Fischer SP. Development and effectiveness of an an-
esthesia preoperative evaluation clinic in a teaching
hospital. Anesthesiology 1996;85:196–206.
[6] Wolfsthal SD. Is blood pressure control necessary be-
fore surgery? Med Clin North Am 1993;77:349–63.
[7] Towne JB, Bernhard VM. The relationship of post-
operative hypertension to complications following
carotid endarterectomy. Surgery 1980;88:575–80.
[8] Prys-Roberts C, Meloche R, Foex P. Studies of an-
esthesia in relation to hypertension: I. cardiovascular
responses of treated and untreated patients. Br J Anesth
1971;43:112–37.
[9] Goldman L, Caldera DL, Nussbaum SR, et al. Multi-
factorial index of cardiac risk in noncardiac surgical
procedures. N Engl J Med 1977;297:845–50.
[10] Goldman L, Caldera D. Risks of general anesthesia and
elective operation in the hypertensive patient. Anes-
thesiology 1979;50:285–92.
[11] Mangano DT, Goldman L. Preoperative assessment of
patients with known or suspected coronary disease.
N Engl J Med 1995;333:1750–6.
[12] Eagle K, Rihal C, Mickel M, Holmes D, Foster E,
Gersh B. Cardiac risk of noncardiac surgery: influence
of coronary disease and type of surgery in 3368 op-
erations. CASS Investigators and University of Michi-
gan Heart Care Program, Coronary Artery Surgery
Study. Circulation 1997;96:1882–7.
[13] Eagle KA, Berger PB, Calkins H, et al. ACC/AHA
guideline update for perioperative cardiovascular eval-
uation for noncardiac surgery—executive summary:
a report of the American College of Cardiology/
American Heart Association Task Force on Practice
Guidelines (Committee to Update the 1996 Guide-
lines on Perioperative Cardiovascular Evaluation for
Noncardiac Surgery). J Am Coll Cardiol 2002;39:
542–53.
[14] Guidelines for assessing and managing the periopera-
tive risk from coronary artery disease associated with
major noncardiac surgery. American College of Physi-
cians. Ann Intern Med 1997;127:309–12.
[15] Detsky AS, Abrams HB, Forbath N, Scott JG, Hilliard
JR. Cardiac assessment for patients undergoing non-
cardiac surgery: a multifactorial clinical risk index.
Arch Intern Med 1986;146:2131–4.
[16] Lee TH, Marcantonio ER, Mangione CM, et al.
Derivation and prospective validation of a simple in-
dex for prediction of cardiac risk of major noncardiac
surgery. Circulation 1999;100:1043–9.
[17] Grayburn PA, Hillis LD. Cardiac events in patients
undergoing noncardiac surgery: shifting the paradigm
from noninvasive risk stratification to therapy. Ann
Intern Med 2003;138:506–11.
[18] Boersma E, Poldermans D, Bax JJ, et al. Predictors of
cardiac events after major vascular surgery: role of
clinical characteristics, dobutamine echocardiography,
and beta-blocker therapy. JAMA 2001;285:1865–73.
[19] Kertai MD, Boersma E, Bax JJ, et al. Optimizing long-
term cardiac management after major vascular surgery:
role of beta-blocker therapy, clinical characteristics,
and dobutamine stress echocardiography to optimize
long-term cardiac management after major vascular
surgery. Arch Intern Med 2003;163:2230–5.
[20] Reul Jr GJ, Cooley DA, Duncan JM, et al. The effect
of coronary bypass on the outcome of peripheral vas-
cular operations in 1093 patients. J Vasc Surg 1986;3:
788–98.
[21] Crawford E, Morris GJ, Howell W, Moorhead D.
Operative risk in patients with previous coronary ar-
tery bypass. Ann Thorac Surg 1978;26:215–21.
[22] Eagle KA, Brundage BH, Chaitman BR, et al. Guide-
lines for perioperative cardiovascular evaluation for
noncardiac surgery. Report of the American College of
Cardiology/American Heart Association Task Force on
Practice Guidelines (Committee on Perioperative Car-
diovascular Evaluation for Noncardiac Surgery). J Am
Coll Cardiol 1996;27:910–48.
[23] Mason JJ, Owens DK, Harris RA, Cooke JP, Hlatky
MA. The role of coronary angiography and coronary
revascularization before noncardiac vascular surgery.
JAMA 1995;273:1919–25.
[24] Fleisher LA, Skolnick ED, Holroyd KJ, Lehmann HP.
Coronary artery revascularization before abdominal
aortic aneurysm surgery: a decision analytic approach.
Anesth Analg 1994;79:661–9.
[25] Mangano DT, Layug EL, Wallace A, Tateo I. Effect of
atenolol on mortality and cardiovascular morbidity
after noncardiac surgery. Multicenter Study of Peri-
operative Ischemia Research Group. N Engl J Med
1996;335:1713–20.
[26] Poldermans D, Boersma E, Bax JJ, et al. The effect of
bisoprolol on perioperative mortality and myocardial
infarction in high-risk patients undergoing vascu-
lar surgery. Dutch Echocardiographic Cardiac Risk
Evaluation Applying Stress Echocardiography Study
Group. N Engl J Med 1999;341:1789–94.
[27] Wallace A, Layug B, Tateo I, et al. Prophylactic ateno-
lol reduces postoperative myocardial ischemia. McSPI
Research Group. Anesthesiology 1998;88:7–17.
[28] Gottlieb SS, McCarter R, Vogel RA. Effect of beta-
blockade on mortality among high-risk and low-risk
patients after myocardial infarction. N Engl J Med
1998;339:489–97.
[29] Sprung J, Abdelmalak B, Gottlieb A, et al. Analysis
of risk factors for myocardial infarction and cardiac
mortality after major vascular surgery. Anesthesiology
2000;93:129–40.
[30] Roldan CA, Shively BK, Crawford MH. Value of the
cardiovascular physical examination for detecting
valvular heart disease in asymptomatic subjects. Am
J Cardiol 1996;77:1327–31.
[31] Abrams J. Approach to the patient with heart

preoperative anesthesia evaluation 315
murmurs. Philadelphia7 Lippincott Williams & Wil-
kins; 2000.
[32] Bonow R. ACC/AHA guidelines for the management
of patients with valvular heart disease: a report of
the American College of Cardiology/American Heart
Association. Task Force on Practice Guidelines (Com-
mittee on Management of Patients with Valvular Heart
Disease). J Am Coll Cardiol 1998;32:1486–8.
[33] Kearon C, Hirsh J. Management of anticoagulation
before and after elective surgery. N Engl J Med 1997;
336:1506–11.
[34] Heit JA. Perioperative management of the chronically
anticoagulated patient. J Thromb Thrombolysis 2001;
12:81–7.
[35] O’Keefe Jr JH, Shub C, Rettke SR. Risk of noncar-
diac surgical procedures in patients with aortic
stenosis. Mayo Clin Proc 1989;64:400–5.
[36] Torsher LC, Shub C, Rettke SR, Brown DL. Risk of
patients with severe aortic stenosis undergoing non-
cardiac surgery. Am J Cardiol 1998;81:448–52.
[37] Raymer K, Yang H. Patients with aortic stenosis:
cardiac complications in non-cardiac surgery. Can J
Anaesth 1998;45:855–9.
[38] Rodriguez RM, Pearl RG. Pulmonary hypertension and
major surgery. Anesth Analg 1998;87:812–5.
[39] Stoelting RK, Dierdorf SF. Valvular heart disease. In:
Stoelting RK, Dierdorf SF, editors. Anesthesia and
Co-Existing Disease. New York7 Churchill Living-
stone; 1993. p. 31.
[40] Thomas SJ, Lowenstein E. Anesthetic management of
the patient with valvular heart disease. Int Anesthesiol
Clin 1979;17:67–96.
[41] Meltzer S, Leiter L, Daneman D, et al. 1998 clinical
practice guidelines for the management of diabetes in
Canada. Canadian Diabetes Association. Can Med
Assoc J 1998;159(Suppl 8):S1–29.
[42] Jacober SJ, Sowers JR. An update on perioperative
management of diabetes. Arch Intern Med 1999;159:
2405–11.
[43] Narr B, Hansen T, Warner M. Preoperative laboratory
screening in healthy Mayo patients: cost-effective
elimination of tests and unchanged outcomes. Mayo
Clin Proc 1991;66:155–9.
[44] Durbridge TC, Edwards F, Edwards RG, Atkinson M.
Evaluation of benefits of screening tests done imme-
diately on admission to hospital. Clin Chem 1976;22:
968–71.
[45] Olsen DM, Kane RL, Proctor PH. A controlled trial
of multiphasic screening. N Engl J Med 1976;294:
925–30.
[46] Sandler G. Costs of unnecessary tests. Br Med J 1979;
2:21–4.
[47] Macpherson P, Teasdale E, McGeorge AP. Direct
puncture versus run up cervical myelography with
iopamidol: a comparison of side effects, EEG changes
and radiographic quality. J Neurol Neurosurg Psychia-
try 1983;46:959–62.
[48] Roizen M. The relative roles of the history and physi-
cal examination and laboratory testing in preoperative
evaluation for outpatient surgery: the Starling curve of
preoperative laboratory testing. Anesthesiol Clin North
Am 1987;5:15–34.
[49] Levinstein MR, Ouslander JG, Rubenstein LZ, For-
sythe SB. Yield of routine annual laboratory tests in
a skilled nursing home population. JAMA 1987;258:
1909–15.
[50] Roizen M. Preoperative Evaluation. In: Jaffe AR,
Samuels IS, editors. Anesthesiologists manual of sur-
gical procedures. 3rd edition. Philadelphia7 Lippincott
Williams & Wilkins; 2004. p. 743–72.
[51] Jaffe AR, Samuels IS. Anesthesiologist’s manual of
surgical procedures. 3rd edition. Philadelphia7 Lippin-
cott Williams & Wilkins; 2004.

Index
Note: Page numbers of article titles are in boldface type.
A
Acetylcholine receptor antibodies, in myasthenia
gravis, 288–289
Acova, in anticoagulation, after thoracic surgery, 255
Activated partial thromboplastin time, in anticoagu-
lated patients, 258–259
b-Agonists, and risk of cardiac disease, 266
Air leaks, after thoracic surgery, as contraindication
to early discharge, 223
Airway obstruction, myasthenia gravis and, 292
Ampicillin/sulbactam, for surgical site infections,
231–232
Amyotrophic lateral sclerosis, versus myasthenia
gravis, 291
Anesthesia, in thoracic surgery, cardiac assessment
for. See Cardiac assessment.
preoperative assessment for, 305–315
ASA classification in, 306–307
diabetes mellitus in, 313
goals of, 305
hypertension in, 307–308
myasthenia gravis in, 293
physician communication in, 306
setting for, 306
tests in, 313
timing of, 305
valvular heart disease in, 309, 311, 313
Angiomax, in anticoagulation, after thoracic surgery,
254–255
Antibiotics, for surgical site infections, 229–235
ampicillin/sulbactam, 231–232
CDC recommendations for, 233
cefazolin, 229–232
cefuroxime, 232
cephalexin, 234
cephalothin, 231
historical aspects of, 229–232
intraoperative, 233
mechanical ventilation and, 233
penicillin G, 231, 232
postoperative, 233
preoperative, 233
randomized studies of, 230–232, 234
Anticoagulated patients, 240, 241, 243–262
antiplatelet agents in, 245–246
bleeding potential in, assessment of, 257–259
clinical, 257–258
laboratory tests in, 258–259
coagulation system in, 243–245
direct thrombin inhibitors in, 240, 253–256
hirudin derivatives, 254
hirulogs, 254–255
small-molecule, 255–256
factor Xa inhibitors in, 250–251
hypercoagulability in, and venous thromboembo-
lism, 259
indirect thrombin inhibitors in, 247–253
low-molecular-weight heparin, 240, 241, 250
complications of, 249
dose and administration of, 248–249
pharmacology and mechanism of action of,
247–248
reversing action of, 256
unfractionated heparin, 240, 241, 247–249
complications of, 249
dose and administration of, 248
pharmacology and mechanism of action of,
247–248
reversing action of, 256
warfarin in, 251–253
complications of, 253
dose and administration of, 252–253
pharmacology and mechanism of action of,
251–252
reversing action of, 256–257
Antidepressants, in smoking cessation, 192
Antiplatelet agents, in anticoagulation, after thoracic
surgery, 245–246
1547-4127/05/$ – see front matter D 2005 Elsevier Inc. All rights reserved.
doi:10.1016/S1547-4127(05)00051-4 thoracic.theclinics.com
Thorac Surg Clin 15 (2005) 317–322

Aortic stenosis, anesthetic risks of, 311, 313
Argatroban, in anticoagulation, after thoracic
surgery, 255
Arixtra, in anticoagulation, after thoracic surgery,
250–251
Arterial blood gas analysis, before lung resection, 298
Arterial thrombosis, in anticoagulated patients, 249
Aspirin, in anticoagulation, after thoracic surgery,
245–246
Atenolol, to reduce risk of cardiac complications, of
thoracic surgery, 271
Azathioprine, for myasthenia gravis, 291
B
Barium esophagogram, before esophageal
surgery, 278
Biopsy, endoscopic, before esophageal surgery, 278
lung, thoracoscopic, early discharge after, 222
Bisoprodol, to reduce risk of cardiac complications,
of thoracic surgery, 271–272
Bivalirudin, in anticoagulation, after thoracic surgery,
254–255
b-Blockers, to reduce risk of cardiac complications,
of thoracic surgery, 309
Botulism, versus myasthenia gravis, 290
Brainstem disorders, versus myasthenia gravis,
290–291
Bronchoscopy, to stage esophageal cancer, 282
Bupropion, in smoking cessation, 192
C
Calcium channel blockers, to reduce risk of cardiac
complications, of thoracic surgery, 272
Cancer, pre-existing, as risk factor, for pulmonary
embolism, 237–238
Cardiac assessment, before esophageal surgery, 283
before thoracic surgery, 263–275, 308–309
chronic obstructive pulmonary disease and,
265–266
clinical predictors of risk in, 268
effects of anesthesia, 264–265
clinical features of, 265
induction agents, 264
narcotic-based, 264–265
neuromuscular blockade, 264
volatile agents, 265
effects of surgery on cardiovascular system,
263–264
exercise tests in, 270, 301
guidelines for, 266, 268–269
inhaled b-agonists and, 266magnetic resonance imaging in, 269–270
risk reduction in, 271–272
pharmacologic, 271-272
revascularization in, 271
surgery-specific risk in, 269
Cardiac disease, anesthetic risks of, 308–309
myasthenia gravis and, 292
Cardiopulmonary exercise tests, before lung
resection, 301
Cardiovascular function, cigarette smoke and,
189–190
Cephalosporins, for surgical site infections.
See Antibiotics.
Chest physiotherapy, in preoperative pulmonary
rehabilitation, 209
Chronic obstructive pulmonary disease, and risk of
cardiac disease, 265–266
Clonidine, in smoking cessation, 192
Clopidogrel, in anticoagulation, after thoracic
surgery, 246
Computed tomography, to stage esophageal cancer,
280–281
Coronary artery bypass grafts, before non-cardiac
surgery, 308–309
preoperative pulmonary rehabilitation in, 206
Cyclosporine, for myasthenia gravis, 291
D
Deep venous thrombosis, and pulmonary embolism.
See Pulmonary embolism.
Depression, versus myasthenia gravis, 291
Diabetes mellitus, anesthetic risks of, 313
Diet, preoperative patient education on, 197
Diffusion capacity, assessment of, before lung
resection, 298
Dipyridamole, in anticoagulation, after thoracic
surgery, 246
Direct thrombin inhibitors.
See Anticoagulated patients.
INDEX318

E
Eaton-Lambert syndrome, versus myasthenia
gravis, 291
Edrophonium test, for myasthenia gravis, 290
Electromyography, of myasthenia gravis, 289–290
Emphysema, lung volume reduction surgery for,
preoperative assessment for, 302
preoperative patient education on, 198–199
preoperative pulmonary rehabilitation in,
204–205
Empyema, after thoracic surgery, prevention of, 232
Endoscopic biopsy, before esophageal surgery, 278
Endoscopic ultrasonography, to stage esophageal
cancer, 282
Epidural analgesia, after thoracic surgery, 223
Esophageal cancer, staging of. See
Esophageal surgery.
Esophageal surgery, mode of resection and
reconstruction in, 283–284
patient selection for, 282–283
preoperative preparation for, 277–285
barium esophagogram in, 278
endoscopic biopsy in, 278
esophagectomy for cancer, 280
manometry in, 278–279
pH monitoring in, 279
staging esophageal cancer, 280–282
bronchoscopy in, 282
computed tomography in, 280–281
endoscopic ultrasonography in, 282
positron emission tomography in, 281–282
Esophagectomy, preoperative patient education
on, 199
Exercise tests, in cardiac assessment, before lung
resection, 301
before thoracic surgery, 270
Exercise training, in preoperative pulmonary
rehabilitation, 208–209
F
Factor Xa inhibitors, in anticoagulation, after thoracic
surgery, 250–251
Fondaparinux, in anticoagulation, after thoracic
surgery, 250–251
G
Gastroesophageal reflux disease, surgery for, preop-
erative preparation for. See Esophageal surgery.
H
Hemorrhage, in anticoagulated patients, 249
Heparin. See Anticoagulated patients.
Hirudin derivatives, in anticoagulation, after thoracic
surgery, 254
Hirulogs, in anticoagulation, after thoracic surgery,
254–255
Hypertension, anesthetic risks of, 307–308
I
Immunoglobulin, intravenous, for myasthenia
gravis, 292
Immunosuppressive drugs, for myasthenia
gravis, 291
Imuran, for myasthenia gravis, 291
Indirect thrombin inhibitors. See
Anticoagulated patients.
Induction agents, in thoracic surgery, cardiac assess-
ment for, 264
Infections, after thoracic surgery, as contraindication
to early discharge, 224
surgical site, antibiotics for. See Antibiotics.
Intermittent pneumatic compression, to prevent
pulmonary embolism, after thoracic surgery,
239–240
International Normalized Ratio, in anticoagulated
patients, 258–259
Inversine, in smoking cessation, 192–193
J
‘‘Jitter test,’’ for myasthenia gravis, 289–290
‘‘Jolly test,’’ for myasthenia gravis, 289
K
Kearns-Sayre syndrome, versus myasthenia
gravis, 291
Kefzol, for surgical site infections, 229–232
L
Lepirudin, in anticoagulation, after thoracic
surgery, 254
Lobectomy, preoperative patient education on, 198
INDEX 319
Low-molecular-weight heparin. See
Anticoagulated patients.
Lung biopsy, thoracoscopic, early discharge
after, 222
Lung cancer, resection of, preoperative assessment
for. See Lung resection.
Lung resection, preoperative assessment for,
297–304
arterial blood gas analysis in, 298
cardiac disease in, 298
diffusion capacity in, 298
exercise tests in, 301
lung volume reduction surgery, 302
occupational and travel history in, 297
patient’s activity level in, 297
prediction of postoperative function in,
298–301
prior or active infections in, 297–298
prior thoracic surgery in, 298
smoking cessation in, 297
spirometry in, 298
underlying parenchymal disorder in, 298
preoperative patient education on, 198
preoperative pulmonary rehabilitation in,
205–206
Lung volume reduction surgery, preoperative
assessment for, 302
preoperative patient education on, 198–199
preoperative pulmonary rehabilitation in,
204–205
M
Magnetic resonance imaging, in cardiac assessment,
before thoracic surgery, 269
Manometry, before esophageal surgery, 278–279
Mecamylamine, in smoking cessation, 192–193
Mitral stenosis, anesthetic risks of, 313
Muscle-sparing thoracotomy, early discharge
after, 222
Myasthenia gravis, 287–295
acetylcholine receptor antibodies in, 288–289
and anesthesia, 293
cardiac disease with, 292
classification of, 289
clinical features of, 287
diagnosis of, 289–290
electromyography in, 289–290
radioimmunoassays in, 290
Tensilon test in, 290
differential diagnosis of, 290–291
management of, 291–293
immunosuppressive drugs in, 291
intravenous immunoglobulin in, 292
plasmapheresis in, 292
pyridostigmine in, 291
steroids in, 291
thymectomy in, 293
physical examination for, 287–288
upper airway obstruction in, 292
with thyroid disorders, 292
N
Narcotic-based anesthesia, in thoracic surgery,
cardiac assessment for, 264–265
Neuromuscular blockade, in thoracic surgery, cardiac
assessment for, 264
Nicotine replacement therapy, in smoking
cessation, 192
Nortriptyline, in smoking cessation, 192
Nosocomial pneumonia, after thoracic surgery, as
contraindication to early discharge, 224
prevention of, 232
Nutrition, preoperative patient education on, 197, 283
P
Pain management, inadequate, after thoracic surgery,
as contraindication to early discharge, 223
preoperative patient education on, 196–197
Penicillin G, for surgical site infections, 231, 232
Penicillinase, and myasthenia gravis syndrome, 290
pH monitoring, before esophageal surgery, 279
Photodynamic therapy, preoperative patient education
on, 199
Physiotherapy, chest, in preoperative pulmonary
rehabilitation, 209
Plasmapheresis, for myasthenia gravis, 292
Pneumatic compression stockings, to prevent pulmo-
nary embolism, after thoracic surgery, 239
Pneumonectomy, preoperative patient education
on, 198
Pneumonia, after thoracic surgery, as contraindication
to early discharge, 224
prevention of, 232
INDEX320

Positron emission tomography, to stage esophageal
cancer, 281–282
Prednisone, for myasthenia gravis, 291
Protamine, to reverse anticoagulation, after thoracic
surgery, 256–257
Psychoneuroses, versus myasthenia gravis, 291
Pulmonary assessment, before esophageal surgery, 283
Pulmonary embolism, after thoracic surgery, 237–242
prevention of, 239–241
guidelines for, 240–241
mechanical techniques for, 239–240
pharmacologic techniques for.
See Anticoagulated patients.
risk factors for, 237–239
pre-existing cancer, 237–238
Pulmonary function, cigarette smoke and, 189
Pulmonary rehabilitation, before thoracic surgery,
203–211
chest physiotherapy in, 209
coronary artery bypass graft, 206
education in, 209
exercise training in, 208–209
goals and proposed benefits of, 203–204
lung resection, 205–206
lung volume reduction surgery, 204–205
outcomes assessment in, 210
patient selection for, 206–207
psychosocial support in, 209–210
pulmonary evaluation in, 207–208
setting for, 204
smoking cessation in. See Smoking cessation.
transplantation, 205
upper abdominal, 206
Pyridostigmine, for myasthenia gravis, 291
R
Radioimmunoassays, for myasthenia gravis, 290
Respiratory hygiene, preoperative patient education
on, 196
S
Small-molecule direct thrombin inhibitors, in
anticoagulation, after thoracic surgery, 255–256
Smoking cessation, before thoracic surgery,
189–194, 197, 206, 207, 297
and early discharge, 221–222
bupropion in, 192
clonidine in, 192
counseling in, 191–192
effects of cigarette smoke, 189–190
on cardiovascular function, 189–190
on pulmonary function, 189
on wound healing, 190
mecamylamine in, 192–193
nicotine replacement therapy in, 192
nortriptyline in, 192
in perioperative period, 191
Spirometry, before lung resection, 298
Steroids, for myasthenia gravis, 291
Surgical site infections, antibiotics for.
See Antibiotics.
T
Tensilon test, for myasthenia gravis, 290
Thienopyridines, in anticoagulation, after thoracic
surgery, 246
Thoracic surgery, early discharge after, 221–228
clinical pathways in, 224–226
contraindications to, persistent air leaks,
223–224
pulmonary infections, 224
muscle-sparing thoracotomy and, 222
pain management and, 223
preoperative education and, 222
preoperative smoking cessation and, 221–222
social factors in, 224
video-assisted thoracoscopic surgery and, 222
in anticoagulated patients.
See Anticoagulated patients.
informed consent in, 213–219
causation in, 216–217
damages and, 217
exceptions to, 217–218
historical aspects of, 213–214
physician’s legal duty: materiality, 214–216
practical aspects of, 217
patient education before, 195–201
audiovisual materials in, 200–201
for esophagectomy, 199
for lung resection, 198
for lung volume reduction surgery, 198–199
for photodynamic therapy, 199
for research protocols, 199–200
for thoracoscopy, 198
for transplantation, 199
on contact numbers, 198
on diet and nutrition, 197, 283
INDEX 321
on pain management, 196–197
on respiratory hygiene, 196
on smoking cessation. See Smoking cessation.
on wound care and drains, 197
postdischarge social issues, 197–198
verbal instructions in, 200
Web-based materials in, 200
written instructions in, 200
preoperative assessment for, cardiac.
See Cardiac assessment.
lung resection. See Lung resection.
preoperative pulmonary rehabilitation in.
See Pulmonary rehabilitation.
pulmonary embolism after.
See Pulmonary embolism.
smoking cessation before. See Smoking cessation.
surgical site infections after, antibiotics for.
See Antibiotics.
Thoracoscopic lung biopsy, early discharge
after, 222
Thoracoscopy, preoperative patient education
on, 198
Thoracotomy, muscle-sparing, early discharge
after, 222
Thrombocytopenia, in anticoagulated patients, 249
Thymectomy, for myasthenia gravis, 293
Thyroid disease, versus myasthenia gravis, 291
with myasthenia gravis, 292
Ticlopidine, in anticoagulation, after thoracic
surgery, 246
Transplantation, preoperative patient education
on, 199
preoperative pulmonary rehabilitation in, 205
U
Ultrasonography, endoscopic, to stage esophageal
cancer, 282
Unasyn, for surgical site infections, 231–232
Unfractionated heparin. See Anticoagulated patients.
Upper abdominal surgery, preoperative pulmonary
rehabilitation in, 206
V
Valvular heart disease, anesthetic risks of, 309,
311, 313
Vena cava filters, to prevent pulmonary embolism,
after thoracic surgery, 240
Venous thrombosis, in anticoagulated patients, 249
Ventilatory muscle training, in preoperative
pulmonary rehabilitation, 209
Video-assisted thoracoscopic surgery, early discharge
after, 222
Vitamin K, to reverse anticoagulation, after thoracic
surgery, 256
W
Warfarin. See Anticoagulated patients.
Water seal, for persistent air leaks, after thoracic
surgery, 223
Wound care, preoperative patient education on, 197
Wound healing, cigarette smoke and, 190
X
Ximelagatran, in anticoagulation, after thoracic
surgery, 255–256
INDEX322