preeclampsia: what’s old is new again · • pregnancy induced hypertension ... • eclampsia •...
TRANSCRIPT
Preeclampsia: What’s old is new again
Gene Chang, MDMaternal Fetal Medicine
Objectives
• Define Preeclampsia
• Review current guidelines
• Role of proteinuria
• Timing of delivery
• Seizure prevention
• Severe Hypertension


Real Disclosure
• Love-Hate Relationship with the new guidelines
• Preeclampsia as dichotomous disorder
• Gestational HTN doesn’t get respect
• Change for sake of change
• Absence of “real world” providers

High PassPass
Marginal
Fail
Honors ABCDF
Preeclampsia• 60 Different names in English/40 in German
• Preeclampsia (Mild vs Severe)
• Pregnancy induced hypertension
• Preclampsia (Mild vs Severe)
• Gestational Hypertension
• Preeclampsia (without severe features vs severe)
• Gestational Hypertension

Pre-eclampsia

Rationale• Incidence increasing
• 50-60,000 deaths worldwide annually
• In US for every death, 50-100 “near-misses”
• Less than optimal care in up to 80%
• Severe maternal complications
• Identification of severe preeclampsia
• Remains difficult
Callaghan t al Am J Obstet Gynecol 2008Kuklina et al. Obstet Gynecol 2009Van Dillen et al. BJOG 2010

What is preeclampsia?
“In pregnancy, the onset of drowsy headaches with heaviness is bad”
Coacae Praenontiones, XXXI, No 523

Preeclampsia Defined
• Pregnancy Specific Hypertensive disorder
• Multisystem involvement
• Variable expression
• New onset HTN + Proteinuria
• Proteinuria is/was the critical finding
• Management based on this finding

Pre-eclampsia
HTN
Proteinuria
Edema
HTN
Proteinuria
HTN
+/- Proteinuria
Everything Else

Classification
• Mild Preeclampsia
• “Never Mild”
• Increased mortality
• Increased morbidity
• Rapid progression

Classification
• Mild preeclampsia false sense of security
• Preeclampsia without severe features
• Preecampsia with severe features

Classification
No Acute Maternal/Fetal Complications Severe Maternal/Fetal Outcomes
Mild Severe
Term Delivery Baby fine
Near term DeliveryProlonged stay
Previable deliveryPerinatal death
Near term deliveryNICU stay
Long-term morbidity
Term SVDMom fine
Cesarean Section
Cesarean ComplicationsHTN urgency
EclampsiaMaternal Death

Hypertension
• New-onset HTN in 2nd trimester
• BP measurement
• Seated
• Arm supported at level of right atrium
• Left lateral falsely lowers BP


Proteinuria
• International guidelines typically support 300mg
• Origin of this number is unclear
• Upper 95% Confidence limit: 260mg/24h1
• Threshold of 500mg/24hr or PCR 0.5
• Possibly better predictor of outcome
• Relevant for outcome and/or hospitalization
1. Higby et al. Am J Obstet Gynecol 1994

Systematic Review
• Thangaratinam et al BMC 2009
• Systematic Review
• Proteinuria as predictor for maternal/fetal complications
• Proteinuria poor predictor
Systematic Review
• Proteinuria poor predictor of complications
• Maternal outcomes studied
• HELLP Syndrome
• Abruption
• Eclampsia
• Small but significant increase in IUFD, SGA, NICU
PIERS
Predetermined guidelines for assessment and managementContinuous Quality Improvement Project
Proteinuria doesn’t singly predict adverse outcome
JOGC 2011

• 946 women studied at risk for PreeclampsiaNested case-control study VIP
• Four groups comparedP300 (300-499 mg/24hr)P500 (>500 mg/24h)GHTNCHTN
PLoS One 2013

0
5
10
15
20
25
30
35
Severe HTN IV Meds Elevated Cr ICU Admit
CHTN
GHTN
U300
U500
*
*

Preeclampsia vs GHTN
• GHTN ≠ Preeclampsia
• Decision to use MgSO4
• Timing of delivery
• Gestational HTN may give false sense of security
748 pts with GHTN 24-35 w46% Progressed to Preeclampsia
9.6% Severe Preeclampsia
Barton AJOG 2001

Proteinuria • Important but not that important
• Should not be sole trigger for delivery <34w
• Reflects what many already do
• ? in patients 34-37w
• Pt w/controlled BP on Labetalol and 5gm/24hr
• Pt w/nonsevere HTN and 5gm/24hr

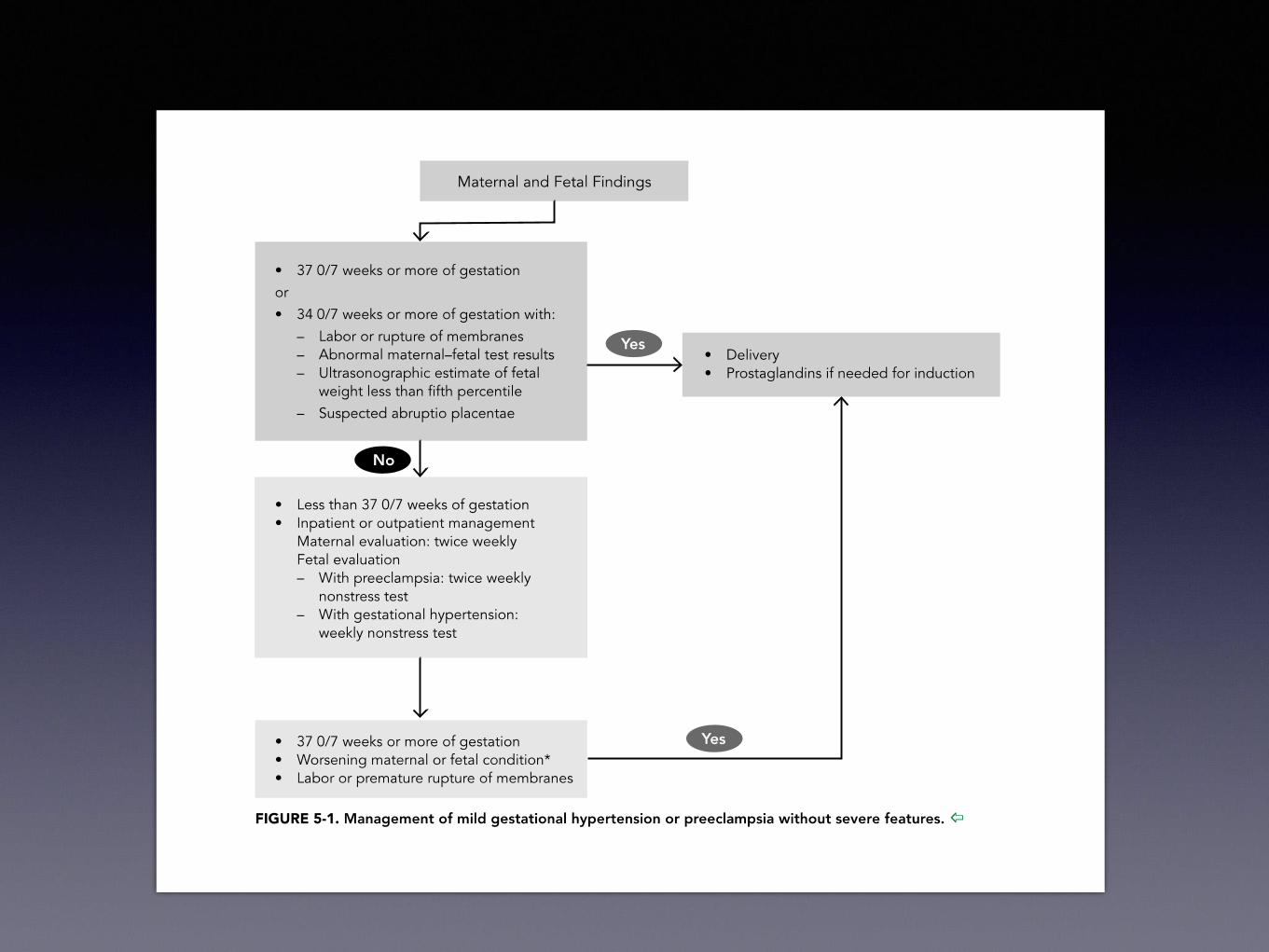
Timing of Delivery


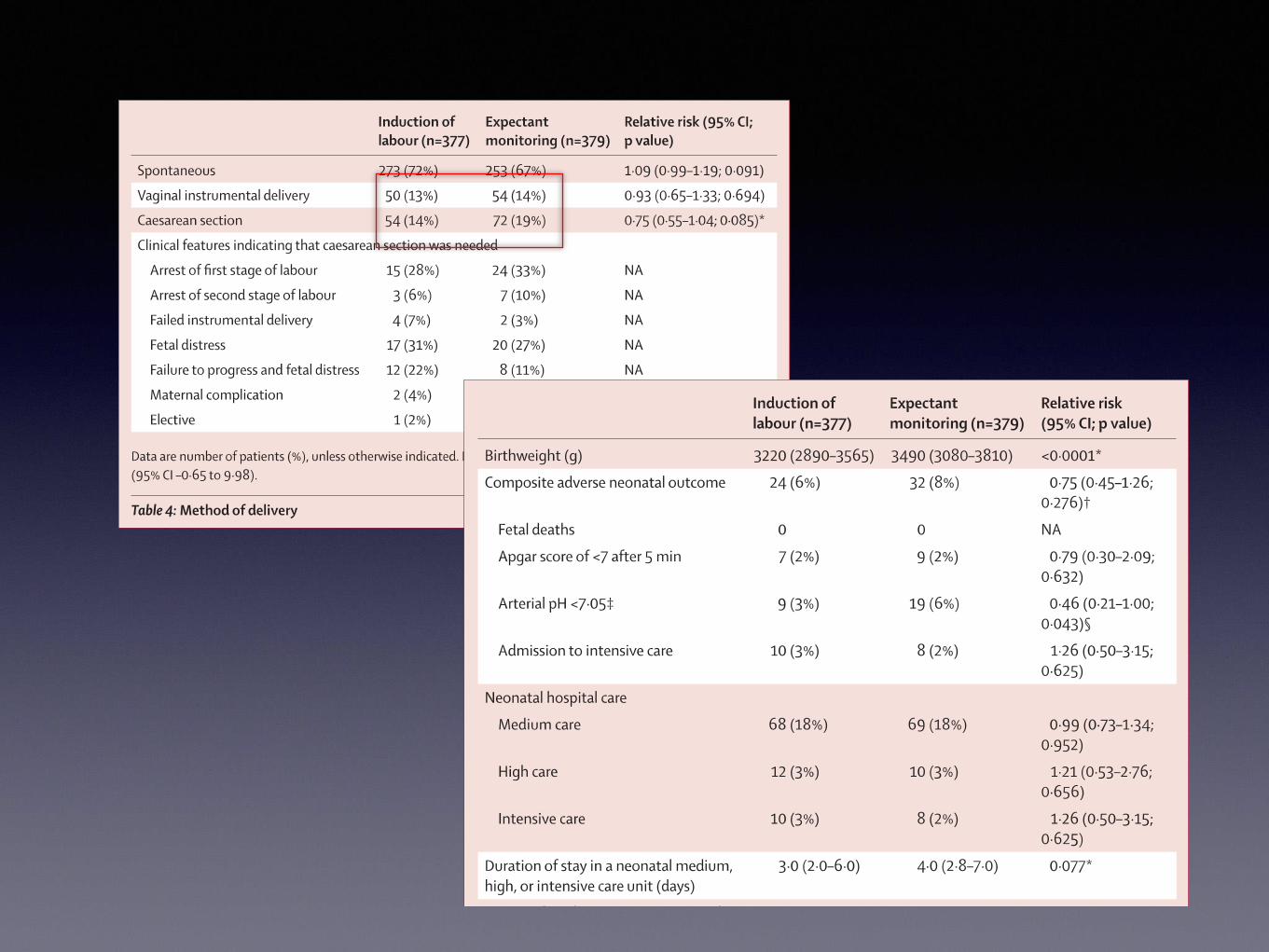
HYPITAT
• 36-41 weeks gestation
• Gestational HTN or Mild Preeclampsia
• Immediate delivery
• Expectant management
• Inpt or outpt

HYPITAT• Expectant group delivered for:
• HELLP
• >5g proteinuria
• Eclampsia
• NRFS
• PROM, MSAF
• >41w

HYPITAT• Primary outcome: composite morbidity
• Eclampsia
• HELLP
• VTE
• Pulmonary edema
• Abruption
• Progression to severe disease


To Mg or not to Mg?

MAGPIE Trial
Multicenter international trial10,141 randomizedHTN and 1+ protein

2 frontal/severe haEpigastric painBlurred visiionHyper-reflexia
Irrespective of BP or proteinuria



MAGPIE
• NNT for Severe Preeclampsia: 63
• NNT for Non-severe preeclampsi:a 91

Management of Severe Hypertension
Severe Hypertension
Hydralazine: drug of choice >45 years
• Onset slow (10-20 minutes)
• Dose: 5-10 mg q20 mins (max 30 mg)
• Mom: Tachycardia, Hypotension, HA
• Neonate: thrombocytopenia, low platelets

Hydralazine: Metanalysis
• Metanalysis of RCT’s 1966-2002
• Short acting antihypertensives
• 21 trials (893 women)
• 8 with Hydralazine v. Nifedipine
• 5 with Hydralazine v. Labetalol
BMJ 2003

Hydralazine: MetanalysisHydralazine:
• Hypotension (13 trials): 3.29 [1.50-7.23]
• C/S (14 trials): 1.30 [1.08-1.59]
• Abruption (5 trials): 4.17 [1.19-14.28]
• Oliguria (3 trials): 2.04 [1.32-3.16]
• Adverse effect on FHR (12 trials):
2.04 [1.32-3.16]
BMJ 2003

Severe Hypertension• Labetalol
• Continuous infusion (1 mg/kg)
• More commonly IV Bolus
• Initial bolus not > 20 mg
• Dose (40, 80, 80, 80) every 15 minutes
• Max dose 300 mg
• Onset: 5 min, Peak: 10-20 min, Duration 6 hrs.

Severe HypertensionNifedipine
• Oral Ca channel blocker
• Used for HTN and for tocolysis
• 10 mg PO q15-30 minutes (max 30 mg)
Long Acting Nifedipine?
• Absorption 70-90 minutes
• Onset of action 45-90 minutes
• Consensus: lower BP w/in 30-60 minutes

Labetalol vs. Nifedipine
Labetalol
• Advantages
• Significant hypotension uncommon
• No decrease in CO vs. B-blockers
• Disadvantages
• Many pts already taking labetalol
• 1% risk of arrhythmia
• 10 mg/min don’t need telemetry1
Frontiers in Bioscience 2007

Labetalol vs. NifedipineNifedipine
• Advantages
• Increases cardiac index1
• Minimal impact on uteroplacental blood flow
• Higher BP = Higher decrease2
• Selective renal arteriolar dilator3
• Disadvantages
• Concern over short-acting Nifedipine
• Risk of Interaction with MgSO4
1. Am J Ob Gyn 1999 2. Am J Med 1985 3. Nephrol Dial Transplant 1988

Labetalol vs. Nifedipine
Am J Ob Gyn 2005
Mg Toxicity requiring Calcium Gluconate 0.5% (n = 162)
Labetalol vs. Nifedipine
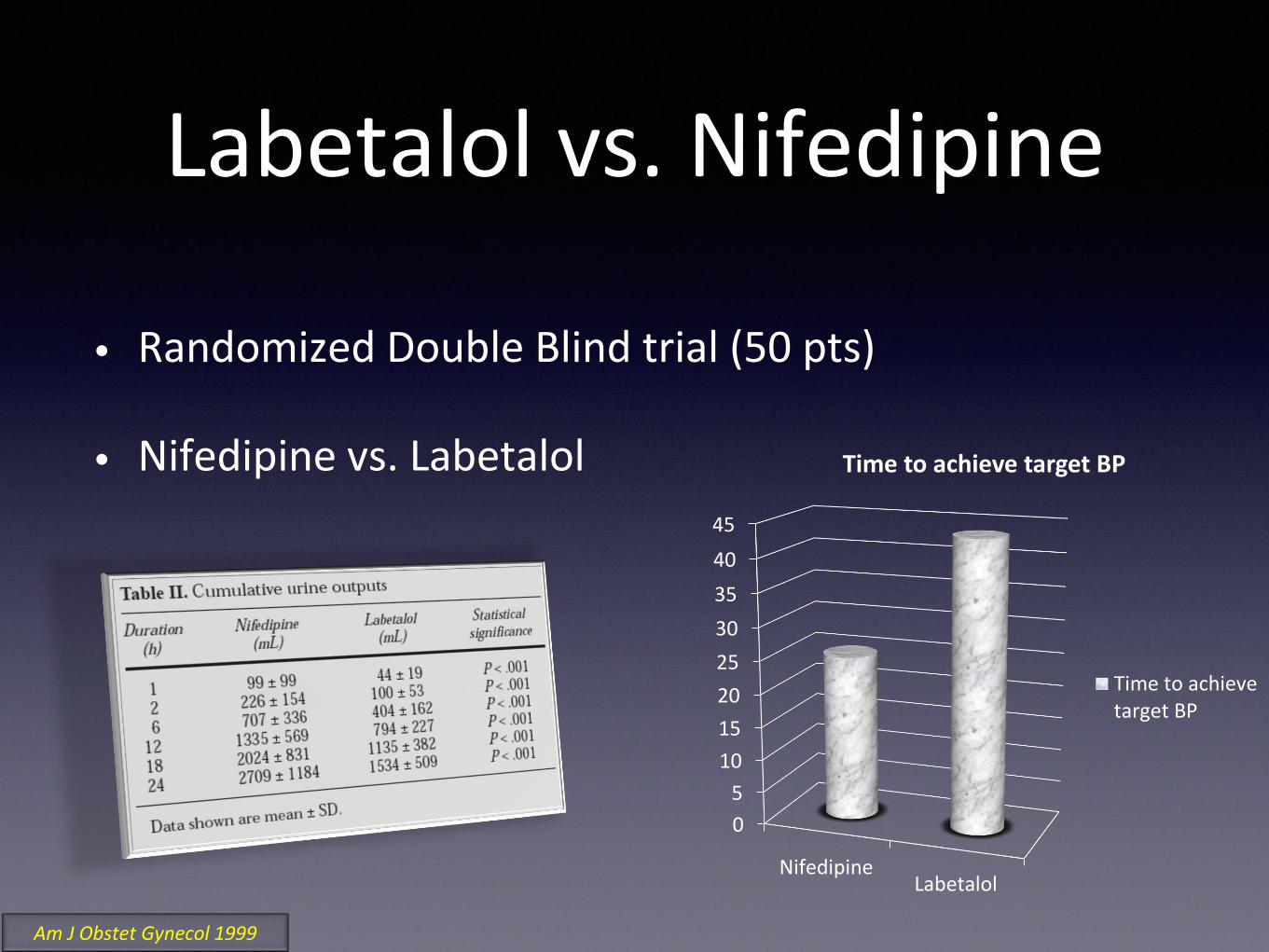
• Randomized Double Blind trial (50 pts)
• Nifedipine vs. Labetalol
0
5
10
15
20
25
30
35
40
45
NifedipineLabetalol
Time to achieve target BP
Time to achievetarget BP
Am J Obstet Gynecol 1999
Severe Hypertension
• 1st line agents
• Labetalol
• Nifedipine
• Avoid when: Known CV disease
• Age > 45 or IDDM > 15 years
• Hydralazine still a consideration
Severe Hypertension
Use what you are comfortable with
Use what is available

PP Management
PP: NSAIDS

NSAID’s and HTN
• Pope et al
• Meta-analysis of 54 trials with 123 trial arms
• 1324 pts mean age 46 (29-62)
• Mean duration of therapy 15d (1-42)
• Mean increase in MAP 3.74 mmHg
Pope et al. Arch Inter Med 1993

NSAID’s and HTN
• Johnson et al
• 50 RCT’s
• 771 subjects
• Mean age 47.6
• Duration of treatment at least 1w
• Map increased 5mmHg
Johnson AG et al. Arch Int Med 1994

NSAID’s and HTN
• Sheridan et al 2005
• Controlled observational study
• HTN on NSAID’s vs. unexposed
• 184 users vs. 762 nonusers
• No significant difference in SBP or DBP



PP: Followup
PP: Followup
• 0.3% PP visits to ER related to HTN disorders
• Symptoms precede stroke and preeclampsia
• Hours to days
• No knowledge regarding benefit of Rx

Conclusions
• Pre-eclampsia
• Multisystem disorder
• Variable presentation
• Trust your clinical assessment of patients

Conclusions
• Proteinuria- important but not important
• Seizure prevention- clinical decision
• Timing of delivery- HYPITAT
• Hypertension- Severe and PP