predictors of smoking cessation among pregnant women in san bernardino county
TRANSCRIPT

Running Head: PREDICTORS OF SMOKING CESSATION AMONG PREGNANT WOMEN
IN SAN BERNARDINO COUNTY
SCHOOL OF PUBLIC HEALTH | GLOBAL HEALTH DEPARTMENT
Loma Linda University
School of Public Health
FIELD PRACTICUM REPORT
Title:
Predictors of Smoking Cessation among Pregnant Women in San Bernardino County:
An Analysis and Evaluation of the Loma Linda Medical Center Perinatal Institute
Comprehensive Tobacco Treatment Program
Presented to the
LLU SPH Department of Global Health and Epidemiology
In partial fulfillment of the requirements for the MPH degree
By:
Temidayo O. Ogunrinu, B.S., MPH (c)
Date:
December 12, 2013
To Faculty Reader:
Pramil Singh, DrPH
Field Supervisor:
Gretchen Page RN, MPH, CNM
Manager, RPPC & CDAPP Programs

PREDICTORS OF SMOKING CESSATION AMONG PREGNANT WOMEN IN SAN
BERNARDINO COUNTY 2
Statement of Original Work
“I hereby declare that the field practicum submission is my own work and to the best of my knowledge it
contains no materials previously written or submitted to the Global Health Department by another
person, except where acknowledgment is made in the report. I also declare that the intellectual content of
this field practicum report is the product of my own work, except to the extent that assistance from others
in report design and formation, presentation, and linguistic expression is acknowledged.”
Student Signature: Temidayo Ogunrinu Date : December 11, 2013
PREDICTORS OF SMOKING CESSATION AMONG PREGNANT WOMEN IN SAN
BERNARDINO COUNTY 3
Table of Contents
Definition of Terms………………………………………………………………………... 4
Abstract…………………………………………………………………………………..... 5
Background……………………………………………………………………………....... 6
Aims……………………………………………………………………………………..… 9
Methods……………………………………………………………………………………. 9
Results……………………………………………………………………………………... 12
Discussion…………………………………………………………………………………. 17
Limitations………………………………………………………………………………… 18
Recommendations…………………………………………………………………………. 19
Evaluation of Field Practicum…………………………………………………………....... 19
References…………………………………………………………………………………. 23
Appendices………………………………………………………………………………… 24

PREDICTORS OF SMOKING CESSATION AMONG PREGNANT WOMEN IN SAN
BERNARDINO COUNTY 4
Definition of Terms
CTTP- Comprehensive Tobacco Treatment Program
FG- Focus Group
LLU-Loma Linda University
LBW-Low birth weight
PTB-Preterm birth
SIDS- Sudden Infant death syndrome
PREDICTORS OF SMOKING CESSATION AMONG PREGNANT WOMEN IN SAN
BERNARDINO COUNTY 5
Abstract
Maternal smoking has many adverse health outcomes, particularly on the unborn child. These
outcomes include low birth weight, sudden infant death syndrome and pre-term birth. Several
studies show that if mothers reach smoking cessation it will significantly decrease these birth
effects. San Bernardino County, the largest county in California has a high rate of maternal
smoking. Currently there is no comprehensive maternal smoking program that serves in this
county except for the Comprehensive Tobacco Treatment Program (CTTP). In 2013 a
retrospective cohort study was done on 233 participants who enrolled in this CTTP from 2012-
2013. Eighty-two percent of the participants who completed the program retain smoking
cessation at their last point of follow up. With these findings investigator sought to determine
which the characteristics made participants successful or unsuccessful in completing the
program. Quantitative analysis was carried out using SAS 9.3 to statistically determine women in
their first and third trimester are less likely to complete the program. Additionally, Whites and
Blacks, had a higher odds of non-completion as well as those who are younger in age. Major
themes in the Focus determined that family of maternal smokers should be incorporated and
more resources to support transportation to the program should be provided.

PREDICTORS OF SMOKING CESSATION AMONG PREGNANT WOMEN IN SAN
BERNARDINO COUNTY 6
Background
Maternal smoking during pregnancy is associated with numerous adverse health effects
particularly for unborn infants. These health effects include but are not limited to infant low birth
weight (LBW), sudden infant death syndrome (SIDS), preterm birth(PTB), and neurological and
cognitive delays which contribute to the increase in neonatal and infant mortality (Cnattingius,
2004). Despite smoking being one of the most modifiable risk factors for disease, the World
Health Organization (WHO) reported that the global maternal rate of smoking has skyrocketed to
12 million as of 2001 and increased to 200 million as of 2006 (Pregnets, n.d.) (WHO, 2001). In
addition, within the United States women smoked nearly the same rate as men and although
smoking rates have decreased among women as of 2004 an estimated 22% of women in
reproductive age smoked(WHO, 2001) (The 2004 united states surgeon general’s report: the
health consequences of smoking, 2004). In 2010 The Centers for Disease Control and
Prevention (CDC), Morbidity and Mortality Weekly Report (MMWR) reported that among 27
US States, 10.7% of women smoked the last trimester of their pregnancy. They also reported that
of the 10.7% of women who smoked during their pregnancy 54.3% quit while pregnant and
15.9% continued to smoke after delivery (MMWR, 2010).
The California Department of Public Health (CDPH) reported their maternal smoking
prevalence was 8.1% which compared to the national average of 10.7% is lower. This was
assessed using the Maternal and Health Assessment (MIHA) Survey, an annual population-based
survey of women with a live births (CDPH, 2011).
In 2007 and 2008 a study carried out in San Bernardino County identified a total of 2,785
mothers who smoked during pregnancy using de-identified birth cohort files. The study found

PREDICTORS OF SMOKING CESSATION AMONG PREGNANT WOMEN IN SAN
BERNARDINO COUNTY 7
that the prevalence of maternal smoking was 6.3% while smoking cessation was 2.0% (Batech,
et al, 2013). In 2010 The MIHA survey also determined that within San Bernardino County there
has been no decline, rather the prevalence of maternal smoking has increased to 8.8%. Although
San Bernardino County does not have the highest percentage of maternal smoking, it is higher
than the California average of 8.1% (CDPH. 2011).
Researcher such as Batech studied that maternal smoking cessation significantly lowers
the risk of LBW, SIDS and PTB (Batech, et al, 2013). Unfortunately, smoking cessation and
relapse prevention are a challenge for many. Some are successful without the use of evidence-
based cessation treatments but others may need these interventions. Such proven interventions
include:
Brief clinical interventions (i.e., when a doctor takes 10 minutes or less to deliver advice
and assistance about quitting)
Counseling (e.g., individual, group, or telephone counseling)
Behavioral cessation therapies (e.g., training in problem solving)
Treatments with more person-to-person contact and intensity (e.g., more time with
counselors)
Cessation Medications (CDC, 2013).
Programs that include some or all of these aspects are useful and serve as a great need.
Currently, San Bernardino County has only one smoking cessation and relapse prevention
program. This program is a First 5 San Bernardino funded program developed by Loma Linda
University Medical Center/Children’s Hospital called the Comprehensive Tobacco Treatment
Program (CTTP). Their main objective is to accomplish smoking cessation and/or relapse
prevention among pregnant women who are currently smoking or have smoked cigarettes during

PREDICTORS OF SMOKING CESSATION AMONG PREGNANT WOMEN IN SAN
BERNARDINO COUNTY 8
the previous 6 months of enrolling in the program. This is an eight (8) week program that screens
pregnant women within selected sites in San Bernardino County. These sites include outpatient
clinics and rehabilitation homes. Once individuals enroll in the CTTP, health educators assess
their smoking status, risk for maternal depression and substance abuse use. An individualized
plan is developed which allows participants to set a quit date and other goals that will enable
their smoking cessation. The health educators provide each participant with health education
regarding tobacco use and the benefits of smoking cessation. The participants are then given
weekly incentives for every week they test negative to a urine tobacco test. The incentives
include diapers and xylitol gum. Once participants complete the program they are followed up at
3, 6 and 9 months.
Currently the CTTP serves 233 clients within several cities within San Bernardino
County. They have one form of evaluation which captures infant health outcomes such as LBW,
neurological and cognitive skills, and whether clients completed the program. However, they
have no evaluation that assess the efficacy of their program. In 2013 a School of Public Health
Student interned with the CTTP to evaluate the programs efficacy. She researched that there
were several studies which identified certain characteristics or predictors that make maternal
pregnant smokers more successful to quit and not relapse. These predictors include Socio-
demographics such as age, education level, marital status, social status, gestational age, parity,
level of smoking, willingness to quit, years of smoking, and partners smoking status and
ethnicity (Woodby, 1999) (Severson, Andrews, Lichtenstein, Wall, & Zoref, 1995). After
assessing the programs efficacy they wish to identify which of these characteristics or predictors
have the most significant impact on their participant’s success or lack of within the program.

PREDICTORS OF SMOKING CESSATION AMONG PREGNANT WOMEN IN SAN
BERNARDINO COUNTY 9
This analysis will allow them to modify the program toward individuals who are less likely to
complete yielding better success rates.
The specific project aims are:
1) To identify demographic, behavioral, and gestational variables associated with
successful completion of the CTT program.
2) To assess the efficacy of program enrollment on achieving smoking cessation or
relapse prevention at three or more months of follow-up.
3) To assess the efficacy of program completion on achieving smoking cessation or
relapse prevention at three or more months of follow-up.
Research Questions
1. What are the characteristics among the program population that predict program non-
completion?
Hypothesis 1: Those who have a willingness to quit as measured by smoking status at enrollment
are more likely to complete the program
Methods
To assess the efficacy of the CTTP and identify the predictors that contribute to
successful completion and non-completion, qualitative and quantitative data most be collected
and analyzed applying the skills utilized from epidemiology, biostatistics and global health
courses. A literature review was conducted before quantitative and qualitative methods began to
guide methodological framework and to ensure research is not contrary to similar and previous
studies carried out.
PREDICTORS OF SMOKING CESSATION AMONG PREGNANT WOMEN IN SAN
BERNARDINO COUNTY 10
Qualitative
A focus group (FG) guide was created in collaboration with the CTTP staff. This can
found in Appendix A. The FG guide was intended to uncover 5 key themes; participants smoking
backgrounds, barriers or challenges participants faced towards their smoking cessation, areas of
CTTP program effectiveness that contributed to their smoking cessation, aspect of the program
that had the biggest impact and areas the programs can improve in. Flyers inviting participants to
join the FG were created and distributed at each site except Spanish speaking cites. Those
interested were instructed to RSVP so that enough incentives and refreshments could be planned
accordingly. The FG took place at the Mountain View Plaza (MVP), which is the home of the
CTTP. The FG was conducted with a facilitator and a note taker. All questions in the focus group
were open ended and discussion based. The FG was recorded and the participants were
instructed that the FG would be kept confidential. Each client signed a consent form. A copy of
the consent form can be found in Appendix B.
Data analysis
Following the focus group the tape recording was transcribed verbatim. Additional notes
from the note taker were also compiled together to assist with the analysis. To analyze the
transcription an A priori code book was created to identify the most essential emerging themes
concerning. The code book can be found in Appendix C.
Quantitative
Study population
The current study is based on a cohort of 233 pregnant women from the county of San
Bernardino enrolled in the CTTP program between 2012 and 2013. Twenty two participants with
missing data on program completion status were excluded from the analysis.

PREDICTORS OF SMOKING CESSATION AMONG PREGNANT WOMEN IN SAN
BERNARDINO COUNTY 11
Program completion data
Subjects were designated to have completed the program if they stayed quit for 8 cumulative
weeks. In addition regardless of their completion status, subject was contacted at 3, 6 and 9 months
interval and their smoking status (yes/no) was assessed.
Covariates
Gestational age was categorized into trimesters, women with gestational age <13 were
classified in the first trimester; those between 13 and 28 were classified as second trimester and
those above 28 as third trimester. Smoking status at enrollment indicates whether the participant
was still smoking or not on the day of program enrollment. The race variable had the following
four levels: Asians, Blacks, Hispanics and Whites. Age was used as a continuous variable.
Statistical analysis
Simple logistic regression was used to assess the effect of individual socio-demographic
variables on program completion. Two multiple logistic regression analysis were conducted; the
first assessed the effect of smoking status at enrollment age race on program completion. The
second analysis looked at the adjusted effects of gestational age race and age on program
completion. All the analysis was done with SAS 9.3.
Results
Qualitative
The FG revealed that each of the participants had a long history of smoking starting in
their teenage years and even as young as nine years old. For most of the participants, peer
pressure from friends or family is what triggered their initial smoking. Drugs and alcohol also
played a huge role in their smoking habits. Each of the participants had stopped smoking
between one month and one week prior of starting the program. Additionally, they each had
PREDICTORS OF SMOKING CESSATION AMONG PREGNANT WOMEN IN SAN
BERNARDINO COUNTY 12
attempted to quit smoking at one point before they started the CTTP program. They all
completed the program. The majority of the participants felt that their experience with the CTTP
program was positive experience. They all felt that the educational materials used were relevant
and made a significant impact for them to not smoke. The incentives played a role, but was not
biggest role in their smoking cessation. However the motivation the health educators gave them
did. The biggest motivating factor was wanting to be alive and healthy for their children which
they all expressed that the CTTP program helped them realize. Because the majority of these
participants where either in a live in facility or where patients at Loma Linda Medical Center, or
the diabetes center they all felt that it was very convenient to see the health educators. The only
concern came from a participant who no longer was a client at a particular facility and did not
have adequate transportation to be seen at the Mountain View Plaza (MVP). This was expressed
as a barrier. Other participants expressed it would be beneficial to include family members
especially significant others in the program, so that they too could act as a motivator to quit
smoking. In addition if their partners were smokers it could help the both of them reach smoking
cessation.
Quantitative
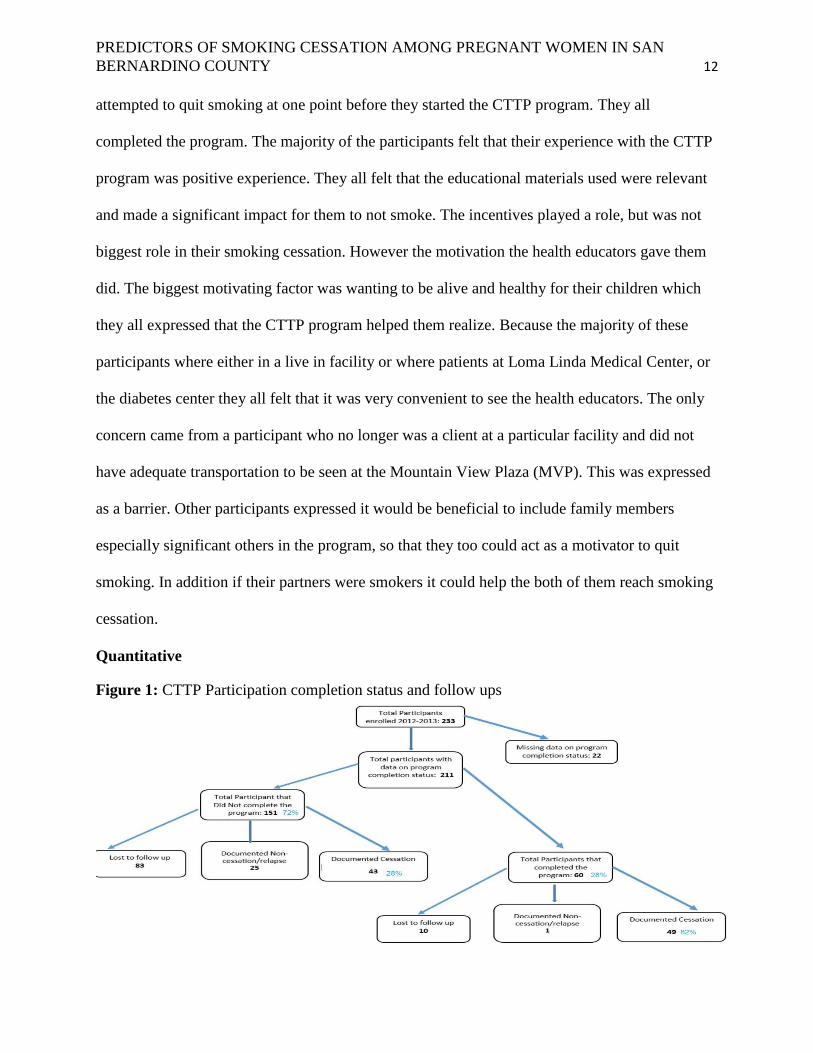
Figure 1: CTTP Participation completion status and follow ups

PREDICTORS OF SMOKING CESSATION AMONG PREGNANT WOMEN IN SAN
BERNARDINO COUNTY 13
Table 1: Demographic, Behavioral, and Gestational Variables among enrollees in the CTTP
Program (San Bernardino County, California) during 2012-2013.
N (%)
Age category
20 or younger 41(17.67)
21-25 96(41.38)
26-30 50(21.55)
31 or older 45 (19.4)
Total 232
Gestational age at enrollment
First trimester 32(14.04)
Second trimester 89 (39.04)
Third trimester 107 (46.93)
Total 228
Race/Ethnicity
Asian/Other 15 (6.47)
Hispanic 107(46.12)
NH Black 38(16.38)
NH White 72 (31.03)
Total 232
Education
9th Grade or less 61(34.66)
High school graduate 64 (36.36)
College education or more 51 (28.98)
Total 176
Income
Less than $10,000 69(51.49)
$10,000-$25,000 40 (29.85)
More than $25,000 25(18.66)
Total 134
Single parent No Yes
No 65 37.14
Yes 110 62.86
Total 175
Partner smokes No Yes
No 100 45.66
Yes 119 54.34

PREDICTORS OF SMOKING CESSATION AMONG PREGNANT WOMEN IN SAN
BERNARDINO COUNTY 14
Total 219
Number of cigarettes at enrollment No Yes
Quit 159 68.83
>= 1 Cigarette 72 31.17
Total 231
Drug use No Yes
No 140 76.5
Yes 43 23.5
Total 183
Alcohol use No Yes
No 96 52.46
Yes 87 47.54
Total
Smoking status at enrollment No Yes
No 153 67.7
Yes 73 32.3
Total 226
Number of pregnancies No Yes
1 or none 63 27.75
2 48 21.15
3 40 17.62
4 35 15.42
5 or more 41 18.06
Total 227
Number of children No Yes
None 80 35.09
1 60 26.32
2 39 17.11
3 or more 49 21.49
Total 228
Cite No Yes
L. Linda 78 33.62
H. Desert 76 32.76
S. Bernardino 54 23.28
Fontana/Rialto 24 10.34
Total 232

PREDICTORS OF SMOKING CESSATION AMONG PREGNANT WOMEN IN SAN
BERNARDINO COUNTY 15
Table 2: Univariable Odds Ratios relating selected variables to Program Non-completion among
enrollees in the CTTP Program (San Bernardino County, California) during 2012-2013.
95% Confidence limits
Age OR LL UL
20 or younger vs. 21-25 0.63 0.26 1.51
26-30 vs. 21-25 0.59 0.26 1.33
31 or older vs. 21-25 0.33 0.15 0.75
Race
Asian/Other vs. Hispanic 1.31 0.42 4.12
NH Black vs. Hispanic 2.84 1.07 7.52
NH White vs. Hispanic 3.93 1.75 8.85
Education
9th Grade or less vs. College education or more 1.64 0.72 3.70
High school graduate vs. College education or more 1.45 0.66 3.16
Income
$10,000-$25,000 vs. More than $25,000 1.05 0.37 2.98
Less than $10,000 vs. More than $25,000 1.77 0.67 4.67
Single parent
Yes vs. No 1.49 0.76 2.92
Partner smokes
Yes vs. No 1.59 0.86 2.94
Cite
Fontana/Rialto vs. L. Linda 0.76 0.28 2.04
H. Desert vs. L. Linda 1.64 0.73 3.68
S. Bernardino vs. L. Linda 0.57 0.26 1.22
Smoking at enrolment
Yes vs. No 3.17 1.44 6.95
Cigarettes
5 or less vs. Non smoker 2.17 0.84 5.62
More than 5 vs. Non smoker 4.68 1.36 16.18
Alcohol use
Yes vs. No 0.99 0.52 1.89
Drug use
Yes vs. No 1.65 0.72 3.78
Gestational age at enrolment
First trimester vs. Second trimester 4.04 1.28 12.72
PREDICTORS OF SMOKING CESSATION AMONG PREGNANT WOMEN IN SAN
BERNARDINO COUNTY 16
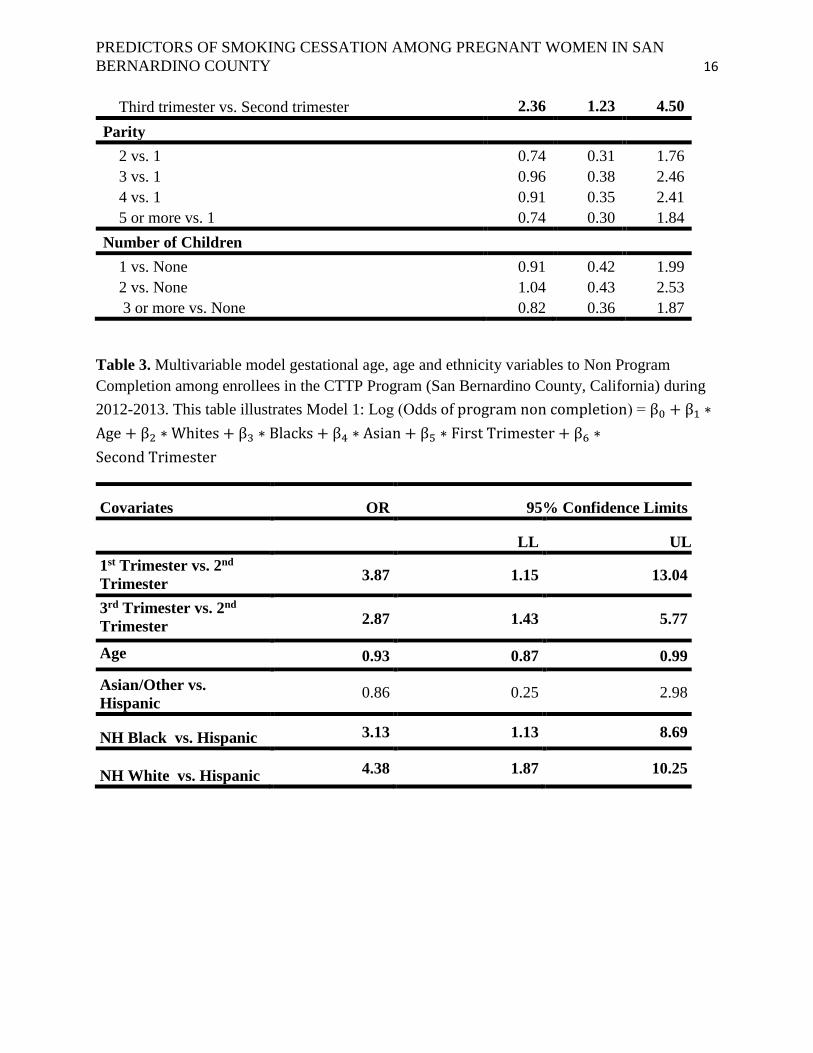
Table 3. Multivariable model gestational age, age and ethnicity variables to Non Program
Completion among enrollees in the CTTP Program (San Bernardino County, California) during
2012-2013. This table illustrates Model 1: Log (Odds of program non completion) = β0 + β1 ∗
Age + β2 ∗ Whites + β3 ∗ Blacks + β4 ∗ Asian + β5 ∗ First Trimester + β6 ∗
Second Trimester
Covariates OR 95% Confidence Limits
LL UL
1st Trimester vs. 2nd
Trimester 3.87 1.15 13.04
3rd Trimester vs. 2nd
Trimester 2.87 1.43 5.77
Age 0.93 0.87 0.99
Asian/Other vs.
Hispanic 0.86 0.25 2.98
NH Black vs. Hispanic 3.13 1.13 8.69
NH White vs. Hispanic 4.38 1.87 10.25
Third trimester vs. Second trimester 2.36 1.23 4.50
Parity
2 vs. 1 0.74 0.31 1.76
3 vs. 1 0.96 0.38 2.46
4 vs. 1 0.91 0.35 2.41
5 or more vs. 1 0.74 0.30 1.84
Number of Children
1 vs. None 0.91 0.42 1.99
2 vs. None 1.04 0.43 2.53
3 or more vs. None 0.82 0.36 1.87
PREDICTORS OF SMOKING CESSATION AMONG PREGNANT WOMEN IN SAN
BERNARDINO COUNTY 17
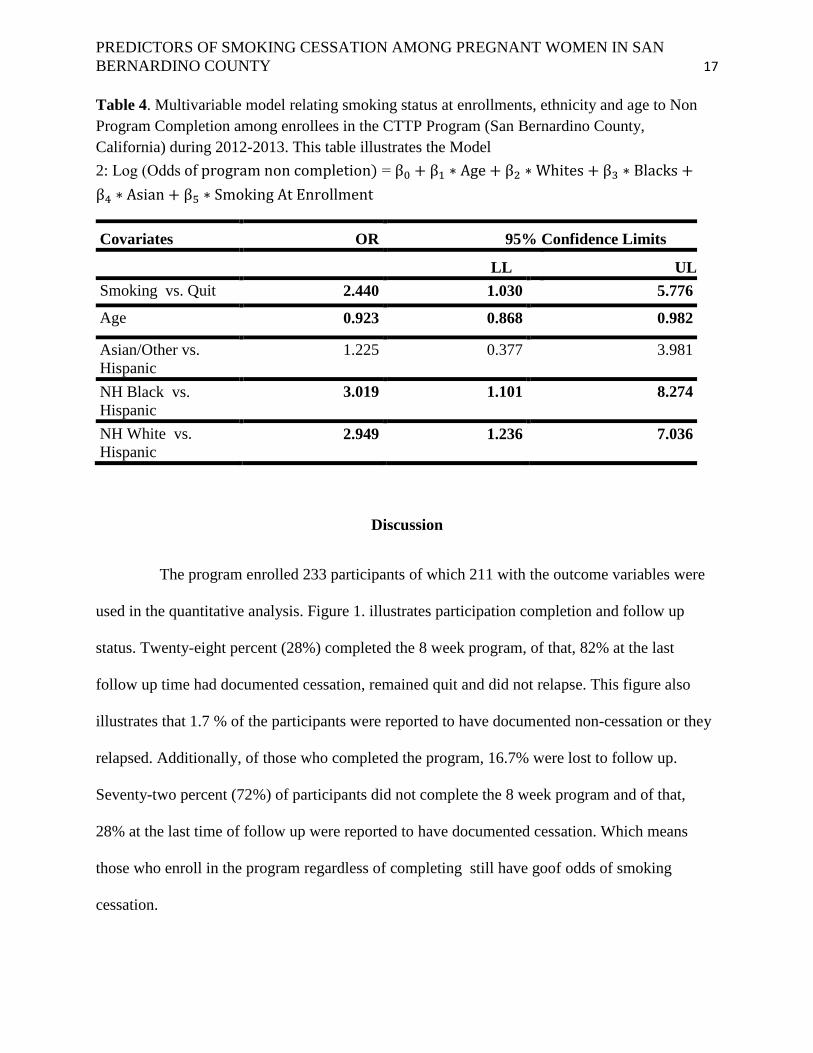
Table 4. Multivariable model relating smoking status at enrollments, ethnicity and age to Non
Program Completion among enrollees in the CTTP Program (San Bernardino County,
California) during 2012-2013. This table illustrates the Model
2: Log (Odds of program non completion) = β0 + β1 ∗ Age + β2 ∗ Whites + β3 ∗ Blacks +
β4 ∗ Asian + β5 ∗ Smoking At Enrollment
Covariates OR 95% Confidence Limits
LL UL
Smoking vs. Quit 2.440 1.030 5.776
Age 0.923 0.868 0.982
Asian/Other vs.
Hispanic
1.225 0.377 3.981
NH Black vs.
Hispanic
3.019 1.101 8.274
NH White vs.
Hispanic 2.949 1.236 7.036
Discussion
The program enrolled 233 participants of which 211 with the outcome variables were
used in the quantitative analysis. Figure 1. illustrates participation completion and follow up
status. Twenty-eight percent (28%) completed the 8 week program, of that, 82% at the last
follow up time had documented cessation, remained quit and did not relapse. This figure also
illustrates that 1.7 % of the participants were reported to have documented non-cessation or they
relapsed. Additionally, of those who completed the program, 16.7% were lost to follow up.
Seventy-two percent (72%) of participants did not complete the 8 week program and of that,
28% at the last time of follow up were reported to have documented cessation. Which means
those who enroll in the program regardless of completing still have goof odds of smoking
cessation.

PREDICTORS OF SMOKING CESSATION AMONG PREGNANT WOMEN IN SAN
BERNARDINO COUNTY 18
When analyzing the characteristics of individuals who do not complete the program or
who successfully complete, the data found that Hispanics had the highest rate of completion
compared to NH Blacks and NH Whites. Research also supports these results indicating
Hispanics generally have lower maternal smoking rates, as well as smoking cessation. Research
also shows Blacks and Whites tend to have similar smoking trends in regards to smoking before
and after delivery and during pregnancy (MMWR, 2013)
Age was run as a categorical variable in the Univariable model in table 1 in order to
see the difference in age categories. Age was found to be a major predicting variable of program
non completion. Those who were older had higher prevalence of program completion, almost
having a protective effect with an OR of .33 and a CL of (.15-.75).
Gestational age was also determined to be a predicting variable for program completion.
Those in their first trimester has a 3.87 times odds of not completing the program than those in
their second trimester with a significant CL of 1.15-13.04. Those in their 3rd trimester had an
almost 3 times odds of not completing the program than those in their second trimester with and
OR of 2.87 and CL of 1.43-5.77.
Smoking at enrollment was another predicting variable that contributed to participants
completing or not completing the program. In table 3 it illustrates that those who were smoking
at enrollment compared to those who had quit have a 2.4 times odd of not completing the
program.
Limitations
The intention of the FG was to reveal some of the hidden barriers and needs of
participants. It was also intended to get a better perspectives of participants overall experience
PREDICTORS OF SMOKING CESSATION AMONG PREGNANT WOMEN IN SAN
BERNARDINO COUNTY 19
with the program. Initially 9 participants represented from different sites were to attend, however
only 5 came, and 2 came half way into the focus group. In addition of those who attended, each
had already finished the program, whereas, the remaining 4 who didn’t attend had yet to finish
the program. This implies that results of the FG are not representative.
The Sample size of the data revealed that only 60 events happened allowing only 6
terms to be in each model. This prevents us from seeing other variables that could have attributed
to program non completion. In addition, this prevented us from testing statistical power as well
as confounders and effect modifiers.
Currently the CTTP staff does not have a standardized procedure to collect and input
data. This was noticed through observation as well as from health educator feedback. This
increased the inconsistency of data and increased the amount of missing data which intern
contributed to an even smaller sample size.
Recommendations
The CTTP program is the only comprehensive smoking cessation program that
focuses on pregnant mothers in San Bernardino County. There is a great need to expand to reach
more clientele but they only have two health educators. Receiving funding and additional grants
would allow them to bring on additional man power to reach more individuals. In addition, this
will allow staff to allocate portions of their program to develop program plans that focus merely
on individuals who are less likely to complete the program (i.e. younger participants, women in
their third and first trimester, etc.). The focus group result yielded that including family in
program especially those who smoke would serve as a benefit to their smoking cessation.
Additional funding would allow for this to happen. They would also benefit from creating mid
and end of the year evaluations in order to make appropriate adjustments in their program as

PREDICTORS OF SMOKING CESSATION AMONG PREGNANT WOMEN IN SAN
BERNARDINO COUNTY 20
needed. Lastly, standardized procedure to collect and input data should be developed and all
former and new staff should be trained on it.
Evaluation of Field Practicum
This field practicum included and embodied many public health competencies from both global
health and epidemiology as seen in Appendix D.
i. The field practicum will be community based:
a. This field practicum took place in San Bernardino County, where it served in
many cities within the county. It provided services to outpatient and rehabilitation
homes.
ii. The field practicum will be in a cross cultural setting:
a. It served many underserved communities in cross cultural settings, serving those
in the San Bernardino County and populations of different ethnicities and
backgrounds. It allowed me to travel to different parts of the county that are
burdened with maternal smoking, and reinforced cultural sensitivity particularly
because maternal smoking for pregnant mothers can be shameful to some. This
was particularly necessary when enrolling patients into the program and
interviewing them with personal question. It was also necessary to exhibit cultural
sensitivity when creating the FG guide and having the focus group because it
would ask very personal questions which would be recorded.
iii. The field practicum will address priority public health needs of underserved
populations.

PREDICTORS OF SMOKING CESSATION AMONG PREGNANT WOMEN IN SAN
BERNARDINO COUNTY 21
a. San Bernardino County has many underserved populations especially when it
comes to smoking cessation. Smoking has many adverse health outcomes and
San Bernardino, although not the highest rate of maternal smoking still has a high
rate of smoking compared to the state of California. Addressing this need is
imperative to not only those who smoke, but those it affects like unborn children
and second hand smokers.
iv. Assist host entity in assessing existing capacity:
a. Analyzing this data served as a baseline assessment as to what would increase the
capacity of the program. The FG also served as needs assessment as to areas of
the concerns participants had. Improvements can be made based on this.
v. Communicate lessons learned to community partners and global constituencies:
a. Apart from the field practicum objectives that needed to be met, I was able attend
meeting with important stakeholders like First 5 San Bernardino. I was also able
to attend meetings with other smoking cessation programs that were nationwide
or didn’t serve our county to learn from their programs and share ideas from what
work with ours.
vi. Implement strategies to engage marginalized and vulnerable populations in making
decisions that affect their health and well-being.
a. The data analysis revealed that there were certain populations that were less likely
to complete the program. Recommendations based on this were made on how we
can incorporate tools to have these populations included so that they can complete
the program and benefit from smoking cessation
vii. Conduct formative assessment/research:

PREDICTORS OF SMOKING CESSATION AMONG PREGNANT WOMEN IN SAN
BERNARDINO COUNTY 22
a. This practicum was a research project which allowed me to use qualitative and
quantitative research methods.
viii. Develop monitoring and evaluation frameworks to asses program:
a. Based on the recommendations a mid and end of the year evaluation plan was
created and will be modified for the CTTP to use as needed.
Other responsibilities included attending meetings as needed, making deliveries to patients
as needed and helping with other task to help health educators. Many observations were made
while interning with the CTTP. One of the many were that the staff had a large work load, which
made it difficult for the health educators to do other work. I also noticed that the health educators
had a good relationship with all their participants and made an effort to always connect with
them in a personable way.
This field practicum was a valuable experience. I believe that it has equipped me with the
tools to be successful in the public health field. It taught me how to work well with small
institutions, how to share my ideas in a meaningful way. It also taught me how to work
efficiently independently, which is everything I need to be successful.
The school of public health was very helpful in facilitating my practicum project and they
were very helpful every step of the way. Additionally so was the organization I interned with.
They made things easier by motivating and guiding me. All in all I am grateful for the
experience.
PREDICTORS OF SMOKING CESSATION AMONG PREGNANT WOMEN IN SAN
BERNARDINO COUNTY 23
References
Batech, Michael, Tonstad, Serena, Job, Jayakaran S., Chinnock, Richard, Oshiro, Bryan,
Merritt, T. Allen, Page, Gretchen &Singh, Pramil N. (2013). Estimating the Impact of
Smoking Cessation During Pregnancy: The San Bernardino County Experience
Center for Addiction and Mental Health (n.d) Pregnancy and Smoking: A literature review that
investigates the unique challenges that women experience during and after pregnancy.
Retrieved from http://www.pregnets.org/dl/Lit%20Review%20FINAL.pdf December,
2013
Center for Disease, Control and Prevention (2013). Smoking and Tobacco Use; Smoking
Cessation. Retrieved from
http://www.cdc.gov/tobacco/data_statistics/fact_sheets/cessation/quitting/ December,
2013
Center for Disease, Control and Prevention. (2004) Smoking During Pregnancy---United States,
1990-2002. Morbidity Mortality Weekly Report,53(39);911-915 Retrieved from
http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5339a1.htm), November 2013.
Cnattingius, S. (2004). The epidemiology of smoking during pregnancy: Smoking prevalence,
maternal characteristics, and pregnancy outcomes. Nicotine & Tobacco Research,
6(Suppl. 2), S125–S140. doi:10.1080/14622200410001669187.
Severson, H. H., Andrews, J. A., Lichtenstein, E., Wall, M., & Zoref, L. (1995). Predictors of
Smoking During and After Pregnancy: A Survey of Mothers of Newborns. Preventive
Medicine, 24(1), 23-28. doi: http://dx.doi.org/10.1006/pmed.1995.1004
Samet JM, Yoon SY (2001) Women and the tobacco epidemic: challenges for the 21st century.
World Health Organization, Geneva
The 2004 United States surgeon general’s report: The health consequences of smoking. (2004).
N S W Public Health Bull, 15(5–6):107.
Woodby, L. L., Windor, Richard A., Snyder Scott W., Diclemente Kohler& Carlo C.,. (1999).
Predictors of Smoking Cessation During Pregnancy. Addiction, 94(2), 10.
PREDICTORS OF SMOKING CESSATION AMONG PREGNANT WOMEN IN SAN
BERNARDINO COUNTY 24
Appendices
Appendix A
Instrument Title: Discussion Guide: Focus Group I: CTTP Evaluation Topics
Total Participant time required: 1 hour + 30 minutes
Total focus group time: 1 hour
Break: 30 minutes
OVERALL QUESTION TO ANSWER IN FOCUS GROUP DISCUSSIONS:
The purpose of the study is to conduct evaluative research to determine
The efficacy of the CTTP
What barriers did participants encounter within the program that hindered their
success?
Which part of the program did they find most effective that attributed to their
smoking cessation?
Which part of the program did they find most ineffective that hindered their
smoking cessation?
Below is a general guide for leading our focus groups. We may modify this guide as needed.
Before the group begins, conduct the informed consent process, including compensation
discussion.
I. Introduction (10 m)
Welcome participants and introduce yourself.
Explain the general purpose of the discussion and why the participants were chosen.
Discuss the purpose and process of focus groups
Explain the presence and purpose of recording equipment and introduce observers.
Outline general ground rules and discussion guidelines such as the importance of
everyone speaking up, talking one at a time, and being prepared for the moderator to
interrupt to assure that all the topics can be covered.
Review break schedule and where the restrooms are.
Address the issue of confidentiality.
Inform the group that information discussed is going to be analyzed as a whole and that
participants' names will not be used in any analysis of the discussion.
Read a protocol summary to the participants.
Discussion Guidelines:
We would like the discussion to be informal, so there’s no need to wait for us to call on
you to respond. In fact, we encourage you to respond directly to the comments other people
make. If you don’t understand a question, please let us know. We are here to ask questions,
listen, and make sure everyone has a chance to share.

PREDICTORS OF SMOKING CESSATION AMONG PREGNANT WOMEN IN SAN
BERNARDINO COUNTY 25
If we seem to be stuck on a topic, we may interrupt you and if you aren’t saying much, we
may call on you directly. If we do this, please don’t feel bad about it; it’s just our way of making
sure we obtain everyone’s perspective and opinion is included.
We do ask that we all keep each other’s identities, participation and remarks private. We
hope you’ll feel free to speak openly and honestly. In order to do so, each of you are assigned a
number, that has been placed on your chair. Before speaking, you each will state the number
and state what you would like to say. For example, “ I am number 10 and I think the food was
really great”
As discussed, we will be tape recording the discussion, because we don’t want to miss
any of your comments. No one outside of the CTTP will have access to these tapes and they will
be destroyed after our report is written.
Helping to assist in this focus group is Andrea and she will be taking notes and be here to assist
me if I need any help. She will also ask questions as needed
Let’s begin. Let’s find out some more about each other by going around the room one at a
time. Tell us what city do you live in and what are your favorite baby colors. I’ll start.
II. (40)
Let’s get started!
1. Initiation (enrollment and recruitment process) This is how they started the program and about how they heard of it
How long have you been in the program?
How did you find out about the program?
2. Background
When did you start smoking?
How long have you been smoking?
How long where you or are you smoking while pregnant?
What made you want to smoke?
Who else in your family smokes?
Have you tried to quit before entering this program?
If yes, why was it not successful?
Who has quit smoking while in the program?
When did you quite?
Who is still smoking?
3. Barriers (challenges and roadblocks to any component of the program)

PREDICTORS OF SMOKING CESSATION AMONG PREGNANT WOMEN IN SAN
BERNARDINO COUNTY 26
For those of you who have not quit could you tell me why you think it has not
happened?
If you did quit but had a very hard time could you talk about some of the reason you
felt it was difficult?
What kind of assistance do you wish you had to help you to quit smoking?
What about transportation?
4. Effectiveness (Contribution of any component of the program to smoking cessation) What was most effective to them?
How much did the incentives help you to quit
Did it have a big role?
How much did the education help you to quit
Did is have a big role?
What part of the program had the biggest impact?
4 Needs improvement (improvement opportunities)
What areas of the program had the least impact on you to quit smoking?
Could you give us some ideas on how we could make the process of quitting smoking easier?
V. Closing (5 minutes)
Closing remarks
Thank the participants
Issue their compensation

PREDICTORS OF SMOKING CESSATION AMONG PREGNANT WOMEN IN SAN
BERNARDINO COUNTY 27
Appendix B
Comprehensive Tobacco Treatment Program (CTTP)
Focus Group - Consent Form
Invitation to Participate & Purpose
You are being invited to participate in evaluating the process of Comprehensive Tobacco
Treatment Program. Thank you for taking time out of your busy schedule to consider
participation.
Voluntary Participation
Your participation in this evaluation is completely voluntary and you may withdraw your
consent to participate at any time during the process. If you choose to do so, any information
derived from your participation will be deleted from the evaluations findings.
Methods/Procedures
The methods of data collection for this evaluation will be a focus a group. The sessions will be
audio-taped, and the audio-tapes transcribed to ensure accurate reporting of the information that
you provide. No one’s name will be asked or revealed during the focus groups or individual
interviews. However, should another participant call you by name, the transcriber will be
instructed to remove all names from the transcription? No one outside of Loma Linda Medical
Center or University will have access to these tapes and they will be destroyed after our report is
written
Confidentiality
If you choose to participate, you will not be asked your name at the focus group. You will not
need to use your name in the focus groups. If by chance, you or someone you know addresses
you by name in the sessions, the transcriber will be instructed to delete all names from the
transcription. All findings used in any written reports or publications which result from this
evaluation will be reported in aggregate form with no identifying information. It is, however
useful to use direct quotes to more clearly capture the meanings in reporting the findings from
this form of evaluation.
Risks and Inconveniences
There are no anticipated physical risks to participants. Focus group members will be asked to
keep the information provided in the groups confidential.
Benefits
A potential benefit to you for participating in this evaluation for you could be having an
opportunity to describe your experience with others who have shared similar experiences.
Additionally, the opportunity to connect with other allies and share similar and divergent
experiences may help clarify and validate your experiences within this program. The benefits to
society would be based on establishing a clearer understanding of the experiences CTTP
members have and some of the obstacles and benefits of being a member of the CTTP. This
information can help the CTTP be more effective, and may provide guidance through lessons
learned.
PREDICTORS OF SMOKING CESSATION AMONG PREGNANT WOMEN IN SAN
BERNARDINO COUNTY 28
Questions
The CTTP appreciates your participation. If you have any questions about the outcomes of this
focus group you are encouraged to email Temidayo Ogunrinu, at [email protected]
Authorization
You will be given a copy of this consent form to keep for your records. Once again, we thank
you for taking time out of your busy schedule to participate in this evaluation process.
Date: _______________________________
_____________________________________
____________________________________
Printed Name of the Participant
Signature

PREDICTORS OF SMOKING CESSATION AMONG PREGNANT WOMEN IN SAN
BERNARDINO COUNTY 29
Appendix C
A Priori Codebook
Focus Group
TOPIC CODE FG Transcription
CTTP Participant
enrollment
process
CTTP_ENRMT_PRCSS Found out within
different sites
“..I found out through the diabetic wellness,
community hospital”
“I found out through Loma Linda Hospital
for high risk pregnancy”
“…I found out through the diabetic
program”
CTTP Participant
Smoking
Background
CTTP_PT_SMK_BKGRND Started smoking
at a young age.
Family smoked
and peer pressure
Stress kept them
smoking
All previously
stopped at one
point in their life
but started
smoking because
of stress or being
around other
smokers
“Started at age 15….and I was 4 weeks and
I haven’t had a cigarette since”
“Started when I was 15….but I am 8 weeks
when I know I am pregnant and quit”
“When I was nine I started smoking…I
smoked till I was 8 months pregnant”
CTTP smoking
status
CTTP_SMK_STATUS All completed the
8 week program
“I’ve completed the program”
“I’ve completed as well”
“I know it was a 8 week program and I
completed”
Smoking
cessation barriers
CTTP_SMK_CSS_BARR No major barriers
“Morning sickness actually helped me quit”
“Highly restricted environment helped me
to stay quit”
“Stress was a barrier”
“Transportation at certain time”

PREDICTORS OF SMOKING CESSATION AMONG PREGNANT WOMEN IN SAN
BERNARDINO COUNTY 30
Additional Excerpts
#4: “I started when I was nine and I started smoking marijuana and I got introduced to cigarettes
and a lot of other stuff...soo”
#3: It was mainly stress, bills, under so stuff; one thing that helped me calm my nerves was to
get a pack of cigarettes and smoke, along with some alcohol.
#4: When I stopped smoking cigarettes in 2008 I had a stroke, because of my heart condition,
because of that it kind of slowed me down, just because I was kind of afraid to lose my life.
Because I have my kids, I had my two baby girls. And my two oldest ones are not from my
husband and it would be selfish If I kept doing what I was doing and lose my life and my kids
would stay by myself. But then I had my third one and she stressed me out a little. I got into a
postpartum depression. And since I am Mexican they don’t believe in depression, they just get
over it, that’s it, there is no depression here, open up your windows and walk out. I guess that
CTTP Effectives
towards smoking
cessation
CTTP_EFTVNS For participants
everything was
effective and
incentives played
a role
Convenience
“No, it was so convenient for us.”
Incentives
“I am number 6 and think that what mostly
motivated me was the diapers. Because I
have a one year and it really came in
handy”
CTTP biggest
impact toward
smoking
cessation
CTTP_BIG_IMPCT Their own
wellness and
health, being
alive and well for
their children
Pregnancy
I don’t think it I was pregnant I would still
be smoking a pack a day and drinking
Motivation
“Like I said, for me it was a big help. I had
someone to talk to”
“Because most of the time people always
say why I should quite, but this program
tells you why you should. It explains to you
and motivates you”
Education
“It just traumatized me. Seeing the man
with the hole inside his neck. The stuff I’ve
seen from the movies just traumatized me.
It makes me not even was to look at a
cigarette.”
CTTP areas of
improvement
CTTP_IMPRV Transportation to
sites and
including family
“I would say, lack of transportation”
Including family
“Yea because they(Family) smoke and just
like it teaches us it will teach them”
PREDICTORS OF SMOKING CESSATION AMONG PREGNANT WOMEN IN SAN
BERNARDINO COUNTY 31
was my way of dealing with it was going back to smoking that was the only way that I was going
to pull myself out of there.
#3: The reason why I quit is because I didn’t want my son to come out with any complications,
asthma, and I see what the smoking done to my step daughter. And her mother did drugs when
she was pregnant and I see what it can do to a child. But I was just really concerned about my
son so I just quit cold turkey. As soon as I found out I was pregnant with my son I just quit.
M: #5 why wasn’t it successful, why didn’t you stay quit?
#5: Um, because I started hanging around the people who did it again, it was just the people in
general. I think it was more of an influence than anything else and at veronicas home we are
highly monitored, we are not allowed to smoke or drink.
#3: I don’t think it I was pregnant I would still be smoking a pack a day and drinking. I used to
have a drink everyday just to deal with life. I stopped when I got pregnant. And I can think
clearer now. I’m not drunk I don’t smoke, so pregnancy was the best thing.
#6: I am going to stay clean, but I think the thing the motivates me the most are my kids and the
fact that I am breast feeding. And I just want my kids to be healthy and they can’t be around that.
#4: Well I am breast feeding, and my husband will probably kill me if I went back to smoking
because I’m am already killing him with diapers and stuff like that for this one and my 18month
old baby.
#1: I will stay clean all the time because I know what will happen and I am breast feeding too. I
don’t think that will happen.
#5: I met Maribel in my program and they have actually helped a lot, a lot of time, the way we
say in Spanish its la maña, it’s just a custom. Your just used to having that cigarette in your hand
so as long as I have a hard candy or a mint or a snack, or beef jerky or that goody bag she offered
us, it keeps me occupied, I figured out it was me just mostly wanting to smoke, the routine of just
wanting to do it.
#6: I am number 6 and think that what mostly motivated me was the diapers. Because I have a
one year and it really came in handy. I was like whelp, I am already testing clean, and so give me
my diapers you know what I mean?
#6: It was some things that I found out and I was like whoa. I am still kind of paranoid about,
like dang, I am ok for smoking that much back then. It was a lot of information I found out that
scared me even when I was pregnant and she did the smoking Suzy with the baby inside, and my
whole pregnancy I was like I hope my baby is ok. I hope I quit soon enough you know.
M: Who is smoking Suzy?

PREDICTORS OF SMOKING CESSATION AMONG PREGNANT WOMEN IN SAN
BERNARDINO COUNTY 32
#5: I was just mention that. Yupp, It was one of the main ways that it got to me. It actually shows
you a visual of what happens to the baby inside your stomach when your smoking a cigarette.
It’s crazy! Just the of knowing your baby can get asthma from that is crazy.
#1: Yea, Diana would say….I was in the party where they smoke a lot and I move and they come
smoke again and I was trying. So she talked to me and say “it’s your life, it’s your opportunity to
say stop smoking or go out and I am pregnant and I have baby”. She told me to do it polite how
to tell the people to stop smoking around me because I pregnant. Because I embarrassed to say
stop smoking, but Diana tell me I need to do those things.
3: I would say, lack of transportation, so something like a bus pass or a gas card if they couldn’t
make it to their appointment if you guys could provide that.
Yea because they (Family) smoke and just like it teaches us it will teach them
Appendix C

PREDICTORS OF SMOKING CESSATION AMONG PREGNANT WOMEN IN SAN
BERNARDINO COUNTY 33