predictors of shift work disorder among nurses: a longitudinal study
TRANSCRIPT

Accepted Manuscript
Title: Predictors of shift work disorder among nurses - a longitudinal study
Author: Siri Waage, Ståle Pallesen, Bente Elisabeth Moen, Nils Magerøy,
Elisabeth Flo, Lee Di Milia, Bjørn Bjorvatn
PII: S1389-9457(14)00381-5
DOI: http://dx.doi.org/doi:10.1016/j.sleep.2014.07.014
Reference: SLEEP 2551
To appear in: Sleep Medicine
Received date: 14-3-2014
Revised date: 7-6-2014
Accepted date: 3-7-2014
Please cite this article as: Siri Waage, Ståle Pallesen, Bente Elisabeth Moen, Nils Magerøy,
Elisabeth Flo, Lee Di Milia, Bjørn Bjorvatn, Predictors of shift work disorder among nurses - a
longitudinal study, Sleep Medicine (2014), http://dx.doi.org/doi:10.1016/j.sleep.2014.07.014.
This is a PDF file of an unedited manuscript that has been accepted for publication. As a service
to our customers we are providing this early version of the manuscript. The manuscript will
undergo copyediting, typesetting, and review of the resulting proof before it is published in its
final form. Please note that during the production process errors may be discovered which could
affect the content, and all legal disclaimers that apply to the journal pertain.

Predictors of shift work disorder among nurses - a longitudinal study
Siri Waage, PhD1,2,*
, Ståle Pallesen, PhD2,3
, Bente Elisabeth Moen, MD, PhD1,4
,
Nils Magerøy, MD PhD5, Elisabeth Flo, PhD
1,2, Lee Di Milia, PhD
6, and
Bjørn Bjorvatn, MD, PhD1,2
1 Department of Global Public Health and Primary Care, University of Bergen, Norway
2 Norwegian Competence Center for Sleep Disorders, Haukeland University Hospital,
Norway
3 Department of Psychosocial Science, University of Bergen, Norway
4 Centre for International Health, University of Bergen, Norway
5 Department of occupational medicine, Haukeland University Hospital, Norway
6 Central Queensland University, School of Management and the Institute for Health and
Social Science Research, Rockhampton, QLD, Australia
*Corresponding author / Request for reprints:
Siri Waage
Department of Global Public Health and Primary Care
Kalfarveien 31
5018 Bergen, Norway
E-mail: [email protected]
keywords: Shift work, sleep problems, sleepiness, insomnia, shift work disorder
Highlights
Survey on shift work, sleep and health among 1533 nurses with a two year follow-up
There was a significant reduction in shift work disorder from baseline to follow-up
Several factors were identified to be predictors of shift work disorder
Page 1 of 24

Abstract
Background: Shift work is associated with sleep problems and impaired health. The main
aim of the present study was to explore predictors of developing shift work disorder (SWD)
among Norwegian nurses using a longitudinal design.
Methods: A total of 1533 nurses participating in a survey on shift work, sleep and health
responded to questionnaires at baseline and about two years later at follow-up. SWD was
defined as problems of excessive sleepiness and/or complaints of insomnia related to the work
schedule.
Results and Conclusions: There was a significant reduction (p<.001) in the prevalence of
SWD from baseline to follow-up, from 35.7% to 28.6%. Logistic regression analyses showed
significant risks of having SWD at follow-up and the following variables measured at
baseline; number of nights worked the last year (OR=1.01, 95% CI=1.01-1.02), having SWD
(OR=5.19, 95% CI=3.74-7.20), composite score on the Epworth Sleepiness Scale (OR=1.08,
95% CI=1.04-1.13), use of melatonin (OR=4.20, 95% CI=1.33-13.33), use of bright light
therapy (OR=3.10, 95% CI 1.14-8.39), and symptoms of depression measured by the Hospital
Anxiety and Depression Scale (OR=1.07, 95% CI=1.00-1.14). In addition, leaving night work
between baseline and follow-up was associated with a significant reduced risk of SWD at
follow-up (OR=0.12, 95% CI=0.07-0.22).
Page 2 of 24
Introduction
Estimates suggest that approximately 20% of workers in Europe are employed in some form
of shift work that involves night work [1]. Shift work is associated with a wide range of health
problems [2, 3]. In work schedules that include night work, sleep problems are among the
most frequently reported health problems [4, 5]. The most common sleep problems among
night shift workers are sleep onset and maintenance difficulties, reduced sleep duration and
excessive sleepiness during work [5]. For Norwegian nurses, it is common to work rotating
shifts, which is a work schedule that could involve morning, evening and night shifts within
the same work week. This is reported to lead to insufficient sleep duration [6], and night work
is reported to be the most important cause of long-term stress and fatigue [7]. Nurses in
rotating shifts have reported more mental health problems compared to nurses working non-
rotating shifts [8] and associations between shift work, anxiety and depression have also been
shown [9]. In a recent Norwegian study, nurses working in intensive care units were found to
report poorer sleep and higher levels of sleepiness, fatigue, anxiety and depression compared
to Norwegian norm groups [10]. However, results linking shift work and mental health are
inconsistent; anxiety and depression were for example not associated with night work in a
cross sectional study of Norwegian nurses [11].
Shift work disorder (SWD) is a circadian rhythm sleep disorder characterized by excessive
sleepiness and complaints of insomnia related to the work schedule [12]. The diagnostic
criteria for SWD are described in the second edition of the International Classification of
Sleep Disorders (ICSD-2) and include the following four criteria: 1) Complaint of insomnia or
Page 3 of 24

excessive sleepiness temporally associated with a recurring work schedule that overlaps the
usual time for sleep, 2) symptoms must be associated with the shift work schedule and present
over the course of at least one month, 3) circadian and sleep-time misalignment as
demonstrated by sleep log or actigraphical monitoring for 7 days or more and finally 4) sleep
disturbance is not explainable by another sleep disorder, a medical or neurological disorder,
mental disorder, medication use or substance use disorder [13].
Varying prevalences of SWD have been reported in cross-sectional studies, ranging from
14.5% among police officers working nights [14], 23.3% among oil rig workers [15], 24.4%
among shift working nurses [16], 32.1% among Australian night workers [17], and up to
44.3% among Norwegian nurses in rotating shift work [18]. SWD is a relatively new
diagnosis, and there is uncertainty and discussion about its operationalization, prevalence,
consequences and treatment [19]. At present, few studies have used standardized questions to
measure SWD and SWD seems to be underestimated in clinical settings. Epidemiological data
on SWD are scarce [20]. One limitation of previous research on SWD is that the studies are
based on cross-sectional design which prevent conclusions concerning directionality and
possible cause-effect relationships related to the development and consequences of SWD.
To address this limitation, the main aim of the present study was to explore predictors of
SWD among Norwegian shift working nurses using longitudinal data. We also aimed to
assess the prevalence of SWD among Norwegian nurses at baseline and follow-up.
Methods
Procedure and participants
Page 4 of 24
The data were collected from an on-going longitudinal cohort study “SUrvey of Shift work,
Sleep and Health (SUSSH)” that was initiated in 2008/2009. A sample of 5400 nurses was
randomly selected from the Norwegian Nurses Organization’s membership roll which
includes most of the nurses in Norway. Survey questionnaires have been sent to this sample
annually and this study presents findings from the first (2008/2009=baseline) and the third
wave (2011=follow-up) of the survey.
The sample comprised five equal strata based on the numbers of years since graduation from
nursing school (0-11 months, 1-3 years, 3.1-6 years, 6.1-9 years, and 9.1-12 years). A total of
2059 (response rate = 38.1%) nurses completed the questionnaire in the first wave (during the
period December 2008 to March 2009). During the spring of 2011, all the nurses that
completed the first wave received an invitation to participate in the third wave. A total of
1533 nurses (91% female) responded, yielding a response rate of 78.5%. All questionnaires
were administered by postal mail with a pre-paid envelope for returning the completed forms.
Up to two reminders were sent for each wave to those who did not respond.
Instruments
Demographics
The questionnaires comprised several sections. We collected data on socio-demographic
variables (gender, age, married/cohabiting, children in household), work-related variables
(work schedule, type and percentage of position worked in a full-time capacity, type of work
place, exposure to night work (years) and number of night shifts per year); as well as life-style
variables (e.g. present daily smoking and caffeine consumption/daily cups of coffee, tea or
cola, use of sleep medication, use of bright light treatment).
Page 5 of 24

Shift work disorder
In line with a number of previous studies three questions based on the minimal criteria from
the ICSD-2 were used to assess SWD [15, 17, 18]. The questions are found to adequately
assess SWD in epidemiological contexts [18]. The questions were: 1) Do you experience
either difficulties sleeping or experience excessive sleepiness? (yes/no), 2) Is the sleep or
sleepiness problem related to the work schedule that makes you work when you normally
would sleep? (yes/no), 3) Have you had this sleep or sleepiness problem related to the work
schedule for at least one month? (yes/no). Subjects were classified as suffering from SWD
when they responded “yes” to all three questions.
Insomnia
Insomnia symptoms were assessed with the Bergen Insomnia Scale (BIS) [21]. The
questionnaire consists of 6 items, where the response alternatives reflects the number of days
per week (0-7) the respondent had experienced a specific insomnia symptom, and is based on
the diagnostic criteria for insomnia found in the fourth edition of the Diagnostic and
Statistical Manual for Mental Disorders (DSM-IV, American Psychiatric Association, 2000).
The scores on each item are added to create a total composite score (0 to 42), and higher
values indicate a greater degree of insomnia symptoms [21]. The Norwegian version of the
BIS has been validated and had shown good psychometric properties [21]. In the present
study, the Cronbach’s alpha was .83 for the baseline data and .82 for the follow-up data.
Sleepiness
Sleepiness was measured with the Norwegian version of the Epworth Sleepiness Scale (ESS)
[22]. The ESS consists of 8 items that measure the subject’s general tendency to sleep or doze
off in 8 different situations. Each item is scored from 0 (no probability) to 3 (high probability),
Page 6 of 24
yielding a total score between 0 and 24. The Norwegian version has shown high validity and
reliability [23]. In the present study the Cronbach’s alpha coefficients were .74 for the
baseline data and .75 for the follow-up data, respectively.
Anxiety and depression
Symptoms of anxiety and depression were assessed with the Norwegian version of the
Hospital Anxiety and Depression Scale (HADS) [24]. This scale consists of 14 items
measuring symptoms of anxiety and depression experienced during the last week. Seven
questions specifically address symptoms of anxiety whereas the other seven questions pertain
specifically to symptoms of depression. The items are rated on a 4-point scale (0-3), yielding
two scores, one for anxiety and one for depression, each ranging from 0 and 21. The HADS
has shown good reliability [25]. In the present study the Cronbach’s alpha coefficients for
both the anxiety and depression subscales were .81 for the baseline data. For the follow-up
data the coefficients were .82 for both the scales.
Morningness
A Norwegian version of the Diurnal Type Scale [26] was used to assess the morningness-
eveningness dimension. The scale consists of 7 items related to this dimension, each rated on
a four-point scale. Higher scores indicate higher levels of morningness (e.g. preference for
rising relatively early in the day, performing activities relatively early in the day and getting
to bed relatively early in the evening). The Diurnal Type Scale has been shown to have high
internal reliability and validity. The Cronbach’s alpha coefficient was .64 at both baseline and
follow-up in the present study.
Ethics
Page 7 of 24

The Regional Committee for Medical and Health Research Ethics of Western Norway (REK-
West) approved the study.
Statistics
PASW Statistics 18 for Windows was used for the statistical analyses. For comparisons of
demographic variables between the nurses with and without SWD at baseline, independent t-
tests and Pearson chi-square tests were used. Significance level was set at .05.
The nurses were divided into four different groups based on having SWD or not at the two
time points of the study. Group one consisted of workers not having SWD in either of the two
waves (54.9%, n=817). The second group comprised nurses defined with SWD solely at
baseline, and not at follow-up (16.5%, n=246). Group three consisted of nurses defined with
SWD solely at follow-up and not at baseline (9.7%, n=144). Finally, the fourth group
comprised of nurses defined with SWD at both baseline and follow-up (18.9%, n=281).
Paired-sample t-tests were used to compare the change for each of the sleep and health
parameters from baseline to follow-up within each of the four groups.
Logistic regression analyses were performed to assess the impact of a number of factors on
the likelihood of nurses having SWD at follow-up. The latter comprised the dependent
variable (0=not having SWD, 1=having SWD). We included age, gender, marital status,
children in household, use of sleep medication (prescription or over the counter), use of
exogenous melatonin, bright light treatment, smoking, caffeine consumption, number of
nights worked the last 12 months, SWD, sleepiness score, insomnia score, anxiety score,
depression score and diurnal type all measured at baseline as independent variables.
Page 8 of 24

Furthermore, we included no longer working night shifts at follow-up (yes/no) also as an
independent variable. All variables were first entered separately (crude analyses) and
secondly they were all entered together at the same time in an adjusted analysis.
Furthermore, logistic regression analyses were performed to assess the impact of the same
factors on the likelihood of disappearance of SWD among nurses having SWS at baseline.
Results
Demographics
At baseline (n=1533), the mean age of the nurses was 33 years, range 21-63. Among the
whole sample, 76.3% worked in somatic hospital departments, 13.5% in psychiatric
departments, 3.5% in nursing homes, 3.7% in home care services, and 2.1% in other work
places, respectively. The mean hours worked per week were 33.9 with a distribution of 2.8%
working <50% position, 28.6% working between 50-75% of full time position, 13.4%
working between 76-90% of full time position, and 55.2% working more than 90% of full
time position. Previous or present night work was reported by 84.3% of the nurses. Working
only daytime was reported by 7.6% of the nurses, 0.1% reported only evening work, 25.0%
worked a two-shift schedule involving day work and evening work, 8.2% worked nights only,
55.0% worked a three-shift schedule involving day, evening and night work, and 3.1%
reported working other schedules involving night work. 14.0% of the nurses quitted night
work between baseline and follow-up. A total of 74.0% of the nurses were married or
cohabiting, and 48.7% reported having children at home. Mean body mass index (BMI)
among the nurses was 24.4 (range 17.3-47.9). The nurses reported a mean of 3 cups of
caffeinated beverages per day (range 0-30), and 10.0% were daily smokers (daily smoking,
yes/no).
Page 9 of 24

Shift work disorder
A total of 54.9% of the nurses did not have SWD at baseline or at follow-up, 16.5% were
defined with SWD at baseline only, 9.7% at follow-up only, and 18.9% of the nurses were
defined with SWD at both baseline and follow-up. Analysing data from all the nurses, there
was a significant reduction (p<.001) in the prevalence of SWD between baseline (35.7%,
n=538) and follow-up (28.6%, n=433). Among the nurses from wave 1 who did not respond
in wave 3, the prevalence of SWD was 33.2% at baseline. The differences in demographics
between nurses with and without SWD at baseline are described in table 1. Having SWD at
baseline was positively associated with male gender, age, currently or previously working
night shifts, numbers of nights the last year, and inversely related to the score on the
morningness dimension (table 1).
Insert table 1 about here
The differences between the two measurements (baseline and follow-up) across the four
groups are presented in table 2. Interestingly, the group that no longer met the criteria for
SWD at follow-up worked significantly fewer nights and also reported a reduction in scores
on the ESS, the BIS, and on symptoms of anxiety and depression. In that group 30.7% of the
nurses had quit night work between the two assessment points, and the mean number of nights
worked the last year was reduced from 27.9 to 18.5 nights. The reductions in the ESS, BIS,
anxiety and depression scores were similar among the nurses who no longer worked night
shifts, and those still working nights shifts at follow-up. For the group that developed SWD at
follow-up, exposure to night work and scores for BIS increased.
Insert table 2 about here
Page 10 of 24

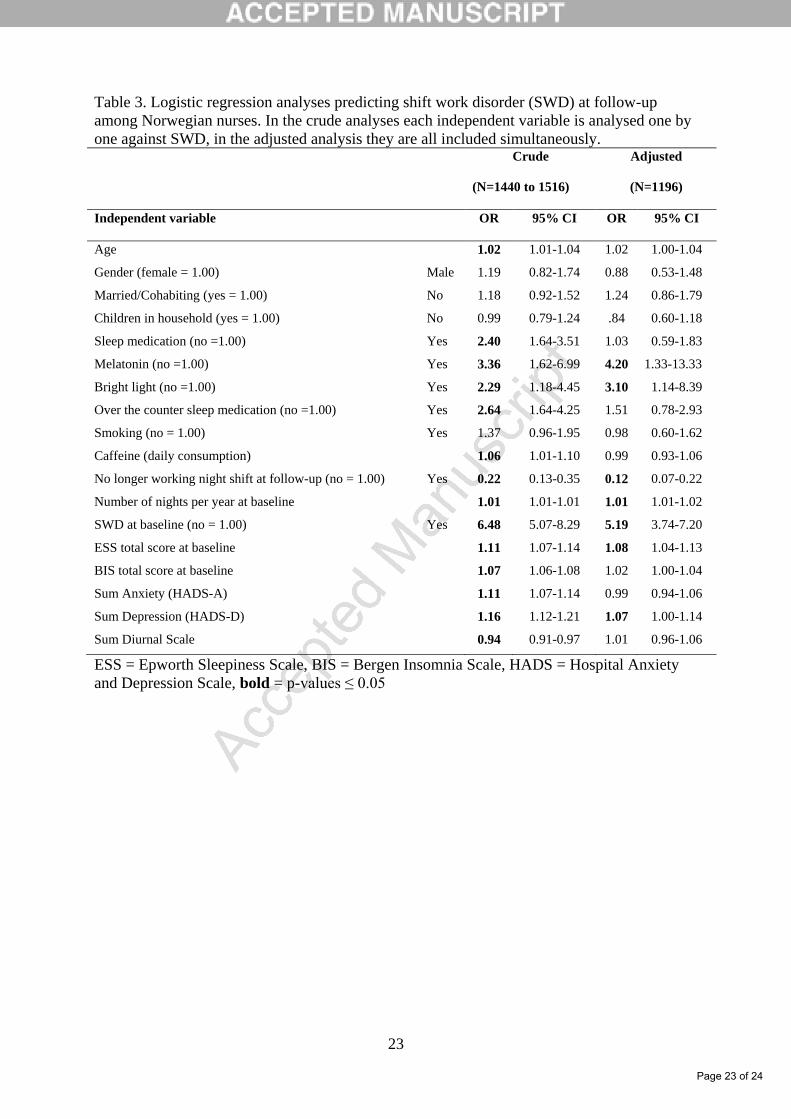
The results from the logistic regression analyses showed a risk of having SWD at follow-up
and the following variables assessed at baseline; use of melatonin, use of bright light therapy,
number of nights worked the last year, having SWD, sleepiness scores, and depression score
(see table 3). In addition, leaving night work between baseline and follow-up significantly
reduced the risk for fulfilling the criteria for SWD at follow-up. In addition, logistic
regression analyses were performed among the nurses who had SWD at baseline to
investigate predictors of cessation of SWD. Not surprisingly, no longer working night shift at
follow-up was the strongest predictor of disappearance of SWD from baseline to follow-up.
Furthermore, numbers of nights worked per year and sleepiness measured by the ESS at
baseline were positively associated maintaining SWD (see table 4).
Insert table 3 and 4 about here
Discussion
Having SWD at baseline, use of exogenous melatonin, use of bright light therapy, number of
nights worked last year, sleepiness score, and depression score were all found to be predictors
of SWD among Norwegian nurses. In addition, quitting night shifts from baseline to follow-
up decreased the risk of SWD at follow-up. Interestingly, there was overall a significant
reduction in the prevalence of shift work disorder (SWD) from 35.7% at baseline to 28.6% at
follow-up.
Measured at baseline, the nurses with SWD were slightly older, comprised more males, were
presently or previously working nights, and worked more nights the last year than the nurses
without SWD. This is in line with studies showing that sleep problems related to shift work
Page 11 of 24
increase with age [27, 28]. However, the difference in age between the two groups was small,
only about one year, and the importance of this in terms of tolerance to shift work seems
negligible. Similarly, most of the other demographic differences between nurses with or
without SWD at baseline are small. One exception is number of nights worked the last year,
where nurses with SWD worked on average nearly 32 nights per year, while the nurses
without SWD worked about 22 nights per year. Also, morning types are reported to have
more difficulties adjusting their circadian rhythms to night work [29]. However, in this study
the nurses with SWD scored lower on the morningness dimension compared to the nurses
with SWD. In line with this, a study on oil rig workers found no significant difference in
diurnal type between workers with SWD and workers without SWD [15]. Not surprisingly,
subjects with SWD scored higher on measures of sleepiness, anxiety and depression than
subjects without SWD.
The strongest predictor for SWD at follow-up was having SWD (OR 5.2) at baseline. This
suggests that the sleep related problems that are experienced by shift workers are chronic for a
significant proportion of the nurses. The number of night shifts worked per year was also a
significant predictor, in line with results from a previous cross-sectional study from SUSSH
including nurses from the same cohort [18]. Changing the work schedule so that it no longer
included night work significantly predicted reduced risk of SWD at follow-up, supporting the
fact that night work seems to be a main determinant of SWD. One of the criteria for SWD is
to have complaints of insomnia or excessive sleepiness associated with a work schedule that
overlaps with the usual time for sleep. Previous studies have reported that SWD is particularly
prevalent among shift workers working night shift and early-morning shifts [30]. Excessive
sleepiness and/or insomnia are criteria for SWD and are frequently reported among shift
workers [4, 5]. Sleepiness score at baseline was one of the predictors of reporting SWD at
Page 12 of 24

follow-up. It therefore was somewhat surprising that this was not the case for insomnia.
However, in our study insomnia was measured by the Bergen Insomnia Scale, which is based
on the diagnostic criteria for insomnia stated in the DSM-IV (American Psychiatric
Association, 2000). The criteria for SWD do not require insomnia as defined by the DSM-IV
diagnostic criteria, which is likely to be more stringent than self-reported insomnia symptoms.
The DSM-IV criteria requests difficulty in falling or maintaining sleep, or the feeling of not
having had restitutional sleep for at least one month in addition to a daytime impairment,
while the questions used to define SWD in this study did for instance not include any
questions about daytime consequences of the sleep problem. However, at baseline the mean
total score of the Epworth Sleepiness Scale (ESS) was about 9.5 among the nurses with SWD
and even lower about (7.7) among the nurses without SWD. A value of 11 or higher on the
total score of the ESS is considered as pathological sleepiness, meaning that the nurses in this
study overall are feeling sleepy, albeit still not above the clinical cut-off value.
Shift workers struggling with adjustment to different work schedules are likely to search for
interventions in order to better adjust to shift work and the problems such work schedules
pose. Adapting circadian rhythms to the work schedule or to adjust it to a normal day
schedule following e.g. a period of night shifts is assumed to be curative of shift work related
problems and SWD [31]. Bright light therapy and exogenous melatonin are as such
recommended in the current treatment guidelines for SWD [30]. Both use of melatonin and
bright light were predictors of having SWD at follow-up. One possible explanation could be
that the nurses reporting use of melatonin or bright light treatment are the nurses with the
most severe sleep or circadian problems, and that the SWD remains as long as they continue
working shift work. A weakness of the study is that we neither collected information on the
timing and dosage of melatonin, nor information about the timing and dosage of bright light.
Page 13 of 24
Future research on the effect of treatment in large randomized clinical trials of shift workers
with SWD is needed to make recommendations regarding the effects of melatonin and bright
light treatment for this disorder.
One of the predictors of SWD was depression at baseline. This is in accordance with results
from a cross-sectional study showing that shift working nurses with SWD showed more
severe depressive symptoms than those without SWD [16]. The strength of our study is the
longitudinal design, being the first study to identify depression as a predictor of developing
SWD. In the cross-sectional study from SUSSH by Flo and co-workers (2012) an association
between SWD and anxiety was reported, but after adjusting for multiple variables, neither
symptoms of anxiety nor depression were associated with SWD [18].
The prevalence of SWD reported in our study was high. Cross-sectional data from the same
Norwegian nurse population including nearly 2000 nurses at baseline, have previously
reported an even higher SWD prevalence ranging from 32.4% to 37.6% depending on the
operationalization [18]. For comparison, a recent cross-sectional study from Japan reported a
prevalence of 24.4% among 997 female hospital nurses engaged in two-shift and three-shift
schedules [16]. The discrepancy between the prevalence rates across these studies could be
explained by differences in working hours and working conditions between Norway and
Japan. For instance the typical night shift start/end times differed between the samples (Japan;
24:00 - 09:00 compared to Norway; 21:30 - 07:00). Other possible explanations for variances
in reported prevalence rates may be differences in the estimation of SWD and methodology.
However, several of the reported studies have used the same questions to estimate SWD,
which highlights that in addition to work schedule differences, individual differences may
also play a role [17].
Page 14 of 24
In the present study, the prevalence of SWD decreased by about 7% from baseline to follow-
up. Different possible factors could be considered to explain this reduction. Like in other
studies on shift workers, it is reasonable to assume that a type of selection bias might be
present, where individuals not coping with shift work tend to terminate this type of work [32].
In the present study, 30.7% of the nurses who had SWD at baseline, but not at follow-up, had
quit night work between the two time points. Among the whole sample, 14% of the nurses
made the same change. This suggests that vulnerable nurses self-selected out of night shift
work. In addition, it is also possible that during the period from baseline to follow-up the
nurses developed better coping strategies to deal with irregular work hours. It is also possible
that this decline in prevalence can be explained by organizational changes in working
conditions or wages, which we do not have information about. Interestingly, the reduction in
SWD prevalence between baseline and follow-up was evident in all different shift work
schedules.
Limitations and strengths
Some limitations of the study should be mentioned. The response rate from the first wave was
only 38% and some may thus question the representativeness of the population. Still, the
response rate at follow-up was high (79%) ensuring that we compared a large sample across
the two time points. The sample comprised only nurses, mainly females, which also pose
some threat to the external validity. On the other hand the relative homogenous sample
reduces the risk of work related confounders to influence the results.
Research on shift work as a risk factor for negative health has some methodological
challenges regarding shift work exposure. A limitation of the study is that we do not have
information about shift work experience before being included in the present cohort study.
Page 15 of 24

Future research should therefore include workers early in their shift work career, as many
nurses may have been exposed to night work before and during their education. Still, a
strength of the study is that the questionnaire consists of detailed information about present
shift work exposure, in addition to the longitudinal design with information about changes in
work schedules among the nurses.
Another limitation of the study includes its reliance on self-reported data only, and no
objective assessments. However, as primarily baseline data were used as predictors for SWD
at follow-up, this significantly reduces the risk of the results being distorted by the common
method bias [33]. Lately, a new version of the ICSD has been published, with an important
change in the criteria for SWD. In ICSD-2 the symptoms associated with the SWD should be
present for at least one month, while in the ICSD-3 this is changed to three months. Future
research should be conducted in accordance with the changes in the criteria.
Many of the odds ratios of the predictors on SWD in the present study were quite small. Still,
it should be noted that many of the variables in the analyses are not dichotomous, and the
odds ratios are consequently not expected to be high. One important factor that was
significant, but had a low odd ratio, was number of night worked last year. This variable was
continuous ranging from 0 to 200 nights per year, meaning that with an odd ratio of 1.01, an
increase of one night shift per year would increase the risk of developing SWD with one
percent. Nevertheless, when interpreting the significant results, the size of the odds ratio
needs to be taken into careful consideration.
The present study also has some valuable assets worth mentioning. As far as we know, this
study is the first longitudinal study assessing SWD, providing an unique opportunity to
Page 16 of 24
investigate directionality between variables and to identify possible causes of SWD.
Longitudinal designs are superior to cross-sectional studies when it comes to discovering
directionalities between variables. Still, the present study would be better if we had included
more than two assessment times. The study furthermore included standardized and well-
validated instruments and the relatively large sample size provides adequate statistical power
to the analyses.
Conclusion
Several factors measured at baseline like reporting SWD, use of exogenous melatonin, use of
bright light therapy, number of nights worked last year, sleepiness score, and depression score
were found to be significant predictors of SWD at follow-up. In addition, quitting night work
between baseline and follow-up was significantly associated with a decreased risk of SWD at
follow-up, suggesting that night work may be a major cause of SWD. There was a significant
reduction in the SWD prevalence rate from 35.7% at baseline to 28.6% at follow up that
might reflect selection of SWD subjects to other types of work schedules, development of
better coping strategies over time or organizational changes.
Page 17 of 24
References
[1] Parent-Thirion A, Vermeylen G, van Houten G, Lyly-Yrjänäinen M, Biletta I, Cabrita J.
Fifth European Working Conditions Survey 2012.
[2] Costa G. The impact of shift and night work on health. Appl Ergon 1996;27:9-16.
[3] Harma M. Are long workhours a health risk? Scand J Work Environ Health 2003;29:167-
9.
[4] Akerstedt T. Shift work and disturbed sleep/wakefulness. Sleep Med Rev 1998;2:117-28.
[5] Akerstedt T. Shift work and disturbed sleep/wakefulness. Occup Med 2003;53:89-94.
[6] Chan MF. Factors associated with perceived sleep quality of nurses working on rotating
shifts. J Clin Nurs 2009;18:285-93.
[7] Winwood PC, Winefield AH, Lushington K. Work-related fatigue and recovery: the
contribution of age, domestic responsibilities and shiftwork. J Adv Nurs 2006;56:438-49.
[8] Jamal M. Shift Work Related to Job-Attitudes, Social-Participation and Withdrawal
Behavior - a Study of Nurses and Industrial-Workers. Pers Psychol 1981;34:535-47.
[9] Pati AK, Chandrawanshi A, Reinberg A. Shift work: consequences and management. Curr
Sci 2001;81:32-52.
[10] Bjorvatn B, Dale S, Hogstad-Erikstein R, Fiske E, Pallesen S, Waage S. Self-reported
sleep and health among Norwegian hospital nurses in intensive care units. Nurs Crit Care
2012;17:180-8.
[11] Oyane NM, Pallesen S, Moen BE, Akerstedt T, Bjorvatn B. Associations between night
work and anxiety, depression, insomnia, sleepiness and fatigue in a sample of norwegian
nurses. PLoS One 2013;8:e70228.
Page 18 of 24
[12] Schwartz JR, Roth T. Shift work sleep disorder: burden of illness and approaches to
management. Drugs 2006;66:2357-70.
[13] American Academy of Sleep M. International Classification of Sleep Disorders 2.nd ed,
Diagnostic and Coding Manual. Westchester, Illinois: American Academy of Sleep Medicine;
2005.
[14] Rajaratnam S, Barger L, Lockley S, Cade B, O'Brien C, White D, et al. Screening for
sleep disorders in north American police officers. Sleep 2007;30:A209-A.
[15] Waage S, Moen BE, Pallesen S, Eriksen HR, Ursin H, Akerstedt T, et al. Shift work
disorder among oil rig workers in the North Sea. Sleep 2009;32:558-65.
[16] Asaoka S, Aritake S, Komada Y, Ozaki A, Odagiri Y, Inoue S, et al. Factors Associated
With Shift Work Disorder in Nurses Working With Rapid-Rotation Schedules in Japan: The
Nurses' Sleep Health Project. Chronobiol Int 2013;30:628-36.
[17] Di Milia L, Waage S, Pallesen S, Bjorvatn B. Shift Work Disorder in a Random
Population Sample - Prevalence and Comorbidities. Plos One 2013;8.
[18] Flo E, Pallesen S, Mageroy N, Moen BE, Gronli J, Nordhus IH, et al. Shift work disorder
in nurses--assessment, prevalence and related health problems. PLoS One 2012;7:e33981.
[19] Sack RL, Auckley D, Auger RR, Carskadon MA, Wright KP, Jr., Vitiello MV, et al.
Circadian rhythm sleep disorders: part I, basic principles, shift work and jet lag disorders. An
American Academy of Sleep Medicine review. Sleep 2007;30:1460-83.
[20] Culpepper L. The social and economic burden of shift-work disorder. J Fam Pract
2010;59:S3-S11.
[21] Pallesen S, Bjorvatn B, Nordhus IH, Sivertsen B, Hjornevik M, Morin CM. A new scale
for measuring insomnia: The Bergen Insomnia Scale. Percept Mot Skills 2008;107:691-706.
[22] Johns MW. A new method for measuring daytime sleepiness: the Epworth sleepiness
scale. Sleep 1991;14:540-5.
Page 19 of 24
[23] Pallesen S, Nordhus IH, Omvik S, Sivertsen B, Tell GS, Bjorvatn B. Prevalence and risk
factors of subjective sleepiness in the general adult population. Sleep 2007;30:619-24.
[24] Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiol Scand
1983;67:361-70.
[25] Bjelland I, Dahl AA, Haug TT, Neckelmann D. The validity of the Hospital Anxiety and
Depression Scale. An updated literature review. J Psychosom Res 2002;52:69-77.
[26] Torsvall L, Akerstedt T. A diurnal type scale. Construction, consistency and validation in
shift work. Scand J Work Environ Health 1980;6:283-90.
[27] Harma, M. Ageing, physical fitness and shiftwork tolerance. Appl Ergonom 1996;27, 25-
29.
[28] Marquié, J. C. Sleep, age, and shiftwork experience. J Sleep Res 1999;8, 297-304.[29]
[29] Arendt, J. Shift work: coping with the biological clock. Occup Med (Lond) 2010;60, 10-
20.
[30] Thorpy M. Understanding and Diagnosing Shift Work Disorder. Postgrad Med
2011;123:96-105.
[31] Wright KP, Bogan RK, Wyatt JK. Shift work and the assessment and management of
shift work disorder (SWD). Sleep Med Rev 2013;17:41-54.
[32] Knutsson A, Akerstedt T. The Healthy-Worker Effect - Self-Selection Among Swedish
Shift Workers. Work and Stress 1992;6:163-7.
[33] Podsakoff PM, MacKenzie SB, Lee JY, Podsakoff NP. Common method biases in
behavioral research: a critical review of the literature and recommended remedies. J Appl
Psychol 2003;88:879-903.
Page 20 of 24
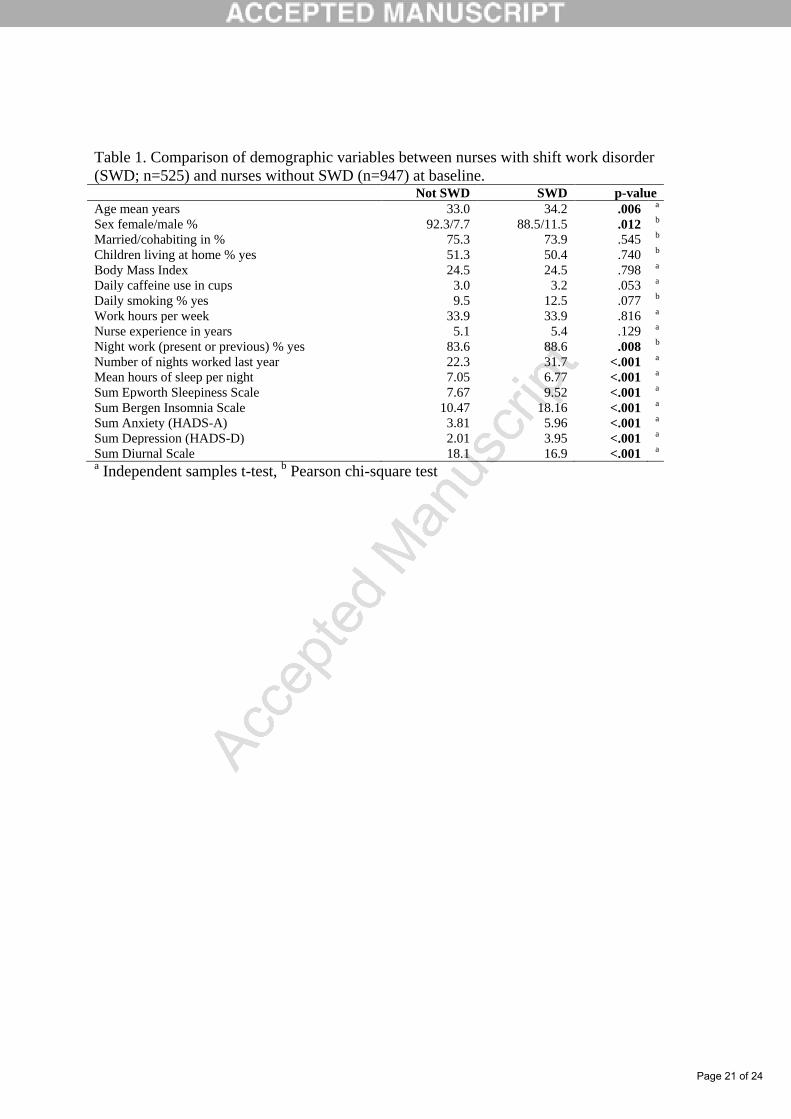
Table 1. Comparison of demographic variables between nurses with shift work disorder
(SWD; n=525) and nurses without SWD (n=947) at baseline. Not SWD SWD p-value
Age mean years 33.0 34.2 .006 a
Sex female/male % 92.3/7.7 88.5/11.5 .012 b
Married/cohabiting in % 75.3 73.9 .545 b
Children living at home % yes 51.3 50.4 .740 b
Body Mass Index 24.5 24.5 .798 a
Daily caffeine use in cups 3.0 3.2 .053 a
Daily smoking % yes 9.5 12.5 .077 b
Work hours per week 33.9 33.9 .816 a
Nurse experience in years 5.1 5.4 .129 a
Night work (present or previous) % yes 83.6 88.6 .008 b
Number of nights worked last year 22.3 31.7 <.001 a
Mean hours of sleep per night 7.05 6.77 <.001 a
Sum Epworth Sleepiness Scale 7.67 9.52 <.001 a
Sum Bergen Insomnia Scale 10.47 18.16 <.001 a
Sum Anxiety (HADS-A) 3.81 5.96 <.001 a
Sum Depression (HADS-D) 2.01 3.95 <.001 a
Sum Diurnal Scale 18.1 16.9 <.001 a
a Independent samples t-test,
b Pearson chi-square test
Page 21 of 24
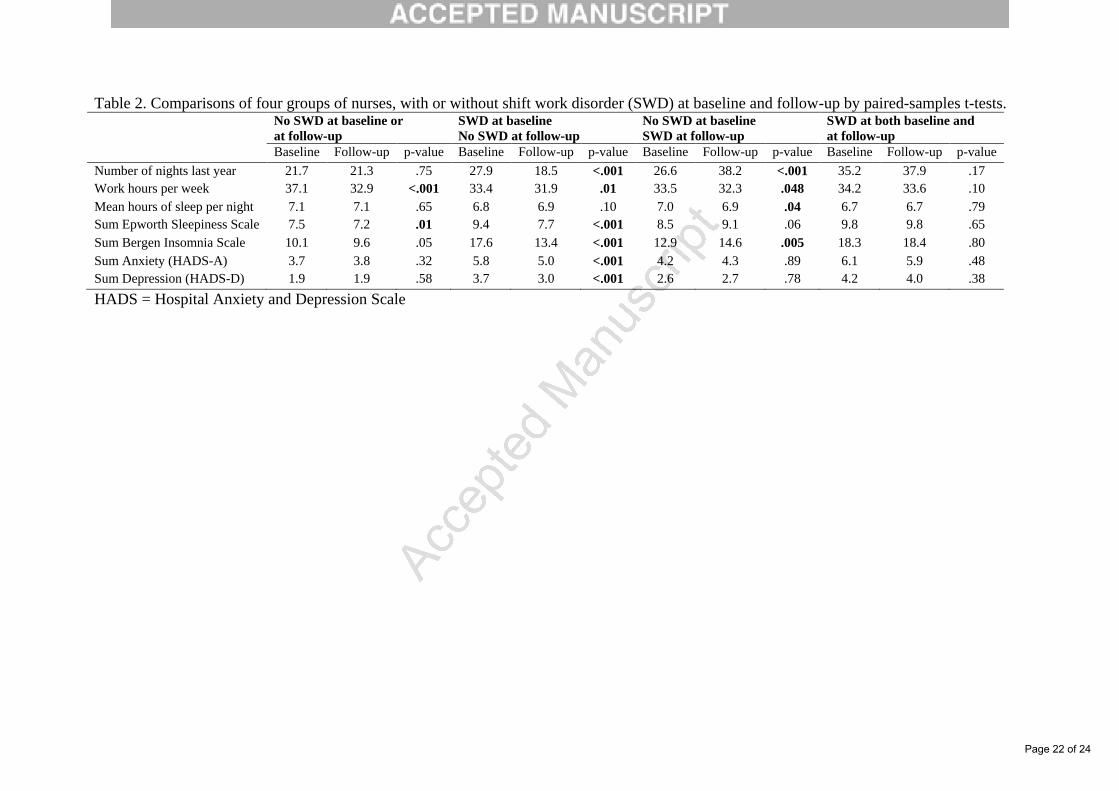
Table 2. Comparisons of four groups of nurses, with or without shift work disorder (SWD) at baseline and follow-up by paired-samples t-tests.
No SWD at baseline or
at follow-up
SWD at baseline
No SWD at follow-up
No SWD at baseline
SWD at follow-up
SWD at both baseline and
at follow-up
Baseline Follow-up p-value Baseline Follow-up p-value Baseline Follow-up p-value Baseline Follow-up p-value
Number of nights last year 21.7 21.3 .75 27.9 18.5 <.001 26.6 38.2 <.001 35.2 37.9 .17
Work hours per week 37.1 32.9 <.001 33.4 31.9 .01 33.5 32.3 .048 34.2 33.6 .10
Mean hours of sleep per night 7.1 7.1 .65 6.8 6.9 .10 7.0 6.9 .04 6.7 6.7 .79
Sum Epworth Sleepiness Scale 7.5 7.2 .01 9.4 7.7 <.001 8.5 9.1 .06 9.8 9.8 .65
Sum Bergen Insomnia Scale 10.1 9.6 .05 17.6 13.4 <.001 12.9 14.6 .005 18.3 18.4 .80
Sum Anxiety (HADS-A) 3.7 3.8 .32 5.8 5.0 <.001 4.2 4.3 .89 6.1 5.9 .48
Sum Depression (HADS-D) 1.9 1.9 .58 3.7 3.0 <.001 2.6 2.7 .78 4.2 4.0 .38
HADS = Hospital Anxiety and Depression Scale
Page 22 of 24
23
Table 3. Logistic regression analyses predicting shift work disorder (SWD) at follow-up
among Norwegian nurses. In the crude analyses each independent variable is analysed one by
one against SWD, in the adjusted analysis they are all included simultaneously. Crude
(N=1440 to 1516)
Adjusted
(N=1196)
Independent variable OR 95% CI OR 95% CI
Age 1.02 1.01-1.04 1.02 1.00-1.04
Gender (female = 1.00) Male 1.19 0.82-1.74 0.88 0.53-1.48
Married/Cohabiting (yes = 1.00) No 1.18 0.92-1.52 1.24 0.86-1.79
Children in household (yes = 1.00) No 0.99 0.79-1.24 .84 0.60-1.18
Sleep medication (no =1.00) Yes 2.40 1.64-3.51 1.03 0.59-1.83
Melatonin (no =1.00) Yes 3.36 1.62-6.99 4.20 1.33-13.33
Bright light (no =1.00) Yes 2.29 1.18-4.45 3.10 1.14-8.39
Over the counter sleep medication (no =1.00) Yes 2.64 1.64-4.25 1.51 0.78-2.93
Smoking (no = 1.00) Yes 1.37 0.96-1.95 0.98 0.60-1.62
Caffeine (daily consumption) 1.06 1.01-1.10 0.99 0.93-1.06
No longer working night shift at follow-up (no = 1.00) Yes 0.22 0.13-0.35 0.12 0.07-0.22
Number of nights per year at baseline 1.01 1.01-1.01 1.01 1.01-1.02
SWD at baseline (no = 1.00) Yes 6.48 5.07-8.29 5.19 3.74-7.20
ESS total score at baseline 1.11 1.07-1.14 1.08 1.04-1.13
BIS total score at baseline 1.07 1.06-1.08 1.02 1.00-1.04
Sum Anxiety (HADS-A) 1.11 1.07-1.14 0.99 0.94-1.06
Sum Depression (HADS-D) 1.16 1.12-1.21 1.07 1.00-1.14
Sum Diurnal Scale 0.94 0.91-0.97 1.01 0.96-1.06
ESS = Epworth Sleepiness Scale, BIS = Bergen Insomnia Scale, HADS = Hospital Anxiety
and Depression Scale, bold = p-values ≤ 0.05
Page 23 of 24

24
Table 4. Logistic regression analyses predicting disappearance of shift work disorder (SWD)
at follow-up among Norwegian nurses with SWD at baseline. In the crude analyses each
independent variable is analysed one by one against SWD, in the adjusted analysis they are all
included simultaneously. Crude
(N=503 to 527)
Adjusted
(N=429)
Independent variable OR 95% CI OR 95% CI
Age 0.98 0.96-1.00 0.97 0.94-1.00
Gender (female = 1.00) Male 0.93 0.55-1.59 1.02 0.51-2.04
Married/Cohabiting (yes = 1.00) No 0.77 0.52-1.14 0.77 0.46-1.30
Children in household (yes = 1.00) No 0.83 0.58-1.17 1.00 6.21-1.61
Sleep medication (no =1.00) Yes 0.53 0.31-0.89 0.71 0.35-1.46
Melatonin (no =1.00) Yes 0.56 0.22-1.41 0.38 0.84-1.69
Bright light (no =1.00) Yes 0.99 0.36-2.80 0.41 0.05-3.27
Over the counter sleep medication (no =1.00) Yes 0.65 0.35-1.21 0.54 0.23-1.25
Smoking (no = 1.00) Yes 1.09 0.65-1.85 1.14 0.58-2.23
Caffeine (daily consumption) 0.90 0.84-.0.97 0.97 0.88-1.07
No longer working night shift at follow-up (no = 1.00) Yes 8.23 4.50-15.05 8.46 4.20-17.00
Number of nights per year at baseline 0.99 0.99-1.00 0.99 0.98-1.00
ESS total score at baseline 0.98 0.93-1.02 0.94 0.89-1.00
BIS total score at baseline 0.99 0.97-1.01 1.00 0.98-1.03
Sum Anxiety (HADS-A) 0.98 0.93-1.02 1.01 0.94-1.09
Sum Depression (HADS-D) 0.96 0.90-1.01 0.93 0.85-1.02
Sum Diurnal Scale 1.02 0.97-1.07 0.99 0.93-1.06
ESS = Epworth Sleepiness Scale. BIS = Bergen Insomnia Scale. HADS = Hospital Anxiety
and Depression Scale. bold = p-values ≤ 0.05
Page 24 of 24