predictors of outcome in panic disorder: a 5-year prospective follow-up study
TRANSCRIPT

JOURNAL OF
AFFECTIVE DISORDERS
Journal of Affective Disorders 3 I (I 996) I I I - I I6 ELSEVIER
Research report
Predictors of outcome in panic disorder: A 5year prospective follow-up study
Gabriele Scheibe ‘, Margot Albus ‘. *
Received 20 February 1996: revised 8 July 1996; accepted 8 July 1996
Abstract
A prospective 5-year follow-up study in patients with panic disorder was carried out in order to determine predictors of outcome. 50 patients presenting at an outpatient clinic for anxiety disorders were enroled initially in a controlled treatment
study using either imipramine or doxepin in addition to supportive psychotherapy and were then followed under naturalistic treatment conditions. By means of multiple stepwise regression analyses comorbidity with current depression, severity of
illness and agoraphobic avoidance turned out to be the strongest predictors. These data confirm the findings of shorter-term prospective follow-up studies and of retrospective studies. In contrast to several reports, illness-related social impairment at
baseline was not found to affect outcome.
Ke~orr/.s: Panic disorder: Predictor: Prospective study; Follow-up
1. Introduction favorable course (Maier and Buller, 1988a; Noyes et
There is a considerable number of variables po-
tentially affecting remission, relapse or the develop- ment of chronicity in patients with panic disorder.
Reviewing the literature, prospective follow-up stud- ies of panic disorder are rare; the majority of follow-
up studies were done prior to the DSM-III (APA, 1980) or DSM-III-R (APA, 1987). were carried out retrospectively, or were short-term follow-up studies. The analysis of predictors of favorable and unfavor- able outcome in patients with panic disorder seems to be especially important, since a rather chronic course (Coryell et al., 1983; Breier et al., 1986; Wittchen and von Zerssen, 1988) as well as a pretty
al., 1989, 1990, 1993) have been reported. Panic or anxiety patients with the complication of
depression were shown to have an unfavorable out-
come or a more chronic illness (von Valkenburg et al., 1984; Thyrer et al., 1985; Breier et al., 1986;
Buller et al., 1986; Krieg et al., 1987; Lelliott et al., 1987; Maier and Buller, 1988b; Noyes et al., 1990;
Scheibe and Albus, 1994). As well, duration of illness before referral has also been shown to be of long-term prognostic relevance (Noyes et al., 1980, 1990; Perssen et al., 1984; Angst and Vollrath, I99 1); patients with a longer duration of illness at admis- sion had a poorer prognosis. In contrast, a chronic nature of panic disorder was reported in patients with
Corresponding author.
a short duration of illness, however severe illness-re- lated psychosocial impairments, by Breier et al.
0 165-0327/96/Z% 15.00 Copyright 0 1996 Elscvier Science B.V. All rights reserved.
PI/ SO 165.0327(96)00077-8
(1986). Also, severity of illness was found to be
associated with a poor prognosis by several authors (Faravelli and Albanesi, 1987: Noyes et al., 1989;
Angst and Vollrath, 1991).
Several naturalistic follow-up studies have shown
that agoraphobia or avoidance behavior predict an unfavorable outcome and a chronic course of anxiety disorders (Noyes et al., 1980; Cloninger et al., 1981;
Perssen et al., 1984; Faravelli and Albanesi, 1987;
Maier and Buller, 1988b; Maier et al., 1989; Noyes
et al., 1990). Conclusively, agoraphobia was sug-
gested to be the best predictor for the severity of anxiety at follow-up (Buller et al., 1986). Some
studies seem to indicate that - even when treatment
significantly reduces the degree and severity of anxi- ety symptoms - avoidance behavior and symptom-
related social consequences tend to persist (Reich,
1986: Krieg et al., 1987; Wittchen and von Zerssen,
1988). Relatively constant levels of illness-related impairment reported Breier et al. (1986), too. Social adjustment at index assessment as predictor of out-
come was reported by Faravelli and Albanesi ( 1987) and by Lelliott et al. (1987).
Until now, there is a lack of information about the long-term course of panic disorder. Shear and Maser
(1994) proposed a standardized assessment package considered essential for panic disorder studies. e.g.,
comorbidity with depression, severity of illness, ago-
raphobic avoidance behavior, duration of illness, and illness-related social disability. The present prospec-
tive S-year follow-up study was designed in order to investigate if there is an effect of these proposed variables on the outcome of patients with panic
disorder. To our knowledge, the present follow-up
study is the first prospective long-term follow-up
study, designed to test predictors of outcome which have been assessed at baseline in patients with panic
disorder during a S-year follow-up period, addressing the question which outcome measures are affected
by comorbidity with depression, symptom variables, as well as illness-related social impairment at base- line.
2. Methods
A total of 89 subjects were recruited through news media and interviewed at the outpatient unit for
anxiety disorders at the Psychiatric Hospital of the
University of Munich; the sample was recruited dur-
ing a I -year time period (April 1987 to May 1988). Of this sample 29 patients did not meet the inclusion
criteria for the initial controlled drug-treatment study
(i.e., age 18-60 years. no additional anxiety disor-
ders. no pregnancy or nursing, no history of physical illness that could explain their symptoms, no suicidal
tendencies, no psychosis, no alcohol or drug depen-
dence). The remaining 60 patients met the DSM-III-R
criteria (APA, 1987) for panic disorder without or
with agoraphobia. Eight of these patients dropped
out of the study, because they refused to participate in the initial controlled drug-treatment study. At
5-year follow-up two patients had moved away and
could not be traced anymore. The total sample fol-
lowed-up for 5 years therefore consisted of 50 pa-
tients with panic disorder (30 without and 20 with concomitant depression at baseline evaluation).
The Structured Clinical Interview for DSM-III-R SCID (Spitzer et al.. 1987) was administered to each
subject by two clinicians (G.S. and M.A.) who were
experienced in using the DSM-III-R classification
system and trained in applying the SCID. In a sub-
sample of patients (II = 30) - randomly selected from the sample investigated - SCID diagnoses were
evaluated independently by both clinicians. The in- terrater-reliability turned out to be good (kappa =
0.89). The SCID was carried out at baseline as well as at S-year follow-up assessment.
Additionally. the following ratings were per-
formed at index assessment and at S-year follow-up. The Hamilton Anxiety Scale (HAMA) (range O-56)
(Hamilton, 1959), and the Hamilton Depression Scale
(HAMD) (range O-67) (Hamilton. 1967). As well, raters took into account all active psychiatric symp-
toms and the overall level of psychosocial adjust- ment to evaluate the Global Assessment Scale (GAS) score (range I- 100) (Spitzer et al., 1976) for the previous 6 months before follow-up.
For the evaluation of panic frequency. the Panic
Attack Scale (Sheehan and Sheehan. 1982). and for the assessment of agoraphobic fear and avoidance and anticipatory anxiety. the Phobia Scale (range O-4 for avoidance behavior: range 0- IO for fear of the phobic stimulus and for intensity of anticipatory anxiety referring to the percentage of time spent in anticipation of a panic episode) (Marks and Math-

G. Scheibe. M. A/bus/Journal ofAffective Disorders 41 (19961 111-116 113
ews, 1979; Cross-National Collaborative Panic Study,
1992), and a Disability Scale rated from 0 = no
impairment to 10 = total impairment (Cross-National
Collaborative Panic Study, 1992) were applied by a telephone or personal interview at least every 3
months during the 2-year follow-up period and at
least every 6 months during the subsequent 3-year
follow-up period. After baseline evaluation, patients were random-
ized and enroled in an S-week controlled drug-treat- ment study of either imipramine or doxepin. In
addition to psychopharmacological treatment, pa-
tients received supportive psychotherapy with a fre- quency of one session per week for 6 to 8 months
depending on their clinical status. After the acute
treatment phase, 58% of the patients markedly im- proved or remitted, 32% of the patients showed a
considerable improvement, and 10% of the patients
showed only slight improvement as measured by the Clinical Global Impressions Scale (CGI; Guy, 1976).
During the following course of the present 5-year
prospective study the patients were treated naturalis-
tically, e.g., no systematic treatment regimen was
applied. The medication was gradually tapered off,
when a patient had been symptom-free for at least 3
months, and drug-treatment was begun again in those patients relapsing after medication discontinuation
(during the 5-year follow-up period in 45% of the sample). During booster sessions symptoms of anxi-
ety and phobic symptoms were evaluated and in-
structions given for in vivo exposure. To evaluate fluctuations of symptoms and social disability and to avoid the bias of inaccurate retrospective reporting,
patients were rated every 3 months during the 2-year follow-up and every 6 months during the subsequent
3-year follow-up period. At 5-year follow-up 37.5% of the patients were taking some anti-anxiety medi-
cation (33.5% in the panic disorder group and 45% of the patients of the comorbid group). Additional
data concerning treatment and evaluations during the 5-year follow-up period have been reported in an- other paper (Albus et al., 1995).
2.1. Sample characteristics
Patients with panic disorder without (n = 12) or with (n = 38) agoraphobia according to DSM-III-R
(APA, 1987) included in the present study were predominantly women (62%). Concerning marital
status 62% of the sample were married, 10% sepa-
rated or divorced, and 28% never married. Mean age
at admission was 38.0 (+ 7.3) years. Age at onset of
panic disorder was on average 28.2 (t- 10.8) years. The patients had a mean duration of illness of 9.9
(kg.61 years. 30 patients met the criteria for panic disorder without a lifetime diagnosis of depression
and 20 patients for panic disorder with a current
diagnosis of major depression (MDE) at baseline
evaluation. The proportion of patients with agora-
phobia (70% and 75%, respectively) was similar in the two groups. As already mentioned, patients with
the presence of other anxiety disorders were not
included in this study. Statistical analyses employed t-tests pairs for de-
pendent samples to test the significance of differ-
ences between index assessment and 5-year follow-up ratings. P values of 0.05 or less were considered as
significant. According to the suggestions of Shear and Maser (1994) a set of 6 potential predictors was
evaluated: Comorbidity with current depression, di-
mensional measures of general anxiety and depres-
sion (HAMA, HAMD), duration of illness, agora-
phobic avoidance behavior, and illness-related social disability at baseline. A stepwise multivariate regres-
sion analysis was performed to test the independent
variables for their predictive power for each outcome
measure. Dependent measures were the following variables at 5-year follow-up: Major depression dur-
ing follow-up, Hamilton Anxiety score, Hamilton Depression score, number of panic attacks, agora-
phobic avoidance behavior, social adjustment, psy- chosocial functioning, and use of psychotropic drugs
during the last 6 months before 5-year follow-up.
3. Results
Index assessment versus 5-year follow-up assess- ment: Significant decreases between index assess- ment and 5-year follow-up occurred in the number of panic attacks as well as in the intensity of anticipa- tory anxiety during the past week, in the Hamilton Anxiety and Depression scores: in agoraphobia (fear
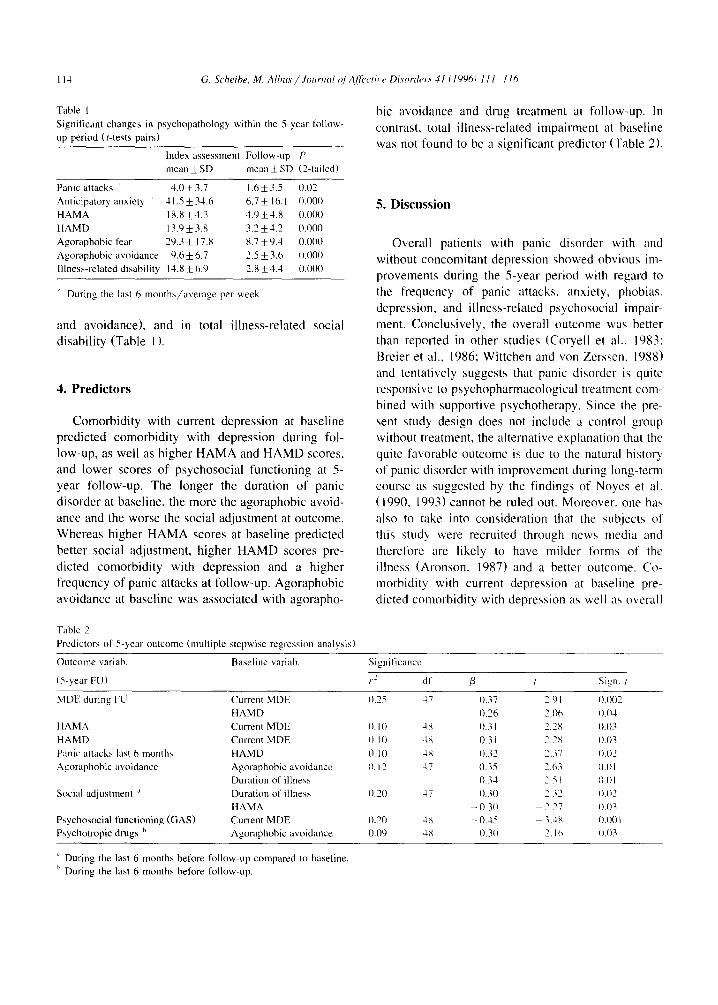
Table I Significant changes in psychopathology within the 5-year follow-
up period (r-tests pairs)
Index assessment Follow-up P
mean f SD mean f SD (Z-tailed)
Panic attacks 1.0 -i_ 3.7 1.6k3.5 0.02
Anticipatory anxiet) 1 I.5 & 34.6 6.7 I 16. I 0.000
HAMA 18.X+4.3 3.9+1.X 0.000
HAMD 13.9+3.x 3.2 k1.2 0.000
Agoraphobic fear 29.3 f 17.8 8.7i9.4 0.000
Agoraphobic avoidance 9.6 f 6.7 2.5 + 3.6 0.000
Illness-related disability 11.8 f 6.9 2.X*1.3 0.000
During the last 6 months/average per week
and avoidance). and in total illness-related social
disability (Table I ).
4. Predictors
Comorbidity with current depression at baseline
predicted comorbidity with depression during fo- low-up, as well as higher HAMA and HAMD scores,
and lower scores of psychosocial functioning at S- year follow-up. The longer the duration of panic
disorder at baseline, the more the agoraphobic avoid-
ance and the worse the social adjustment at outcome. Whereas higher HAMA scores at baseline predicted
better social adjustment, higher HAMD scores pre- dicted comorbidity with depression and a higher
frequency of panic attacks at follow-up. Agoraphobic
avoidance at baseline was associated with agorapho-
Table 2
Predictors of 5-year outcome (multiple stepwiae regression analysis)
bit avoidance and drug treatment at follow-up. In
contrast. total illness-related impairment at baseline was not found to be a significant predictor (Table 2).
5. Discussion
Overall patients with panic disorder with and
without concomitant depression showed obvious im- provements during the S-year period with regard to
the frequency of panic attacks, anxiety. phobias.
depression, and illness-related psychosocial impair-
ment. Conclusively, the overall outcome was better
than reported in other studies (Coryell et al.. 1983;
Rreier et al.. 1986; Wittchen and von Zerscen. 1988) and tentatively suggests that panic disorder is quite
responsive to psychopharmacological treatment com-
bined with supportive psychotherapy. Since the pre-
sent study design does not include a control group without treatment, the alternative explanation that the
quite favorable outcome is due to the natural history
of panic disorder with improvement during long-term course as suggested by the findings of Noyes et al.
( 1990, I9931 cannot be ruled out. Moreover. one haa
also to take into consideration that the subjects of this study were recruited through news media and
therefore are likely to have milder forms of the illness (Aronson. 1987) and a better outcome. Co- morbidity with current depression at baseline pre-
dicted comorbidity with depression as well as overall
Outcome variab
(T-year FU)
MDE during FL1
HAMA
HAMD
Panic attacks last 6 months
Agoraphobic avoidance
Social adjustment ”
Psychosocial functioning (GAS)
Psychotropic drugs h
Baseline variah Significance
Current MDE
HAMD
Current MDE
Current MDE
HAMD
Agomphobic a\ oidance
Duration of illness
Duration of illness
HAMA
Current MDE
Agoraphobic avoidance
p dl P / sign. ,
0.75 17 0.37 2 91 0.002
0.16 0. IO 4X 0.31
0. IO 4X 0.31
0. IO 4s 0.32
0. I2 17 0.35
0.34
0.20 47 0.30
- 0.30 0.20 4X - 0.15 _
0.09 4X 0..10
0.01
0.03
0.03
0.02
0.01
0.01
0.07
0.03
0.00 I 0.03
“ During the last 6 months before follow-up compared to baseline
’ During the last 6 months hefore follow-up.
severity (HAMA, HAMD) and psychosocial func-
tioning (GAS) at follow-up in accordance with other
reports (Breier et al., 1986; Maier and Buller, 1988b;
Noyes et al., 1990, 1993; Lelliott et al., 1987; Pol- lack et al., 1993; Ball et al., 1994; Scheibe and
Albus, 1994). This finding strongly suggests that
comorbidity with depression is the best known com-
plication in panic patients influencing a less favor-
able outcome.
In our study a higher severity of depressive symp-
toms due to current MDE at index assessment as
measured by the HAMD predicted comorbidity with depression as well as frequency of panic attacks at
follow-up. In concordance with other reports, sever-
ity of illness or symptom ratings turned out to be
associated with poorer prognosis (Faravelli and Al-
banesi, 1987; Noyes et al., 1989, 1990, 1993). Our finding that a longer duration of illness be-
fore index assessment predicts a worse outcome
concerning agoraphobic avoidance behavior and so-
cial adjustment is in line with most other authors
(Noyes et al., 1980, 1990, 1993; Perssen et al., 1984;
Angst and Vollrath, 1991; Pollack et al., 19931, suggesting that course is best predicted by former
course. These results point at the necessity to treat
panic patients as early in the course of the illness as
possible. Agoraphobic avoidance behavior at baseline pre-
dicted agoraphobic avoidance behavior as well as intake of psychotropic drugs during the last 6 months
before 5-year follow-up. This finding is in line with Noyes et al. (1989) who reported that the agorapho-
bic symptom complex remains stable over time in
patients with panic disorder and agoraphobia. Con- clusively, avoidance behavior as predictor of a Iess
favorable outcome of anxiety disorders was found to be in line with many other studies (Noyes et al.,
1980; Cloninger et al., 198 1; Perssen et al., 1984; Faravelli and Albanesi, 1987; Maier and Bullet-,
1988b; Maier et al., 1989; Noyes et al., 1990). In contrast to several other studies (Breier et al.,
1986; Reich, 1986; Faravelli and Albanesi, 1987; Lelliott et al., 1987; Noyes et al., 1989) we found total illness-related social impairment at baseline as measured by the social adjustment scale not to be a significant predictor. These contrasting results can be explained by the relatively low level of overall im- pairment in our patient group at S-year follow-up
compared to the above cited studies, suggesting that the majority of patients seems to function satisfacto-
rily in their daily lives. Therefore, when taking into
account the data on outcome in panic disorder pub- lished so far, one can assume, that a treatment regimen with initial treatment with psychotropic
drugs and psychotherapy had influenced the course of panic disorder with or without concomitant de-
pression favorably.
In summary, the data of this prospective long-term
follow-up study confirm the findings of shorter-term prospective follow-up studies and of retrospective
studies that comorbidity with current depression,
severity of illness, duration of illness, and agorapho-
bic avoidance behavior at baseline are the most
relevant predictors of outcome in patients with panic disorder. In contrast, the degree of illness-related
social impairment at baseline as a relevant predictor
of outcome is not supported by our data.
References
Albus, M., Scheibe, G. and Scherer, J. (1995) Panic disorder with
or without concomiiant depression 5 years after treatment: a
prospective follow-up. J. Affect. Disord. 34, 109-l 15.
American Psychiatric Association (I 980) Diagnostic and Statisti-
cal Manual of Mental Disorders, 3rd Edn. (DSM-III). Ameri-
can Psychiatric Association, Washington, DC.
American Psychiatric Association (1987) Diagnostic and Statisti-
cal Manual of Mental Disorders. 3rd Edn.-Revised (DSM-III-
R). American Psychiatric Association, Washington, DC.
Angst, J. and Vollrath, M. (1991) The natural history of anxiety
disorders. Acta Psychiatr. Stand. 84, 446-452.
Aronson. T.A. (1987) A follow-up of two panic disorder agora-
phobic study populations; the role of recruitment biases. J.
Nerv. Ment. Disord. 17.5, 595-598.
Ball. S.G., Otto, M.W., Pollack, M.H. and Rosenbaum, J.F.
(1994) Predicting prospective episodes of depression in pa-
tients with panic disorder: a longitudinal study. J. Consult.
Clin. Psychol. 62, 359-365.
Breier, A., Charney, D.S. and Heninger. G.R. (1986) Agoraphobia
with panic attacks. Development, diagnostic stability, and
course of illness. Arch. Gen. Psychiatry 43. lO29- 1036.
Buller. R.. Maier, W. and Benkert, 0. (1986) Clinical subtypes in panic disorder: Their descriptive and prospective validity. J.
Affect. Disord. I I, 105-l 14.
Cloninger, C.R., Martin, R.L., Clayton, P. and Guze, J.B. (1981)
A blind follow-up and family study of anxiety neurosis:
Preliminary analysis of the St. Louis 500. In: Klein, D.F. and
Rabkin, J. (Eds.). Anxiety: New Research and Changing Con-
cepts. Raven Press, New York, NY. pp. 137-148.
Coryell. W.. Noyes, R. and Clancy. J. (1983) Panic disorder and
I I6 G. Scheibe, M. A/bus/ Jounml @Aff~riw Disorder.\ 41 (10961 I I I- I I6
primary unipolar depression: A comparison of background and
outcome. J. Affect. Disord. 5, 31 l-317.
Cross-National Collaborative Panic Study, Second Phase Investi-
gators (1992) Drug treatment of panic disorder. Comparative
efficacy of alprazolam, imipramine. and placebo. Br. J. Psy-
chiatry 160, I9 I-202.
Faravelli, C. and Albanesi, G. (1987) Agoraphobia with panic
attacks - One year prospective follow-up. Compr. Psychiatry
28. 48 l-487.
Guy, W. (1976) CGI. Clinical global impressions. In: ECDEU
Assessment Manual for Psychopharmacology. Rev. Ed.,
Rockville. MD. pp. 217-222.
Hamilton, M.A. (1959) The assessment of anxiety states by rating.
Br. J. Med. Psychol. 32, 50-55.
Hamilton, M.A. (1967) Development of a rating scale for primary
depressive illness. Br. J. Clin. Psycho]. 6, 278-296.
Krieg, J.-C., Bronisch, T., Wittchen, H.-U. and von Zerssen, D.
(1987) Anxiety disorders: A long-term prospective and retro-
spective follow-up study of former inpatients suffering from
an anxiety neurosis or phobia. Acta Psych&. Stand. 76,
36-47.
Lelliott. P.T.. Marks, I.M.. Monteiro. W.O.. Tsakiris, F. and
Noshirvani, H. (1987) Agoraphobics 5 years after imipramine
and exposure: Outcome and predictors. J. Nerv. Ment. Dis.
175, 599-605.
Maier. W. and Buller, R. ( I988a) The course of panic attacks and
agoraphobia. Arch. Gen. Psychiatry 45, 501.
Maier. W. and Buller, R. (1988b) One-year follow-up of panic
disorder. Eur. Arch. Psychiatr. Neural. Sci. 238, 105-109.
Maier, W., Rosenberg, R., Argyle, N., Buller, R., Roth. M.,
Brandon, S. and Benkert, 0. (1989) Avoidance behaviour and
major depression in panic disorder: A report from the Crosa-
National Collaborative Panic Study. Psychiatr. Dev. 2. 123-
142.
Marks, I.M. and Mathews, A.M. (1979) Brief standard self-rating
for phobic patients. Behav. Res. Ther. 17, 263-267.
Noyes, R., Clancy, J., Hoenk. P.R. and Slymen, O.J. (1980) The
prognosis of anxiety neurosis. Arch. Gen. Psychiatry 37, 173-
178.
Noye\, R., Garvey, M.J. and Cook, B.L. (1989) Follow-up study
of patients with panic disorder and agoraphobia with panic
attacks treated with tricyclic antidepressants. J. Affect. Disord.
16. 249-257.
Noyes. R.. Reich, J., Christiansen, J., Suelzer, M., Pfohl, B. and
Coryell, W.A. (1990) Outcome of panic disorder: Relationship
to diagnostic subtypes and comorbidity. Arch. Gen. Psychiatry
37. 809-X 18.
Noyes, R.. Clancy, J.. Woodman, C.. Holt. C.S.. Sueller, M..
Christiansen, J. and Anderson, D.J. (1993) Environmental
factors related to the outcome of panic disorder. A heven-yea,
follow-up study. J. Nerv. Ment. Di\. 181. 529-538.
Persscn. G., Alstrom, J.E. and Nordlund, C.L. (1984) Prognostic
factor\ with four treatment method?. for phobic disorders. Acta
Psychiatr. Stand. 69, 307-3 18.
Pollack. M.H.. Otto. M.W.. Tesar. G.E.. Cohen. L.S.. Meltc.er-
Brody. S. and Rosenbaum. J.F. (1993) Long-term outcome
after acute treatment with alprazolam or clonaLepam for panic
disorder. J. Clin. Psychopharmacol. 13. 257-263.
Reich. J. (19X6) The epidemiology of anxiety. J. Nerv. Ment. Dia.
174, 129.- 136.
Scheihe. G. and Albus. M. (1994) Prospective follow-up study
lasting 2 years in patients with panic disorder with and without
depreasibt: disorders. Eur. Arch. Psychiatry Clin. Neuroaci.
344, 39-43.
Shear. M.K. and Maser. J.D. (1994) Standardized assessment fog
panic disorder research. Arch. Gen. Psychiatry 5 I, 346-354.
Sheehan. D.V. and Sheehan, K.E. (1982) The classification of
anxiety and hysterical states. J. Clin. Psychopharmacology 2.
235-243
Spitzer. R.L.. Gibbon. M., Endicott. J.. Fleias, J.L. and Cohen, J.
(1976) The Global Assessment Scale: A procedure for measur-
ing overall severity of psychiatric disturbance. Arch. Gen.
Psychiatry 33. 766-77 I. Spitzer, R.L.. Williams, J.B.W. and Gibbon. M. (19X7) Structured
Intervieu for DSM-III-R (SCID). Biometric\ Reseal-ch Depdrt-
ment. New York State Psychiatric Institute. New York, NY.
Thyrer. B.A., Nesse. R.M.. Cameron, O.G. and Curtis. G.C.
(1985) Agoraphobia: A test of the \eparation anxiety hypothe-
sib. Behav. Res. Ther. 23. 75-78.
van Valkenburg, C., Akiskdl, H.S.. Purantian, V. and Rosenthal.
T. (1984) Anxious depressions: Clinical, family history. and
naturalistic outcome-compari\onh with panic and major de-
prehsive disorders. J. Affect. Diaord. 6. 67-Q.
Wittchen. H.-U. and van Zersben. D. (198X) Verlzufe hehandelter
und unhehandelter Depresaionen und Angslhtiirungen.
Springer. Berlm.