predictive value of hemostatic factors for sudden death in patients with stable angina pectoris
TRANSCRIPT

Predictive Value of Hemostatic Factors for Sudden Death in Patients With Stable
Angina Pectoris Daniel Benchimol, MD, Jean-FranCois Dartigues, MD, PhD, H&l&e Benchimol, MD,
Franqoise Drouillet, BA, Philippe Lauribe, MD, Marc Marazanof, MD, Thierry Couffinhal, MD, PhD, and Jacques Bonnet, MD
To assess hemostatic risk factors for sudden death in patients with stable angina, 323 consecutive patients were recruited prospectively. Patients with clinical heart failure or recent myocardial infarction were excluded. The followin gender, smo &
clinical variables were recorded: age, ing habits, hypertension, previous myo-
cardial infarction, left ventricular hypertrophy, and severe ventricular arrhythmia. Angiographic variables included coronary extent, assessed from Jenkins’ and mean atherosclerotic scores, and left ventricular eiec- tion fraction. Lipid variables included total cholesterol, triglycerides, high-density lipoprotein cholesterol, low- density lipoprotein cholesterol, and a lipoproteins A-l and B. Hemostatic factors included ibrinogen, fibrin- r opeptide A, antithrombin III, factor VIII antigen, factor WI coagulant, protein C, plasminogen, a2 antiplasmin, eu be!
lobulin clot lysis time, tissue plasminogen activator ore and after venous occlusion, and plasminogen
activator inhibitor. There were 34 deaths, 19 of which were sudden during the follow-up period (60 2 17 months). The association between each variable and the risk of sudden death was assessed by calculating the relative risk with the Cox univariate model. All sig- nificant predictors from the univariate analysis were then incorporated in a Cox multivariate model to select the independent predictors of sudden death. The inde-
r ndent predictors of sudden death were left ventricu-
ar h 1
pertrophy (p cO.O4), lower left ventricular ejec- tion raction (p cO.O4), and shorter euglobulin clot lysis time after venous occlusion (p <0.02), whereas fibrin- ogen (p ~0.07) and Jenkins’ score (p eO.08) were bor- derline. Determination of hemostatic variables, es
tK e-
cially those pertaining to dynamic fibrinolysis, may us be of value in assessing risk of sudden death.
(Am J Cardiol 1995;76:241-244)
C oronary artery disease remains the most important cause of sudden death in adu1ts.l Numerous studies
have established clinical,2,3 electrocardiographic,4 elec- trophysiologic,5 and ventriculographic4 risk factors for sudden cardiac death, especially after myocardial infarc- tion, but there are few published data on possible bio- logic risk factors in patients with stable angina. Biolog- ic factors, especially those involving hemostasis, appear to play an important role in the onset of acute ischemic episodes leading to sudden death in patients with coro- nary artery disease. 1~6,7 Acute ischemia is thought to be a major determinant of the fatal arrhythmia, probably in connection with other triggering factors (preexisting pathologic myocardium, ventricular premature beats, metabolic disturbances, autonomic nervous system dis- turbances, toxic effect of drugs, and so forth). This find- ing is supported by the results of postmortem examina- tions of patients who died suddenly.8 The present prospective study was therefore designed to identify bio- logic risk factors, especially with respect to hemostatic factors and the markers of atherogenesis, for sudden death in patients with stable angina pectoris and with- out clinical heart failure. From the Service de Cardiologie et Maladies Vasculaires, Ho ital Cardiologique, Pessac, the Departement d’lnformatique Medica e et P de Statistiques Universite de Bordeaux II/ INSERM Unite 330, Bor- deaux, and the INSERM Unite 8 de Cardiologie, Pessac, France. Manuscript received February 6, 1995; revised manuscript received and accepted May 23, 1995.
Address for reprints: Jacques Bonnet, MD, Service de Card& gie et des Maladies Vasculaires, Hopital Cardiologique, 33604 Pes- sac, France.
PATIENTS Selection criteria: Consecutive patients with angina
that was stable or had been stabilized for 22 weeks with oral antianginal therapy, or those presenting for a. rou- tine angiographic examination after a previous myocar- dial infarction 22 months previously, were prospectively included. Patients had blood samples taken for deter- mination of lipid and hemostatic factors before the coro- nary angiographic examination, which they all under- went to assess the presence and extent of their coronary artery disease. The antianginal drugs most often taken were 6 blockers, long-acting nitrates, and calcium antag- onists. To avoid possible effects on the factors measured, patients with angina not stabilized or those who had had a recent myocardial infarction, or recent arterial punc- ture or hematoma were excluded. Noncoronary artery disease (except for hypertension), clinical heart failure, chronic systemic disease (inflammatory or infectious), or neoplasic pathologies that could affect the test results or the follow-up were also considered exclusion criteria.
Patient population: Between October 1984 and Feb- ruary 1987,384 consecutive patients admitted in our car- diology department for a coronary angiography were preselected. Among these 384 patients, only 323 with angiographically documented coronary artery disease and a complete blood sample were finally included in the study population. Forty-eight patients with strictly normal coronary angiograms were excluded. Thirteen other patients were excluded: 2 refused the planned coro- nary arteriography, 9 had an incomplete blood sample, and the last 2 died before inclusion.
CORONARY ARTERY DISEASE/HEMOSTATIC RISK FACTORS FOR SUDDEN DEATH 241
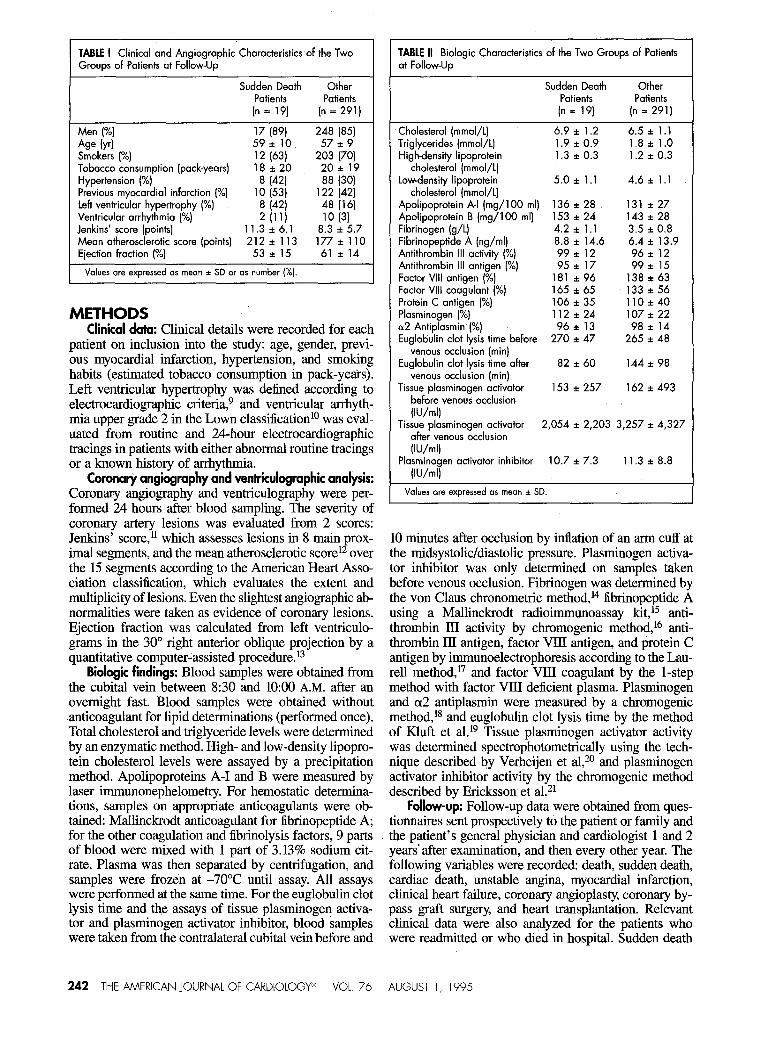
TABLE I Clinical and Angiographic Characteristics of the Two Groups of Patients at Follow-Up
Sudden Death Other Patients Patients
(n = 19) (n = 291)
Men (%) 17 (89) 248 (85)
Age (yd 59* 10 57 f 9 Smokers (%) 12 (63) 203 (70) Tobacco consumption (pack-years) 18i20 20* 19 Hypertension (%) 8 (421 88 (30) Previous myocardial infarction (%) 10 (53) 122 (42) Left ventricular hypertrophy (%) 8 (42) 48 (16) Ventricular arrhythmia (%) 2 (111 10 13) Jenkins’ score (points) 11.3 zt 6.1 8.3 A 5.7 Mean atherosclerotic score (points) 2 12 + 1 13 177* 110 Ejection fraction (%) 53*15 61 sz 14
Values are exp’ressed CIS mean * SD or as number (%I.
METHODS _ _ Clinical data: Clinical details were recorded for each
patient on inclusion into the study: age, gender, previ- ous myocardial infarction, hypertension, and smoking habits (estimated tobacco consumption in pack-ye&s). Left ventricular hypertrophy was defined according to electrocardiographic criteria,9 and ventricular arrhyth- mia upper grade 2 in the Lown classification10 was eval- uated from routine and 24-hour electrocardiographic tracings in patients with either abnormal routine tracings or a known history of arrhythmia.
Corona* angiography and ventriculographic analysis: Coronary angiography and ventriculography were per- formed 24 hours after blood sampling. The severity of coronary artery lesions was evaluated from 2 scores: Jenkins’ score,” which assesses lesions in 8 main prox- imal-segments, and the mean atherosclerotic score12 over the 15 segments according to the American Heart Asso- ciation classtication, which evaluates the extent and multiplicity of lesions. Even the slightest angiographic ab- normalities were taken as evidence of coronary lesions. Ejection fraction was calculated from left ventriculo- grams in the 30” right anterior oblique projection by a quantitative computer-assisted procedure.13
Biologic findings: Blood samples were obtained from the cubital vein between 8:30 and lo:00 A.M. after an overnight fast. Blood samples were obtained without .anticoagulant for lipid determinations (performed once). Total cholesterol and triglyceride levels were determined by an enzymatic method. High- and low-density lipopro- tein cholesterol levels were assayed by a precipitation method. Apolipoproteins A-I and B were measured by laser immunonephelometry. For hemostatic determina- tions, samples on appropriate anticoagulants were ob- tained: Mallinckrodt anticoagulant for fibrinopeptide A; for the other coagulation and fibrinolysis factors, 9 parts of blood were mixed with 1 part of 3.13% sodium cit- rate. Plasma was then separated by centrifugation, and samples were frozen at -70°C until assay. All assays were performed at the same time. For the euglobulin clot lysis time and the assays of tissue plasminogen activa- tor and plasminogen activator inhibitor, blood samples were taken from the contralateral cubital vein before and
242 THE AMERICAN JOURNAL OF CARDIOLOGY@ VOL. 76
TABLE II Biologic Characteristics of the Two Groups of Patients at Follow-Up
Sudden Death Other Patients Potients (n = 19) (n = 291)
Cholesterol (mmol/t) 6.9 i 1.2 6.5 i 1.1 Triglycerides (mmol/L) 1.9 * 0.9 1.8 * 1.0 High-density lipoprotein 1.3 i 0.3 1.2 * 0.3
cholesterol (mmol/L) Lowdensity lipoprotein 5.0 * 1.1 4.6 zt 1.1
cholesterol (mmol/L) Apolipoprotein A-l (mg/lOO ml) 136 * 28 131 zt 27 Apolipoprotein B (mg/lOO ml) 153 * 24 143 zt 28 Fibrinogen (g/t) 4.2 A 1.1 3.5 i 0.8 Fibrinopeptide A (rig/ml) 8.8 zt 14.6 6.4 i 13.9 Antithrombin Ill activity (%) 99*12 96~12 Antithrombin Ill antigen (“A) 95i17 99i.5 Factor VIII antigen (%) 181 zt 96 138 it 63 Factor VIII coagulant (%) 165 zt 65 133 i 56 Protein C antigen (%) 106 * 35 110*40 Plasminogen (%) 112i24 107*22 or2 Antiplasmin (%) 96+13 98+14 Euglobulin clot lysis time before 270 * 47 265 A 48
venous occlusion (min) Euglobulin clot lysis time after 82 *60 144 * 98
venous occlusion (min) Tissue plasminogen activator 153 + 257 162 * 493
before venous occlusion
VJ/mll Tissue plasminogen activator 2,054 * 2,203 3,257 * 4,327
after venous occlusion NJ/ml1
Plasminogen activator inhibitor 10.7 * 7.3 11.3 i 8.8
(Wmll
Values are expressed as mean * SD.
10 minutes after occlusion by inflation of an arm cuff at the midsystolic/diastolic pressure. Plasminogen activa- tor inhibitor was only determined on samples taken before venous occlusion. Fibrinogen was determined by the von Claus chronometric method,14 fibrinopeptide A using a Mallinckrodt radioimmunoassay k&l5 anti- thrombin III activity by chromogenic method,” anti- $rombin ID antigen, factor VIII antigen, and protein C antigen by immunoelectrophoresis according to the Lau- rell method,17 and factor VIII coagulant by the l-step method with factor VIII deficient plasma. Plasminogen and a2 antiplasmin were measured by a chromogenic metbod,18 and euglobulin clot lysis time by the method of Kluft et al.l9 Tissue plasminogen activator activity was determined spectrophotometrically using the tech- nique described by Verheijen et al,2o and plasminogen activator inhibitor activity by the chromogenic method described by Ericksson et a1.21
Follow-up: Follow-up data were obtained from ques- tionnaires sent prospectively to the patient or family and the patient’s general physician and cardiologist 1 and 2 years’ after examination, and then every other year. The following variables were recorded: death, sudden death, cardiac death, unstable angina, myocardial infarction, clinical heart failure, coronary angioplasty, coronary by- pass graft surgery, and heart transplantation. Relevant clinical data were also analyzed for the patients who were readmitted or who died in hospital. Sudden death
AUGUST 1, 1995

was defined as death occurring within 1 hour after onset of symptoms in the absence of any noncardiac cause.22 Cardiac death was defined as that from any cardiac cause (sudden death, fatal myocardial infarction, heart failure).
Statistical analysis: The association between the stud- ied variables and the risk of sudden death was assessed by calculating the relative risk and its corresponding 95% confidence interval using the Cox univariate proportion- al-hazards model (BMDP software). All significant cor- relates of sudden death emerging from the univariate analyses were then incorporated in a Cox multivariate model to identify independent predictors of sudden death.
RESULTS Patient characteristics: Among the 323 patients (278
men and 45 women, mean age 57 2 9 years) included in the study, hypertension was found in 102 (32%), and 140 (44%) had had a myocardial infarction. There were 227 smokers (70%) and 96 nonsmokers (30%). Mean tobac- co consumption was 20 f 19 pack-years. Fifty-six patients (17%) had left ventricular hypertrophy. A ventricular arrhythmia was found in 12 patients (4%). Jenkins’ score was 8.6 f 5.8 and the mean atherosclerotic score was 180 + 110. Mean ejection fraction was 60 f 14%. One hun- dred one patients received l3 blockers (31%), 233 calci- um antagonists (72%), 223 long-acting nitrates (69%), 142 oral anticoagulants (44%), and 73 lipid-lowering fibrates (23%). The mean follow-up period was 60 + 17 months for a total of 310 patients. There were 34 deaths (11 %), of which 24 were cardiac (8%) and 19 were sudden (6%). Ten patients (3%) died from noncardiac causes (cancer in 5, septicemia in 1, acute hemorrhagic pancreatitis in 1, renal insufficiency in 1, suicide in 1, and a car accident in 1). Ten patients (3%) developed clinical heart failure, lead- ing to heart transplantation in 2. Seven patients (2%) had a new myocardial infarction, and unstable angina was found in 36 patients (12%). Coronary angioplasty was per- formed in 53 patients (17%), and 9 (3%) had a second angioplasty; 93 patients (30%) underwent coronary artery bypass graft surgery.
Univariate analysis of sudden death risk factors: The clinical and angiographic characteristics of patients (sud- den deaths and the others) for whom follow-up was obtained are listed in Table I. The biologic data are list- ed in Table II. The univariate predictors of sudden death were lower ejection fraction (p <0.03), left ventricular hypertrophy (p ~0.02) Jenkins’ score (p <0.03), fib- rinogen (p <0.0003), von Willebrand factor (p <O.Ol), factor VIII coagulant (p <0.02), and euglobulin clot lysis time after venous occlusion (p cO.02).
Multivariate analysis of sudden death risk factors: To define the independent risk factors of sudden death, the univariate correlates of sudden death were analyzed in a Cox multivariate model. The independent predictors of sudden death were lower ejection fraction (p ~0.04) and a relative risk of 0.74 for a decrease of lo%, left ventricular hypertrophy (p ~0.04) with a relative risk of 2.94, and euglobulin clot lysis time after venous occlu- sion (p ~0.02) with a relative risk of 0.90 for a decrease of 10 minutes. Fibrinogen (p ~0.07) and Jenkins’ score (p ~0.08) were borderline.
DISCUSSION We found a 6% incidence of sudden death in our pa-
tients with stable coronary artery disease. We also iden- tified the usual clinical and angiographic predictors of sudden death, namely low left ventricular ejection frac- tion23,24 and left ventricular hypertrophy.25 These 2 fac- tors are indicative of a severely altered myocardium, which may predispose to sudden death. We found that the severity of the stenoses of major proximal arteries, as reflected by Jenkins’ score, bore a relation to the risk of sudden death, whereas the diffuse extent of coronary atherosclerosis, as assessed by the mean atherosclerotic score, did not.
The lipid markers and predictors of atherosclerosis progression were not found to be predictors of sudden death. This result for cholesterol is in line with the results of the combined Albany-Framingham studies.2 Among the markers of coagulation and thrombosis, fibrinogen levels appeared to be the sole significant predictors. This result is consistent with its predictive value for cardiac death and myocardial infarction.26,27 The negative results for most of the hemostatic factors tested were not alto- gether unexpected, because these factors, especially fib- rinopeptide A, tend to be elevated in acute circumstances in the presence of an evolving thrombotic process, and according to inclusion criteria these circumstances were excluded in our study. However, there is also evidence for possible sudden death independent of an acute ische- mic process mainly through arrhythmic mechanisms.28 The most unexpected finding was the fibrinolytic profile of the patients who died suddenly. The euglobulin clot lysis time after venous occlusion emerged as an inde- pendent predictor of sudden death. This shorter lysis time, corresponding to a higher fibrinolytic potential, might be regarded as protective.
Malmberg et a12g pointed out an elevation in plas- minogen activator inhibitor activity in young men after a recent myocardial infarction that predicted long-term cardiac death. However, this population was quite dif- ferent from ours. Jansson et a130 observed that a higher tissue plasminogen activator mass concentration was predictive of long-term mortality in patients with coro- nary artery disease. Thus, a higher fibrinolytic potential rather than a patent fibrinolytic deficiency seems predic- tive of cardiac and sudden death risk. As suggested by Jansson et al,3o this is probably the correlate of complex interactions between circulating and parietal fibrinolytic factors. It is noteworthy that the alteration observed was in the dynamic euglobulin clot lysis time, which proba- bly reflects enhanced parietal release of tissue plas- minogen activator. The absence of a relation to tissue plasminogen activator and plasminogen activator in- hibitor may have been due to the fact that when this study was begun, we were only able to assay activity.
Another problem was to determine whether the per- turbation of fibrinolytic potential was a chronic risk fac- tor. The assays performed in stable clinical conditions supported such hypothesis. Genetic polymorphism con- trolling the plasma levels of tissue plasminogen activa- tor and its inhibitor is not yet clearly established. Sev- eral possibilities could account for the link between this
CORONARY ARTERY DISEASE/HEMOSTATIC RISK FACTORS FOR SUDDEN DEATH 243

higher fibrinolytic potential and the risk of sudden death. The higher fibrinolytic potential of the vascular system under stimulation may be just an indirect marker of severe endothelial dysfunction. The endothelial distur- bance could, in acute circumstances, contribute to pari- eta1 complications, which in turn trigger fatal arrhyth- mia through ischemia. The higher levels of factor VIII may be a further indicator of parietal disturbance. Anoth- er possibihty is that a higher fibrinolytic potential is a direct risk for sudden death through a rapid dissolution of the thrombus induced in an acute cardiac event, lead- ing to severe arrhythmia during reperfusion. The analy- sis of markers of dynamic physiologic fibrinolysis and of endothelial dysfunction as risk factors for sudden death in patients with coronary artery disease will be of interest.
The main limitation of this study was the few patients who had sudden death; this causes a lack of statistical power. Moreover, with the number of variables tested, 2 other problems may have occurred during the statistical analysis: the multiplicity of tests and a possible lack of fit for the logistic model. However, in the multivariate analysis, only 7 variables were tested, which reduces this kind of limitation.
1. Myerburg R, Kessler K, Bassett A, Castellanos A. A biological approach to sud- den cardiac death. Structure, function, and cause. Am JCardiol1989;15:1512-1516. 2. Kannel WB, Doyle JT, McNamara PM, Quickenton P, Gordon T. Precursors of sudden coronary death: factors related to the incidence of sudden death. Circula- tion 1975;51:6Oti13. 3. Doyle JT, Kannel WB, McNamara PM, Quickenton P, Gordon T. Factors relat- ed to suddenness of death from coronary disease: combined Albany-Framingham studies. Am J Cardiol 1976;37:1073-1078. 4. Bigger JT Jr, Fleiss JL, Kleiger R, Miller JP, Rohritzky LM. The relationships among ventricular arrhythmias, left ventricular dysfunction, and mortality in the 2 years after myocardial infarction. Circulation 1984;54:25l.%258. 5. Hamer A, Vohra J, Hunt D, Sloman G. Prediction of sudden death by electro- physiologic studies in high risk patients surviving acute myocardial infarction. Am J Cardiol 1982;50:223-229. 6. Goldstein S. Toward a new understanding of the mechanism and prevention of sudden death in coronary heart disease. Circulation 1990:82:284-288. 7. Verheugt FWA, Brugada P. Sudden death after acute myocardial infarction: the forgotten thrombotic view. Am J Cardiol 1991;67:113&1134. 8. Davies MJ, Thomas AC. Thrombosis and acute coronary artery lesion in sud- den cardiac ischemic death. N EngJ J Med 1984;310:1137-1140. 9. Levy D, Lahib SB, Anderson KM, Christiansen JC, Kannel WB, Castelli WP. Determinants of sensitivity and specificity of electrocardiographic criteria for left
ventricular hypertrophy. Circulatioion 1990;81:815-820. 10. Lawn B, Wolf M. Approaches to sudden death from coronary heart disease. Circulation 1971;44:130-142. 1 I. Jenkins PJ, Harper RW, Nestel PJ. Severity of coronary atherosclerosis relat- ed to lipoprotein concentration. Br Med J 1978;2:388-391. 12. Oysel N, Bonnet J, Vergnes C, Benchimol D, Boisseau MR, Moreau C, Bernadet P, Baudet E, Larrue J, Bricaud H. Risk factors for myocardial infarction during coronary artery bypass graft surgery. Eur Heart J 1989;10:806815. 13. Colle JP, Rahal S, Ohayon J, Bonnet J, Le Goff G, Besse P, Bricaud H. Glob-
al left ventricular function and regional wall motion in pure mitral stenosis. Clin Cardiol 1984;7:573-580. 14. van Claus A. Gerhmungsphysiologische schnelhnethode zur bestimmung des tibrinogens. Acta Haemntol 1957;17:237-246. 15. Hockum C. Radioimmunoassay of flbrinopeptide A. Clinical applications. Thromb Res 1976;8:225-236. 16. Abildgaard U, Lie M, Odegard OR. Antithrombm (heparin cofactor) assay with new chromogenic substrates (S-2238 and chromozym TH). Thromb Res 1977;ll: 549-553. 17. Laurel1 CB. Quantitative estimation of proteins by electrophoresis in agarose gel containing antibodies. Ann Biochem 1966;15:57-65. 18. Frieberger P, Knos M, Gustavsson S, Aurell L, Gleason G. Methods for the determination of plasmin, antlplasmin and plasminogen by means of substrate S- 2251. Haemostasis 1978;7:138-145. 19. Kluft C, B&man P, Veldhyzn-Stolk EC. Screening of i’ibrinolytic activity in the plasma euglobulin fractions on the fibrin plate. Ix Davidson JF, Samama M, Desnoyerse PC, eds. Progress in Chemical Fibrinolysis and Thrombosis. New York: Raven Press, 19765765. 20. Verheijen JH, Mullaart E, Chang GTG, Kluft C, Wijngaards G. A simple sen- sitive spectrophotometric assay for exttinsix (tissue type) plasminogen activator applicable to measurement in plasma. Thromb Huemost 1982;48:266-269. 21. Ericksson E, Ranby M, Grysander E, Risberg B. Determination of plasmino- gen activator inhibitor in plasma using tI?A and chromogenic single point poly-D- lysine stimulated assay. T/womb Res 1988;50:91-101. 22. Goldstein S. The necessity of a uniform definition of sudden coronary death: wimessed death within 1 hour of the onset of acute symptoms. Am Heart J 1982; 102:156-159. 23. Gradman A, Deedwania P, Cody R, Massie B, Packer M, Pitt B, Goldstein S. Predictors of total mortality in sudden death in mild to moderate heart failure. JAm Cdl Cardiol 1989;14:564-570. 24. Rockman HA, Juneau C, Chatterjee K, Rouleau JL. Long-term predictors of sudden and low output death in chronic congestive heart failure secondary to coro- nary artery disease. Am J Cardiol 1989$X1344-1348. 25. Anderson KP. Sudden death, hypertension and hypertrophy. J Cardiovasc Phar- macol 1984;6(suppl IlI):S498-S503. 26. Kannel WB, Wolf PA, Castelli WI’, D’Agostino RB. Fibrinogen and risk of cardiovascular disease. The Framingham Study. JAMA 1987;258:1183-1186. 27. Meade TW, Mellows S, Brozovic M, Miller GJ, Chakrabarti RR, North WRS, Hahaes AP, Stirling Y, Imeson JD, Thompson SG. Haemostatic function and ische- mic heart disease: principal results of the Northwick Park heart study. Lancer 1986; 2:533-537. 28. Meissner MD, Akhtar M, Lehmann MH. Nonischemic sudden tachyarrhyth- mic death in atherosclerotic hcatt disease. Circulation 1991;84:905-912. 29. Malmberg K, Bavenholm P, Hamsten A. Clinical and biochemical factors asso- ciated with prognosis after myocardial infarction at a young age. J Am Coil Car- dial 1994;24:592-599. 30. Jansson JH, Olofsson BO, Nilsson TK. Predictive value of tissue plasminogen activator mass concentration on long-term mortality in patients with coronary artery disease. A ‘I-year follow-up. Circulation 1993;88(part 1):2030-2034.
244 THE AMERICAN JOURNAL OF CARDIOLOGY@ VOL. 76 AUGUST 1, 1995