predictive factors of barrett esophagus
TRANSCRIPT

Predictive Factors of Barrett Esophagus
Multivariate Analysis of 502 Patients With Gastroesophageal Reflux Disease
Guilherme M. R. Campos, MD; Steven R. DeMeester, MD; Jeffrey H. Peters, MD;Stefan Oberg, MD; Peter F. Crookes, MD; Jeffrey A. Hagen, MD; Cedric G. Bremner, MD;Lelan F. Sillin III, MD; Rodney J. Mason, MD; Tom R. DeMeester, MD
Hypothesis: Risk factors for the presence and extent ofBarrett esophagus (BE) can be identified in patients withgastroesophageal reflux disease (GERD).
Design: Case-comparison study.
Setting: University tertiary referral center.
Patients: Five hundred two consecutive patients withGERD documented by 24-hour esophageal pH monitor-ing and with complete demographic, endoscopic, andphysiological evaluation, divided in groups according tothe presence and extent of BE (328 patients without BEand 174 with BE [67 short-segment BE and 107 long-segment BE]).
Main Outcome Measures: Clinical, endoscopic, andphysiological data, studied by multivariate analysis, toidentify the independent predictors of the presence andextent of BE.
Results: Seven factors were identified as predictors ofBE. They were abnormal bile reflux (odds ratio [OR], 4.2;95% confidence interval [CI], 1.9-9.7), hiatal hernia larger
than 4 cm (OR, 4.1; 95% CI, 2.1-8.0), a defective loweresophageal sphincter (OR, 2.7; 95% CI, 1.4-5.4), malesex (OR, 2.6; 95% CI, 1.6-4.3), defective distal esopha-geal contraction (OR, 2.2; 95% CI, 1.4-3.5), abnormalnumber of reflux episodes lasting longer than 5 minutes(OR, 2.2; 95% CI, 1.1-4.6), and GERD symptoms last-ing for more than 5 years (OR, 2.1; 95% CI, 1.4-3.2). Onlyabnormal bile reflux (OR, 4.8; 95% CI, 1.7-13.2) was iden-tified as a predictor of short-segment BE (baseline, no BE).Three factors were identified as predictors of long-segment BE (baseline short-segment BE). They were hia-tal hernia larger than 4 cm (OR, 17.8; 95% CI, 4.1-76.6), a defective lower esophageal sphincter (OR, 16.9;95% CI, 1.6-181.4), and an abnormal longest reflux epi-sode (OR, 8.1; 95% CI, 2.8-24.0).
Conclusions: Among patients with GERD, specific fac-tors are associated with the presence and extent of BE.Elimination of reflux with an antireflux operation inpatients with 1 or more of these factors may prevent thefuture development of BE.
Arch Surg. 2001;136:1267-1273
B ARRETT ESOPHAGUS (BE), theacquired transformation ofnormal esophageal squa-mous epithelium into spe-cialized columnar epithe-
lium with goblet cells, is a complicationof increased reflux of gastric juice into thedistal esophagus.1-3 The factors that leadto the development of BE in some pa-tients with gastroesophageal reflux dis-ease (GERD) and the reasons why short-segment BE (SSBE) develops in some andlong-segment BE (LSBE) in others re-main incompletely understood.4,5 Fur-ther, it is unknown whether SSBE merelyrepresents an earlier stage of LSBE, or ifSSBE and LSBE occur as a consequence ofdifferent processes.
The clinical importance of both SSBEand LSBE lies in the fact that each is as-sociated with an increased risk of malig-nancy compared with patients without BE.6
Consequently, surveillance endoscopy has
been recommended for all patients withBE7,8 and has been demonstrated to re-sult in the detection of esophageal adeno-carcinoma at an earlier, more curablestage.9 The problem has been that mostpatients with reflux-related adenocarci-noma of the esophagus never had a pre-cancer diagnosis of BE, and conse-quently, they were not in a surveillanceprogram.10,11 Ideally, individuals withGERD and at increased risk for develop-ment of BE would be identified prospec-tively. Such patients could then undergodefinitive antireflux surgery with the in-tent of preventing the development ofBE or, alternatively, be followed moreclosely. Therefore, the identification ofpathophysiological factors predictive of thepresence and extent of BE is a clinicallyimportant goal. The aim of this study wasto identify, by means of a multivariateanalysis, factors predictive of the pres-ence and extent of BE.
ORIGINAL ARTICLE
From the Department ofSurgery, Keck Schoolof Medicine, Universityof Southern CaliforniaLos Angeles.
(REPRINTED) ARCH SURG/ VOL 136, NOV 2001 WWW.ARCHSURG.COM1267
©2001 American Medical Association. All rights reserved.

RESULTS
UNIVARIATE ANALYSIS
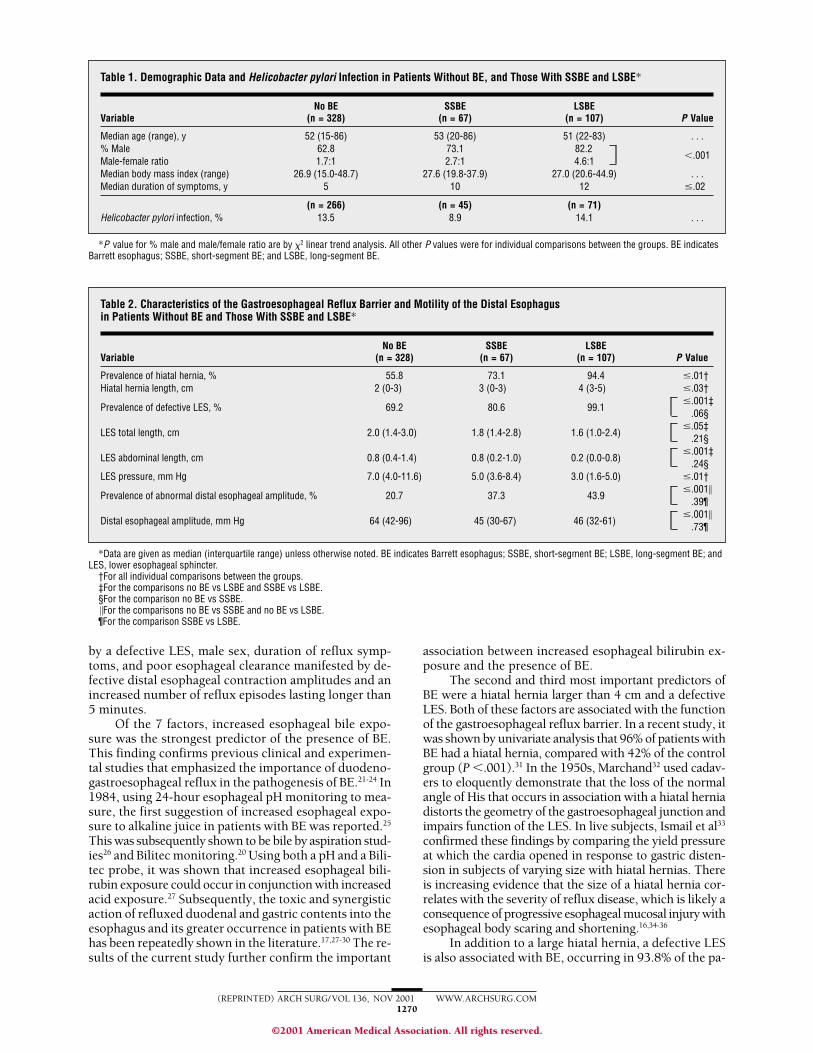
Three hundred twenty-eight patients with GERD but noBE were compared with 174 patients with GERD and BE(67 SSBE and 107 LSBE). Table 1 presents the age, sex,body mass index, and duration of GERD symptoms inpatients without BE and in those with SSBE and LSBE.The proportion of male patients and the duration of GERDsymptoms was lowest in patients without BE and andhighest in patients with LSBE. There was no significantdifference in age, BMI, and H pylori infection status be-tween groups.
As presented in Table 2, the prevalence of hiatalhernia was higher, and the hernias were larger in pa-tients with LSBE than in patients with SSBE; and largerin patients with SSBE compared with those without BE.Likewise, the manometric characteristics of the LES weremost abnormal in patients with LSBE. In patients withSSBE, the LES pressure was significantly lower than itwas in patients without BE. Distal esophageal body mo-tility was similar in patients with SSBE and LSBE, but bothwere significantly worse compared with that of patientswithout BE.
As presented in Table 3, all parameters from the24-hour esophageal pH monitoring became progres-sively more abnormal going from patients without BE to
PATIENTS AND METHODS
STUDY POPULATION
The study population consisted of 502 patients with GERDdocumented by abnormal acid exposure on 24-hour esoph-ageal pH monitoring (composite acid score �14.76) (343men and 159 women; median age, 52 years [age range, 15-86years]). All patients were evaluated in the Department ofSurgery, Keck School of Medicine, University of SouthernCalifornia, Los Angeles, between August 1991 and Febru-ary 1999. In addition to 24-hour pH testing, all patientscompleted a standard questionnaire, underwent upper gas-trointestinal tract endoscopy with extensive protocol-based biopsies, and had lower esophageal sphincter (LES)and esophageal body manometry. The presence of Helico-bacter pylori infection was evaluated in 382 patients by gas-tric biopsy. Two hundred six patients were evaluated forthe reflux of bilirubin into the esophagus using a Bilitecprobe (Medtronic Functional Diagnostics, Shoreview,Minn). Patients with named motility disorders and thosewith a history of previous esophageal or gastric surgery wereexcluded from the study.
DATA COLLECTION AND DEFINITIONS
A standard questionnaire was used to discern the presenceand duration of typical reflux symptoms (heartburn, regur-gitation, and dysphagia) as well as atypical or extraesopha-geal symptoms of reflux, such as chest or epigastric pain, as-piration symptoms, recurrent pneumonia, wheezing, orpersistent cough. Body mass index (BMI) was calculated foreach patient using the following formula:
weight in pounds � 703 / (height in inches)2
Patients were classified as normal (BMI, 19-25), moder-ately obese (BMI, 25.1-35), and morbidly obese (BMI, �35).
Lower esophageal sphincter pressure was measuredby a stationary pull-through technique as the mean pres-sure of 5 recordings at the respiratory inversion point. Theoverall and abdominal lengths of the LES were calculatedfrom the mean of 5 recordings as previously described.12
A structurally defective sphincter was defined by a restingpressure of less than 6 mm Hg, an overall length less than2 cm, or an abdominal length less than 1 cm. Esophagealbody motility was assessed using a 5-hole catheter and awater perfusion technique as previously described.13 We
analyzed a total of 10 wet swallows (5 mL of distilled wa-ter), with a 20-second interval between each. Defectiveesophageal body motility was defined by the presence ofdistal esophageal contraction amplitudes below the fifth per-centile of normal (36 mm Hg).13
Ambulatory 24-hour esophageal pH monitoring wasperformed using a glass electrode (Ingold Incorporated, Ur-dorf, Switzerland) placed 5 cm above the upper border ofthe manometrically defined LES. As previously described,the upper limit of normal for each parameter measured dur-ing the 24-hour pH monitoring period was defined as the95th percentile from a group of healthy volunteers.14,15 Thepattern of esophageal acid exposure was determined basedon the 24-hour pH test as previously described.16 Postpran-dial reflux was defined as abnormal percent time with esoph-ageal pH less than 4 during the 2-hour postprandial pe-riod (�8.4%) in the setting of normal upright and supineacid exposure; upright reflux, abnormal percent time withesophageal pH less than 4 only in the upright position(�8.4%) and regardless of whether the postprandial ex-posure was normal or abnormal; supine reflux, abnormalpercent time with an esophageal pH less than 4 only in thesupine position (�3.4%); and bipositional reflux, abnor-mal percent time with an esophageal pH less than 4 in boththe upright and supine positions.
Esophageal bilirubin monitoring (Bilitec 2000;Medtronic Synectics, Shoreview, Minn) was performed si-multaneously with pH monitoring in a subset of 206 pa-tients. An absorbance threshold of 0.2 was selected, andbilirubin exposure was considered abnormal when greaterthan 1.7% of the total time was above this threshold as pre-viously described.17-20
Upper gastrointestinal endoscopy was performed inall patients. The location of the gastroesophageal junction(GEJ) was defined as the site where the proximal extent ofthe gastric rugal folds met the tubular esophagus. A hiatalhernia was diagnosed when the difference between the po-sition of the crural impression, identified by having the pa-tient sniff, and the gastroesophageal junction was 2 cm ormore. The size of the hiatal hernia was noted. A columnar-lined esophagus (CLE) was suspected when the squamo-columnar junction or any part of its circumference ex-tended above the GEJ. This included an irregularsquamocolumnar junction with tongues of columnar mu-cosa extending into the esophagus. The presence of a CLEwas confirmed by histological evaluation of biopsy speci-mens. When a columnar-lined segment was observed, mul-tiple biopsy specimens were obtained from the area, and
(REPRINTED) ARCH SURG/ VOL 136, NOV 2001 WWW.ARCHSURG.COM1268
©2001 American Medical Association. All rights reserved.

those with SSBE and LSBE. The prevalence of biposi-tional reflux also increased progressively from patientswithout BE to those with SSBE and LSBE. Lastly, whilebile exposure in the distal esophagus was similar in pa-tients with SSBE and LSBE, it was significantly higher inboth groups compared with patients without BE.
MULTIVARIATE ANALYSIS
All variables identified as independently predictive for thepresence of BE by multivariate analysis are listed in rankorder in Table 4. The strongest predictor was the pres-ence of bile in the distal esophagus, as indicated by in-creased esophageal bilirubin exposure. Abnormal bile re-
flux was found to be the only independent predictor forthe presence of SSBE compared with patients without BE(OR, 4.8; 95% confidence interval [CI], 1.7-13.2; P=.002).Three variables were identified as independently predic-tive for the presence of LSBE (Table5). The strongest pre-dictor was the presence of a large hiatal hernia.
COMMENT
Multivariate analysis identified 7 factors predictive of thepresence of BE in patients with GERD. They were in-creased esophageal bile exposure, alteration of thegeometry of the gastroesophageal junction by a hiatalhernia, loss of the gastroesophageal barrier manifested
at each level the distance from the incisors was recorded. Bi-opsy specimens were fixed in 10% buffered formalin, em-bedded in paraffin, sectioned, mounted on slides, and stainedwith hematoxylin-eosin using standard techniques. Intesti-nal metaplasia was defined by the presence of a columnar epi-thelium with a villiform surface, mucous glands, and well-defined goblet cells. The presence of goblet cells was confirmedby positive staining with Alcian blue at pH 2.5. Barrett esopha-gus was identified by the presence of an endoscopically vis-ible segment of columnar lining in the distal esophagus, re-gardless of length, with histological analysis demonstratinggoblet cells indicative of intestinal metaplasia. Short- seg-ment BE vs LSBE was determined in each patient based onthe length of columnar epithelium (�3 cm or �3 cm,respectively). Biopsy specimens from the gastric antrum wereevaluated in a subset of 382 patients for the presence ofH pylori infection using a Giemsa stain.
DEFINITION OF STUDY VARIABLES
Dependent/Outcome Variables
The outcome of interest in this analysis was the presenceand extent of BE. Consequently, 3 comparison groups wereused: patients without BE, patients with SSBE, andpatients with LSBE.
Independent/Potentially Predictive Variables
The numerical independent variables studied at the uni-variate level were as follows: age; BMI; duration of GERDsymptoms; size of hiatal hernia; percent total time withesophageal pH less than 4; number of reflux episodes, num-ber of reflux episodes lasting longer than 5 minutes, andthe duration of the longest reflux episode on 24-hour esoph-ageal pH monitoring; percent time of Bilitec probe absorp-tion greater than 0.2 on 24-hour esophageal bilirubin moni-toring; LES length and pressure; and distal esophagealcontraction amplitudes. The categorical variables studiedat the univariate level were as follows: sex; pattern of esoph-ageal acid exposure; and the presence of a hiatal hernia,defective LES, defective distal esophageal contraction am-plitudes, and abnormal bilirubin exposure.
To simplify clinical interpretation and for optimal useof the logistic regression method, the potentially predic-tive variables were converted to categorical data. The vari-ables regarding hiatal hernia and numerical variables fromthe 24-hour esophageal pH monitoring were divided into
3 categories (normal, abnormal to the calculated 75th per-centile of the study population; abnormal, above the cal-culated 75th percentile of the study population). This per-mitted us to study the association between BE and thepresence and size of a hiatal hernia, as well as individualparameters from the 24-hour pH monitoring test. The vari-ables were (1) age (�50 years and �50 years); (2) sex (maleor female); (3) BMI (normal, 19-25; obese, 25.1-35; or mor-bidly obese, �35); (4) duration of GERD symptoms (�5years and �5 years); (5) hiatal hernia (no hiatal hernia, hia-tal hernia 2-4 cm, hiatal hernia �4 cm); (6) percent totaltime esophageal pH less than 4 (normal: 0 to 4.4%; 4.5 to14.7% and �14.7%); (7) number of reflux episodes (nor-mal: �47, 47-167 and �167); (8) number of reflux epi-sodes �5 min (normal: 0-3, 4-7 and �7); (9) longest re-flux episode (normal: 0-19.8, 19.9-31.7 and �31.7); (10)pattern of esophageal acid exposure (postprandial,upright, supine, or bipositional); (11) bilirubin exposure(normal: 0-1.7% and abnormal �1.7%); (12) H pyloriinfection status (no infection or infection); (13) LEScompetence (competent or defective); and (14) distalesophageal amplitude (normal, �36; or hypocontractive,�36 mm Hg).
STATISTICS
Values are expressed as medians and interquartile rangesunless otherwise stated. A univariate analysis was per-formed to assess the isolated effect of each variable on thepresence and extent of BE. Continuous variables were stud-ied using their numerical values and previously defined cat-egorical variables. The �2 test was used to compare pro-portions between groups, and the Mann-Whitney U test wasused to compare distribution of continuous variables be-tween individual groups. Statistical significance was con-sidered to be � �.05.
Forward stepwise logistic regression was performedto assess the joint effect of all potentially predictive vari-ables and to define those that are independently associ-ated with the presence and extent of BE. To stay in themodel, variables were required to be significant at � �.05.The variables found to be significant were then analyzedin a multivariate model to obtain the predictive effect ofeach adjusted for the presence of the other significant vari-ables (adjusted odds ratio [OR]). The software SPSS 10.0.1(Statistical Product and Service Solutions 10.0.1 StandardVersion for Windows; SPSS Inc, Chicago, Ill) was used forall statistical analyses.
(REPRINTED) ARCH SURG/ VOL 136, NOV 2001 WWW.ARCHSURG.COM1269
©2001 American Medical Association. All rights reserved.
by a defective LES, male sex, duration of reflux symp-toms, and poor esophageal clearance manifested by de-fective distal esophageal contraction amplitudes and anincreased number of reflux episodes lasting longer than5 minutes.
Of the 7 factors, increased esophageal bile expo-sure was the strongest predictor of the presence of BE.This finding confirms previous clinical and experimen-tal studies that emphasized the importance of duodeno-gastroesophageal reflux in the pathogenesis of BE.21-24 In1984, using 24-hour esophageal pH monitoring to mea-sure, the first suggestion of increased esophageal expo-sure to alkaline juice in patients with BE was reported.25
This was subsequently shown to be bile by aspiration stud-ies26 and Bilitec monitoring.20 Using both a pH and a Bili-tec probe, it was shown that increased esophageal bili-rubin exposure could occur in conjunction with increasedacid exposure.27 Subsequently, the toxic and synergisticaction of refluxed duodenal and gastric contents into theesophagus and its greater occurrence in patients with BEhas been repeatedly shown in the literature.17,27-30 The re-sults of the current study further confirm the important
association between increased esophageal bilirubin ex-posure and the presence of BE.
The second and third most important predictors ofBE were a hiatal hernia larger than 4 cm and a defectiveLES. Both of these factors are associated with the functionof the gastroesophageal reflux barrier. In a recent study, itwas shown by univariate analysis that 96% of patients withBE had a hiatal hernia, compared with 42% of the controlgroup (P �.001).31 In the 1950s, Marchand32 used cadav-ers to eloquently demonstrate that the loss of the normalangle of His that occurs in association with a hiatal herniadistorts the geometry of the gastroesophageal junction andimpairs function of the LES. In live subjects, Ismail et al33
confirmed these findings by comparing the yield pressureat which the cardia opened in response to gastric disten-sion in subjects of varying size with hiatal hernias. Thereis increasing evidence that the size of a hiatal hernia cor-relates with the severity of reflux disease, which is likely aconsequence of progressive esophageal mucosal injury withesophageal body scaring and shortening.16,34-36
In addition to a large hiatal hernia, a defective LESis also associated with BE, occurring in 93.8% of the pa-
Table 1. Demographic Data and Helicobacter pylori Infection in Patients Without BE, and Those With SSBE and LSBE*
VariableNo BE
(n = 328)SSBE
(n = 67)LSBE
(n = 107) P Value
Median age (range), y 52 (15-86) 53 (20-86) 51 (22-83) . . .% Male 62.8 73.1 82.2
�.001Male-female ratio 1.7:1 2.7:1 4.6:1Median body mass index (range) 26.9 (15.0-48.7) 27.6 (19.8-37.9) 27.0 (20.6-44.9) . . .Median duration of symptoms, y 5 10 12 �.02
(n = 266) (n = 45) (n = 71)Helicobacter pylori infection, % 13.5 8.9 14.1 . . .
*P value for % male and male/female ratio are by �2 linear trend analysis. All other P values were for individual comparisons between the groups. BE indicatesBarrett esophagus; SSBE, short-segment BE; and LSBE, long-segment BE.
Table 2. Characteristics of the Gastroesophageal Reflux Barrier and Motility of the Distal Esophagusin Patients Without BE and Those With SSBE and LSBE*
VariableNo BE
(n = 328)SSBE
(n = 67)LSBE
(n = 107) P Value
Prevalence of hiatal hernia, % 55.8 73.1 94.4 �.01†Hiatal hernia length, cm 2 (0-3) 3 (0-3) 4 (3-5) �.03†
Prevalence of defective LES, % 69.2 80.6 99.1�.001‡
.06§
LES total length, cm 2.0 (1.4-3.0) 1.8 (1.4-2.8) 1.6 (1.0-2.4)�.05‡
.21§
LES abdominal length, cm 0.8 (0.4-1.4) 0.8 (0.2-1.0) 0.2 (0.0-0.8)�.001‡
.24§LES pressure, mm Hg 7.0 (4.0-11.6) 5.0 (3.6-8.4) 3.0 (1.6-5.0) �.01†
Prevalence of abnormal distal esophageal amplitude, % 20.7 37.3 43.9�.001�
.39¶
Distal esophageal amplitude, mm Hg 64 (42-96) 45 (30-67) 46 (32-61)�.001�
.73¶
*Data are given as median (interquartile range) unless otherwise noted. BE indicates Barrett esophagus; SSBE, short-segment BE; LSBE, long-segment BE; andLES, lower esophageal sphincter.
†For all individual comparisons between the groups.‡For the comparisons no BE vs LSBE and SSBE vs LSBE.§For the comparison no BE vs SSBE.�For the comparisons no BE vs SSBE and no BE vs LSBE.¶For the comparison SSBE vs LSBE.
(REPRINTED) ARCH SURG/ VOL 136, NOV 2001 WWW.ARCHSURG.COM1270
©2001 American Medical Association. All rights reserved.

tients.37 Fein et al37 explored the interplay between theLES and a hiatal hernia and noted that a hiatal herniaplaced the LES at a mechanical disadvantage, particu-larly during episodes of gastric distension. When the LEScomponents are defective in the presence of a hiatal her-nia, as seen in BE, the effects are additive, and gross in-competency exists. This makes control of reflux diffi-cult with medical therapy. Katzka and Castell38 as wellas Sampliner39 have shown that in this situation, high-dose proton pump inhibitor therapy is often unsuccess-ful at normalizing esophageal acid exposure.
Similar to others, we found a higher prevalence ofmale patients with BE (78%) compared with patientswithout BE (63%) (P�.001).31,40,41 By multivariateanalysis, male sex was determined to be an independentpredictor of BE. We noted, as others have, that themale-female ratio approaches 1:1 as the length of BE
decreases.42,43 In LSBE, where the male-female ratio is4.6:1, we found that women had the same pathophysi-ologic derangements as men (data not shown), indicat-ing that fewer women, for reasons unknown, havesevere reflux diseases.
The multivariate analysis also identified both de-creased distal esophageal contraction amplitudes and anincreased number of reflux episodes lasting longer than 5minutes as independent predictors for the presence ofBE. These factors are indicators of impaired esophagealclearance, and they reinforce the importance of pro-longed esophageal mucosal contact to refluxed gastricjuice in the development of BE. This suggests that the reflux-induced injury extends beyond the mucosa into the mus-cularis propria of the esophagus and leads to inflamma-tory damage and scarring of esophageal muscle. Progressiveloss of esophageal muscle function can induce a spiral ofprogressive loss of esophageal clearance, more mucosal in-jury, and ultimately end-stage esophageal disease.
The duration of GERD symptoms increased signifi-cantly across the 3 study groups. In the multivariate analy-
Table 3. Esophageal Acid and Bilirubin Exposure in Patients Without BE and Those With SSBE and LSBE*
VariableNo BE
(n = 328)SSBE
(n = 67)LSBE
(n = 107) P Value
% Total time pH�4 7.6 (5.6-11.3) 9.3 (6.8-14.7) 16.5 (11.2-34.1) �.001†No. of reflux episodes 77 (51-119) 95 (57-178) 184 (105-268) �.04†No. of reflux episodes �5 min 4 (2-6) 5 (2-7) 7 (4-15) �.02†
Longest reflux episode, min 17.8 (10.2-29.0) 18.0 (13.3-26.0) 28.0 (19.2-50.0)�.001‡
.52§PEAE, %
Postprandial 17.4 6.0 0.9Upright 23.2 13.4 8.4
�.001†Supine 32.0 38.8 26.2Bipositional 27.4 41.8 64.5
(n = 132) (n = 32) (n = 42)
Prevalence of abnormal bilirubin exposure, % 53.0 84.4 88.1�.001�
.64‡
Bilirubin absorption �0.2, % time over 24-h period 3.0 (0.1-10.7) 13.3 (2.8-26.5) 17.3 (6.9-34.3)�.002�
.19‡
*Data are given as median (interquartile range) unless otherwise noted. BE indicates Barrett esophagus; SSBE, short-segment BE; LSBE, long-segment BE; andPEAE, pattern of esophageal acid exposure.
†For all individual comparisons between the groups.‡For the comparison SSBE vs LSBE.§For the comparison no BE vs SSBE.�For the comparisons no BE vs SSBE and no BE vs LSBE.
Table 4. Multivariate Analysis: Factors Predictivefor the Presence of Any Length of Barrett Esophagus*
VariableOdds Ratio(95% CI)
PValue
Abnormal bilirubin exposure 4.2 (1.9-9.7) .001Hiatal hernia
�4 cm 4.1 (2.1-8.0) �.0012-4 cm 2.4 (1.4-4.6) .002
Defective LES 2.7 (1.4-5.4) .004Male sex 2.6 (1.6-4.3) �.001Defective distal contraction amplitude 2.2 (1.4-3.5) .001No. of reflux episodes �5 min
�7 min 2.2 (1.1-4.6) .034-7 min 2.1 (1.2-3.7) .006
Duration of GERD symptoms �5 y 2.1 (1.4-3.2) .001
*CI indicates confidence interval; LES, lower esophageal sphincter; andGERD, gastroesophageal reflux disease.
Table 5. Multivariate Analysis: Factors Predictivefor the Presence of Long-Segment Barrett Esophagus*
VariableOdds Ratio(95% CI)
PValue
Hiatal hernia�4 cm 17.8 (4.1-76.6) �.0012-4 cm 8.5 (2.3-31.7) .002
Defective LES 16.9 (1.6-181.4) .02Longest reflux episode
�31.7 min 8.1 (2.8-24.0) �.00119.9-31.7 min 6.8 (2.3-20.1) .001
*Baseline values are for short-segment Barrett esophagus. CI indicatesconfidence interval; LES, lower esophageal sphincter.
(REPRINTED) ARCH SURG/ VOL 136, NOV 2001 WWW.ARCHSURG.COM1271
©2001 American Medical Association. All rights reserved.

sis, GERD symptoms present for more than 5 years wasassociated with BE. The length of time necessary to de-velop BE may provide an opportunity for early surgicalintervention to stop reflux and potentially prevent thedevelopment of BE. This needs to be the focus of futurestudies since the ultimate solution for the rising inci-dence of esophageal adenocarcinoma may be to preventthe development of BE with early surgical therapy in thosepatients with appropriate risk factors.
It is interesting to note that the percentage of timethat the esophagus was exposed to a pH less than 4 on24-hour monitoring was not a significant independentpredictor of the presence of BE. However, an inclusioncriteria for this study was the presence of an abnormalscore on 24-hour pH monitoring, and by univariate analy-sis, the percentage of time that the esophageal pH wasless than 4 was significantly higher in those with BE. Wehave previously shown that the length of columnar mu-cosa without intestinal metaplasia increases progres-sively with increasing percentage of time that the esoph-ageal pH is less than 4 on 24-hour pH monitoring.44 Thisgave rise to the theory that columnarization of the distalesophagus is caused by increased esophageal exposureto acid (pH � 4), and that this columnar mucosa is theprecursor to BE.8,45Thus, while acid exposure is associ-ated with the formation of columnar mucosa, we foundthat bile exposure had the strongest association with thepresence of intestinal metaplasia. Consequently, in-creased esophageal acid exposure may be a necessary, butnot a sufficient factor for the development of BE, since itdoes not differentiate between those who do and do notdevelop intestinal metaplasia.
The role of H pylori infection in the pathogenesisof GERD and its complications is still controversial. Thereis evidence suggesting that H pylori may protect againstthe development of erosive esophagitis,46,47 BE, and esoph-ageal adenocarcinoma.48,49 Furthermore, it has been sug-gested that eradication of H pylori may precipitate re-flux esophagitis in patients with duodenal ulcers.50,51 Inour study population, the prevalence of patients with gas-tric H pylori infection was similar in the study groups andwas not related to either the presence or extent of BE.
A second aim of our study was to evaluate the patho-physiologic factors related to the length of BE. Our studyshowed that BE was associated with an increased esoph-ageal exposure to bilirubin. Interestingly, we also foundthat the prevalence and degree of increased esophagealbilirubin exposure was not significantly different be-tween patients with SSBE or LSBE. This suggests that ab-normal bile reflux is the key determinant associated withintestinal metaplasia, and that other factors determine thelength of BE.
By multivariate analysis, 3 independent factors werepredictive of the presence of LSBE, whereas the sole pre-dictor for the presence of SSBE was only increased bileexposure. The strongest predictor for LSBE was the pres-ence of a large (� 4 cm) hiatal hernia, followed by a de-fective LES and long reflux episodes. Taken together, thesefactors all indicate that patients with LSBE have more pro-found derangements in their gastroesophageal reflux bar-rier and consequently more severe reflux disease. Whileincreased bilirubin exposure is the major factor associ-
ated with intestinal metaplasia of any length, it is pro-gressive deterioration of the antireflux barrier and themechanisms of esophageal clearance that seem to be themajor factors associated with LSBE.
Importantly, our data show that patients with SSBEhave similar pathophysiologic abnormalities as those withLSBE, but to a lesser extent. Thus, SSBE likely repre-sents an earlier stage of disease within the GERD spec-trum. Our data refute the theory that BE develops rap-idly to its full length without subsequent alteration. Thisconcept is largely based on the longitudinal observationof 21 patients with BE longer than 3 cm published by Cam-eron and Lomboy.52 Note, however, that all these pa-tients by definition already had LSBE. Our data wouldsuggest that they in all likelihood had large hiatal her-nias, a defective LES, and impaired esophageal clear-ance. Consequently, it is little wonder that they failed tochange significantly during the observation period.44,53
We conclude that the independent predictors for thepresence of BE are increased esophageal bile exposure,alteration of the geometry of the gastroesophageal junc-tion by a hiatal hernia, a defective LES, male sex, dura-tion of reflux symptoms, and poor esophageal clear-ance. Of these, increased esophageal exposure to bile isthe most important independent predictive factor and wasthe only independent predictive factor for the presenceof SSBE. Identification of these factors in patients with-out BE and prompt intervention with antireflux surgerymay prevent the development of BE. This should be-come the aim of future prospective surgical studies.
Presented at the 108th Scientific Session of the Western Sur-gical Association, Dana Point, Calif, Novemer 14, 2000.
Silvia Tan, MS, from the Department of Biometry,University of Southern California, was our validating stat-istician.
Corresponding author and reprints: Steven R.DeMeester, MD, Department of Surgery, Keck School ofMedicine, University of Southern California, 1441 East-lake Ave, Suite 7418, Los Angeles, CA 90033-0804 (e-mail: [email protected]).
REFERENCES
1. Bremner CG, Bremner RM. Barrett’s esophagus. Surg Clin North Am. 1997;77:1115-1137.
2. Nandurkar S, Talley NJ. Barrett’s esophagus: the long and the short of it. Am JGastroenterol. 1999;94:30-40.
3. Winters C Jr, Spurling TJ, Chobanian SJ, et al. Barrett’s esophagus: a prevalent,occult complication of gastroesophageal reflux disease. Gastroenterology. 1987;92:118-124.
4. Fennerty MB. Barrett’s esophagus: what do we really know about this disease?Am J Gastroenterol. 1997;92:1-3.
5. Falk GW. Reflux disease and Barrett’s esophagus. Endoscopy. 1999;31:9-16.6. Rudolph RE, Vaughan TL, Storer BE, et al. Effect of segment length on risk for
neoplastic progression in patients with Barrett esophagus. Ann Intern Med. 2000;132:612-620.
7. Levine DS, Blount PL, Rudolph RE, Reid BJ. Safety of a systematic endoscopicbiopsy protocol in patients with Barrett’s esophagus. Am J Gastroenterol. 2000;95:1152-1157.
8. DeMeester SR, DeMeester TR. Columnar mucosa and intestinal metaplasia ofthe esophagus: fifty years of controversy. Ann Surg. 2000;231:303-321.
9. Peters JH, Clark GW, Ireland AP, Chandrasoma P, Smyrk TC, DeMeester TR. Out-come of adenocarcinoma arising in Barrett’s esophagus in endoscopically sur-veyed and nonsurveyed patients. J Thorac Cardiovasc Surg. 1994;108:813-821.
(REPRINTED) ARCH SURG/ VOL 136, NOV 2001 WWW.ARCHSURG.COM1272
©2001 American Medical Association. All rights reserved.

10. Nigro JJ, DeMeester SR, Hagen JA, et al. Node status in transmural esophagealadenocarcinoma and outcome after en bloc esophagectomy. J Thorac Cardio-vasc Surg. 1999;117:960-968.
11. Provenzale D, Schmitt C, Wong JB. Barrett’s esophagus: a new look at surveil-lance based on emerging estimates of cancer risk. Am J Gastroenterol. 1999;94:2043-2053.
12. Zaninotto G, DeMeester TR, Schwizer W, Johansson KE, Cheng SC. The loweresophageal sphincter in health and disease. Am J Surg. 1988;155:104-111.
13. Costantini M, DeMeester TR. Preoperative assessment of esophageal func-tion. In: Bremner CG, DeMeester TR, Peracchia A, eds. Modern Approach toBenign Esophageal Disease. St Louis, Mo: Quality Medical Publishing Inc;1995:17-56.
14. Jamieson JR, Stein HJ, DeMeester TR, et al. Ambulatory 24-h esophageal pHmonitoring: normal values, optimal thresholds, specificity, sensitivity, and re-producibility. Am J Gastroenterol. 1992;87:1102-1111.
15. Mason RJ, Oberg S, Bremner CG, et al. Postprandial gastroesophageal reflux innormal volunteers and symptomatic patients. J Gastrointest Surg. 1998;2:342-349.
16. Campos GM, Peters JH, DeMeester TR, Oberg S, Crookes PF, Mason RJ. Thepattern of esophageal acid exposure in gastroesophageal reflux disease influ-ences the severity of the disease. Arch Surg. 1999;134:882-887.
17. Vaezi MF, Singh S, Richter JE. Role of acid and duodenogastric reflux in esoph-ageal mucosal injury: a review of animal and human studies. Gastroenterology.1995;108:1897-1907.
18. Bechi P, Pucciani F, Baldini F, et al. Long-term ambulatory enterogastric refluxmonitoring: validation of a new fiberoptic technique. Dig Dis Sci. 1993;38:1297-1306.
19. Vaezi MF, Lacamera RG, Richter JE. Validation studies of Bilitec 2000: an am-bulatory duodenogastric reflux monitoring system. Am J Physiol. 1994;267:1050-1057.
20. Kauer WK, Burdiles P, Ireland AP, et al. Does duodenal juice reflux into the esopha-gus of patients with complicated GERD? evaluation of a fiberoptic sensor for bil-irubin. Am J Surg. 1995;169:98-103.
21. Bateson MC, Hopwood D, Milne G, Bouchier IA. Oesophageal epithelial ultra-structure after incubation with gastrointestinal fluids and their components.J Pathol. 1981;133:33-51.
22. Harmon JW, Johnson LF, Maydonovitch CL. Effects of acid and bile salts on therabbit esophageal mucosa. Dig Dis Sci. 1981;26:65-72.
23. Hopwood D, Bateson MC, Milne G, Bouchier IA. Effects of bile acids and hydro-gen ion on the fine structure of oesophageal epithelium. Gut. 1981;22:306-311.
24. Lillemoe KD, Johnson LF, Harmon JW. Role of the components of the gastro-duodenal contents in experimental acid esophagitis. Surgery. 1982;92:276-284.
25. DeMeester TR, Attwood SE, Smyrk TC, Therkildsen DH, Hinder RA. Surgical therapyin Barrett’s esophagus. Ann Surg. 1990;212:528-540.
26. Stein HJ, Feussner H, Kauer W, DeMeester TR, Siewert JR. Alkaline gastro-esophageal reflux: assessment by ambulatory esophageal aspiration and pH moni-toring. Am J Surg. 1994;167:163-168.
27. Kauer WK, Peters JH, DeMeester TR, Ireland AP, Bremner CG, Hagen JA. Mixedreflux of gastric and duodenal juices is more harmful to the esophagus than gas-tric juice alone: the need for surgical therapy re-emphasized. Ann Surg. 1995;222:525-531.
28. Kauer WK, Peters JH, DeMeester TR, Feussner H, Ireland AP, Stein HJ, SiewertRJ. Composition and concentration of bile acid reflux into the esophagus of pa-tients with gastroesophageal reflux disease. Surgery. 1997;122:874-881.
29. Nehra D, Howell P, Pye JK, Beynon J. Assessment of combined bile acid and pHprofiles using an automated sampling device in gastro-oesophageal reflux dis-ease. Br J Surg. 1998;85:134-137.
30. Nehra D, Howell P, Williams CP, Pye JK, Beynon J. Toxic bile acids in gastro-oesophageal reflux disease: influence of gastric acidity. Gut. 1999;44:598-602.
31. Cameron AJ. Barrett’s esophagus: prevalence and size of hiatal hernia. Am J Gas-troenterol. 1999;94:2054-2059.
32. Marchand P. A study of the forces productive of gastroesphageal regurgitationand herniation through the diaphragmatic hiatus. Thorax. 1957;12:189-202.
33. Ismail T, Bancewicz J, Barlow J. Yield pressure, anatomy of the cardia and gastro-esophageal reflux. Br J Surg. 1995;82:943-947.
34. Sloan S, Rademaker AW, Kahrilas PJ. Determinants of gastroesophageal junc-tion incompetence: hiatal hernia, lower esophageal sphincter, or both? Ann In-tern Med. 1992;117:977-982.
35. Stene LG, Weberg R, Friyshov LI, Bjirtuft O, Hoel B, Berstad A. Relationship ofoverweight to hiatus hernia and reflux oesophagitis. Scand J Gastroenterol. 1988;23:427-432.
36. Patti MG, Goldberg HI, Arcerito M, Bortolasi L, Tong J, Way LW. Hiatal herniasize affects lower esophageal sphincter function, esophageal acid exposure, andthe degree of mucosal injury. Am J Surg. 1996;171:182-186.
37. Oberg S, Ritter MP, Crookes PF, et al. Gastroesophageal reflux disease and mu-cosal injury with emphasis on short-segment Barrett’s esophagus and duodeno-gastroesophageal reflux. J Gastrointest Surg. 1998;2:547-553.
38. Katzka DA, Castell DO. Successful elimination of reflux symptoms does not in-sure adequate control of acid reflux in patients with Barrett’ s esophagus. Am JGastroenterol 1994;89:989-991.
39. Sampliner RE. Effect of up to 3 years of high-dose lansoprazole on Barrett’ s esopha-gus. Am J Gastroenterol. 1994;89:1844-1848.
40. Hirota WK, Loughney TM, Lazas DJ, Maydonovitch CL, Rholl V, Wong RK. Spe-cialized intestinal metaplasia, dysplasia, and cancer of the esophagus and esopha-gogastric junction: prevalence and clinical data. Gastroenterology. 1999;116:277-285.
41. Ouatu LR, Fitzgerald RC, Triadafilopoulos G. Differentiation and proliferation inBarrett’s esophagus and the effects of acid suppression. Gastroenterology. 1999;117:327-335.
42. Weston AP, Krmpotich P, Makdisi WF, et al. Short segment Barrett’s esophagus:clinical and histological features, associated endoscopic findings, and associationwith gastric intestinal metaplasia. Am J Gastroenterol. 1996;91:981-986.
43. Weston AP, Krmpotich PT, Cherian R, Dixon A, Topalosvki M. Prospective long-term endoscopic and histological follow-up of short segment Barrett’s esopha-gus: comparison with traditional long segment Barrett’s esophagus. Am J Gas-troenterol. 1997;92:407-413.
44. Oberg S, DeMeester TR, Peters JH, et al. The extent of Barrett’s esophagus de-pends on the status of the lower esophageal sphincter and the degree of esoph-ageal acid exposure. J Thorac Cardiovasc Surg. 1999;117:572-580.
45. Oberg S, Peters JH, DeMeester TR, et al. Determinants of intestinal metaplasiawithin the columnar-lined esophagus. Arch Surg. 2000;135:651-656.
46. Werdmuller BF, Loffeld RJ. Helicobacter pylori infection has no role in the patho-genesis of reflux esophagitis. Dig Dis Sci. 1997;42:103-105.
47. Oberg S, Peters JH, Nigro JJ, et al. Helicobacter pylori is not associated with themanifestations of gastroesophageal reflux disease. Arch Surg. 1999;134:722-726.
48. Varanasi RV, Fantry GT, Wilson KT. Protective role of Helicobacter pylori infec-tion in gastroesophageal reflux disease [abstract]. Gastroenterology. 1998;114:322.
49. Chow WH, Blaser MJ, Blot WJ, et al. An inverse relation between cagA+ strainsof Helicobacter pylori infection and risk of esophageal and gastric cardia adeno-carcinoma. Cancer Res. 1998;58:588-590.
50. Vicari JJ, Peek RM, Falk GW, et al. The seroprevalence of cagA-positive Helico-bacter pylori strains in the spectrum of gastroesophageal reflux disease. Gas-troenterology. 1998;115:50-57.
51. Labenz J, Blum AL, Bayerdorffer E, Meining A, Stolte M, Borsch G. Curing Heli-cobacter pylori infection in patients with duodenal ulcer may provoke reflux esopha-gitis. Gastroenterology. 1997;112:1442-1447.
52. Cameron AJ, Lomboy CT. Barrett’s esophagus: age, prevalence, and extent ofcolumnar epithelium. Gastroenterology. 1992;103:1241-1245.
53. Salminen JT, Tuominen JA, Ramo OJ, Farkkila MA, Salo JA. Oesophageal acidexposure: higher in Barrett’s oesophagus than in reflux oesophagitis. Ann Med.1999;31:46-50.
(REPRINTED) ARCH SURG/ VOL 136, NOV 2001 WWW.ARCHSURG.COM1273
©2001 American Medical Association. All rights reserved.