prediction basedoncology for breast cancer - clara · prediction‐basedoncology for breast cancer...
TRANSCRIPT

Prediction‐based Oncology for Breast Cancer
Daniel BirnbaumCentre de Recherche en Cancérologie de Marseille
Lyon Clara/LyricApril 2015

1950 20001980
AmplifiedERBB2
CellularSRC
Philadelphiachromosome
t(9;22)
1970
HerceptinMutatedRAS
BCR‐ABL Glivec
Targeted therapy>Precision oncology
KIT/imatinib/GISTBRAF/vemurafenib/MelanomaEML4‐ALK/crizotinib/NSCLCEGFR/gefitinib/NSCLCBRCA/olaparib/breast


Personnalized medicine: principles
Existence of markers and targets
Each patient is different
Each tumor is different (inter‐tumor heterogeneity)
Each malignant cell is different ? (intra‐tumor heterogeneity)
How to predict outcome?
How to give the most appropriate treatment to each patient ?
“Prediction is very difficult, especially if it's about the future”
Niels Bohr
« Un choix est le seul (petit) moyen de prédire le futur »
Personnalized medicine: principles
Existence of markers and targets
Each patient is different
Each tumor is different (inter‐tumor heterogeneity)
Each malignant cell is different ? (intra‐tumor heterogeneity)
How to predict outcome?
How to give the most appropriate treatment to each patient ?
The treatment must be chosen on a rationale basis and the response must be predicted

PatientTreatmentselection
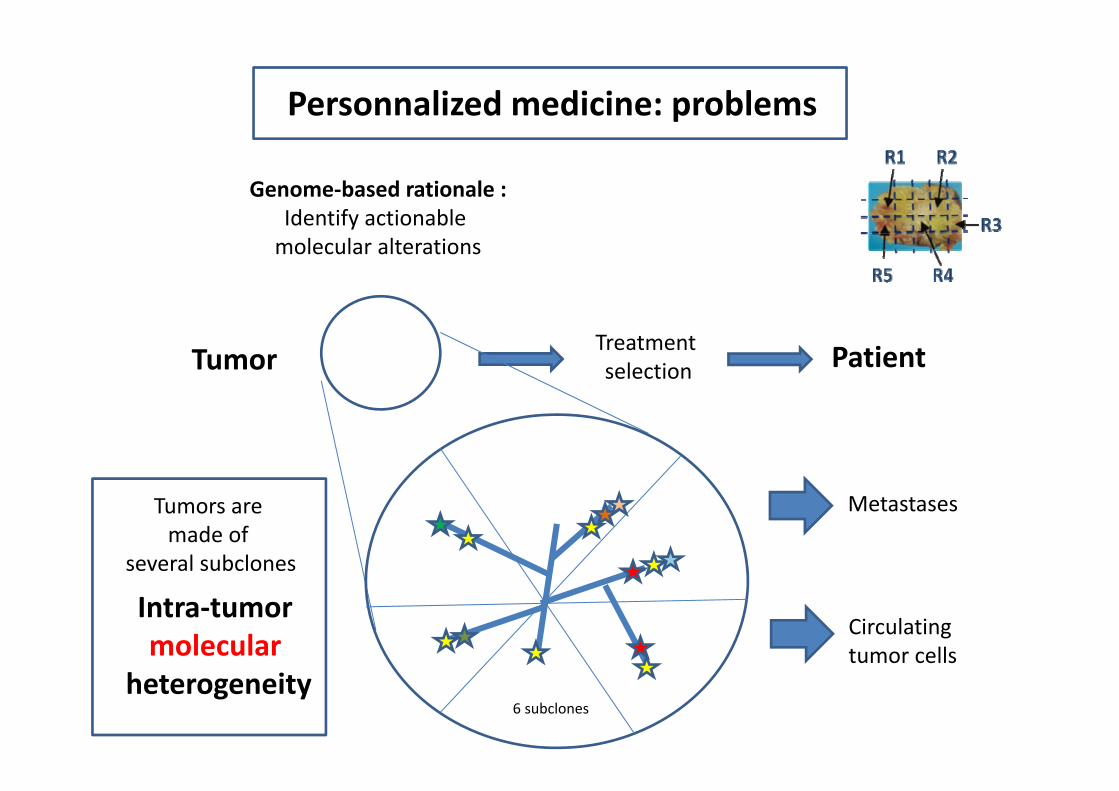
Genome‐based rationale :Identify actionable
molecular alterations (= targets and/or markers)
Tumor
Model‐based prediction:Measure the effect
of drugs on malignant cellsin vitro and/or in vivo
Personnalized medicine: principles
PatientTreatmentselection
Genome‐based rationale :Identify actionablemolecular alterations
Tumor
Personnalized medicine: problems
Intra‐tumormolecular
heterogeneity
Tumors are made of
several subclones
Metastases
Circulatingtumor cells
6 subclones

Subclonal structure within 10 metastatic prostate cancers
Gundem et al., Nature 2015

PatientTreatmentselectionTumor
Model‐based prediction:Measure the effect
of drugs on malignant cellsin vitro and/or in vivo
Personnalized medicine: problems
Intra‐tumorcellular
heterogeneity
Tumors are made of
several types of cells
Metastases
Circulatingtumor cells
Cellular hierachy
Cancer stem cells

Personnalized medicine: basis and problem
Tumor: the mess inside

How to give the most appropriate treatment to each patient ?
The treatment must be selected on a rationale basis and/or the response predicted
= the right drug against the right molecular and cellular target(s)

PatientTreatmentselection
Genome‐based prediction:Identify actionable
molecular alterations by using:
Tumor
Next generation sequencing
Personnalized medicine: tools

High-throughputanalyses
Gene expression profilingAffymetrix, RNA-seq
Mutated genesSelected panel, exome, genome
Genome ProfilingArray-CGH, SNP-array
Personnalized medicine: genome‐based
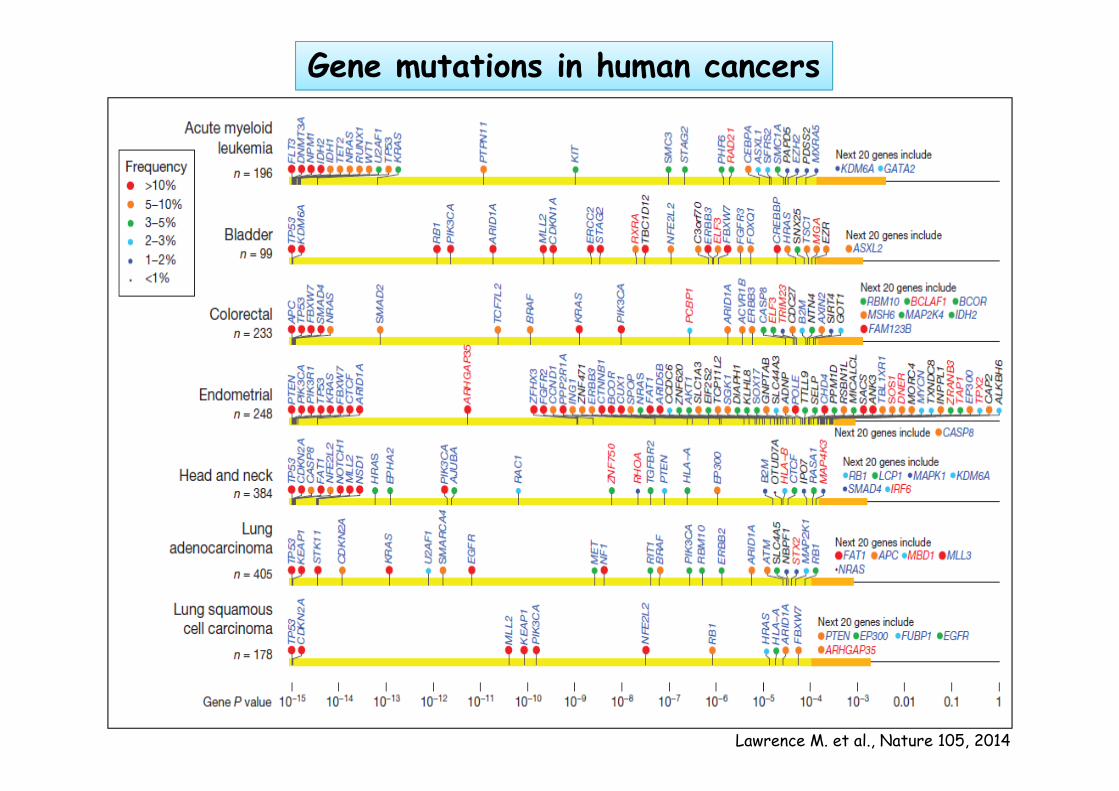
Lawrence M. et al., Nature 105, 2014
Gene mutations in human cancers

Driver mutations were identified in several new cancer genes including AKT2, ARID1B,
CASP8, CDKN1B, MAP3K1, MAP3K13, NCOR1, SMARCD1 , TBX3…
Gene mutations in breast cancer

Case‐specific mutations shaded according toclonal frequencies in known driver genes, plus genes from integrin signalling and ECM‐related proteins
Network analysis of 254 recurrently mutated genes by somatic point mutations and indels.

Genomic profile using array-CGHPANDORA1

423 patients enroled
299 patients suitable for genomic analysis
195 patients with targetable
genomic alterations
55 patients received targeted
therapies
4 patients with objective
responses
100%
70%
46%
13%
1%André et al. Lancet Oncol 2014
Is this approach efficient? The SAFIR01 example

Use the term “variant” with the following modifiers:
‐ pathogenic, ‐ likely pathogenic,‐ uncertain significance, ‐ likely benign, or ‐ benign
A major issue: what is a target ?
The Variant of Unknown Significance (VUS) problem! (ACMG Standards and Guidelines, Genetics and Medicine 2015)
Future : Functional validations

dbNSFP (via annovar) fourni les scores pré‐calculés pour les outils suivants :‐ SIFT (séquence, PSSM)‐ Polyphen2 (séquence + structure, bayes classifier)‐ LRT (séquence, log‐ratio test)‐MutationTaster (séquence + annotation, bayes model)‐MutationAssessor (séquence)‐ FATHMM (séquence, HMM) ‐ RadialSVM‐ LR
Our in silico pipeline for variant calling and significance
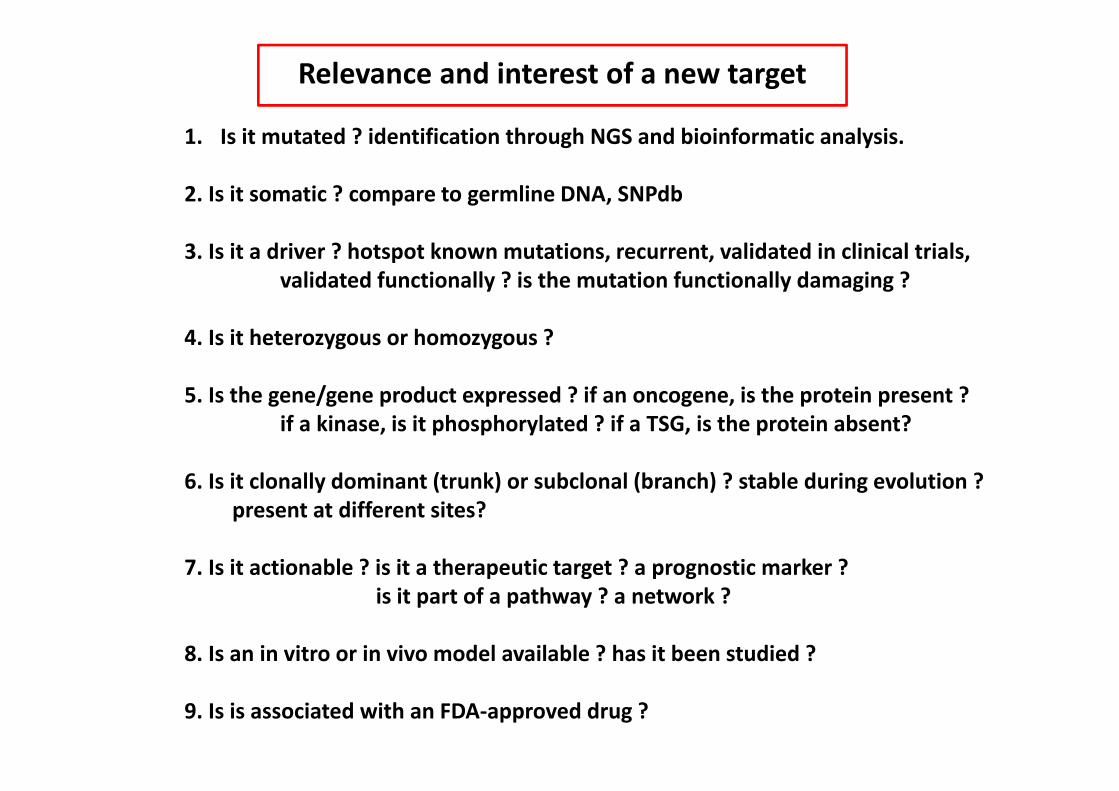
Relevance and interest of a new target
1. Is it mutated ? identification through NGS and bioinformatic analysis.
2. Is it somatic ? compare to germline DNA, SNPdb
3. Is it a driver ? hotspot known mutations, recurrent, validated in clinical trials, validated functionally ? is the mutation functionally damaging ?
4. Is it heterozygous or homozygous ?
5. Is the gene/gene product expressed ? if an oncogene, is the protein present ? if a kinase, is it phosphorylated ? if a TSG, is the protein absent?
6. Is it clonally dominant (trunk) or subclonal (branch) ? stable during evolution ? present at different sites?
7. Is it actionable ? is it a therapeutic target ? a prognostic marker ? is it part of a pathway ? a network ?
8. Is an in vitro or in vivo model available ? has it been studied ?
9. Is is associated with an FDA‐approved drug ?



PANDORA4 – 102627UT
PANDORA4 – 102627PER
PANDORA4 – 102627CAR
ERBB2 Amplication No 17q12 3 1.84 (1.84;1.84) 1.84 (7.18)MutationNo Mutation
ERBB2 Gain or Amplication No 17q12 3 0.95 (0.95;0.95) 0.95 (3.87)Symbol Mutation COSMIC RS Note FreqERBB2 p.L755S COSM14060 HotSpot0.07
ERBB2 Gain or Amplication No 17q12 3 0.51 (0.51;0.51) 0.51 (2.85)MutationNo Mutation
L755S, showed a lapatinib‐resistant phenotype, but it did not cause oncogenic transformation.L755S required doses of 1μm lapatinib or more to inhibit HER2 signaling, but it was sensitive to the irreversible tyrosine kinase inhibitors, neratinib (Fig. 3D) and canertinib (CI‐1033, Supplementary Fig. S3).
PER‐102627/PAND4

Actionable targets in our first series of cases
patient number (n;%) 28 (82%)target number 59median (range) 2(1‐5)Nature:mutation 30amplification 22deletion 7
mutation 30PIK3CA 8ESR1 4KIT 3AKT1 2BRCA2 2HER2 2PIK3C2B 1RET 1NTRK2 1TSC2 1JAK1 1RPS6K1 1KRAS 1PTCH1 1HER4 1
amplification 22CCND1 7CCNE1 2FGFR1 2IGF1R 2FGFR3 1FGFR2 1AKT1 1AKT2 1JAK2 1CDK4 1CDK6 1EGFR 1MDM2 1
deletion 7PTEN 3CDKN2A 2BRCA2 1STK11 1

Table 4. genomic‐driven therapeutic proposals
Clinical trial
number of candidate patients 18 (52%)trial available per patient (median, range) 1.5 (1‐4)
number of patients enrolled 4
therapeutic response:objective response 0progressive disease 2not available 2
Off‐trial therapeutic proposalnumber of candidate patients 17 (50%)registered drug available 30number of patients treated 6therapeutic response:
objective response 1stable disease > 6 months 1progressive disease 4*
* heterogenous response was observed (some lesions decreased and others increased)

Identification of targets : what is the best strategy ?
What to use ?
Genome : NGS (mutations: selected panel of genes, exome, whole genome?methylations, miRNA….)
Proteome : IHC, MS…
Activome (phosphorylations…) , metabolome…
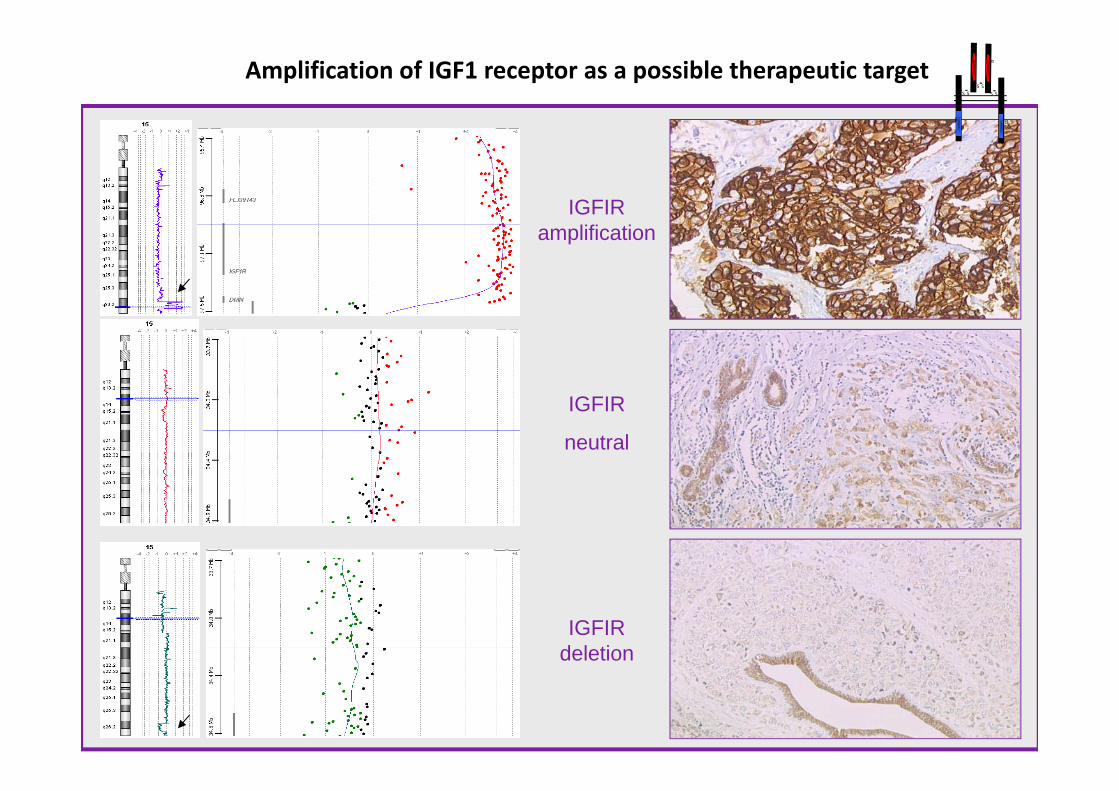
IGFIR amplification
IGFIR
neutral
IGFIR deletion
Amplification of IGF1 receptor as a possible therapeutic targetS S
S SS S
α α
β β
If sequencing, what to sequence ?
‐ Tumor cells ?‐ Primary , Metastatic ? ‐ Cancer stem cells ?‐ Normal cells ?‐ Circulating cells ?‐ Circulating DNA ?‐ Single cells ?
How important is depthHow important is coverageHow important is bioinformaticsHow important is validation
in each case?

What workflow ?
‐ Biobank‐Who should prepare the DNA ?‐Who should prescribe the NGS test ?‐Who should sign the results ? ‐What results to tell the patient ?
(all, germline with value?, only somatic, none? = patient choice)
‐What SOP ? ‐ RCP
What line of treatment ?
‐ Primary tumor ? ‐Metastatic? ‐ How many lines? ‐What combinations? ‐ Routine or trial ?‐ How much knowledge needed about host background?

Personnalized medicine: tools
PatientTreatmentselectionTumor
Model‐based prediction:Measure the effect
of drugs on malignant cellsin vitro by using: chemograms/drug response profiling
and/or in vivo by using: avatars

Time from birth (weeks)
3 5 7 12
-oestradiol
+ MatrigelTumoral growth monitoring
Primary Tumor
Dissociation
Humanization
Human fibroblasts
«Clearing»
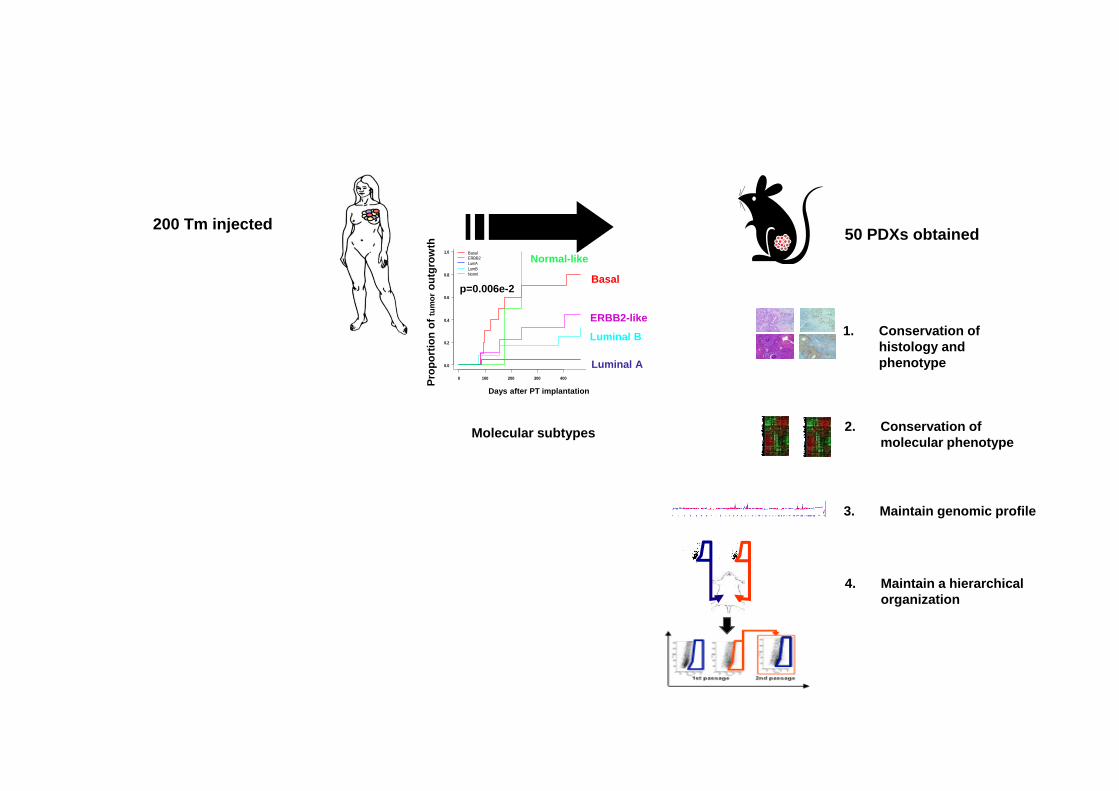
Personnalized medicine: avatars

200 Tm injected 50 PDXs obtained
Molecular subtypes
Days after PT implantation
Prop
ortio
n of
tum
orou
tgro
wth
0 100 200 300 400
0.0
0.2
0.4
0.6
0.8
1.0 BasalERBB2LumALumBNorml Basal
ERBB2-like
p=0.006e-2
Luminal B
Luminal A
Normal-like
1. Conservation of histology and phenotype

CRCM 224 PT
CRCM 224X
HES
HES
ER
ER PR
PR ERBB2
ERBB2

200 Tm injected 50 PDXs obtained
Molecular subtypes
Days after PT implantation
Prop
ortio
n of
tum
orou
tgro
wth
0 100 200 300 400
0.0
0.2
0.4
0.6
0.8
1.0 BasalERBB2LumALumBNorml Basal
ERBB2-like
p=0.006e-2
Luminal B
Luminal A
Normal-like
1. Conservation of histology and phenotype
2. Conservation of molecular phenotype
Charafe-Jauffret et al, Cancer Research 2013
200 Tm injected 50 PDXs obtained
Molecular subtypes
Days after PT implantation
Prop
ortio
n of
tum
orou
tgro
wth
0 100 200 300 400
0.0
0.2
0.4
0.6
0.8
1.0 BasalERBB2LumALumBNorml Basal
ERBB2-like
p=0.006e-2
Luminal B
Luminal A
Normal-like
1. Conservation of histology and phenotype
2. Conservation of molecular phenotype
3. Maintain genomic profile
4. Maintain a hierarchical organization

n° IPC n°biobank Grafting MDX Susceptibility HR status Subtype Targeted NGS Main mutations aCGH
0900753 none 1FP 06/11/13 yes nd TN bas? PGM none complex (IGF1R, 20q..)1315233 24308 no no nd HER2+/HR+ ERBB2 PGM PIK3CA ERBB2, CCND1, MDM2…1105841 24324 2FP 25/11/13 yes no HER2+/HR‐ ERBB2 PGM/MiSeq PIK3CA ERBB2, CCNE10102627 24339 1FP 02/12/13 nd HER2+/HR+ ERBB2 PGM PIK3CA, PTEN ERBB2, CCND1, 20q…0102627 24340 1FP 02/12/13 nd HER2+/HR+ ERBB2 PGM PIK3CA, PTEN, ERBB2 "0102627 24341 1FP 02/12/13 nd HER2+/HR+ ERBB2 PGM PIK3CA, PTEN "0405907 24378 no no no HER2‐/HR+ lum? PGM PIK3CA, ESR1 CCND11313133 24418 1FP 08/01/14 yes nd TN bas? PGM P53 CCNE1…
1312288 24445 1 FP 14/01/14 yes no TN lum? MiSeq P53 IGF1R, CCND1…1304501 24487 1 FP 21/01/14 no nd HER+/HR+ ERBB2 PGM none ERBB2
0805665 24608 1FP 18/02/14 nd HER2‐/HR+ >TN bas? MiSeq PIK3CA, P53 complex, 20q…0802153 24631 1FP 25/02/14 no no HER2‐/HR+ lum? MiSeq none complex1402128 24632 1FP 25/02/14 nd HER2+/HR+ MiSeq none IGF1R, 20q…1203496 24646 1 FP 26/02/14 no TN bas? MiSeq P53 complex1402241 24661 1FP 28/02/14 yes nd HER2‐/HR+ lum ? MiSeq none complex0904684 24666 2FP 04/03/14 nd HER2‐/HR+ lumA? MiSeq ERBB2, ESR1 1q16q…1308955 24581 no no nd HER2‐/HR+ MiSeq none complex1004419 24729 1 FP 18/03/14 nd HER2‐/HR+ lumB? MiSeq ESR1 CCND1, 20q…1315720 24823 2 FP 15/04/14 BRCA2 HER2‐/HR+ lumB? MiSeq BRCA2 complex1405053 24838 2FP 18/04/14 yes no TN bas? MiSeq P53 complex1204731 24841 1FP 23/04/14 nd HER2+/HR+ ERBB2 MiSeq none simplex0906291 24846 1FP 23/04/14 no HER2‐/HR+ MiSeq none complex1300665 24871 1 FP 30/04/14 yes no TN bas? MiSeq complex0502630 24978 1 FP 03/06/14 no HER2‐/HR+ MiSeq PI3KCA hom MAP2K41305071 24737 no no BRCA2 TN MiSeq BRCA2, KRAS, AKT1 complex1309394 24848 no no no TN lum? MiSeq none simplex1307201 none 4 FP 12/06/14 yes nd TN MiSeq AKT1 complex0003309 25100 1 FP 27/06/12 no HER2‐/HR+ MiSeq complex1403077 2509 no no nd lum B MiSeq FLT4 IRS2, IGF1R
Exemples from a pilot study

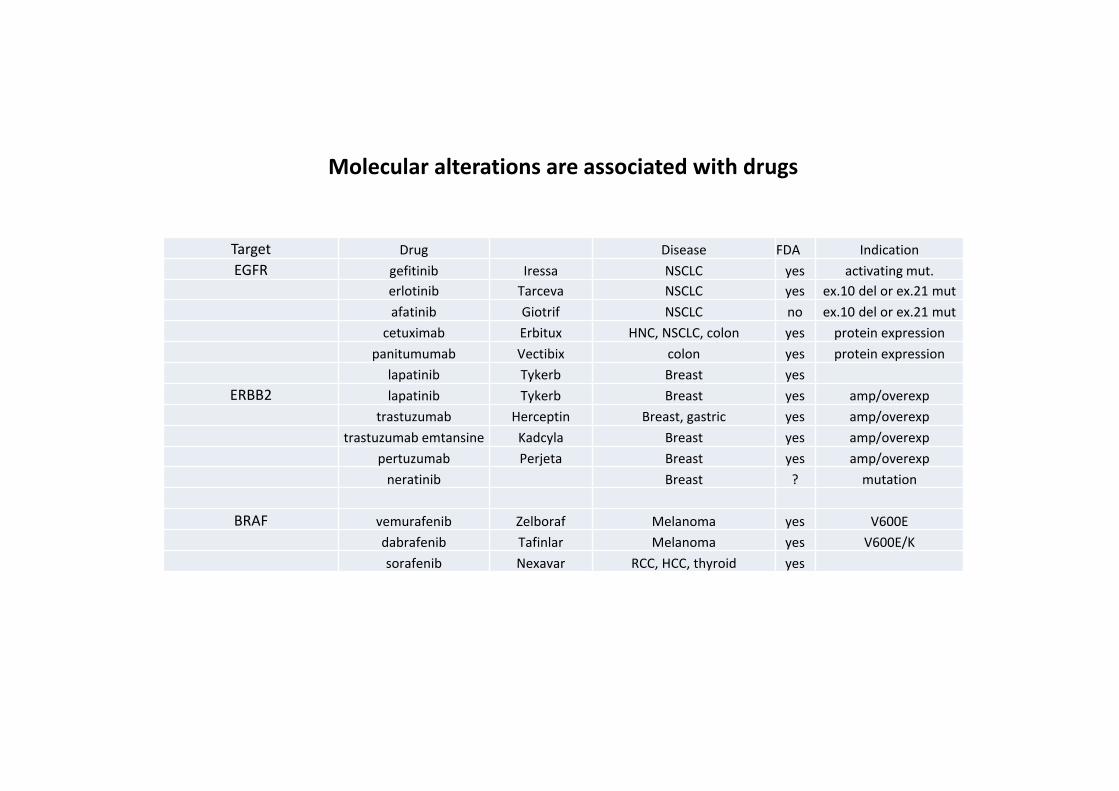
Molecular alterations are associated with drugs
Target Drug Disease FDA IndicationEGFR gefitinib Iressa NSCLC yes activating mut.
erlotinib Tarceva NSCLC yes ex.10 del or ex.21 mutafatinib Giotrif NSCLC no ex.10 del or ex.21 mut
cetuximab Erbitux HNC, NSCLC, colon yes protein expressionpanitumumab Vectibix colon yes protein expression
lapatinib Tykerb Breast yesERBB2 lapatinib Tykerb Breast yes amp/overexp
trastuzumab Herceptin Breast, gastric yes amp/overexptrastuzumab emtansine Kadcyla Breast yes amp/overexp
pertuzumab Perjeta Breast yes amp/overexpneratinib Breast ? mutation
BRAF vemurafenib Zelboraf Melanoma yes V600Edabrafenib Tafinlar Melanoma yes V600E/Ksorafenib Nexavar RCC, HCC, thyroid yes

Test of drugs directly on short‐term cultures of malignant cells
Personnalized medicine: model‐based ?
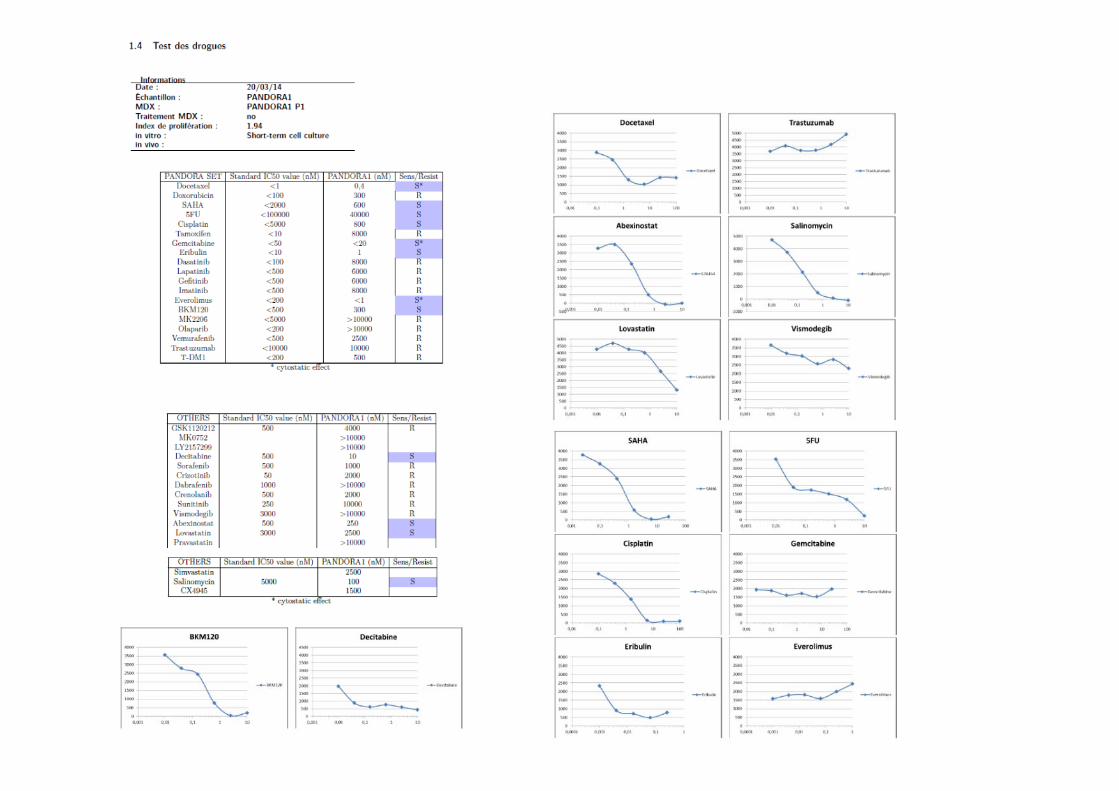

Bulk drug screening CSC drug screening
Short Term Culture (STC) assay Mininiaturized Aldefluor assay

Relevance and interest of a drug
1. Availability: FDA‐approved, clinical trials…
2. Existence of a (frequent, specific) target
3. Existence of a companion test
4. Few/no off‐target effects
5. Known/measurable effects: cytotoxic, cytostatic, effects on CSC….
6. Combos (synthetic lethality, synergy, additivity, antagonists…)
7. Costs
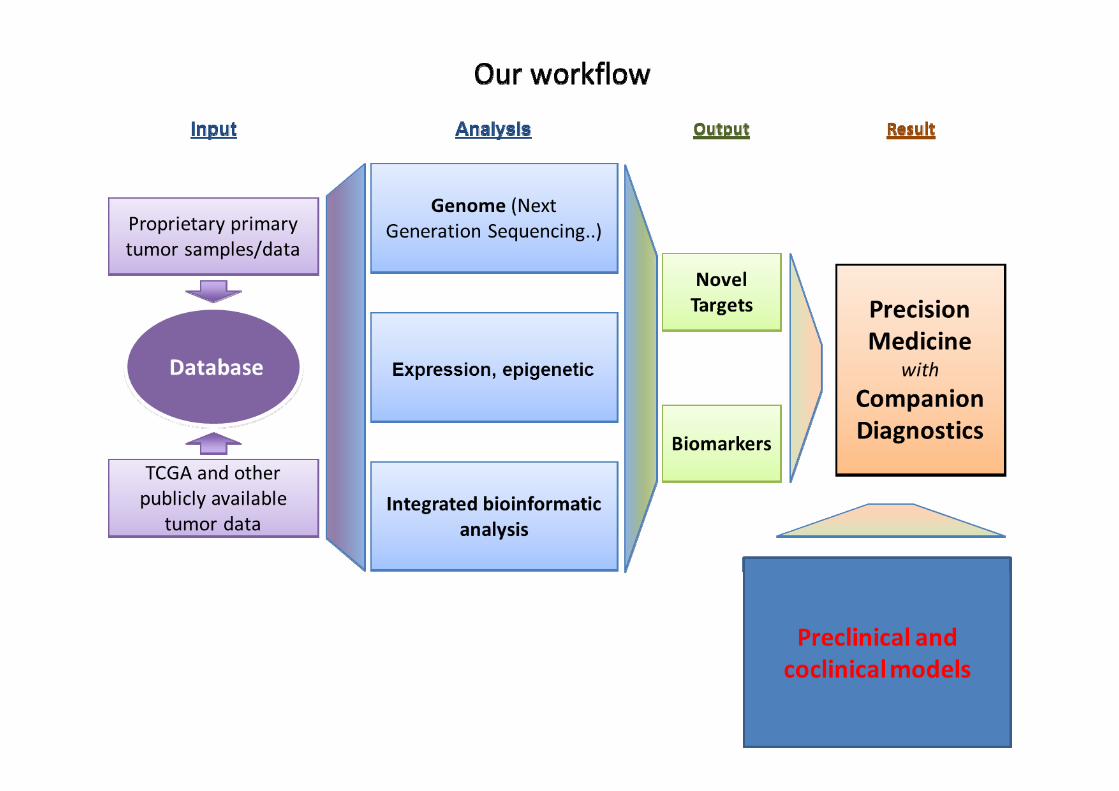

Our program: establish correlations, solve challenges
* Challenge: shunt avatar, cells from tumor/meta, CTC or ctDNA
Patient’s response
Genomics Avatar Drug responseprofiling (ex vivo cells)
Stem cells
Correlation 1 Correlation 2
Correlation 3 Correlation 4
Correlation 5
* ***
** Best method: NGS selected panel, exome, genome ? Activome? GES?

Correlation 4

Personnalized medicine: Why it may fail
1 ‐ No target
2 – Targets but not validated (driver?)
3 – Target but no drug
4 – Target and drug but too late
5 ‐ Too much heterogeneity, minor clones undetected and resistant
6 – Unknown: good prediction but no response

Subclonal structure within 10 metastatic prostate cancers
Gundem et al., Nature 2015
Personalized medicine: many challenges
1. Ethical issues: Patients are interested in this new development of care and are willing to be enrolled
2. Technical issues: Methods and tools are available, but must be improvedand/or adapted
3. Medical issues: Actionable targets are identified with variable frequency, depending on the type of cancer
Challenges: what to test (CSC, CTC, ctDNA…), what method, costs,intra tumor heterogeneity (lack of target?), VUS (germline, driver: validations), lack of FDA drugs, drug combinations (toxicity, off‐target effects)target prioritization (trunk? branches?), treatment combinations (targeted t. + immunotherapy)implementation in clinical setting: organization, time frame

Summary for current practice
Establish a genomic diagnosis as comprehensive as possible
Establish a predictor as precise/comprehensive as possible
Detect and follow minor clones with aggressive mutations (e.g. P53)
Target cancer stem cells with available drugs
For current research
New targets: validation+++
New drugs, combinations, combinations with immunotherapy
Better definition of cancer stem cells
Fight metastases adaptation
FUTURE
Shortly
‐ Every patient at diagnostic‐ Selection of drug cocktails ‐ Follow‐up every 6 months
Soon
‐ Everybody: connected body‐ « Sensor nanochip » in blood, checking for CTCs and CDNA > smartphone‐ Smartphone > Preloaded « Delivery nanochip » killing CTCs

Personnalized medicine: people

The genomics team in the NGS room

The bioinformaticians: Arnaud Guille and Pascal Finetti
P. Finetti

François Bertucci
Marc Lopez
Olivier Cabaud
Anthony Gonçalvès
Oncologists
Master of avatars
Chemogramwizard

CSC team