predicting the risk of traumatic lumbar punctures in children … · days since previous lp, and a...
TRANSCRIPT
Predicting the Risk of Traumatic Lumbar Punctures in Children with Acute Lymphoblastic Leukemia:
A Retrospective Cohort Study using Repeated-Measures Analyses
by
Furqan Shaikh
A thesis submitted in conformity with the requirements for the degree of Masters of Science, Clinical Epidemiology and Health Care Research
Institute of Health Policy, Management & Evaluation University of Toronto
© Copyright by Furqan Shaikh (2012)

ii
Predicting the Risk of Traumatic Lumbar Punctures in Children with Acute Lymphoblastic Leukemia:
A Retrospective Cohort Study using Repeated-Measures Analyses
Furqan Shaikh
Master of Science
Institute of Health Policy, Management and Evaluation University of Toronto
2012
ABSTRACT
Traumatic lumbar punctures (TLPs) in children with acute lymphoblastic leukemia are
associated with a poorer prognosis. The objective of this study was to determine risk factors
for TLPs using a retrospective cohort. We compared and contrasted three different regression
methods for the analysis of repeated-measures data. In the multivariable model using
generalized estimating equations, variables significantly associated with TLPs were age < l
year or ≥ 10 years; body mass index percentile ≥ 95; platelet counts < 100 x 103/µL; fewer
days since previous LP, and a preceding TLP. The same variables, with similar estimates and
confidence-intervals, were identified by the random-effects model. In a fixed-effects model
where each patient was used as their own control, days since prior LP and the effect of using
image-guidance were significant. Random-effects and GEE lead to similar conclusions,
whereas fixed-effects discards between-subject comparisons and leads to different estimates
and interpretation of results.
iii
ACKNOWLEDGMENTS
This work would not have been possible without the support of my thesis supervisor, Dr. Lillian
Sung, who has been the greatest mentor that anyone could have asked for. She has been instantly
available and constantly helpful. She has been a role model of the scientific process through her own
superb work ethic and intellectual rigor. It has been an indescribable privilege to have been a graduate
student under her tutelage.
I am extremely grateful to my thesis committee members. It was through casual conversations
with Dr. Sarah Alexander at a medical conference that this project was born, and she has inspired and
helped me every step of the way. She has kept me on track and held me to high standards, in both my
research and clinical work. Dr. Teresa To and Dr. Andrea Doria have provided continual insights,
perspective, and encouragement. Their invaluable contributions have been crucial to the development and
completion of this thesis.
Thank you to the Pediatric Oncology Group of Ontario (POGO). Their financial and moral
support provide young investigators like myself with the wonderful opportunity to pursue dedicated
training in health research methods, allowing us to become useful citizens in the community of childhood
cancer researchers. None of this could have happened without that opportunity.
I’d like to thank my appraisers, Dr. Kuckarczyk and Dr. Ringash, and my defense chair Dr.
Laupacis for the generosity with their time and ideas. Lastly, I’d like to thank the many wonderful staff at
the Institute for Health Policy, Management and Evaluation for organizing and delivering such an
enlightening and valuable degree program.
Finally, a special thank you to parents and to my wife Safia for their limitless patience,
understanding and love. Safia has no doubt at times wondered whether MSc stands for Monster Spouse.
We look forward to the post-thesis era and to a well-deserved vacation!

iv
TABLE OF CONTENTS
ABSTRACT ...................................................................................................................................................... ii
ACKNOWLEDGMENTS .................................................................................................................................. iii
TABLE OF CONTENTS .................................................................................................................................... iv
LIST OF TABLES ............................................................................................................................................ vii
LIST OF FIGURES ......................................................................................................................................... viii
LIST OF APPENDICES .................................................................................................................................... ix
LIST OF ABBREVIATIONS ............................................................................................................................... x
CHAPTER 1: INTRODUCTION ......................................................................................................................... 1
1.1 Traumatic Lumbar Punctures in Children with Acute Lymphoblastic Leukemia ................................ 1
1.1.1 The Concept of CNS-Directed Therapy ........................................................................................ 1
1.1.2 Risk Factors for CNS Relapse ........................................................................................................ 2
1.1.3 The Lumbar Puncture in Pediatric Oncology ............................................................................... 2
1.1.4 Traumatic Lumbar Punctures ....................................................................................................... 3
1.1.5 Consequences of Traumatic Lumbar Punctures .......................................................................... 4
1.1.6 Risk Factors for Traumatic Lumbar Punctures ............................................................................. 8
1.1.7 Limitations of the Previous Literature ......................................................................................... 9
1.2 The Statistical Analysis of Repeated Measures Data ....................................................................... 10
1.2.1 Clustered and Longitudinal Data ................................................................................................ 10
1.2.2 Advantages and Types of Longitudinal Studies.......................................................................... 11
1.2.3 Alternatives to Longitudinal Data Analyses ............................................................................... 12
1.2.4 Notation ..................................................................................................................................... 13
1.2.5 Random Effects Methods .......................................................................................................... 15
1.2.6 Fixed Effects Methods ................................................................................................................ 16
1.2.7 Hybrid Random-Fixed Effects Method ....................................................................................... 17
1.2.8 Marginal Models (Generalized Estimating Equations) ............................................................... 18
1.2.9 Strengths and Limitations of Each Method ............................................................................... 19
1.3 Study Objectives ............................................................................................................................... 23
1.3.1 Primary objective: ...................................................................................................................... 23
1.3.2 Secondary objectives: ................................................................................................................ 23

v
1.4 Study rationale ................................................................................................................................. 24
CHAPTER 2: METHODS ................................................................................................................................ 25
2.1 Study Design ...................................................................................................................................... 25
2.2 Study Population ............................................................................................................................... 25
2.2.1 Inclusion Criteria ........................................................................................................................ 25
2.2.2 Exclusion Criteria ........................................................................................................................ 25
2.2.3 Study Timeline............................................................................................................................ 25
2.3 Variables ............................................................................................................................................ 27
2.3.1 Primary Outcome Variable ......................................................................................................... 27
2.3.2 Secondary Outcome Variable .................................................................................................... 27
2.3.3 Predictor Variables ..................................................................................................................... 27
2.4 Data Sources and Measurement ...................................................................................................... 29
2.5 Sample Size ....................................................................................................................................... 30
2.6 Statistical Analyses ............................................................................................................................ 31
2.6.1 Descriptive Statistics .................................................................................................................. 31
2.6.2 Model Building ........................................................................................................................... 31
2.6.3 Conventional Logistic Regression ............................................................................................... 32
2.6.4 Generalized Estimating Equations ............................................................................................. 32
2.6.5 Random-Effects (Generalized Linear Mixed Models) ................................................................ 33
2.6.6 Fixed-Effects (Conditional Logistic Regression) ......................................................................... 33
2.6.7 A Hybrid Method ........................................................................................................................ 33
2.6.8 Kaplan-Meier Survival Curves .................................................................................................... 34
CHAPTER 3: RESULTS ................................................................................................................................... 35
3.1 Descriptive Statistics ......................................................................................................................... 35
3.1.1 Participants and Procedures ...................................................................................................... 35
3.1.2 Characteristics ............................................................................................................................ 35
3.1.3 Primary Outcome: Traumatic Lumbar Punctures ...................................................................... 36
3.2 Inferential Statistics .......................................................................................................................... 40
3.2.1 Collinearity and Correlations ..................................................................................................... 40
3.2.2 Model Building .......................................................................................................................... 41
3.2.3 Secondary Outcome: Event-Free Survival .................................................................................. 49
CHAPTER 4: DISCUSSION ............................................................................................................................. 50
vi
4.1 Summary of Main Findings ............................................................................................................... 50
4.2 Factors Predictors of TLP .................................................................................................................. 50
4.3 Pertinent Negative Findings .............................................................................................................. 52
4.4 Survival Analysis ................................................................................................................................ 53
4.5 Comparison of Repeated-Measures Analysis Methods .................................................................... 53
4.6 Study Limitations .............................................................................................................................. 56
4.7 Study Strengths ................................................................................................................................. 57
4.8 Future Research ................................................................................................................................ 58
REFERENCES ................................................................................................................................................ 59
APPENDICES ................................................................................................................................................ 63

vii
LIST OF TABLES
Table 1. Incidence of CNS status and effect on event-free survival
Table 2. Comparison of repeated-measures analysis methods
Table 3. List of predictor variables and rationale
Table 4. Patient characteristics
Table 5. Pearson correlation coefficients
Table 6. Conventional logistic regression
Table 7. Generalized estimating equations
Table 8. Random effects with generalized linear mixed models
Table 9. Fixed effects with conditional logistic regression
Table 10. The hybrid method
Table 11. Comparison of multivariable models

viii
LIST OF FIGURES
Figure 1. Timeline of study inclusion and follow-up
Figure 2. Flow of patients and lumbar punctures through the study
Figure 3. CNS status and proportion of patient with traumatic lumbar punctures at first LP
Figure 4. Kaplan-Meier survival curves by CNS status

ix
LIST OF APPENDICES
Appendix 1. Approach to Classifying TLP+ Status Varies Between SJCRH and COG Systems
Appendix 2. ALL risk stratification
x
LIST OF ABBREVIATIONS
CI Confidence interval ALL Acute lymphoblastic leukemia AML Acute myeloid leukemia BLP Bloody lumbar puncture CDC Center for Disease Control CNS Central nervous system COG Children’s Oncology Group CSF Cerebrospinal fluid EFS Event-free survival ER Emergency room FE Fixed effects FLP Failed lumbar puncture GEE Generalized estimating equations HR Hazard ratio IGT Image-guided therapy IQR Interquartile range KM Kaplan-Meier LMWH Low molecular weight heparin N/A Not available OR Odds ratio OS Overall survival RBC Red blood cell RE Random effects Ref Reference SD Standard deviation SE Standard error SJCRH St. Jude Children’s Research Hospital TLP Traumatic lumbar puncture TLP+ Traumatic lumbar puncture with blast cells TLP- Traumatic lumbar puncture without blast cells WBC White blood cell χ2 Chi-square µL microliter

1
CHAPTER 1: INTRODUCTION
1.1 Traumatic Lumbar Punctures in Children with Acute Lymphoblastic
Leukemia
1.1.1 The Concept of CNS-Directed Therapy
Acute lymphoblastic leukemia (ALL) is a cancer of the white blood cells. It is the most
common childhood malignancy, accounting for approximately 25% of all pediatric cancers. At
an incidence of 4 per 100,000 child-years, there are an estimated 250 new cases of childhood
ALL every year in Canada.1
Prior to the 1970s, approximately 50-80% of children with ALL who achieved remission
subsequently experienced a relapse of leukemia within the central nervous system (CNS).2 This
led to the recognition of the CNS as a sanctuary site for leukemia cells. A major advance in the
treatment of childhood leukemia was the addition of pre-symptomatic CNS-directed therapy for
all patients with ALL.3 CNS-directed therapy could include intrathecal chemotherapy injected
directly into the cerebrospinal fluid (CSF) via a lumbar puncture (LP)4,5 or rarely via an Ommaya
reservoir;6 systemic oral or intravenous chemotherapy that crosses the blood-brain barrier;7
and/or cranial radiation.8 The development of such approaches has dramatically improved the
prognosis of children with ALL, reducing CNS relapses to less than 6% of patients.9 However,
more intensive CNS-directed therapy, in particular the use of cranial radiation, is associated with

2
more long-term sequelae of therapy in survivors, including neuro-cognitive defects,
endocrinopathies, and secondary malignancies.10-12
1.1.2 Risk Factors for CNS Relapse
Several factors for predicting an increased risk of CNS relapse have been identified. The
most important factor is the presence of leukemia blast cells in the CSF at diagnosis. In some
regimens, the risk was greater if the presence of blast cells was accompanied by a white blood
cell (WBC) count over 5 cells/µL.13 Therefore, a trichotomous risk-classification for “CNS
status” was proposed and remains in current use.14 CNS1 denotes the absence of any leukemia
blast cells in the CSF; CNS2 denotes the presence of blast cells in a sample that contains less
than 5 WBCs/µL; and CNS3 denotes the presence of blast cells in a sample that contains ≥5
WBCs/µL. The latter category, considered to be overt CNS leukemia, is present in 2-5% of
children with newly diagnosed ALL.2
Risk-stratification allows the treatment intensity to be tailored to the individual. For
example, many regimens recommend the addition of cranial radiation for patients with CNS3
status.7,15 Therefore, accurate diagnosis of CNS status is essential. Misclassification of CNS
status could lead to a child receiving under-treatment and a consequent increased risk of relapse,
or receiving over-treatment and a greater risk of long-term sequalae.
1.1.3 The Lumbar Puncture in Pediatric Oncology
The determination of CNS status is achieved by means of the first (“diagnostic”) lumbar
puncture (LP), prior to initiation of chemotherapy. CSF is collected and microscopically
examined for blast cells.16 The correctly-performed LP is therefore a vital procedure for CNS
3
staging. At the time of the first LP and with each of multiple subsequent LPs, chemotherapy is
delivered directly into the intrathecal space.4,17 On contemporary treatment protocols, children
receive between 14 and 30 LPs over the entire course of ALL treatment, the exact number being
determined by the sum of risk factors and the type of additional CNS-directed therapies.14
Therefore, the LP is the most commonly performed procedure for all pediatric oncologists. As
the focus of research shifts to trying to avoid cranial radiation for as many children as
possible,15,18-20 the importance of intrathecal chemotherapy further increases.
1.1.4 Traumatic Lumbar Punctures
Cerebrospinal fluid is normally a clear and colorless liquid containing no red blood cells
(RBCs). A traumatic lumbar puncture (TLP) occurs when RBCs from neighboring blood vessels
leak into the CSF. In most cases, the RBCs are thought to have entered the CSF as a result of
needle laceration of the vessels during the performance of the LP.
The definition of a TLP varies across the medical literature. In the general pediatrics and
emergency medicine literature, a TLP is generally defined as the presence of ≥ 400 RBCs/µL of
CSF on microscope examination.21 This is approximately the cell count at which clear CSF
begins to develop a red or pink color, but does not yet appear grossly bloody. In the pediatric
oncology literature, however, a TLP is defined at a much stricter threshold of 10 RBCs/µL, for
reasons that will be examined below. At this level, no redness is visible except on microscopy,
and the CSF appears clear.

4
1.1.5 Consequences of Traumatic Lumbar Punctures
There are several negative consequences of a TLP. First, the presence of RBCs in the
CSF can obscure the diagnostic information that was sought from the procedure.22 If the first
diagnostic LP for a patient with ALL is a TLP with blasts (TLP+), it is unclear whether the blasts
were present in the CNS to begin with, or whether they were introduced from the bloodstream by
the needle laceration. Different pediatric oncology groups approach this uncertainty in different
ways, which further adds to the complexity of interpreting a TLP+. At the St Jude Children’s
Research Hospital (SJCRH), a TLP+ is considered to be its own CNS group without further sub-
classification.22 Theoretically, in such a system, children with actual CNS1 status or actual CNS3
status could both be classified as a TLP+, thus potentially leading to either over- or under-
treatment. In contrast, other treatment groups such as the Children’s Oncology Group (COG)
utilize a ratio-based mathematical calculation that attempts to determine whether the white blood
cells and blasts are likely to have been present in the CNS or to have been introduced from the
bloodstream (see Appendix I).14 However, to our knowledge, the recommended formula has not
been derived from published empirical research and has never been evaluated for its diagnostic
properties or ability to correctly predict outcome. Therefore, it is unknown whether the formula
is able to consistently and accurately classify CNS status that occurs after a TLP+.
Second, and most important, multiple studies have shown that the presence of a TLP+ is
a risk factor for leukemia relapse.22-24 These studies observed a 7% to 17% decrease in event-free
survival (EFS) in children who had a TLP+ compared to those who had CNS1 status. A TLP+ in
each of these studies was defined as ≥ 10 RBCs/µL in the presence of leukemia blasts,
suggesting that even microscopic trauma during the first LP carried the associated risk. The
results of these studies are summarized in Table 1.

5
It is worth noting that among all the risk factors for relapse in childhood ALL, a TLP+ is
the only one that may have an iatrogenic component. Apart from treatment itself, it is the only
risk factor that has the potential to be modifiable. All other known risk factors are properties of
the patient characteristics or the disease biology (see Appendix II). They are thus generally fixed
upon the patient’s presentation to the health care system. The iatrogenic nature of this risk factor
increases the burden upon the operating physician to ensure that all reasonable measures to avoid
a TLP are undertaken.
Third, according to current treatment protocols, children with TLP+ receive additional
therapy compared to TLP- or CNS1 patients.14,20 At a minimum, a child with TLP+ will receive
two additional doses of intrathecal chemotherapy compared to one who is CNS1. Patients with
TLP+ may also receive increased intensity of systemic chemotherapy.
Fourth, although it is the first LP that influences outcomes directly, the subsequent LPs
that a child receives are still important for the proper instillation of intrathecal chemotherapy and
for screening CSF for signs of relapse. A study of radionuclide imaging of the CNS observed
that in 11% of intrathecal injections, a radioisotope was inadvertently placed outside the
subarachnoid space.25 Furthermore, TLPs often occur as a sign of difficult LPs or multiple
attempts. The latter are associated with more pain and discomfort after the procedure.26-28
Lastly, when a child with ALL is observed to have repeatedly difficult, bloody, or
unsuccessful LPs, the usual course of action at many institutions is to refer him or her to
interventional radiology, where LPs are performed under fluoroscopic guidance. While
fluoroscopy does allow for the acquisition of otherwise difficult LPs,29,30 this recourse has some
obvious disadvantages. Fluoroscopy is not available at many centers. When available, its use
leads to scheduling delays, increased cost, more time under anesthesia, and decreased availability

6
of the equipment for other procedures. Moreover, it leads to radiation exposure which can have
long term consequences with cumulative exposure.31,32 A lateral abdominal fluoroscope provides
an estimated dose of 0.26 to 1.1 mSV of radiation per minute, varying by age and magnification
level. By comparison, a standard 2-view chest X-ray provides 0.08 mSV of radiation.33

7
TABLE 1. Incidence of CNS status and Effect on Event-Free Survival
Study
(Year)
CNS1 CNS2 CNS3 TLP- TLP+ Log-
rank P
Value*
HR
(95% CI)
Gajjar
et al.22
(2000)
Number (%)
(N=546)
336 (62) 80 (15) 16 (3) 54 (10) 60 (11)
5y-EFS (±SE) 77 (±2) 55 (±6) 38 (±11) 76 (±6) 60 (±6) 0.026 N/A
Burger
et al.23
(2003)
Number (%)
(N=2021)
1605 (79) 103 (5) 58 (3) 111 (6) 135 (7)
5y-EFS (±SE) 80 (±1) 80 (±4) 50 (±8) 83 (±4) 73 (±4) 0.003 1.5
(1.02-2.2)
te Loo
et al.24
(2006)
Number (%)
(N=526)
304 (58)
111 (21) 10 (2) 62 (12) 39 (7)
10y-EFS (±SE) 73 (±3) 70 (±5) 67 (±19) 82 (±5) 58 (±8) <0.01 3.5
(1.4-8.8)
*P-values refer to log-rank test comparing EFS of TLP+ to CNS1 status, and hazard ratios refer
to comparison of TLP+ to CNS1 in Cox proportional hazards multivariable analyses.
For abbreviations of all tables, refer to page 9.

8
1.1.6 Risk Factors for Traumatic Lumbar Punctures
There is only one previous study that investigated risk factors for TLP specifically in
children with ALL.34 Howard et al, assessed all children diagnosed with ALL at SJCRH between
1984 and 1998. They examined the first LP and a median of four subsequent LPs for each child.
To adjust for dependence within repeated measures from the same patient, the study utilized
generalized estimating equations (GEE). In total, the dataset included 956 children undergoing
5609 LPs. The estimated OR and (95% CI) for the identified risk factors included 2.3 (1.7-3.0)
for age younger than 1 year vs 1 year or older; 1.5 (1.2-1.8) for black vs white race; 1.5 (1.2-1.8)
for platelet count less vs more than 100 x103/µL; 1.4 (1.1-1.8) for the least vs the most
experienced operator; 10.8 (7.7-15.2) for short (1 day) vs longer (>15 days) interval since the
previous LP; 1.6 (1.4-1.9) for a previous TLP; and 1.4 (1.2-1.7) for early vs recent era when
sedation was routinely used.
Several other studies have also evaluated risk factors for TLP in contexts other than
childhood ALL, often using a different definition of TLP.35-40 Shah et al defined a TLP as >400
RBC/µL and found a rate of 16% in adults visiting the ER, with a significant risk factor being the
inability to visualize spine landmarks.40 Using the same definitions, Glatstein et al found a TLP
rate of 24% for children, with a risk factor being the need for multiple attempts,41 and Pappano
found a rate of 7% TLP in children for LPs performed by a single experienced operator.21 Lastly,
Nigovic et al defined TLP as >10,000 RBC/µL, had a rate of 35% TLP, and identified risk
factors as increased patient movement, less operator experience, local anesthetic not used, and
needle stylet not removed.38,39

9
1.1.7 Limitations of the Previous Literature
The study by Howard et al34 had several limitations that prompted us to undertake our
study. First, there were important potential predictor variables that were not examined. For
example, the effect of body mass index (BMI) percentile or obesity on the rate of TLP; the effect
of first LP (and active leukemia) versus subsequent LPs; the effect of being treated with
anticoagulants or having abnormal coagulation tests; or the influence of using fluoroscopic-
guidance on the rate of TLPs were not explored. Also, that study did not describe its handling of
failed LPs, which are very likely to be traumatic due to the repeated insertions and attempts.
Second, there is a concern that the study is not generalizable to the present clinical
setting, as the range of procedural practices and operator experience has changed over time.42
Howard et al included a large number of LPs performed without sedation and LPs performed by
operators including medical students, residents and nurses. In the current setting, nearly all LPs
are performed under deep sedation,43 and procedures are restricted only to certified oncology
fellows and staff. Therefore, it would be useful to investigate the incidence of TLP and the
identified risk factors in a more recent setting.
Lastly, the Howard study also had some methodological limitations. It examined a
median of four LPs per child. A child with ALL typically undergoes an average of 20 LPs. Thus,
the study could be biased if the risk of TLPs changes across the course of treatment. Secondly, it
used a repeated measures analysis with generalized estimating equations (GEE). While this is an
appropriate method to adjust for longitudinal data, the study did not describe the rationale for
selecting this method nor determine whether other methods of longitudinal analysis may have
been appropriate for the study.44

10
1.2 The Statistical Analysis of Repeated Measures Data
Conducting this study requires the correct application of statistical methods for analyzing
repeated measures data. In this section we will review the objectives, methods and differences
among the various statistical methods available for such analyses. This will form the background
for the further discussion of the methods used for the analysis of risk factors for TLP and help
with understanding and interpreting the results.
1.2.1 Clustered and Longitudinal Data
In a traditional cross-sectional study, where unique individuals are measured on a single
occasion, one aims to obtain estimates of between-subject differences in an outcome variable. In
the experimental setting, such as a randomized controlled trial (RCT), comparisons of the
outcome variable are made across sub-populations that differ in a single predictor variable of
interest, such as an assigned treatment. The process of randomization aims to ensure that all
other extraneous variables are, on average, balanced among the two groups. An important
assumption of all statistical tests used for the analysis of such data is that each individual
observation is independent of any other.
The assumption of independence is violated if there is any reason for individual
observations to be correlated,45 and statistical tests that assume independence will lead to
incorrect results.44 Many health science studies give rise to data that are clustered.46 This can
occur, firstly, if individuals are sampled from naturally occurring groups (such as families,
neighborhoods, hospitals, or clinics). Observations within a group are likely to be positively
correlated, that is they are more likely to be similar within a group than two observations
between groups.

11
Second, clustering can occur if each individual is observed on more than one point in
time. In fact, longitudinal data can be understood as a special case of clustered data.46 Instead of
individuals clustered within groups, here observations are clustered within an individual.
Observations within an individual are more likely to be similar to each other than observations
between individuals. Individuals tend to be persistently high or persistently low in measures of
outcomes. Therefore, appropriate statistical techniques must explicitly account for these positive
correlations or else risk spurious results.45
1.2.2 Advantages and Types of Longitudinal Studies
The defining characteristic of all longitudinal studies is that multiple measurements of the
same individual (or the same research unit such as a tumor or a cell line) are taken over time.46
There are two major advantages to longitudinal studies that are not available to cross-sectional
studies, and these correspond broadly to two different longitudinal study types.
First, longitudinal studies allow the investigation of change over time.47 This is because,
in addition to between-subject comparisons, they allow one to study within-subject changes.
Indeed, in most longitudinal studies, these within-subject changes and the factors that influence
heterogeneity are the primary objective. For example, longitudinal studies may allow one to
study the trajectory of a measure over time (eg. size of a tumor) and how changes depend on a
covariate (eg. cytogenetics of the tumor). In the experimental setting, groups of subjects can be
defined by exposure category and followed. The objective of statistical testing is to compare the
trajectories of the outcome variable between groups. Notably, each individual is only exposed to
one level of the primary predictor variable throughout the study. This subset of longitudinal

12
studies is sometimes referred to as “growth curve analysis” and forms the bulk of the
longitudinal study literature.47
Second, a longitudinal study can allow the comparison of an outcome variable of an
individual subject under different conditions.46 That is, the level of the predictor variable that
each individual is exposed to changes across measurements. In this case, one is not interested in
the change over time per se, but in the effect of different circumstances or covariates on the
outcome variable. This subset of longitudinal studies are often referred to as “repeated measures
studies.”44 Similar to time in the previous example, the experimental condition can be treated as
a within-subject factor and the conditions can be compared using within-subject contrasts.
In the non-experimental setting, the advantages of the repeated measures design are
particularly attractive, since bias from the effects of confounding covariates are ubiquitous in
observational studies and randomization is not available as a solution.48 Furthermore, the gain in
power from multiple observations per individual means that a sufficient sample size can be
accrued from a smaller number of locations or eras.49
1.2.3 Alternatives to Longitudinal Data Analyses
Often, longitudinal studies are analyzed with conventional statistical methods that ignore
the issue of positive correlations.50 The procedure will incorrectly assume that all of the
observations are independent. While the resulting effect estimates may be similar, the standard
errors are often very biased (either larger or smaller) and thus so are the statistical tests of
significance.51 In observational studies, ignoring the correlation most often leads to
underestimation of the variability.50 This in turn results in standard errors that are too small and
test statistics that are too large, risking type I errors.

13
Another common approach is to reduce the data from repeated measures into a summary
measure that can then allow standard statistical methods to be applied.46 For example, one may
estimate the difference between first and last value of an outcome variable, or calculate the area
under the curve (AUC). However, the drawback here is that it forces the analyst to concentrate
on just a single aspect of the repeated measurements, and this leads to loss of valuable
information that may be present in the totality of data. Individuals with very different trajectories
of response may be reduced to having the same summary measure. Two curves with very
different shapes may have the same slope or the same AUC. Moreover, summary measures do
not allow the inclusion of time-varying covariates, and one loses the advantage of the ability to
use the subject as his or her own control.
For a repeated measures study with a continuous outcome variable and a completely
balanced design, ANOVA or MANOVA may be used. However, these methods cannot handle
unbalanced designs, missing data, or binary outcomes.51
Therefore, the most commonly used methods for the analysis of longitudinal data involve
a number of closely-related techniques based on regression methods.46 These include mixed
models (random effects), conditional models (fixed effects) and marginal models (GEEs). We
will discuss the relative strengths and limitations of these methods in the following sections.
1.2.4 Notation
A basic linear regression model from a cross-sectional study can be written as:
Yi = β0 + βXi + εi
In this notation,46 Yi is the value of the outcome variable for individual i. β0 is the
intercept term in the model. Xi is a vector of covariates that varies between individuals, such as

14
the platelet count or gender. β is the fixed parameter that is estimated by regression and that
relates Xi to Yi. ε is a random error term. This is the standard notation that is familiar to
researchers from conventional linear regression. The same equation applies to non-linear (or
generalized linear) regression if a link function or transformation of Yi is used.51
In repeated measures data, there is one record for each individual at each time point.
There is an identifying number (or subject variable i) that is the same for all records that come
from the same individual. Additionally, there is also an observation number (or time variable t)
that indicates which time point the record comes from.
In a repeated measures model, the familiar vector of covariates Xi is “partitioned” into
two types of covariates: those whose values do not change for an individual over the duration of
the study (time-invariant or between-subject covariates) and those whose values do change over
time (time-varying or within-subject covariates).46,48 This new model can be written as:
Yit = β0 + βXit + Wi + αi + εit
In this notation, Yit is the value of the outcome variable for individual i at time t. β0 is the
intercept term in the model. Xit is a vector of time-varying variables, such as the platelet count
prior to a procedure. Wi is a vector of measured time-invariant covariates, such as gender or
ethnicity. Finally, αi denotes the vector of all time-invariant characteristics of individuals that are
not otherwise accounted for by the Wi term. Such covariates can include an individual’s genomic
profile, internal anatomy, and all other characteristics that are stable over time. These covariates
can influence the individual’s level of response, but they remain unknown to the investigator.
Models of this type are known as linear mixed models. The “linear” denotes that they can
be expressed as a linear equation, and “mixed” indicates that they contain both fixed and random
15
terms. The word “generalized” is added when they are extended to logistic, poisson or other
regression methods through a link function.
An important choice now arises regarding the nature of αi. It can be treated as either a
random variable or a fixed variable.48 This choice underlies the fundamental difference between
two analysis methods and lends them their names.
1.2.5 Random Effects Methods
αi can be treated as a random variable with a specified probability distribution. In this
case, it is allowed to vary between individuals (and can potentially be estimated for each
individual if desired).51 The underlying premise of this type of model is that some subset of
regression parameters vary from one individual to another, and these account for sources of
natural heterogeneity in the population. That is, individuals in the population are assumed to
have their own subject-specific mean responses and their own subset of regression parameters.
Individuals are either “high-responders” or “low-responders.” The response is modeled as a
combination of population characteristics, β and W, that are assumed to be shared by all
individuals, and subject-specific effects that are unique to a particular individual. The former are
referred to as fixed effects, while the latter are referred to as random effects. The term “mixed
models” in this context therefore indicates that the model contains both fixed effects and random
effects. (Although confusing, common use in the literature refers to these models as simply
“random effects,” though it should be remembered that they contain both types).44
In simplified terms, what the estimation procedure does is calculate a regression equation
for each individual in the study, with unique subject-specific estimates of αi, and then compute a
weighted average all such equations to arrive at an estimate of β and W. The mixed model

16
utilizes all within-subject and between-subject comparisons and arrives at an estimate of the
parameter for both time-invariant and time-varying covariates.52 In concrete terms, this is akin to
asking the question “If a child has a traumatic LP on k days, what factors are different about
those days compared to any other day or any other child?”48
1.2.6 Fixed Effects Methods
On the other hand, if αi is treated as a set of fixed parameters, it is no longer easy to
estimate αi by regression. The αi term is now perfectly collinear with the Wi term, and thus both
cannot be estimated. They can however be conditioned out of the estimation process.
To better understand this important concept, let us examine the simplest case of a study
with only two repeated measures (e.g. a crossover trial with an outcome variable measured
before and after starting a treatment). To estimate β, the effect of the treatment, we can calculate
the within-subject changes in the outcome variable, Yi2 – Yi1, as follows:46,48
Yi2 – Yi1 =
β0 + βXi2 + Wi + αi + εi2
- ( β0 + βXi1 + Wi + αi + εi1 )
----------------------------------------------------
= β (Xi2 – Xi1) + (εi2 – εi1)
Note that in calculating this difference, the intercept terms, the time-invariant covariate
effects and the stable characteristics term αi have all disappeared or cancelled out. Therefore, the
stable individual characteristics can have no effect on the estimate of β, even if αi is correlated to
β or is a confounder of the relationship between X and Y.

17
Seen another way, the fixed effects model performs only within-subject comparisons and
discards all between-subject comparisons. In concrete terms, this is akin to asking the question
“If John had a traumatic LP on k days but not on other days, what was different about John on k
days compared to John on other days?”48 We may check to see if the days with a TLP were
associated with a particularly low platelet count. However, since John was a male on all days, the
effect of gender cannot be estimated and has been conditioned out. It makes no sense to ask what
effect male gender had on some days compared to other days. This is not to say that the effect of
gender is discarded, but rather that it is controlled for or balanced across comparisons. In the
example of the before and after experiment that we outlined above, the only variable that differed
between the two time points was the experimental treatment. There was no possible confounding
by gender, age, race, genetics or any other stable covariate. The essence of the fixed effects
method is captured by saying that each individual serves as his or her own control.48
1.2.7 Hybrid Random-Fixed Effects Method
There is a hybrid method that allows one to “disentangle” a covariate into its fixed effect
and random effect components.46,48 This is done by calculating the means and deviations of the
covariate, and regressing on these parameters separately. The estimate of the deviation variable
corresponds closely to the fixed effect. This method has the advantage of combining the best of
both worlds, providing control for bias from stable characteristics where desired while also
allowing inclusion of time-invariant covariates. However, it has the significant disadvantage of
losing parsimony and being difficult to understand by most health science readers. It may be
equally acceptable to simply report both effects as separate analyses if this is desired.

18
1.2.8 Marginal Models (Generalized Estimating Equations)
Despite their many differences, both the random and fixed effects models begin from the
linear mixed model paradigm. They are thus usually distinguished from a third method for the
analysis of repeated measures data known as marginal models, which use an entirely different
approach for accounting for the within-subject correlations.
The term “marginal” indicates that the model for the mean response depends only on the
covariates of interest, and not on any random effects or previous responses. There is no vector of
random effects and no subject-specific coefficients. In other words, there is no model constructed
for each individual, but rather one model for the mean response of the whole population.
Individuals are not distinguished as high responders or low responders but as contributing to an
overall average or “generalized” response. Hence, the most common method for estimating
marginal models is known as generalized estimating equations (GEE).
GEE models the mean response and separately models the within-subject associations
among the repeated measures.53 The goal is to make inferences about the former, while the latter
is treated as a nuisance variable that must be accounted for and thus “removed.”50 Therefore,
GEE estimates two different equations, one for the mean relations and one for the covariance
structure.51 The latter is specified as a “working” correlation matrix. The correlation matrix is a
two-dimensional array of conditional variances and covariances. The covariance structure can be
specified by the analyst to allow an expected pattern.50 An unstructured matrix imposes no
particular assumption about the covariance structure. The exchangeable (or compound-
symmetry) covariance structure specifies a single correlation that applies to all pairs of

19
observations. An independent structure assumes zero correlations. An autoregressive structure
assumes that observation are only related to their own past values and correlations decline with
time. While specifying the correct covariance structure may increase efficiency,54 overall the
GEE estimation is quite robust to misspecifications.55
1.2.9 Strengths and Limitations of Each Method
Recall that the major advantage of RCTs is their ability to balance confounding
covariates across groups, even if they are unmeasured or unknown. In non-experimental studies,
researchers try to approximate a randomized experiment by statistically controlling for potential
confounding covariates using methods such as multivariable regression or propensity scores.
However, the researcher can only control for confounding covariates that are known, thought
about, and accurately measured. Some important covariates are almost always omitted. As a
result, estimates from non-experimental studies are always at risk of confounding bias.
In the fixed effects model outlined above, the same advantage of an RCT becomes
available to an observational study due to the availability of repeated measures and within-
subject comparisons. Confounding covariates (that are stable over time) are always balanced
across comparisons. The estimate of the effect of the predictor variable of interest is free of any
potential confounding effect of stable covariates, even those that have not been measured or
identified. This eliminates potentially large sources of bias.
However, there are three important disadvantages to fixed effects methods. First, as we
have already seen, fixed effects methods do not estimate a coefficient for time-invariant
characteristics, such as gender or ethnicity.44 If these covariates are of primary importance to the
20
researcher, then fixed effects methods would not be preferred. For similar reasons, fixed effects
may not be useful for variables that do change over time but only to a small degree. For example,
a fixed effects analysis may show a significant effect for height in children followed over a
decade, but is unlikely to do so for adults since height changes are minimal. Second, fixed effects
methods discard all information for subjects that have no variability in the outcome throughout
the study.48 If John never has a TLP, we cannot ask what factors put him at risk for TLP, and his
data drop out of the analysis. Thus, the effective sample size for fixed effects methods is usually
smaller relative to random effects methods.44 If a significant portion of subjects show no
variability in the outcome, the loss of information may become substantial. Third, by discarding
the between-person comparison, fixed effects in observational studies has more sampling
variability and thus yield standard errors that are considerably larger when compared to methods
that utilize both between- and within-subject comparisons. In summary, fixed effects offers
researchers a trade-off between reduced bias at the expense of increased variability and loss of
information.48
The relative strengths and weaknesses of random effects methods are a mirror image of
those for fixed effects. Random effects perform both within-subject and between-subject
comparisons and so typically have less sampling variability. They do allow for estimation of the
effects of stable characteristics such as gender and ethnicity. They do not discard information for
individuals whose outcome variable does not change. However, they do not control for
unmeasured stable characteristics of the individual.
Despite the differences in how they are derived, GEE models are similar to those
estimated by the random effects method, especially when an exchangeable covariance structure
is specified.50 Both perform within-subject and between subject contrasts, provide an estimate for

21
time-invariant covariates, but do not control for bias from stable characteristics. If the latter
factor is of primary interest, then once again fixed effects are to be preferred.
However, the separation of the modeling of the mean response and the correlations has
important implications for the interpretation of the regression parameters. While the parameters
from random and fixed effects methods are referred to as “subject-specific,” those from GEE are
referred to as “population-averaged.”50 For the former, the target of inference is the individual.
For the latter, it is the population. The regression parameters β are said to have population-
averaged interpretations. Therefore, the choice between random effects and GEE is not made on
statistical but rather on subject-matter grounds. If the researcher is interested in determining
subject-specific coefficients, such as the expected benefit of treatment for an individual patient,
then random effects are preferred. If the researcher is interested in the potential reduction in
morbidity for a population if the new treatment is universally implemented, GEE is
preferred.44,50,55
In health science studies, however, the subject-specific responses for individuals are often
not shown in published reports. The random effects method does produce a “marginal” mean
estimate of the β coefficients by averaging over the distribution of the random effects.50 The
estimates may be very identical to those produced by GEE. However, when there is significant
unobserved heterogeneity, the estimates produced by GEE are usually smaller, as they undergo
“heterogeneity shrinkage,” or an attenuation towards zero in the presence of heterogeneity.55
Some authors state that the heterogeneity shrinkage is corrected by the random or fixed effects
models and therefore the latter are preferred,50 while others believe that the random effects
estimates are biased upwards, and that if the goal is to make an inference about the population
average mean of Yi, that GEE should be adopted. Either model may be equally acceptable, and
22
Fitzmaurice et al write that the controversy of GEE versus random effects “has generated more
heat than light.”46
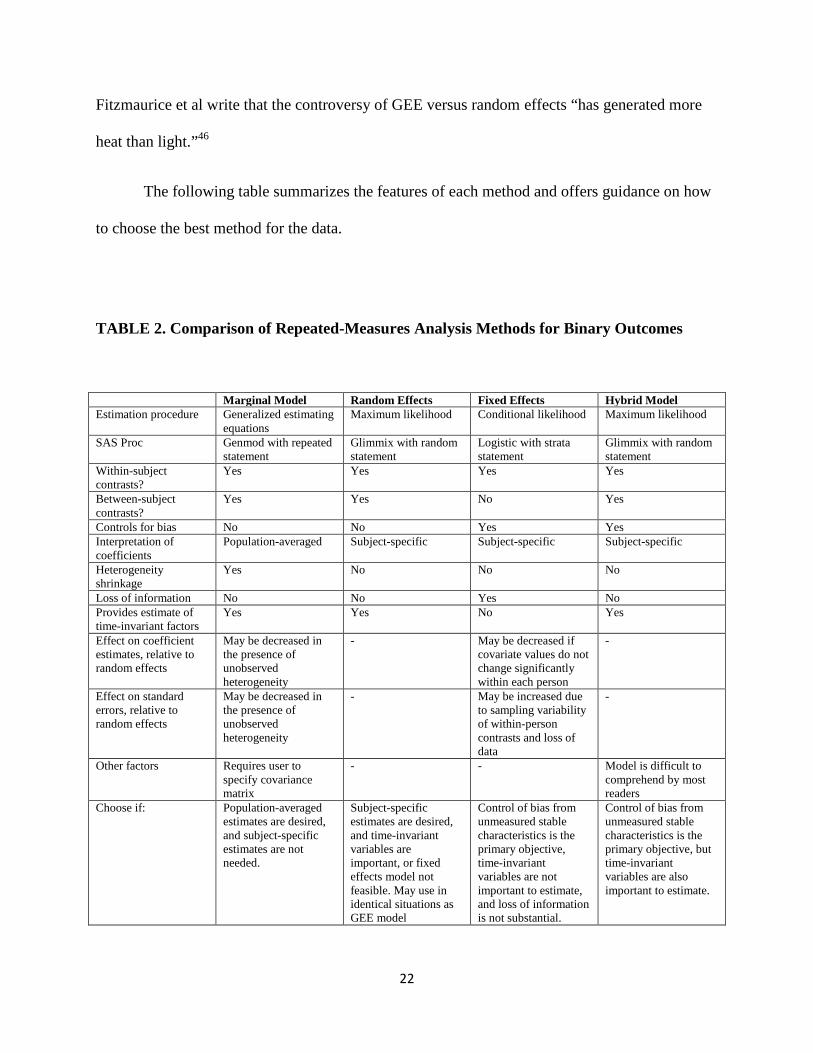
The following table summarizes the features of each method and offers guidance on how
to choose the best method for the data.
TABLE 2. Comparison of Repeated-Measures Analysis Methods for Binary Outcomes
Marginal Model Random Effects Fixed Effects Hybrid Model Estimation procedure Generalized estimating
equations Maximum likelihood Conditional likelihood Maximum likelihood
SAS Proc Genmod with repeated statement
Glimmix with random statement
Logistic with strata statement
Glimmix with random statement
Within-subject contrasts?
Yes Yes Yes Yes
Between-subject contrasts?
Yes Yes No Yes
Controls for bias No No Yes Yes Interpretation of coefficients
Population-averaged Subject-specific Subject-specific Subject-specific
Heterogeneity shrinkage
Yes No No No
Loss of information No No Yes No Provides estimate of time-invariant factors
Yes Yes No Yes
Effect on coefficient estimates, relative to random effects
May be decreased in the presence of unobserved heterogeneity
- May be decreased if covariate values do not change significantly within each person
-
Effect on standard errors, relative to random effects
May be decreased in the presence of unobserved heterogeneity
- May be increased due to sampling variability of within-person contrasts and loss of data
-
Other factors Requires user to specify covariance matrix
- - Model is difficult to comprehend by most readers
Choose if: Population-averaged estimates are desired, and subject-specific estimates are not needed.
Subject-specific estimates are desired, and time-invariant variables are important, or fixed effects model not feasible. May use in identical situations as GEE model
Control of bias from unmeasured stable characteristics is the primary objective, time-invariant variables are not important to estimate, and loss of information is not substantial.
Control of bias from unmeasured stable characteristics is the primary objective, but time-invariant variables are also important to estimate.

23
1.3 Study Objectives
1.3.1 Primary objective:
To determine risk factors for TLPs in children with ALL
1.3.2 Secondary objectives:
1) To determine whether the EFS for patients who are TLP+ is significantly lower than those
who are CNS1 treated on contemporary regimens
2) To compare and contrast three different methods for the analysis of repeated-measures data:
GEE, random effects, and fixed effects methods.

24
1.4 Study rationale
Knowing the risk factors for TLPs in children with ALL would allow clinicians to frame
guidelines to optimize modifiable factors. This would allow pediatric oncologists to determine
the optimal platelet threshold, the minimal level of experience for suitable operators, and the
utility of image-guidance. Knowing which children are at highest risk of TLP would be very
important in directing appropriate prospective interventions to those who would most benefit
from such interventions. Some examples of potential interventions that could be tested in future
studies may include non-traumatic needles, improved guidelines or training programs, or
ultrasound-guidance for procedures.

25
CHAPTER 2: METHODS
2.1 Study Design
We conducted a retrospective cohort repeated-measures study utilizing hospital-based
health care records. The study received institutional and research ethics board approval from The
Hospital for Sick Children (SickKids) and the University of Toronto.
2.2 Study Population
2.2.1 Inclusion Criteria
The study population included children with ALL newly diagnosed at SickKids between
January 1, 2005 and December 31, 2009 who were between 0 to 18 years of age at diagnosis.
2.2.2 Exclusion Criteria
Children with relapsed ALL, secondary ALL, Burkitt leukemia (L3), and children who
did not undergo any LPs were excluded.
2.2.3 Study Timeline
The timeline for the inclusion of children in the study and the follow-up of the cohort is
shown in Figure 1. The last date of data extraction and the study end-date was March 1, 2012.

26
FIGURE 1. Timeline of study inclusion and follow-up
Accrual Window
Observation Window
TIME
Accrual start date: Jan 1, 2005
Accrual End Date: Dec 31, 2009
Maximum Follow-up Date: March 1, 2012

27
2.3 Variables
2.3.1 Primary Outcome Variable
The primary outcome variable was a TLP, defined as an LP that contained at least 10
RBCs per microliter of CSF.
2.3.2 Secondary Outcome Variable
The secondary outcome variable was EFS, defined as the time interval from date of
diagnosis to relapse, second malignancy, treatment-related mortality, death, or date last seen
(whichever occurred first).
2.3.3 Predictor Variables
The potential predictor variables (covariates) included patient, disease, operator, and
procedure-related variables. Furthermore, as for repeated-measures studies, covariates were also
classified as being either time-varying (if they could have different values at different
observations, such as age at LP), or time-invariant (if they could not have different values at
different observations, such as age at diagnosis or gender).
All continuous variables were categorized according to cut-offs determined from
previous literature or the clinical judgment of study investigators. The list of variables, their
categories, the rationale for selected categorizations, and comments related to their importance or
analysis are shown in Table 3.

28
TABLE 3. List of Predictor Variables and Rationale
Variable Categories Comments A. Patient-Related Variables Age at LP <1 year
1-<10 year ≥10 year
National Cancer Institute/Rome criteria for ALL risk stratification
Gender Male Female
Ethnicity White Black Other
Categorized as per Howard et al.34 Race was a risk factor for TLP, possibly due to variations in lumbar lordosis by race.
BMI percentile 0-<95 ≥95
BMI percentile ≥ 95 is a standard definition for obesity, but not previously investigated for association with TLP.
B. Disease-Related Variables Initial WBC (x103/µL)
0-100 ≥100
Risk factor in Gajjar et al.22 High WBC may be a marker of inflammation. Note that this variable is only meaningful for the first LP.
Platelets (x103/µL)
0-50 51-75 76-100 >100
Categorized as per Howard et al.34 Platelet count below 100 x103/µL was a risk factor for TLP.
INR or PTT Normal Abnormal
INR and PTT are tests of coagulation and abnormal values may lead to increased bleeding risk.
C. Operator-Related Variables Position Oncology Fellow
Oncology Staff Radiologist
Radiologists only conducted LPs for referred patients using fluoroscopic-guidance. Association with TLP not previously investigated. Note that the comparison of radiologists versus oncologists also represents the effect of using image-guidance.
D. Procedure-Related Variables Phase of treatment
First LP Pre-maintenance Maintenance
To determine if rate of TLPs varies between first LP and subsequent LPs. The pre-maintenance phase is a time of high treatment intensity, usually lasting 6 months, followed by a 2-3 year maintenance phase.
Use of Anticoagulation
None Prophylactic dose Treatment dose
Effect of anticoagulation on bleeding during LPs has not been previously investigated.
Days since previous LP
0-3 4-7 8-15 ≥16
Categorized as per Howard et al.34 This and next 2 variables related to previous LP, to allow adjustment for the potential residual or “lag” effects of previous LP. Theoretically, red blood cells from a previous TLP may be seen at the next one.
Previous TLP Yes No
Identified as a risk factor by Howard et al.34
Platelet count at previous LP (x103/µL)
0-50 51-75 76-100 >100
Identified as a risk factor by Howard et al.34
29
2.4 Data Sources and Measurement
Children were identified through querying a prospective database maintained by
information coordinators in the Division of Hematology/Oncology at SickKids. For each
included child, data were recorded for all LPs from diagnosis until end of therapy, relapse, bone
marrow transplant, death, or date last seen. For children who experienced a relapse, second
malignancy or received a bone marrow transplant, LP variables were only collected preceding
and not after these events.
Each of the specified predictor variables for this study was documented as part of routine
clinical care. The principle data source was the electronic patient chart (EPC) which includes
scanned copies of all hand-written or typed clinical documentation at SickKids. Data on the
outcome variable as well as all laboratory tests were collected from the hospital’s electronic
repository of laboratory results (Sunrise Kidcare).
Data on the identity of the operator was abstracted in a hierarchical manner from multiple
sources. This allowed double-data verification in the large majority of cases. First, we searched
for a progress note or signature for the operator in the EPC. The signatures were compared to a
master-sheet containing signatures of all staff and fellows in Hematology/Oncology. Second, we
compared these names with the most recently-updated monthly schedule for the procedure room.
When procedures were performed instead in the operating room (OR) or image-guided therapy
(IGT) department, the name of the operator was found in the OR log. Third, we obtained paper
copies of the procedure room records maintained by the nurse in charge, which also included the
name of the operator. Lastly, as a method of confirmation, we sorted our dataset by the date of
procedure. In doing so, all operator identifiers for a particular date would be expected to be
identical, and any discrepancies were further investigated. If results were discrepant, the order of

30
reliability was considered to be signatures (most reliable), OR logs, nursing paper records, and
then monthly schedule (least reliable).
Height and weight were abstracted from the clinical visit on the day of or most proximate
to the day of the LP. As height was not recorded at each visit, the process of last observation
carried forward (LOCF) was used. Since clinic visits for ALL occur frequently and height is
unlikely to change significantly between visits, this is a reasonable approach. Using height and
weight, BMI was calculated as weight (in kilograms) divided by height (in meters) squared. BMI
at each time point was compared to age and sex references to determine BMI percentile based on
the 2000 growth charts of the Centers for Disease Control and Prevention (CDC), using a SAS
macro.56 Cut-offs were made as per the definition of childhood obesity as a BMI percentile ≥ 95
for children 2 years of age or older, or as a weight-for-height percentile ≥ 95 for children less
than 2 years old.57
2.5 Sample Size
At SickKids, there are approximately 50-60 children with newly diagnosed ALL each
year. Each child receives an average of 20 LPs. Using inclusion of a five-year period, we
expected to have 250 patients and 5,000 procedures in our cohort. The expected baseline rate of
TLPs, based on our preliminary analysis, was around 16%. Therefore, we expected to have
approximately 800 events in our study. Simulation studies have shown that a minimum of 10
events per variable in a logistic regression model are required, and that below this number
coefficient estimates are biased and variance estimates are inefficient. If we were to use the
approach of 10 events per variable for this study,58,59 we would have sufficient power to examine
up to 80 variables. However, in a repeated-measures study, the number of events needed per
31
covariate also depends on the degree of dependency among observations.49 Sample size can thus
be challenging to estimate and presently requires simulation techniques.51 Nevertheless, a sample
size of 800 events would be conservatively expected to provide sufficient power for the intended
analyses.
2.6 Statistical Analyses
All analyses were conducted using SAS version 9.3 for windows (SAS Institute, Cary,
NC). Statistical significance was defined as a p-value <0.05. Given that the primary objective
was to identify predictor variables and not to test particular hypotheses, no adjustment for
multiple comparisons was made. We reported odds ratios (ORs) with 95% CIs. An OR over 1.0
indicated that the predictor variable was associated with an increased risk of TLP relative to the
reference level.
2.6.1 Descriptive Statistics
Demographic and disease characteristics were calculated for the presentation of
descriptive statistics. Normality of data was tested for continuous variables using histograms and
the Kolmogorov-Smirnov test. Non-normally distributed variables were presented with median
and interquartile range. Categorical variables were presented with number and percentage.
2.6.2 Model Building
Collinearity was tested for all covariates. A variance inflation factor (VIF) >2.5 and
tolerance of <0.4 were used to define collinearity. Correlations were tested using Pearson

32
correlations, with a value of 0.2-0.4 considered a moderate correlation and a value above 0.4
considered a high correlation. Variables that were either collinear or highly correlated were not
both included within the same multivariable model.
To compare different methods available for the analysis of longitudinal data, univariate
and multivariable models were constructed using five different methods. Within each method,
the final multivariable model was developed using a backward selection strategy. From among
the five models, the final model to be presented was based on a combination of clinical judgment
and the suitability of the method to the data as summarized in Table 2.
2.6.3 Conventional Logistic Regression
First, univariate and multivariable models were constructed using conventional logistic
regression methods by utilizing SAS Proc LOGISTIC.55 This method assumes independence of
all observations and thus is an incorrect method for analyzing longitudinal data. It is knowingly
included here only for instructional purposes, in order to compare the resulting effect estimates,
standard errors, p-values and final models between methods that do and do not adjust for the
dependence among repeated measures.
2.6.4 Generalized Estimating Equations
Second, we fit a marginal model with GEE using SAS Proc GENMOD with an
exchangeable (compound symmetry) working correlation matrix.55 This method produces
population-averaged coefficients and conducts both within-person and between-person
comparisons.
33
2.6.5 Random-Effects (Generalized Linear Mixed Models)
Third, we fit a generalized linear mixed model with maximum likelihood estimation
using SAS Proc GLIMMIX.48 Although the name includes linear, the procedure can be used to
model a dichotomous outcome through a link function. This method produces subject-specific
coefficients by incorporating a term for a random intercept variable representing unobserved
heterogeneity. It conducts both within-person and between-person comparisons. The resulting
coefficients can be interpreted as answering “what is the probability of a patient with this
variable having a TLP when compared to patients without this variable?”
2.6.6 Fixed-Effects (Conditional Logistic Regression)
Next, we fit a fixed effects model using SAS Proc LOGISTIC with a STRATA statement
for the subject term.48 This method conditions out all stable characteristics of subjects and
examines only time-varying covariates. It conducts only within-subject comparisons, thereby
allowing each patient to be used as his or her own control. The resulting coefficients can be
interpreted as answering “what is the probability of this patient having a TLP when exposed to
this variable as compared to the same patient when not exposed to this variable?”
2.6.7 A Hybrid Method
Lastly, we fit a hybrid method that combines the fixed-effects and random-effects
approach, allowing us to embed the fixed effects of interest within a random-effects model. This
is accomplished by incorporating means and deviations for each time-varying predictor within
the model specified by Proc GLIMMIX.48 The deviation estimate represents the fixed effects.

34
2.6.8 Kaplan-Meier Survival Curves
For the secondary objective, to determine the association between CNS status and EFS
the Kaplan-Meier product-limit estimator method was used.60 CNS status was classified based on
the results of the first LP using the SJCRH system. EFS was stratified by CNS status, and a two-
sided log-tank test used to compare TLP+ with CNS1 status.
35
CHAPTER 3: RESULTS
3.1 Descriptive Statistics
3.1.1 Participants and Procedures
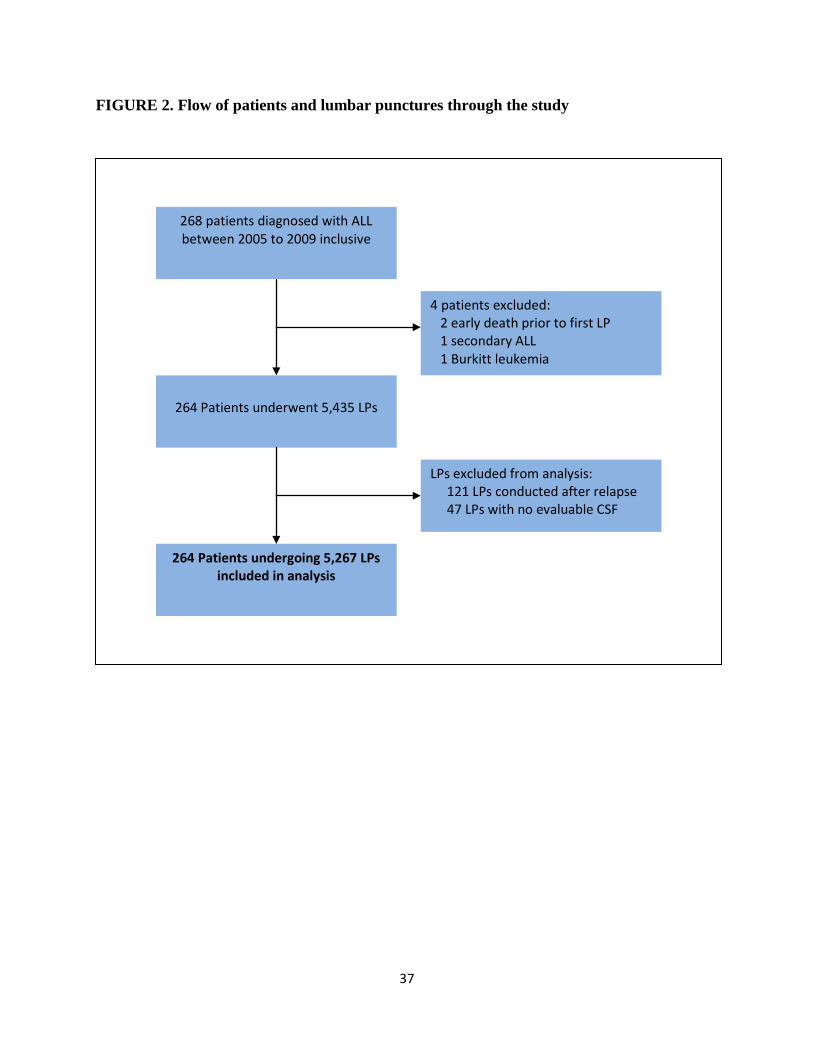
Of the 268 children diagnosed with ALL during the 5-year period, 2 were excluded
because of early death before the first LP, 1 due to a diagnosis of secondary ALL, and 1 due to a
subsequent diagnosis of Burkitt leukemia. The remaining 264 children underwent 5,435 LPs. Of
these, 121 LP observations were excluded as they occurred after a diagnosis of relapse. Sixteen
LPs were documented as being successful but did not have an available CSF RBC count. A
further 31 LPs were failed procedures (0.6%) that also did not have an available CSF RBC count.
Failed LPs were those where documented attempts could not lead to evaluable CSF. These 47
LPs with missing CSF values could not be used in analyses involving the outcome variable of
TLP. They were, however, kept within the dataset as complete exclusion would have affected
variables determined from the previous procedure (such as days since previous LP).
In total, therefore, 264 children undergoing 5267 LPs were included in the final analysis.
The mean number of evaluable LPs was 20.0, and ranged from 1 to 31 per child. The flow of
patients and procedures through the study are shown in Figure 2.
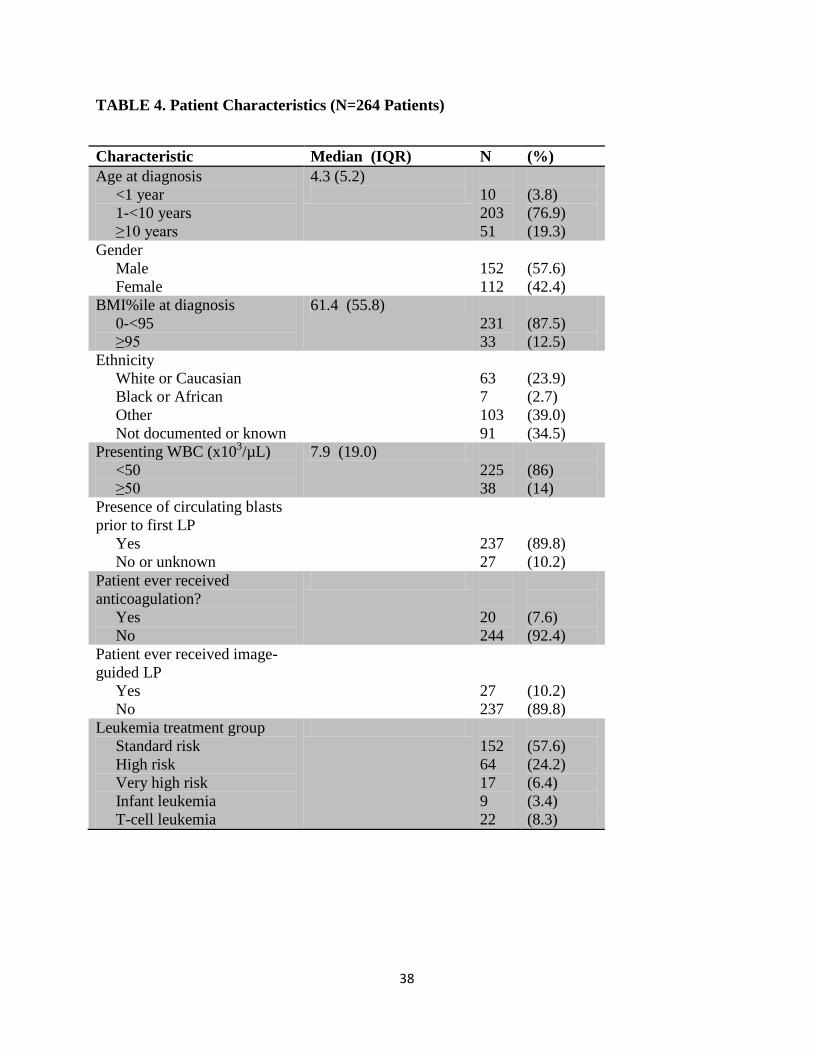
3.1.2 Characteristics
The demographic and disease characteristics for 264 children are shown in Table 4.
These characteristics include time-invariant variables or the value of time-varying covariates at
the day of the first LP. As all continuous variables were non-normally distributed, they are
presented with median and interquartile range.
36
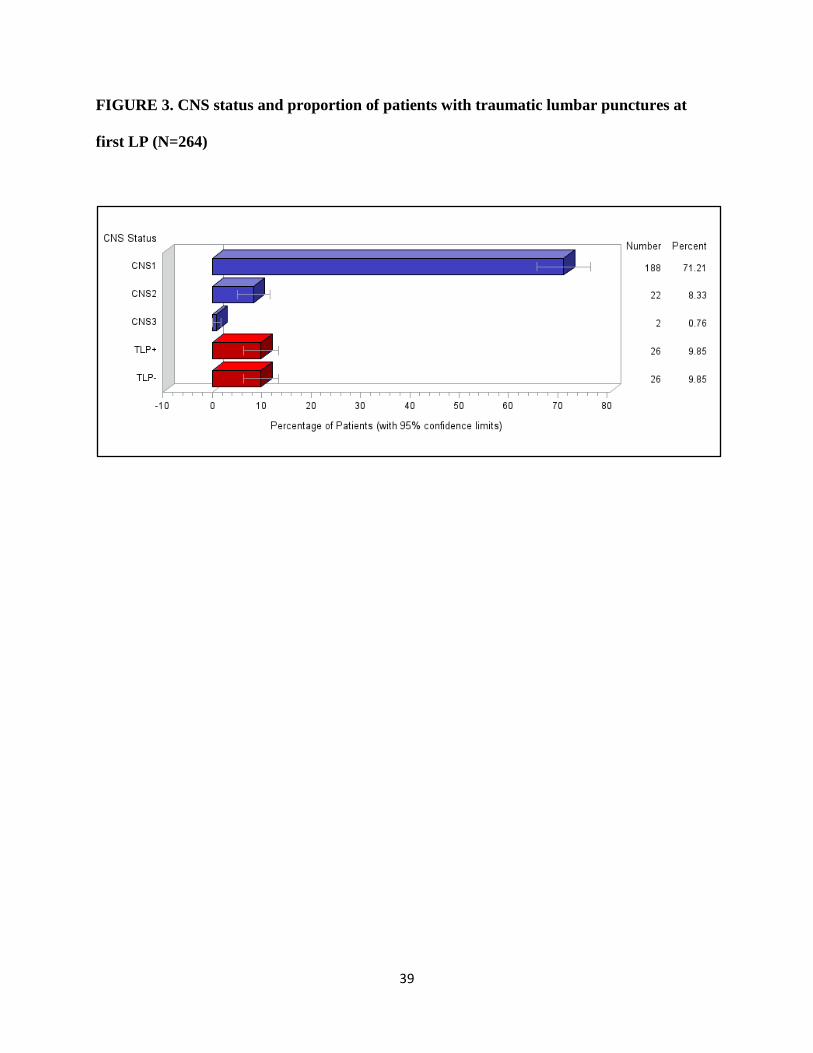
3.1.3 Primary Outcome: Traumatic Lumbar Punctures
Among all 5267 evaluable LPs, there were 943 (17.9%) TLPs. Among the 264 first LPs,
there were 52 (19.7%) TLPs. There were 26 (9.8%) TLP+ containing blasts, and 26 TLP-
containing no blasts. The distribution of CNS status using the SJCRH system are shown in
Figure 3. Of the 26 TLP+ patients, 16 required the treating physician to use the Steinherz-Bleyer
formula to determine the COG CNS status, and 10 could be classified as CNS2 without the
formula.
37
FIGURE 2. Flow of patients and lumbar punctures through the study
268 patients diagnosed with ALL between 2005 to 2009 inclusive
264 Patients underwent 5,435 LPs
264 Patients undergoing 5,267 LPs included in analysis
4 patients excluded: 2 early death prior to first LP 1 secondary ALL 1 Burkitt leukemia
LPs excluded from analysis: 121 LPs conducted after relapse 47 LPs with no evaluable CSF
38
TABLE 4. Patient Characteristics (N=264 Patients)
Characteristic Median (IQR) N (%) Age at diagnosis <1 year 1-<10 years ≥10 years
4.3 (5.2)
10 203 51
(3.8) (76.9) (19.3)
Gender Male Female
152 112
(57.6) (42.4)
BMI%ile at diagnosis 0-<95 ≥95
61.4 (55.8) 231 33
(87.5) (12.5)
Ethnicity White or Caucasian Black or African Other Not documented or known
63 7 103 91
(23.9) (2.7) (39.0) (34.5)
Presenting WBC (x103/µL) <50 ≥50
7.9 (19.0) 225 38
(86) (14)
Presence of circulating blasts prior to first LP Yes No or unknown
237 27
(89.8) (10.2)
Patient ever received anticoagulation? Yes No
20 244
(7.6) (92.4)
Patient ever received image-guided LP Yes No
27 237
(10.2) (89.8)
Leukemia treatment group Standard risk High risk Very high risk Infant leukemia T-cell leukemia
152 64 17 9 22
(57.6) (24.2) (6.4) (3.4) (8.3)
39
FIGURE 3. CNS status and proportion of patients with traumatic lumbar punctures at
first LP (N=264)
40
3.2 Inferential Statistics
3.2.1 Collinearity and Correlations
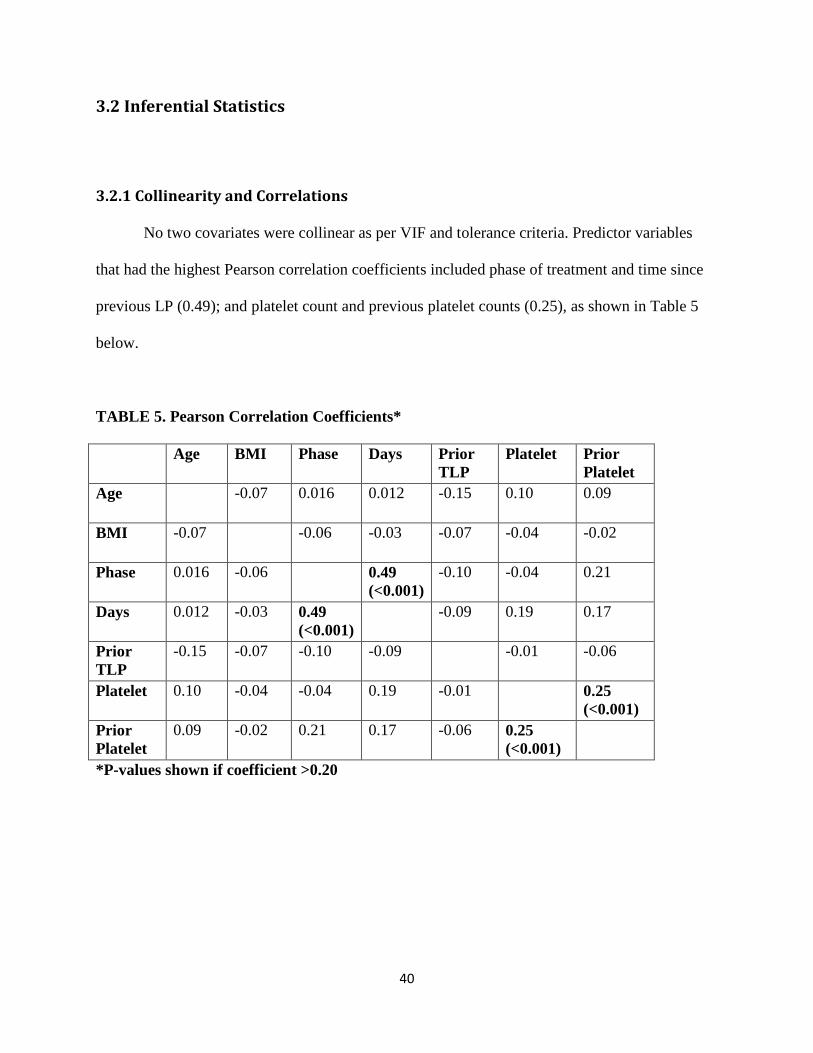
No two covariates were collinear as per VIF and tolerance criteria. Predictor variables
that had the highest Pearson correlation coefficients included phase of treatment and time since
previous LP (0.49); and platelet count and previous platelet counts (0.25), as shown in Table 5
below.
TABLE 5. Pearson Correlation Coefficients*
Age BMI Phase Days Prior TLP
Platelet Prior Platelet
Age -0.07 0.016 0.012
-0.15 0.10 0.09
BMI -0.07 -0.06 -0.03 -0.07 -0.04 -0.02
Phase 0.016 -0.06 0.49 (<0.001)
-0.10 -0.04 0.21
Days 0.012 -0.03 0.49 (<0.001)
-0.09 0.19 0.17
Prior TLP
-0.15 -0.07 -0.10 -0.09 -0.01 -0.06
Platelet 0.10 -0.04 -0.04 0.19 -0.01 0.25 (<0.001)
Prior Platelet
0.09 -0.02 0.21 0.17 -0.06 0.25 (<0.001)
*P-values shown if coefficient >0.20

41
3.2.2 Model Building
From the list of 13 potential predictor variables listed in Table 3, nine were tested in the
repeated-measures multivariable regression analyses. Initial WBC count and coagulation tests
(INR/PTT) were excluded as they were relevant only to first LPs and were not significantly
associated with first LPs being traumatic. Phase of treatment, although significant in univariate
analyses, was excluded due to its high correlation with days since previous LP. The covariate
ethnicity was difficult to measure. In about one-third of our cases, we could not find any
documentation of ethnicity, and in many other situations found it difficult to classify. Therefore
ethnicity was not further examined as a predictor variable in regression modeling.
The results for univariate and multivariable regression modeling using each of five
methods is shown in Tables 6 to 10. Variables to be included in multivariable models were
selected using backward elimination. The final multivariable models are displayed comparatively
in Table 11. For models that utilized between-subject comparisons (all except fixed effects), the
same five variables were selected using automated or manual backward elimination procedures.
These variables included age at LP (1-<10 years versus < 1 or ≥ 10 years), BMI percentile (≥ 95
versus < 95), platelet count at LP (over 100 x103/L versus 0-50, 51-75 or 76-100 x x103/L), days
since the prior LP (≥16 vs 0-3, 4-7 or 8-15 days), and a preceding TLP.
Both the effect estimates and the confidence intervals produced by each of these methods
were very similar across all covariates, even when accounting for repeated measures was ignored
as in the conventional logistic regression model. The confidence intervals for the conventional
model were only slightly larger than for the GEE model. The effect estimates and CIs produced
by GEE and random effects were slightly different in univariate analysis but became nearly
equivalent in multivariable analysis.

42
In the fixed effects univariate model, platelet count at LP, platelet count at previous LP,
days since previous LP and operator position (radiologist versus oncologist) were significant. In
multivariable analysis, only days since prior LP and operator (radiologist versus oncologist)
remained, and the effect of radiology was seen to reduce the odds of TLP. In total, 27 children
underwent 233 LPs under radiologic guidance. This latter variable was not selected in any other
model. In general, the fixed effects method produced much larger confidence intervals than the
other methods. As expected, it did not produce any estimate for the time-invariant variable, sex.
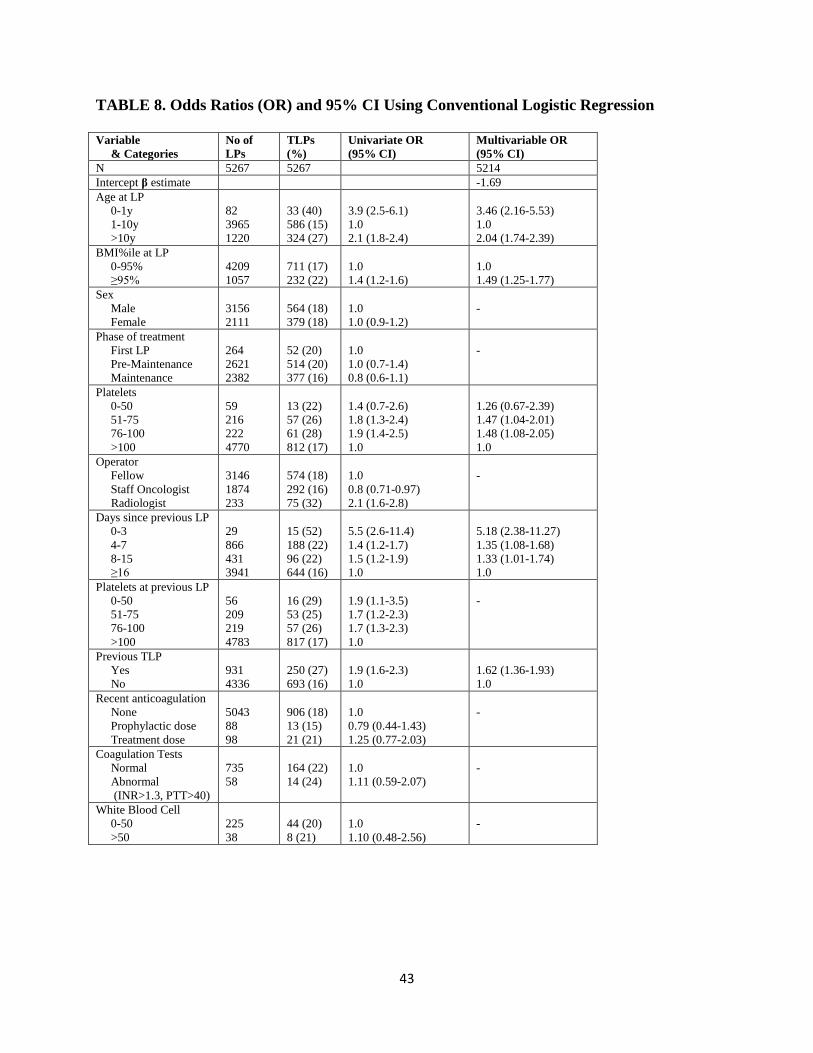
43
TABLE 8. Odds Ratios (OR) and 95% CI Using Conventional Logistic Regression
Variable & Categories
No of LPs
TLPs (%)
Univariate OR (95% CI)
Multivariable OR (95% CI)
N 5267 5267 5214 Intercept β estimate -1.69 Age at LP 0-1y 1-10y >10y
82 3965 1220
33 (40) 586 (15) 324 (27)
3.9 (2.5-6.1) 1.0 2.1 (1.8-2.4)
3.46 (2.16-5.53) 1.0 2.04 (1.74-2.39)
BMI%ile at LP 0-95% ≥95%
4209 1057
711 (17) 232 (22)
1.0 1.4 (1.2-1.6)
1.0 1.49 (1.25-1.77)
Sex Male Female
3156 2111
564 (18) 379 (18)
1.0 1.0 (0.9-1.2)
-
Phase of treatment First LP Pre-Maintenance Maintenance
264 2621 2382
52 (20) 514 (20) 377 (16)
1.0 1.0 (0.7-1.4) 0.8 (0.6-1.1)
-
Platelets 0-50 51-75 76-100 >100
59 216 222 4770
13 (22) 57 (26) 61 (28) 812 (17)
1.4 (0.7-2.6) 1.8 (1.3-2.4) 1.9 (1.4-2.5) 1.0
1.26 (0.67-2.39) 1.47 (1.04-2.01) 1.48 (1.08-2.05) 1.0
Operator Fellow Staff Oncologist Radiologist
3146 1874 233
574 (18) 292 (16) 75 (32)
1.0 0.8 (0.71-0.97) 2.1 (1.6-2.8)
-
Days since previous LP 0-3 4-7 8-15 ≥16
29 866 431 3941
15 (52) 188 (22) 96 (22) 644 (16)
5.5 (2.6-11.4) 1.4 (1.2-1.7) 1.5 (1.2-1.9) 1.0
5.18 (2.38-11.27) 1.35 (1.08-1.68) 1.33 (1.01-1.74) 1.0
Platelets at previous LP 0-50 51-75 76-100 >100
56 209 219 4783
16 (29) 53 (25) 57 (26) 817 (17)
1.9 (1.1-3.5) 1.7 (1.2-2.3) 1.7 (1.3-2.3) 1.0
-
Previous TLP Yes No
931 4336
250 (27) 693 (16)
1.9 (1.6-2.3) 1.0
1.62 (1.36-1.93) 1.0
Recent anticoagulation None Prophylactic dose Treatment dose
5043 88 98
906 (18) 13 (15) 21 (21)
1.0 0.79 (0.44-1.43) 1.25 (0.77-2.03)
-
Coagulation Tests Normal Abnormal (INR>1.3, PTT>40)
735 58
164 (22) 14 (24)
1.0 1.11 (0.59-2.07)
-
White Blood Cell 0-50 >50
225 38
44 (20) 8 (21)
1.0 1.10 (0.48-2.56)
-
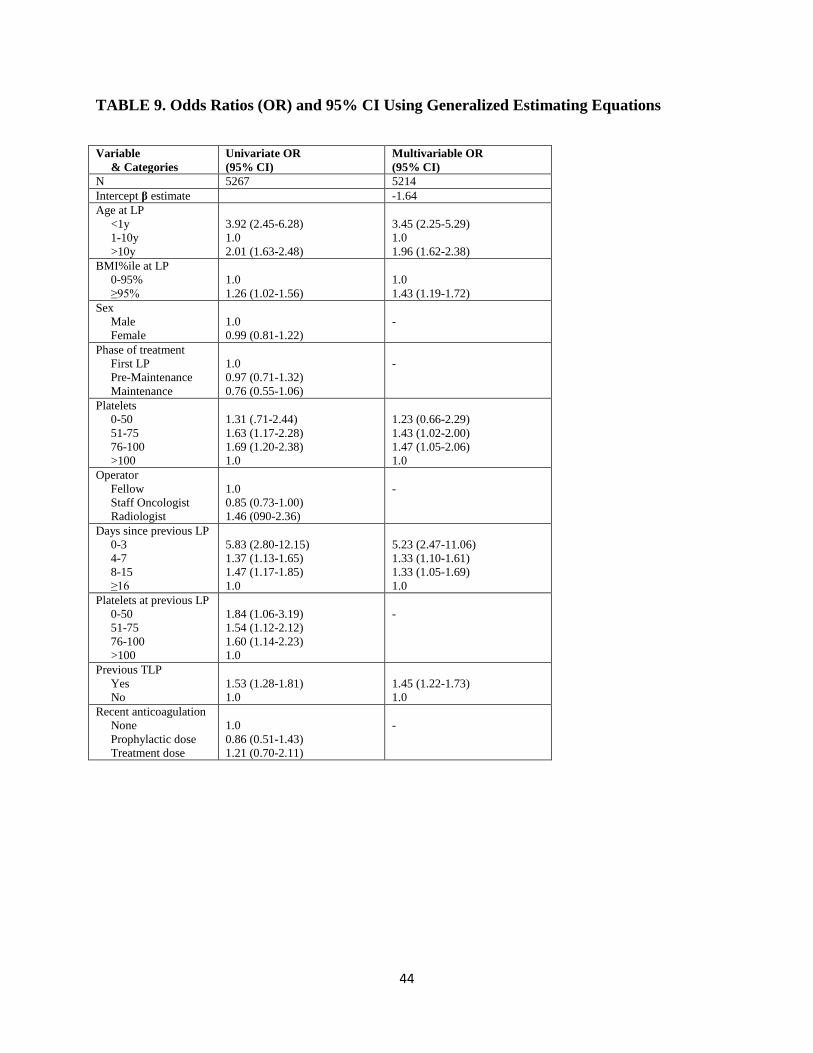
44
TABLE 9. Odds Ratios (OR) and 95% CI Using Generalized Estimating Equations
Variable & Categories
Univariate OR (95% CI)
Multivariable OR (95% CI)
N 5267 5214 Intercept β estimate -1.64 Age at LP <1y 1-10y >10y
3.92 (2.45-6.28) 1.0 2.01 (1.63-2.48)
3.45 (2.25-5.29) 1.0 1.96 (1.62-2.38)
BMI%ile at LP 0-95% ≥95%
1.0 1.26 (1.02-1.56)
1.0 1.43 (1.19-1.72)
Sex Male Female
1.0 0.99 (0.81-1.22)
-
Phase of treatment First LP Pre-Maintenance Maintenance
1.0 0.97 (0.71-1.32) 0.76 (0.55-1.06)
-
Platelets 0-50 51-75 76-100 >100
1.31 (.71-2.44) 1.63 (1.17-2.28) 1.69 (1.20-2.38) 1.0
1.23 (0.66-2.29) 1.43 (1.02-2.00) 1.47 (1.05-2.06) 1.0
Operator Fellow Staff Oncologist Radiologist
1.0 0.85 (0.73-1.00) 1.46 (090-2.36)
-
Days since previous LP 0-3 4-7 8-15 ≥16
5.83 (2.80-12.15) 1.37 (1.13-1.65) 1.47 (1.17-1.85) 1.0
5.23 (2.47-11.06) 1.33 (1.10-1.61) 1.33 (1.05-1.69) 1.0
Platelets at previous LP 0-50 51-75 76-100 >100
1.84 (1.06-3.19) 1.54 (1.12-2.12) 1.60 (1.14-2.23) 1.0
-
Previous TLP Yes No
1.53 (1.28-1.81) 1.0
1.45 (1.22-1.73) 1.0
Recent anticoagulation None Prophylactic dose Treatment dose
1.0 0.86 (0.51-1.43) 1.21 (0.70-2.11)
-

45
TABLE 10. Odds Ratios (OR) and 95% CI Using Random Effects with Generalized Linear
Mixed Models
Variable & Categories
Univariate OR (95% CI)
Multivariable OR (95% CI)
N 5267 5266 Intercept β estimate -1.70 Age at LP <1y 1-10y >10y
4.01 (2.32-6.95) 1.0 2.05 (1.68-2.51)
3.46 (2.06-5.81) 1.0 2.00 (1.66-2.4)
BMI%ile at LP 0-95% ≥95%
1.0 1.28 (1.04-1.58)
1.0 1.44 (1.19-1.75)
Sex Male Female
1.0 0.99 (0.81-1.22)
-
Phase of treatment First LP Pre-Maintenance Maintenance
1.0 0.98 (0.71-1.36) 0.76 (0.55-1.06)
-
Platelets 0-50 51-75 76-100 >100
1.27 (0.66-2.43) 1.65 (1.19-2.29) 1.73 (1.26-2.39) 1.0
1.15 (0.60-2.20) 1.42 (1.01-1.98) 1.49 (1.08-2.07) 1.0
Operator Fellow Staff Oncologist Radiologist
1.0 0.85 (0.72-0.99) 1.39 (0.94-2.08)
-
Days since previous LP 0-3 4-7 8-15 ≥16
6.25 (2.84-13.78) 1.40 (1.16-1.69) 1.46 (1.14-1.89) 1.0
5.13 (2.34-11.25) 1.35 (1.11-1.63) 1.31 (1.02-1.70) 1.0
Platelets at previous LP 0-50 51-75 76-100 >100
1.86 (1.00-3.44) 1.56 (1.11-2.18) 1.59 (1.14-2.21) 1.0
-
Previous TLP Yes No
1.52 (1.27-1.83) 1.0
1.43 (1.19-1.73) 1.0
Recent anticoagulation None Prophylactic dose Treatment dose
1.0 0.83 (0.42-1.66) 1.21 (0.68-2.17)
-
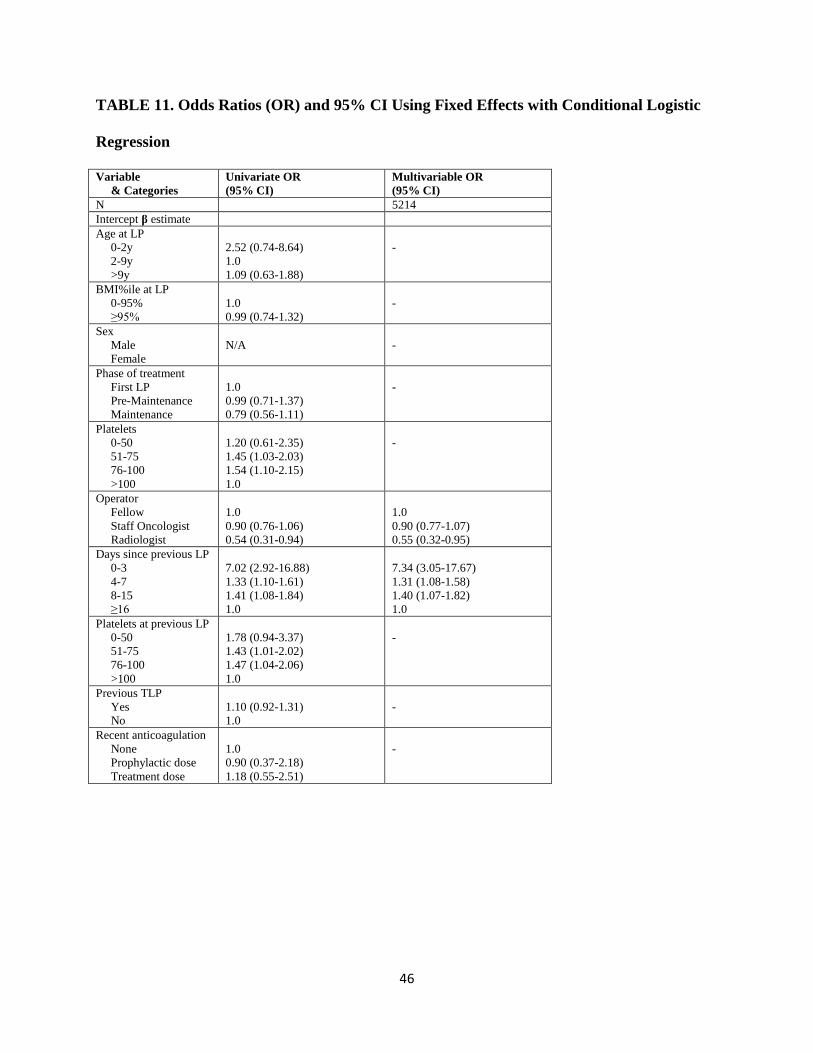
46
TABLE 11. Odds Ratios (OR) and 95% CI Using Fixed Effects with Conditional Logistic
Regression
Variable & Categories
Univariate OR (95% CI)
Multivariable OR (95% CI)
N 5214 Intercept β estimate Age at LP 0-2y 2-9y >9y
2.52 (0.74-8.64) 1.0 1.09 (0.63-1.88)
-
BMI%ile at LP 0-95% ≥95%
1.0 0.99 (0.74-1.32)
-
Sex Male Female
N/A
-
Phase of treatment First LP Pre-Maintenance Maintenance
1.0 0.99 (0.71-1.37) 0.79 (0.56-1.11)
-
Platelets 0-50 51-75 76-100 >100
1.20 (0.61-2.35) 1.45 (1.03-2.03) 1.54 (1.10-2.15) 1.0
-
Operator Fellow Staff Oncologist Radiologist
1.0 0.90 (0.76-1.06) 0.54 (0.31-0.94)
1.0 0.90 (0.77-1.07) 0.55 (0.32-0.95)
Days since previous LP 0-3 4-7 8-15 ≥16
7.02 (2.92-16.88) 1.33 (1.10-1.61) 1.41 (1.08-1.84) 1.0
7.34 (3.05-17.67) 1.31 (1.08-1.58) 1.40 (1.07-1.82) 1.0
Platelets at previous LP 0-50 51-75 76-100 >100
1.78 (0.94-3.37) 1.43 (1.01-2.02) 1.47 (1.04-2.06) 1.0
-
Previous TLP Yes No
1.10 (0.92-1.31) 1.0
-
Recent anticoagulation None Prophylactic dose Treatment dose
1.0 0.90 (0.37-2.18) 1.18 (0.55-2.51)
-

47
TABLE 12. Odds Ratios (OR) and 95% CI Using The Hybrid Method
Variable & Categories
Multivariable OR (95% CI)
N 5249 Intercept β estimate -1.68 Age at LP <1y 1-10y >10y
3.48 (2.10-5.77) 1.0 1.80 (1.49-2.18)
BMI%ile at LP 0-95% ≥95%
1.0 1.35 (1.11-1.63)
Sex Male Female
-
Phase of treatment First LP Pre-Maintenance Maintenance
-
Platelets 0-50 51-75 76-100 >100
1.13 (0.59-2.18) 1.38 (0.99-1.94) 1.43 (1.03-1.98) 1.0
Operator (Oncologist vs Radiologist) Fixed Effects Random Effects
0.56 (0.33-0.96) 2.19 (1.38-3.47)
Days since previous LP 0-3 4-7 8-15 ≥16
5.19 (2.38-11.36) 1.32 (1.09-1.60) 1.32 (1.02-1.71) 1.0
Platelets at previous LP 0-50 51-75 76-100 >100
-
Previous TLP Yes No
1.44 (1.19-1.73) 1.0
Recent anticoagulation None Prophylactic dose Treatment dose
-
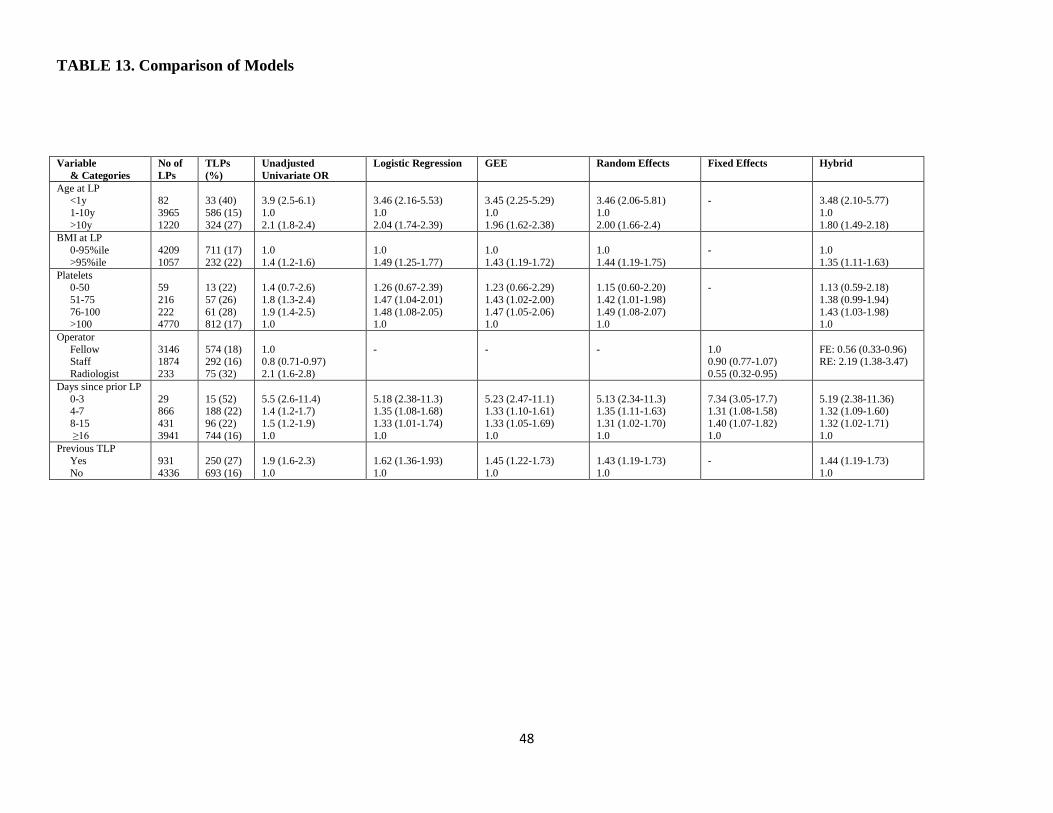
48
TABLE 13. Comparison of Models
Variable & Categories
No of LPs
TLPs (%)
Unadjusted Univariate OR
Logistic Regression GEE Random Effects Fixed Effects Hybrid
Age at LP <1y 1-10y >10y
82 3965 1220
33 (40) 586 (15) 324 (27)
3.9 (2.5-6.1) 1.0 2.1 (1.8-2.4)
3.46 (2.16-5.53) 1.0 2.04 (1.74-2.39)
3.45 (2.25-5.29) 1.0 1.96 (1.62-2.38)
3.46 (2.06-5.81) 1.0 2.00 (1.66-2.4)
-
3.48 (2.10-5.77) 1.0 1.80 (1.49-2.18)
BMI at LP 0-95%ile >95%ile
4209 1057
711 (17) 232 (22)
1.0 1.4 (1.2-1.6)
1.0 1.49 (1.25-1.77)
1.0 1.43 (1.19-1.72)
1.0 1.44 (1.19-1.75)
-
1.0 1.35 (1.11-1.63)
Platelets 0-50 51-75 76-100 >100
59 216 222 4770
13 (22) 57 (26) 61 (28) 812 (17)
1.4 (0.7-2.6) 1.8 (1.3-2.4) 1.9 (1.4-2.5) 1.0
1.26 (0.67-2.39) 1.47 (1.04-2.01) 1.48 (1.08-2.05) 1.0
1.23 (0.66-2.29) 1.43 (1.02-2.00) 1.47 (1.05-2.06) 1.0
1.15 (0.60-2.20) 1.42 (1.01-1.98) 1.49 (1.08-2.07) 1.0
-
1.13 (0.59-2.18) 1.38 (0.99-1.94) 1.43 (1.03-1.98) 1.0
Operator Fellow Staff Radiologist
3146 1874 233
574 (18) 292 (16) 75 (32)
1.0 0.8 (0.71-0.97) 2.1 (1.6-2.8)
-
-
-
1.0 0.90 (0.77-1.07) 0.55 (0.32-0.95)
FE: 0.56 (0.33-0.96) RE: 2.19 (1.38-3.47)
Days since prior LP 0-3 4-7 8-15 ≥16
29 866 431 3941
15 (52) 188 (22) 96 (22) 744 (16)
5.5 (2.6-11.4) 1.4 (1.2-1.7) 1.5 (1.2-1.9) 1.0
5.18 (2.38-11.3) 1.35 (1.08-1.68) 1.33 (1.01-1.74) 1.0
5.23 (2.47-11.1) 1.33 (1.10-1.61) 1.33 (1.05-1.69) 1.0
5.13 (2.34-11.3) 1.35 (1.11-1.63) 1.31 (1.02-1.70) 1.0
7.34 (3.05-17.7) 1.31 (1.08-1.58) 1.40 (1.07-1.82) 1.0
5.19 (2.38-11.36) 1.32 (1.09-1.60) 1.32 (1.02-1.71) 1.0
Previous TLP Yes No
931 4336
250 (27) 693 (16)
1.9 (1.6-2.3) 1.0
1.62 (1.36-1.93) 1.0
1.45 (1.22-1.73) 1.0
1.43 (1.19-1.73) 1.0
-
1.44 (1.19-1.73) 1.0

49
3.2.3 Secondary Outcome: Event-Free Survival
The mean length of follow-up was 3.9 years (SD 1.6 years). For 188 children with CNS1
status, the 5-year EFS was 93% (SE±2). For 26 children with TLP+ status, the 5-year EFS was
77% (±8). The difference between these two groups was statistically significant (Log-rank p=
0.002). Kaplan-Meier survival curves are shown in Figure 4.
FIGURE 4. Kaplan-Meier survival curves by CNS status

50
CHAPTER 4: DISCUSSION
4.1 Summary of Main Findings
In our retrospective cohort study of 5267 LPs, we observed an overall TLP rate of 17.9%
and a first TLP rate of 19.7%. In terms of identifying predictors of TLP, we found that among
the random effects model and GEE, the variables independently associated with TLP were age
less than 1 or over 10 years, BMI percentile over 95, platelet count less than 100 x103/µL, fewer
days since the previous LP, and a previous TLP. However, in the fixed effects model, the
variables independently associated with TLP were fewer days since the previous LP, and the use
of image-guidance by a radiologist.
The overall proportion of TLPs in our study is lower than that reported by Howard et al
(29.3%).34 This is likely due to the fact that Howard et al included only the first few LPs per
child, and therefore had a greater proportion of LPs in the intensive phases of treatment where
LPs are performed closer together. It may also be related to the study being conducted during an
era when procedural sedation was not routinely used, and when junior trainees such as medical
students and residents also performed LPs on children with ALL. Nevertheless, given the
significant consequences of TLPs in ALL, we believe that our proportion of TLPs is still high
and that further attempts at minimizing this complication are still needed.
4.2 Factors Predictors of TLP
The proportion of TLP was higher among infants than children 1-<10 years of age in our
study. This may be due to the technical challenges of performing the procedure within a smaller

51
anatomic space. Due to the shallower distances between the subarachnoid space and the posterior
venous plexus, the infant spine offers a narrower margin of error. Thus even small
miscalculations in estimating distance or angle of needle insertion, coupled with the larger
relative size of the LP needle to the anatomic structures, may increase the chance of blood vessel
laceration. The proportion of TLP was also significantly higher among children older than 10
years compared to those between 1-10 years of age. A different set of technical challenges
probably account for this observation. As children grow older and larger, the distance between
the skin and the spinous processes increases, which makes the spinous processes and thus the
optimal site of needle insertion more difficult to visualize and palpate. With increased distance,
any deviation from the ideal angle at the skin puncture site becomes amplified. Lastly, older
children often require longer needles which are more technically challenging to use. Longer
needles can curve or bend on insertion and are therefore harder to direct in a straight trajectory.
Obesity was also significantly associated with TLP. The reasons for this may be similar
as for older age. Procedure landmarks are harder to palpate in the presence of obesity, and needle
distances are greater. Shah et al found that being unable to visualize (let alone palpate) the
spinous processes for adults in the emergency room was a risk factor for traumatic LPs.40 This
variable was not assessed by Howard et al.34
Age and obesity are both patient-related factors. They are not modifiable at the time of
the LP. However, they are useful as predictor variables in that they can identify those subsets of
patients with a higher risk of TLP. Such risk-stratification would be important to allow directing
interventions to reduce TLP to those patients who are most likely to benefit.
A lower platelet count before the LP was a modifiable risk factor, as children with
thrombocytopenia can be given a platelet transfusion prior to their procedure. We found that the

52
risk of a TLP is significantly associated with all platelet counts under 100 x 103/µL.
Interestingly, patients in all categories with platelet counts less than 100 x 103/µL had an
increased risk, and the risk was not substantially different across the categories below this
threshold. These results are remarkably similar to those identified by Howard et al. The authors
of that study recommended that “in those settings in which traumatic LP is particularly
undesirable and the benefit of transfusion outweighs the disadvantages, such as the diagnostic LP
in a child with ALL and circulating leukemic cells, platelet transfusion for a count of 100 x
103/µL or lower is warranted.”34 Therefore, at SJCRH all children with newly diagnosed ALL
are transfused if their platelet count is below this threshold prior to their first LP.61 Our findings
support this practice. This same threshold was not included as a recommendation in a recent
Canadian platelet transfusion guideline for pediatric cancer patients.62
The proportion of TLPs was significantly higher when a prior LP was performed within
the preceding 15 days, and also if the prior LP was itself traumatic. Both these variables can be
regarded as “lag” variables. Although they are not themselves clinically useful, they are
important to include as potential confounders in a repeated-measures study. By adjusting for
them within the multivariable model, the results obtained from sequential LPs can be more
meaningfully applied to understanding predictors of TLPs.
4.3 Pertinent Negative Findings
In addition to these five identified risk factors, there were two pertinent negative findings
of our study worth highlighting.
First, although TLP rates varied widely among different operators, we found no
significant difference in the rate of TLPs between oncology fellows and staff. Therefore, rather

53
than restrict fellows from performing first LPs, institutions should consider identifying their best
performers within all positions who can be called upon to perform first LPs, especially in
children with higher risk of TLP.
Secondly, our study is the first to look for an association between the use of recent
anticoagulation therapy and the proportion of TLPs. No significant association was found. This
result is important because approximately 5% of all children with ALL will experience a
thrombotic event requiring anticoagulation with either heparin or LMWH.63 Large bleeds within
the spinal canal, known as spinal hematomas, are a rare but devastating complication of LPs that
can lead to paraplegia or death.64,65 Consequently, at SickKids, our institutional practice is to
hold unfractionated heparin for 4 hours and LMWH for 24 hours prior to an LP without requiring
coagulation testing. Our results suggest that this practice is sufficient to prevent even
microscopic bleeding.
4.4 Survival Analysis
Consistent with previous studies,22-24 we found a significant reduction in EFS for children
with TLP+ compared to those who had CNS1 status. This shows that TLP+ continues to be a
prognostic factor even in the context of contemporary therapy with additional treatments given to
these children. This lends further importance to the need to reduce first TLPs to as low as
possible in children with ALL.
4.5 Comparison of Repeated-Measures Analysis Methods
The five risk factors highlighted above were all identified as being the most significant
factors in models fitted using either conventional logistic regression, GEE or random effects

54
mixed models. Indeed, both the effect estimates and the confidence intervals produced by each of
these methods were very similar across all covariates. The similarity of findings across the
different regression methods means that our results are robust to the choice of statistical method.
It also suggests that within-patient correlations and unobserved heterogeneity were not
significant factors within this dataset.
In going from a model that incorrectly ignored dependence among individuals to those
that accounted for it, no substantial change in results was seen. Generally speaking, regression
models that ignore correlation tend to overestimate the standard errors of time-varying
covariates, while the effect on the size of the coefficient estimates is less pronounced.50,55 While
the confidence intervals may be slightly wider for the conventional logistic regression model
compared to GEE in our study, the differences are very subtle. This might suggest that residual
intra-individual correlation was not a strong factor in this setting. Lastly, it may perhaps imply
that TLP risk does not tend on average to cluster within individuals, and hence that there is either
not much variation in TLP risk between individuals and/or that most variation in TLP proportion
is for reasons extrinsic to the individual.
The effect estimates and CIs produced by GEE and random effects were again equivalent.
This reinforces the similarities between these two models in spite of the very different underlying
estimation methods.46 We did not observe any heterogeneity shrinkage in the GEE model relative
to the random effects model, which suggests that unobserved heterogeneity was minimal. Indeed,
the GEE estimates tended to be slightly smaller than the corresponding random effects estimates
in univariate analysis, but more similar in multivariable analysis as the unobserved heterogeneity
was reduced by the addition of covariates. However, this again leads us to conclude that

55
variation in subject-specific effects is small. Indeed, while TLP proportion between individuals
does vary, it tends to do so mainly within the range of 10% to 30%.
In contrast, the fixed effects model led to very different results. As might have been
expected, no significant association for age at LP or BMI percentile was seen. This is because
these variables do not change much over the course of 3 years of observation, especially when
they are categorized at cut-points. They in effect behaved as time-invariant variables when
restricted to just one individual. The number of days since prior LP remained a strong predictor,
but had much larger confidence intervals, as would be expected. Since fixed effects discards data
for any patient whose outcome variable does not change across predictor categories, it makes
inefficient use of the data and thus works with effectively smaller sample sizes.
Furthermore, in the fixed effects method one additional factor was noted to be significant:
the use of fluoroscopic image-guidance by an interventional radiologist. In our cohort, 27
children underwent 233 LPs under fluoroscopy. These were all children who were referred to the
interventional radiologist by the patient’s oncology team after either failed or repeatedly difficult
LPs. Moreover, these procedures often occurred within a few days after a prior LP attempt. One
would therefore expect to see susceptibility bias and/or confounding-by-indication in this group
of children. Indeed, it is instructive to observe how the estimated effect of this variable changed
across the different analytic methods. In unadjusted analysis, the image-guided LPs were
traumatic twice as often as all other LPs, with an overall rate of 32% and an OR of 2.1. In
univariate GEE adjusting only for correlations, the OR declined to 1.39 and lost statistical
significance. It further declined to 1.16 in multivariable GEE accounting for all other significant
covariates, likely due mostly to the added adjustment for days since prior LP (data not shown).
Lastly, in the fixed effects analysis, the effect of image-guidance reversed direction and was seen
56
to be significantly protective against TLP, with an OR of 0.55. The fixed effects method balances
unobserved but stable covariates and uses each patient as their own control.48 This suggests that
among the small group of patients selected for a referral to image-guidance, there is an intrinsic
but un-measured variable that predisposes them to a higher rate of TLP. Within these patients,
the use of image-guidance can reduce the risk of TLP.
After comparing the strengths and limitations of all models, we selected the GEE model
for final presentation. The differences between GEE and the random effects model are minimal,
and we based our decision on the fact that we are most interested in population-averaged rather
than subject-specific effects. The population-averaged coefficients allow users to estimate the
average change in the proportion of the outcome if modification of a risk factor was applied
across all patients.50
4.6 Study Limitations
Our study had several limitations. As a retrospective study, recording of covariates was
limited to those which were documented as part of routine clinical care. Therefore, several
potential predictor variables could not be assessed. For example, we could not assess the
potential impact of depth of anesthesia or degree of patient movement, the positioning of the
patient during the procedure, the width or length of needle used for the LP, or particular operator
practices such as removing the stylet. However, these particular variables would not be expected
to vary much within our cohort, as most procedures are performed within consistent parameters.
Unlike Shah et al,40 we could not assess whether operators were able to visualize or palpate the
spinous landmarks or whether this variable correlated with obesity. Furthermore, unlike Glatstein
57
et al,41 we could not assess whether multiple attempts increased the risk of TLP, as operators did
not document their number of attempts except in rare cases.
As with all non-experimental research, it is always possible that other important
explanatory variables were omitted as a result of not having been considered at all. Indeed, the
results of our fixed effects analysis on image-guidance does strongly suggest that some
unmeasured variable(s) accounts for a high proportion of TLP in at least a subgroup of children.
Lastly, a limitation of our study is that SickKids is a large tertiary-care referral center.
Therefore our results may not be generalizable to smaller or non-academic centers.
4.7 Study Strengths
A strength of our study is its large sample size. Furthermore, those covariates which were
included for the study had very low rates of missing data. Since nearly all LPs for childhood
cancer patients at SickKids are performed under deep sedation, documentation for procedures is
generally of a high quality. Only 47 (0.9%) LPs had missing outcome data (no CSF RBC count)
and only another 53 LPs (1.0%) had data missing on covariate values for the final model.
Another strength of this study was our use and comparison of multiple regression
methods for repeated-measures, which allowed us to gain better insights into the data and present
the most suitable multivariable model. Since results were consistent across all models that
performed within-person comparisons, the results of our analysis were robust to the choice of
method.
Our study had broad inclusion criteria and included all LPs for all children with any type
of ALL. Therefore, the study results should be generalizable to other large pediatric oncology

58
institutions where the routine practices regarding deep sedation and operator experience are
similar to ours.
4.8 Future Research
The findings from this study provide a foundation for future research. Image-guidance
may have the potential to reduce TLPs in children with particular susceptibility, and this
hypothesis should be further investigated. We are currently planning a study to determine
whether ultrasound-guidance performed in the oncology procedure room can reduce the
proportion of TLPs. Another future direction could be to determine prospectively whether
implementation of the clinical recommendations from this study, such as platelet transfusion
thresholds, identification of selected operators for first LPs, and/or image-guidance, are able to
reduce the proportion of first TLPs over time.
Lastly, the dataset in this study led to similar conclusions regardless of whether
conventional logistic regression, random effects, or GEE was used, and thus the relative
strengths and weaknesses of each method were not specifically highlighted. Future research
could therefore utilize simulations with varying degrees of intra-individual correlation and
unobserved heterogeneity in order to determine the relative strengths, bias, and efficiency of
each method under specific conditions. This could provide further guidance to researchers on
which method to use under different circumstances.
59
REFERENCES
1. SEER Cancer Statistics Review, 1975-2008, National Cancer Institute., 2011. (Accessed 2011, at http://seer.cancer.gov?csr/1975_2008/.) 2. Pui CH, Thiel E, Pui C-H, Thiel E. Central nervous system disease in hematologic malignancies: historical perspective and practical applications. Semin Oncol 2009;36:S2-S16. 3. Pui C-H, Howard SC. Current management and challenges of malignant disease in the CNS in paediatric leukaemia. Lancet Oncol 2008;9:257-68. 4. Hvizdala E, Berry DH, Chen T, et al. Impact of the timing of triple intrathecal therapy on remission induction in childhood acute lymphoblastic leukemia: a Pediatric Oncology Group study. Med Pediatr Oncol 1984;12:173-7. 5. Pullen J, Boyett J, Shuster J, et al. Extended triple intrathecal chemotherapy trial for prevention of CNS relapse in good-risk and poor-risk patients with B-progenitor acute lymphoblastic leukemia: a Pediatric Oncology Group study. J Clin Oncol 1993;11:839-49. 6. Iacoangeli M, Roselli R, Pagano L, et al. Intrathecal chemotherapy for treatment of overt meningeal leukemia: comparison between intraventricular and traditional intralumbar route. Ann Oncol 1995;6:377-82. 7. Moghrabi A, Levy DE, Asselin B, et al. Results of the Dana-Farber Cancer Institute ALL Consortium Protocol 95-01 for children with acute lymphoblastic leukemia. Blood 2007;109:896-904. 8. Cherlow JM, Sather H, Steinherz P, et al. Craniospinal irradiation for acute lymphoblastic leukemia with central nervous system disease at diagnosis: a report from the Children's Cancer Group. Int J Radiat Oncol Biol Phys 1996;36:19-27. 9. Pui CH. Central nervous system disease in acute lymphoblastic leukemia: Prophylaxis and treatment. Hematology 2006. 10. Meadows AT, Gordon J, Massari DJ, Littman P, Fergusson J, Moss K. Declines in IQ scores and cognitive dysfunctions in children with acute lymphocytic leukaemia treated with cranial irradiation. Lancet 1981;2:1015-8. 11. Uruena M, Stanhope R, Chessells JM, Leiper AD. Impaired pubertal growth in acute lymphoblastic leukaemia. Arch Dis Child 1991;66:1403-7. 12. MacLean WE, Jr., Noll RB, Stehbens JA, et al. Neuropsychological effects of cranial irradiation in young children with acute lymphoblastic leukemia 9 months after diagnosis. The Children's Cancer Group. Arch Neurol 1995;52:156-60. 13. Mahmoud HH, Rivera GK, Hancock ML, et al. Low leukocyte counts with blast cells in cerebrospinal fluid of children with newly diagnosed acute lymphoblastic leukemia. N Engl J Med 1993;329:314-9. 14. Children's Oncology Group. 2011. (Accessed December, 2011, at www.childrensoncologygroup.org.) 15. Schrappe M, Reiter A, Henze G, et al. Prevention of CNS recurrence in childhood ALL: results with reduced radiotherapy combined with CNS-directed chemotherapy in four consecutive ALL-BFM trials. Klin Padiatr 1998;210:192-9. 16. Practice parameters: lumbar puncture (summary statement). Report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology 1993;43:625-7.
60
17. Rech A, de Carvalho GP, Meneses CF, Hankins J, Howard S, Brunetto AL. The influence of traumatic lumbar puncture and timing of intrathecal therapy on outcome of pediatric acute lymphoblastic leukemia. Pediatr Hematol Oncol 2005;22:483-8. 18. Conter V, Arico M, Valsecchi MG, et al. Extended intrathecal methotrexate may replace cranial irradiation for prevention of CNS relapse in children with intermediate-risk acute lymphoblastic leukemia treated with Berlin-Frankfurt-Munster-based intensive chemotherapy. The Associazione Italiana di Ematologia ed Oncologia Pediatrica. J Clin Oncol 1995;13:2497-502. 19. Nachman J, Sather HN, Cherlow JM, et al. Response of children with high-risk acute lymphoblastic leukemia treated with and without cranial irradiation: a report from the Children's Cancer Group. J Clin Oncol 1998;16:920-30. 20. Pui CH, Campana D, Pei D, et al. Treating childhood acute lymphoblastic leukemia without cranial irradiation. N Engl J Med 2009;360:2730-41. 21. Pappano D. "Traumatic tap" proportion in pediatric lumbar puncture. Pediatric Emergency Care 2010;26:487-9. 22. Gajjar A, Harrison PL, Sandlund JT, et al. Traumatic lumbar puncture at diagnosis adversely affects outcome in childhood acute lymphoblastic leukemia. Blood 2000;96:3381-4. 23. Burger B, Zimmermann M, Mann G, et al. Diagnostic cerebrospinal fluid examination in children with acute lymphoblastic leukemia: significance of low leukocyte counts with blasts or traumatic lumbar puncture. J Clin Oncol 2003;21:184-8. 24. te Loo DM, Kamps WA, van der Does-van den Berg A, et al. Prognostic significance of blasts in the cerebrospinal fluid without pleiocytosis or a traumatic lumbar puncture in children with acute lymphoblastic leukemia: experience of the Dutch Childhood Oncology Group. J Clin Oncol 2006;24:2332-6. 25. Larson S, Schall G, Di Chrio G. The influence of previous lumbar puncture and pneumoencephalography on the incidence of unsuccessful radioisotope cisternography. Journal of Nuclear Medicine 1971;12. 26. Chordas C. Post-dural puncture headache and other complications after lumbar puncture. J Pediatr Oncol Nurs 2001;18:244-59. 27. Holdsworth MT, Raisch DW, Winter SS, et al. Pain and distress from bone marrow aspirations and lumbar punctures. Ann Pharmacother 2003;37:17-22. 28. Ebinger F, Kosel C, Pietz J, Rating D. Headache and backache after lumbar puncture in children and adolescents: A prospective study. Pediatrics 2004;113:1588-92. 29. Eskey CJ, Ogilvy CS. Fluoroscopy-guided lumbar puncture: Decreased frequency of traumatic tap and implications for the assessment of CT-negative acute subarachnoid hemorrhage. American Journal of Neuroradiology 2001;22:571-6. 30. Yu SD, Chen MY, Johnson AJ. Factors associated with traumatic fluoroscopy-guided lumbar punctures: a retrospective review. Ajnr: American Journal of Neuroradiology 2009;30:512-5. 31. Sidhu M, Coley B, Goske M, et al. Image Gently, Step Lightly: increasing radiation dose awareness in pediatric interventional radiology. Pediatric Radiology 2009;39:1135-8. 32. Chong AL, Grant R, Ahmed B, Thomas K, Connolly BL, Greenberg M. Imaging in pediatric patients: Time to think again about surveillance. Pediatr Blood Cancer 2010;55:407-13.

61
33. Miksys N, Gordon CL, Thomas K, Connolly BL. Estimating effective dose to pediatric patients undergoing interventional radiology procedures using Anthropomorphic Phantoms and MOSFET dosimeters. Am J Roentgenol 2010;194:1315-22. 34. Howard SC, Gajjar AJ, Cheng C, et al. Risk factors for traumatic and bloody lumbar puncture in children with acute lymphoblastic leukemia. Jama 2002;288:2001-7. 35. Shah K, Richard KM, Nicholas S, Edlow J. Incidence of traumatic lumbar puncture. Academic Emergency Medicine 2003;10:151-4. 36. Molina A, Fons J. Factors associated with lumbar puncture success. Pediatrics 2006;118:842-4; author reply 4. 37. Kaushal HS, Daniel M, Jeffrey S, Jonathan AE. Predicting difficult and traumatic lumbar punctures. The American journal of emergency medicine 2007;25:608-11. 38. Nigrovic L, Kuppermann N, Neuman M. Risk Factors for Traumatic or Unsuccessful Lumbar Punctures in Children. Annals of emergency medicine 2007;49:762-71. 39. Nigrovic LE, McQueen AA, Neuman MI. Lumbar Puncture Success Rate Is Not Influenced by Family-Member Presence. Pediatrics 2007;120:e777-82. 40. Shah K, McGillicuddy D, Spear J, Edlow J. Predicting difficult and traumatic lumbar punctures. The American journal of emergency medicine 2007;25:608-11. 41. Glatstein MM, Zucker-Toledano M, Arik A, Scolnik D, Oren A, Reif S. Incidence of traumatic lumbar puncture: experience of a large, tertiary care pediatric hospital. Clin Pediatr (Phila) 2011;50:1005-9. 42. Airhart A, Doyle J, Airhart C, Abla O, Alexander S. Assessment of pediatric haematology/oncology fellows' training in the performance of lumbar punctures [abstract]. Pediatr Blood Cancer 2009;52:721. 43. Ljungman G, Gordh T, Sorensen S, Kreuger A. Lumbar puncture in pediatric oncology: conscious sedation vs. general anesthesia. Med Pediatr Oncol 2001;36:372-9. 44. Gardiner JC, Luo Z, Roman LA. Fixed effects, random effects and GEE: What are the differences? Statistics In Medicine 2009;28:221-39. 45. Edwards LJ. Modern statistical techniques for the analysis of longitudinal data in biomedical research. Pediatric Pulmonology 2000;30:330-44. 46. Fitzmaurice GM, Laird NM, Ware JH. Applied Longitudinal Analysis. New Jersey: Wiley; 2011. 47. Singer JD, Willett JB. Applied Longitudinal Data Analysis: Modeling Change and Event Occurrence. Madison Avenue, New York: Oxford University Press, Inc; 2003. 48. Allison PD. Fixed Effects Regression Methods for Longitudinal Data: Using SAS. Cary, NC: SAS Institute Inc; 2005. 49. Lipsitz RS, Fitzmaurice GM. Sample size for repeated measures studies with binary responses. Statistics In Medicine 1994;13:1233-9. 50. Hu FB, Goldberg J, Hedeker D, Flay BR, Pentz MA. Comparison of population-averaged and subject-specific approaches for analyzing repeated binary outcomes. American Journal of Epidemiology 1998;147:694-703. 51. Locascio JJ, Atri A. An overview of longitudinal data analysis methods for neurological research. Dement Geriatr Cognitive Disorders Extra 2011;1:330-57.

62
52. Cheng J, Edwards LJ, Maldonado-Molina MM, Komro KA, Milluer KE. Real longitudinal data analysis for real people: Building a good enough mix model. Statistics In Medicine 2010;29:504-20. 53. Liang KY, zeger SL. Longitudinal data analysis using generalized linear models. Biometrika 1986;73:13-22. 54. Pan W. Akaike's information criterion in generalized estimating equations Biometrcs 2001;57:120-5. 55. Allison PD. Logistic Regression Using the SAS System: Theory and Application. . Cary NC: SAS Institute Inc.; 1999. 56. A SAS Program for the CDC Growth Charts. Centers for Disease Control and Prevention, 2011. (Accessed March 2012, at http://www.cdc.gov/nccdphp/dnpao/growthcharts/resources/sas.htm.) 57. Barlow SE. Expert committee recommendations regarding the prevention, assessment, and treatment of child and adolescent overweight and obesity: Summary report. Pediatrics 2007;120:S164-S92. 58. Peduzzi P, Concato J, Kemper E, Holford T, Feinstein A. A simulation study of the number of events per variable in logistic regression analysis. Journal of Clinical Epidemiology 1996;49:1373-9. 59. Concato J, Peduzzi P, Holford T, et al. Importance of events per independent variable in proportional hazards analysis. I. Background, goals, and general strategy. Journal of Clinical Epidemiology 1995;48:1495-501. 60. Allison PD. Survival Analysis Using SAS: A Pratcical Guide. Second ed. Cary NC: SAS Institute Inc; 2010. 61. Howard SC, Gajjar A, Ribeiro RC, et al. Safety of lumbar puncture for children with acute lymphoblastic leukemia and thrombocytopenia. Jama 2000;284:2222-4. 62. Guideline for platelet transfusion thresholds for pediatric hematology/oncology patients: Complete reference guide. The C17 Guidelines Committee, 2010. (Accessed March 2011, at http://www.c17.ca/index.php?cID=86.) 63. Caruso V, Iacoviello L, Di Castelnuovo A, et al. Thrombotic complications in childhood acute lymphoblastic leukemia: a meta-analysis of 17 prospective studies comprising 1752 pediatric patients. Blood 2006;108:2216-22. 64. Kreppel D, Antoniadis G, Seeling W. Spinal hematoma: a literature survey with meta-analysis of 613 patients. Neurosurgical Review 2003;26:1-49. 65. van Veen JJ, Nokes TJ, Makris M. The risk of spinal haematoma following neuraxial anaesthesia or lumbar puncture in thrombocytopenic individuals. British Journal of Haematology 2010;148:15-25.

63
APPENDICES
APPENDIX I. Approach to Classifying TLP+ Status Varies Between SJCRH and COG
Systems
In the SHCRH system, a TLP+ is defined as its own CNS group without further attempt to
distinguish the possible underlying status:
CNS1 Absence of blasts in CSF, and <10 RBC/µL
CNS2 <5 WBC/µL, <10 RBC/µL, blasts
CNS3 ≥5 WBC, <10 RBC/µL, blasts
TLP- Absence of blasts in CSF, and ≥10 RBC/µL
TLP+ ≥10 RBC/µL, blasts
In contrast, the COG system uses the following Steinherz/Bleyer algorithm for all patients with
TLP+ to try and distinguish between underlying CNS2 and CNS3 disease:
CSF WBC > 2X CSF RBC Blood RBC
Blood WBC
A patient whose CSF WBC/RBC is 2x greater than the blood WBC/RBC ratio is considered to
have CNS3 disease at diagnosis.

64
APPENDIX II. Risk Group Definitions for B-cell Precursor ALL
Risk Group Definition Standard Risk Age 1.0 to 9.99 years
WBC < 50,000/µL Standard risk-low Not CNS2 or CNS3 or testicular disease
Favourable genetics Day 8 peripheral blood MRD <0.01% Day 29 bone marrow MRD <0.01% No steroid pretreatment
Standard-risk average No unfavourable genetics Day 8 peripheral blood MRD ≥ 0.01% or CNS2 status Day 29 bone marrow MRD < 0.01% No CNS3 or testicular disease
High-Risk Age <1 or ≥10 years WBC ≥50,000/µL CNS3 or testicular disease Steroid pretreatment
Very High-Risk ALL BCR-ABL fusion Hypodiploidy Induction failure MLL rearrangement and slow-early response after induction