predicting perioperative mi: a revisit homer yang professor & chair department of anesthesia
TRANSCRIPT
Predicting Predicting Perioperative MI: Perioperative MI:
A RevisitA Revisit
Homer YangHomer YangProfessor & ChairProfessor & Chair
Department of AnesthesiaDepartment of Anesthesia

ObjectivesObjectives
• Is knowing the coronary anatomy preop Is knowing the coronary anatomy preop enough in predicting MI?enough in predicting MI?
• Preop Stratification & limitationsPreop Stratification & limitations• A “re-look”A “re-look”
– Identify population for majority of periop cardiac Identify population for majority of periop cardiac complicationscomplications
– Other factorsOther factors
Ellis et al. Am J Cardiol 1996; 77: 1126 - 28
Angiographic Correlates of Peri-op Cardiac Angiographic Correlates of Peri-op Cardiac Death & MIDeath & MI case-control studycase-control study between 1984 and 1991: aortic, femoral-between 1984 and 1991: aortic, femoral-
popliteal, and femoral-tibial surgerypopliteal, and femoral-tibial surgery between 1989 and 1991: carotid between 1989 and 1991: carotid
endarterectomyendarterectomy 1242 patients1242 patients 21 with pre-op angio + in-hospital death / MI21 with pre-op angio + in-hospital death / MI 1:2 ratio of control on basis of age, year, & Sx1:2 ratio of control on basis of age, year, & Sx

Ellis et al. Am J Cardiol 1996; 77: 1126 - 28
Angiographic Correlates of Peri-op Cardiac Angiographic Correlates of Peri-op Cardiac Death & MIDeath & MI
angiography performed a median of 6 days pre-opangiography performed a median of 6 days pre-op 14 / 21 had identifiable stenosis14 / 21 had identifiable stenosis
8 / 14 had inadequate collaterals8 / 14 had inadequate collaterals 0 / 14 had stenosis 70 - 99%0 / 14 had stenosis 70 - 99%
7 / 21 had no culprit sites7 / 21 had no culprit sites high grade stenosis may have pre-op CABG / PTCAhigh grade stenosis may have pre-op CABG / PTCA retrospective study without CPK or troponin assays retrospective study without CPK or troponin assays
(underestimation)(underestimation)
Can we predict MI?Can we predict MI?
• 70 - 80% of coronary thrombosis occur where 70 - 80% of coronary thrombosis occur where stenosis is previously insignificantstenosis is previously insignificant– Little et al. Circulation 1988; 78:1157 - 66Little et al. Circulation 1988; 78:1157 - 66– Webster et al. JACC 1990; 15:218AWebster et al. JACC 1990; 15:218A– Giroud et al. Am J Cardiol 1992; 69:729 - 32Giroud et al. Am J Cardiol 1992; 69:729 - 32

Davies MJ et al. Eur Heart J 1989; 10:203 - 8
Plaque Fissure in DM & HBP patientsPlaque Fissure in DM & HBP patients
• 168 test subjects who “died within 6 hrs of onset of 168 test subjects who “died within 6 hrs of onset of any symptoms in their last illness”any symptoms in their last illness”
• 129 controls who “died suddenly and in whom 129 controls who “died suddenly and in whom autopsy showed non-cardiac deaths”autopsy showed non-cardiac deaths”– 69 with an atheroma related disease69 with an atheroma related disease
• Cause of death: intracrebral hemorrhage, ruptured AAACause of death: intracrebral hemorrhage, ruptured AAA– 60 with no atheroma related disease60 with no atheroma related disease
• Cause of death: traffic accidents, suicideCause of death: traffic accidents, suicide

Davies MJ et al. Eur Heart J 1989; 10:203 - 8
• Test subjectsTest subjects– 19% had no new acute lesions19% had no new acute lesions– 7.7% plaque fissure7.7% plaque fissure– 43.5% mural thormbi but not occlusive43.5% mural thormbi but not occlusive– 29.8% occlusive thrombi29.8% occlusive thrombi
• Atheroma related deathsAtheroma related deaths– 16.7% plaque fissure16.7% plaque fissure– 5% mural thrombi5% mural thrombi
• Non-atheroma related deathsNon-atheroma related deaths– 8.7% plaque fissure8.7% plaque fissure
Plaque Fissure in DM & HBP patientsPlaque Fissure in DM & HBP patients

Dawood et al. Intern J Cardiol 1996; 57:37 - 44
• Periop MI (30 days postop) 42 vs Non-periop MI 25Periop MI (30 days postop) 42 vs Non-periop MI 25• Periop MI (42)Periop MI (42)
– Subendocardial MI 13 (31%)Subendocardial MI 13 (31%)
– Circumferential 3 (7%)Circumferential 3 (7%)
• Plaque rupture, plaque haemorrhage, & intraluminal thrombus Plaque rupture, plaque haemorrhage, & intraluminal thrombus (one or more) 23 (55%)(one or more) 23 (55%)
• 19 (45%) have no identifiable plaque rupture or intraluminal 19 (45%) have no identifiable plaque rupture or intraluminal thrombusthrombus
• Formation of thrombus at or in the immediate distal vicinity or Formation of thrombus at or in the immediate distal vicinity or atheroma was considered indirect evidence of plaque atheroma was considered indirect evidence of plaque disruption.disruption.
• ““Severity of preexisting underlying stenosis did not predict Severity of preexisting underlying stenosis did not predict the resulting infarct territory”the resulting infarct territory”
Fatal Periop MIFatal Periop MI

Circulation 2009; 119:2936-44

JACC 2007; 50(17):1707-32
Circulation 1999; 100:1043-9
Lee’s RCRILee’s RCRI
• In Validation CohortIn Validation Cohort• Class 1, 0 factors, 0.4% cardiac complicationsClass 1, 0 factors, 0.4% cardiac complications• Class 2, 1 factors, 0.9%Class 2, 1 factors, 0.9%• Class 3, 2 factors, 7%Class 3, 2 factors, 7%• Class 4, Class 4, ≥ 3 factors, 11%≥ 3 factors, 11%

Database ResultsDatabase Results
• HHSC Chart Audit 1996 – 1997 elective THR & TKRHHSC Chart Audit 1996 – 1997 elective THR & TKR– 679 charts679 charts– 38/49 (77.5%) cardiac complications in Detsky 0 or 538/49 (77.5%) cardiac complications in Detsky 0 or 5
• LHSC Referral ConsultsLHSC Referral Consults– 2035 patients2035 patients– 95/130 (73.0%) of MI, unstable angina, CHF, or death in 95/130 (73.0%) of MI, unstable angina, CHF, or death in
Detsky stratum 1Detsky stratum 1
• TOH 2002 – 2006 elective THR & TKRTOH 2002 – 2006 elective THR & TKR– 5158 patients in Data Warehouse5158 patients in Data Warehouse

Anesthesiology 2009; 111(4): 690-4
Effect of Effect of ββ-blockers in Postop Hip & Knee Replacements-blockers in Postop Hip & Knee Replacements
23 (5.0–106)14 (0.3%)2 (2.6%)Class IV
38 (19–75)63 (1.2%)15 (19.5%)Class III
10 (6.1–17)502 (9.9%)32 (41.6%)Class II
4502 (88.6%)28 (36.4%)Class I
ORNo POMI (n=5081)POMI (n=77)

Lindenauer et al. NEJM 2005; 353:349 - 61
Periop Periop ββ-blocker & mortality after major non-cardiac -blocker & mortality after major non-cardiac surgery (Propensity Analysis)surgery (Propensity Analysis)
• Retrospective cohort of patients undergoing major Retrospective cohort of patients undergoing major non-cardiac surgery in 329 hospitals in 2000 & 2001non-cardiac surgery in 329 hospitals in 2000 & 2001
• 782969 patients, 663635 without contraindications to 782969 patients, 663635 without contraindications to ββ-blockers-blockers
• 13454 mortality (2%)13454 mortality (2%)• Number of RCRI factorsNumber of RCRI factors
– 0: 3139690: 313969– 1: 769831: 76983– 3: 156553: 15655– ≥ ≥ 4: 14164: 1416

Lindenauer et al. NEJM 2005; 353:349 - 61
Perioperative MortalityPerioperative Mortality
541297(did not receive -blockers)
10771 (1.98%)
RCRI Factors ≤ 1 RCRI Factors ≥ 2
8443 (1.73%) 2328 (4.23%)
78% of all mortality 22 % of all mortality

Emergency SxEmergency Sx
• CRI: 4 pointsCRI: 4 points• Detsky’s: 10 pointsDetsky’s: 10 points• RCRI: only on elective SxRCRI: only on elective Sx• Ottawa Hospital Chart Audit 2003Ottawa Hospital Chart Audit 2003
– 88 perioperative MI or cardiac arrest88 perioperative MI or cardiac arrest– 42 after urgent or emergent surgery42 after urgent or emergent surgery

Anesthesiology 2009; 111(4): 690-4
Effect of Effect of ββ-blockers in Postop Hip & Knee Replacements-blockers in Postop Hip & Knee Replacements
• THR & TKR at The Ottawa Hospital (2002 – 2006)THR & TKR at The Ottawa Hospital (2002 – 2006)• On day of Sx:On day of Sx:
– I: I: ββ-blockers & continued during stay or until POD 7-blockers & continued during stay or until POD 7
– II: II: ββ-blockers but d/c during stay-blockers but d/c during stay
– III: No III: No ββ-blockers-blockers
• NN = 5158 patients; Mortality 54 (1.0%); POMI 77 (1.5%) = 5158 patients; Mortality 54 (1.0%); POMI 77 (1.5%)• Withdrawal of Withdrawal of ββ-blockers postop is associated with POMI [OR -blockers postop is associated with POMI [OR
10; 5.8 – 18]10; 5.8 – 18]• Postop Hb < 100 g/L associated with POMI [OR 3.5; 1.8 – 6.8]Postop Hb < 100 g/L associated with POMI [OR 3.5; 1.8 – 6.8]• Together, compound riskTogether, compound risk

Anesthesiology 2010; 112:25 - 33
Acute Surgical Anemia Influences the Acute Surgical Anemia Influences the Cardioprotective Effects of Cardioprotective Effects of ββ-Blockade-Blockade• Retrospective Review of Records between Mar 2005 – Jun Retrospective Review of Records between Mar 2005 – Jun
2006, 12006, 1° outcomes: MI, non-fatal CA, in-hospital death° outcomes: MI, non-fatal CA, in-hospital death• Nadir Hb – lowest Hb in first 3 days postopNadir Hb – lowest Hb in first 3 days postop• 1:1 Propensity Analysis with matching1:1 Propensity Analysis with matching• 4387 patients with nadir Hb4387 patients with nadir Hb
– 1153 (26%) received 1153 (26%) received ββ-blockers (BB) within 24 hr postop-blockers (BB) within 24 hr postop– Propensity matching in 827Propensity matching in 827– Major cardiac event 54 (6.5%) in BB & 25 (3.0%) in non-BB (RR Major cardiac event 54 (6.5%) in BB & 25 (3.0%) in non-BB (RR
2.38; CI 1.43 – 3.96, p = 0.0009)2.38; CI 1.43 – 3.96, p = 0.0009)– Hb drop > 35% Hb drop > 35%
• BB: RR 3.5; CI 1.8 – 5.5, p<0.0001BB: RR 3.5; CI 1.8 – 5.5, p<0.0001• Non-BB: RR 2.17; CI 0.97 – 4.86, p=0.0533Non-BB: RR 2.17; CI 0.97 – 4.86, p=0.0533
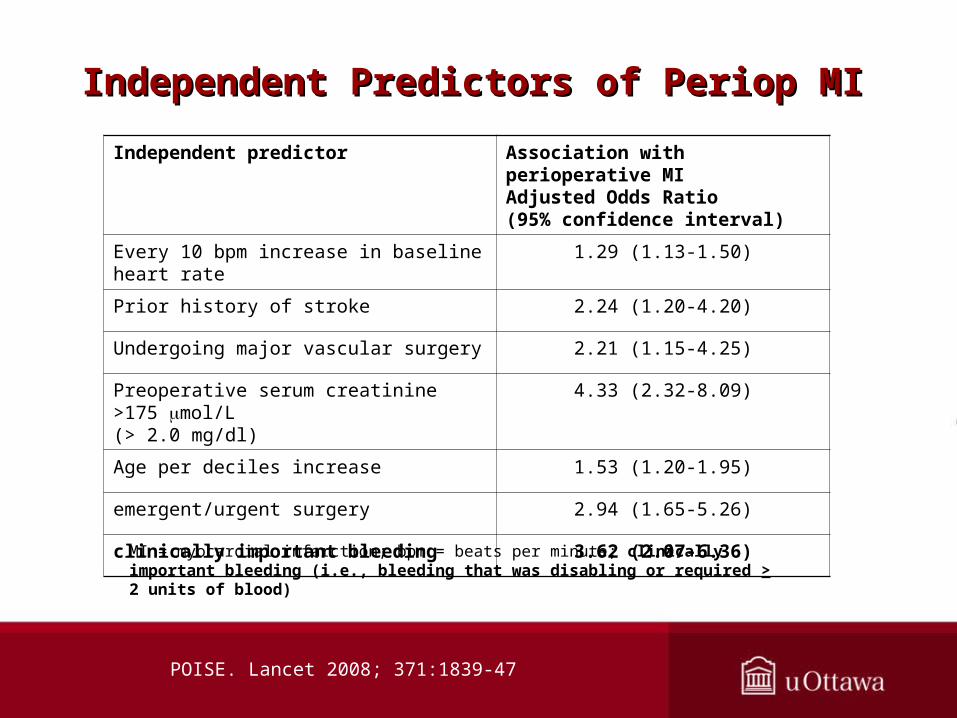
POISE. Lancet 2008; 371:1839-47
Independent Predictors of Periop MIIndependent Predictors of Periop MI
Independent predictor Association with perioperative MIAdjusted Odds Ratio(95% confidence interval)
Every 10 bpm increase in baseline heart rate 1.29 (1.13-1.50)
Prior history of stroke 2.24 (1.20-4.20)
Undergoing major vascular surgery 2.21 (1.15-4.25)
Preoperative serum creatinine >175 mol/L (> 2.0 mg/dl)
4.33 (2.32-8.09)
Age per deciles increase 1.53 (1.20-1.95)
emergent/urgent surgery 2.94 (1.65-5.26)
clinically important bleeding 3.62 (2.07-6.36)
MI = myocardial infarction; bpm = beats per minute; clinically important bleeding (i.e., bleeding that was disabling or required > 2 units of blood)
SummarySummary
• Most cardiac complications (& mortality) occur in Most cardiac complications (& mortality) occur in lower risk patients lower risk patients
• Most MIs do not occur at sites of previous highest Most MIs do not occur at sites of previous highest stenotic areas, in angio & in autopsy studiesstenotic areas, in angio & in autopsy studies– Approx 16% of plaque fissure occurring in asymptomatic Approx 16% of plaque fissure occurring in asymptomatic
patients as a “baseline”patients as a “baseline”
• Significant % of POMI due to Supply & DemandSignificant % of POMI due to Supply & Demand– 45% of periop cardiac deaths are not explained by 45% of periop cardiac deaths are not explained by
intraluminal or occlusive thrombi: supply & demandintraluminal or occlusive thrombi: supply & demand– At least 7 – 19% of periop MI on autopsy are circumferential At least 7 – 19% of periop MI on autopsy are circumferential
or multi-site (supply & demand)or multi-site (supply & demand)– Is supply & demand a postop problem?Is supply & demand a postop problem?

ConclusionConclusion
• Preop ACC / AHA guidelines appropriatePreop ACC / AHA guidelines appropriate• Diagnosing CAD does not equal predicting Diagnosing CAD does not equal predicting
perioperative cardiac eventsperioperative cardiac events• ““Low Risk” Patients are neglectedLow Risk” Patients are neglected• Factors to watch forFactors to watch for
– PostopPostop Hb Hb– Emergency casesEmergency cases
• Needs more research, especially in postop periodNeeds more research, especially in postop period

Winterlude 2012, Feb 4 – 5Winterlude 2012, Feb 4 – 5Ottawa, CanadaOttawa, Canada