practice teaching on pain management
TRANSCRIPT
pain it is management & theories
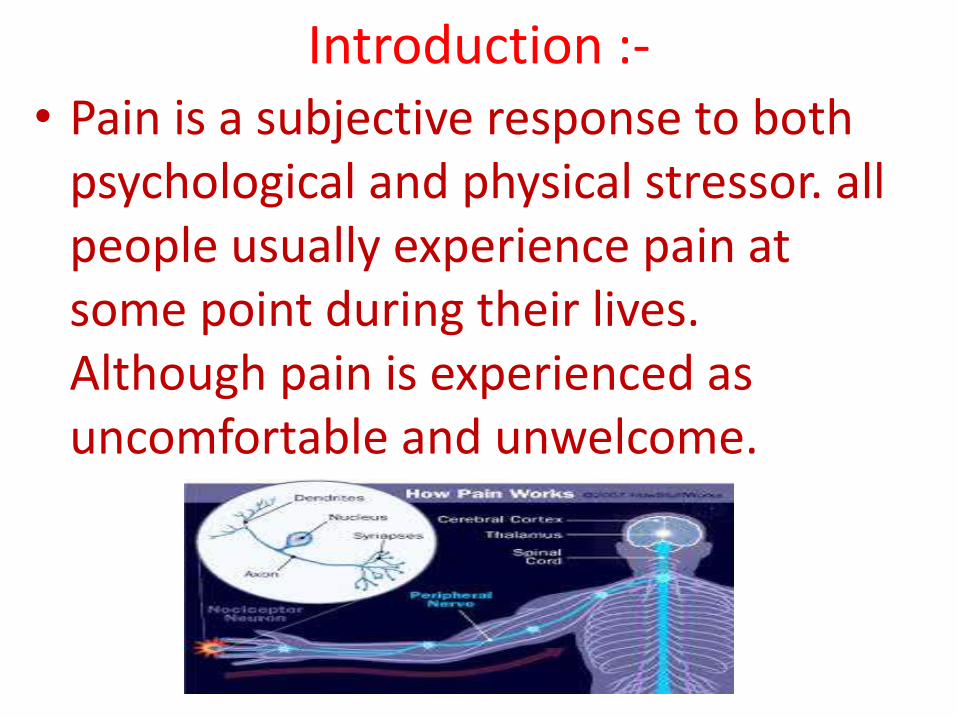
Introduction :-• Pain is a subjective response to both
psychological and physical stressor. all people usually experience pain at some point during their lives. Although pain is experienced as uncomfortable and unwelcome.

Definition :-
• pain is an, unpleasant sensory and emotional experience associated with actual or potential tissue damage.
• pain is a personal and subjective experience that can only be felt by the sufferer.

Types of pain:-• Acute pain:-Usually of recent onset and commonly
associated with a specific injury, acute pain indicates that damage or injury has occurred. Pain is significant in that it draws attention to its existence and teaches people to avoid similar potentially painful situations.
• Chronic pain:- chronic pain is constant or intermittent pain that persists beyond the expected healing time and that can seldom be attributed to a specific cause or injury.


Types of pain:-
• 1.Somatic pain:- caused by direct tumor involvement of sensory receptors in cutaneousand deep tissues.A. usually described as dull, sharp, aching, and throbbing. Usually constant and localized.
• 2.Neuropathic pain.A. Result from nerve injury or compression.B. includes phantom pain and postherpetic neuralgia.
• 3.Visceral pain.A. Usually described as deep, dull, aching, squeezing, or pressure sensation. It can be vague or ill-defined and can be referred to cutaneous site,


Other types of cancer related pain:-
• 1. NOCICEPTIVE PAIN:-This refers to pain resulting from stimulation of peripheral nerves through nociceptors. Pain impulses enter the spinal cord through the dorsal horn, where they ascend to higher centre’s in the brain. Inhibitory impulses block transmission.
• 1. Peripheral neuropathic pain.
Peripheral neuropathic pain is caused by damage within the peripheral nervous

Other types of pain conti..
• 2. Central neuropathic pain:-Central neuropathic pain is neuropathic pain caused by damage within the central nervous system. There is usually an area of altered sensation incorporating the area of pain. Cerebrovascular accident, or spinal cord damage.
• 3. Sympathetically maintained pain:Sympathetically maintained pain is due to sympathetic nerve injury. Essential features are pain (often burning) and sensory disorder related to a vascular as opposed to neural distribution.

Principles of pain management:-• 1.The goal of pain management is complete relief of
pain.
• 2.placebos are never indicated for the treatment of pain.
• 3.physical dependence and tolerance commonly occur, patient may require escalating doses of medications to control pain.
• 4.it is essential that physicians and nurses and do not confuse addiction with tolerance addiction is an unrelated medical disorder with behavioral components. These facts must also be stressed with patients who are reluctant to take medications.


Assessment of pain:-
• Assessment of a patient’s pain is a crucial skill, which requires a structured approach, actively listening ears and sharp eyes. Accurate assessment is also helped by experience, and is not a “one off” event, but constantly needs to be re-evaluated by the health care team as they gather more information and understanding.
Assessment questions:-
• There are many approaches to assessing pain, and each professional will develop his / her own approach to taking a pain history. Having a good assessment technique is the basis for prompt and appropriate management of a patient’s pain.

Pain History Principles:-
• 1. Seek to establish a relationship with the patient.
• 2. Encourage the patient to do most of the talking.
• 3. Begin with a wide-angle open question before clarifying and focusing with more specific ones.
• 4. Watch the patient for clues regarding pain.

Remember, as you are assessing the patient, he/she is assessing you
1. Eye to eye level contact.
2. Clear introduction.
3. Avoid over-familiarity.
4. Explain what you plan to do.
5. Summaries back to the patient, “Have I heard things correctly?“
6. Avoid patronizing.
7. Use language and terms appropriate to the patient.


Pain Assessment Scales:-• Explain to the person that each face is for a person
who feels happy because he has no pain (hurt) or sad because he has some or a lot of pain. Face 0 is very happy because he doesn’t hurt at all. Face 1 hurts just a little bit. Face 2 hurts a little more. Face 3 hurts even more. Face 4 hurts a whole lot. Face 5 hurts as much as you can image, although you don’t have to be crying to feel this bad.

Theories of pain1-The specificity theory.
This theory was based on the assumption that pain was perceived following injury because there was a single, dedicated, hard wired system of afferent nerves which carried messages from specific pain receptors in the periphery to a pain centre in the brain. The simple idea proposed that specific nerve endings in the skin and other tissues respond exclusively to nociceptive stimuli .

Theories of pain conti….
2- pattern theory.
This relate to the perception of pain to patterns of impulses in the nervous system rather than to impulses in dedicated pain pathways. The patterns may be temporal(in time) or spatial(in space). Pattern thepries may explain som chronic or recurrent pains which occur when there are nerve lesions.

Theories of painconti…...
3-The gait control theory.
In 1965, melzack and wall proposed the control pain theory, which was the first one recognizing the psychological aspects of pain are as important as physiological aspects. The gate control theory combined cognitive, sensory, and emotional components in addition to the physilogical aspects and proposed that they can act on a gate control system to block the individual’s perception of pain. The basic premise is that transmission of potentially painful nerve impulses to the cortex is modulated by spinal cord gating mechanism and by CNS activity. As a result, the level of conscious awareness of painful sensation is altered.

Theories of pain conti…..
• Neuromatrix theory
• A newer theory of pain that answered some of these questions. This new theory the neuromatrix theory. Stipulates that every human being has. An innate network of neurons that they named the body self neuromatrix, each persons matrix of neurons in unique and is affected by all facets of the persons physical, physiological and cognitive traits and also by their experience.

Theories of pain conti….
• Central baising theory.
This theory can explain the concept of learned behaviour, this theory builds on the gate theory(acting within the spinal cord) and addresses brain influence on incoming and outgoing messages. Cognitive effects can alter sensory discrimination, the location of the pain source. The pain (eg:referred pain)

Theories of painconti…….
• Endogenous opiates theory.
Least understood of all the theories simulation of A-delta & C fibers causes release of B-endorphins carried a ACTH/B- lipotropin is released from the anterior pituatry in response to pain- broken down into B- endorphins and corticosteroids mechanism of action- similar to enkephalms to block ascending nerve impulses transcutaneouselectrical nerve stimulation .(low frequency & long pulse duration)

PAIN MANAGEMENT:-• Pain is traditionally classified into different
modalities:- physical, psychosocial and spiritual. Exploring a patient‘s anxieties and frequent misconceptions related to these modalities can be very beneficial. Pain will not be adequately managed unless patients feel a degree of participation/control over their situation. To ignore such psychological aspects of care may often be the reason for persisting pain.

MANAGEMENT OF NOCICEPTIVE PAIN:-
• STEP 1 (Mild pain) Non-Opioid ± adjuvant.
Start treatment with paracetamol 500mg - 1g 6 hourly (q.d.s.) regularly. If step 1 medication are not adequate in 24 hours, proceed to step 2.
STEP 2 (Mild to moderate pain) Weak Opioid ± step one medication Start treatment with a combined preparation of paracetamol with dextropropoxyphene or codeine, or tramadol. Dextropropoxyphene is available in combination with paracetamol. total daily dose of 260mg .

Management of nonceptive pain conti…
• STEP 3 (Moderate to severe pain) Strong Opioid ±step onen medication If step two medication is inadequate consider starting oral morphine. For a patient taking 260mg dextropropoxyphene a day, a minimum of morphine 5mg four hourly/ six times a day, i.e. a daily total of 30mg of morphine is required.

ADJUVANTANALGESICS (CO-ANALGESICS) noncept….type……..conti.
• An adjuvant analgesic drug is a drug which is not an analgesic in its prime function but in combination with an analgesic can enhance pain control.
• 1.Secondary analgesics:
Corticosteroids - pain caused by oedema
Antidepressants - neuropathic pain.
Anticonvulsants - neuropathic pain.
Muscle relaxants- muscle cramps.
Antispasmodics - bowel colic.
Antibiotics - infection pain.

MANAGEMENT OF NEUROPATHIC PAIN:-
• Up to 40% of cancer-related pain may have a neuropathic mechanism involved. Neuropathic pain may be difficult to control, so a wide variety of treatments may be needed.
• 1st line 2nd line
• Opoids ketamine.
• Antidepressants ligocaine infusion.
• Anticonvulsant
• NSAIDs tens neurolytic Procedure.
• Corticosteroid capsaicin.

DRUGS USED IN NEUROPATHIC PAINOPIOIDS:-
• Opioids are usually partially effective in both cancer-related and non-malignant neuropathic pain. Opioids other than morphine have been shown to be effective are tramadol and fentanyl.
• An alternative opioid analgesic may be tried (tramadol, fentanyl) Management of side effects can be tried (haloperidol to reduce hallucinations).

Neuropathic pain opoids TRICYCLIC ANTIDEPRESSANTS conti……
• The mechanism of analgesic action is principally by facilitation of descending inhibitory pain pathways. (They inhibit pre synaptic reuptake of norepinephrine and serotonin. e.g:- amitriptyline25-100mg imipramine 25 100mg
Many patients do not tolerate amitriptylineespecially in higher doses, therefore consider changing to imipramine. Lower doses of tricyclicantidepressants are found to produce pain relief and faster response when compared with their doses used in depressive.

ANTICONVULSANTS:-Neuropathic painconti…….opoids drug……………….
• These drugs work by dampening abnormal electrical signals in the central nervous system e.g.
• valproate 100-600mg b.d.
• carbamazepine 100-400mg t.d.s.
• clonazepam 1-4mg o.d.
• gabapentin 100-600mg t.d.s.
• pregabalin 25-150mg b.d.

Neuropathic painconti…….opoids drug…………
• The benefits of a lower incidence of gastrointestinal side effects from using COX-2 NSAIDs is reduced by concurrent use of low dose aspirin. This makes the use of COX-2 NSAIDs hard to justify when low dose aspirin is being concurrently administered.
• Non-selective NSAIDs
• e.g.: ibuprofen 200-400mg t.d.s.( p.o.)
• diclofenac 50mg t.d.s. (i/m or suppository)
• naproxen 250-500mg b.d. (p.o. or suppository)
• ketorolac 10-30mg q.d.s (SC,p.o.)

MANAGEMENT OF POORLY CONTROLLED PAIN:-
• Headache due to cerebral edema - Dexamethasone.
• Painful wound - antibiotic.
• Liver capsule pain - dexamethasone.
• Gastric mucosa irritation - omeprazole.
• Gastric distension - methoclopramide.
• Skeletal musclesapsm - buclofen.
• Cardiac pain - nifedipine.
• Oesophageal spasm - nifedipine.
• Intestine colic - hyoscine butyl bromide.

MANAGEMENT OF POORLY CONTROLLED PAIN:- conti…………….
• BREAKTHROUGH PAIN:-Breakthrough pain is a flare in pain of rapid onset, moderate to severe intensity and of short Duration. Incident pain, when pain occurs in response to a specific activity e.g. standing up, walking, changing wound dressings, rectal examination, manual evacuation. Spontaneous pain,
• HEADACHE:-Headache due to raised intracranial pressure often responds well to the use of steroids

MANAGEMENT OF POORLY CONTROLLED PAIN:- conti…………….
• BONE PAIN:-A single fraction of radiotherapy aimed at a localised area in the skeleton may prove beneficial in the relief of bone pain, whereas more widespread bone pain may be improved by wider field radiotherapy or by treatment with a bone seeking isotope e.g. radioactive Sumarium NSAIDS.
• MUSCLE SPASM:-This can be hard to control, but the use of skeletal muscle relaxants such as diazepam 2mg t.d.s. or baclofen 5mg t.d.s.

MANAGEMENT OF POORLY CONTROLLED PAIN:- conti…………….
• LIVER CAPSULE PAIN:-The pain is caused by stretching of the peritoneum on the liver surface and can often be eased by the use of steroids (dexamethasone 4 -6 mg.
• INTESTINAL and URINARY TRACT COLIC:-Pain due to bowel cramps is largely insensitive to morphine but can be eased by smooth muscle relaxants such as hyoscine butyl bromide.

ALTERNATIVE OPIOIDS TO MORPHINE
• 1st line morphine.
• 2nd line oxycodone, fentanyl, hydromorphone
• 3rd line methadone.
• Opioids control pain by blocking receptors (mainly mu and kappa), which are present predominantly in the dorsal horn of the spinal cord but also in the brain stem and in the peripheral nerves.

SPECIFIC MANAGEMENT OF OPIOID SIDE EFFECTS:-
Opioid induced Drowsiness & Cognitive impairment
Hallucinations or Delirium. . Renal failure alone can cause myoclonus, but also causes opioidmetabolites to accumulate which increase the risk of opioid toxicity. Constipation. Nausea & Vomiting
Pruritus. Generalized Pain (Rare). an increase in the opioid dose may lead to worsening of the pain and opioid toxicity.
NON-PHARMACOLOGICAL INTERVENTIONS:-
• Complementary Therapies.
• Acupuncture:it is stimulate of specific acupointalong the skin of body involving various method like heat. Pressure. Or laser or penetration of thin needles{chines medication.
• Reflexology:-it is zone therapy is an alternative medicine or pseudo science involving the physical act of applying pressure to the feet to improve natural function.
• Art therapy:-it is very due to its origins in two fields art and psychotherapy it can focus on the making process therapeutic.

NON-PHARMACOLOGICAL INTERVENTIONS:-
• Touch therapy:-it is therapeutic touch know as some as non contact therapeutic touch is an energy therapy which practitioness claim promotes healing and reduce pain and anxiety.
• Aromatherapy:-it is a form of alternative medicine that uses volantile plant materials know as essential oils. Other aromatic compounds for the purpose of altering a persons mind, mood, cognitive function.

NON-PHARMACOLOGICAL INTERVENTIONS:-
• Music therapy:-it is use of interventions to accomplish individual goal within therapeutic relationship by a professional it is improve a cognitive functioning or motor or skills.
• Hypnotherapy:-it is a form of psychotherapy used to create unconscious change in the patient in the form of new respone thoughts, attitudes behavior feelings it called hypnotherapy.

NON-PHARMACOLOGICAL INTERVENTIONS:-
• Other Non-Pharmacological Intervention.
• Positioning:-it is activity and process of identifying a problem or approtunity and developing a solution based on research.
• Reassurance:-to restore the confidence to assure again. They are very worried and need someone to help them. Stop worrying by saying kind or helpful things.
• Good communication:-the ability to communicate effectively is important in relationship education and work .

NON-PHARMACOLOGICAL INTERVENTIONS:-
• Diversional therapy:the diversional therapists promote the involvement in leisure, recreation and play by reducing barrier of clients providing apportunity.
• Splinting of a fractured limb:-it used a cast will cause pressure sore you can choose wheter or not you will put a layer of cotton wool or orthopaedic.
• Psychological support. it help individuals and communities to heal the psychological wound and rebuild social structure after emergency critical event.

NON-PHARMACOLOGICAL INTERVENTIONS:-
• Relaxation:-this therapy is use any method, process, procedures or activity that help a person to relax stat of increased calmness.
• Joint mobility - passive & active:-the hands on therapy where the patients must physical move their joints and muscles as part of the treatment process.
• Spiritual counseling:-psycho-spiritual counseling take the soul. Rather than the mind as its starting point of balance it has an expanded view of life.

Nursing intervention in pain :-• 1.Screen for pain at each visit, evaluate objectively
the nature of the patients pain, including location, duration, quality, and impact on daily activities.
• 2.Assess patient history and physical examination findings and laboratory values to differentiate expected pain.
• 3.Use a pain intensity scale of 0 {no pain} to 10 {worst possible pain} or other pain scale as appropriate. on the possible,
• 4.Assess relief from medications and duration of relief.
• 5.Base the initial analgesic choice on the patients report of pain.

Nursing intervention in pain :-• 6.Administer drugs orally whenever possible,
avoid I.M. injection.
• 7.Administer analgesia, around the clock, rather than as needed.
• 8.convey the impression that the patients pain is understood and that the pain can be controlled.
• 9.provide ongoing support and open communication.
• 10.Use alternative measures to relieve pain such as guided, imagery, relaxation, and biofeedback
