practical, esthetic options for retention of removable
TRANSCRIPT

Prosthodontics
Practical, esthetic options for retention of removable partial dentnres:A case report
Stephen E. Reagan*/Trent M. Rold**
Abstract This case report describes the treatment of an adult patient with a combination ofßxed and removable prosthodontics. Tke patient was very conscious of esthetics andasked to have no clasps showing. Therefore, retentive features that produced goodesthetics without being overly complex or expensive were provided. This reportdescribes two less commonly used yet very practical and esthetic retentive featuresthat can be used in many situations. (Quintessence Int ¡996:27:333-340.)
Introduction
Even in this era of dental implants, removable partialdentures (RPDs) play a significant role in the practiceof restorative dentistry. Removable pattial denturescan provide a very satisfactory replacement for missinganterior or posterior teeth. However, when they areused in or near the anterior part of the mouth, estheticconsiderations are important. Retentive features suchas circumferential clasps and I bars can be quiteunesthetic in certain situations. This case report willillustrate two retentive features that can be used inesthetically critical situations.
Case report
A 60-year-old man requested comprehensive care. Hehad no health problems. His chief complaint was; "Iwould like to have fixed bridgework for my upper frontteeth. I play a trombone and my existing partialdenture moves around when I play." A comprehensive
* Associate Professur and Director, Advanced General Demislry,University of Oklahoma, College of Dentistry, Oklahoma City.Oklahoma,
" Advanced General Dentistry Resident, University of Oklahoma,College of Dentistiy, Oklahoma City. Oklahoma
Reprint reqjests: Dr Stephen E. Reagan, Associate Professor andDirector, Advanced General Dentistry, University of Oklahoma, Collegeof Dentistry, 1001 Stamon L. Young Boulevard, Room 305, PO Box26901, Oklahoma City, Oklahoma 73190.
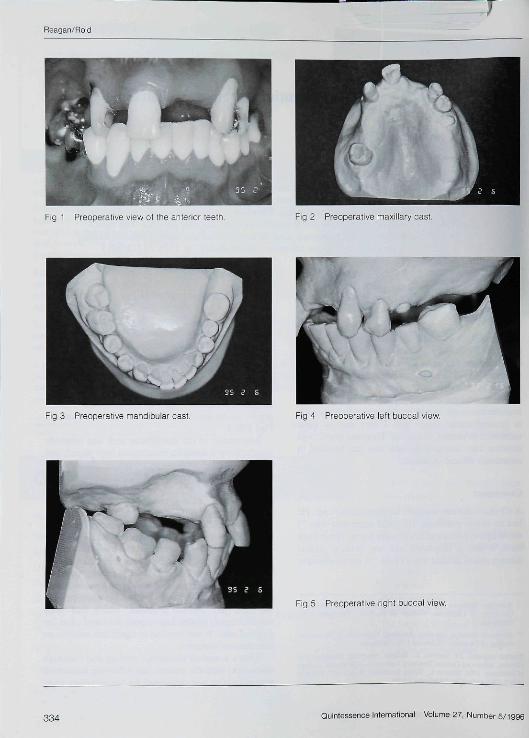
examination revealed no significant periodontal prob-lems, but the patient had several missing and cariousteeth, and his plaque control needed improvement. Hehad no signs or symptoms of temporomandibular jointproblems. Clinical examination and diagnostic mount-ing of the patient's casts demonstrated no discrepancybetween the centric relation and maximal inter-cuspation positions (Eigs 1 to 5). Preoperative radio-graphs of the maxiiiary anterior teeth can be seen inEigs 6 to 8.
Restoration of the mandibular arch was relativelysimple. Several amalgam restorations were placed, anda compiete gold crown was placed on the left firstmolar to level and improve the occlusal plane in thatarea.
Restoration of the maxillary arch was much morecomplex and was influenced by the fact that the patientwas very conscious of esthetics. The patient only hadsix teeth remaining in the maxillary arch: the rightcentral incisor, canine, and third molar and left canine,first premolar, and second premolar. Papillary hypcr-plasia was evident (Eig 9). The patient declinedimplants, making treatment with a removable partialdenture the only viable option. In addition, themaxillary left second premolar, which had beenendodontically treated had recently fractured off at thegingival crest. It was decided to retain this tooth as anoverdenture abutment.
After a complete diagnostic workup and thoroughdiscussion with the patient, the following sequencedtreatment plan was developed for the maxillary arch:
Quintessence International Volume 27, Number 5/1996 333
Reagan/Rol d
Fig 1 Preoperafive view of fhe anferior teefh. Fig 2 Preoperative maxillary oast.
Fig 3 Preoperafive mandibular cast. Fig 4 Preoperafive leff buceal view.
Fig 5 Preoperative righf buceal view
334 Quintessence International Volume 27, Number 5/1996

Reagan/Rold
Figs 6 fo 8 Preoperafive radiographs of fhe maxillary anterior leelh
Fig 6 Fig 7 Fig 8
1, A six-unit fixed partial denture (teeth 13-11-23),with the right canine functioning as a survey crown.An IC attachment (APM-Stemgold) was plannedfor the distal aspect of the canine, and an Equipoiseclasp was suggested to engage the distobuccalundercut on the left first premolar.
2, Survey crowns for the right third molar and left flrstpremolar,
3, A maxillary removable partial denture.
First, a diagnostic waxup was completed to preparefor the provisional restoration. Another set of castswas used to survey and design the removable partialdenture so that all aspects of the RPD could beconsidered prior to tooth preparation. Then, the rightcentral incisor and catiine and left canine wereprepared for the metal-ceramic fixed partial denture(Fig 10), impressions were made, and casts werearticulated. The left first premolar and right third molarwere not prepared at this time because they were theonly vertical stops remainitig. This allowed the existingverticai dimension of occlusion to be maintained.
The left canine and first premolar were not splintedtogether for the following reasons: (I) The firstpremolar was not mobile and had good bone support;(2) Splinting them would have increased the com-plexity of the anterior ftxed partial denture and made
cleaning the area more difficult; (3) This maxillaryRPD was tooth supported on the right side and a veryfirm ridge was present on the left side; therefore, it wasnot thought that the stresses on the first premolarwould be excessive,
A full contour waxup of the fixed partial denturewas completed using a reference cast of the provisionalrestoration after ineisal edge position, esthetics, andphonetics had been verified. The wax cutback for theceramic portion of the restoration was completed, andthe waxup was invested and cast. The patient's lip linewas low enough to allow metal margins on the fixedpartiai denture abutments.
Tbe metal framework was tried in, and tbe frame-work was cut, indexed, and soldered when tbe fit of tbeoriginal casting was found to be unsatisfactory. Aftertbe fit of the soldered framework was verified, por-celain was added to the restoration; again the referencecast from the provisional restoration was used. Thefixed partial denture was cemented after properesthetics, phonetics, and occlusion were verified{Fig 11),
The next step in treatment was placement of anamalgam restoration in the left second premolar (theoverdenture tooth) and fabrication of survey crownsfor tbe left fhrst premolar and rigbt third molar (Figs 12and 13), After both castings were cemented, a final
Quinfessence internationai Voiume 27, Number 5/t996 335

Reagan/Rold
Fig 9 Preoperative clinical view oi the maxillary arch Fig 10 Maxillary anterior tooth preparations.
Fig 11 Completed maxillary anterior fixed partial denture. Fig 12 Survey crowns on the master cast.
Fig 13 Evaluation of the distobuccal undercut and guide- Fig 14 Completed RPD framework,plane where the Equipoise Clasp will be placed.
336 Quintessence Intemational Volume 27, Number 5/1996

Reagan/Rold
Fig 15 Completed restoration. Fig 16 Compleled restoration.
Fig 17 Left side of the completed restoration; the tip ofEquipoise clasp engaging the distobuccal undercut on themaxillary first premolar.
Fig 18 Right side of the compieted restoration: the ICattachment on the distal surface of the canine is not visible.
alginate impression was tnade (Accudent Systetn II.Accu-dent) to allow fabrication of the removablepartial denture framework (Fig 14). At the RPDframework try-in appointment, the IC attachment wasadded. The framework was sent to the laboratory forsetting of the artificial teeth and processing.
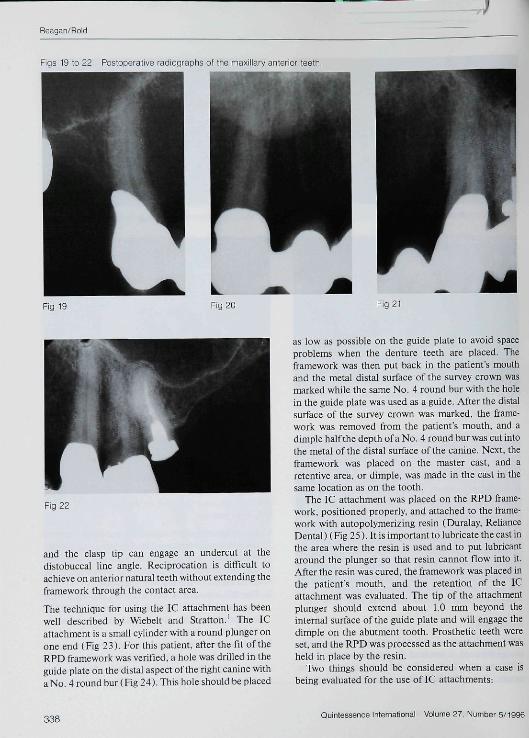
When the maxillary RPD was delivered to thepatient, he was extremely pleased with the function,retention, and esthetics (Figs 15 to 18). The patientwas also more comfortable playing his trombone. Post-operative radiographs can be seen in Figs 19 to 22.
Discussion
Although the treatment for this patient was reasonablystraightforward, it involved the use of two very usefulRPD retentive features for the anterior part of themouth. Either the Equipoise clasp or the IC attach-
ment could have been used on both sides of the RPD,but the IC attachment was used on the patient's rightand the Equipoise was used on the patient's left for thefollowing reasons:
1. The IC attachment was used on the distal aspect ofthe right canine because it is a slightly more estheticsystem than the Equipoise, and the distal aspect ofthe canine was more esthetically critical than thedistal aspect of the left first premolar.
2. The IC attachment was used on the right sidebecause the RPD on that side was totally toothsupported, and IC attachments work particularlywell in these situations.
3. The Equipoise clasp was used on the distal aspectof the left first premolar because this system worksvery well with premolar abutments. The occlusalrest provides excellent reciprocation for the clasp.
Quintessence International Volume 37. Nutnber 5/1996 337
Reagan/Rold
Figs 19 to 22 Posioperative radiographs of the maxillary anterior teelh.
Fig 19 Fig 20 Fig 21
Fig 22
and the clasp tip can engage an undercut at thedistobuccal line angle. Reciprocation is difficult toachieve on anterior natural teeth without extending theframework through the contact area.
The technique for using the IC attachment has beenwell described by Wiebelt and Stratton.' The ICattachment is a small cylinder with a round plunger onone end (Eig 23). Eor this patient, after the fit of theRPD framework was verified, a hole was drilled in theguide plate on the distal aspect of the right canine witha No. 4 round bur (Eig 24). This hole should be placed
as low as possible on the guide plate to avoid spaceproblems when the denture teeth are placed. Theframework was then put back in the patient's mouthand the metal distal surface of the survey crown wasmarked while the same No. 4 round bur with the holein the guide plate was used as a guide. After the distalsurface of the survey crown was marked, the frame-work was removed from the patienfs mouth, and adimple half the depth of a No. 4 round bur was cut intothe metal of the distal surface of tbe canine. Next, theframework was placed on the master cast, and aretentive area, or dimple, was made in the cast in thesame location as on the tooth.
The IC attachment was placed on the RPD frame-work, positioned properly, and attached to the frame-work with autopolymerizing resin (Duralay, RelianceDental) (Fig 25). It is important to lubricate the cast inthe area where the resin is used and to put lubricantaround the plunger so that resin cannot flow into it.After the resin was cured, the framework was placed inthe patient's mouth, and the retention of the ICattachment was evaluated. The tip of the attachmentplunger should extend about 1.0 mm beyond theinternal surface of the guide plate and will engage thedimple on the abutment tooth. Prosthetic teeth wereset, and the RPD was processed as the attachment washeid in place by the resin.
Two things should be considered when a case isbeing evaluated for the use of IC attachments:
338Quintessence International Volume 27, Number 5/1996

Reagan/Rold
23 IC aftachment Fig 24 Hole in the guide plate distal ot fhe maxillary rightcanine.
Fig 25 IC attachmeni held in place wifh resin.
1, The guide plate must have enough vertical height toallow room for the attachment; a minimum of about4.0 mm is required,
2. These attachments make it more difftcult to set theartificial teeth because of the space they occupy. Ifvertical space is minimal, the esthetics of theartificial teeth may be slightly comprotnised.
The Equipoise claspiitg system was used for reten-tion of the RPD on the distal aspeet of the maxillaryleft first premolar, Goodman^-^ developed and de-seribed the Equipoise system and advocated it foresthetics and preservation of the abutment teeth. Whenthe Equipoise clasp is used on a premolar next to adistal-extension area, such as in this case, a prominentQcclusal rest seat should be placed on the side of theabutment tooth opposite the edentulous area. Theretentive clasp extends from the mesial rest and circles
around the lingual and distal surfaces of the tooth andengages a distobuccal undercut. This clasp is estheticbecause no clasp is present on the buceal surface; it isalso kind to abutment teeth because it disengages whenthe pariial denture is in ilinction.
Reciprocation and lack of retention can be a problemwith the Equipoise clasp, Goodman--' advocatedremovai of 0,5 mm of tooth structure from adjacentteeth so that rigid metal of the RPD framework canextend into this area and provide reciprocation for theclasp. This procedure actually opens the contactbetween teeth. This works well, but can be slightlyunesthetic and requires the sacrifice of considerabletooth structure.
We have found that survey crowns can provideadequate reciprocation for an Equipoise clasp byextending the framework as far buccaiiy as possiblewithout breaking contact and by creating a prominentocciusal rest seat. This rest seat should be 1,5 to 2,0mm deep and should be about one third the mesio-distal diameter of the tooth and about one half thebuccolingual diameter of the tooth.
Another problem with the Equipoise clasp canoccur during processing. Excess acrylic resin may beallowed to surround the clasp if the laboratorytechnician is not familiar with its design. When thishappens, the clasp is not able to flex into the retentivearea, and the appliance may not seat in the patient'smouth. If the ciasp is not free to flex properiy. it mayalso place unfavorable forces on the abutment tooth."Freeing up" the clasp after processing is difficult andtime consuming. These problems can be prevented ifStalite spacer (Buffalo Dental) is placed around theciasp during processing (Figs 26 and 27), The spaceris easily removed during finishing and polishing of thepartial denture.
Quintessence International Volume 27, Number 5/1996 339

Reagan/Roid
Fig 26 Equipoise clasp on fhe maxiiiary ieff first premoiar. Fig 27 Staute materiai covering the Equipoise ciasp foprevent resin from fouohing fhe clasp.
Summary
This case study illustrated the use of two very practical
and effective means of retention for removable partial
dentures tbat can be used when esthetics is of great
concern. Use of the IC attachment and Equipoise clasp
should be considered wben the restorative dentist
plans to fabricate removable partial denttires.
References
1. Wiebelt FJ. Slratton RJ The \C partial denture attachment. J ColoDent Assoc l983;(May-]une):3-5.
2. Goodman JJ. Tiie Equipoise retnovable rebturation. Trends Tech-niques Contemp Dent Lab i99i;8:45-52.
3. Goodman JJ. Sixteen Basic Designs for Removabie Prostheses.Tenally, NJ: Dental Prostiietic Corp, 1977; i-26. D
340 Quintessence internafional Volume 27, Number 5/i99e