power of one: strategies for preventing cla-bsi’s & …€¦ · power of one: strategies for...
TRANSCRIPT

Power of One: Strategies for Preventing CLA -BSI’s &
VAP on Your Watch
Pat Posa RN, BSN, MSASystem Performance Improvement Leader
St. Joseph Mercy Health SystemAnn Arbor, MI
Target Zero

Disclosures
•Consultant-Michigan Hospital Association Keystone Center•Consultant-Missouri Center for Patient Safety•Contracted consultant for •Contracted consultant for Advancing Nursing, LLC
– Consulting services:
• Edward Lifesciences
• Sage Products

Session Objectives
• Identify risk factors for the development of central line associated blood stream infections and ventilator associated pneumonia
• Define key care practices based on the evidence that can reduce and sustain zero BSI’sreduce and sustain zero BSI’s
• Define key care practices based on the evidence that can reduce and sustain zero VAP’s
• Discuss strategies to work on a safety culture as care practices are changed.

Infection epidemic carves deadly pathPoor hygiene, overwhelmed workers contribute to thousands of deathsJuly 21, 2002| By Michael J. Berens, Tribune staff reporter.
“A hidden epidemic of life-threatening infections is contaminating America's hospitals, needlessly killing tens of thousands of patients each year. These infections often are characterized by the health-care industry as random and inevitable byproducts of lifesaving care. But a Tribune investigation found that in 2000, nearly three-quarters of the deadly infections--or about 75,000—were preventable, the result of unsanitary facilities, germ-laden instruments, unwashed hands and other lapses…”

Why HAI’s?
• 2.5 million HAI’s year/USA• Everyday, 247 people die in the USA as a
result of a HAI• 5-10% of all patients admitted to US hospital • 5-10% of all patients admitted to US hospital
annually contract HAI’s (1 of every 10-20 patients)
• 6th leading cause of death in the US• Higher nurse staffing results in lower HAI’s*
*Hugonnet S et al CCM 2007;35:76-81*Pronovost PJ et al JAMA 1999;281:1310-1317*Needleman J et al. N Engl of Med 2002;346:1715-1722
WHO 2005Yokoe DS, et al. Infect Control Hosp Epidemiol 2008;29:S12-S21.

• 44,00 to 98,000 preventable death in hospitals related to medical errors annually (IOM report, 1999)
• 92,888 deaths directly attributable to safety indicators between 2005-2007 (HealthGrades 2009)
It is Time to Change!!
between 2005-2007 (HealthGrades 2009)
– post-op infections, failure to rescue & pressure ulcers
• National Patient Safety Goals include prevention of HAI’s
• Lack of reimbursement for preventable injury
Yokoe DS, et al. Infect Control Hosp Epidemiol 2008;29:S12-S21.Needleman J et al. N Engl of Med 2002;346:1715-1722

It is Time to Change!!
• $50 billion in total costs for preventable injury
• 2011 mandatory federal reporting of CLA-BSI’s
• 2013-lowest percent improvement/total • 2013-lowest percent improvement/total Medicare cut
• HHS goal to reduce HAI’s by 40% in 3 years (1 billion to assist in achieving goal)
Yokoe DS, et al. Infect Control Hosp Epidemiol 2008;29:S12-S21.Needleman J et al. N Engl of Med 2002;346:1715-1722http://www.hhs.gov/news/press/2011pres/06/20110622a.htmlhttp://content.healthaffairs.org/content/30/4/723.abstract

How Big of a Problem are Health Care-AssociatedInfections (HAIs) in U.S. Hospitals?
Total HAI’s / year = 1.7 million; 98,987 deaths
SSI
BSI
11%
Other
22%
133,368
263,810
274,098
-967
-21
-28,725
TOTAL
HRN
WBN
Non-newborn ICU
Klevens, et al. Pub Health Rep 2007;122:160-6
20%
UTI
36%PNEU
11%424,060
129,519
-28,725
244,385
Non-newborn ICU
= SSI
HRN=High Risk Newborn, WBN=Well Baby Nursery, ICU=Intensive Care Unit, SSI=Surgical Site Infection, BSI=Bloodstream Infection, UTI=Urinary Tract Infection, Pneu=Pneumonia

Value Sets Platform for Performance ImprovementThe Vision of Health Care in the U.S. 2012 -
Volume-
driven
healthcare
Cost
• Fragmented• Fee-for-service
• Connectedhealthcare
VALUE-driven
healthcare
Quality
• Connected• Bundled• Accountable

The Journey Towards Value-Based Purchasing Begins
• Payment reforms for inpatient hospital services in 2008:– …ensure that Medicare no longer pays for the additional costs
of certain preventable conditions (including certain infections) acquired in the hospital…
1) Serious preventable events: Object left in during surgery; air embolism; Delivering ABO-incompatible blood or blood productsembolism; Delivering ABO-incompatible blood or blood products
2) catheter-associated urinary tract infections (CAUTIs)3) pressure ulcers4) Vascular catheter associated infection5) Mediastinitis after CABG surgery6) Patient falls – refining for FY09Coming attractions?: VAP – Not yet, S. aureus BSI – Yes but
limited to MRSA LabID, MRSA- No, CDI – Yes, LabID

Health Care Quality Comparison
Defects per Detection &
Overall Healthcare in US (RAND) Outpatient ABX for colds
Healthcare-associated infections (HAIs)Hospital patients
Injured through negligence
Airline baggage handling
Post MIβ-blockers10,000
100,000
1,000,000
per million
σ Level (% defects)
US industry best-in-class
Detection & treatment of depression
Adverse drug events
handling
Anesthesia-related fatality rate
Food safety1
10
100
1,000
(69%) (31%) (7%) (0.6%) (0.002%) (0.00003%)1 2 3 4 5 6

HAI Event Facility Type Reporting Start Date
CLABSIAcute Care Hospitals
Adult, Peds, and Neonatal ICUsJanuary 2011
CAUTIAcute Care Hospitals
Adult and Pediatric ICUsJanuary 2012
New and Coming Attractions from CMS: Pay 4 Reporting (P4R)
SSIAcute Care Hospitals
Colon and abdominal hysterectomyJanuary 2012
CLABSI Long Term Care Hospitals * October 2012
CAUTI Long Term Care Hospitals * October 2012
CAUTI Inpatient Rehabilitation Facilities October 201 2
* Long Term Care Hospitals are called Long Term Acute Care Hospitals in NHSN
CMS 2012 IPPS final rule released; August 18 2011 Feder al Register 76 (no. 160)

HAI Event Facility Type Reporting Start Date
MRSA Bacteremia Lab ID * Acute Care Hospitals – facility wide
January 2013
C. difficile LabID EventAcute Care Hospitals – facility
January 2013
New and Coming Attractions from CMS: Pay 4 Reporting (P4R)
C. difficile LabID Eventwide
January 2013
HCW Influenza Vaccination
(aggregate data will be allowed; updates to NHSN HCP module
underway )
Acute Care HospitalsJanuary – March
2013
* Lab ID = reports positive cultures detected > day 3 of hospitalization
CMS 2012 IPPS final rule released; August 18 2011 Feder al Register 76 (no. 160)

2003 2010
2011Power of the Consumer: Growth in State-based
Legislation on HAI Reporting Mandates
CMS. Pay 4 Reporting:CLABSI in ICUs, 2011; Colon surg, Abd. Hyst, & CAUTIs: 2012
2011

HHS HAI Prevention Dashboard
CDC press, 10/19/11
TOPIC METRIC & TARGET Progress Report
Central line-assoc.
bloodstream infection
(CLABSI)
CLABSI Std Infection Ratio
(SIR); 50% drop
18% drop in 2009
33% drop in 2010!
CLABSI Insert. Bundle Proportion of insertions using
bundle; 100% adherence
Sample of Hospitals = 92% - on
target, 2009
C. difficile Infection (CDI) Rate/1000 discharges; 30% Rate/1000 discharges; 30%
reductionreduction
8.9 in 2009; 9.4 in 2010 8.9 in 2009; 9.4 in 2010 –– not not
likely to meet target likely to meet target
HAI Prevention Dashboard: How are we doing?U.S. Hospitals
reductionreduction likely to meet target likely to meet target
Catheter-assoc. UTI (CAUTI) CAUTI rate ; 25% reduction Estimate in ’08 = 5% reduction
7% reduction, 2010
MRSA Rate invasive MRSA/100k pop.;
50% reduction
22.72 in 2009 = 13.4% drop
compared to ’07-’08
18% reduction, HA-MRSA, 2010
SSI SIR; 25% reduction 5% reduction SSIs, 2009
10% reduction, 2010
SSI Proportion SCIP measures;
95% adherence
> 92% in 2009 – on target

Advocacy Starts with Us

Notes on Hospitals: 1859
“It may seem a strange principle to enunciate as the very first requirement in a Hospital that it should do the sick in a Hospital that it should do the sick no harm.”
Florence Nightingale
Advocacy = Safety

Patient Advocacy/Safety Related to Clinical Practice
• Nurses knowledge of the evidence based care• Ability to deliver the care to the right patient at the
right time, every time it is needed• The ability to communicate patient concerns in a • The ability to communicate patient concerns in a
concise, data driven manner and take appropriate action
• Understanding the chain of command when faced with resistance

Translating Evidence into Practice(Johns Hopkins model)

Four E’s• Engage: help staff understand the preventable harm
– Share stories about patients affected– Estimate number of patients harmed– Develop a business case
• Educate: ensure staff and senior leaders understand what they need • Educate: ensure staff and senior leaders understand what they need to do to prevent injury and improve teamwork and communication– Conference calls, webcasts, meetings
• Execute: how given the resources and culture they would ensure that all patients received the evidence– Share with working, what’s not– Coaching calls
• Evaluate: project leader monitors that team are using standardized definitions, report their data and make it transparent at the unit level
Goeschel CA, et al. Nursing in Critical Care, 2011;16:35-42

Central Line -Associated Blood Stream InfectionsStream Infections

The Problem is Large
• 15 million catheters inserted ICU’s per yr
• 80,000 CLA-BSI in U.S. ICUs annually
• Majority are preventable
• Mortality: 18% (12%-25%) 28,000 deaths
• NHSN CVC: 1.0 (PICU) – 5.6 (Burn ICU) per/1000 cath days• NHSN CVC: 1.0 (PICU) – 5.6 (Burn ICU) per/1000 cath days
• Rate may be higher in wards vs. ICU’s*/Use 16%
• PICC rates: 3.63 per 1000 cath days (Single center)
• Cost per episode: $18,000
• 300 million to 2.3 Billion
• LOS � up to 12 daysCDC. MMWR 2002; Rosenthal VD, et al. Am J of Infect Control, 2008;36:627-37Edwards JR, et al. Am J of Infect Control, 2008;36:609-26 ;Perencevich EN, et al. JAMA, 2009;301:1285-1287Coello R, et al. J Hosp Infect, 2003;53:46-57 , *Zingg W, et al. J Hosp Infect 2009; *Al-Rawaifah OM, et al. Infect Control Hosp Epidemiol, 2009;30:1036-1044Ajenjo MC, et al. Infect control Hosp Epidemiol, 2011;32:125-130

Potential Sources of Infection for Intravascular Devices
Clin Infect Dis 2002;34:1232-42

CUSP & CLABSI Interventions
1. Educate on the Science
of Safety
CUSP CLABSI
1. Insertion
2. Maintenance
Adaptive /Cultural Technical
of Safety
2. Identify Defects (Staff
Safety Assessment)
3. Senior Executive
Partnership
4. Learn from Defects
5. Implement Teamwork
& Communication
Tools
2. Maintenance
a. Assessment & Site
Care
b. Tubing, Injection
Ports, Catheter Entry
24

Updated HICPAC Categorization Scheme for Recommendations

• Remove/Avoid unnecessary lines (IA)• Hand hygiene (IB)• Maximal barrier (IB)• Chlorhexadine for skin prep (IA)
Blood Stream Infection (BSI) Prevention Bundle (IB)
• Chlorhexadine for skin prep (IA)• Avoid femoral lines (IA)
CDC. Prevention of Catheter Infection: MMWR 2002;51 (No. RR-10):[1-29]http://www.guideline.gov/summary/summary.aspx?doc_id=13395&nbr=006806&string=CLA-BSI –Oct 2008www.ihi.orgGrady NP, et al. CDC Guidelines for the Prevention of Intravascular Catheter-Related Infections, 2011. www.cdc.govhttp://www.onthecuspstophai.org/
Education & Culture of Safety

What Does the ‘Bundle’ Evidence Tell Us?

Hand Hygiene is the Single Most Important Factor in Preventing the Spread of
Infection

Guidelines for Hand Hygiene in Health Care Settings
• If hands are not visibly soiled, use an alcohol-based hand rub for routinely decontaminating hands in all other clinical situations (1A)
• When hands visibly soiled or exposure to potential spore forming organisms, wash with either a non-antimicrobial or antimicrobial soap & water (IB)
• Decontaminate hands after removing gloves• When washing with soap & water, wet hands first, apply
soap, rub vigorously for 15 seconds, rinse and dry. Use towel to turn of faucet. (Duration 40 seconds)
• Provide HCW with hand lotions & creams to minimize occurrence of irritant contact dermatitis (IA)
• Use multidimensional strategies to improve hand hygiene practice (IA)
• Do not wear artificial fingernails or extenders (IA)
CDC. Hand Hygiene Guidelines: MMWR 2002; 51(No. RR-16):[1-45]WHO Hand Hygiene Guidelines 2009

When to Wash
Pittet D. Infect Control Hosp Epidemiol, 2009;30(7):611-622

Reasons for Non-Compliance
• Lack of knowledge on importance and how the hands become contaminated
• Lack of understanding of correct techniquetechnique
• Understaffing and overcrowding• Poor access• Irritant contact dermatitis associated with
frequent exposure• Lack of institutional commitment to good hand
hygiene
Pittet D et al. Lancet Infect Dis. 2001;1:9-20

Correct use can reduce colony forming units by 90%, incorrect use only 60%. 1-3mL correct amount per HH episodeLausten S, et al. Infect Control Hosp Epidemio, 2008;29:954-956

Prevention Strategies Targeting Hand Hygiene & Catheter Care Impact Outcomes
• Baseline period– 499 patients– 6200 catheter days– 3.9 per 1000 catheter
• Intervention Period– Multimodal education
campaign• 4 educational modules 90
minutes apiecedays– 59% hand hygiene– 22.5% correctly
performed hand hygiene
minutes apiece
– 500 patients– 7279 catheter days– 1.0 per 1000 catheter days
(p<0.001)– 65% hand hygiene– 42.6% correctly performed
hand hygiene (p=0.003)Zingg W, et al. Crit Care Med, 2009;37:2167-2173

What Does the ‘Bundle’ Evidence Tell Us?

CDC Guidelines for Insertion Site Preparation
� Sterile technique; cap, mask, gown, gloves, and a large sterile drape (IB)
� Recommend 2% Chlorhexidine be the cleanser of choice if available (IA)cleanser of choice if available (IA)
Prevention of Catheter Infection: MMWR 2002;51 (No. RR-10):[1-29]Grady NP, et al. CDC Guidelines for the Prevention of Intravascular Catheter-Related Infections, 2011. www.cdc.gov

What are Maximal Barrier Precautions?
• For Provider:– Hands hygiene– Non-sterile cap and
mask• All hair should be under cap• Mask should cover nose
and mouth tightly
– Sterile gown and gloves• For the Patient
– Cover patient’s head and body with a large sterile drape

Efficacy of Maximal Sterile Barrier Precautions
Minimal* Maximum**
Local inf. 7.2% 2.3%
CVC-BSI 3.6% 0.6%CVC-BSI 3.6% 0.6%
** sterile gloves, small sterile drape* cap, mask, sterile gloves, sterile gown, head/body of patient
covered with large sterile drape
Raad II, et al. Infect Control Hosp Epidemiol 1994;15:231-8

Chlorhexidine vs Povidone Iodine for Catheter Site Care
Ann Intern Med 2002:136:792-801

What Site Should Not Be Used: Femoral (1-A)
• RCT of femoral and SC lines in the ICU– 145 pts femoral/144 pts SC
• Outcomes– Higher rate of infectious complications in femoral – Higher rate of infectious complications in femoral
grp: 19.8% vs 4.5% (p<.001)– Higher rate of thrombotic complications in femoral
grp: 21.5% vs 1.9% (p<.001); complete thrombosis 6% vs 0%
– Similar rates of mechanical complications: 17.3% vs 18.8% (p=NS)
Merrer, et al JAMA 2001,286: 700-7; Lorente e tal, 2005

What About the Jugular for Infection/Injury Risk?
2-fold risk of CLA-BSI’s using Jugular vs. Subclavian
Crit Care Med, 2001;30:454-460
Subclavian(Nagashima G, et al. J Infect Chemother, 2006;12:363-365)

2011 Recommendations: Site Location
• Avoid using the femoral vein for central venous access in adult patients (1A)
• Use a subclavian site, rather than a jugular or a femoral site, in adult patients to minimize infection risk for nontunneled CVC placement (1B) CVC placement (1B)
• Avoid the subclavian site in hemodialysis patients and patients with advanced kidney disease, to avoid subclavian vein stenosis (1A)
Grady NP, et al. CDC Guidelines for the Prevention of Intravascular Catheter-Related Infections, 2011. www.cdc.gov

2011: Additional Placement Guidelines
• Use ultrasound guidance to place central venous catheters (if this technology is available) to reduce the number of cannulation attempts and mechanical complications. Ultrasound guidance should only be used by those fully trained in its technique. (IB)
• Use a CVC with the minimum number of ports or lumens • Use a CVC with the minimum number of ports or lumens essential for the management of the patient (IB)
• Promptly remove any intravascular catheter that is no longer essential. (IA)
• Use a sutureless securement device to reduce the risk of infection for intravascular catheters. (II)
Grady NP, et al. CDC Guidelines for the Prevention of Intravascular Catheter-Related Infections, 2011. www.cdc.gov

CDC Recommendation for Catheter Replacement
• When adherence to aseptic technique cannot be ensured replace the catheter as soon as possible, i.e, within 48 hours. (IB)
• Do not routinely replace CVCs, PICCs, hemodialysis catheters, or pulmonary artery catheters to prevent catheter-catheters, or pulmonary artery catheters to prevent catheter-related infections. (IB)
• Use a guidewire exchange to replace a malfunctioning non-tunneled catheter if no evidence of infection is present. (IB)
• Do not use guidewire exchanges to replace a non-tunneled catheter suspected of infection. (IB)
• Routine culture of the tip is not recommended.• .CDC. Prevention of Catheter Infection: MMWR 2002;51 (No. RR-10):[1-29]
Grady NP, et al. CDC Guidelines for the Prevention of Intravascular Catheter-Related Infections, 2011. www.cdc.gov

Dressing Care
• Use a transparent or gauze dressing to cover site (IA)• Change transparent dressing and perform site care with a CHG
based antiseptic every 7 days (IB) or more frequent if the dressing is soiled, loose, or damp; (IB)
• Change gauze dressings every 2 days or more frequent if the dressing is loose, soiled or damp (II)
• Use a chlorhexidine-impregnated sponge dressing for temporary short-term catheters in patients older than 2 months of age if the CLABSI rate is not � despite EBP (1B)
• No recommendation is made for other types of chlorhexidinedressings.
SHEA and IDSA, Infection Control and Hospital Epidemiology Oct 2008Prevention of Catheter Infection: MMWR 2002;51 (No. RR-10):[1-29]Salgado CD, et al. Infect Control and Hosp Epidemi, 2007;28:684-688Grady NP, et al. CDC Guidelines for the Prevention of Intravascular Catheter-Related Infections, 2011. www.cdc.gov
Care After Insertion
• Scrubbing the access port with an appropriate antiseptic (chlorhexidine, povidone iodine, an iodophor, or 70% alcohol) and accessing the port only with sterile devices.(IA)
• 3 sec, 10 sec & 15 sec scrub showed no difference in reducing bacterial load (Simmons S, et al. Crit Care Nurs Q, 2011;34:31-35)
Replace administration sets not used for blood, blood products or lipids
• Split system value designs are preferred over positive pressure mechanical valves because they are associated with lower CLA-BSI rates.
• In 2008 FDA required 9 companies to conduct post market surveillance of positive displacement needless connectors
Rupp ME, et al. Clin Infect Dis. 2007;44(11):1408-1414• Replace administration sets not used for blood, blood products or lipids at intervals not longer than 96 hours (IA)
• Replace tubing used to administer blood, blood products, or fat emulsions within 24 hours of initiating the infusion. (IB)
• When needleless system used, consider a split septum valve versus a mechanical valve.(II)
• Change the needleless components at least as frequently as the administration set. (II)
• Use a 2% chlorhexidine wash for daily skin cleansing to reduce CRBSI (II )
Rupp ME, et al. Clin Infect Dis. 2007;44(11):1408-1414FDA Medical Device Alert 2008

Additional Strategies Used When Basic Care Has Not Achieve Zero
� CHG Baths (II)
� CHG Dressings (IB)
� Antimicrobial impregnated CVC (IA)� Antimicrobial impregnated CVC (IA)
� Antimicrobial locks (II)
� Appropriate nursing staff levels in ICUs. (1B)
Coffin SE, et al. Infection Control & Hosp Epid, 2008;29(1):S31-S40Grady NP, et al. CDC Guidelines for the Prevention of Intravascular Catheter-Related Infections, 2011. www.cdc.gov

CHG Bathing Reduces CLA-BSI’s (II)
• 52 week, 2 arm, cross-over design clinical trial• 22 bed MICU with 11 beds in 2 geographically
separate areas• 836 MICU patients
– 1st 28 weeks: 1 hospital randomize to bathe – 1st 28 weeks: 1 hospital randomize to bathe with (Sage 2%) CHG cloths & the other unit bathe with soap & water
– 2 week wash out period– 2nd 24 weeks: methods were crossed over
• Measured: Primary outcomes: incidence of CA-BSI’s & clinical sepsis. Secondary: other infections
Bleasdale SC. et al. Arch Internal Med, 2007;167(19):2073-2079

CHG Bathing Reduces CLA-BSI’s (II)
Results: � CHG arm were significantly less likely to acquire a CA-BSI 4.1 vs. 10.4 infections per
Bleasdale SC. et al. Arch Internal Med, 2007;167(19):2073-2079
vs. 10.4 infections per 1000 patient days
� Benefit against primary CA-BSI’s by CHG cleansing after 5 days in MICU
� No difference in clinical sepsis or other infections
Pre-Op Prep
• Antisepsis must demonstrate a 3.0 log 10 from baseline in groin, 2.0 10 log reduction on the abdomen and maintain effectiveness for minimum of 6 hrs.
• CHG shower/bathing versus soap & water showed no difference in SSI (Cochrane EBR: 2007:CD004985)
• 2% prep cloth more effective in reducing bacterial load • 2% prep cloth more effective in reducing bacterial load than 4% CHG solution that must be rinsed off/Inguinal sites sustained action at 10min, 30 min, 6 hrs > than 4% (Edmiston CE. Et al AJIC, 2007;35:89-96)
• CDC recommends must bathe or shower night before– Compliance issues, consistency in application, unable to
bathe self• Chlorhexidine is absorbed onto fibers of certain fabrics,
particularly cotton (Denton GW. Chlorhexidine. In Block S, ed. Disinfection, Sterilization and preservation, 4th ed. Philadelphia: Lea & Febiger, 1991:274-89)
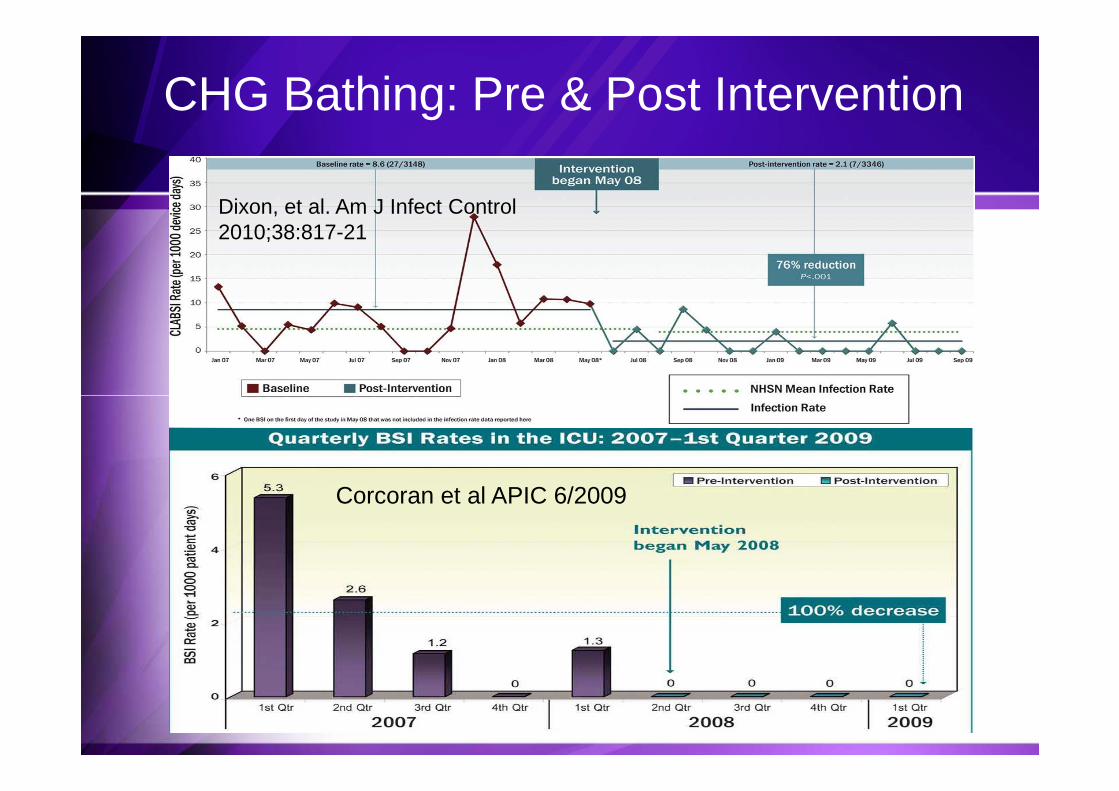
CHG Bathing: Pre & Post Intervention
Dixon, et al. Am J Infect Control 2010;38:817-21
Corcoran et al APIC 6/2009

Additional Strategies Used When Basic Care Has Not Achieve Zero
� CHG Baths (II)
� CHG Dressings (B-I)
� Antimicrobial impregnated CVC (A-I)� Antimicrobial impregnated CVC (A-I)
� Antimicrobial locks (II)
� Appropriate nursing staff levels in ICUs. (1B)
Coffin SE, et al. Infection Control & Hosp Epid, 2008;29(1):S31-S40Grady NP, et al. CDC Guidelines for the Prevention of Intravascular Catheter-Related Infections, 2011. www.cdc.gov

CHG-Impregnated Sponges for Prevention of CLA-BSI (IB)
Methodology:• Multi-center, randomized controlled trial • 7 ICUs participated• Included all patients who required arterial or central
venous catheter for 48 hours or longer• Included all patients who required arterial or central
venous catheter for 48 hours or longer• Use of CHG dsg vs standard dsg• Already using maximal barrier precautions, try and use
subclavian site for central line, use alcohol/povidone-iodine prep solution (not CHG)
• Looked at 3 day vs. seven day dressing change (but changed when dsg was loose, soiled or damp in all groups)
Timsit JF, et al. JAMA 2009;301:1231-1241

CHG-Impregnated Sponges for Prevention of CLABSI (IB)
• 1636 patients (3778 catheters, 28,931 catheter days)• Median duration of catheter insertions 6 days (4-10)• Use of CHG dressing decreased the CLA-BSI rate from:
– 1.3 per 1000 catheter days to 0.4 per 1000 catheter days
Results:
– 1.3 per 1000 catheter days to 0.4 per 1000 catheter days• Use of CHG dressing not associated with greater
resistance of bacteria in skin samples at removal• 8 episodes of contact dermatitis with patch ( 817 pts)• No difference in site colonization between dressing
changes at 3 days or 7 days
Timsit JF, et al. JAMA 2009;301:1231-1241
Prevented 1 Major CLA-BSI per 117 Catheters

01-CHSS Blue Plus-Antimicrobial Impregnated
02-Silver Impregnated-Antimicrobial Impregnated
03-Minocycline-Rifampin-Antibiotic
04-Miconazole & Rifampicin -Antibiotic
2011 CDC Recommendations:Use a chlorhexidine/silver sulfadiazine or minocycline/rifampin -impregnated CVC in patients Rifampicin -Antibiotic
05-Benzalkonium Chloride Impregnated-Antimicrobial Impregnated
06-CHSS-Antimicrobial coated
Hockenhull JC, et al. Crit Care Med, 2009;3792): 702-712Matheos T, et al. Infect Control Hosp Epidemiol 2010;31:295-297Grady NP, et al. CDC Guidelines for the Prevention of Intravascular Catheter-Related Infections, 2011. www.cdc.gov
minocycline/rifampin -impregnated CVC in patients whose catheter is expected to remain in place >5 days if, after successful implementation of a comprehensive strategy to reduce rates of CLABSI, the CLABSI rate is not decreasing. (IA)

It is More than Just the Checklist!!!
Berenholtz et al, 2004; Tsuchida et al, 2007
It is More than Just the Checklist!!!

CUSP & CABSI Interventions
1. Educate on the Science
of Safety
CUSP CLABSI
1. Insertion
2. Maintenance
Adaptive /Cultural Technical
of Safety
2. Identify Defects (Staff
Safety Assessment)
3. Senior Executive
Partnership
4. Learn from Defects
5. Implement Teamwork
& Communication
Tools
2. Maintenance
a. Assessment & Site
Care
b. Tubing, Injection
Ports, Catheter Entry
56

Pre-Procedure Briefing Steps:
• Make introductions• Discuss patient information and procedure• Agree upon a time for line insertion• Review best practice for line insertion(if necessary)• Review best practice for line insertion(if necessary)• Nurse defines their role to physician: provide
equipment, monitor patient, provide patient comfort, observe for compliance with best practices and STOP procedure if sterile process compromised– Establish communication expectation for sterile procedure breaks– Examples include: your sleeve has touched the IV pole, the
guidewire touched the headboard

Pre-Procedure Briefing Steps:
• Identify any special supply or procedural needs
• Discuss any special patient issues (ie: patient confused, patient issues (ie: patient confused, patient awake)
• Answer any additional questions
TIME OUT: RIGHT PATIENTRIGHT PROCEDURE

• 103 ICU’s in state of Michigan reported data
• Examine 375,757 catheter days
• Implementation of the BSI Bundle/checklist
• ResultsMedian rate of CLA-BSI per 1000 catheter days went 2.7 to
Intervention to Decrease CLA-BSIStatewide Collaborative-Keystone ICU
– Median rate of CLA-BSI per 1000 catheter days went 2.7 to 0 at 3 months ((p<0.002)
– Mean rate of CLA-BSI’s per 1000 catheter days went 7.7 to 1.4 at 18 month follow up (p<0.002)
– �in mortality when compared to other mid-west states
Pronovost P et al, N Engl J Med;2006;355:2725-2732Pronovost P et al. BMJ, 2010;340:309Liptiz-Snyderman A, et al. BMJ, 2011;342:219
36 Months Post Initial Implementation: 90 of original 103 ICU’s evaluatedResults: Mean rate 1.1 per 1000 catheter days/ Median: Zero 2009: mean .88 per 1000 catheter days (personal communication)

50
60
70
80
90
100%
of
resp
on
den
ts w
ith
in a
n IC
U r
epo
rtin
g g
oo
d t
eam
wo
rk c
limat
eTeamwork Climate Across Michigan ICUs
The strongest predictor of clinical excellence:caregivers feel comfortable speaking up if they perceive a problem with patient care
60
0
10
20
30
40
50
% o
f re
spo
nd
ents
wit
hin
an
ICU
rep
ort
ing
go
od
tea
mw
ork
clim
ate
No BSI 21%No BSI 21% No BSI 44%No BSI 44%No BSI 31% No BSI 31%
No BSI = 5 months or more w/ zeroNo BSI = 5 months or more w/ zero
Health Services Research, 2006;41(4 Part II):1599.

On the CUSP: Stop BSIA National Initiative
• AHRQ government funded 3 year initiative• HRET and American Hospital Association• John Hopkins Quality & Safety Research Group• MHA’s Keystone Center for Patient Safety & Quality• Goals:• Goals:
– Eliminate CLA-BSI: <1/1000 catheter days, median 0– Improve safety culture by 50%– Learn from 1 defect a month
• Build an infrastructure for future efforts• Baseline and monthly CLA-BSI rate, hospital survey on
patient safety & monthly survey on teamwork barriers
http://www.onthecuspstophai.org/

Stop CLA-BSI: Progress Report
• Progress Report– 45 state hospital associations recruited 700 hospital & 1100
hospital teams in 2009– 14 additional states and the District of Columbia joined in
20102010– Eight states, including Puerto Rico began in 2011– � 1.8 infections per 1000 days to 1.17 infections per 1000
days central line use (RR. 35%) in 22 states (350 hospitals)– < 20% of US hospitals are participating– CDC reported 58% drop in CLA-BSI between 2001 in 2008
• 6,000 lives saved• 1.8 billion cost avoidance http://www.onthecuspstophai.org/
http:/blogs.wsj/health/2011/04/05/progress-on-reducing-bloodstream-infections/
Potential Barriers
• Perception of lack of time or the importance• Lack of evidence based education…just do it!!!!• Absence of a define protocol/procedure• Staff turnover/Replacement staff• Staff turnover/Replacement staff• Inaccessibility of needed supplies• No real clinical lead on the unit• Lack of feedback on progress• Lack of accountability/responsibility
O’keefe-McCarthy S, et al. Worldviews on Evidence Based Nursing, 2008:193-204Abott CA, et al. Worldviews on Evidence Based Nursing:2008:193-204

Implementation Framework2 more E’s
Frontline StaffTeam
Leaders
Senior
Executives
Has this become business as usual?
How do I know it will last?
Embed
How do I know it will last?
Make policies and procedures, train new
people, walk the process
Learn from each defect
Expand
Who else needs to know this?
What’s next?
Pass it on to other units
Identify and address your next challenges

Frontline StaffTeam
Leaders
Senior
Executives
Has this become business as usual?
How do I know it will last?
65
Embed
How do I know it will last?
Make policies and procedures, train new
people, walk the process
Learn from each defect
Expand
Who else needs to know this?
What’s next?
Pass it on to other units
Identify and address your next challenges

Interventions To Ensure Patient Receive Evidence & Sustain Benefit
• Education…to all caregivers…it works* • Ask Daily if line is needed• Checklist, nurse• Empower nurses
Products/Processes that make it easy for the frontline • Products/Processes that make it easy for the frontline caregiver to provide the care
• Measurement/Feedback**
• Setting targets/Celebrating successes
• Placement of new practice/education in orientation
• Simulation training of residents reduced CRBSI’s.**** Parra AP, etal. Infect Control Hosp Epidemiol 2010;31(9):964-967**Westwall S. Nursing in Critical Care, 2008;13(4):203-207*** Barsuk JH, et al. Arch Intern Med, 2009;169:1420-1423
Fuchs MA, et al. J Nurs Care Qual, 2011;26:101-109Nolan SC, et al. JONA, 2010:40(9):374-383

Ventilator Associated Associated Pneumonia

Hospital Acquired Pneumonia (HAP) and Ventilator-Associated Pneumonia(VAP)
� VAP crude mortality approximately 10-40%.� HAP crude mortality 15-18%� Pooled mean ranges 0.7 (Ped CVICU) to 7.4 (Burn
ICU) per 1000 ventilator days� HAP rates 5-15 per 1000 patient days � HAP rates 5-15 per 1000 patient days � Est cost $30,000-$40,000 per VAP � Calculated loss for VAP against matched
controls=$12,780 � Increase LOS up to 4-14 days� Annual cost $2 billion dollars.
Rello J. Chest. 2002;12:2115-2121
ATS Guidelines for HealthCare Acquired Pneumonia 2006
Coffin SE, et al. Infect Control & Hosp Epidemiol, 2008;29(1):S31-S40
Rosenthal VD, et al. Am J of Infect Control, 2008;36:627-37
Edwards JR, et al. Am J of Infect Control,
2007;35:290-301
Kollef MH, et al. Chest, 2005:128:3854-3862
Collard HR. Ann Intern Med. 2003;138:494-501
Restrepo MI, et al. Infect Control Hosp Epidemiol,
2010;31:509-515

The Vent Bundle…To the VAP Bundle
• Applying evidence-based practice• BUNDLE:
– HOB 30°, – Spontaneous Awakening Trial,– Daily assessment for SBT – Daily assessment for SBT – Oral care with an antiseptic
• 4 activities that when done 100% of the time has shown a reduction in VAP, LOS, Time on Vent, Cost and Mortality
• Additions: Mobility, Subglottal suctioning ET tube, OG vs. NGT

CUSP & VAP Interventions
1. Educate on the Science
of Safety
CUSP VAP
1. HOB > 30 degrees
2. Sedation protocol with
Adaptive /Cultural Technical
of Safety
2. Identify Defects (Staff
Safety Assessment)
3. Senior Executive
Partnership
4. Learn from Defects
5. Implement Teamwork
& Communication
Tools
2. Sedation protocol with
Spontaneous Awakening
Trial
3. Spontaneous Breathing
Trial
4. Oral care with CHG
5. Subglottal suctioning
70

European VAP Bundle
• No ventilator circuit change unless specifically indicated
• Alcohol based hand hygienehygiene
• Appropriately educated and trained staff
• Incorporation of sedation and weaning protocols
• Oral care with CHG Rello J, et al. Intensive Care Medicine, 2010;36:773-780

Wake Up and Breathe
• 333 ventilated patients randomized• All patients received “patient-targeted” sedation• Control patients receive a SBT safety screen each morning
– Oxygenation, inspiratory effort, ischemia, no vasopressors, no elevated ICP
• If pass the SBT screen, they go on to SBT
Girard et al. Lancet 2008:371:126-34

Wake Up and Breathe
Girard et al. Lancet 2008:371:126-34

Spontaneous Awakening Trial-BOTH groups getting patient targeted sedation-

Spontaneous Breathing Trial

Wake up and BreathResults
Intervention group Control goup P value
Vent free days 14.7 11.6 P=0.02
ICU LOS 9.1 12.9 P=0.01
Hosp LOS 14.9 19.2 P=0.04
Passed SBT 53 52 P=0.70

Wake Up and Breathe
32% less likely to die at one year
Girard et al.
Lancet
2008:371:126
-34

Healthcare Acquired Pneumonia
• Risk Factor Categories– Factors that increase
bacterial burden or bacterial burden or colonization
– Factors that increase risk of aspiration

Factors that Increase Bacterial Burden or Colonization
� Extreme age, severe underlying condition/ immunosuppression
� Administration of
� Lack of oral care
� Poor infection control practices
� Administration of antibiotics
� Agents which raise the gastric pH
� Withholding gastric feeding
� Mechanical ventilation
� Contaminated respiratory equipment/contaminated condensate
� Saline administration
� Immobility

Endotracheal / Nasogastric Tube/ Sinusitis
• Carriage of oropharyngeal bacteria during intubation• If cuff pressure < 20 cm 4x � risk VAP• Cuff pressure range btwn 25-40cm (JBI-Level A) with
maintenance at 25cm-30cm of H2O pressure.– Continuous monitoring resulted in a lower portion of – Continuous monitoring resulted in a lower portion of
out of range cuff pressure (11% vs. 51.7% p< 0.001)• NGT increases risk of sinusitis/gastric reflux &
increases oropharyngeal colonization• Use oral ET versus nasal (CDC-Cat IB)• Sinusitis increases the risk of nosocomial pneumonia
by 3 fold CDC. 2003 Guidelines for Prevention of Healthcare Associated Pneumonia; MMWR; 2004:53(no RR-3)Davis KA. J Intensive care Med, 2006;21(4):211-226Muscedere J & Canadian Trails Group. J of Crit Care, 2008;23:126-137Carstens J. Joanna Briggs Institute, 2010Sole, ML, et al. AJCC, 2011;20:109-117


Oropharyngeal Colonization
• 89 critically ill patients• Examined microbial colonization of the oropharynx
through out ICU stay
Methodology:
• Used pulse field gel electrophoresis to compare chromosomal DNA
Garrouste-Orgeas et. al. Am J Respir Crit Care Med. 1997;156:1647-1655
Results:
• Diagnosed 31 VAPs• 28 of 31 VAP’s the causative organism was
identical via DNA analysis

Dental Plaque
• 49 elderly nursing home residents admitted to the hospital
• Examined baseline dental plaque scores & microorganism within
Methodology:
scores & microorganism within dental plaque
• Used pulse field gel electrophoresis to compare chromosomal DNA
El-Solh AA. Chest. 2004;126:1575-1582
Results:
� 14/49 adults developed pneumonia� 10 of 14 pneumonias, the causative organism
was identical via DNA analysis

Role of Salivary Flow
• Provides mechanical removal of plaque and microorganisms
• Innate & specific immune components (IgA, cortisol, components (IgA, cortisol, lactoferrin)
• Patients receiving mechanical ventilation have dry mouth which in turn contributes to accumulation of plaque & reduced distribution of salivary immune factors
Munro CL & Grap MJ. AJCC. 2004;13:25-34
BrushCHX rinse alone
CHX rinse in CombinationCHX rinse in CombinationSwab/Clean/Moisturize
Suction
All of the above

BRUSH & SWAB
• 77% more clean approximal sites with brushing
• 44% more clean crevice sites with brushing• Benefit of brushing is directly correlated with
technique technique • Foam swabs could not remove plaque from
sheltered areas on or between teeth
Pearson LS. et. al. J of Adv Nursing. 2002;39(5):480-489
Toothbrush; grade D, Swabs; unresolved, Use of flexible suction catheter post oral cleansing; Grade D (Berry AM et al. AJCC, 2007;16:552-563)

Oral Care Reduces Pneumonia In Nursing Homes
� 11 nursing homes in Japan over 2 year period� 417 enrolled / 366 residents analyzed (death from
other causes)� 184 received oral care program/182 did not
Methodology
� 184 received oral care program/182 did not� Tooth brushing after each meal (teeth or dentures) &
1x weekly review by dentist/or hygienist
Results
No OralNo Oral Oral CareOral Care p valuep value
FebrileFebrile 29%29% 15%15% p<.01p<.01
PneumoniaPneumonia 19%19% 11%11% p<.05p<.05
DeathDeath 16%16% 7%7% p<.01p<.01
MMSEMMSE IncreaseIncrease p<.05p<.05Yoneyama et al. JAGS. 2002;50:430-433

H2 O2, Cetylpyridium Chloride (CPC) & Biotene
• >3% may cause harm, <1% no benefit in plaque removal.• Must be diluted properly, not with normal saline.• 3x a day mouth rinse with 1.5% H2 02 revealed no mucosal damage,
improved plaque scores and overall gingival health.
H2O2
CPC
West TL et. al. Journal of Peridontol. 1983; 54(6):339Tombes MA et. al. Nursing Research. 1993; 42(6):332-337Beck S. Cancer Nursing. 1979; 2:185-189.
Gunsolley JC.J Am Dent Assoc 2006;137(12):1649-57Gomes BC et.al. Clin Prev Dentistry. 1984; 6:21-25Boyd RL. et. al. J Clin Periodentol.1989; 16:557-563
CPC• Cetylpyridium chloride had significant antigingivitis
effects in several individual studies• Used in some over the counter plaque reduction rinses (Crest rinse)
Biotene• Contains salivary enzymes• Moisturize, Some oral care kits

Oral Decontamination for the Prevention of Pneumonia in Mechanically Ventilated Patients:
Systematic Review and Meta Analysis
Meta Analysis• 298 articles screened• 11randomized controlled
trials used• 3242 patients• 4 trails (1098 pts) no
Chan EY, et al. BMJ, 2007;334:889
• 4 trails (1098 pts) no significant difference with oral antibiotics
• 7 trials (2144 pts) Oral application of antiseptics significantly reduced VAP rates
• No decrease in Mortality, mechanical ventilation or LOS

Comprehensive Oral Care Program

Comprehensive Oral Care Protocol: The Good Shepherd Study
Methodology:• Retrospective study 10 bed Med-Surg• Protocol included: Covered Yankauer for
non-traumatic oral suctioning, soft-suction non-traumatic oral suctioning, soft-suction toothbrush, Suction Oral Swab, use of a 1.5% H2O2 peroxide mouth rinse for cleansing, subglottic suction catheter used 4x daily, dedicated oral suction line for infection control and ease of use.
• Education provided and presence of clinical champion.
Schleder B. et al. J Advocate Health 2002;4(1):27-30

Literature Review: Oral Care Impact of VAP
Comprehensive Oral Care:• Reduction in VAP from 5.6 to 2.2 (Schleder B. et al. J
Advocate Health 2002;4(1):27-30)• Reduction in VAP from 4.10 (2005) to (2.15) in 2006
with addition of CPC & comprehensive oral care. with addition of CPC & comprehensive oral care. Vent bundle & rotational therapy already being performed
• Reduction in VAP from 12.0 to 8.0 (p=.060) with 80% compliance, vent bundle already being preformed, 1538 patients randomized to control or study group, Additional outcomes; � vent days (p=.05), � ICU LOS (p=.05) � time to VAP (p= <.001) & reduction in mortality (p=.05) (Garcia R et al AJCC, 2009;18:523-534)

Literature Review: Oral Care Impact of VAP
Comprehensive Oral Care & CHG:• Reduction in VAP to zero for 2 years, vent bundle, mobility, oral
care & CHG with comprehensive education preformed (Murray TM et al. AACN Advanced Critical Care. 2007;18(2):190-199)
• Dickinson S et al. SCCM Critical Connections, Feb 2008

Does Compliance Make A Difference?
Oral care compliance & use of the ventilator bundle resulted in bundle resulted in a 89.7% reduction in VAP
Hutchins K, et al. Presented at APIC Annual Conference June 2008

Subglottic Secretion Drainage
Risk of VAP
Mortality
5 level 2 trials conclude that subglotticsecretion drainage is associated with a
Dezfulian C. et al. Am J of Med, 2005;118,11-18
Mortality
Risk of Early VAP
secretion drainage is associated with a reduction in VAP
Muscedere J & Canadian Trials Group. J of Crit Care, 2008;23:126-137

1 2
3 4

HOB Research
• 86 patients• Randomly assigned to supine position or HOB 45 degrees (39
semi recumbent, 47 supine)• Monitored clinical suspected & microbiologically confirmed
Methodology:
• Monitored clinical suspected & microbiologically confirmed nosocomial pneumonias
Drakulovic MB. et. al. Lancet. 1999;354:1851-1858
Results:• Microbiologically confirmed nosocomial pneumonia lower in the
semi recumbent group 2/39 (5%) vs. 11/47 (23%)• Supine position & enteral nutrition were independent risk factors
for VAP & had the greatest number of VAP’s 14/28 (50%)

HOB Research
• Methodology– Prospective multicenter trial randomly assigned to targeted 45°
vs.10°HOB– 112 to targeted 45°vs. 109 patients to 10°– Continuous measurement of backrest elevation first wk of MV– Dx of VAP by bronchoscopic techniques– Dx of VAP by bronchoscopic techniques
• Results– Baseline characteristics similar– Average elevations
• 10°group day 1 & 7: 9.8 & 16.1 • 45°group day 1 & 7: 28.1 & 22.6*
– Target 45°not achieved 85% of the time– VAP: 10°= 6.5% vs. 45°= 10.7%
Van Nieuwenhoven CA, et al. Crit Care Med, 2006;34:396-402*p < .001


Cushion Based Rotation Bed

Goldhill DR et al. Amer J Crit Care, 2007;16:50-62

CLRT to Prevent VAP
• Prospective randomized controlled trial, 3 medical ICUs at a single center
• Eligible if ventilated < 48 hours & free from pneumonia, ALI or in ARDS
• 150 patients with 75 in each group• 35 CLRT patients allocated to undergo percussion before
Methodology
• 35 CLRT patients allocated to undergo percussion before suctioning
• Measures to prevent VAP were standardized for both groups including HOB
Results: CLRT vs. Control• VAP: 11% vs. 23% p = .048• Ventilation duration: 8 + 5 days vs. 14 + 23 days, p = .02• LOS: 25 + 22 vs. 39 + 45 days, p = .01• Mortality: no difference
Staudinger t, et al. Crit Care Med, 2010;38.

CLRT Practical Challenges
• CLRT is an advance therapeutic technique• The therapy is driven by a protocol and
changes in settings are nursing orders• Yearly competency based education to • Yearly competency based education to
ensure proper use of the therapy• Monitor initial turn cycle to ensure one lung
is above the other• Automation of turning requires insertion of
usual assessment practices• Minimum of 18 hours per day & six cycles
per hour

Creative Technology
• Endotracheal tube cuff that prevents leakage through a re-design
• Impregnated endotracheal tube • Impregnated endotracheal tube that minimize the bacteria biofilm
• A phase III multicenter, prospective, randomized, controlled trial demonstrated a significant reduction of microbiologically documented– VAP (4.8% in the silver group vs.
7.5% in the control group, p < 0.05)Kollef MH, et al. Intensive Care Med, 2007:Suppl September:S65

Can we change practice through Can we change practice through process improvement alone?process improvement alone?
oror
Will successful change require Will successful change require an altering of the value structure an altering of the value structure
within the unit?within the unit?

CUSP & VAP Interventions
1. Educate on the Science
of Safety
CUSP VAP
1. HOB > 30 degrees
2. Sedation protocol with
Adaptive /Cultural Technical
of Safety
2. Identify Defects (Staff
Safety Assessment)
3. Senior Executive
Partnership
4. Learn from Defects
5. Implement Teamwork
& Communication
Tools
2. Sedation protocol with
Spontaneous Awakening
Trial
3. Spontaneous Breathing
Trial
4. Oral care with CHG
5. Subglottal suctioning
106

Be Courageous
We all are responsible for the safety of our patients……Own the Issues
•“If not this, then what??”•“If not now, then when?”•“If not me, then who??”