postpartum hemorrhage - vouch · 98%)22. conclusion of the compression suturing techniques...
TRANSCRIPT
WORLD-WIDE REPORTS
The current level of application of the B-Lynchsuture world-wide includes over 1300 success-ful cases; of these, there are only 19 failures.
The Indian subcontinent has the largest numberof reported successful applications, over 250,followed by Africa, South America, NorthAmerica, Europe and other countries. The
294
POSTPARTUM HEMORRHAGE
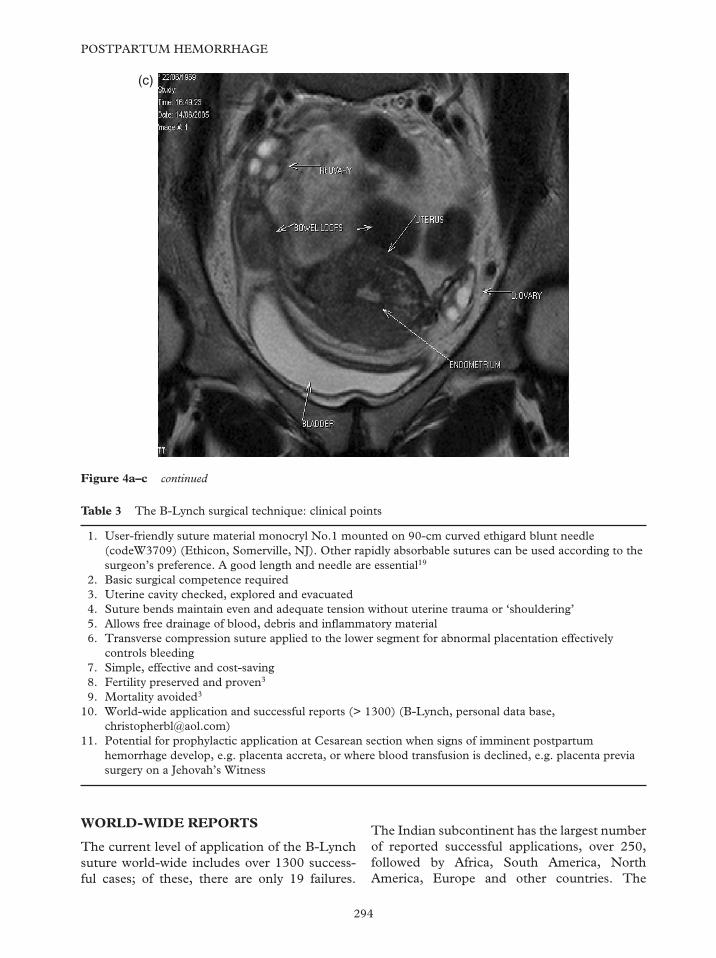
Figure 4a–c continued
1.
2.3.4.5.6.
7.8.9.
10.
11.
User-friendly suture material monocryl No.1 mounted on 90-cm curved ethigard blunt needle(codeW3709) (Ethicon, Somerville, NJ). Other rapidly absorbable sutures can be used according to thesurgeon’s preference. A good length and needle are essential19
Basic surgical competence requiredUterine cavity checked, explored and evacuatedSuture bends maintain even and adequate tension without uterine trauma or ‘shouldering’Allows free drainage of blood, debris and inflammatory materialTransverse compression suture applied to the lower segment for abnormal placentation effectivelycontrols bleedingSimple, effective and cost-savingFertility preserved and proven3
Mortality avoided3
World-wide application and successful reports (> 1300) (B-Lynch, personal data base,[email protected])Potential for prophylactic application at Cesarean section when signs of imminent postpartumhemorrhage develop, e.g. placenta accreta, or where blood transfusion is declined, e.g. placenta previasurgery on a Jehovah’s Witness
Table 3 The B-Lynch surgical technique: clinical points
(c)
316Z:\Sapiens Publishing\A5211 - Postpartum Hemorrhage\Make-up\Postpartum Hemorrhage - Voucher Proofs #T.vp30 August 2006 14:23:05
Color profile: Generic CMYK printer profileComposite Default screen
17 reported failures were because of delay inapplication, poor technique, defibrination andinappropriate material. Various suture materialshave been used. However, the monocryl suture(code WC3709) is recommended because it isuser- and tissue-friendly with uniform tensiondistribution and is easy to handle20. Holtsemaand colleagues recently opined, in a review, thatthe B-Lynch technique for postpartum hemor-rhage should be an option for every gyne-cologist21. Wohlmuth and colleagues publishedoutcome of a large series with a 91% successrate (world-wide cumulative success rate98%)22.
CONCLUSION
Of the compression suturing techniques des-cribed above, the B-Lynch procedure has beenrecommended by the 2000–2002 TriennialConfidential Enquiry into Maternal Deaths inthe United Kingdom23, The Royal College of
Obstetricians and Gynaecologists in the UK,and the Cochrane Database of systematicreviews. To date, no serious adverse outcomeshave been associated with the B-Lynch surgicaltechnique3,17,20,22,24. Furthermore, the latest2000–2002 Triennial Confidential Enquirystates that no deaths were reported in womenwho had had interventional radiology orB-Lynch suture in the management ofpostpartum hemorrhage23.
It is important to remember that, if a patientis a known or appreciated risk for postpartumhemorrhage, then the elective delivery should beperformed in the day time, with prearrangedco-operation between the imaging departmentand the obstetric team. Theater staff should bealerted in time so that conservative surgery canbe carried out quickly if needed. Patients atparticular risk are those with obesity, cardio-myopathy, coagulopathy, abnormal placenta-tion, polyhydramnios and specific religiousconvictions contraindicating blood transfusion.
PLACEMENT OF LIGATURES INSTEPWISE DEVASCULARIZATION
The essential requirements are not simple andmay not be available in every unit. First, there isa need for a competent obstetrician who is con-versant and competent at pelvic gynecologicalprocedures, and who has a working knowledgeof the pelvic anatomy, including the vascularand neurological supply of the pelvic organs.Second, there is a need for an obstetric anesthe-tist, as well as a vascular and/or gynecologicalcancer surgeon on standby. Finally, provisionsmust be available for admission postoperativelyto the intensive care unit.
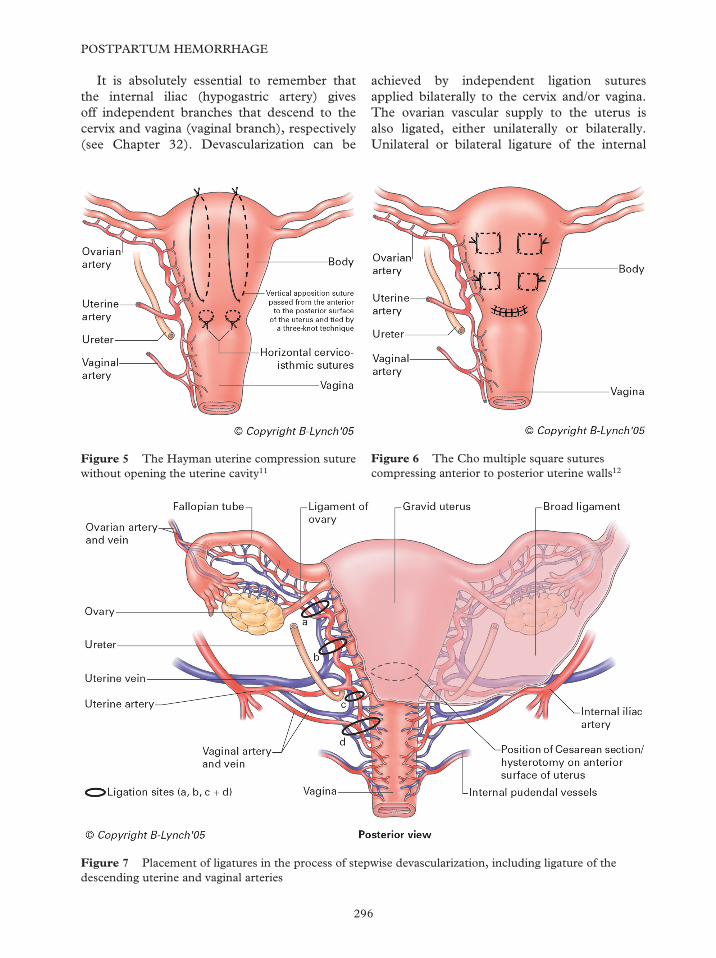
This set of requirements takes full accountof the extraordinarily generous blood supply tothe uterus and the pelvic organs (see Figure 7).The surgical approach starts with ligature of theuterine artery and its distribution to the uterus,preferably as it emerges from crossing over theureter or as it approaches the uterine wall topenetrate and establish its division25. This couldbe carried out unilaterally or bilaterally about2 cm from the uterine angle at Cesarean sectionor where the lower segment is opened after con-servative surgery for postpartum hemorrhagehas failed (Figure 8).
295
Conservative surgical management
1.
2.3.4.5.6.
Lower uterine segment or uterine cavity notopenedUterine cavity not explored under direct visionProbably quicker to applyNo feed-back data on fertility outcomeMorbidity feed-back data limitedUnequal tension leads to segmented ischemiasecondary to slippage of suture – ‘shouldering’with venous obstruction
Table 4 The Hayman uterine compression suture:clinical points
1.
2.
3.4.5.
6.
Multiple full-thickness square sutures applied,probably time-consuming if many squaresutures requiredUterine cavity drainage restriction – pyometrarisk15
No feed-back data on fertility outcomeMorbidity feed-back data limitedRhythmic contraction not facilitated andinvolution impededThe production of multiple uterine senechiae(see Chapter 24)
Table 5 The Cho multiple square sutures: clinicalpoints
317Z:\Sapiens Publishing\A5211 - Postpartum Hemorrhage\Make-up\Postpartum Hemorrhage - Voucher Proofs #T.vp30 August 2006 14:23:05
Color profile: Generic CMYK printer profileComposite Default screen
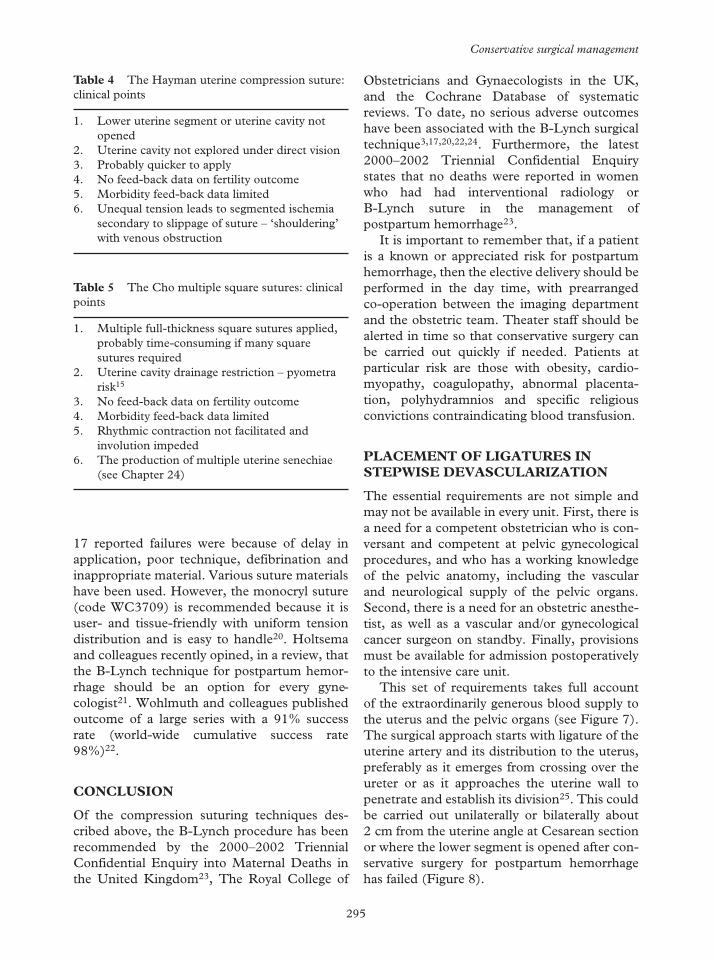
It is absolutely essential to remember thatthe internal iliac (hypogastric artery) givesoff independent branches that descend to thecervix and vagina (vaginal branch), respectively(see Chapter 32). Devascularization can be
achieved by independent ligation suturesapplied bilaterally to the cervix and/or vagina.The ovarian vascular supply to the uterus isalso ligated, either unilaterally or bilaterally.Unilateral or bilateral ligature of the internal
296
POSTPARTUM HEMORRHAGE
Figure 5 The Hayman uterine compression suturewithout opening the uterine cavity11
Figure 7 Placement of ligatures in the process of stepwise devascularization, including ligature of thedescending uterine and vaginal arteries
Figure 6 The Cho multiple square suturescompressing anterior to posterior uterine walls12
319Z:\Sapiens Publishing\A5211 - Postpartum Hemorrhage\Make-up\Postpartum Hemorrhage - Voucher Proofs #X.vp09 October 2006 15:48:29
Color profile: Generic CMYK printer profileComposite Default screen
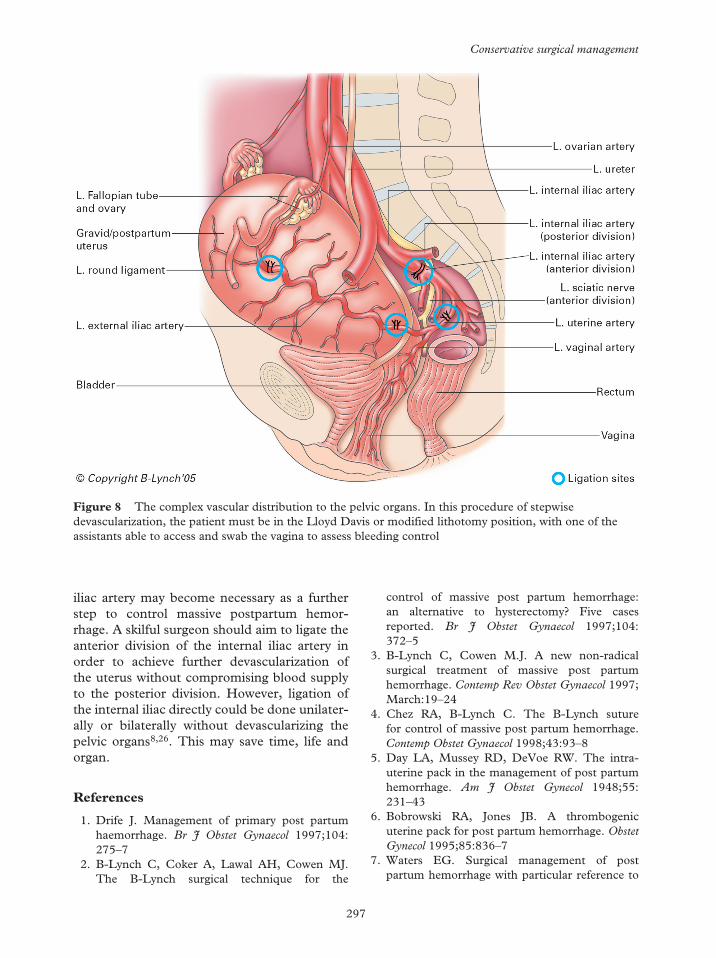
iliac artery may become necessary as a furtherstep to control massive postpartum hemor-rhage. A skilful surgeon should aim to ligate theanterior division of the internal iliac artery inorder to achieve further devascularization ofthe uterus without compromising blood supplyto the posterior division. However, ligation ofthe internal iliac directly could be done unilater-ally or bilaterally without devascularizing thepelvic organs8,26. This may save time, life andorgan.
References
1. Drife J. Management of primary post partumhaemorrhage. Br J Obstet Gynaecol 1997;104:275–7
2. B-Lynch C, Coker A, Lawal AH, Cowen MJ.The B-Lynch surgical technique for the
control of massive post partum hemorrhage:an alternative to hysterectomy? Five casesreported. Br J Obstet Gynaecol 1997;104:372–5
3. B-Lynch C, Cowen M.J. A new non-radicalsurgical treatment of massive post partumhemorrhage. Contemp Rev Obstet Gynaecol 1997;March:19–24
4. Chez RA, B-Lynch C. The B-Lynch suturefor control of massive post partum hemorrhage.Contemp Obstet Gynaecol 1998;43:93–8
5. Day LA, Mussey RD, DeVoe RW. The intra-uterine pack in the management of post partumhemorrhage. Am J Obstet Gynecol 1948;55:231–43
6. Bobrowski RA, Jones JB. A thrombogenicuterine pack for post partum hemorrhage. ObstetGynecol 1995;85:836–7
7. Waters EG. Surgical management of postpartum hemorrhage with particular reference to
297
Conservative surgical management
Figure 8 The complex vascular distribution to the pelvic organs. In this procedure of stepwisedevascularization, the patient must be in the Lloyd Davis or modified lithotomy position, with one of theassistants able to access and swab the vagina to assess bleeding control
319Z:\Sapiens Publishing\A5211 - Postpartum Hemorrhage\Make-up\Postpartum Hemorrhage - Voucher Proofs #T.vp30 August 2006 15:02:49
Color profile: Generic CMYK printer profileComposite Default screen
ligation of uterine arteries. Am J Obstet Gynecol1952;64:1143–8
8. Evans S, McShane P. the efficacy of internaliliac artery ligation in obstetric hemorrhage. SurgGynaecol Obstet 1985;160:250–3
9. Abdrabbo SA. Step-wise uterine devasculariza-tion: a novel technique for management ofuncontrollable post partum hemorrhage with thepreservation of the uterus. Am J Obstet Gynecol1999;171:694–700
10. Baskett TF. Surgical management of severeobstetric hemorrhage: experience with anobstetric hemorrhage equipment tray. J ObstetGynaecol Can 2004;26:805–8
11. Hayman RG, Arulkumaran S, Steer PJ. Uterinecompression sutures: surgical management ofpost partum hemorrhage. Obstet Gynecol 2002;99:502–6
12. Cho JH, Jun HS, Lee CN. Hemostaticsuturing technique for uterine bleeding duringcesarean delivery. Obstet Gynecol 2000;96:129–31
13. Roman A, Rebarbar A. Seven ways to controlpost partum haemorrhage. Contemp ObstetGynaecol 2003;48:34–53
14. WHO Report of Technical Working Group.The Prevention and Management of Post PartumHaemorrhage. Geneva: World Health Organisa-tion, 1999;WHO/MCH/90–7
15. Ochoa M, Allaire AD, Stitely ML. Pyometraafter hemostatic square suture technique. ObstetGynecol 2002;99:506–9
16. Ferguson JE, Bourgeois FJ, Underwood PB,B-Lynch C. Suture for post partum hemorrhage.Obstet Gynecol 2000;95:1020–2
17. El-Hammamy E, B-Lynch C. A worldwidereview of the uses of the uterine compres-sion suture techniques as alternative to
hysterectomy in the management of severepost-partum haemorrhage. J Obstet Gynaecol2005;25:143–9
18. Tsitpakidis C, Lalonde A, Danso D, B-Lynch C.Long term anatomical and clinical observationsof the effects of the B-Lynch uterine compressionsuture for the management of post partumhemorrhage – ten years on. J Obstet Gynaecol2006; in press
19. Wu HH, Yeh GP. Uterine cavity synechiae afterhemostatic square suturing technique. ObstetGynecol 2005;105:1176–8
20. Price N, B-Lynch C. Technical description ofthe B-Lynch suture for treatment of massivehemorrhage and review of published case. Int JFertil Womens Med 2005;50:148–63
21. Holtsema H, Nijland R, Huisman A, Dony J,van den Berg PP. The B-Lynch technique forpost partum haemorrhage: an option for everygynaecologist. Eur J Obstet Gynaecol Reprod Biol2004;115:39–42
22. Wohlmuth C, Gumbs J, Quebral-Ivie J. B-Lynchsuture, a case series. Int J Fertil Womens Med2005;50:164–73
23. Department of Health. Why Mothers Die:Report on Confidential Enquiries into MaternalDeaths in the United Kingdom 2000–2002Triennial Report. London: RCOG Press, 2004:94–103
24. Allam MS, B-Lynch C. The B-Lynch andother uterine compression suture techniques. IntJ Gynaecol Obstet 2005;89:236–1
25. O’Leary JA. Uterine artery ligation in the controlof post-caesarean hemorrhage. J Reprod Med1995;40:189–93
26. Clarke SL, Koonings P, Phelan JP. Placentaaccreta and prior cesarean section. Obstet Gynecol1985;66:89–92
298
POSTPARTUM HEMORRHAGE
320Z:\Sapiens Publishing\A5211 - Postpartum Hemorrhage\Make-up\Postpartum Hemorrhage - Voucher Proofs #T.vp30 August 2006 14:23:26
Color profile: Generic CMYK printer profileComposite Default screen