postoperative care of the bariatric surgery patient
TRANSCRIPT

Image source: http://www.canstockphoto.com© Can Stock Photo
Copyright © 2012 by RN.com All Rights Reserved
Reproduction and distribution of these materials is prohibited without the
express written authorization of RN.com
Postoperative Care of the Bariatric Surgery Patient
Contact Hours: 2.0
First Published: December 18, 2012 Course Expires: March 31, 2018
Acknowledgements RN.com acknowledges the valuable contributions of… Hilary Blackwood received her Bachelor's degree in Nursing from the University of North Carolina in Chapel Hill. She obtained her Master's degree in Nursing and a post-master’s certification as an Acute Care Nurse Practitioner from the University of Virginia in Charlottesville, Virginia. She worked for several years in critical care nursing, caring for burn and trauma patients, first as a bedside care nurse, then as a nurse manager. She has also practiced as a nutrition support nurse. While in Virginia, she began her work with the Weight Loss Surgery Program at the University of Virginia. She then worked with the Duke Center for Metabolic and Weight Loss for ten years, assuming responsibility for the clinical management of both preoperative and postoperative Roux-en-Y GastricBypass, Adjustable Gastric Banding, Vertical Sleeve Gastrectomy, and Bilopancreatic Diversion/Duodenal Switch patients. In September 2012 she joined WakeMed Hospital in Raleigh, North Carolina where she continues clinical practice for preoperative and postoperative bariatric surgical patients. A special thanks to the Bariatric Surgeons at WakeMed Hospital in Raleigh, North Carolina for their contributions to this program.

Disclaimer RN.com strives to keep its content fair and unbiased. The authors, planning committee, and reviewers have no conflicts of interest in relation to this course. Conflict of Interest is defined as circumstances a conflict of interest that an individual may have, which could possibly affect Education content about products or services of a commercial interest with which he/she has a financial relationship. There is no commercial support being used for this course. Participants are advised that the accredited status of RN.com does not imply endorsement by the provider or ANCC of any commercial products mentioned in this course. There is no "off label" usage of drugs or products discussed in this course. You may find that both generic and trade names are used in courses produced by RN.com. The use of trade names does not indicate any preference of one trade named agent or company over another. Trade names are provided to enhance recognition of agents described in the course. Note: All dosages given are for adults unless otherwise stated. The information on medications contained in this course is not meant to be prescriptive or all-encompassing. You are encouraged to consult with physicians and pharmacists about all medication issues for your patients. Purpose The purpose of this course is to prepare nurses for dealing with the challenges that the bariatric patient may present with during their acute and subsequent hospital admissions. This course will provide a foundation for the understanding of postoperative gastrointestinal anatomy, assist nurses in assessment and care of the obese patient, and enhance knowledge base for prompt recognition of early and long term postoperative complications associated with the treatment of bariatric surgical patients.

Learning Objectives After completion of this course you will be able to:
1. Describe the incidence of morbid obesity. 2. Explain the health implications of obesity. 3. Discuss the various surgical procedures for treatment of morbid obesity. 4. Describe the nursing interventions associated with postoperative care of the bariatric
surgery patient. 5. Identify early postoperative surgical complications and their treatments.
Introduction Obesity is an epidemic in the United States and worldwide, affecting people of both sexes, all ages, ethnic groups, and backgrounds. Severe obesity is a chronic condition that often adversely affects a person’s heath, increasing the risk of multiple health problems, and a shortened life expectancy. Bariatric surgery is an option for persons who have been unable to lose and sustain weight loss through nonsurgical methods. A strong understanding of the pathophysiology of obesity and the common surgical procedures being performed will help nurses manage patient co-morbidities and provide optimal postoperative patient care.
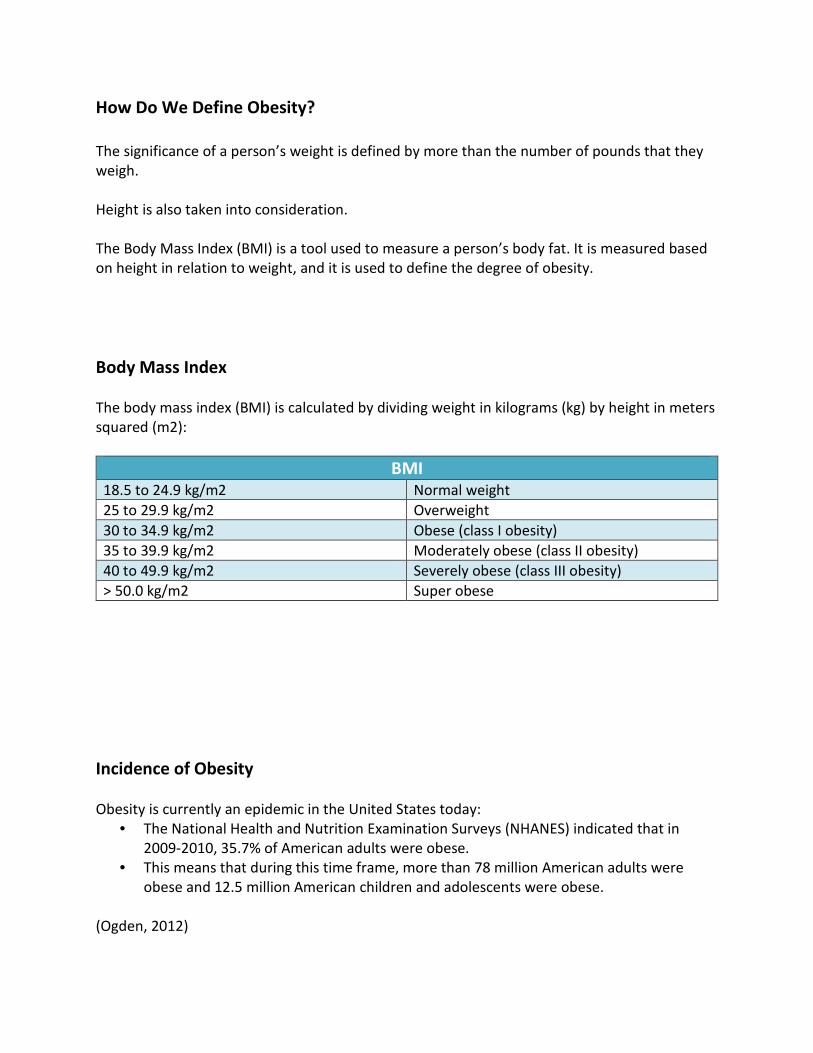
How Do We Define Obesity? The significance of a person’s weight is defined by more than the number of pounds that they weigh. Height is also taken into consideration. The Body Mass Index (BMI) is a tool used to measure a person’s body fat. It is measured based on height in relation to weight, and it is used to define the degree of obesity. Body Mass Index The body mass index (BMI) is calculated by dividing weight in kilograms (kg) by height in meters squared (m2):
BMI 18.5 to 24.9 kg/m2 Normal weight 25 to 29.9 kg/m2 Overweight 30 to 34.9 kg/m2 Obese (class I obesity) 35 to 39.9 kg/m2 Moderately obese (class II obesity) 40 to 49.9 kg/m2 Severely obese (class III obesity) > 50.0 kg/m2 Super obese
Incidence of Obesity Obesity is currently an epidemic in the United States today:
• The National Health and Nutrition Examination Surveys (NHANES) indicated that in 2009-2010, 35.7% of American adults were obese.
• This means that during this time frame, more than 78 million American adults were obese and 12.5 million American children and adolescents were obese.
(Ogden, 2012)
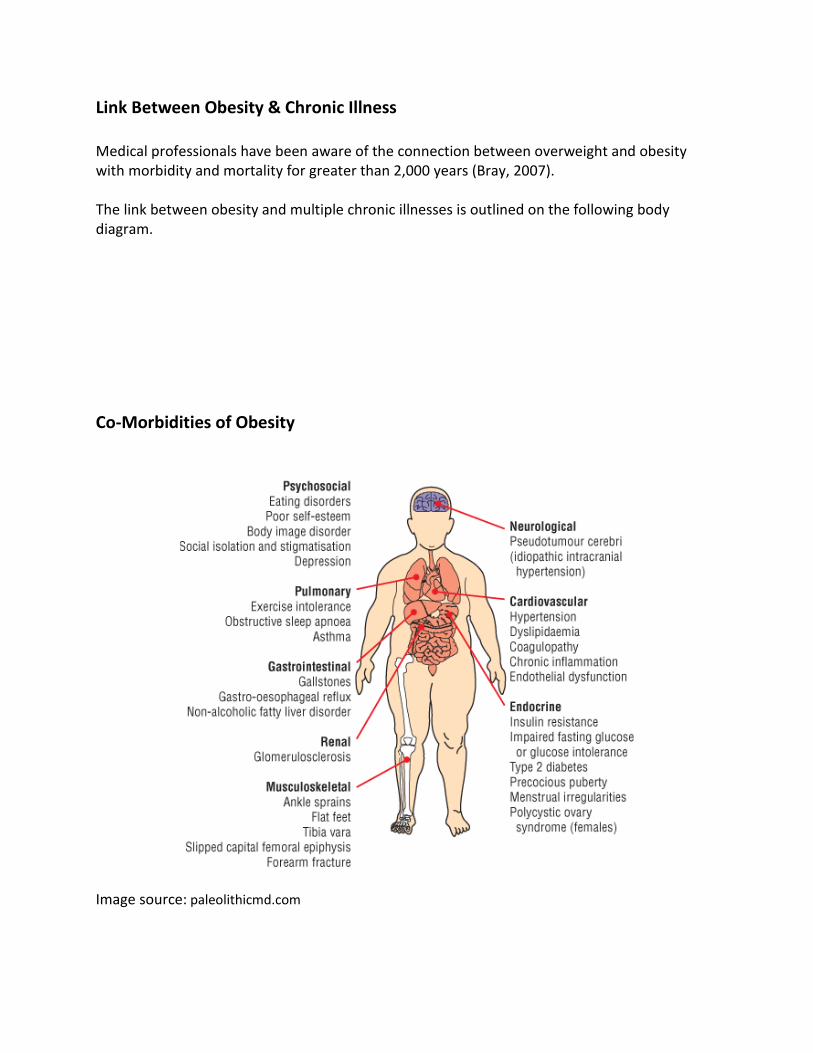
Link Between Obesity & Chronic Illness Medical professionals have been aware of the connection between overweight and obesity with morbidity and mortality for greater than 2,000 years (Bray, 2007). The link between obesity and multiple chronic illnesses is outlined on the following body diagram. Co-Morbidities of Obesity
Image source: paleolithicmd.com

The Framingham Study The Framingham Heart Study is a long-term, ongoing cardiovascular study on the residents of Framingham, Massachusetts. It is currently on the third generation of participants. In the Framingham study of 3,457 subjects of patients between the ages of 30 and 49, obese persons with a BMI 30 kg/m2 or greater at 40 years of age lived six to seven years less than those who were not obese (Peeters, 2003). Link Between Obesity & Mortality The association of BMI with overall and cause-specific mortality is best measured by long-term prospective follow-up of large numbers of people. The Prospective Studies Collaboration sought to investigate these associations by sharing data from 57 prospective studies with 894,576 participants in Western Europe and North America. BMI was found to be a strong predictor of overall mortality. At a BMI of 30-35 kg/m2, median survival is reduced by 2-4 years; at 40-45 kg/m2, it is reduced by 8-10 years (which is comparable with the effects of smoking). This represents a 30% increase in mortality for each 5 kg/m2 increase in BMI (Whitlock, 2009). Did You Know? The increase in life expectancy over the past 200 years could possibly come to an end, secondary to the increasing rise in obesity (Olshansky, 2005).
Risk Factors for Obesity What factors affect the individual development of obesity in an individual? The Causes of Obesity are Multifactorial
Genetics & Obesity Genetic factors contribute to a person’s tendency to develop obesity. Genes offer protection against starvation by allowing the body to store fat when excess food is consumed during times of abundance.
Genetics Behavior
Environment
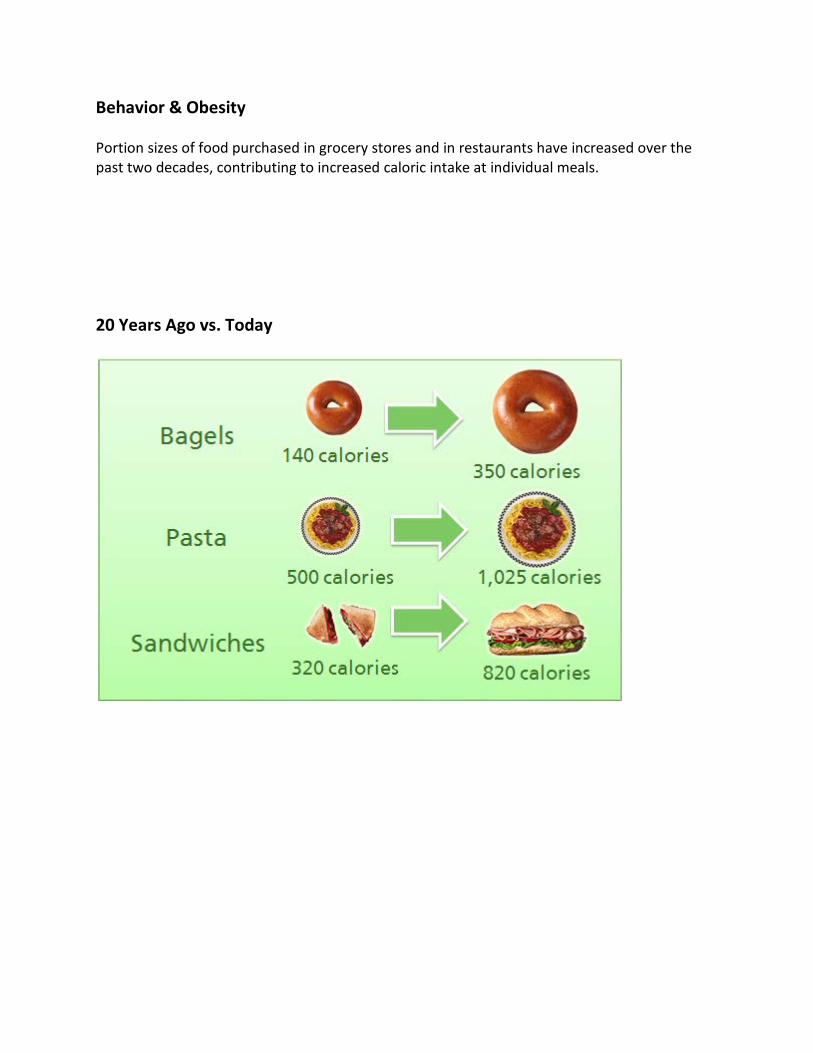
Behavior & Obesity Portion sizes of food purchased in grocery stores and in restaurants have increased over the past two decades, contributing to increased caloric intake at individual meals. 20 Years Ago vs. Today

Environment & Obesity Readily available food supply has led to a decreased need to farm or hunt our own food supply. The development of labor-saving technologies has decreased the need for physical activity. For example, more people drive a personal car or take public transportation to work, with decreased numbers of people walking or biking to work. The net result may be caloric intake > caloric expenditure leading to weight gain. What Can Be Done to Alter the Development of Obesity? Lifestyle changes may be undertaken to control a person’s weight. Useful techniques may include:
• Dieting • Behavioral modification • Exercise • Medications • Psychological counseling
Importance of Maintaining Weight Loss Weight loss of even five to ten percent can offer improvement in obesity-related medical conditions such as hypertension and type 2 diabetes. Health improvement is not maintained if the lost weight is regained, and rebound in weight gain above the pre-intervention weight is the ultimate outcome in most cases (Belle, 2007). The problem for many obese persons is not how to lose their excess weight, but rather how to sustain the loss over time.
What is Bariatric Surgery? Bariatric surgery stems from the Greek words “baros” meaning “weight”, and “iatrikos” meaning “medicine”. Bariatric surgery is an operation performed on the stomach and/or intestines for the purpose of weight loss. Who is Candidate for Bariatric Surgery? In 1991 the National Institutes of Health Consensus Conference on Gastrointestinal Surgery for Severe Obesity recommended obesity surgery for weight loss and long-term maintenance of lost weight for persons with:
• BMI > 40 kg/m2 or • BMI > 35 kg/m2 with requirement for associated co-morbidities
(NIH Conference, 1991) Guidelines for Bariatric Surgery The NIH Consensus Conference report continues to be the standard guideline used by insurance companies for initial consideration of a patient’s candidacy for bariatric surgery. In addition to meeting BMI guidelines, the patient must be able to show evidence of attempted nonsurgical weight loss without sustained success.
Restrictive & Malabsorptive Procedures Bariatric surgical procedures affect weight loss via three basic mechanisms:
1. Restriction 2. Malabsorption 3. Combination procedures
Restrictive Procedures Restrictive procedures limit solid food intake by surgically reducing the stomach capacity. The absorptive capacity of the small intestine remains wholly intact. The two commonly performed restrictive procedures are the:
1. Adjustable Gastric Band 2. Vertical Sleeve Gastrectomy
Malabsorptive Procedures Malabsorptive procedures decrease nutrient absorption by bypassing a portion of the small bowel absorptive surface area or diverting biliopancreatic enzymes that aid absorption. Combination Restrictive & Malabsorptive Procedures Some procedures provide a combination of restriction and malabsorption to promote weight loss. A surgically created small gastric pouch restricts oral intake, combined with nutrient malabsorption caused by reduction of contact between ingested nutrients and the small intestine, or diversion of digestive enzymes. Two commonly performed combination procedures are the Roux en Y Gastric Bypass (RYGB) and the Biliopancreatic Diversion (BPD) and Biliopancreatic Diversion with Duodenal Switch (BPD/DS).
Restrictive Surgeries Let’s start by examining the restrictive procedures: the Adjustable Gastric Band and the Vertical Sleeve Gastrectomy Adjustable Gastric Banding Adjustable Gastric Banding is a purely restrictive procedure that involves laparoscopic placement of a silicone band around the upper portion of the stomach, connected to an infusion port that is secured to the abdominal wall under the subcutaneous tissue. Placement of the band around the upper portion of the stomach creates a small stomach reservoir for food that holds approximately ½ cup of food. There is no interruption of bowel integrity; all nutrients are absorbed normally.
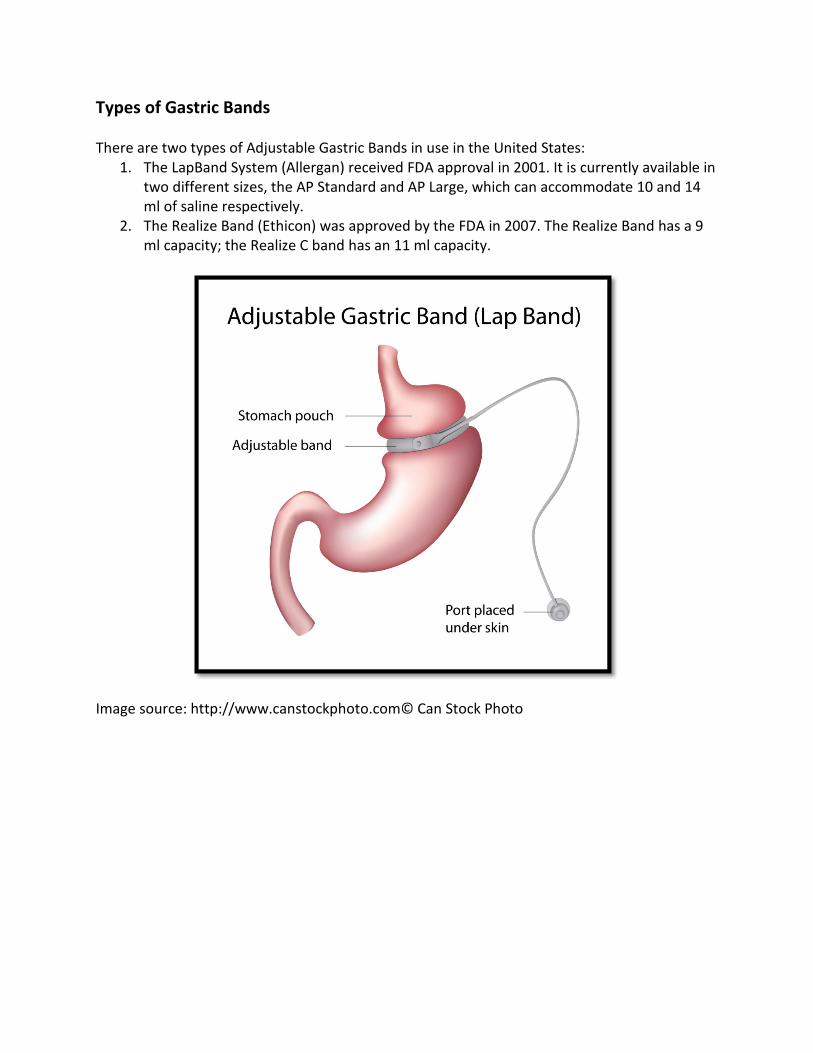
Types of Gastric Bands There are two types of Adjustable Gastric Bands in use in the United States:
1. The LapBand System (Allergan) received FDA approval in 2001. It is currently available in two different sizes, the AP Standard and AP Large, which can accommodate 10 and 14 ml of saline respectively.
2. The Realize Band (Ethicon) was approved by the FDA in 2007. The Realize Band has a 9 ml capacity; the Realize C band has an 11 ml capacity.
Image source: http://www.canstockphoto.com© Can Stock Photo
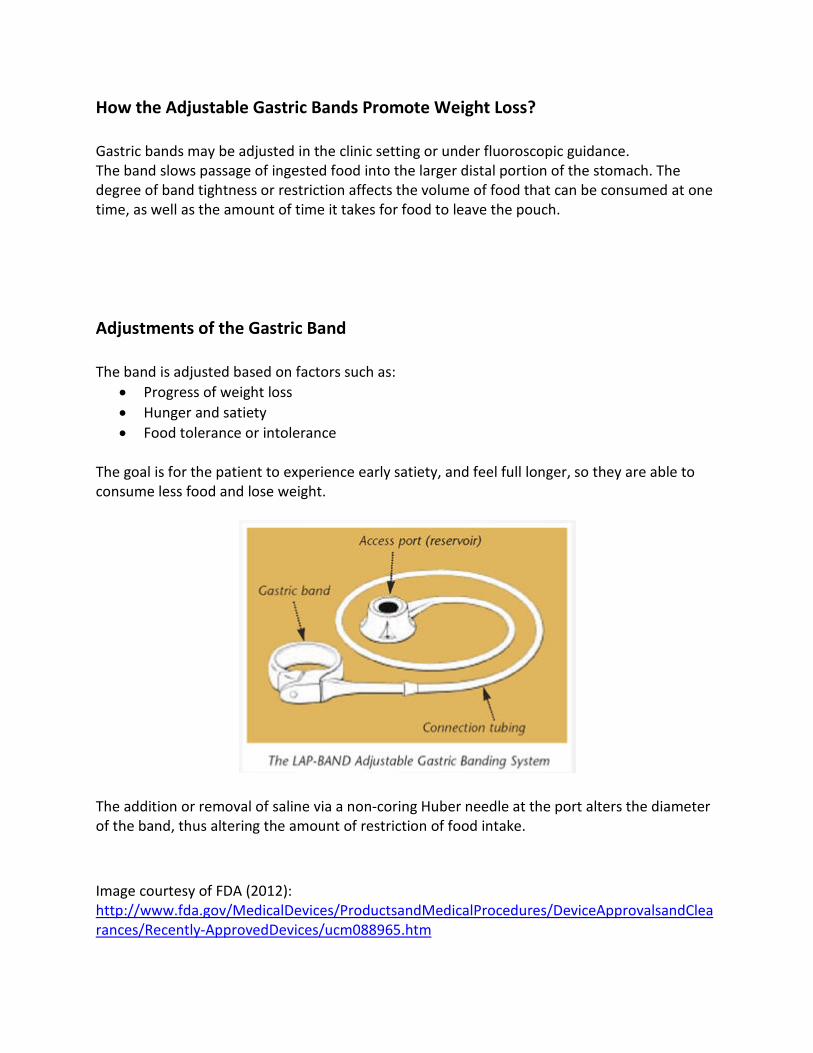
How the Adjustable Gastric Bands Promote Weight Loss? Gastric bands may be adjusted in the clinic setting or under fluoroscopic guidance. The band slows passage of ingested food into the larger distal portion of the stomach. The degree of band tightness or restriction affects the volume of food that can be consumed at one time, as well as the amount of time it takes for food to leave the pouch. Adjustments of the Gastric Band The band is adjusted based on factors such as:
• Progress of weight loss • Hunger and satiety • Food tolerance or intolerance
The goal is for the patient to experience early satiety, and feel full longer, so they are able to consume less food and lose weight.
The addition or removal of saline via a non-coring Huber needle at the port alters the diameter of the band, thus altering the amount of restriction of food intake. Image courtesy of FDA (2012): http://www.fda.gov/MedicalDevices/ProductsandMedicalProcedures/DeviceApprovalsandClearances/Recently-ApprovedDevices/ucm088965.htm

Vertical Sleeve Gastectomy This procedure is also a purely restrictive procedure. It involves a partial gastrectomy, in which the greater curvature of the stomach is excised, creating a tubular shaped stomach with significantly decreased capacity. The shape of the stomach is resistant to stretching because of absence of the fundus.
Image source: http://www.canstockphoto.com© Can Stock Photo How the Vertical Sleeve Gastrectomy Promotes Weight Loss The surgically created stomach is shaped like a tube, or banana. The smaller stomach capacity limits food consumption at one meal. The new stomach also produces less of the hormone ghrelin that causes the sensation of hunger, so the patient feels satiated with less food intake. Similarly to the Adjustable Gastric Band, there is no interruption of bowel integrity; all nutrients fully absorbed.
Combination Procedures Now let’s examine the procedures with a combination of restriction and malabsorption as the mechanism of action. These procedures are the Roux en Y Gastric Bypass, and the Biliopancreatic Diversion with a Duodenal Switch.
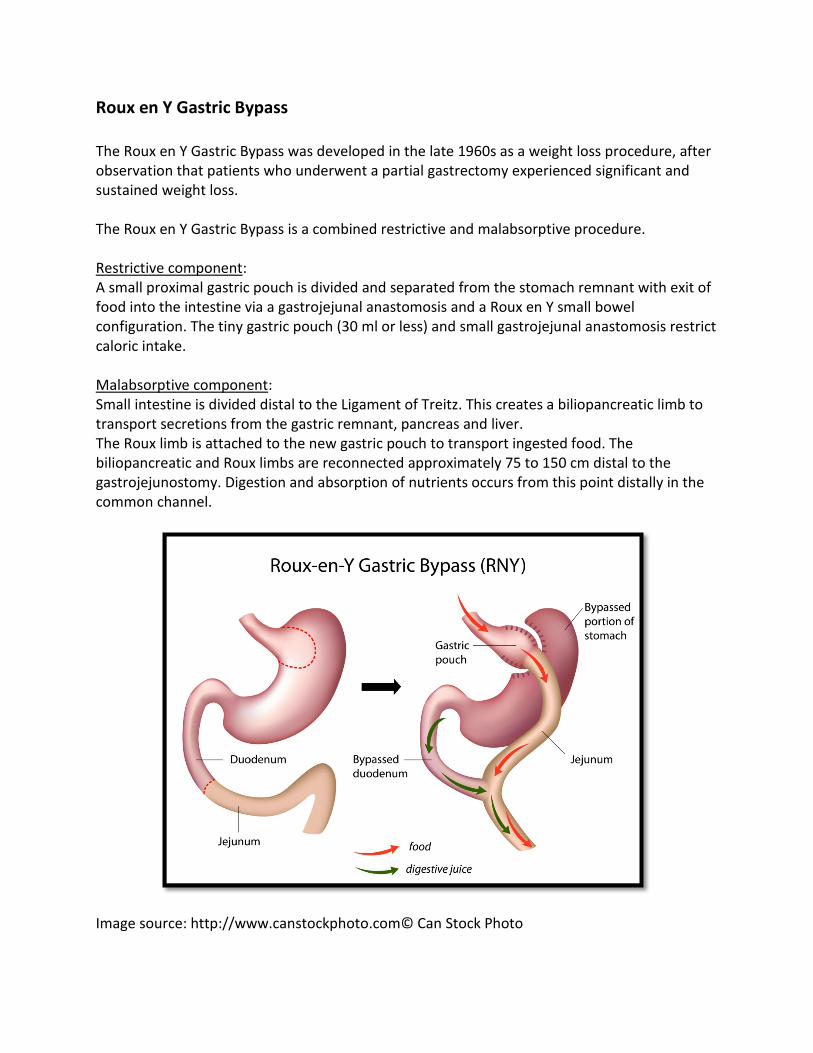
Roux en Y Gastric Bypass The Roux en Y Gastric Bypass was developed in the late 1960s as a weight loss procedure, after observation that patients who underwent a partial gastrectomy experienced significant and sustained weight loss. The Roux en Y Gastric Bypass is a combined restrictive and malabsorptive procedure. Restrictive component: A small proximal gastric pouch is divided and separated from the stomach remnant with exit of food into the intestine via a gastrojejunal anastomosis and a Roux en Y small bowel configuration. The tiny gastric pouch (30 ml or less) and small gastrojejunal anastomosis restrict caloric intake. Malabsorptive component: Small intestine is divided distal to the Ligament of Treitz. This creates a biliopancreatic limb to transport secretions from the gastric remnant, pancreas and liver. The Roux limb is attached to the new gastric pouch to transport ingested food. The biliopancreatic and Roux limbs are reconnected approximately 75 to 150 cm distal to the gastrojejunostomy. Digestion and absorption of nutrients occurs from this point distally in the common channel.
Image source: http://www.canstockphoto.com© Can Stock Photo
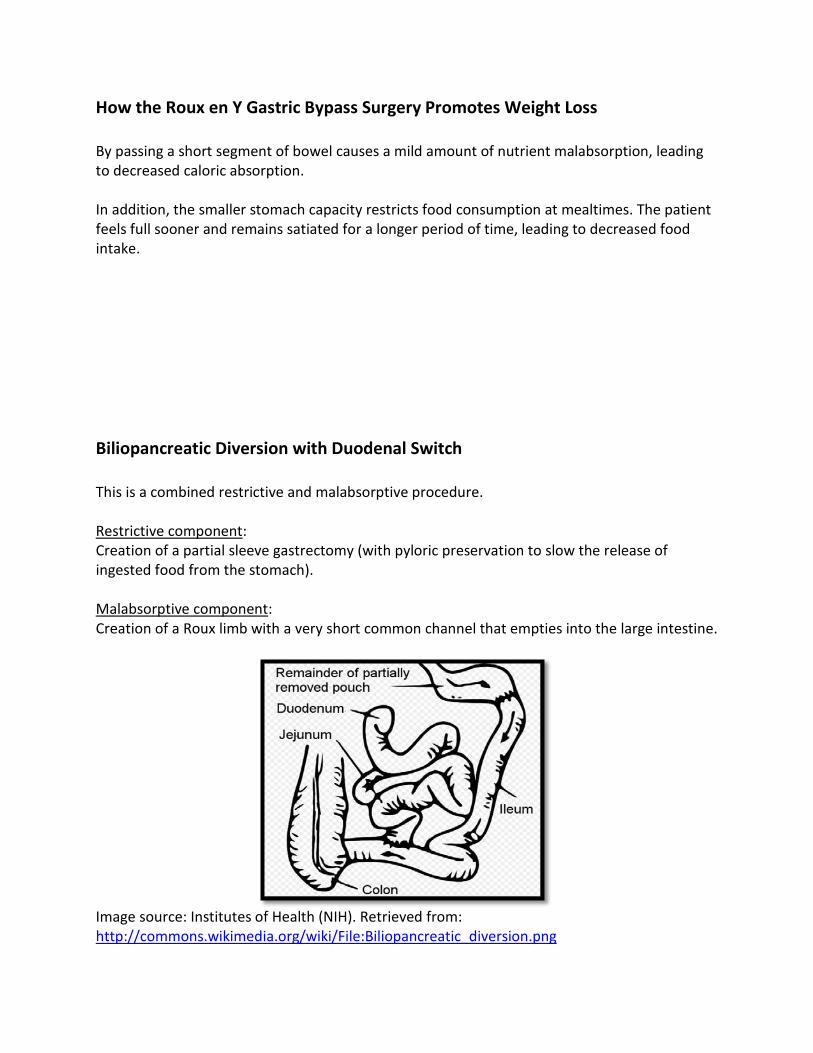
How the Roux en Y Gastric Bypass Surgery Promotes Weight Loss By passing a short segment of bowel causes a mild amount of nutrient malabsorption, leading to decreased caloric absorption. In addition, the smaller stomach capacity restricts food consumption at mealtimes. The patient feels full sooner and remains satiated for a longer period of time, leading to decreased food intake. Biliopancreatic Diversion with Duodenal Switch This is a combined restrictive and malabsorptive procedure. Restrictive component: Creation of a partial sleeve gastrectomy (with pyloric preservation to slow the release of ingested food from the stomach). Malabsorptive component: Creation of a Roux limb with a very short common channel that empties into the large intestine.
Image source: Institutes of Health (NIH). Retrieved from: http://commons.wikimedia.org/wiki/File:Biliopancreatic_diversion.png
How the Biliopancreatic Diversion Promotes Weight Loss The Biliopancreatic Diversion with Duodenal Switch works in three ways to combat obesity. First, the surgically created stomach is a gastric sleeve, with a tubular, banana shaped stomach. The smaller stomach capacity limits food consumption at one meal. The patient feels satiated sooner and longer, leading to decreased food intake. Secondly, fat absorption is significantly decreased by bypassing the duodenum. Finally, decreased contact between ingested food and biliary and pancreatic enzymes affects nutrient absorption. Obesity Affects Postoperative Assessment & Care Nurses provide the same postoperative care for obese patients as those required by non-obese patients, including hemodynamic support, airway maintenance, skin and wound care, promotion of activity and ambulation, and pain management. But obese persons often have significantly altered physiologic and anatomic characteristics.
Pathophysiology of Obesity Knowledge of the pathophysiology of obesity is essential to assist nurses in guiding the postoperative course and managing preoperative co-morbidities. In addition, assessment and care planning for an obese patient requires specialized physical assessment skills. Let’s look at the cardiovascular, pulmonary, skin integrity, mobility and pain management needs specific to care of the obese patient. Cardiovascular Considerations in Obesity Obesity causes an increase in circulating blood volume. Cardiac output also increases linearly with weight gain (0.1 L/min increase per kilogram of adipose tissue). As cardiac output rises, stroke volume rises. The result is often hypertension and cardiomegaly secondary to increased afterload. Higher circulating volume leads to increased preload, and possibly to increased right ventricular dysfunction. Cardiac Co-Morbidities of Obesity Common cardiac co-morbidities of obesity include:
• Hypertension • Atherosclerosis • Congestive heart failure • Cardiomegaly
Cardiovascular Assessment of the Obese Patient The use of a bariatric blood pressure cuff is essential for accurate blood pressure readings in the obese patient. If the patient is able to sit upright or lean forward in bed, ask them to lean forward to bring the heart closer to the chest wall, or roll to a left lateral side-lying position. Supine patients may raise their arms above their heads to spread out chest-wall soft tissues, or you may need to displace skin folds. Note that a thick chest wall obscures heart sounds in an obese person. Pulmonary Considerations in Obesity Increased fat on the chest wall makes the chest heavy and difficult to lift during normal respiration. The patient’s diaphragm may also be elevated by increased abdominal size. These factors combine to increase the work of breathing and predisposes the patient to hypoxia and closure of the small airways (atelectasis). Chronic pulmonary problems such as asthma also affect lung compliance. Pulmonary Co-Morbidities of Obesity Common pulmonary co-morbidities of obesity include:
• Obesity Hypoventilation Syndrome • Obstructive Sleep Apnea
Obesity Hypoventilation Syndrome Obesity Hypoventilation Syndrome, also known as Pickwickian syndrome, is caused by chronically shallow or slow breathing secondary to decreased lung expansion and chest wall compliance. The result is chronic hypoxia (PaO2<70 on room air) and hypercapnia (PaCO2>45MMHg). This leads to a state of chronic respiratory insufficiency. Obstructive Sleep Apnea Sleep apnea is a sleep disorder characterized by abnormally low breathing or pauses of breathing (apnea). Supine positioning during sleep leads to increased pressure on the tissue and muscles of the neck, which is worsened with relaxation during sleep or sedation. The tongue may fall back into the posterior pharynx causing obstruction of the airway and resultant decreased oxygen saturation of the blood. Hypoxia can affect heart rhythm and can cause sudden death. Sleep apnea is treated with a CPAP or BiPap machine. CPAP is continuous airway pressure delivered by a machine to keep the airway open during sleep. A BiPap machine uses variable levels of pressure to maintain airway patency. All patients with diagnosed obstructive sleep apnea should be asked to bring their CPAP or BiPAP machine with them to the hospital for use in the postoperative period.

Optimizing Pulmonary Status in the Obese In order to optimize the pulmonary status of an obese patient, the nurse can:
• Elevate the head of the patient’s bed 30-45 degrees unless contra-indicated. Obese persons may be short of breath at rest, with noted worsening upon exertion. By elevating the head of the bed, there is decreased abdominal pressure on the diaphragm and this maximizes tidal volume.
• Encourage deep breathing and coughing exercises, as well as frequent use of an incentive spirometer to prevent atelectasis and pneumonia.
Skin Concerns of Obese Patients Adipose tissue is poorly vascularized, leading to delayed wound healing. Obese patients may have skin folds over the abdomen, elbows, back, perineum, thighs and knees. The weight of large amounts of excess skin can cause tissue injury to underlying tissue and may lead to atypical pressure ulcers. Additionally, tubes and catheters may burrow into skin folds and lead to skin breakdown.
Fluid retention and a low ratio of skin to body mass may lead to excessive sweating and thus increase the risk of excoriation, rashes and infections. Neuropathy caused by diabetes may cause decreased sensitivity over pressure points.
Skin folds on an obese adult male. Courtesy of Wikipedia Public Domain. Retrieved from: http://en.wikipedia.org/wiki/File:Obesity6.JPG

Skin Assessment & Care Patients may have difficulty reaching their perineum, under the abdomen, breasts and legs, making independent toileting and bathing difficult or impossible.
• Keeping the skin clean and dry is key to prevention of skin breakdown. • Avoid use of cornstarch powders, as they promote fungal infections. • Change linens as needed and use moisture barrier ointments in the perineum to prevent
contact of urine with the skin. • Avoid the use of plastic under-pads because they trap heat and hold moisture close to
the skin. Skin Care Considerations It is important to consider skin care issues when positioning or moving an obese patient. Care should be taken to avoid shear injuries when moving a patient up in bed or over to a stretcher for transport. When the patient is re-positioned, care should be taken to prevent the patient from lying on tubes or catheters. Padding of the patient’s bedrails or chair, as well as padding for pressure points will help prevent pressure ulcers and skin tears. Pressure reducing mattresses should be considered if the patient is not mobile after recovery from anesthesia. Wound, ostomy, and continence nursing specialists should be consulted for specialized patient care concerns.
Mobility Concerns of the Obese Patient Bariatric surgery patients are at increased risk for deep vein thrombosis and pulmonary emboli secondary to venous stasis and polycythemia (elevated red blood cell count) from obesity hypoventilation. Obesity also leads to joint degeneration and osteoarthritis which may lead to chronic pain and decreased mobility. Care Considerations Regarding Mobility Sequential compression devices should be used when the patient is at rest in either the bed or the chair for prevention of deep venous thrombosis and pulmonary embolism. A foot device may provide better fit and prevent heat intolerance of long-leg devices. Low molecular weight heparin will also be ordered subcutaneously to prevent development of blood clots. It is important to assess the patient’s preoperative abilities for independent mobility and transfer, in order to prevent injury to the patient or staff member. Nurses should discuss the patient’s level of independence and preoperative need for assistive devices such as canes, walkers, wheelchairs, lifts, and slider devices in order to make comprehensive plans for transfers, getting out of bed, and ambulation.
Sequential Compression Device (SCD)
Image courtesy of Lympha Press®, 601, Sequential Compression Device (DVT Prevention) located at: http://www.biohorizonmedical.com/prevlympha-press-601-sequential-compression-device Pharmacotherapy Medication management may require alteration when a drug is administered to an obese patient. Note that pharmacokinetics is the study of what the body does to a specific drug, and how the drug is absorbed, distributed, metabolized, and excreted. Bioavailability is the proportion of a drug or other substance which enters the circulation when it is introduced into the body and is therefore able to have an active effect.
Pharmacokinetic Considerations in Obesity The pharmacokinetics may be affected by a person’s body fat percentage and medication dosing may need to be altered. Highly lipophilic (lipid affinity) drugs, such as narcotics, have a higher volume of distribution in obese persons, which may lead to longer elimination half-lives. Hydrophilic (water affinity) drugs have a limited volume of distribution and should be dosed on ideal body weight rather than actual body weight. Bioavailability Considerations in Obesity Delayed release, enteric coated, and extended release medications require a longer absorptive phase in the small intestine. Gastric bypass procedures bypass the proximal small intestine, a primary site of drug absorption. This may decrease the bioavailability of these medications. Crushable medications or liquid preparations offer more immediate release and increased bioavailability (Miller, 2006).
Morbidity & Mortality Post operative complications following bariatric surgery differ based on the surgical procedure performed, but they are documented as high as 40%. Mortality for all procedures is less than 1%. (Encinosa, 2009 & Longitudinal Assessment of Bariatric Surgery Consortium, Flum, et al, 2009) Preoperative Risk Assessment What can be done preoperatively to assess the patient’s surgical risk? Risk assessment and stratification is a very important component of care that helps to determine the patient’s surgical risk prior to bariatric surgery. A scoring system to predict mortality has been developed and validated, with body mass index, male gender, hypertension, risk of pulmonary embolus, and age determined to be the most significant risk factors. Patients are grouped into three risk categories:
1. Class A (low) is associated with a 0.3% risk of mortality 2. Class B (intermediate) has a 1.0% risk 3. Class C (high) has a 7.6% mortality risk
(DeMaria, 2007)
Early Postoperative Complications Prompt recognition and treatment of any postoperative complication is essential for optimal recovery from surgery. Early complications that may occur within one to six weeks after bariatric surgery may include:
• Deep venous thrombosis • Pulmonary embolism • Bleeding • Anastomotic leaks • Cardiovascular and/or pulmonary compromise
Deep Venous Thrombosis & Pulmonary Embolism Factors to Consider: A deep venous thrombosis, a blood clot in the deep veins of the legs, may break free and travel to the lungs or heart, causing a pulmonary embolism. A pulmonary embolism is the most common cause of mortality in the early postoperative period after bariatric surgery, accounting for up to 50% of deaths (Podnos, 2003). Causes: Common risk factors for development of a pulmonary embolism include venous stasis, obesity hypoventilation, BMI > 60, and truncal obesity (Sapala, 2003). Postoperative standard of care for prevention of deep venous thrombosis and pulmonary embolism include use of pneumatic compression devices and unfractionated or low molecular weight heparin. Presentation: The patient experiencing a deep venous thrombosis may present with a variety of symptoms including leg pain or tenderness or leg swelling or there may be no clinical symptoms. A pulmonary embolism may cause chest pain, tachypnea, cough, diaphoresis, dyspnea at rest or with exertion, or anxiety. Diagnosis: The diagnosis of deep venous thrombosis is confirmed with venous ultrasonography and D-dimer testing. A pulmonary embolus is confirmed with an IV contrast enhanced chest CT scan. Treatment: Treatment involves immediate anticoagulation in patients with a high level of clinical suspicion.
Postoperative Intra-Abdominal Bleeding Factors to Consider: Early postoperative bleeding may occur from a surgical anastomotic site or staple line, and may be intra luminal or intra abdominal. Presentation: Patients may evidence bright red blood from the mouth or rectum, sanguinous drainage from surgical drains, melena, tachycardia, decreased hematocrit, or hypotension. Treatment: Treatment consists of bolus IV fluids, serial hematocrit/hemoglobin measurements, type and cross match for packed red cells, stopping any anticoagulant therapy, checking renal function tests, careful monitoring of vital signs, and urine output. The need for insertion of a Foley catheter and placement of a large IV or central line should be considered. The patient may require surgical intervention if they remain hypotensive, the hematocrit continues to drop despite blood transfusion, or tachycardia continues for greater than four hours despite fluid bolus or blood transfusion.
Anastomotic Leaks Factors to Consider: An interruption of the gastro-jejunal anastomosis after a Roux en Y Gastric Bypass or along the staple line of a vertical sleeve gastrectomy or biliopancreatic diversion with duodenal switch is one of the most severe early postoperative complications, as it can lead to sepsis. Presentation: Early clinical symptoms of an anastomotic leak may be very subtle. Patients develop unstable vital signs with progressive tachycardia greater than 120 bpm, progressive fever > 101F, hypotension, tachypnea, hypoxemia, and decreased urine output. These are the same presenting symptoms of a pulmonary embolism, so this complication must be ruled out during evaluation. Diagnosis: Diagnosis involves abdominal CT scan, but a negative finding does not rule out a leak. Treatment: Conservative management is an option if the leak can be drained and if the patient is clinically stable. Surgical exploration for identification and repair of the leak, broad spectrum antibiotics, and external drainage may be required if the patient remains unstable or the leak is not contained. Cardiovascular Complications Cardiovascular complications after bariatric surgery may include myocardial infarction and cardiac failure. Cardiology consult to assess cardiovascular risk factors and optimize cardiac status is critical in the preoperative planning process.

Pulmonary Complications after Bariatric Surgery Atelectasis is a common finding in postoperative patients after general anesthesia, and it may be worsened in obese patients who may already have decreased pulmonary compliance secondary to an elevated diaphragm, and a large chest wall that increases the work of breathing. Patients who have been diagnosed with obstructive sleep apnea preoperatively should bring their CPAP or BiPAP machines with them to the hospital for postoperative use to promote optimal pulmonary support. Procedure Specific Complications: Roux en Y Gastric Bypass There are also potential postoperative complications specific to the bariatric surgical procedure that is performed. Possible complications following the Roux en Y Gastric Bypass procedure may include:
• Gastric remnant distension • Anastomotic stenosis • Marginal ulcers • Internal hernia
Gastric Remnant Distension after Roux en Y Gastric Bypass Surgery Gastric remnant distension occurs secondary to progressive distension of the blind remnant due to distal mechanical obstruction or paralytic ileus. If left untreated, it may lead to rupture and leakage of bile, pancreatic enzymes, acid, and bacteria into the peritoneum. Clinical symptoms include abdominal pain, shoulder pain, left upper abdomen tympany, hiccups, dyspnea, or tachycardia. Treatment consists of operative or percutaneous gastrostomy tube placement. Surgical exploration is required if perforation is suspected. Anastomotic Stenosis after Roux en Y Gastric Bypass Surgery Anastomotic stenosis is a possible post surgical complication that may present several weeks after Roux en Y Gastric Bypass Surgery. Anastomotic stenosis, or stricture, is a narrowing of the gastrojejunostomy, the stoma created at the junction of the stomach pouch and the jejunum. Patients present weeks to months after surgery with dysphagia, reflux, early satiety, nausea and vomiting, and postprandial pain. The dysphagia is progressive, with gradually increased difficulty tolerating solids, progressing to soft foods, then liquids. Diagnosis is confirmed by an upper GI series or endoscopy. Treatment is endoscopic balloon dilatation of the stricture, and more than one dilation may be necessary. Surgical revision of the stoma may be necessary to treat persistent stenosis.
Marginal Ulcers after Roux en Y Gastric Bypass A marginal ulcer is an ulcer that forms at or near the gastro-jejunal anastomosis. Potential contributing factors for ulcer development include poor tissue perfusion at the anastomosis secondary to tissue tension or ischemia, irritation from staples or non-absorbable suture material, H pylori colonization, non-steroidal drug use, and smoking. Patients present with abdominal pain that may worsen with eating and they may report gastrointestinal bleeding. Diagnosis of a marginal ulcer is made by upper endoscopy. Treatment involves acid suppression with proton pump inhibitor therapy. Patients should be instructed to avoid use of any non-steroidal medication and cease all smoking. If the ulcer is refractory to medical management or recurs after initial healing, surgical revision of the gastrojejunostomy with a truncal vagotomy is considered.
Internal Hernias after Roux en Y Gastric Bypass Surgery Internal hernias are a serious and potentially life threatening postoperative complications after Roux en Y Gastric Bypass surgery. Postoperative Roux en Y anatomy is associated with surgically created openings within the abdominal cavity. These openings create potential internal spaces, through which herniation of the small bowel can occur. The patient who presents with crampy abdominal pain, nausea and vomiting may be experiencing symptoms of an internal hernia. Internal hernias may be diagnosed with abdominal CT scan, but may be intermittent and difficult to detect. An internal hernia is considered life threatening and urgent surgical treatment is needed secondary to the risk of bowel necrosis and resultant need for bowel resection.
Procedure Specific Complications: Gastric Banding Potential complications after Gastric Banding may include:
• Port malfunction • Band slippage • Band erosion
Port Malfunction after Gastric Banding Port malfunction is caused by disconnection of the port from the connecting tubing, leakage of saline from within the system, or partial or complete disconnection of the port from the abdominal wall. Malfunction of the port causes an inability to access the port or maintain a volume of saline within the system. Port malfunction can occur at any time after surgery. Surgical intervention is required to repair or replace hardware to restore integrity of the system.
Band Slippage after Gastric Banding Band slippage is a prolapse of part of the stomach through the band, causing varied degrees of gastric obstruction. Patients present with symptoms of dysphagia, nausea and vomiting, and heartburn. Diagnosis of a slipped band can be confirmed by an upper GI. Band slippage requires decompression of the band through removal of saline. Surgical repair and repositioning of the band may be necessary. Band Erosion after Gastric Banding Band erosion is an erosion of the band through the wall of the stomach, believed to be caused by ischemia of the gastric tissue from an over-tight band, mechanical trauma from the buckle of the band, or thermal trauma during band placement. Patients may present with epigastric pain, nausea and vomiting or hematemesis, or sudden band restriction. Band erosion is diagnosed by an endoscopy. If erosion is confirmed, removal of the band is required. Removal can be done surgically or endoscopically.
Procedure Specific Complications: Vertical Sleeve Gastrectomy Potential complications after Vertical Sleeve Gastrectomy may include:
• Gastric leaks • Gastric stenosis
Gastric Leak after Vertical Sleeve Gastrectomy Gastric leaks specific to a sleeve gastrectomy occur along the staple line or at the gastroesophageal junction. Leaks along the staple line may be caused by ischemia caused by cautery during surgery. Leaks at the gastroesophageal junction may be secondary ischemia from decreased vascularity at the site. The patient may present with fever, abdominal pain, hypotension, tachypnea, tachycardia, and nausea. Diagnosis involves abdominal CT scan, but a negative finding does not rule out a leak. Conservative management is an option if the leak can be percutaneously drained and if the patient is clinically stable. Surgical exploration for identification and repair of the leak, broad spectrum antibiotics, and external drainage is required if the patient is unstable or the leak is not contained.

Stenosis after Vertical Sleeve Gastrectomy Narrowing or stenosis after a gastric sleeve can lead to obstruction of the gastric outlet. The narrowing occurs at the gastroesophageal junction, or the incisura angularis near the pylorus. Patient symptoms include dysphagia, nausea and vomiting, and possible dehydration. Treatment of stenosis is endoscopic dilation of the affected area.
Case Study One Ms. B is a 42 year old female who underwent laparoscopic placement of an Adjustable Gastric Band 18 months ago. Her height is 66 inches; preoperative weight was 240 pounds, giving her a BMI of 39. Her preoperative co-morbidities included hypertension and sleep apnea. Initial Symptoms Over the past weekend, Ms. B noted an increased sense of band restriction, as well as severe epigastric pain whenever she eats any solid food. Initially, she thought she may have simply overeaten, but the pain is present even when she eats only a few bites of food. For the past 24 hours, she has also had some nausea and vomiting, which has prompted her to present to the Emergency Room. Additional Information Upon questioning, Ms. B happily reports that she has had several band adjustments and that her band is currently “very tight”, but she is happy with it because she has lost 42 pounds since her surgery, and her Primary Care physician has discontinued her blood pressure medication. She states that she doesn’t believe that her symptoms are related to a gastrointestinal illness, because she doesn’t feel sick. She is alert and orientated, and says that the only reason she came into the ER is that her stomach hurts so much when she tries to eat. What investigations do you anticipate will be ordered? Physical Assessment Data Lab work is ordered as well as radiological studies:
• CBC (complete blood count) • CMP (complete metabolic panel) • Upper GI series
Ms. B’s vital signs are as follows:
• BP 118/76 • HR 112 • Temp 98.4 • Oxygen saturation on room air 96% • Blood sugar 92
Reviewing the Results The CBC reveals mildly elevated WBC count of 11.6; CMP is within normal limits. The upper GI series reveals emptying of contrast around the band. Ms. B is then scheduled for an upper endoscopy, in which the band is found to have eroded through the stomach wall. Ms. B is scheduled for surgical removal of her gastric band.
Case Study Two Mr. G is a 54 year old male who is post-op day two after undergoing a laparoscopic Sleeve Gastrectomy. His first postoperative day was uneventful and he is planning to go home later today. Earlier this morning, he had been walking in the hallways and talking to other patients and staff members, but when his nurse, Sheila, begins to complete discharge teaching with him, she notes that he is slightly tachypneic. She asks him how he feels and he tells her that his stomach hurts more than it did earlier, but he’s sure that he is just tired from walking in the halls. Physical Examination Sheila examines Mr. G and checks his vital signs. She finds his respiratory rate to be 18 breaths per minute, heart rate is 98, blood pressure 100/70, and oral temperature 100.4 (baseline respiratory rate is 12 bpm, HR 80, BP 136/88, T 98.8). On examination, his breath sounds are clear and his heart sounds normal. His abdomen is soft, very tender to palpation, and pain scale rating of 7/10. Sheila decides to page Mr. G’s surgeon. The surgeon cancels Mr. G’s discharge orders, orders a CBC and CMP, as well as hourly vital sign and urine output recordings, and IV fluids. He also orders a chest x ray and an abdominal CT scan. What do you suspect is happening? Progression of Symptoms Mr. G reports that he is feeling worse, and that his pain is increasing. Despite IV fluids and careful monitoring, Mr. G’s BP drops to 88/68, HR 122, T 101.4, and RR 20. His pain scale report is 8/10. Differential for the etiology of Mr G’s symptoms include pulmonary embolism, intra-abdominal bleeding, or a gastric leak.
Outcome CT scan confirmed a gastric leak along the gastric staple line. Mr. G underwent emergent surgical exploration for repair of the leak, and placement of a JP drain. He was kept NPO and given parenteral nutrition, and treated with broad spectrum of antibiotics. Over the course of the next several days, Mr. G’s vital signs normalized, his pain lessened and he felt well enough to ambulate in the halls and visit with others again. He was discharged home to complete 14 days of IV antibiotics, and he continued his TPN. Two weeks after discharge, his JP drainage was scant, vital signs stable and he was pain free. A repeat abdominal CT scan revealed no continued gastric leak, and he was able to begin oral fluid intake. Conclusion Obesity is a growing epidemic in the United States and worldwide that often adversely affects a person’s heath and decreases life expectancy. Bariatric surgery is an option for persons who have been unable to lose and sustain weight loss through nonsurgical methods. Understanding of the pathophysiology of obesity and the common surgical procedures being performed will assist nurses in managing patient co-morbidities and providing optimal postoperative patient care.

References Belle, SH, Berk, PD, Courcoulas, AP, et al. (2007). Safety and Efficacy of Bariatric Surgery: Longitudinal Assessment of Bariatric Surgery. SOARD 2007; 3:116. Bray, GA. (2007). The Battle of the Bulge: A History of Obesity Research, Dorrance, Pittsburg 2007. DeMaria EJ, Portenier, D, Wolfe, L. (2007). Obesity Surgery Mortality Risk Score: Proposal for a Clinically Useful Score to Predict Mortality Score to Predict Mortality Risk in Patients Undergoing Gastric Bypass. SOARD 2007; 3:134. DeMaria EJ. Murr M. Buryne TK, et al. (2007). Validation of the Obesity Surgery Mortality Risk Score in a Mulitcenter Study Proves it Stratifies Mortality Risk in Patients Undergoing Gastric Bypass for Morbidobesity. Ann Surg 2007; 246: 578. Encinosa, WE, Bernard, DM, Du, D, Steiner, CA. (2009). Recent Improvements in Bariatric Surgery Outcomes. Med Care 2009; 47:531. Longitudinal Assessment of Bariatric Surgery (LABS) Consortium, Flum DR, Belle SR, et al. (2009). Perioperative Safety in the Longitudinal Assessment of Bariatric Surgery. N Engl J Med 2009; 361:445. Miller, AD, Smith, KM. (2006). Medication and Nutrient Administration Considerations after Bariatric Surgery. Am J Health Syst Pharm 2006; 63:1852. NIH Conference. Gastrointestinal Surgery for Severe Obesity. (1991). Consensus Development Conference Panel. Ann Intern Med 1991; 115:956. Olshansky, SJ, Passaro, DJ, Hershow, RC, et al. (2005). A Potential Decline in Life Expectancy in the United States in the 21st Century. N Engl J Medicine 2005; 352:1138. Ogden CL, Carroll MD, Kit BK, Flegal KM. (2012). Prevalence of Obesity in the United States, 2009–2010. NCHS data brief, no 82. Hyattsville, MD: National Center for Health Statistics. Peeters A, Barendregt JJ, Willekens F. et al. (2003). Obesity in Adulthood and Its Consequences for Life Expectancy: A Life-Table Analysis. Ann Intern Med 2003; 138:24. Podnos YD, Jimenez JC, Wilson SE, et al. (2003). Complications after Laparoscopic Gastric Bypass: A Review of 3464 Cases. Arch Surg 2003; 138:957. Prospective Studies Collaboration, Whitlock, G, Lewington, S, et al. (2009). Body-Mass Index and Cause-Specific Mortality in 900,000 Adults; Collaborative Analysis of 54 Prospective Studies. Lancet 2009; 373:1083. Sapala JA, Wood MH, Schuhknecht MP, Sapala MA. (2003). Fatal Pulmonary Embolism after Bariatric Operations for Morbid Obesity: A 24 Yer Year Retrospective Analysis. Obes Surg 2003; 13:819.

Please Read This publication is intended solely for the use of healthcare professionals taking this course, for credit, from RN.com. It is designed to assist healthcare professionals, including nurses, in addressing many issues associated with healthcare. The guidance provided in this publication is general in nature, and is not designed to address any specific situation. This publication in no way absolves facilities of their responsibility for the appropriate orientation of healthcare professionals. Hospitals or other organizations using this publication as a part of their own orientation processes should review the contents of this publication to ensure accuracy and compliance before using this publication. Hospitals and facilities that use this publication agree to defend and indemnify, and shall hold RN.com, including its parent(s), subsidiaries, affiliates, officers/directors, and employees from liability resulting from the use of this publication. The contents of this publication may not be reproduced without written permission from RN.com.