polypharmacy in elderly patients:an intervention study in therapeutic management
TRANSCRIPT

POLYPHARMACY IN ELDERLY PATIENTS:
AN INTERVENTION STUDY IN THERAPEUTIC
MANAGEMENT
Rosario Falanga¹, G. Pessa¹, B. Basso²,
A. Bertoli², A. Franzo², D. Little², G. Simon² ¹General Practitioner, SIMG, Pordenone, Italy,
²Azienda per l’Assistenza Sanitaria n.5 “Friuli Occidentale”,
Pordenone, Italy
Background
The increase in average life expectancy has over time resulted in a rising incidence of chronic degenerative diseases and consequent polypharmacy in older adults, with an augmented risk of Adverse Drug Reactions (ADRs) and Potentially Inappropriate Drug Prescriptions (PIDP).
Older people are medically frail because of age-related pharmacokinetic and pharmacodynamic changes.
Deprescribing will reduce the risk of adverse drug reactions due to age-related physiological changes and inappropriate prescriptions.
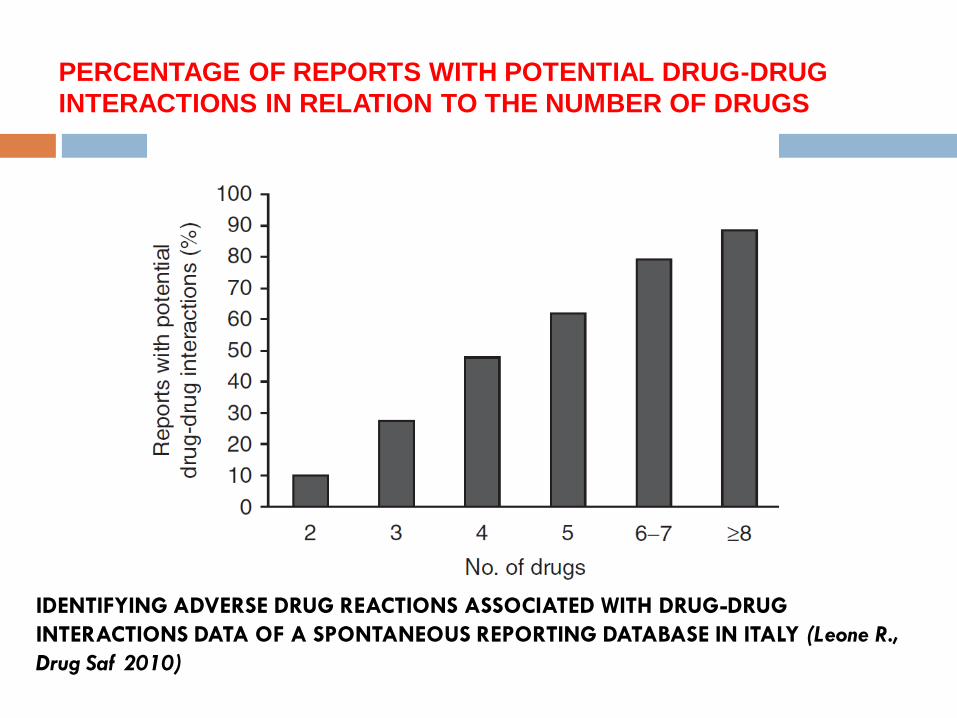
PERCENTAGE OF REPORTS WITH POTENTIAL DRUG-DRUG
INTERACTIONS IN RELATION TO THE NUMBER OF DRUGS
IDENTIFYING ADVERSE DRUG REACTIONS ASSOCIATED WITH DRUG-DRUG
INTERACTIONS DATA OF A SPONTANEOUS REPORTING DATABASE IN ITALY (Leone R.,
Drug Saf 2010)

Ippocrate (460 - 335 B.C.)
“PRIMUM NON NOCERE”
(First, do not harm)

Polypharmacy in elderly patients: an intervention
study in therapeutic management
Pharmacovigilance project financed by the Italian Medicines Agency (AIFA).
Participating Organisations and Facilities:
AAS5 “Agency for Public Health Service n.5 Western Friuli” (Office of the Medical Director, Internal Medicine Department, Pharmacy Department, Territorial Health Districts, Dept. of Mental Health, Nursing Services)
General Practitioners (SIMG, Pordenone)
Nursing homes in the Province of Pordenone
Objectives
We conducted a qualitative and quantitative
analysis of polypharmacy in elderly patients, in
therapy with multiple prescription medicines
evaluating the risk of ADRs, drug interactions
and therapeutic errors before and after
adequate staff training aimed at reducing the
number of administered drugs and ADRs in this
population.
Methods (1)
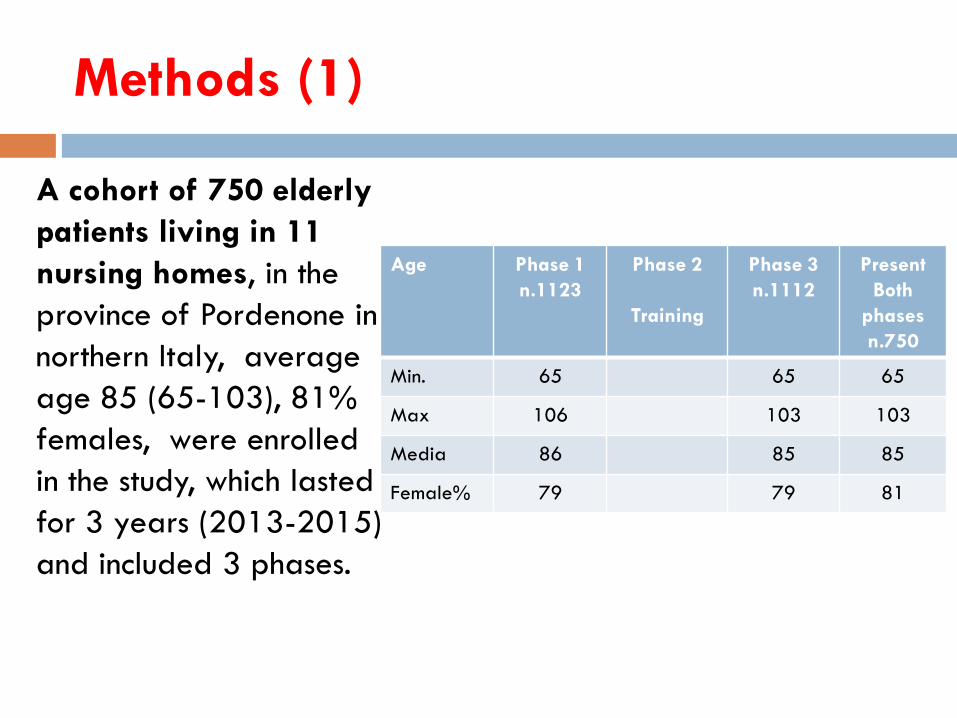
A cohort of 750 elderly
patients living in 11
nursing homes, in the
province of Pordenone in
northern Italy, average
age 85 (65-103), 81%
females, were enrolled
in the study, which lasted
for 3 years (2013-2015)
and included 3 phases.
Age Phase 1
n.1123
Phase 2
Training
Phase 3
n.1112
Present
Both
phases
n.750
Min. 65 65 65
Max 106 103 103
Media 86 85 85
Female% 79 79 81

Methods (2)
Phase 1: included medical record audit, data collection of drug therapy and drug management, evaluating the risk of ADRs, drug interactions and therapeutic errors, data analysis, problems detection and planning for adequate training.
Phase 2: we carried out multidisciplinary staff training with nurses, general practitioners, specialist doctors, pharmacists and created adequate operative tools
(“Do not crush list”, a specific handbook).
Phase 3: included a second data collection and the analysis of drug management, therapy and hospital admissions for adverse events.
The analysis was conducted using 2 tools:
Beers Criteria for potentially inappropriate medications.
Micromedex 2.0 for drug interactions.

Phase 1 - Top Ten Drug Interactions
CLORPROMAZINA
QUETIAPINA
ACIDO
ACETILSALICILICO
SERTRALINA
ACIDO
ACETILSALICILICO
ENOXAPARINA
PANTOPRAZOLO
CITALOPRAM
METOCLOPRAMIDE
CLORPROMAZINA
LEVOFLOXACINA
QUETIAPINA
LEVOFLOXACINA
CLORPROMAZINA
ALOPERIDOLO
QUETIAPINA
METOCLOPRAMIDE
ALOPERIDOLO
METOCLOPRAMIDE
QUETIAPINA
These 10 drug interactions
represent 33% of all
interactions in the study
55% of patients in
the study had at
least 1 of these
interactions.

Beers Criteria for Potentially Inappropriate Medication
Therapeutic category, Drug(s) Phase 1 Phase 3 Beers Warning
Digoxin 132 106 Avoid doses >0,125mg digoxin
Furosemide+Spironolactone 75 57 Avoid doses >25mg spironolactone
Doxazosin 38 32 Avoid as first line therapy
Antiarrhythmic drugs
(Amiodarone,Flecainide,
Propafenone, Sotalol)
67 62 Avoid as first line therapy
Proton Pump Inhibitors 750 704 Avoid use for > 8 weeks unless for
high risk patient
Benzodiazepines (Lorazepam,
Triazolan, Flurazepam)
667 651 Avoid for treatment of insomnia,
agitation or delirium

Phase 2 – Multiprofessional training (Nurses,
Pharmacists, GPs, Specialist doctors)
Session 1: we discuss, clinical risk
management, therapeutic errors
Session 2: we carry out, field training
and share procedures
Session 3: we look at therapeutic
reconciliation, pharmacovigilance and
reduce polypharmacy

The practice of crushing medications

“Do not crush list”,
a specific handbook

Results (1)
Nursing home Reconciled meds N. of Interactions Crushing
1 -1,1 -29% -37%
2 +0,1 12% -3%
3 +0,04 -26% -6%
4 -0,5 41% -33%
5 +0,7 20% 8%
6 -0,2 -1% -7%
7 +0,02 8% 18%
8 +0,7 -1% 10%
9 -0,3 -33% -22%
10 -0,5 -23% 6%
11 -0,2 12% -28%
-0,1 -7% -9%
The interventions reduced the drug interactions by 7% and the
practice of crushing medication by 9%
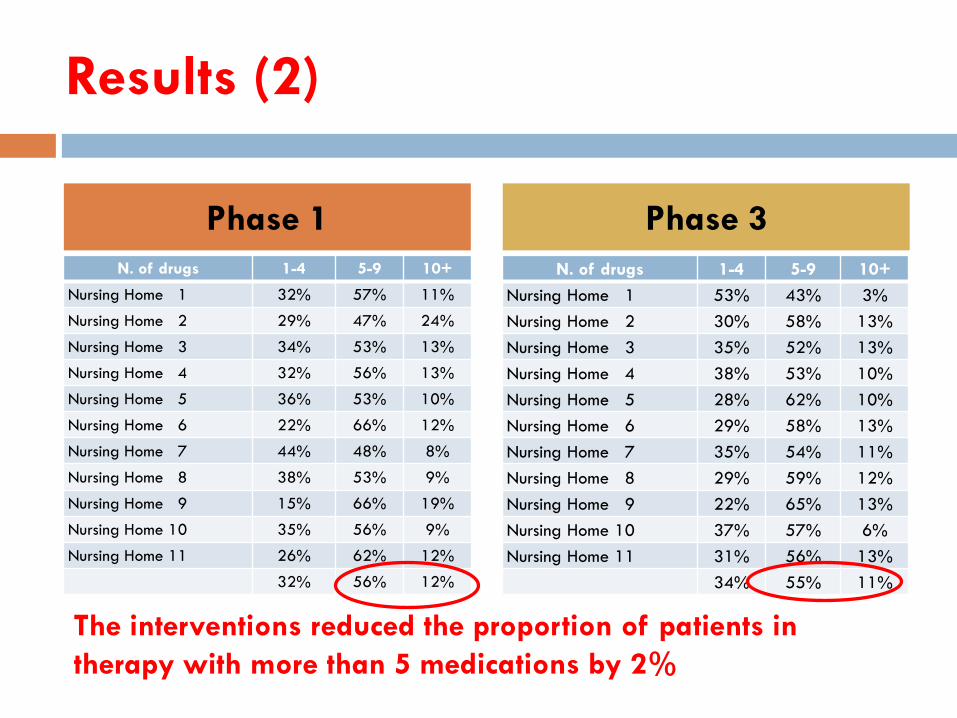
Results (2)
N. of drugs 1-4 5-9 10+
Nursing Home 1 53% 43% 3%
Nursing Home 2 30% 58% 13%
Nursing Home 3 35% 52% 13%
Nursing Home 4 38% 53% 10%
Nursing Home 5 28% 62% 10%
Nursing Home 6 29% 58% 13%
Nursing Home 7 35% 54% 11%
Nursing Home 8 29% 59% 12%
Nursing Home 9 22% 65% 13%
Nursing Home 10 37% 57% 6%
Nursing Home 11 31% 56% 13%
34% 55% 11%
Phase 1 Phase 3
N. of drugs 1-4 5-9 10+
Nursing Home 1 32% 57% 11%
Nursing Home 2 29% 47% 24%
Nursing Home 3 34% 53% 13%
Nursing Home 4 32% 56% 13%
Nursing Home 5 36% 53% 10%
Nursing Home 6 22% 66% 12%
Nursing Home 7 44% 48% 8%
Nursing Home 8 38% 53% 9%
Nursing Home 9 15% 66% 19%
Nursing Home 10 35% 56% 9%
Nursing Home 11 26% 62% 12%
32% 56% 12%
The interventions reduced the proportion of patients in
therapy with more than 5 medications by 2%
Reduce and reconcile ....
... If we remove drugs, does it
worsen the state of patients’
health?

Results (3)
Pre
Intervention
(2013)
Post
Intervention
(2015)
95%
Confidence Interval
Admissions for ADRs 610 393
Hospital days 653,600 660,866
Rate post intervention 5.95 5.37 6.56
Rate pre intervention 9.33 8.61 10.10
Rate ratio 0.64 0.56 0.72
Rate difference -3.39 -4.33 -2.44
The hospital admissions for adverse events in nursing home
residents in the post intervention group were reduced by 36%.
The difference between the two rates is statistically significant.
Conclusions
The study demonstrated how health personnel training can impact upon medication management in nursing homes.
The most significant variations were evident in facilities in which it was possible to modify nursing and medical management in a multidisciplinary approach.
The best results occurred in those facilities where all health professionals participated in the project and worked together for improvement.
