pol presentation.doc
TRANSCRIPT

Name: Shawn Johnson
Date: November 17, 2013
Course: MDSC1105 Musculo-skeletal (Locomotor) System
Group: POL 12
A 24 yr old male was shot from a buckshot rifle in his upper left forearm. The man presented to the emergency unit about 4 hours later with significant swelling of the arm. Apart from obvious pain and multiple small entry wounds, the hand was noted to be pale and there were no radial or ulnar pulses. X Rays showed fracture to the shafts of the radius and ulna bone. He was immediately prepared for and taken to the operating theatre where he had fixation of the fractures, followed by direct repair to the brachial artery which was transected and repair of the median nerve. Following the surgery the man was noted to have much more swelling of the forearm with decreased pulses 6 hours after surgery. He was again taken back to theatre for further surgery with a successful outcome.
1) Describe the histology of a typical neuron and its axon (in a peripheral nerve), and describe the changes that occur following nerve repair.
Neurons are the cells which constitute the functional units of the nervous system. Neurons are capable of transmitting electrical impulses and this provides the means of communication between receptors, the cells or organs which receive stimuli, and effectors, the tissues or organs which react to stimuli, such as muscles or glands.
Neurones may be classified according to their specific functions. Neurons which conduct impulses towards the central nervous system (the brain and spinal cord) are called sensory neurons, whilst those which conduct impulses awat from the CNS are called motor neurons. Neurons which frequently connect the sensory neurons with the motor neurons are referred to as interneurons (also known as relay neurons). Nerves of the Peripheral nervous system (PNS) contain both sensory and motor neurons.
A typical neuron is commonly composed of: 1) a cell body, 2) dentrites, 3) axon, 4) axon hillock and 4) synaptic knob/terminal.
Cell bodyEach neuron possesses a cell body (also referred to as a soma or perikaryon), which contains a nucleus, a nucleolus and the other organelles of the cell among which Groups of ribosomes and rough endoplasmic reticulum, collectively known as Nissl’s granules, as well as Golgi apparatus commonly feature.
DentritesDendrites are short filaments or extensions that branch off the cell body, forming a tree-like structure. They may extend hundreds of micrometers from the cell body. Dendrites receive information from

sensory neurons. Because the dendrites branch so extensively, the dendritic tree of a single neuron can receive input from many neurons. A highly branched dendtrite can send up to 100,000 signals to a single interneuron.
The axon and myelin sheathThe axon is a single, large filament that arises from one side of the cell body at a region called the axon hillock. The axon is by far the largest part of the neuron; its length can be tens, hundreds, or even tens of thousands of times the diameter of the soma. In humans, some axons extend up to one meter away from the soma, and the distance may be even more in other species. Each neuron has only one axon, but the axon usually has extensive branching at its end, enabling it to communicate with many other neurons. Each branch ends in a synaptic terminal that is filled with a chemical, or neurotransmitter.
The axon is surrounded by a fatty, insulating myelin sheath. In the peripheral nervous system, this sheath is formed by another type of cell called a Schwann cell. Myelin is composed of lipids (80%) and proteins (15%). It extends along the length of axons to its terminal branches. The main purpose of a myelin layer (or sheath) is to increase the speed at which impulses propagate along the myelinated fiber. The myelin sheath is interrupted at regular intervals at about 1mm by nodes of Ranvier.The nodes occur between the Schwann cells. These gaps (nodes) assist in accelerating the conduction of nerve impulses.
The axon hillockThe axon hillock is an enlarged region where an axon attaches to the cell body. It has the greatest density of sodium channels, making it the most easily-excited part of the neuron.
The synaptic knob (axon terminal)The end of an axon breaks up into many fine branches with swollen endings called synaptic knobs. These do not join directly to the next nerve cell in the pathway. Instead, there is a tiny gap across which a chemical called a neurotransmitter must pass in order to stimulate the next nerve cell (or effector). The neurotransmitter is released from the synaptic knob in response to a nerve impulse travelling along the axon. The sites of these gaps are galled synapses. Immediately below is a graphical representation of a neuron of the Peripheral nervous system.

Nerve Injury and Repair ( in the human hand)
Definition: A nerve is a cordlike structure that contains many axons, also called nerve fibres. Within a nerve, each axon is surrounded by a layer of connective tissue called the endoneurium. The axons are bundled together into groups called fascicles, and each fascicle is wrapped in a layer of connective tissue called the perineurium. Finally, the entire nerve is wrapped in a layer of connective tissue called the epineurium.
Nerve Injury (in the human hand: Nerves are quite fragile structures. An injured nerve cannot transmit nerve signals. An injured nerve can cause la lack of sensation, movement or both. Nerves are most frequently injured on the dominant hand. Ulnar and radial injuries in the fingers are the most common type of nerve injuries of the hand.

DIAGRAMATICAL REPRESENTATION OF A NERVE
Cuts, pressure, stretching, or crush injuries can cause damage to the nerves in the hand. These types of injuries result most frequently from falls, vehicle accidents, gunshot wounds, and other sources of physical trauma. Burns, freezing temperatures, electrical shock, radiation, and vibration can also cause hand nerve injuries.
A wide range and variety of nerve injury types have been classified. Two classification schemes have been practiced widely by clinicians to describe nerve injuries (see Table 1). The scheme proposed by Seddon in 1943 uses the terms neurapraxia, axonotmesis, and neurotmesis to describe the severity. The second scheme, proposed by Sunderland, divides the gamut of injury types into 5 degrees that overlap nicely with Seddon's but provide a more specific scale for grading patients.
Table 1. Clinical Progression Based on Degree of Injury
Degree Severity Description Tinel Sign
Progress Distally
Recovery Pattern
Rate of Recovery
Surgery
First Neurapraxia Demyelination with restoration in weeks
— Fast Complete Fast (days to 12 wk)
None
Second Axonotmesis Disruption of axon with regeneration and full recovery
+ + Complete Slow (3 cm/mo)
None
Third Disruption of axon and endoneurium causing disorganized regeneration
+ + Varies* Slow (3 cm/mo)
Varies
Fourth Disruption of axon, endoneurium, and perineurium, with intact
+ — None None Yes

epineurium and no regeneration
Fifth Neurotmesis Transection of the nerve + — None None Yes
Sixth Neuroma-in-continuity
Mixture of one or more of the above conditions
Varies by fascicle, depending on injury
*Recovery is at least as good as nerve repair but varies from excellent to poor, depending on the degree of endoneurial scarring and the amount of sensory and motor axonal misdirection within the injured fascicle.
N.B. Tinel’s sign (named after French neurologist Jules Tinel) is a method of detecting nerve irritation. It is performed by lightly tapping (percussing) over the nerve to elicit a sensation of tingling or "pins and needles" in the distribution of the nerve.
Nerve Repair:
All nerve injury results in a predictable response. While all the changes that occur after a nerve injury are usually considered a normal physiologic response, it is a normal response to a very abnormal situation. Depending on the type of injury, the response is different but still somewhat predictable. If the axon is spared, such as in first-degree injury, conduction is interrupted due to demyelination, but it is reinstated whenever the aggravating stimulus is removed and the myelin layers are restored. If the axon, or more, is transected, causing a second- to fifth-degree injury, the response has 2 main phases, degeneration and regeneration, and takes substantially longer.
The first phase of axon injury, degeneration, has been known as wallerian degeneration (named after British neurophysiologist Augustus Volney Waller who first described the process in 1850). Following injury, changes occur in the axon, cell body, and the Schwann cell covering of the nerve to help prepare for regeneration. Distally, the axon begins to disintegrate and undergoes apoptosis, releasing vesicles of cytosol and organelles. This same process occurs proximally, although the extent varies with the severity of injury and is eventually stopped by the regeneration process. Local Schwann cells and macrophages that migrate across the local vessels clean up the apoptotic debris, creating long, clean endoneurial tubes.
Once the debris has been removed and the macrophages have returned to the peripheral circulation, Schwann cells begin to proliferate and organize themselves into columns that lie within the endoneurial tubes, thus creating what are known as the bands of Büngner.
While the distal portion of the nerve is being cleared and prepared for reinnervation, the proximal portions of the neurons are going through a process of regeneration. Immediately after injury, the cell body swells, the nucleus becomes hypochromatic, and the production of mRNA and proteins is greatly increased. These products are transported down the axon, providing the material and energy for nerve elongation to the distal tip. While the cell body is busy making raw materials, the newly severed axon end begins to sprout, initially sending out transient axonal processes that are retracted and replaced by more permanent filopodia that contain a cytoskeleton and are capped by an expanded region known as the growth cone.

The growth cone has been shown to be the site of axon elongation and is the location of selectivity. This structure sends out many small processes that seek specific markers, which influence the axon in its movements to preferentially select neural tissue and even exhibit a preference for endoneurial tubes that have the same function. For instance, when a motor axon reaches a nerve gap, it moves across small gaps into the severed distal end and finds a motor tube to begin growing down. This helps preserve function but is not specific enough to recreate innervations identical to those that existed prior to injury. This mechanism was first described in 1898, and it has been elucidated further by Cajal (a Spanish pathologist famous for his silver staining method), and many other prominent scientists in the field of neurology.
The axon's response is known to be regulated by chemical signals that exhibit neurotropic and neurotrophic influences. Neurotropic factors are responsible for directing and attracting the regenerating axons. Neurotrophic factors are involved with inducing maturation and elongation of the axon. Macrophages, Schwann cells, and other supporting cells in the area release these chemical factors and attempt to create a microenvironment that promotes axon elongation. Limits exist on directing axon regeneration. If the nerve is too far away, the axons are not strongly attracted to the distal end and eventually stop advancing, resulting in a neuroma. If the nerve is too close, the axons cannot exhibit specificity of function, causing severely aberrant patterns of innervation at the end organ level.
Despite the systems in place for proper reinstatement of nerve function, many different events can impede axon sprouts. Depending on the severity of the injury, the proximal axon stump may have retracted. Usually, more retraction occurs with more severe injuries, and the regenerating axon requires longer sprouts to reach the nerve gap. Additionally, the possibility exists that the metabolic demands placed on the cell for regeneration exceed the capabilities of the cell, eventually leading to atrophy.
Large gaps, usually those greater than 15-30 mm, cannot be crossed reliably by axons. This is usually because proliferating Schwann cells or fibroblasts grow between the severed nerve ends and form a physical blockade. Alternatively, if suitable tissue is not found within a set distance, the axon sprouts stop proliferating and take residence in nonneural tissue, forming a neuroma. Neuromas can occur in any situation in which an axon or collateral sprout remains in nonneural tissue.
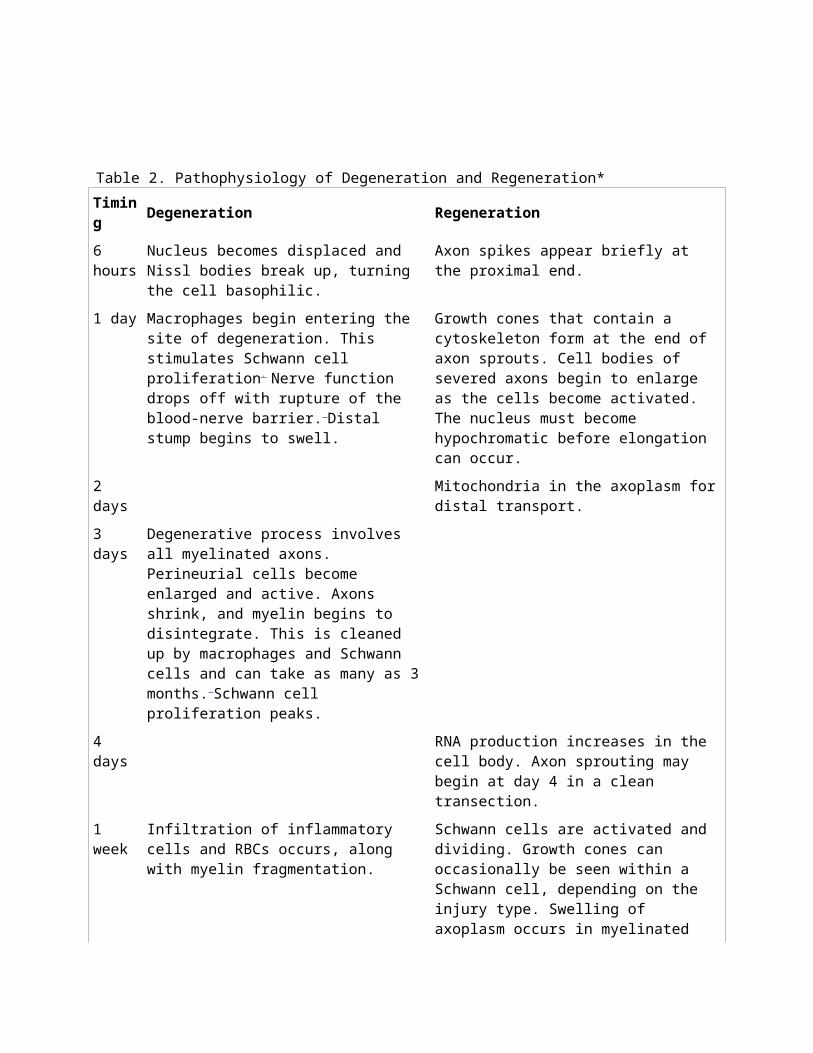
Table 2. Pathophysiology of Degeneration and Regeneration*
Timing Degeneration Regeneration
6 hours Nucleus becomes displaced and Nissl bodies break up, turning the cell basophilic.
Axon spikes appear briefly at the proximal end.
1 day Macrophages begin entering the site of degeneration. This stimulates Schwann cell proliferation. Nerve function drops off with rupture of the blood-nerve barrier. Distal stump begins to swell.
Growth cones that contain a cytoskeleton form at the end of axon sprouts. Cell bodies of severed axons begin to enlarge as the cells become activated. The nucleus must become hypochromatic before elongation can occur.
2 days Mitochondria in the axoplasm for distal transport.
3 days Degenerative process involves all myelinated

axons. Perineurial cells become enlarged and active. Axons shrink, and myelin begins to disintegrate. This is cleaned up by macrophages and Schwann cells and can take as many as 3 months. Schwann cell proliferation peaks.
4 days RNA production increases in the cell body. Axon sprouting may begin at day 4 in a clean transection.
1 week Infiltration of inflammatory cells and RBCs occurs, along with myelin fragmentation.
Schwann cells are activated and dividing. Growth cones can occasionally be seen within a Schwann cell, depending on the injury type. Swelling of axoplasm occurs in myelinated fibers, caused by mitochondria.
2 weeks
Schwann cell proliferation has peaked, and endoneurial clearance is proceeding. As the contents of the tubes are removed, they shrink; if collagen is laid down, the reduced size can become permanent.
Schwann cells near regenerating axons stop myelin destruction and surround axons.
3 weeks
The distal portion of the axon is finishing the degenerative processes, and the myelin is fragmenting.
The axon is surrounded completely by myelin, and the organelle count in the Schwann cell drops. Most of the regenerating axons are found outside the degenerating endoneurial tubes. Metabolic changes in the axon peak. Axon sprouting usually starts and can cross the anastomoses.
4 weeks
Remyelination starts and perineurial cells decrease in size once the nerve is remyelinated.
*Times can vary extensively with the type and extent of damage.
It must be noted that three major factors determine how effective nerve repair will be after surgical intervention. These are: 1) age of the patient, 2) the manner in which the nerve was injured and 3) the severity of the injury.
AgeRecovery of a nerve after surgical repair depends mainly on the age of the patient. Young children can recover close-to-normal nerve function. In contrast, a patient over 60 years old with a cut nerve in the hand would expect to recover only protective sensation; that is, the ability to distinguish hot/cold or sharp/dull.
The manner in which the nerve was injuredSharp injuries, such as a knife wound, damage only a very short segment of the nerve, availing for direct suture. In contrast, nerves that are divided by stretch or crush may be damaged over long segments.

These nerve injuries are more difficult to treat and generally have a poorer outcome. In addition, associated injuries, like injury to bone, muscle and skin, can make nerve recovery more difficult.
The severity of the injury After a nerve is repaired, the regenerating nerve endings must grow all the way to their target. For example, a nerve injured at the wrist that normally provides sensation to the thumb must grow to the end of the thumb in order to provide sensation. The return of function decreases with increased distance over which a nerve must grow.
2. Describe the arterial blood supply of the forearm and hand.
Overview
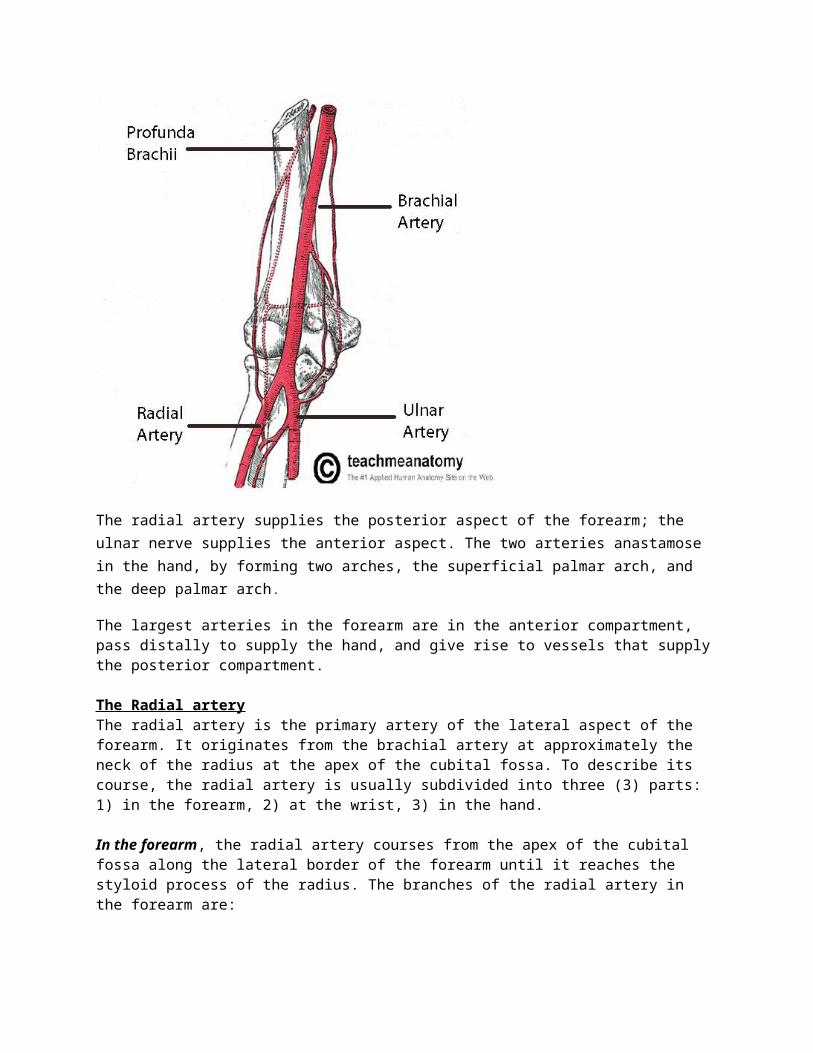
The forearm and the hand are chiefly supplied by the radial and ulnar arteries and their respective branches. Both the radial and ulnar arteries are branches of the brachial artery which descends from the upper arm. The brachial artery bifurcates (i.e. split into two) into the radial artery and the ulnar artery at the level of the neck of the radius in the cubital fossa.
The radial artery supplies the posterior aspect of the forearm; the ulnar nerve supplies the anterior aspect. The two arteries anastamose in the hand, by forming two arches, the superficial palmar arch, and the deep palmar arch.
The largest arteries in the forearm are in the anterior compartment, pass distally to supply the hand, and give rise to vessels that supply the posterior compartment.
The Radial arteryThe radial artery is the primary artery of the lateral aspect of the forearm. It originates from the brachial artery at approximately the neck of the radius at the apex of the cubital fossa. To describe its course, the radial artery is usually subdivided into three (3) parts: 1) in the forearm, 2) at the wrist, 3) in the hand.
In the forearm, the radial artery courses from the apex of the cubital fossa along the lateral border of the forearm until it reaches the styloid process of the radius. The branches of the radial artery in the forearm are:1) Radial recurrent artery which arises just after the radial artery comes off the brachial artery. It travels superiorly to anastomose with the radial collateral artery around the elbow joint
2)Palmar carpal branch of radial artery ( a small vessel) which arises near the lower border of the pronator quadratus
3)Superficial palmar branch which arises just where the radial artery is about to wind around the lateral side of the wrist.
At the wrist, the radial artery crosses the radial collateral ligament deep to the tendons of the Abductor pollicis longus and Extensor pollicis brevis to enter the “anatomical snuffbox”. The branches of the radial artery at the wrist are:
Dorsal carpal branch of radial artery , a small vessel which arises beneath the extensor tendons of the thumb.
First dorsal metacarpal artery which arises just before the radial artery passes between the two heads of the first dorsal interosseous muscle and divides almost immediately into two branches which supply the adjacent sides of the thumb and index finger; the lateral side of the thumb receives a branch directly from the radial artery.
In the hand, the radial artery pierces between the two heads of the first dorsal interosseous muscle then between the two heads of the adductor pollicis to access the deep plane of the palm . It then courses ulnarward and anastomoses with the deep palmar branch of the ulnar artery to form the deep palmar arch. The branches of the radial artery in the hand are:
Princeps pollicis artery which arises from the radial artery just as it turns medially to the deep part of the hand.

Radialis indicis which arises close to the princeps pollicis. The two arteries may arise from a common trunk, the first palmar metacarpal artery.
Deep palmar arch which is the terminal part of radial artery.
The Ulnar arteryThe ulnar artery is the chief blood vessel (transporting oxygenated blood) of the medial aspect of the forearm. It arises from the brachial artery and terminates in the superficial palmar arch, which joins with the superficial branch of the radial artery. To describe its course, the ulnar artery is usually subdivided into two (2) parts: 1) in the forearm, 2) in the hand.
In the forearm, the ulnar artery, the larger of the two terminal branches of the brachial artery,exits the cubital fossa by passing deep to the pronator teres muscle, and then passes through the forearm in the fascial plane between flexor carpi ulnaris and flexor digitorum profundus muscles.
In the distal forearm, the ulnar artery often remains tucked under the anterolateral lip of the flexor carpi ulnaris tendon, and is therefore not easily palpable. The branches of the ulnar artery in the foream are:
Ulnar recurrent artery (with anterior and posterior branches) which contribute to an anastomotic network of vessels around the elbow joint.
Common interosseous artery which itself is subdivided into posterior and anterior branches:
Anterior interosseous artery passes distally along the anterior aspect of the interosseous membrane and supplies muscles of the deep compartment of the fore arm and the radius and ulna. It has numerous branches, which perforate the interosseous membrane to supply deep muscles of the posterior compartment; it also has a small branch, which contributes to the vascular network around the carpal bones and joints. Perforating the interosseous membrane in the distal forearm, the anterior interosseous artery terminates by joining the posterior interosseous artery.
Posterior interosseous artery passes dorsally over the proximal margin of the interosseous membrane into the posterior compartment of the forearm.
Dorsal and Carpal Palmar arteries which are small arteries supplying the wrist.
In the hand, The ulnar artery enters the hand on the medial side of the wrist. The vessel lies between the palmaris brevis and the flexor retinaculum and is lateral to the ulnar nerve and the pisiform bone. Distally, the ulnar artery is medial to the hook of the hamate bone and then swings laterally across the palm, forming the superficial palmar arch. The branches of the ulnar artery in the hand are :
Deep palmar arch which arises from the medial aspect of the ulnar artery, just distal to the pisiform, and penetrates the origin of the hypothenar muscles. It curves medially around the hook of the hamate to access the deep plane of the palm and to anastomose with the deep palmar arch derived from the radial artery.
Superficial palmar arch which arises from the medial aspect of the ulnar artery, just distal to the

pisiform, and penetrates the origin of the hypothenar muscles. It curves medially around the hook of the hamate to access the deep plane of the palm and to anastomose with the deep palmar arch derived from the radial artery. The superficial palmar arch itself is also divided into two prominent vascular features. These are :1) a palmar digital artery to the medial side of the little finger and 2) three large, common palmar digital arteries, which ultimately provide the principal blood supply to the lateral side of the little finger, both sides of the ring and middle fingers, and the medial side of the index finger. These common palmar digital arteries, in turn, give rise distally to the proper palmar digital arteries.
The following image gives a more vivid description of the vascular interplay of both ulnar and radial arteries in supplying the hand with oxygenated blood.
Palm of the left hand showing the radial and ulnar arteries and their respective branches
References
Green, N. P. O., Stout, G. W., & Taylor, D. J. (1997). Biological sciences 1 & 2. (3rd ed.) Cambridge University Press.
Clugston, M., Flemming, R. (2000). Advanced chemistry. (1ˢᵗ ed.) Oxford University Press.
Drake, L.R., Mitchell, A., Vogl, W. (2004). Gray’s anatomy for students. (1ˢᵗ ed.) Curchill Livingstone.
Health Spot. (2013). Hand nerve injury and repair. Retrieved November 15, 2013, fromhttp://meddb.eznetpublish.ihealthspot.com/tabid/9153/mid/14786/ContentPubID/126/ContentClassificationGroupID/-1/Default.aspx
Medscape. (2013). Hand nerve injury repair. Retrieved October 15, 2013, fromhttp://emedicine.medscape.com/article/1287077-overview
Teach me anatomy Health. (2013). Arteries of the upper limb. Retrieved November 16, 2013, fromhttp://www.idph.state.ia.us/genetics/common/pdf/sickle_cell.pdf
