podiatry and the treatment of rheumatoid arthritis sue mcausland podiatrist, blackpool teaching...
TRANSCRIPT
Podiatry and the treatment of Rheumatoid Arthritis
Sue McAuslandPodiatrist,
Blackpool Teaching Hospitals NHS Trust
Standards /Guidelines
• NICE (2009) guidelines (CG79)• Podiatry Rheumatic Care Association (PRCA)• Arthritis and Musculoskeletal Alliance (ARMA)
Standards of Care for people with musculoskeletal conditions
• North West Clinical Effectiveness Guidelines for RA- objective to improve foot and ankle assessment an management
NICE Guidelines
• Rheumatoid Arthritis is an inflammatory disease that largely affects synovial joints which are lined with a specialised tissue called synovium.
• It typically affects the small joints of the hands and the feet, usually both sides (symmetrical), although any synovial joint can be affected.
Stats
• 400,000 in UK have RA.• 12,000 a year in UK develop RA• 2-4 times greater in woman than men• Peak age is 70, but can develop at any age • People who have synovitis of undetermined cause should
have hands and feet x-rayed• The foot is affected in nearly all people with RA eventually• In the foot, joint pain and stiffness is the most common initial
presentation, but other features eg tenosynovitis, nodule formation and tarsal tunnel syndrome may present, reflecting soft tissue involvement.
National Guidelines and Podiatry
• All People with RA and foot problems should have access to a podiatrist for assessment and periodic review of their foot health needs (NICE Recommendation 14)
• ARMA recommends people with RA should be seen by specialist within 12 weeks to confirm diagnosis and to give access to MDT access including foot health assessment- it does not have to be a podiatrist.
• Functional insoles and therapeutic footwear should be available for all people with RA if indicated (NICE Recommendation 15)

Basically
• Doing the right thing• To the right patient• In the right way• At the right time

How can RA affect the feet?
• Hallux valgus• Valgus heel deformity• Lesser toe deformities causing hard skin (callus)
formation. For some this leads to foot ulceration particularly in those with poor tissue viability
• Bacterial and fungal infections• Nail pathologies that increase risk of ulceration
and systemic infection
What are we attempting to do?
• Relieve pain• Maintain foot function• Improve quality of life• Using safe/cost effective treatments such as:– Palliative foot care– Prescribed orthoses– Specialist footwear
What do Podiatrists provide• Aiding early recognition of undiagnosed MSK disease as foot may be
first site of involvement before any other manifestation of the disease• Education – self management advice including footwear advice.
Considered the minimum standard for people with RA. Footwear flyers. British Footwear Assoc for hard to find footwear
• General foot care, nail cutting, corn and callus, padding , offloading pressure areas.
• Provision of orthoses• Monitoring of risk factors due to RA such as ulcerations, skin
conditions• Treatment of ulcers• Referral for surgical opinion when joints become unmanageable

Callus on feet
• Should we remove it?• Argument for and against.• Callus removed – does it help pain relief. Needs
to be often to be of benefit• Callus removal may be necessary to expose an
ulcer.• Argument against suggest that pressure relief is
more effective management in the long-term with use of orthoses.
Fungal infections
• At increased risk with immuno-suppressed• Increased risk of ulcer underneath nail if left
untreated
• Treatment:• Take nail clippings/ positive result treat with
oral meds/nail lacquer
Ingrowing toenails
• Mild condition• Conservative + antibiotics (where indicated)
• Severe condition– Partial or total nail removal
– Biologics – may complication treatment path /consult rheumatologist
Orthoses
• Early intervention for symptomatic pain– To help reduce pain and prevent further deformity
• Advanced problems• May prevent tissue breakdown for poor tissue
• Types of insoles:– Simple cushioning– Insoles with padding– Contoured padding (custom or off-shelf)
Footwear
• Where do we start!
• Ill fitting footwear

What makes a good shoe
• Stable/firm heel• Extended heel counter• Padded topline• No prominent internal seams• Increase toe spring or rocker sole• Low laced for ease of access
• Useful website: www.britfoot.com
Can’t find a suitable shoe on the high street?
• Refer to surgical appliances• Stock or bespoke shoes
• Beware there are cosmetic downsides
• Consider surgery- as an alternative
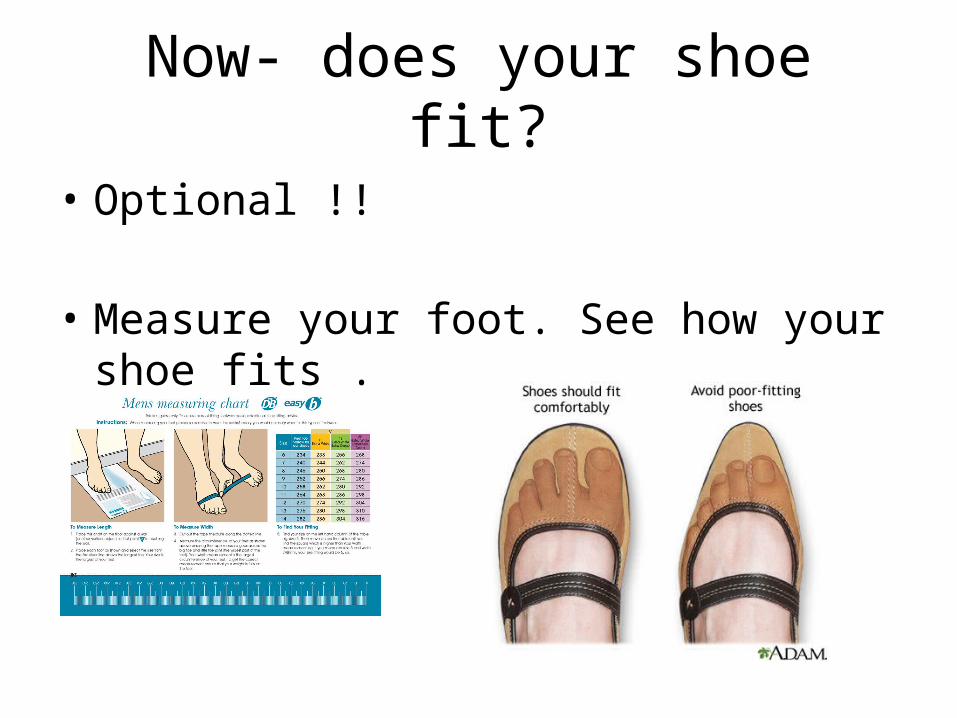
Now- does your shoe fit?
• Optional !!
• Measure your foot. See how your shoe fits .
• I hope you found this useful.
• Thank you for listening.
• Any question?