pneumocystis carinii, an opportunist in immunocompromised ... · carinii is required to establish...
TRANSCRIPT

CLINICAL MICROBIOLOGY REVIEWS, Apr. 1991, p. 137-149 Vol. 4, No. 2
0893-8512/91/020137-13$02.00/0Copyright © 1991, American Society for Microbiology
Pneumocystis carinii, an Opportunist inImmunocompromised Patients
M. S. BARTLETT* AND J. W. SMITH
Department of Pathology, Division of Clinical Microbiology, N340 University Hospital,Indiana University School of Medicine, Indianapolis, Indiana 46202-5250
INTRODUCTION............................ 137TAXONOMY............................ 137EPIDEMIOLOGY............................ 138PATHOLOGY AND PATHOGENESIS ............................ 138CLINICAL MANIFESTATIONS............................ 139LABORATORY DIAGNOSIS............................ 139TREATMENT............................ 141REFERENCES............................ 144
INTRODUCTION
Although Pneumocystis carinii was described in 1909 byChagas (29), who believed it to be a form of Trypanosomacruzi, it was not appreciated as a pathogen of humans untilyears later, when there were epidemics of "plasma cellpneumonia" (65) in malnourished infants in European or-phanages at the end of World War II. Gajdusek (59) alertedpediatricians in the United States to the threat of Pneumo-cystis pneumonia in children with immune deficiencies.Sporadic cases or clusters of cases of Pneumocystis pneu-monia were reported in patients receiving immunosuppres-sive therapy for transplantation or malignancy (52, 133).Pneumocystis pneumonia was a frequent cause of severedisease in children being treated for acute lymphocyticleukemia (195) and in transplant patients, but overall, P.carinii was considered an uncommon pathogen. Even so,with the advent of trimethoprim-sulfamethoxazole (TMP-SMX) for prophylaxis of patients known to be at risk (89),the incidence of Pneumocystis pneumonia declined until theepidemic of AIDS. The occurrence of Pneumocystis pneu-monia in apparently healthy homosexual men (51) was one ofthe first factors that led to recognition of the epidemic ofAIDS. Today P. carinii is a major cause of life-threateningpneumonia in immunocompromised patients, occurring in upto 80% of patients with AIDS. Morphologic detection of P.carinii is required to establish the diagnosis and institute anappropriate therapy.
TAXONOMYThe genus Pneumocystis has been considered to contain
one or several species (65). Because strains from humans,rats, and other animals have not been clearly differentiated,most reports use the species P. carinii for all Pneumocystisorganisms. In 1976, Frenkel (53) proposed that Pneumocys-tis organisms from humans be called Pneumocystis jiroveci;however, that nomenclature has not been used widely.Recently, Hughes and Gigliotti (87) proposed retaining thename P. carinii but following it with the Latin designation forthe host genus so that organisms from humans would becalled P. carinii Humanus and Pneumocystis from ratswould be designated P. carinii Rattus. Whether this system
* Corresponding author.
will be adopted remains to be seen. It is also not clearwhether there are strain differences among Pneumocystisorganisms from the same host species. Pulsed-field gelelectrophoresis has been used to study Pneumocystis spp.from humans and rats. Two groups of researchers haveshown that there are differences in organisms isolated fromthe same host species (82, 116). Hong et al. presented datathat suggest two Pneumocystis strains coinfected one rat.Because most karyotype studies have been done with organ-isms separated from rat lung and because the organism hasbeen variously reported as having 16 to 20 (197), 17 to 22(82), and 13 (116) chromosomes, it is possible that contam-inating rat lung DNA is being included in the evaluations.
In addition to uncertainty as to species, subspecies, andstrain differences, the taxonomic position of the organismshas yet to be decided. One investigator even proposed thatP. carinii is a mitochondrion (15). Early literature containsarguments supporting the inclusion of Pneumocystis spp.among the fungi (37) or the protozoa (95). Some argumentsfor including it among the fungi probably resulted from thegrowth of colonizing yeast cells from samples of lung tissuecultured on fungal medium. Arguments for including Pneu-mocystis spp. among the protozoa were based on morpho-logic similarities between Pneumocystis spp. and variousprotozoa. Vavra and Kucera (182) favored inclusion ofPneumocystis spp. among the fungi because the character-istic organelles of protozoa, such as rhoptries, subpelliculartubules, and conoids, could not be demonstrated in theirultrastructural studies.
Recently, there have been several reports of taxonomicassignments based on evaluations of rRNA. Edman et al.(44), evaluating sequences of 16S-like rRNA, concluded thatthe organism is most closely related to the yeast genusSaccharomyces. Sogin and Edman (172) also found that the16S-like rRNA contains a group I intron, the first report ofsuch an intron in a fungal nuclear rRNA gene. On the otherhand, Watanabe et al. (189), comparing the 5S rRNA ofPneumocystis carinii with that of other organisms, suggesteda close relationship with Rhizopoda, Myxomycota, andZygomycota but not with fungi such as Saccharomyces spp.A study of the 16S-like rRNA of Giardia lamblia showedthat Giardia rRNA was more similar to that of bacteria thanthat of other protozoa (173).As technology provides new methods of assessing rela-
tionships among organisms, there may be many changes in
137
on February 27, 2019 by guest
http://cmr.asm
.org/D
ownloaded from

138 BARTLETT AND SMITH
traditional taxonomy. For the construction of meaningfulphylogenetic trees, it will be necessary to use sequencesfrom a type species as a standard for comparison withsequences from other organisms and to use standardizedtechniques of sequence preparation and analysis. Currentknowledge of evolutionary relationships may be faulty, andrelatedness diagrams may thus be inaccurate. It has beensuggested that a better understanding of the relationship ofP. carinii to other eucaryotes will be a natural consequenceof the in-depth studies now being carried out (54, 84).
EPIDEMIOLOGY
It is well documented that healthy animals may becomeinfected when housed with infected animals (12, 55, 76). Foryears, researchers have capitalized on the airborne transmis-sion of Pneumocystis spp. in maintaining infected rat colo-nies. Although person-to-person transmission has not beendocumented, clusters or outbreaks of infection suggest thatthis occurs (161, 168). The reports of hundreds of cases ofPneumocystis pneumonia in children in institutions or othercrowded conditions in the years following World War II alsopoint to person-to-person spread. Certainly, epidemics orclusters of cases of Pneumocystis pneumonia, beginningwith the epidemics in Western Europe, outbreaks in hospi-tals (31, 49, 159), and outbreaks in organ transplant units (72,161, 176) suggest person-to-person transmission. A report ofincreased incidence of Pneumocystis infection in immuno-suppressed patients without AIDS in an institution wherethere was an increased incidence of AIDS is suggestive (74).Whether strains differ in their abilities to be transmitted andinfect various hosts is not known. It has been demonstratedthat most children in the United States and the Netherlandsacquire antibody to the organisms by the age of 4 years (122,137). Work by Kovacs et al. (101) showed that none of seveninfants had antibody specific to P. carinii but that seven ofeight normal adults did have specific antibody. It is thuspresumed that the organisms are commonly present in theenvironment.
Differences in organisms from rats and humans have beendescribed by various workers (101, 187), suggesting that ifinfections are acquired by transfer across species lines, thehosts then modify the organisms. It is possible that P. carinjihas an as yet undiscovered life stage that does not require amammalian host or that there are dormant stages that persistin plants and soil. The one condition required for prolifera-tion sufficient to cause pneumonia in any recognized hostappears to be suppression of the host immune response.Pneumocystis pneumonia has been seen in most countries
of the world, but its prevalence varies. There are specificcase reports from Johannesburg (139), Puerto Rico (32), andScandinavia (109), while in North America, approximately60 to 80% of patients with AIDS develop Pneumocystispneumonia at least once. In contrast, it is estimated that inAfrica, only 7% of patients with AIDS develop Pneumocys-tis pneumonia. Although few cases of Pneumocystis pneu-monia have been reported from Africa (46, 114), the diseaseis seen in African patients in Europe (17). Whether this muchlower African infection incidence results from differences inthe virulence ofPneumocystis strains in Africa or from a lowincidence of subclinical (latent) infection in the population orboth is not known. Furthermore, although plasma cell pneu-monia caused by P. carinii was originally described inchildren in orphanages of Western Europe, such infectionstill occurs. For example, there have been recent reports ofinfection in adopted Vietnamese infants (45, 78, 152).
PATHOLOGY AND PATHOGENESIS
Traditionally, Pneumocystis pneumonia has been diag-nosed by pathologists examining sections of lung tissue. Theoriginal descriptions of organism-host cell interactions werebased on appearances of pulmonary lesions in hematoxylin-eosin stains. The foamy eosinophilic exudate and "honey-comb" appearance of the lung tissue were described ashallmarks of Pneumocystis pneumonia. Cysts could be re-vealed in this exudate by using methenamine-silver nitratestains.With additional techniques for the evaluation of tissue and
fluid specimens and with a much larger number of casestudies, a great deal more has been learned about theinfection processes. P. carinii proliferates as a trophozoiteform that appears to preferentially associate with type Ipneumocytes (198) by apposition of parasite and host cellmembranes. It has been suggested that type II pneumocytesare sometimes affected (113). A damaging "aggressive"parasite attachment (73) to host cells was demonstrated byelectron microscopy. The Pneumocystis trophozoites dam-age pneumocytes and cause desquamation of alveolar liningcells. Proliferation of Pneumocystis trophozoites, formationof cysts, and host response to the damaged tissue lead tofilling of the alveoli with the foamy exudate described above.Host immune globulins are associated with the Pneumocys-tis exudate (21, 26).
P. carinii may occasionally elicit other host responses.Granulomatous pulmonary lesions (18, 19, 36, 75) and cavi-tary lung disease (47, 140) have been described. However, itis important to note that patients with AIDS may haveclinical and morphologic evidence of pulmonary damage inwhich there is no evidence of an etiologic agent (148). Thehost cell population in bronchoalveolar lavage specimensfrom patients with P. carinii pneumonia has fewer alveolarmacrophages and more neutrophils than specimens frompatients with adult respiratory distress syndrome (50).
Various pathogenic mechanisms have been postulated(175). The organisms produce foci of necrosis and cellulardebris in extrapulmonary sites (146). It has been suggestedthat fibronectin plays a role in specific binding (143) and thatthere is cytoskeletal protein binding and damage to host cells(110).The roles of humoral and cell-mediated immunity are still
being assessed. Because AIDS patients have deficient T4cells and development of Pneumocystis pneumonia corre-lates with depletion of CD4 cells to below 200/mm3 (102),some investigators postulate that cell-mediated immunity isparamount in protection. leki et al. (91) reported that the roleof neutrophils is negligible; Furuta et al. (58) showed thatboth T cells and antibody are important for resistance toinfection. The presence of antibody in AIDS patients hasbeen evaluated, and it was found that anti-P. carinii immu-noglobulin M was absent (80). Some episodes of Pneumo-cystis pneumonia have been seen in patients with hypogam-maglobulinemia or agammaglobulinemia (149, 164).Probably both humoral and cell-mediated immunity areimportant in host defense.AIDS patients who do not receive prophylaxis after treat-
ment often develop second episodes of Pneumocystis pneu-monia (39) that may be refractory to therapy. These episodesmay result from Pneumocystis organisms from the initialinfection remaining viable or from reacquisition of P. carinii.The relative importance of these modes of recurrence is notknown. A comparison of patients with AIDS and patientswithout AIDS who developed Pneumocystis pneumonia
CLIN. MICROBIOL. REV.
on February 27, 2019 by guest
http://cmr.asm
.org/D
ownloaded from

P. CARINII IN IMMUNOCOMPROMISED PATIENTS 139
showed that those with AIDS had many more organisms butthat those without AIDS had greater lung inflammation, as
evidenced by more neutrophils. The greater inflammationwas associated with lower arterial oxygen tension andpoorer survival (111).
CLINICAL MANIFESTATIONS
Because P. carinii may be present with no apparentdeleterious effect on the host, it is assumed that most clinicalmanifestations result from activation of latent infections.Organisms proliferate when there is some compromise of theimmune system. In patients receiving treatment for acutelymphocytic leukemia, the time of onset of clinical Pneumo-cystis pneumonia varied from 30 to 100 days after the start ofchemotherapy, suggesting that in this situation, a minimumof one month is required for the P. carinii organisms to reachsufficient numbers to cause disease (159). Progression ofdisease, types of host cell infiltration, and response toanti-Pneumocystis therapy all vary according to the type andseverity of immunosuppression. Probably most infectionsremain subclinical. Differences in rapidity of development ofpneumonia, degree of lung involvement and hypoxemia, andresponse to therapeutic regimens have been described forpatients immunocompromised by malignancy and chemo-therapy and for those immunocompromised by human im-munodeficiency virus (201). Children immunocompromisedby protein calorie malnutrition have a slowly developingdisease, while individuals given chemotherapy for malig-nancy or organ transplantation frequently have rapidly de-veloping pulmonary disease. Patients with AIDS most oftenhave slowly developing disease (83, 177).
Malnutrition probably contributes to immunosuppressionin those with AIDS just as it did in children with plasma cellpneumonia. Radiographic patterns may be variable. Al-though it is usually reported that P. carinii causes bilateralfluffy infiltrates, atypical (42), one-sided, nodular, and cavi-tary lesions have also been reported (10, 56). Patientsreceiving aerosolized pentamidine for prophylaxis may showperipheral apical pneumonia because these areas are more
difficult to reach with aerosol. Chest radiographs oftenappear normal when blood gas levels and clinical appear-ances suggest severe pneumonia (67). Gallium-67 scans havebeen reported to be more sensitive than chest radiographs(11, 196); however, it appears that the uptake of gallium isnot specific for P. carinii but indicates an inflammatoryprocess (79, 104).
Prior to the AIDS epidemic, few cases of disseminateddisease were reported (6, 9, 147). In fact, workers tried todetermine why P. carinii had such a clear predilection forlung tissue and seemed to be confined to it. Now reportshave shown infection in almost every organ; manifestationsinclude thymoma (27), choroiditis (117, 150), pneumocys-toma (60), necrotizing vasculitis (112), and infections of thesmall intestine (28), liver (142), spleen (181), bone marrow
(151, 158, 159), ear (165, 170), and skin (35). The use ofaerosol pentamidine for prophylaxis has contributed to thisvariety by suppressing lung infection while organisms dis-seminate to other organs.The classic symptoms of patients with Pneumocystis
pneumonia are a dry, nonproductive cough, fever, weightloss, and shortness of breath. Often, the P02 is lower than
would be expected from the clinical signs and symptoms and
the chest radiograph.
LABORATORY DIAGNOSIS
Although some have suggested that empiric therapy isjustified for patients with symptoms compatible with Pneu-mocystis pneumonia (115), this is not prudent because anti-Pneumocystis treatment would be inappropriate for otheropportunistic infections. A variety of other common oppor-tunistic infections have been reported (200), including infec-tions with Histoplasma capsulatum (191), Cryptococcusneoformans (193), Coccidioides immitis (171), Mycobacte-rium avium complex (120), Nocardia spp. (132), Toxoplasmagondii (71), cytomegalovirus, and bacteria such as Strepto-coccus pneumoniae. Some patients may have coinfectionswith P. carinii and one or more of these infectious agents. Inour experience at Indiana University Medical Center, histo-plasmosis frequently has been the diagnosis when historyand clinical presentation suggested Pneumocystis infection.The treatment used for Pneumocystis pneumonia is noteffective for histoplasmosis, just as antifungal agents areineffective against Pneumocystis pneumonia.
In addition, the infiltrates demonstrated on chest radio-graphs and altered lung function with a lowered PO2 anddiminished diffusion capabilities may result from noninfec-tious processes. Ruling out infection prevents these patientsfrom being treated with potentially toxic antimicrobialagents.
Currently, the only proven method for establishing adiagnosis of infection with P. carinii is morphologic demon-stration of organisms. Clinical presentations, radiographs,and pulmonary function tests may be suggestive but are notspecific for P. carinii because they can only indicate lungdamage (33). Reports on elevated serum lactate dehydroge-nase levels (61, 97, 167) and angiotensin converting enzyme(169) suggest that these enzymes may be useful in assessingpatient response to therapy and prognosis. Increased levelsof these enzymes indicate inflammation, alveolar damage, ormacrophage dysfunction.Although organisms from rat or mouse lung have been
grown to a limited extent in culture (13, 38, 106, 129, 178),organisms from human lung have not been cultured success-fully. Culture, the gold standard of microbiology, is notuseful for diagnosis at present.
Tests for antibody to P. carinii are not helpful for diagno-sis because most healthy individuals have antibody that canbe detected by methods currently in use, while severelyimmunocompromised individuals with proven Pneumocystispneumonia may not have antibody. Detection of P. cariniiantigen in serum has been described (136, 138) but has notbeen specific and sensitive enough for establishing a diagno-sis and thus is not recommended. Studies of patient groupswith positive antigen tests have not always included suffi-cient controls to differentiate false-positive tests from thoseof subclinically infected individuals (85).A DNA probe has been described (183) which has been
used successfully to detect P. carinii in bronchoalveolarlavage samples and appears promising as a diagnostic testbut it is not commercially available (184).At present, diagnosis of Pneumocystis pneumonia re-
quires demonstration of organisms in tissue or secretionsfrom the lung (or from some extrapulmonary site). Tissueobtained by open-lung biopsy or transbronchial biopsy sam-
ples may be used. Transthoracic cutting-needle biopsy israrely used because of the high rate of complications asso-
ciated with this technique (8). Open-lung biopsy, historicallythe method of choice (7, 93), is seldom performed todayexcept for some pediatric patients or patients with unusual
VOL. 4, 1991
on February 27, 2019 by guest
http://cmr.asm
.org/D
ownloaded from

140 BARTLETT AND SMITH
diagnostic problems. Transbronchial biopsies are useful (22),but they must be performed by a skilled bronchoscopist andmultiple biopsy samples must be obtained (94). Percutane-ous needle aspiration has been used to obtain specimens,especially from children, and is a relatively safe procedure(8).Most pulmonary specimens are collected by bronchos-
copy and, in addition to transbronchial biopsy (see above),may include bronchoalveolar lavage fluid, bronchial brush-ings, and bronchial washings. Bronchoalveolar lavage fluidsare superior to bronchial washings because they containcells and organisms from the alveoli, whereas bronchialwashings may contain material only from the tracheobron-chial tree. Bronchial washings may not show organisms insome patients with Pneumocystis pneumonia. A variety ofbronchoscopic techniques with and without fluoroscopicguidance have been described (123), and their yields havebeen compared. The usefulness of bronchial washings (155);endobronchial brushings (162); and minilavages, samplesobtained from instillation of 20 to 50 ml of saline (199), havebeen compared, and their diagnostic efficacy varies frominstitution to institution. There are many additional reportson these procedures and various modifications. In our expe-rience, bronchoalveolar lavage and transbronchial biopsyhave been most useful.Sputum induction is a less expensive method than bron-
choscopy to procure suitable specimens from both adultsand children (16, 103, 135). Although at some institutions thediagnostic yields from sputum samples have been excellent,at others the yields have not been satisfactory (40, 154).Induced sputum specimens have been less useful for diag-nosing P. carinii pneumonia in non-AIDS than AIDS pa-tients. Patients with AIDS usually have very large numbersof organisms present, so that induced sputum specimens arelikely to allow diagnosis. However, sputum specimens can-not be used to detect certain other organisms, whereasbronchoalveolar lavage specimens have been reported to beuseful in the detection of infectious agents such as fungi(171). In one report on the successful use of induced sputumspecimens for diagnosing P. carinii pneumonia, it was em-phasized that training for those performing the inductionprocess, the presence of a special team to work withpatients, and careful attention to all details of the protocolare required (107). One report suggests that nasotrachealsuctioned specimens are superior to induced sputum fordiagnosis of P. carinii pneumonia (105). Unless inducedsputum examination has been demonstrated to be bothsensitive and specific for diagnosis in a particular institution,a negative sputum sample should be followed by a broncho-alveolar lavage to ensure optimal detection of organisms.Examination of induced sputum samples for diagnosis ofPneumocystis pneumonia may not be cost-effective in insti-tutions in which only a few patients with opportunisticinfections are seen.
Individuals with AIDS often have severe infections, withnumerous clumps of Pneumocystis organisms present inspecimens, making diagnosis easy. However, bronchoalve-olar lavage specimens from patients who have been givenaerosolized pentamidine do not always contain organisms,and diagnosis may require a transbronchial biopsy (96). Innon-AIDS patients, Pneumocystis organisms may be sparse,making their demonstration more difficult (111).
Procuring specimens and processing them for optimaldetection ofP. carinii and other opportunists requires skilledindividuals, including bronchoscopists or respiratory thera-pists and microbiologists or pathologists. Selection of appro-
priate procedures should be based on the numbers and typesof patients seen at an institution as well as the availability ofappropriately skilled personnel. For these reasons, diagnos-tic yields from various specimens will vary among institu-tions.
If a bronchoscopy is performed, there may be one or morespecimens, including lavages, brushings, washings, and tis-sue. Tissue may be submitted for surgical pathology exam-inations and/or used to make impression smears for stainingand examination in the microbiology or cytopathology lab-oratory. For impression smears, the tissue is blotted on asterile surface to remove excess liquid and then pressedagainst glass slides to make impressions. Usually, severalslides are prepared. Brushes may be pressed against slidesfor impression smears, or brushings may be vortexed insaline and centrifuged to pellet the cells before smears aremade of the pellet. Lavage and wash samples are centri-fuged, and slides are prepared from the pellets. A bloodyspecimen may require treatment of a portion of the specimenwith an agent such as saponin, Zaptoglobin, or Lyse to lysethe erythrocytes. An erythrocyte lysis product used forautomated leukocyte counts can usually be obtained fromthe hematology laboratory. By lysing erythrocytes, it ispossible to concentrate the specimen and yet not destroy theappearance of the organisms.Wash samples may contain quantities of mucus that re-
quire treatment with a mucolytic agent such as Sputolysin.Specimen is added to an equal volume of the mucolytic agentand then centrifuged to pellet the cells, after which thesediment is used to prepare slides. Induced sputum samplesshould be treated with mucolytic agents as described forwash samples. Protocols for handling induced sputum orbronchoalveolar lavage specimens may include processingby cytocentrifugation (119), which is widely used to evaluatecell populations. Mucolytic agents must be used and thenumber of cells present must be evaluated to determine theamount of material to cytocentrifuge.How slides are fixed depends on the staining procedures to
be performed. For most histochemical stains, methanolfixation is satisfactory. For some immunologic stains, ace-tone fixation is required.
Opinions differ as to the most effective stain or combina-tion of stains. The three kinds of stains are (i) organismstains, such as Giemsa and various rapid Giemsa stains,which stain trophozoites or intracystic bodies; (ii) cyst wallstains, such as the traditional methenamine-silver nitrate,which stain cyst walls and do not stain trophozoites orintracystic organisms; and (iii) immunospecific stains. Somelaboratories use only a cyst wall stain, and others use only anorganism stain; we recommend that both an organism andcyst wall stain be used. For patients with numerous clumpsof organisms, staining lavage fluid with a rapid Giemsa stainsuch as Diff Quik or Giemsa Plus may allow diagnosis in 1 or2 min. Traditional Giemsa staining takes approximately 30min, but it provides better morphologic detail and mayreveal rare clusters of trophozoites more clearly than therapid modifications. A comparison of stain methods empha-sizes the usefulness of Giemsa stain for demonstratingtrophozoites (81). Wright stain (41) is similar to Giemsa stainbut results in less color contrast.
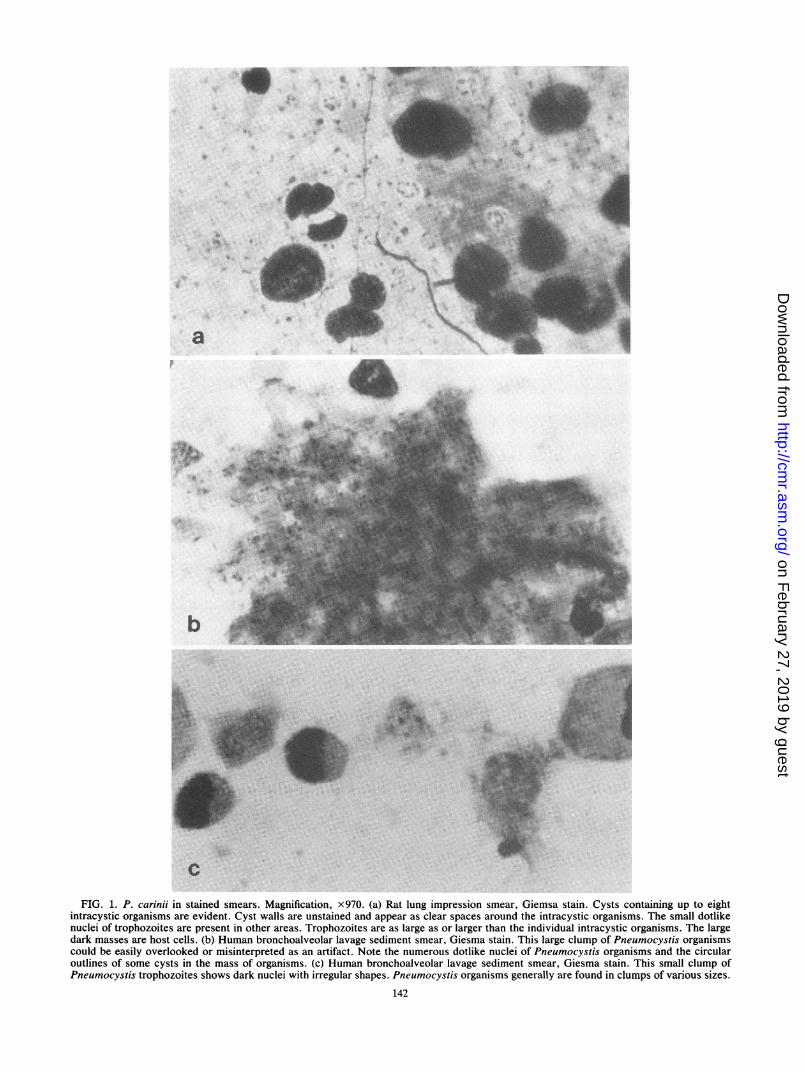
In Giemsa stains, trophozoites and intracystic bodies havea dotlike red to violet nucleus with a blue cytoplasm sur-rounding it (Fig. 1). Trophozoites are from 2 to 5 ,um indiameter and often occur in groups. Individual trophozoitesmay be difficult to distinguish from cell fragments. Whenmature, cysts have intracystic bodies which vary from round
CLIN. MICROBIOL. REV.
on February 27, 2019 by guest
http://cmr.asm
.org/D
ownloaded from

P. CARINII IN IMMUNOCOMPROMISED PATIENTS 141
to spindle shaped. The cyst wall does not stain and is seen asa clear halo around the intracystic organisms. In patientswith severe infections, especially patients with AIDS, theremay be very large clumps of P. carinii which can be easilyoverlooked because they are so dense and deeply stainedthat individual organisms are not distinguishable. On closeexamination, cysts and trophozoites can often be recognizedin the thinner areas of these clumps. P. carinii is generallyextracellular, but organisms may occasionally be detected inmacrophages.Cyst wall stains include methenamine-silver nitrate and
modifications of this stain for rapid processing (25, 77, 118,130, 141), cresyl echt violet (23, 62), toluidine blue 0 (30,69), Gram-Weigert (156), and calcofluor (14). Problems withtoluidine blue 0 sulfation reagents (166) and differences indye lots (194) have been reported. Because cyst walls of P.carinii contain chitin (185), whitening agents such as calco-fluor may be used (14) to demonstrate P. carinii by fluores-cence microscopy. In cyst wall stains, cysts frequently havedark areas that are often described as "parentheses" or dots(Fig. 1). Cyst walls may have folds, and cysts may be cupshaped. The dot and parenthesislike shapes indicate differ-ences in cell wall thickness, a correlation demonstrated bythe excellent histochemical electron micrograph studies ofWatts and Chandler (190). There may be some variation inthe intensity of staining of cysts. If only occasional silver-stained organisms are seen, it may not be possible todifferentiate Pneumocystis cysts from yeast cells or otherfungal elements. This may make evaluations of specimensfrom patients with AIDS more difficult, as these patientsfrequently have oropharyngeal candidiasis.Both Gram (48) and Papanicolaou (63) stains have de-
tected cysts but are not optimal stains and should not berelied upon for detection of P. carinii.
Since these methods demonstrate cyst walls of P. cariniiand walls of fungi, Pneumocystis-positive, Pneumocystis-negative, and yeast-positive samples should be included ascontrols. Experience is required to ensure that yeasts are notmistakenly identified as Pneumocystis cells. Control slidesare not needed for Giemsa stain and its modifications be-cause host cells in the specimen serve as internal controls.Immunologic staining with monoclonal antibodies specific
for P. carinii from human lung (64) may allow more accuratediagnosis than histochemical staining. Commercial productsare available, and some have been evaluated (20, 134).Immune-specific staining with commercial reagents has notbeen used widely enough to predict its usefulness, anddifficulties have been reported (99). An evaluation of onecommercial immune-specific stain method suggests that theindirect fluorescent-antibody stain (IFA) is more sensitivethan conventional histochemical stains (134). Of 182 speci-mens examined, 17 were positive by IFA but none of theother stains; thus, the sensitivity of IFA was 30% higher thanthat of histochemical stains. However, of these 17 IFA-positive specimens, only 3 could be determined to be truepositives. If the 14 that were positive only by IFA wereexcluded, there would be no significant difference in sensi-tivity between IFA and histochemical staining. In this study,a change in IFA evaluation criteria to minimize false posi-tives would have changed the detection rate for known-positive specimens (positive by other stains) to 51%. Whenthe laboratory examines specimens from many patients withPneumocystis pneumonia or from AIDS patients who havenumerous organisms, diagnosis can be made in minutes witha rapid Giemsa stain; therefore, the cost of and time forimmune-specific staining are not justified (20). Another dis-
advantage of immunologic stains is that they do not allowdetection of other organisms, such as Histoplasma andCryptococcus spp., bacteria, and Toxoplasma gondii.Immunologic staining might be reserved for specimens
that are negative by rapid histochemical stains. With kits forimmunologic stains, the package directions must be followedclosely. Positive controls must be included with all cyst walland immunologic stain procedures for P. carinii. If thoseexamining slides are not highly skilled in differentiating P.carinii cysts from yeast cells, a slide of material containingyeast cells should be included as a negative control. Themorphology of P. carinii is quite different in cyst wall stainsand in organism stains.We recommend that a laboratory perform one cyst wall
stain and one organism stain to ensure accurate diagnosis ofPneumocystis pneumonia and to allow detection of otheropportunistic infections. If one or two P. carinii cysts arefound in both organism and cyst wall stains, most likely theorganisms represent infection. Determining whether theinfection is the cause of clinical symptoms requires interpre-tation by the attending physician.
TREATMENT
Pentamidine isethionate was used to treat children withimmune deficiencies or patients receiving transplants whodeveloped Pneumocystis pneumonia until Hughes demon-strated the usefulness of TMP-SMX. He first tested it inanimal models (90) and then used it to treat children withPneumocystis pneumonia (86) and for prophylaxis (89).Since 1975, TMP-SMX has been considered the drug ofchoice for the treatment of Pneumocystis pneumonia and hasbeen widely used for prophylaxis in patients receiving trans-plants or antineoplastic therapy. Although, as with mosttherapeutic agents, there were side effects in non-AIDSpatients, these effects were not common and were lesscommon and less severe than those caused by pentamidine.In AIDS patients, the proven-effective regimen of TMP-SMX caused severe adverse reactions (68, 92), includingskin rashes, granulocytopenia, and liver function changes inup to two-thirds of patients. Because of these adversereactions, desensitization strategies (192) and changes indosage (121) have been tried. Some clinicians prefer tocontinue TMP-SMX despite rash development becauserashes may clear. However, because of the high frequencyof adverse reactions, TMP-SMX has not been widely usedfor prophylaxis in AIDS patients.
Parenteral pentamidine has been reported to cause hypo-glycemia (174, 188), hyperglycemia (131), neutropenia (5),abscess formation at injection sites (5), and fatal acutepancreatitis (202). Intravenous administration is the usualroute when treating Pneumocystis pneumonia. Most of theside effects of pentamidine can be avoided by changing theroute of administration from intravenous or intramuscularinjection to aerosol inhalation. When pentamidine is aero-
solized, it is deposited in the lungs, where organisms are
concentrated. Levels of the drug in serum and nonpulmo-nary tissue are much lower than when it is given intramus-cularly or intravenously, and therefore toxicity is decreased.Aerosolized pentamidine has been used both for prophylaxisand for treatment (34, 125-127), although it is most widelyused for prophylaxis. Since the adoption of pentamidine forprophylaxis, many reports of disseminated Pneumocystisinfection in patients receiving aerosolized pentamidine pro-phylaxis suggest that it only suppresses development ofpulmonary infection (142, 151, 170). One report of extrapul-
VOL. 4, 1991
on February 27, 2019 by guest
http://cmr.asm
.org/D
ownloaded from
6
a
+. .gi, rv~~~~~~~~M~n'O
..6.J,.i4
b
c
FIG. 1. P. carinii in stained smears. Magnification, x970. (a) Rat lung impression smear, Giemsa stain. Cysts containing up to eightintracystic organisms are evident. Cyst walls are unstained and appear as clear spaces around the intracystic organisms. The small dotlikenuclei of trophozoites are present in other areas. Trophozoites are as large as or larger than the individual intracystic organisms. The largedark masses are host cells. (b) Human bronchoalveolar lavage sediment smear, Giesma stain. This large clump of Pneumocystis organismscould be easily overlooked or misinterpreted as an artifact. Note the numerous dotlike nuclei of Pneumocystis organisms and the circularoutlines of some cysts in the mass of organisms. (c) Human bronchoalveolar lavage sediment smear, Giesma stain. This small clump ofPneumocystis trophozoites shows dark nuclei with irregular shapes. Pneumocystis organisms generally are found in clumps of various sizes.
142
on February 27, 2019 by guest
http://cmr.asm
.org/D
ownloaded from

N~~~~~~~V~~~~V
S
4
'.:
4-
4
d~ip
f~~
(d) Human bronchoalveolar lavage sediment smear, rapid methenamine-silver nitrate stain. This clump of Pneumoc-ystis organisms is similarto that shown in panel b. The number of cysts is much smaller than the number of trophozoites, and some clumps do not contain cysts (panelc). Note that cysts often have thickened areas in the wall that stain more darkly and may appear to be a single dot or a set of parentheses.Some cysts show linear folds. (e) Human bronchoalveolar lavage sediment smear, rapid methenamine-silver nitrate stain. These cysts are
siiaotoeiae btsansmwa akr Flsaepoieti oe yt.( ua rnhavelrlvg eietser
similar to those in panel d but stain somewhat darker. Folds are prominent in some cysts. (f) Human bronchoalveolar lavage sediment smear,modified toluidine blue 0 stain. These cysts are similar in appearance to those stained with rapid methenamine-silver.
143
on February 27, 2019 by guest
http://cmr.asm
.org/D
ownloaded from

144 BARTLETT AND SMITH
monary infection in 2.5% of AIDS patients at autopsysuggests that aerosol pentamidine prophylaxis may not beoptimal (179). In addition, recurrences of pulmonary Pneu-mocystis infection may occur in some patients while they are
receiving prophylaxis (1, 24).Successful Pneumocystis treatment and prophylaxis with
TMP-SMX suggested that other antifolate inhibitors mightbe effective. The effects of drugs on dihydrofolate reductaseextracted from Pneumocystis organisms were studied (3),and the drugs were tested in animal models. Two potentdihydrofolate reductase inhibitors, trimetrexate and piri-trexim, showed anti-Pneumocystis activity in animal models(100, 144) and clinical trials (2, 163). Trimetrexate waseffective for therapy, but relapse after treatment was fre-quent. Patients treated with trimetrexate required concur-
rent leucovorin rescue, making the regimen costly. Dapsonehas been used both alone and in combination with SMX or
TMP (43, 108). The dapsone combinations are effective, butsome problems with adverse reactions remain (153). Supple-mental steroid therapy in addition to the use of anti-Pneu-mocystis drugs has been successful with certain groups ofpatients (4, 128, 186), but was usually reserved for those withsevere pneumonia who were failing on other treatments. Areport that using corticosteroids early in treatment of pa-
tients with moderately severe P. carinii infection improvessurvival has led to wider use of corticosteroids (124). Otherdrugs that have been used in limited trials include difluoro-methylornithine (66) and fansidar, which is a combination ofpyrimethamine and sulfadiazine (70). Data on the usefulnessof difluoromethylornithine are difficult to interpret becausethe drug has been used primarily in salvage protocols and theresidual effects of previously used drugs make responses
difficult to interpret. Recurrent infection after treatment withfansidar has been reported (57), and this drug may cause
serious adverse reactions, such as Stevens-Johnson syn-
drome, which limit its usefulness. Drugs directed to targetsother than folate metabolism may avoid the adverse reac-tions associated with these compounds.The combination of clindamycin and primaquine was
shown to be effective in animals (145) and has been usedsuccessfully for the treatment of Pneumocystis pneumonia(98, 160, 180). Other 8-aminoquinolines have been evaluatedfor treatment and prophylaxis in animal models and appear
to be very effective (12a, 12b). The compounds are beingconsidered for clinical trials.A new compound, hydroxynaphthoquinone (566C80), has
been reported to be effective in animals (88), and earlyclinical trials are in progress.
A drug with little toxicity which can be taken orally forlong-term prophylaxis is urgently needed because patientswith AIDS have recurring or multiple infections. Patients athigh risk for opportunistic infections (CD4 counts of lessthan 200/mm3) and patients who have recovered from Pneu-mocystis pneumonia require prophylaxis. As improved anti-viral therapies, such as zidovudine and dideoxyinosine,increase the lifespans of AIDS patients, opportunistic infec-tions become more important. Prophylactic regimens whichsimultaneously prevent infections with P. carinii plus T.gondii or Cryptosporidium spp. would be especially appeal-ing.The role of immune modulators is not clear. As yet, there
are no reports of their effective use for treatment or preven-
tion of Pneumocystis infection. Good nutrition probably isvery important because malnutrition is itself immunosup-pressive.
Until a niche in the environment has been described for P.
carinii and until more is known about the spread of theorganism among people and the role, if any, of reservoirhosts, ways to avoid acquiring the organisms cannot bedetermined with certainty. To prevent disease from devel-oping, we must prevent severe immunosuppression or pro-vide drug prophylaxis to prevent proliferation of organisms.
Basic studies on host cell-parasite interactions and de-scription of the adherence mechanism may allow specificintervention in the process and prevent initial attachmentand establishment of infection.
In the future, some of the genes cloned and DNA or RNAsequences specific to P. carinii being developed by workerstoday may be made available commercially in kits that areconvenient and effective for detection of P. carinii. Suchmethods would rapidly and accurately diagnose Pneumocys-tis pneumonia and replace the morphologic diagnosticmethod, which requires skilled personnel and is time con-suming.
REFERENCES1. Abd, A. G., D. M. Nierman, J. S. Ilowite, R. N. Pierson, Jr.,
and A. L. L. Bell, Jr. 1988. Bilateral upper lobe Pneumocystiscarinii pneumonia in a patient receiving inhaled pentamidineprophylaxis. Chest 94:329-331.
2. Allegra, C. J., B. A. Chabner, C. U. Tuazon, D. Ogata-Arakaki,B. Baird, J. C. Drake, and H. Masur. 1988. Treatment ofPneumocystis carinii pneumonia with trimetrexate in acquiredimmunodeficiency syndrome (AIDS). Semin. Oncol. 15:46-49.
3. Allegra, C. J., J. A. Kovac, J. C. Drake, J. C. Swan, B. A.Chabner, and H. Masur. 1987. Activity of antifolates againstPneumocystis carinii dihydrofolate reductase and identifica-tion of a potent new agent. J. Exp. Med. 165:926-931.
4. Amandson, D. E., K. M. Murray, S. Brodine, and E. C.Oldfield. 1989. High-dose corticosteroid therapy of Pneumo-cystis carinii in patients with acquired immunodeficiency syn-drome. South. Med. J. 82:711-714.
5. Andersen, R., M. Boedicker, M. Ma, and E. J. C. Goldstein.1986. Adverse reactions associated with pentamidine isethion-ate in AIDS patients: recommendations for monitoring ther-apy. Drug Intell. Clin. Pharm. 20:862-868.
6. Awen, C. F., and M. A. Baltzan. 1971. Systemic disseminationof Pneumocystiis carinii pneumonia. Can. Med. Assoc. J.104:809-812.
7. Balantine, T. V. N., J. L. Grosfeld, R. M. Knapek, and R. L.Baehner. 1977. Interstitial pneumonitis in the immunologicallysuppressed child: an urgent surgical condition. J. Pediatr.Surg. 12:501-508.
8. Bandt, P. D., N. Blank, and R. A. Castellino. 1972. Needlediagnosis of pneumonitis: value in high-risk patients. J. Am.Med. Assoc. 220:1578-1580.
9. Barnett, R. N., J. G. Hull, V. Vortel, and J. Schwarz. 1969.Pneumocystis carinii in lymph nodes and spleen. Arch. Pathol.88:175-180.
10. Barrio, J. L., M. Suarez, J. L. Rodriguez, M. J. Saldana, andA. E. Pitchenik. 1986. Pneumocystis carinii pneumonia pre-senting as cavitating and noncavitating solitary pulmonarynodules in patients with the acquired immunodeficiency syn-drome. Am. Rev. Respir. Dis. 134:1094-1096.
11. Barron, T. F., N. S. Birnbaum, L. B. Shane, S. J. Goldsmith,and M. J. Rosen. 1985. Pneumocystis carinii pneumonia stud-ied by gallium-67 scanning. Radiology 154:791-793.
12. Bartlett, M. S., M. M. Durkin, M. A. Jay, S. F. Queener, andJ. W. Smith. 1987. Sources of rats free of latent Pneumocystiscarinii. J. Clin. Microbiol. 25:1794-1795.
12a.Bartlett, M. S., S. F. Queener, M. M. Durkin, M. M. Shaw, andJ. W. Smith. 1989. Program Abstr. 29th Intersci. Conf. Anti-microb. Agents Chemother., abstr. no. 1023.
12b.Bartlett, M. S., S. F. Queener, M. A. Jay, M. M. Dorkin, andJ. W. Smith. 1988. Program Abstr. 28th Intersci. Conf. Anti-microb. Agents Chemother., abstr. no. 1023.
13. Bartlett, M. S., P. A. Verbanca, and J. W. Smith. 1979.
CLIN. MICROBIOL. REV.
on February 27, 2019 by guest
http://cmr.asm
.org/D
ownloaded from

P. CARINII IN IMMUNOCOMPROMISED PATIENTS 145
Cultivation of Pneumocystis carinii with WI-38 cells. J. Clin.Microbiol. 10:796-799.
14. Baselski, V. S., M. K. Robison, L. W. Pifer, and D. R. Woods.1990. Rapid detection of Pneumocystis carinii in bronchoalve-olar lavage samples by using Cellufluor staining. J. Clin.Microbiol. 28:393-394.
15. Beautyman, W. 1983. Pneumocystis carinii is an endogenousliposomally modified mitochondrion. Med. Hypothesis 10:281-289.
16. Bigby, T. D., D. Margolskee, J. L. Curtis, P. F. Michael, D.Sheppard, W. K. Hadley, and P. C. Hopeweli. 1986. Theusefulness of induced sputum in the diagnosis of Pneumocystiscarinii pneumonia in patients with the acquired immunodefi-ciency syndrome. Am. Rev. Respir. Dis. 133:515-518.
17. Biggar, R. J. 1986. The clinical features of HIV infection inAfrica. Br. Med. J. 293:1453-1454.
18. Bleiweiss, I. J., J. S. Jagirdar, M. J. Klein, J. L. Siegel, D. J.Krellenstein, A. R. Gribetaz, and J. A. Strauchen. 1988. Gran-ulomatous Pneumocystis carinii pneumonia in three patientswith the acquired immune deficiency syndrome. Chest 94:580-583.
19. Blumenfeld, W., N. Basgoz, W. F. Owen, Jr., and D. M.Schmidt. 1988. Granulomatous pulmonary lesions in patientswith the acquired immunodeficiency syndrome (AIDS) andPneumocystis carinii infection. Ann. Intern. Med. 109:505-507.
20. Blumenfeld, W., and J. A. Kovacs. 1988. Use of a monoclonalantibody to detect Pneumocystis carinii in induced sputum andbronchoalveolar lavage fluid by immunoperoxidase staining.Arch. Pathol. Lab. Med. 112:1233-1236.
21. Blumenfeld, W., R. E. Mandrell, G. A. Jarvis, and J. M.Friffiss. 1990. Localization of host immunoglobulin G to thesurface of Pneumocystis carinii. Infect. Immun. 58:456-463.
22. Blumenfield, W., E. Wagar, and W. K. Hadley. 1984. Use ofthe transbronchial biopsy for diagnosis of opportunistic pulmo-nary infections in acquired immunodeficiency syndrome(AIDS). Am. J. Clin. Pathol. 81:1-5.
23. Bowling, M. C., IL M. Smith, and S. L. Wescott. 1973. A rapidstaining procedure for Pneumocystis carinii. Am. J. Med.Technol. 39:267-268.
24. Bradburne, R. M., D. B. Ettensohn, S. M. Opal, and F. D.McCool. 1989. Relapse of Pneumocystis carinii pneumonia inthe upper lobes during aerosol pentamidine prophylaxis. Tho-rax 44:591-593.
25. Brinn, N. T. 1983. Rapid metallic histological staining using themicrowave oven. J. Histotechnol. 6:125-129.
26. Brzosko, W. J., K. Krawezynski, K. Madalinski, and A. Nowo-slawski. 1976. Immunopathologic aspects of Pneumocystiscarinii pneumonia in infants as revealed by immunofluores-cence and electron microscopy. Natl. Cancer Inst. Monogr.43:163-168.
27. Buff, D. D., S. D. Greenberg, P. Leong, and F. S. Paulumbo.1988. Thymoma, Pneumocystis carinii pneumonia, and AIDS.N.Y. State J. Med. 88:276-277.
28. Carter, T. R., P. H. Cooper, W. A. Petri, Jr., C. K. Kim, P. D.Walzer, and R. L. Guerrant. 1988. Pneumocystis carinii infec-tion of the small intestine in a patient with acquired immunedeficiency syndrome. Am. J. Clin. Pathol. 89:679-683.
29. Chagas, C. 1909. Nova trypanozomiaza humana. Estudossobre a morfolojia e o ciclo evolutivo do Schizotrypanum cruzin. gen., n. sp. ajente etiologio de nova entidade morbida dehomen. Mem. Inst. Oswaldo Cruz Rio de J. 1:159-218.
30. Chalvardjian, A. W., and L. A. Grawe. 1963. A new procedurefor the identification of Pneumocystis carinii cysts in tissuesections and smears. J. Clin. Pathol. 16:383-384.
31. Chusid, M. J., and K. A. Heyrman. 1978. An outbreak ofPneumocystis carinii pneumonia at a pediatric hospital. Pedi-atrics 62:1031.
32. Climent, C., G. Lasala, R. Velez, C. Baldizon, and M. L.Santaella. 1985. Acquired immune deficiency syndrome(AIDS): experience in the Puerto Rico medical center. Bol.Asoc. Med. P.R. 77:50-55.
33. Coleman, D. L., P. M. Dodek, J. A. Golden, J. M. Luce, E.
Golden, W. M. Gold, and J. F. Murray. 1984. Correlationbetween serial pulmonary function tests and fiberoptic bron-choscopy in patients with Pneumocystis carinii pneumonia andthe acquired immune deficiency syndrome. Am. Rev. Respir.Dis. 129:491-493.
34. Corkery, K. J., J. M. Luce, and A. B. Montgomery. 1988.Aerosolized pentamidine for treatment and prophylaxis ofPneumocystis carinii pneumonia: an update. Respir. Care33:676-685.
35. Coulman, C. U., I. Greene, and R. W. R. Archibald. 1987.Cutaneous pneumocystosis. Ann. Intern. Med. 106:396-398.
36. Cruickshank, B., and F. R. C. Path. 1975. Pulmonary granulo-matous pneumocystosis following renal transplantation. Am.J. Clin. Pathol. 63:384-390.
37. Csillag, A., and L. Brandstein. 1954. The role of a blastomycesin the aetiology of interstitial plasmocytic pneumonia of thepremature infant. Acta Microbiol. 1-2:179-190.
38. Cushion, M. T., and P. D. Walzer. 1984. Growth and serialpassage of Pneumocystis carinii in the A549 cell line. Infect.Immun. 44:245-251.
39. DeLorenzo, L. J., G. P. Maguire, G. P. Wormser, M. M.Davidian, and D. J. Stone. 1985. Persistence of Pneumocystiscarinii pneumonia in the acquired immunodeficiency syn-drome. Chest 88:79-82.
40. del Rio, C., J. Guarner, E. G. Honig, and B. A. Slade. 1988.Sputum examination in the diagnosis of Pneumocystis cariniipneumonia in the acquired immunodeficiency syndrome. Arch.Pathol. Lab. Med. 112:1229-1232.
41. Domingo, J., and H. W. Waksal. 1984. Wright's stain in rapiddiagnosis of Pneumocystis carinii. Am. J. Clin. Pathol. 81:511-514.
42. Doppman, J. L., G. W. Gedhoed, and V. T. DeVita. 1975.Atypical radiographic features in Pneumocystis carinii pneu-monia. Radiology 114:39-44.
43. Edelson, P. J., and C. G. Metroka. 1985. Dapsone, tri-methoprim-sulfamethoxazole, and the acquired immunodefi-ciency syndrome. Ann. Intern. Med. 103:963.
44. Edman, J. C., J. A. Kovacs, H. Masur, D. V. Santi, H. J.Elwood, and M. L. Sogin. 1988. Ribosomal RNA sequenceshows Pneumocystis carinii to be a member of the fungi.Nature (London) 334:519-522.
45. Eidelman, A. I., G. S. Giebink, C. E. Stracener, M. C.Madigan, T. M. Vernon, B. S. Levy, and T. L. Nghiem. 1976.Epidemiologic notes and reports: Pneumocystis carinii pneu-monia in Vietnamese orphans. Morbid. Mortal. Weekly Rep.25:15.
46. Elvin, K. M., C. M. Lumbwe, N. P. Luo, A. Bjorkman, C.Kallenius, and E. Linder. 1989. Pneumocystis carinii is not amajor cause of pneumonia in HIV-infected patients in Lusaka,Zambia. Trans. R. Soc. Trop. Med. Hyg. 83:553-555.
47. Eng, R. H. K., E. Bishburg, and S. M. Smith. 1987. Evidencefor destruction of lung tissues during Pneumocystis cariniiinfection. Arch. Intern. Med. 147:746-749.
48. Felegie, T. P., A. W. Pasculle, and A. Dekker. 1984. Recogni-tion of Pneumocystis carinii by Gram stain in impressionsmears of lung tissue. J. Clin. Microbiol. 20:1190-1191.
49. Fenelon, L. E., C. T. Keane, M. Bakir, and I. J. Temperley.1985. A cluster of Pneumocystis carinii infections in children.Br. Med. J. 291:1683.
50. Fleury, J., E. Escudier, M.-J. Pocholle, C. Carre, and J. F.Bernaudin. 1985. Cell population obtained by bronchoalveolarlavage in Pneumocystis carinii pneumonitis. Acta Cytol. 29:721-726.
51. Foliansbee, S. E., D. F. Busch, C. B. Wofsy, D. L. Coleman, L.Gullet, G. P. Aurigemma, T. Ross, W. K. Hadley, and W. L.Drew. 1982. An outbreak of Pneumocystis carinii pneumonia inhomosexual men. Ann. Intern. Med. 96:705-713.
52. Fossieck, B. E., and S. V. Spagnolo. 1980. Pneumocystis cariniipneumonitis in patients with lung cancer. Chest 78:721-722.
53. Frenkel, J. K. 1976. Pneumocystis jiroveci sp. from man:morphology, physiology and immunology in relation to pathol-ogy. Natl. Cancer Inst. Monogr. 43:13-30.
54. Frenkel, J. K., M. S. Bartlett, and J. W. Smith. 1990. RNA
VOL. 4, 1991
on February 27, 2019 by guest
http://cmr.asm
.org/D
ownloaded from

146 BARTLETT AND SMITH
homology and the reclassification of Pneumocystis. Diagn.Microbiol. Infect. Dis. 13:1-2.
55. Frenkel, J. K., J. T. Good, and J. A. Shultz. 1966. LatentPneumocystis infection of rats, relapse, and chemotherapy.Lab. Invest. 15:1559-1577.
56. Friedman, B. A., B. D. Wenglin, R. N. Hyland, and D. Rifkind.1975. Roentgenographically atypical Pneumocystis cariniipneumonia. Am. Rev. Respir. Dis. 3:89-96.
57. Frissen, P. H. J., A. Stronkhorst, J. K. M. Eeftinck Schatten-kerk, and S. A. Danner. 1988. Fansidar and Pneumocystiscarinii pneumonia. Ann. Intern. Med. 108:638-639.
58. Furuta, T., K. Ueda, K. Fujiwara, and K. Yamanouchi. 1985.Cellular and humoral immune responses of mice subclinicallyinfected with Pneumocystis carinii. Infect. Immun. 47:544-548.
59. Gajdusek, C. 1957. Pneumocystis carinii-etiologic agents ofinterstitial plasma cell pneumonia of premature and younginfants. Pediatrics 19:543-565.
60. Gallo, L., A. Perchick, I. Graf, M. Finfer, R. Schinella, andD. E. Burstein. 1987. Cytologic findings in 13 fine-needleaspirates of cystic intraparotid lesions, including cases withAIDS or AIDS risk factors. Acta Cytol. 31:677-678.
61. Garay, S. M., and J. Greene. 1989. Prognostic indicators in theinitial presentation of Pneumocystis carinii pneumonia. Chest95:769-772.
62. Genaw, C. 1989. Use of cresyl echt violet for the staining ofPneumocystis carinii as compared to Grocott's (GMS) andGiemsa methods. J. Histotechnol. 12:39-40.
63. Ghali, V., R. L. Garcia, and J. Skolom. 1983. Fluorescence ofPneumocystis carinii in Papanicolaou smears. Hum. Pathol.15:907-909.
64. Gill, V., G. Evans, F. Stock, J. Parillo, H. Masur, and J.Kovacs. 1987. Detection of Pneumocystis carinii by fluores-cent-antibody stain using a combination of three monoclonalantibodies. J. Clin. Microbiol. 25:1837-1840.
65. Goetz, O., and P. Peller. 1974. Pneumocystis-carinii-Pneumo-nien. Ubersichten Med. Klin. 69:1774-1778.
66. Golden, J. A., A. Sjoerdsma, and D. V. Santi. 1984. Pneumo-cystis carinii pneumonia treated with ox-difluoromethylorni-thine. West. J. Med. 141:613-623.
67. Goodman, J. L., and D. P. Tashkin. 1983. Pneumocystis withnormal chest x-ray film and arterial oxygen tension. Arch.Intern. Med. 143:1981-1982.
68. Gordin, F., G. Simon, C. Wofsy, and J. Mills. 1984. Adversereactions to trimethoprim-sulfamethoxazole in patients withthe acquired immunodeficiency syndrome. Ann. Intern. Med.100:495-499.
69. Gosey, L. L., R. M. Howard, F. G. Witebsky, F. P. Ognibene,T. C. Wu, V. J. Gill, and J. D. MacLowry. 1985. Advantages ofa modified toluidine blue 0 stain and bronchoalveolar lavagefor the diagnosis of Pneumocystis carinii pneumonia. J. Clin.Microbiol. 22:803-807.
70. Gottlieb, M., S. Knight, R. Mitsuyasu, J. Weisman, M. Roth,and L. S. Young. 1984. Prophylaxis of Pneumocystis cariniiinfection in AIDS with pyrimethamine-sulfadoxine. Lancetii:398-399.
71. Gransden, W. R., and P. M. Brown. 1983. Pneumocystispneumonia and disseminated toxoplasmosis in a male homo-sexual. Br. Med. J. 286:1614.
72. Gryzan, S., I. L. Paradis, A. Zeevi, R. J. Duquesnoy, J. S.Dummer, B. P. Griffith, R. L. Hardesty, A. Trento, M. A.Nalesnik, and J. H. Dauber. 1988. Unexpectedly high incidenceof Pneumocystis carinii infection after lung-heart transplanta-tion: implications for lung defense and allograft survival. Am.Rev. Respir. Dis. 137:1268-1274.
73. Ham, E. K., S. D. Greenberg, R. C. Reynolds, and D. B. Singer.1971. Ultrastructure of Pneumocystis carinii. Exp. Mol.Pathol. 14:362-372.
74. Haron, E., G. P. Bodey, M. A. Luna, R. Dekmezian, and L.Elting. 1988. Has the incidence of Pneumocystis carinii pneu-
monia in cancer patients increased with the AIDS epidemic?Lancet ii:904-905.
75. Hartz, J. W., K. R. Geisinger, M. Scharyj, and H. B. Muss.
1985. Granulomatous pneumocystosis presenting as a solitarypulmonary nodule. Arch. Pathol. Lab. Med. 109:466-469.
76. Hendley, J. O., and T. H. Weller. 1971. Activation and trans-mission in rats of infection with Pneumocystis. Proc. Soc. Exp.Biol. Med. 137:1401-1404.
77. Hinds, I. 1988. A rapid and reliable silver impregnation methodfor Pneumocystis carinii and fungi. J. Histotechnol. 11:27-29.
78. Hodson, E. M., and B. J. Springthorpe. 1976. Medical prob-lems in refugee children evaluated from South Vietnam. Med.J. Aust. 2:747-749.
79. Hoffer, P. 1980. Gallium and infection. J. Nucl. Med. 21:484-488.
80. Hoffman, B., L. P. Ryder, W. Holten-Anderson, N. Odum, A.Svejgaard, J. Gerstoft, P. Platz, P. B. Nielsen, J. 0. Nielsen, andM. Mojon. 1985. Humoral responses of Pneumocystis carinii inpatients with acquired immunodeficiency syndrome and inimmunocompromised homosexual men. J. Infect. Dis. 152:838-840.
81. Holten-Anderson, W., and H. J. Kolmos. 1989. Comparison ofmethenamine silver nitrate and Giemsa stain for detection ofPneumocystis carinii in bronchoalveolar lavage specimensfrom HIV-infected patients. Acta Pathol. Microbiol. Immunol.Scand. 97:745-747.
82. Hong, S.-T., P. E. Steele, M. T. Cushion, P. D. Walzer, S. L.Stringer, and J. R. Stringer. 1990. Pneumocystis carinii kary-otypes. J. Clin. Microbiol. 28:1785-1795.
83. Hopewell, P. C. 1988 Diagnosis of Pneumocystis carinii pneu-monia. Infect. Dis. Clin. North Am. 2:409-418.
84. Hughes, W. T. 1989. Pneumocystis carinii: taxing taxonomy.Eur. J. Epidemiol. 5:265-269.
85. Hughes, W. T. 1985. Serodiagnosis of Pneumocystis. Chest87:700.
86. Hughes, W. T., S. Feldman, and S. K. Sanyal. 1975. Treatmentof Pneumocystis carinii pneumonitis with trimethoprim-sul-famethoxazole. Can. Med. Assoc. J. 112:47-50.
87. Hughes, W. T., and F. Gigliotti. 1988. Nomenclature forPneumocystis carinii. J. Infect. Dis. 157:432-433.
88. Hughes, W. T., V. L. Gray, W. E. Gutteridge, V. S. Latter, andM. Pudney. 1989. Efficacy of a hydroxynaphthoquinone,566C80, in experimental Pneumocystis carinii pneumonitis.Antimicrob. Agents Chemother. 34:225-228.
89. Hughes, W. T., S. Kuhn, S. Chaudhary, S. Feldman, M.Verzosa, R. J. A. Aur, C. Pratt, and S. L. George. 1977.Successful chemoprophylaxis for Pneumocystis carinii pneu-monitis. N. Engl. J. Med. 297:1419-1426.
90. Hughes, W. T., P. C. McNabb, T. B. Makres, and S. Feldman.1974. Efficacy of trimethoprim and sulfamethoxazole in theprevention and treatment of Pneumocystis carinii pneumonitis.Antimicrob. Agents Chemother. 5:289-293.
91. leki, R., T. Furuta, S. Asano, S. Mori, S. Kudoh, H. Kimura,and F. Takaku. 1989. Effect of recombinant human granulocytecolony-stimulating factor on Pneumocystis carinii infection innude mice. Jpn. J. Exp. Med. 59:51-58.
92. Jaffe, H. S., D. I. Abrams, A. J. Ammann, B. J. Lewis, andJ. A. Golden. 1983. Complications of co-trimoxazole in treat-ment of AIDS-associated Pneumocystis carinii pneumonia inhomosexual men. Lancet ii:1109-1111.
93. Jaffe, J. P., and D. G. Maki. 1981. Lung biopsy in immuno-compromised patients: one institution's experience and anapproach to management of pulmonary disease in the compro-mised host. Cancer 48:1144-1153.
94. Jenkins, R., R. L. Myuerowitz, T. Kavic, and S. Slasky. 1978.Diagnostic yield of transbronchoscopic biopsies. Am. J. Clin.Pathol. 72:926-930.
95. Jirovec, O., and J. Vanek. 1954. Morphology of Pneumocystiscarinii and pathogenesis of Pneumocystis carinii pneumonia.Zentralbl. Alig. Pathol. Pathol. Anat. 92:424-437.
96. Jules-Elysee, K. M., D. E. Stover, M. B. Zaman, E. M. Ber-nard, and D. A. White. 1990. Aerosolized pentamidine: effecton diagnosis and presentation of Pneumocystis carinii pneu-monia. Ann. Intern. Med. 112:750-757.
97. Kagawa, F. T., C. M. Kirsch, G. G. Yenokida, and M. L.Levine. 1988. Serum lactate dehydrogenase activity in patients
CLIN. MICROBIOL. REV.
on February 27, 2019 by guest
http://cmr.asm
.org/D
ownloaded from

P. CARINII IN IMMUNOCOMPROMISED PATIENTS 147
with AIDS and Pneumocystis carinii pneumonia. Chest 94:1031-1033.
98. Kay, R., and R. E. DuBois. 1990. Clindamycin/primaquinetherapy and secondary prophylaxis against Pneumocystis car-inii pneumonia in patients with AIDS. South. Med. J. 83:403-404.
99. Koch, M., and W. Heizmann. 1990. Problems in the detectionof Pneumocystis carinii by indirect immunofluorescence. Eur.J. Clin. Microbiol. Infect. Dis. 9:58-59.
100. Kovacs, J. A., C. J. Allegra, S. Kennedy, J. C. Swan, J. Drake,J. E. Parrillo, B. Chabner, and H. Masur. 1988. Efficacy oftrimetrexate, a potent lipid-soluble antifolate, in the treatmentof rodent Pneumocystis carinii pneumonia. Am. J. Trop. Med.Hyg. 39:491-496.
101. Kovacs, J. A., J. L. Halpern, J. C. Swan, J. Moss, J. E.Parrillo, and H. Masur. 1988. Identification of antigens andantibodies specific for Pneumocystis carinii. J. Immunol. 140:2023-2031.
102. Kovacs, J. A., and H. Masur. 1989. Prophylaxis of Pneumo-cystis carinii pneumonia: an update. J. Infect. Dis. 160:882-886.
103. Kovacs, J. A., V. L. Ng, H. Masur, G. Leoung, W. K. Hadley,G. Evens, H. C. Lane, F. P. Ognibene, J. Shelhamer, J. E.Parrillo, and V. J. Gill. 1988. Diagnosis ofPneumocystis carinjipneumonia: improved detection in sputum with use of mono-clonal antibodies. N. Engl. J. Med. 318:589-593.
104. Kramer, E. L., J. J. Sanger, S. M. Garay, J. B. Greene, S. Tiu,H. Banner, and D. I. McCauley. 1987. Gallium-67 scans of thechest in patients with acquired immunodeficiency syndrome. J.Nucl. Med. 28:1107-1114.
105. Larson, R. P., and R. J. Maunder. 1987. Non-bronchoscopicdiagnosis of Pneumocystis carinii pneumonia. Respir. Care32:896.
106. Latorre, C. R., A. J. Sulzer, and L. G. Norman. 1977. Serialpropagation of Pneumocystis carinii in cell line cultures. Appl.Environ. Microbiol. 33:1204-1206.
107. Leigh, T. R., P. Parsons, C. Hume, 0. A. N. Husain, B.Gazzard, and J. V. Collins. 1989. Sputum induction for diag-nosis of Pneumocystis carinii pneumonia. Lancet ii:205-206.
108. Leoung, G. S., J. Mills, P. C. Hopewell, W. Hughes, and C.Wofsy. 1986. Dapsone-trimethoprim for Pneumocystis cariniipneumonia in the acquired immunodeficiency syndrome. Ann.Intern. Med. 105:45-48.
109. Lidman, C., A. Ortquist, P. Lundbergh, I. Julander, and S.Bergdahl. 1989. Pneumocystis carinii pneumonia in Stock-holm, Sweden: treatment, outcome, one-year follow-up andpyrimethamine prophylaxis. Scand. J. Infect. Dis. 21:381-387.
110. Limper, A. H., and W. J. Martin II. 1990. Pneumocystiscarinii: inhibition of lung cell growth mediated by parasiteattachment. J. Clin. Invest. 85:391-396.
111. Limper, A. H., K. P. Offord, T. F. Smith, and W. J. Martin II.1989. Differences in lung parasite number and inflammation inpatients with and without AIDS. Am. Rev. Respir. Dis.140:1204-1209.
112. Liu, Y. C., J. F. Tomashefski, Jr., J. W. Tomford, and H.Green. 1989. Necrotizing Pneumocystis carinii vasculitis asso-ciated with lung necrosis and cavitation in a patient withacquired immunodeficiency syndrome. Arch. Pathol. Lab.Med. 113:494-497.
113. Long, E. G., J. S. Smith, and J. L. Meier. 1986. Attachment ofPneumocystis carinii to rat pneumocytes. Lab. Invest. 54:609-615.
114. Lucas, S. B. 1988. AIDS in Africa-clinicopathological as-pects. Trans. R. Soc. Trop. Med. Hyg. 82:801-802.
115. Luce, J. M., and D. E. Stover. 1988. Presumed Pneumocystiscarinii pneumonia should be treated empirically in patientswith the acquired immunodeficiency syndrome. Am Rev.Respir. Dis. 138:1076-1077.
116. Lundgren, B., R. Cotton, J. C. Lundgren, J. C. Edman, andJ. A. Kovacs. 1990. Identification of Pneumocystis cariniichromosomes and mapping of five genes. Infect. Immun.58:1705-1710.
117. Magher, A. M., D. S. Bardenstein, L. E. Zimmerman, C. K.
Steigman, L. Pastore, D. M. Poretz, and L. J. Eron. 1987.Pneumocystis carinii choroiditis in a male homosexual withAIDS and disseminated pulmonary and extrapulmonary P.carinii infection. N. Engl. J. Med. 316:1092.
118. Mahan, C. T., and G. E. Sale. 1978. Rapid methenamine silverstain for Pneumocystis and fungi. Arch. Pathol. Lab. Med.102:351-352.
119. Martin, W. J., II, T. F. Smith, D. R. Sanderson, W. M.Brutinel, F. R. Cockerill Im, and W. W. Douglas. 1987. Role ofbronchoalveolar lavage in the assessment of opportunisticpulmonary infections: utility and complications. Mayo Clin.Proc. 62:549-557.
120. Masur, H. 1982. Mycobacterium avium-intracellulare: An-other scourge of individuals with the acquired immunodefi-ciency syndrome. J. Am. Med. Assoc. 248:3013.
121. McLean, I., C. R. Lucas, M. L. Mashford, and P. J. Harmon.1987. Modified trimethoprim-sulphamethoxazole doses inPneumocystis carinii pneumonia. Lancet ii:857-858.
122. Meuwissen, J. H. E. T., I. Tauber, A. D. E. M. Leeuwenberg,P. J. A. Beckers, and J. Sieben. 1977. Parasitologic andserologic observations of infection with Pneumocystis in hu-mans. J. Infect. Dis. 136:43-49.
123. Milligan, S. A., J. M. Luce, J. Golden, M. Stulbarg, and P. C.Hopewell. 1988. Transbronchial biopsy with fluoroscopy inpatients with diffuse roentgenographic infiltrates and the ac-quired immunodeficiency syndrome. Am. Rev. Respir. Dis.137:486-488.
124. Montaner, J. S. G., L. M. Lawson, N. Levitt, A. Belzberg,M. T. Schechter, and J. Ruedy. 1990. Corticosteroids preventearly deterioration in patients with moderately severe Pneu-mocystis carinii pneumonia and the acquired immunodefi-ciency syndrome (AIDS). Ann. Intern. Med. 113:1420.
125. Montgomery, A. B., R. J. Debs, J. M. Luce, K. J. Corkery, J.Turner, E. N. Brunette, E. T. Lin, and P. C. Hopewell. 1988.Selective delivery of pentamidine to the lung by aerosol. Am.Rev. Respir. Dis. 137:477-478.
126. Montgomery, A. B., R. J. Debs, J. M. Luce, K. J. Corkery, J.Turner, E. N. Brunette, E. T. Lin, and P. C. Hopewell. 1987.Aerosolized pentamidine as sole therapy for Pneumocystiscarinii pneumonia in patients with acquired immunodeficiencysyndrome. Lancet ii:480-482.
127. Montgomery, A. B., R. J. Debs, J. M. Luce, K. J. Corkery, J.Turner, and P. C. Hopewell. 1989. Aerosolized pentamidine assecond-line therapy in patients with AIDS and Pneumocystiscarinii. Chest 95:747-750.
128. Mottin, D., M. Denis, H. Dombret, J. Rossert, C. Mayaud, andG. Akoun. 1987. Role for steroids in treatment of Pneumocystiscarinii pneumonia in AIDS. Lancet ii:519.
129. Murphy, M. J., L. L. Pifer, and W. T. Hughes. 1977. Pneumo-cystis carinii in vitro. Am. J. Pathol. 86:387-402.
130. Musto, L., M. Flanigan, and A. Elbadawi. 1982. Ten-minutesilver stain for Pneumocystis carinii and fungi in tissue sec-tions. Arch. Pathol. Lab. Med. 106:292-294.
131. Naafs, B. 1985. Pentamidine-induced diabetes mellitus. Trans.R. Soc. Trop. Med. 79:141.
132. Natale, R. B., A. Yagoda, A. Brown, C. Singer, D. Stover, andD. Bajorunas. 1981. Combined Pneumocystis carinii and No-cardia asteroides pneumonitis in a patient with an ACTH-producing carcinoid. Cancer 47:2933-2935.
133. Neiman, P. E., E. D. Thomas, W. C. Reeves, C. G. Ray, G.Sale, K. G. Lerner, C. D. Buckner, R. A. Clift, R. Storb, P. L.Weiden, and A. Fefer. 1976. Opportunistic infection and inter-stitial pneumonia following marrow transplantation for aplasticanemia and hematologic malignancy. Transplant. Proc. 8:663-667.
134. Ng, V. L., D. M. Yajko, L. W. McPhaul, I. Gartner, B. Byford,C. D. Goodman, P. S. Nassos, C. A. Sanders, E. L. Howes, G.Leough, P. C. Hopewell, and W. K. Hadley. 1990. Evaluation ofan indirect fluorescent-antibody stain for detection of Pneumo-cystis carinii in respiratory specimens. J. Clin. Microbiol.28:975-979.
135. Ognibene, F. P., V. J. Gill, P. A. Pizzo, J. A. Kovacs, C.Godwin, A. F. Suffredini, J. H. Shelhamer, J. E. Parrillo, and
VOL. 4, 1991
on February 27, 2019 by guest
http://cmr.asm
.org/D
ownloaded from
148 BARTLETT AND SMITH
H. Masur. 1989. Induced sputum to diagnose Pneumocystiscarinii pneumonia in immunosuppressed pediatric patients. J.Pediatr. 115:430-433.
136. Pifer, L. L. 1985. Serodiagnosis of Pneumocystis carinii. Chest87:698-699.
137. Pifer, L. L., W. T. Hughes, S. Stagno, and D. Woods. 1978.Pneumocystis carinii infection: evidence for high prevalence innormal and immunosuppressed children. Pediatrics 61:35-41.
138. Pifer, L. L., H. B. Neill, B. J. Morrison, J. D. Counce, Jr.,J. M. Freeman, D. R. Woods, and C. L. Neely. 1982. Pneumo-cystis carinii antigenemia in adults with malignancy, infection,or pulmonary disease. J. Clin. Microbiol. 20:887-890.
139. Pincus, P. S., M. D. Hurwitz, J. M. Kallenback, J. A.Abramowitz, and S. Zwi. 1987. Pneumocystis carinii pneumo-nia in Johannesburg. S. Afr. Med. J. 71:289-293.
140. Pincus, P. S., M. A. Sandler, G. E. Naude, J. M. Kallenbach, C.Isaacson, and S. Zwi. 1987. Multiple pulmonary cavities, an
unusual complication of Pneumocystis carinii pneumonia. S.Afr. Med. J. 72:871-872.
141. Pintozzi, R. L. 1978. Technical methods: modified Grocott'smethenamine silver nitrate method for quick staining of Pneu-mocystis carinii. Am. J. Clin. Pathol. 31:803-805.
142. Poblete, R. B., K. Rodriguez, R. T. Foust, K. R. Reddy, andM. J. Saldana. 1989. Pneumocystis carinii hepatitis in theacquired immunodeficiency syndrome (AIDS). Ann. Intern.Med. 110:737-738.
143. Pottratz, S. T., and W. J. Martin II. 1990. Role of fibronectinin Pneumocystis carinii attachment to cultured lung cells. J.Clin. Invest. 85:351-356.
144. Queener, S. F., M. S. Bartlett, M. A. Jay, M. M. Durkin, andJ. W. Smith. 1987. Activity of lipid-soluble inhibitors ofdihydrofolate reductase against Pneumocystis carinii in cultureand in a rate model of infection. Antimicrob. Agents Chemo-ther. 31:1323-1327.
145. Queener, S. F., M. S. Bartlett, J. D. Richardson, M. M. Durkin,M. A. Jay, and J. W. Smith. 1988. Activity of clindamycin andprimaquine against Pneumocystis carinii in vitro and in vivo.Antimicrob. Agents Chemother. 32:807-813.
146. Radin, D. R., E. L. Baker, E. C. Klatt, E. J. Balthazar, R. B.Jeffrey, Jr., A. J. Megibow, and P. W. Ralls. 1990. Visceral andnodal calcification in patients with AIDS-related Pneumocystiscarinii infection. Am. J. Roentgenol. 154:27-31.
147. Rahimi, S. A. 1974. Disseminated Pneumocystis carinii inthymic alymphoplasia. Arch. Pathol. 97:162-165.
148. Ramaswamy, G., V. Jagadha, and V. Tchertkoff. 1985. Diffusealveolar damage and interstitial fibrosis in acquired immuno-deficiency syndrome patients without concurrent pulmonaryinfection. Arch. Pathol. Lab. Med. 109:408-412.
149. Rao, C. P., and E. W. Gelfand. 1983. Pneumocystis cariniipneumonitis in patients with hypogammaglobulinemia and in-tact T cell immunity. J. Pediatr. 103:410-412.
150. Rao, N. A., P. L. Zimmerman, D. Boyer, J. Biswas, D. Causey,J. Beniz, and P. W. Nichols. 1989. A clinical, histopathologic,and electron microscopic study of Pneumocystis carinii chor-oiditis. Am. J. Ophthalmol. 107:218-228.
151. Raviglione, M. C., G. R. Garner, and M. P. Mullen. 1988.Pneumocystis carinii in bone marrow. Ann. Intern. Med.109:253.
152. Redman, J. C. 1974. Pneumocystis carinii pneumonia in an
adopted Vietnamese infant: a case of diffuse, fulminant dis-ease, with recovery. J. Am. Med. Assoc. 230:1561-1563.
153. Reiter, W. M., and P. J. Cimoch. 1987. Dapsone-inducedmethemoglobinemia in a patient with P. carinii pneumonia andAIDS. N. Engl. J. Med. 317:1740-1741.
154. Rolston, K. V. I., S. Rodriguez, L. McRory, G. Uribe-Botero,R. Morice, and P. W. A. Mansell. 1988. Diagnostic value ofinduced sputum in patients with the acquired immunodefi-ciency syndrome. Am. J. Med. 85:269.
155. Rorat, E., R. L. Garcia, and J. Skolom. 1985. Diagnosis ofPneumocystis carinii pneumonia by cytologic examination ofbronchial washings. JAMA 254:1950-1951.
156. Rosen, P. P., N. Martini, and P. Armstrong. 1975. Pneumocys-tis carinii pneumonia. Am. J. Med. 58:794-802.
157. Rossi, J. F., A. DuBois, C. Bengler, C. Arich, C. Gervais, A.Delage, and C. Janbon. 1985. Pneumocystis carinii in bonemarrow. Ann. Intern. Med. 102:868.
158. Rossi, J. F., J. F. Eledjam, A. Delage, C. Dengler, J. F. Schued,and J. Bonnafoux. 1990. Pneumocystis carinii infection of bonemarrow in patients with malignant lymphoma and acquiredimmunodeficiency syndrome. Arch. Intern. Med. 150:450-452.
159. Ruebush, T. K., R. A. Weinstein, R. L. Baehner, D. Woff, M.Bartlett, F. Gonzales-Crussi, A. J. Sulzer, and M. G. Schultz.1978. An outbreak of Pneumocystis pneumonia in childrenwith acute lymphocytic leukemia. Am. J. Dis. Child. 132:143-148.
160. Ruf, B., and H. D. Pohle. 1989. Clindamycin/primaquine forPneumocystis carinii pneumonia. Lancet ii:626-627.
161. Santiago-Delpin, E. A., E. Mora, Z. A. Gonzalez, L. A. Mo-rales-Otero, and R. Bermudez. 1988. Factors in an outbreak ofPneumocystis carinii in a transplant unit. Transplant. Proc.20:462-465.
162. Sarkar, T. K., P. V. Barker, and V. V. Gumaste. 1985. Role ofbronchial brush biopsy in AIDS with Pneumocystis cariniipneumonia. Chest 87:553-554.
163. Sattler, F. R., C. J. Allegra, T. D. Verdegem, B. Akil, C. U.Tuazon, C. Hugnlett, D. Ogata-Arakaki, J. Feinberg, J. Shel-hamer, H. C. Lane, R. Davis, C. T. Boylen, J. M. Leedom, andH. Masur. 1990. Trimetrexate-leucovorin dosage evaluationstudy for treatment of Pneumocystis carinii pneumonia. J.Infect. Dis. 161:91-96.
164. Saulsbury, F. T., M. T. Bernstein, and J. A. Winkelstein. 1979.Pneumocystis carinii pneumonia as the presenting infection incongenital hypogammaglobulinema. J. Pediatr. 95:559-561.
165. Schinella, R. A., S. D. Breda, and P. E. Hammerschlag. 1987.Otic infection due to Pneumocystis carinii in an apparentlyhealthy man with antibody to the human immunodeficiencyvirus. Ann. Intern. Med. 106:399-400.
166. Settnes, 0. S., and P. Larsen. 1979. Inhibition of toluidine blueO stain for Pneumocystis carinii by additives in the diethylether. Am. J. Clin. Pathol. 72:493-494.
167. Silverman, B. A., and A. Rubinstein. 1985. Serum lactatedehydrogenase levels in adults and children with acquiredimmune deficiency syndrome (AIDS) and AIDS-related com-plex: possible indicator of B cell lymphoproliferation anddisease activity. Am. J. Med. 78:728-736.
168. Singer, C., D. Armstrong, P. P. Rosen, and D. Schottenfeld.1975. Pneumocystis carinii pneumonia: a cluster of elevencases. Ann. Intern. Med. 82:772-777.
169. Singer, F., W. Talavera, and B. Zumoff. 1989. Elevated levelsof angiotensin-converting enzyme in Pneumocystis carinjipneumonia. Chest 95:803-806.
170. Smith, M. A., L. S. Hirschfield, G. Zahtz, and F. P. Siegal.1988. Pneumocystis carinii otitis media. Am. J. Med. 85:745-746.
171. Sobonya, R. E., R. A. Barbee, J. Wiens, and D. Trego. 1990.Detection of fungi and other pathogens in immunocompro-mised patients by bronchoalveolar lavage in an area endemicfor coccidioidomycosis. Chest 97:1349-1355.
172. Sogin, M. L., and J. C. Edman. 1989. A self-splicing intron inthe small subunit rRNA gene of Pneumocystis carinii. NucleicAcids Res. 17:5349-5359.
173. Sogin, M. L., H. J. Ganderson, H. J. Emwood, R. A. Alonso,and D. A. Peattie. 1988. Phylogenetic meaning of the kingdomconcept. An unusual ribosomal RNA from Giardia lamblia.Science 243:75-77.
174. Stahl-Bayliss, C. M., C. M. Kalman, and 0. L. Laskin. 1986.Pentamidine-induced hypoglycemia in patients with the ac-quired immune deficiency syndrome. Clin. Pharmacol. Ther.39:271-275.
175. Stoigescu, V. 1977. Some aspects of the invasion mechanism inhuman pneumocystosis. Arch. Roum. Pathol. Exp. Microbiol.36:301-306.
176. Talseth, T., H. Holdaas, D. Albrechtsen, K. J. Berg, P.Fauchald, A. Naalsund, K. P. Nordal, A.-G. Skar, G. Sodal,and A. Flatmark. 1988. Increasing incidence of Pneumocystiscarinii pneumonia in renal transplant patients. Transplant.
CLIN. MICROBIOL. REV.
on February 27, 2019 by guest
http://cmr.asm
.org/D
ownloaded from
P. CARINII IN IMMUNOCOMPROMISED PATIENTS 149
Proc. 20:400-401.177. Tapper, M. L. 1984. Clinical features of Pneumocystis pneu-
monia in the acquired immune deficiency syndrome. Am. Rev.Respir. Dis. 130:689-694.
178. Tegoshi, T. 1988. New system of in vitro cultivation of Pneu-mocystis carinii without feeder cells. J. Kyoto Prefect. Univ.Med. 97:1473-1482.
179. Telzak, E. E., R. J. Cote, J. W. M. Gold, S. W. Campbell, andD. Armstrong. 1990. Extrapulmonary Pneumocystis cariniiinfections. Rev. Infect. Dis. 12:380-386.
180. Toma, E., S. Fournier, M. Poisson, R. Morisset, D. Phaneuf,and C. Vega. 1989. Clindamycin with primaquine for Pneumo-cystis carinii pneumonia. Lancet i:1046-1048.
181. Unger, P. D., M. Rosenblum, and S. E. Krown. 1988. Dissem-inated Pneumocystis carinii infection in a patient with acquiredimmunodeficiency syndrome. Hum. Pathol. 19:113-116.
182. Vavra, J., and K. Kucera. 1970. Pneumocystis carinii Delanoe,its ultrastructure and ultrastructural affinities. Protozoology17:463-483.
183. Wakefield, A. E., J. M. Hopkin, J. Burns, J. B. Hipkiss, T. J.Stewart, and E. R. Moxon. 1988. Cloning of DNA fromPneumocystis carinii. J. Infect. Dis. 158:859-862.
184. Wakefield, A. E., F. J. Pixley, S. Banerji, K. Sinclair, R. F.Miller, E. R. Moxon, and J. M. Hopkin. 1990. Detection ofPneumocystis carinii with DNA amplification. Lancet 336:451-453.
185. Walker, A. N., R. E. Garner, and M. N. Horst. 1990. Immuno-cytochemical detection of chitin in Pneumnocystis carinii. In-fect. Immun. 58:412-415.
186. Walmsley, S., I. E. Salit, and J. Brunton. 1988. The possiblerole of corticosteroid therapy for Pneumocystis pneumonia inthe acquired immune deficiency syndrome (AIDS). J. AcquiredImmune Defic. Syndr. 1:354-360.
187. Walzer, P. D., and M. J. Linke. 1987. A comparison of theantigenic characteristics of rat and human Pneumocystis cari-nii by immunoblotting. J. Immunol. 138:2257-2265.
188. Waskin, H., J. K. Stehr-Green, C. G. Helmick, and F. R.Sattler. 1988. Risk factors for hypoglycemia associated withpentamidine therapy for Pneumocystis pneumonia. J. Am.Med. Assoc. 260:345-347.
189. Watanabe, J., H. Hori, K. Tanabe, and Y. Nakamura. 1989.Phylogenetic association of Pneumocystis carinii with therhizopoda/myxomycota/zygomycota group indicated by com-parison of 5S ribosomal RNA sequences. Mol. Biochem.Parasitol. 32:163-168.
190. Watts, J. C., and F. W. Chandler. 1985. Pneumocystis carinii
pneumonitis. Am. J. Surg. Pathol. 9:744-751.191. Wheat, L. J., P. Connolly-Stringfield, R. B. Kohler, P. T.
Frame, and M. R. Gupta. 1989. Diagnosis and management ofdisseminated histoplasmosis in patients with acquired immu-nodeficiency syndrome by Histoplasma capsulatum polysac-charide antigen detection. Am. J. Med. 87:396-400.
192. White, M. V., Z. H. Haddad, E. Brunner, and C. Sainz. 1989.Desensitization to trimethoprim-sulfamethoxazole in patientswith acquired immune deficiency syndrome and Pneumocystiscarinii pneumonia. Ann. Allergy 62:177-179.
193. Winslow, D. J., and B. M. Hathaway. 1959. Pulmonary pneu-mocystosis and cryptococcosis. Am. J. Clin. Pathol. 31:337-342.
194. Witebsky, F. G., J. W. B. Andrews, V. J. Gill, and J. D.MacLowry. 1988. Modified toluidine blue 0 stain for Pneumo-cystis carinii: further evaluation of some technical factors. J.Clin. Microbiol. 26:774-775.
195. Wolff, L. J., M. S. Bartlett, R. L. Baehner, J. L. Grosfeld, andJ. W. Smith. 1977. The causes of interstitial pneumonitis inimmunocompromised children: an aggressive, systematic ap-proach to diagnosis. Pediatrics 60:41-45.
196. Woolfenden, J. M., J. A. Carrasquillo, S. M. Larson, J. T.Simmons, H. Masur, P. D. Smith, J. H. Shelhamer, and F. P.Ognibene. 1987. Acquired immunodeficiency syndrome: Ga-67citrate imaging. Radiology 162:383-387.
197. Yoganathan, T., H. Lin, and G. A. Buck. 1989. An electropho-retic karyotype and assignment of ribosomal genes to resolvedchromosomes of Pneumocystis carinii. Mol. Microbiol.3:1473-1480.
198. Yoneda, K., and P. D. Walzer. 1983. Attachment of Pneumo-cystis carinii to type I alveolar cells studied by freeze-fractureelectron microscopy. Infect. Immun. 40:812-815.
199. Yoo, 0. H., H. C. Ho-Soon, R. A. Cucco, E. Desmond, and M.Lesser. 1989. Pneumocystis carinii pneumonia in the acquiredimmunodeficiency syndrome: diagnosis using minilavage sam-ples. South. Med. J. 82:829-832.
200. Young, L. S. 1986. Management of opportunistic infectionscomplicating the acquired immunodeficiency syndrome. Med.Clin. North Am. 70:677-691.
201. Ziefer, A., and J. A. Abramowitz. 1989. Pneumocystis cariniipneumonia in HIV-positive and HIV-negative patients: anepidemiological, clinical and histopathological study of 18patients. S. Afr. Med. J. 76:308-313.
202. Zuger, A., B. Z. Wolf, W. El-Sadr, M. S. Simberkoff, and J. J.Rahal. 1986. Pentamidine-associated fatal acute pancreatitis. J.Am. Med. Assoc. 256:2383-2385.
VOL. 4, 1991
on February 27, 2019 by guest
http://cmr.asm
.org/D
ownloaded from