pm185 trends in mortality following percutaneous coronary intervention
TRANSCRIPT
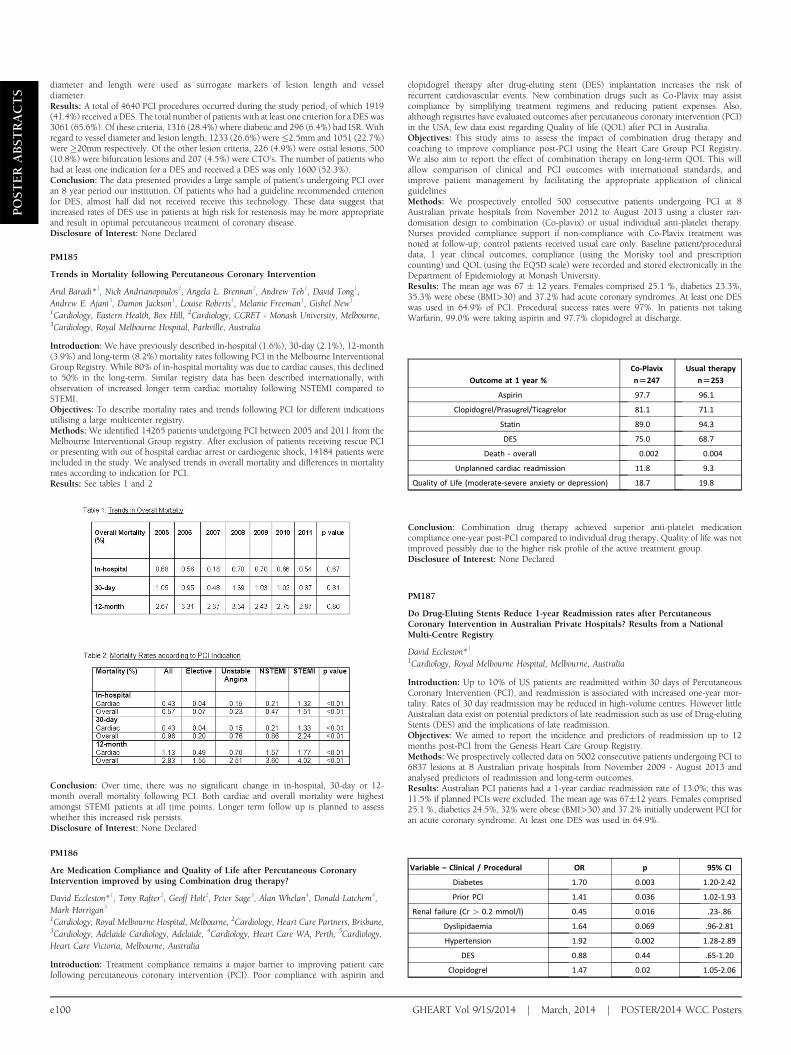
Outcome at 1 year %
Co-Plavix
n[247
Usual therapy
n[253
Aspirin 97.7 96.1
Clopidogrel/Prasugrel/Ticagrelor 81.1 71.1
Statin 89.0 94.3
DES 75.0 68.7
Death - overall 0.002 0.004
Unplanned cardiac readmission 11.8 9.3
Quality of Life (moderate-severe anxiety or depression) 18.7 19.8
Variable – Clinical / Procedural OR p 95% CI
Diabetes 1.70 0.003 1.20-2.42
Prior PCI 1.41 0.036 1.02-1.93
Renal failure (Cr > 0.2 mmol/l) 0.45 0.016 .23-.86
Dyslipidaemia 1.64 0.069 .96-2.81
Hypertension 1.92 0.002 1.28-2.89
DES 0.88 0.44 .65-1.20
Clopidogrel 1.47 0.02 1.05-2.06
POST
ERABST
RACTS
diameter and length were used as surrogate markers of lesion length and vesseldiameter.Results: A total of 4640 PCI procedures occurred during the study period, of which 1919(41.4%) received a DES. The total number of patients with at least one criterion for a DES was3061 (65.6%). Of these criteria, 1316 (28.4%) where diabetic and 296 (6.4%) had ISR. Withregard to vessel diameter and lesion length, 1233 (26.6%) were �2.5mm and 1051 (22.7%)were �20mm respectively. Of the other lesion criteria, 226 (4.9%) were ostial lesions, 500(10.8%) were bifurcation lesions and 207 (4.5%) were CTO’s. The number of patients whohad at least one indication for a DES and received a DES was only 1600 (52.3%).Conclusion: The data presented provides a large sample of patient’s undergoing PCI overan 8 year period our institution. Of patients who had a guideline recommended criterionfor DES, almost half did not received receive this technology. These data suggest thatincreased rates of DES use in patients at high risk for restenosis may be more appropriateand result in optimal percutaneous treatment of coronary disease.Disclosure of Interest: None Declared
PM185
Trends in Mortality following Percutaneous Coronary Intervention
Arul Baradi*1, Nick Andrianopoulos2, Angela L. Brennan2, Andrew Teh1, David Tong1,Andrew E. Ajani3, Damon Jackson1, Louise Roberts1, Melanie Freeman1, Gishel New1
1Cardiology, Eastern Health, Box Hill, 2Cardiology, CCRET - Monash University, Melbourne,3Cardiology, Royal Melbourne Hospital, Parkville, Australia
Introduction: We have previously described in-hospital (1.6%), 30-day (2.1%), 12-month(3.9%) and long-term (8.2%) mortality rates following PCI in the Melbourne InterventionalGroup Registry. While 80% of in-hospital mortality was due to cardiac causes, this declinedto 50% in the long-term. Similar registry data has been described internationally, withobservation of increased longer term cardiac mortality following NSTEMI compared toSTEMI.Objectives: To describe mortality rates and trends following PCI for different indicationsutilising a large multicenter registry.Methods: We identified 14265 patients undergoing PCI between 2005 and 2011 from theMelbourne Interventional Group registry. After exclusion of patients receiving rescue PCIor presenting with out of hospital cardiac arrest or cardiogenic shock, 14184 patients wereincluded in the study. We analysed trends in overall mortality and differences in mortalityrates according to indication for PCI.Results: See tables 1 and 2
Conclusion: Over time, there was no significant change in in-hospital, 30-day or 12-month overall mortality following PCI. Both cardiac and overall mortality were highestamongst STEMI patients at all time points. Longer term follow up is planned to assesswhether this increased risk persists.Disclosure of Interest: None Declared
PM186
Are Medication Compliance and Quality of Life after Percutaneous CoronaryIntervention improved by using Combination drug therapy?
David Eccleston*1, Tony Rafter2, Geoff Holt2, Peter Sage3, Alan Whelan4, Donald Latchem4,Mark Horrigan51Cardiology, Royal Melbourne Hospital, Melbourne, 2Cardiology, Heart Care Partners, Brisbane,3Cardiology, Adelaide Cardiology, Adelaide, 4Cardiology, Heart Care WA, Perth, 5Cardiology,Heart Care Victoria, Melbourne, Australia
Introduction: Treatment compliance remains a major barrier to improving patient carefollowing percutaneous coronary intervention (PCI). Poor compliance with aspirin and
e100
clopidogrel therapy after drug-eluting stent (DES) implantation increases the risk ofrecurrent cardiovascular events. New combination drugs such as Co-Plavix may assistcompliance by simplifying treatment regimens and reducing patient expenses. Also,although registries have evaluated outcomes after percutaneous coronary intervention (PCI)in the USA, few data exist regarding Quality of life (QOL) after PCI in Australia.Objectives: This study aims to assess the impact of combination drug therapy andcoaching to improve compliance post-PCI using the Heart Care Group PCI Registry.We also aim to report the effect of combination therapy on long-term QOL This willallow comparison of clinical and PCI outcomes with international standards, andimprove patient management by facilitating the appropriate application of clinicalguidelinesMethods: We prospectively enrolled 500 consecutive patients undergoing PCI at 8Australian private hospitals from November 2012 to August 2013 using a cluster ran-domisation design to combination (Co-plavix) or usual individual anti-platelet therapy.Nurses provided compliance support if non-compliance with Co-Plavix treatment wasnoted at follow-up; control patients received usual care only. Baseline patient/proceduraldata, 1 year clincal outcomes, compliance (using the Morisky tool and prescriptioncounting) and QOL (using the EQ5D scale) were recorded and stored electronically in theDepartment of Epidemiology at Monash University.Results: The mean age was 67 � 12 years. Females comprised 25.1 %, diabetics 23.3%,35.3% were obese (BMI>30) and 37.2% had acute coronary syndromes. At least one DESwas used in 64.9% of PCI. Procedural success rates were 97%. In patients not takingWarfarin, 99.0% were taking aspirin and 97.7% clopidogrel at discharge.
Conclusion: Combination drug therapy achieved superior anti-platelet medicationcompliance one-year post-PCI compared to individual drug therapy. Quality of life was notimproved possibly due to the higher risk profile of the active treatment group.Disclosure of Interest: None Declared
PM187
Do Drug-Eluting Stents Reduce 1-year Readmission rates after PercutaneousCoronary Intervention in Australian Private Hospitals? Results from a NationalMulti-Centre Registry
David Eccleston*11Cardiology, Royal Melbourne Hospital, Melbourne, Australia
Introduction: Up to 10% of US patients are readmitted within 30 days of PercutaneousCoronary Intervention (PCI), and readmission is associated with increased one-year mor-tality. Rates of 30 day readmission may be reduced in high-volume centres. However littleAustralian data exist on potential predictors of late readmission such as use of Drug-elutingStents (DES) and the implications of late readmission.Objectives: We aimed to report the incidence and predictors of readmission up to 12months post-PCI from the Genesis Heart Care Group Registry.Methods:We prospectively collected data on 5002 consecutive patients undergoing PCI to6837 lesions at 8 Australian private hospitals from November 2009 - August 2013 andanalysed predictors of readmission and long-term outcomes.Results: Australian PCI patients had a 1-year cardiac readmission rate of 13.0%; this was11.5% if planned PCIs were excluded. The mean age was 67�12 years. Females comprised25.1 %, diabetics 24.5%, 32% were obese (BMI>30) and 37.2% initially underwent PCI foran acute coronary syndrome. At least one DES was used in 64.9%.
GHEART Vol 9/1S/2014 j March, 2014 j POSTER/2014 WCC Posters