plantar plate rupture - acurity...plantar plate function • fibrocartilaginous structure • acts...
TRANSCRIPT

Plantar Plate Injuries
Kim Tottenham
Podiatrist

Exercise is Medicine
• Physical inactivity is a major health
problem
• Keep people moving.

Plantar Plate Injuries
• Anatomy
• Mechanism of injury
• Assessment and clinical tests
• Diagnosis and differential dx
• Imaging
• Conservative treatment options.

Plantar Plate Function
• Fibrocartilaginous
structure
• Acts as an attachment for
PF
• Stabilising digits
• Reduces compressive
loads on met heads
• Role in windlass action
• Helps with the line of pull
of the lumbricals and
FDL.

Anatomy 3 points regarding injuries:
1. Differences at origin & insertion
2. Avascular nature
3. Length of metatarsals – vulnerability
(acknowledgement for Ted Jedynak, 2015)

Plantar Plate Injuries
tarsal

Assessment
Signs and Symptoms:
• Focal pain distal to MTPJ’s
• Hx of trauma/tripping
• c/o “lump” or “bruised feeling”
• Notice gradual hammering of
digit
• Associated hallux valgus
• Forefoot in prolonged
dorsiflexion.
• Callus formation if chronic.
Mechanism of Injury:
• Excessive load on MTPJ while
in dorsiflexion.
• Progressive overload eg 1st
MTPJ arthritis, HAV, short 1st
met, long 2nd, abnormal bmx
overloading mets, steroid
injection, acute trauma.
• What is the patient telling you:
– “I’m a rugby prop/ a ballroom
dancer/do lots of gardening...”
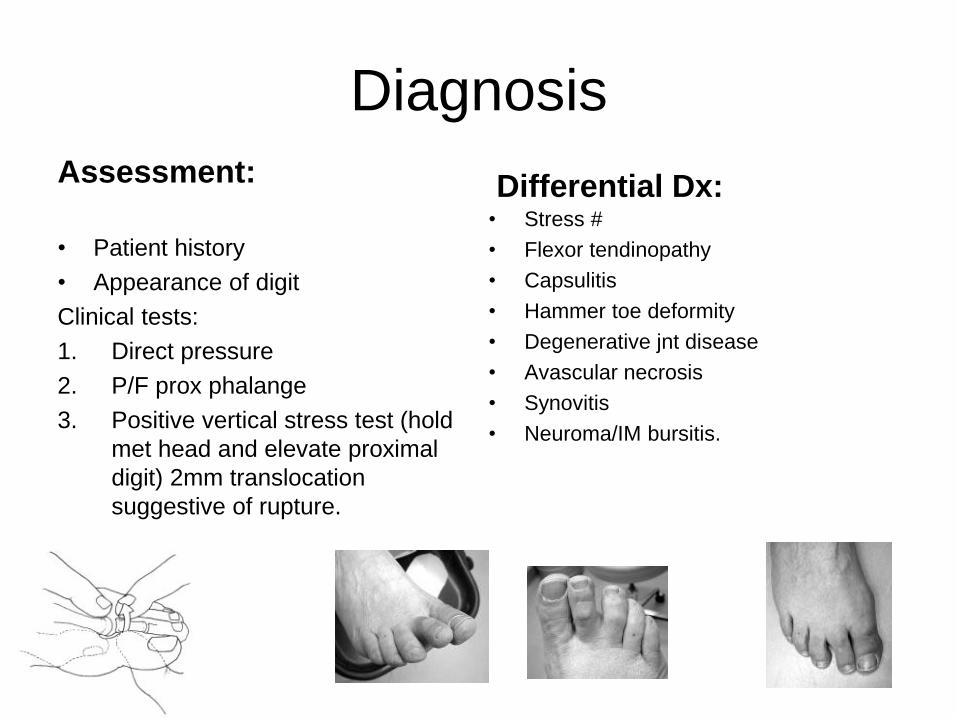
Diagnosis
Assessment:
• Patient history
• Appearance of digit
Clinical tests:
1. Direct pressure
2. P/F prox phalange
3. Positive vertical stress test (hold
met head and elevate proximal
digit) 2mm translocation
suggestive of rupture.
• Stress #
• Flexor tendinopathy
• Capsulitis
• Hammer toe deformity
• Degenerative jnt disease
• Avascular necrosis
• Synovitis
• Neuroma/IM bursitis.
Differential Dx:

Imaging
X-ray always WB, DP and lateral
Shows subluxation/dislocation
Ultrasound is helpful, dynamic
Differential dx:
• Tear
• Rupture
• Neuroma/IM bursitis.
1. Sonographer can stress the tissues in different directions, to identify where the breakdown of the plantar plate lies.
2. Colour doppler is useful can detect blood flow.
3. Useful if there is a cortisone injection for guidance. (Not recommended).

Treatment
Aim: realignment of digit/pl plate.
Facilitate “toe purchase”. Prevent or
slow progressive deformity. Cushion
painful MTPJ’s. Reduce pain.
•Strapping/taping (6-12 weeks) , esp if
no deformity.
•Rest from aggravating factors.
•Orthotics/padding to realign digit.
Aim to provide a dorsiflexory force to
the metatarsals while allowing plantar
flexion of digits. Improves the
apposition of torn ligament tissues.
•Shoes with a rocker bottom.
•Avoid U-shaped design (p/f of met)
can worsen the hammering of the
digit.
•Immobilisation
•Physical Therapy - self mobilise
dorsal extensor tissues - exercises
•NSAID’s
•Corticosteroids oral
–No injections (weakens connective
tissues/small risk of sepsis)
•Surgery.

Three Key Elements for
Successful Treatment
1. Clear communication
2. Remove tissue stress
3. Dorsal extensor releases.
(Acknowledgement to Ted Jedynak, educator)

Forefoot Pain