pkh spot check - fkm ui · djazuly chalidyanto, skm, mars – fakultas kesehatan masyarakat...
TRANSCRIPT

PKH SPOT CHECK
QUANTITATIVE AND QUALITATIVE ASSESSMENTS TO MONITOR HOUSEHOLD CONDITIONAL CASH
TRANSFERS OPERATIONS
Center for Health Research University of Indonesia
Submitted to the World Bank
Jakarta, 2010

i
RESEARCH TEAM AND LOCAL PATNERS
Research Team:
Prof. dr. Budi Utomo, MPH, PhD
Prof. dr. Hasbullah Thabrany, MPH, DrPH
Dr. drg. Mardiati Nadjib, M.Sc
Dr. dr. Sabarinah Prasetyo, M.Sc
Nur Berlian Venus Ali, M.Ec
Drs. Heru Suparno, M.Kes
Purwa Kurnia Sucahya, SKM, M.Si
Besral, SKM, MPH
Vetty Yulianty Permanasari, S.Si, MPH
Amila Megraini, SE, MBA
Hendri Hartati, SKM, MKM, MPH
Kurnia Sari, SKM, MSE
Puput Oktamianti, SKM, MM
Dwiastuti Yunita Saputri, SKM
Local Partners:
Ir. Abdullah Dja’far, MS – Fakultas Pertanian Universitas Lambung Mangkurat
Kalimantan Selatan
Anwar Fachry, M.Sc – Pusat Penelitian Kependudukan dan Pembangunan Universitas
Mataram
Agus Dwi Setiawan, S.Sos, M.Kes – Pusat Penelitian Kesehatan Universitas Indonesia
Djazuly Chalidyanto, SKM, MARS – Fakultas Kesehatan Masyarakat Universitas
Airlangga
Rahmat, SE, ME – CEDS (Center for Economics and Development Studies) Universitas
Padjajaran

ii
PREFACE
Our praise and gratitude to God the Almighty that with His grace and strength, this
report is completed. Spot-check was undertaken in nine districts in six provinces
involving 1,800 participants, nine operators, 108 facilitators, 108 schools, 108 health
facilities, and a number of relevant sectors in the national and local levels from
October 2009 to February 2010.
The goal of the spot check is to assess the program process as one component of the
monitoring and evaluation of Keluarga Harapan (literally means “Family of Hope”, it
is a Conditional Cash Transfer) Program. The foci of the spot check are primarily on
the program components: payment mechanism, compliance of participants to
requirements, education and health service delivery, data validation and updates,
system for accepting and resolving complaints, dissemination, training and
coordination, and relevant actors’ understanding of rules and procedures. The spot
check was under the Auspices of the National Development Planning Agency
(Bappenas), funded by the World Bank, and implemented in collaboration with the
Center for Health Research, University of Indonesia.
A number of people and institutions have provided assistance either directly or
indirectly so that spot check was carried out and the report is completed. First of all,
our research team would like to thank all informants, participants, team leaders,
facilitators, operators, and actors in relevant sectors at central and local levels that
provided their time and the information we needed. In particular, our research team
thanked the interviewees at the central level that have provided inputs and support
from field visit to report preparation especially to DR. Pungky Sumadi (Bappenas),
DR. Harapan Lumban Gaol (Ministry of Social Affairs), DR. Budi Hidayat (the World
Bank), DR. Vivi Alatas (the World Bank) and many others whose names cannot be
mentioned one by one.
Finally, we hope that the results of the spot check will contribute to improvement of
the CCT (Keluarga Harapan) Program.
Depok, April 2010
The Research Team
The Center for Health Research, University of Indonesia, Room 211, Building G,
FKMUI, UI Campus, Depok, 16424. Telephone: 021-7270154, Facs: 021-7270153

iii
TABLE OF CONTENT
RESEARCH TEAM AND LOCAL PATNERS ......................................................................................i
PREFACE...................................................................................................................................... ii
TABLE OF CONTENT ................................................................................................................... iii
LIST OF TABLE ........................................................................................................................... vii
ABREVIATION ............................................................................................................................. ix
EXECUTIVE SUMMARY .............................................................................................................. xii
INTRODUCTION .................................................................................................................... xii
DATA AND METHODS .......................................................................................................... xiii
RESULTS AND DISCUSSION .................................................................................................. xiv
SUMMARY AND RECOMMENDATIONS ............................................................................. xxiv
Chapter 1 Introduction ............................................................................................................ 1
1.1. Background ..................................................................................................................... 1
1.2 Objectives ....................................................................................................................... 4
CHAPTER 2 METHODOLOGY ..................................................................................................... 5
2.1 Framework/ detail of pkh spot check activities .............................................................. 6
2.2. Data Sources ................................................................................................................... 8
Survey to Relevant Stakeholders ..................................................................................... 10
2.3 Informants ..................................................................................................................... 13
2.4 Location and samples .................................................................................................... 13
2.5 Process to maintain quality of Spot check .................................................................... 14
2.6 Ethical Review ................................................................................................................ 14
2.7 Permit ............................................................................................................................ 15
2.8 questionnaire and data collection protocols................................................................. 15
2.9 Personnel competency .................................................................................................. 15
2.10 Local partners and capacity improvement .................................................................. 15
2.11 Trainings ...................................................................................................................... 16
2.12 Data collection ............................................................................................................. 16
2.13 Supervision .................................................................................................................. 17
2.14 Data Entry .................................................................................................................... 17
2.15 Data quality monitoring .............................................................................................. 17
2.16 Analysis ........................................................................................................................ 18

iv
CHAPTER 3 CHARACTERISTICS OF PKH BENEFICIARIES .......................................................... 19
3.1 Pregnancy, childbirth and child(ren) under 15 years old ............................................. 19
3.2 Demographic Profile of household members ............................................................... 20
3.3 Main job of head of households .................................................................................... 21
3.4 Poverty indicators .......................................................................................................... 22
3.5 Participation in poverty alleviation program ................................................................ 23
3.6 smoking behavior .......................................................................................................... 25
CHAPTER 4 DATA VALIDATION AND UPDATE .......................................................................... 26
4.1 Validation....................................................................................................................... 27
4.1.1 Validation during the first meeting ........................................................................ 27
4.1.2 Constraints in conducting initial meeting ............................................................... 28
4.2 Data Updates ................................................................................................................. 29
4.2.1 Household demographic changes reported by beneficiaries and facilitators ........ 29
4.2.2 Database entry and management problems .......................................................... 31
4.2.3 Discrepancy of beneficiaries data in the central database and on the field .......... 32
CHAPTER 5 THE PAYMENT PROCESS ....................................................................................... 37
5.1 amount of payment ....................................................................................................... 37
5.1.1 Payment Based on Household Composition ........................................................ 37
5.1.2 Payment against signed receipt............................................................................. 39
5.2 the Payment process .................................................................................................... 41
5.2.1 Payment Reconciliation .......................................................................................... 41
5.2.2 Schedule and Delay of Payment ............................................................................. 41
5.2.3 The Role of Facilitator in the Payment Process ...................................................... 43
5.2.4 Payment Location and Transportation Cost ........................................................... 43
5.2.5 Waiting Time in the Payment Location .................................................................. 43
5.3 Deduction of the cash transfer fund ............................................................................. 43
5.4 The use of PKH fund ...................................................................................................... 44
5.5 Pawned beneficiary’s card ............................................................................................. 45
CHAPTER 6 COMPLIANCE TO CONDITIONALITY ...................................................................... 46
6.1 Utilization of education services ................................................................................... 47
6.1.1 6-15 year-old child(ren) who do not go to school and drop out ............................ 47
6.1.2 Children 6-15 year old who go to school ............................................................... 48
6.2 Utilization of health services ......................................................................................... 49
6.3 Compliance verification process.................................................................................... 51

v
6.3.1 Printing of verification Forms ................................................................................. 51
6.3.2 Verification form acceptance ................................................................................. 52
6.3.3 Completion of verification forms ........................................................................... 54
6.3.4 Collection of verification forms from service facilities ........................................... 56
6.3.5 Delivery of verification forms to the UPPKH district / municipality ....................... 57
6.3.6. Constraints in entering verified data and forwarding them to central ................. 57
6.3.7. Utilization of verification results ........................................................................... 58
CHAPTER 7 SERVICE PROVISION .............................................................................................. 60
7.1 Provision of education services ..................................................................................... 60
7.1.1 Distance, travel time and modes of transportation to school ............................... 60
7.1.2. Tuition Fee ............................................................................................................. 62
7.1.3 Quality of education services ................................................................................. 63
7.2 Provision and quality of health services ........................................................................ 68
7.2.1 Access to health services ........................................................................................ 68
7.2.2 Health Service Quality ............................................................................................ 69
CHAPTER 8 COMPLAINT RESOLUTION SYSTEM ....................................................................... 80
8.1 Beneficiaries are not well-informed on how to submit complaints .............................. 81
8.2 Complaint mechanism is not well running ................................................................... 82
8.3 Solution for the complaints ........................................................................................... 83
8.4 Problems encountered in submitting complaints ......................................................... 84
CHAPTER 9 SOCIALIZATION, TRAINING AND COORDINATION ................................................ 86
9.1 Socialization ................................................................................................................... 86
9.1.1 Ineffective socialization to other sectors ............................................................... 86
9.1.2 Unclear Roles & Responsibilities for Sectors Implementing Socialization, Mainly
Ministry of Communications and Information Technology (MCIT) ................................. 89
9.1.3 Unqualified socialization ........................................................................................ 91
9.2 Training .......................................................................................................................... 94
9.3 Coordination .................................................................................................................. 96
CHAPTER 10 Knowledge of program rules and procedures ................................................. 101
CHAPTER 11 Discussions, Conclusion and Recommendation. .............................................. 106
11.1. Discussions ............................................................................................................... 106
Database validation and update.................................................................................... 107
Payment ......................................................................................................................... 108
Compliance to conditionality......................................................................................... 109

vi
Service provision ........................................................................................................... 110
Complaint acceptance and resolution system .............................................................. 111
Socialization, training and coordination ........................................................................ 112
Knowledge of program rules and procedures ............................................................... 113
11.2. Conclusion and recommendations ........................................................................... 114

vii
LIST OF TABLE
Table 2. 1. The Framework of The PKH Spot Check.................................................................. 6
Table 2. 2. Relevant Institutions / stakeholders, Informants, and Data.................................. 10
Table 3.1. Percentage of households with childbirth in the last 24 months, child(ren) under
15 years old and pregnancy during survey. ............................................................................. 19
Table 3.2. Demographic characteristics of PKH household members .................................... 21
Table 3.3. Distribution of head of households’ job ................................................................ 22
Table 3.4. Characteristics of socio economic of PKH beneficiaries’ ........................................ 23
Table 3.5. Distribution of participants who received aid from other poverty alleviation
programs ................................................................................................................................. 24
Table 3.6. Smoking rate and expenses .................................................................................... 25
Table 4.1. Validation of beneficiary’s household data ............................................................ 27
Table 4.2. Percentage of households who experienced changes since PKH recruitment until
the time of this survey, by province ........................................................................................ 30
Table 4.3. Percentage of households that reported changes and signed the form out of all
households that had these changes ........................................................................................ 31
Table 4.4. Percentage of households with different data between central database and
results of spot check ................................................................................................................ 33
Table 4.5. Discrepancy of pregnant women data of spot check and ...................................... 34
Table 4.6. Discrepancy of under-five children data in the central database and result of spot
check ........................................................................................................................................ 34
Table 4.7. Discrepancy of school age children data in the central database .......................... 35
Table 5.1. Percentage of beneficiaries with correct and incorrect payment as compared to
the household composition ..................................................................................................... 38
Table 5.2. The average of Incorrect Payment (Rupiah) as Compared to ................................ 38
Table 5.3. Percentage of Beneficiaries Receiving Same Amount of Payment as What They
signed on the receipt ............................................................................................................... 39
Table 5.4. Reason for payment delay (%) ............................................................................... 42
Table 5.5. Percentage of beneficiaries who had and did not have Cash Transfer deduction 44
Table 5.6. Distribution (%) of the use of PKH cash transfer ................................................... 45
Table 6.1. Distribution (%) of school-age children who do not go to school and drop out .... 47
Table 6.2. Distribution of children 6-15 years who go to school by levels and attendance ... 48
Table 6.3. Percentage of health service utilization for under-five children ............................ 49
Table 6.4. Percentage of pregnant women who utilized health services by type of services 50
Table 6.5. Percentage of Delivery , Post Partum and newborns who utilized health services 51
Table 6.6. Verification forms received by the facilities .......................................................... 52
Table 6.7. Completion of verification forms at school and Puskesmas ................................... 54
viii
Table 6.8. Collection of verification forms from service facilities by PT Pos .......................... 56
Table 6.9. Delivery of verification forms to the District/Municipality UPPKH ....................... 57
Table 6.10. Distribution (in %) of data entry problems in UPPKH District/municipality ........ 58
Table 7.1. Mean Distance (km) from Home to School ............................................................ 60
Table 7.2. Travel time (minute) from home to school ............................................................ 61
Table 7.3. Distribution of transportation modes from home to school .................................. 61
Table 7.4. Transportation Fee from Home to School .............................................................. 62
Table 7.5. Percentage of PKH beneficiary’s school-age children who had scholarship and
paid tuition fee ........................................................................................................................ 63
Table 7.6. Distribution of number of teacher by Province and school level ........................... 64
Table 7.7. Distribution of teachers who meet quality standard by province and school levels
................................................................................................................................................. 65
Table 7.8. Ratio of learning group per classrooms and number of students per learning group
................................................................................................................................................. 66
Table 7.9. Percentage of facility-infrastructure at schools ..................................................... 67
Table 7.10. Availability of Personnel in the Puskesmas by Type and Province (%) ................. 69
Table 7.11. Provision of Puskesmas Services by Provinces (%) ............................................... 70
Table 7.12. Percentage of Puskesmas with ANC or Delivery Service Equipment by Province 71
Table 7.13. Percentage of Puskesmas that Had Vaccine Stock Out in the Last One Year by
Province ................................................................................................................................... 72
Table 7.14. Percentage of Puskesmas by Drugs and Vaccines Storage ................................... 73
Table 7.15. Availability of Supporting mmaterials for Services in Puskesmas ........................ 74
Table 7. 16. Percentage of Puskesmas that Did Postpartum Visits as Required by the Health
Service Protocols ..................................................................................................................... 75
Table 8.1. Percentage of types of complaints according to PKH beneficiaries ....................... 82
Table 8.2. Percentage of respondents who were aware of UPM and have been informed on
how to submit complaint ........................................................................................................ 83
Table 8.3. Percentage of beneficiaries who were offered solutions and who considered them
to be satisfactory ..................................................................................................................... 84
Table 9.1. Percentage of Operator and Facilitator Who Ever Exposed to or Know About
Socialization Activity by CCT Implementing Organization ....................................................... 91
Table 9.2. Percentage of respondents who ever received socialization materials ................. 93
Table 9.3. Value scale on Training Organization conducted by Operator and Facilitator (%) 95
Table 10.1. The knowledge of beneficiaries on PKH ............................................................. 102
Figure 2. 1. Source of Data and Assessment Verification of PKH Processes ............................. 9

ix
ABREVIATION ANC : Antenatal Care
APBD : Anggaran dan Pendapatan Belanja Daerah = Local Government Funding
APBN : Anggaran dan Pendapatan Belanja Negara = Central Government Funding
ART : Anggota Rumah Tangga = Member of Household
ATK : Alat Tulis Kantor = Office Supply
Balita : Bawah Lima Tahun = Under Five Years Old
Bappeda : Badan Perencana Pembangunan Daerah = Bureau of Local Development Planning
Bappenas : Badan Perencana Pembangunan Nasional + Bureau of National Development Planning
Imunisasi BCG : Imunisasi “Bacilli Calmette Guerin” untuk mencegah penyakit Tuberculosis = BCG Immunization
BLT : Bantuan Langsung Tunai = Unconditional Cash Transfer
BPS : Badan Pusat Statistik = Central Board of Statistics
Bulin : Ibu Bersalin = Woman in birth delivery
Bumil : Ibu Hamil = Preganant woman
CCT : Conditional Cash Transfer
Co PI : Co Principal Investigator
DFC : District Field Coordinator
Dinkes : Dinas Kesehatan = Provincial or District/ Municipal Health Office
Dinsos : Dinas Sosial = Provincial or District/ Municipal Social Affair Office
Disdik : Dinas Pendidikan = Provincial or District/ Municipal Education Office
Imunisasi DPT : Imunisasi untuk mencegah penyakit Dipteri, Pertusis, Tetanus = Diphtheria, Pertusis, and Tetanus Immunization
Fasdik : Fasilitas Pendidikan = Education Facility
Faskes : Fasilitas Kesehatan = Health Facility
FGD : Focus Group Discussion
ILO : International Labor Organization
IPA : Ilmu Pengetahuan Alam = Natural Science

x
IPS : Ilmu Pengetahuan Sosial = Social Science
Jabar : Jawa Barat = West Java
Jamkesmas : Jaminan Kesehatan Masyarakat = Social Health Insurance
Jatim : Jawa Timur = East Java
K1 : Kunjungan pertama antenatal = First antenatal care visit
K4 : Kunjungan keempat antenatal = Fourth antenatal care visit
Kabupaten HSS : Kabupaten Hulu Sungai Selatan = Hulu Sungai Selatan District
Kades : Kepala Desa = Village Head
Kalsel : Kalimantan Selatan = South Kalimantan
Kemendiknas : Kementerian Pendidikan Nasional = Ministry of National Education
Kemenkes : Kementerian Kesehatan = Ministry of Health
Kemenkominfo: Kementerian Komunikasi dan Informasi = Ministry of Communication and Information
Kemensos : Kementerian Sosial = Ministry of Social Affairs
KIA : Kesehatan Ibu dan Anak = Mother and Child Health
KMS : Kartu Menuju Sehat = Health Card
Korwil : Koordinator Wilayah = Regional Coordinator
KRT : Kepala Rumah Tangga = Head of Household
KTM : Kartu Tanda Miskin = Poor Card
KTP : Kartu Tanda Penduduk = Resident Identity Card
MDGs : Millennium Development Goals
MI : Madrasah Ibtidaiyah= Elementary Islamic School
MTs : Madrasah Tsanawiyah = Junior High Islamic School
NSPK : Norma, Standar, Prosedur, Kriteria = Norm, Standard, Procedure, Criteria
NTB : Nusa Tenggaran Barat = West Nusa Tenggara
Pemda : Pemerintah Daerah = Local Government
Penjaskes : Pendidikan Jasmani dan Kesehatan = Physical and Health Education
PFC : Provincial Field Coordinator
PI : Principal Investigator
PKH : Program Keluarga Harapan = Family Hope Program
PLC : Provincial Local Counterpart
Posyandu : Pos Pelayanan Terpadu = Integrated Health Post

xi
PPKUI : Pusat Penelitian Kesehatan Universitas Indonesia = Center for Health Research University of Indonesia
Puskesmas : Pusat Kesehatan Masyarakat = Health Center
Pustu : Puskesmas Pembantu = Auxiliary Health Center
RASKIN : Beras Miskin = Rice for the poor
Rombel : Rombongan Belajar = Learning Group
RTSM : Rumah Tangga Sangat Miskin = Very Poor Household
S1 : Strata satu, sarjana = Bachelor degree
Sarpras : Sarana dan Prasarana = Equipment and Infrastructure
SD : Sekolah Dasar = Elementary School
SIM PKH : Sistem Informasi Manajemen Program Keluarga Harapan = Management Information System for the Family Hope Program
SKS : Satuan kredit Semester = Credit Unit Semester
SKTM : Surat Keterangan Tidak Mampu = Letter Explaining the Poor
SLT : Sumbangan Langsung Tunai = Unconditional Cash Transfer
SLTP : Sekolah Lanjutan Tingkat Pertama = Junior High School
SNP : Standar Nasional Pendidikan = National Standard of Education
SOP : Standard Operating Procedure
TKPKD : Tim Koordinasi Pengentasan Kemiskinan Daerah = Local Coordination Team for Poverty Eradication
TOT : Training of Trainer
TT : Tetanus Toxoid
UPM : Unit Pengaduan Masyarakat = Community Complaint Unit
UPPKH : Unit Pelaksana Program Keluarga Harapan = Implementing Unit of the Family Hope Program
UPTD : Unit Pelaksana Teknis Daerah = Local Technical Implementing Unit

xii
EXECUTIVE SUMMARY
INTRODUCTION
As part of the commitment to achieve the MDGs, the Government of Indonesia
implemented programs to reduce poverty by improving education and health of
young people among other the PKH (CCT). The PKH started in July 2007 to cover
382,000 very poor households (RTSM) in seven provinces and in 2008 it is expanded
to 720,000 RTSM in 13 provinces. Requirements to join PKH are RTSMs with
pregnant, or lactating woman and/or having under-16 child(ren) or up to 18 who do
not complete nine years of basic education.
Mothers in RTSM are selected as the recipient of PKH because they play the key
roles and are most responsible in improving child(ren)'s education and health along
with their own health. Eligible women receive a minimum of Rp 200,000 a year in
cash. Then, additional cash transfer is given when they meet the conditionality on
utilization of basic education and/or health services. The amount of cash transfer will
increase to a maximum of Rp 2,200,000 per year per RTSM in accordance with the
number of pregnant or lactating mothers, and/or having under-16 or up to 18
child(ren) who met the conditionality of utilizing basic education and health services.
The implementation of PKH is under the responsibility of the Ministry of Social
Affairs (Kemensos) Central Executive Unit Office of PKH (UPPKH) and Provincial and
District/City Social Affairs Office’s UPPKH under the coordination of the Governor or
Bupati/Mayor at the district/city level. Other sectors or organizations involved in
PKH are Bappenas, BPS, PT. Pos, Kemendiknas (Ministry of National Education),
Kemenkes (Ministry of Health), Kemenkominfo (Ministry of Telecommunication and
Information) and relevant offices at the provincial and district / city levels. Due to
the involvement of a number of sectors and organizations, PKH management
becomes a very complex issue and requires the best organization and management.
Due to its complexity, PKH implementation is susceptible to problems and
misconducts against applicable rules and procedures. Some of the problems include
inaccurate targeting, incompliance to conditionality, inappropriate payment,

xiii
problem in provision and quality of services, sub optimum data update, and
inappropriate complaint acceptance and solution. Reliable management information
system is needed to detect all problems and misconducts and correct them. Spot
check were conducted from October 2009 to February 2010 by non-PKH
organizations to ensure objectivity and constituted an important part of the
management information system. The spot check focused on 7 (seven) important
components of PKH including: 1) payment, 2) incompliance to conditionality, 3)
education and health service delivery, 4) data validation and update, 5) complaint
management of, 6) dissemination and training, and 7) understanding of relevant
actors about PKH rules and procedures.
DATA AND METHODS
The method used for the spot check is a survey, complemented with qualitative
studies to identify problems and misconducts in the program implementation
process and to explain why the problems occurred. The focus was the
implementation process and this spot check did not assess the achievement of the
objectives of the program.
Out of 13 PKH provinces, the spot check purposively select 5 (five) of them, three
provinces represented areas that started the program in 2007 and two other
represented program commenced in 2008. The province selection design was
originally intended to assess whether the starting year was related with
performance. In fact the three provinces that started the program in 2007 are in Java
Island (DKI Jakarta, West and East Java) and two other provinces that started in 2008
are provinces outside Java (West Nusa Tenggara and South Kalimantan). It
complicated the spot check to explain differences in program performance between
PKH starting in 2007 and 2008, whether these differences are due to the starting
year or the locations (in and outside Java Island).
Next, except for DKI Jakarta, in each province we selected two districts/cities and in
each of these districts we selected 4 (four) sub districts. The selection of a
district/city took into account the number of PKH participants to ensure adequate

xiv
sampling. In each selected sub district the survey was done to 50 woman-
participants, five women as group leaders, three facilitators, two Elementary Schools
or Madrasah Ibtidaiah(MIs)-Islamic Elementrary School, one Junior High School/
Madrasah Tsanawiyah (MT)—Islamic Middle School and one Puskesmas and its
network. Overall, through surveys the spot check collected data of 1,800 participant
mothers, 180 mothers as group leaders, 108 facilitators, 36 sub district post offices,
72 Elementary Schools/MIs, 36 Junior High Schools/MTs, and 36 Puskesmas and their
networks across 36 sub districts in nine cities/districts in five provinces. At the
district/city level, the survey involved 9 operators/ UPPKH and nine post offices. In-
depth interviews were conducted to key personnel in relevant sectors at central and
district/city levels, relevant personnel or informants at the sub district level down to
women as group leaders. A focus group discussion was conducted to one group of
facilitators and one group of participants per district/city.
Quantitative data were collected through survey using structured questionnaire that
had been tested for validity and reliability, while the qualitative data through in-
depth interviews and focus group discussions using semi structured question
guideline. The questions for respondents or informants were about program
implementation process.
RESULTS AND DISCUSSION
Results from spot check were presented in the form of findings classified into seven
key themes and expected to serve as materials for program improvement. The
findings identify the extent of the implementation process whether it was in line
with the rules and procedures established in the PKH guidelines.
Data validation and updates were reported on special forms to the district/city to be
entered into an online information system and submitted to the central level to be
approved. The results of spot check showed that the process was not satisfactory. As
many as 95% of participants surveyed attended the initial meeting but only 85% of
them were validated. Not all of those who were not present at the initial meeting,

xv
were visited for validation. Taking into account those who did not come at the initial
meeting, only 82% of participants could be validated during the initial meeting.
Inaccurate names, unknown addresses, spread out houses, and difficult geographical
conditions were among the constraints in distributing invitation for the initial
meeting or home visit for validation.
In some villages, facilitator’s and community reports showed intentional
mistargeting or unsuitable listing of a poor household (RTSM). A facilitators’ group
discussion in one province revealed that some PKH participants in some villages
were village staff or relatives of village staff who were not qualified as RTSM. This
could happen because the particular village staff was the data collectors for a BPS
survey in 2005 to identify RTSM. There were many complaints from the community
who felt poorer than the participants but were not listed as PKH participants. In the
concept, PKH participants deserved benefits from other poverty alleviation
programs, but spot check revealed that only 69% of them had Jamkesmas card and
only 18% of them received scholarships for the poor.
In the PKH guideline, participant database should be updated in line with the
household demographic changes timely. However, not all households reported
demographic changes. Out of all participants with demographic changes, only 54% of
2007 PKH participants and 76% of 2008 PKH participants admitted that they signed
the update form. Scarcity of update forms was among the barrier for not reporting
demographic changes.
Despite availability of updated form, database was not automatically updated. Six of
nine district/city operators inputed changes three times in 2009, while the guideline
requires updates once a month. In some districts, the change was entered only if
there was a plan for payment.
Difficulties in demographic updates at district/city level included frequent power
shut down and limited computers and/or operators. In some cases, the operators
entered the update, but the participant’s data printed in the payment did not
change. This could happen because: (1) online application system between

xvi
district/city and central databases often did not function, (2) changes in the
district/city database were not automatically approved by Central MIS officials.
Spot check revealed data mismatched between spot check and the central database.
As many as of data of 27% pregnant mothers or school children parameters in the
spot check did not matched with the central database. Some findings of discrepancy
data recorded at the central database are: an old woman who lived alone with no
child registered as PKH beneficiary, Mrs. X was reported dead, but she is still listed as
PKH beneficiary, participant X haa moved, but the address was not updated for
payment, a person did not receive any payment but her name is in the payment list,
a child who graduated from Junior High School was still recorded in the P form, a
woman who had delivered a baby, but she was listed as pregnant mother, etc.
Many factors are believed to contribute to the discrepancy of central database with
actual RTSM data. These include: different time reference between spot check and
last data update, some candidates’ RTSM data were not validated, and participants
did not report demographic changes immediately. In addition, facilitator failed to
recognize or to report household changes to UPPKH at the district/city. Furthermore,
at the district/city level, operators, due to other things, did not input changes
immediately into the database. In the meantime, staff at the Central UPPKH
sometimes did not immediately approve changes by the district/city operators and
update into the central database. The consequence of inaccurate data of the central
database was inaccurate amount of payment according to the composition of RTSM
members.
Payment to participants is based on household composition data and compliance of
participants to conditionality in utilizing education and health services. Spot check
revealed that the program made payments to participants based on household
composition data, but not on compliance to conditionality. Payment based on
compliance to conditionality will be implemented gradually starting in early 2010. To
do this, the program piloted compliance-based payment in 23 districts. For smooth
application of compliance-based payment, the Central UPPKH staff needs to
understand the importance of a fully functional compliance verification system.

xvii
The amount of payment should be based on household composition of pregnant,
lactating mothers, school age children, or under-16 or 18-year old children who have
not completed Junior High Schools/MTs. Based on composition household data, the
spot check survey found that 75% of participants received appropriate payments, 8%
received less and 17% received more than they should. Payment schedule and
frequency in some districts/cities did not follow a predetermined schedule. The
guideline indicates that payments should be made 4 (four) times a year, but in many
subdistricts payments were made 3 (three) times and even in some others only 2
(two) times a year. The central level contributed to the irregular payments and
affected the readiness of district/city management to proceed the payments.
Irregularities of payment schedule and frequency made participants to utilize the
money for their basic needs. Rounding of payment also caused differences in the
amount of money a participant received with the receipt he/she signed.
As many as 94% of participants confirmed that they received the same amount of
money as written in the receipt they signed. However, 16% of participants confessed
that they gave a tip or their money was deducted. A group discussion with
facilitators and interviews with participants confirmed that there were deductions or
tip varied from 10 to 50 thousand Rupiahs per payment depending on the amount
paid. Some participants who had this deduction did not bother about it, but instead,
they were grateful to accept the cash transfer. No clear and strict sanctions made to
those who deducted the beneficiaries’ money.
On the other hand, there were cases of dishonest beneficiaries to obtain greater
amount of cash transfer such as, a woman who was not pregnant admitted that she
was pregnant, or a woman who claimed her child was in elementary school but
actually the child was only 4 (four) years old. The majority of beneficiaries’
understood that PKH is a conditional cash transfer program with the condition of
basic education and health services utilization.
Compliance to conditionality is implemented through a series of activities, from
printing participant’s compliance verification form based on central database,
distribution and collection of verification form from PKH schools (Fasdik) and health

xviii
centers (Faskes) ; filling education verification form (by fasdik) and health
verification form (by faskes); entering compliance verification data online by
district/city operators, and approval as well as updating database (by the Central
UPPKH MIS). In some cases, actor was so rigid in ensuring compliance verification by
attaching photocopy of school report or child monitoring health card (KMS) () as
proof for attendance.
Many beneficiaries in this spot check did not comply with conditionality to utilize
basic health and education services. Only 84% of beneficiaries of PKH 2007 and 75%
of PKH 2008 reported that their childbirths were attended by a health a personnel.
Only 82% infants of PKH 2007 and 69% infants of PKH 2008 were weighed in the last
three months before the survey was taken. Immunization coverage for children age
one year old or above were only 71% for BCG, 29% for polio (1 initial and 2 booster),
24% for DPT (1 initial and 2 boosters), 68% for measles, and 19% for hepatitis (1
initial and 2 booster). Overall immunization coverage of 2008 PKH (outside Java)
were lower than that of 2007 PKH (Java). For compliance to education, only 2.2% of
school age children did not attend the relevant school because they did not want to
go or had no money.
Substandard verification on compliance to conditionality faced many problems such
as, inaccurate or incompatible names on the lists pregnant/childbirth mothers or
school children and delays in distribution and collection verification forms. Out of
the 30 post offices surveyed, 93% respondents stated that they sent verification
forms to faskes and fasdik, but on the other hand, only 79% of 107 faskes and 83% of
96 fasdik surveyed confirmed that they received forms. Spread out locations of
faskes and fasdik (in South Kalimantan & West Nusa Tenggara) created barrier or
difficulties in distribution and collection of verification form .
Despite the availability of verification forms, there was no guarantee that the forms
were completed accurately. Completion of K and P form were problematic in many
faskes and fasdik. Out of all K forms received by Puskesmas, only 14% were
completed, and out of all P forms submitted by the fasdik, only 27% of them were
completed. The failures to complete the forms were related with lack of financial

xix
incentives for the employees in the facilities, no knowledge on how to fill them out,
incompatible names and addresses in the forms, and difficulties in collection of
verification forms.
In addition to distribution problems, completion and collection of verification form
after they had been completed, operators in the districts/cities encountered a
number of challenges in inputing and transmitting verification data to the central
level. The challenges include: PT Pos did not submit verification forms on time,
hardware facilities were inadequate or were not working properly; lack of quantity
or quality of entry staff; frequent electricity shut down and software application and
online connection problems. The spot check confirmed the problems with central
UPPKH MIS staff.
Non-management challenges that hindered verification include: 1) participants did
not understand the conditionality to receive the cash transfer, 2) Facilitators could
not explain the urgency of compliance to all participants, 3) no enforcement or
punishment for not meeting conditionality creating false perception of no
conditionality is needed, 4) Officers at PT. Pos were not aware that optimum
distribution and collection of verification forms determine the amount of payment,
5) insufficient copies of verification forms, 6) Staff in a number of faskes and fasdik
did not know how to fill out the verification form, and 7) Staff in some faskes and
fasdik thought that filling out the verification form was an additional burden and PKH
was not theirs. As a result, some staff in relevant sectors and the community in
general considered that PKH was not different from BLT (non-conditional cash
transfer).
In quantity, Basic education services were sufficient, but the standard of quality did
matter. Only 85% of schools met the standard of teacher per learning group ratio
(rombel) of greater than one for Elementary Schools/MIs and greater than 1.5 for
Junior High Schools/MTs. Approximately two third of teachers in Elementary
schools/MIs and 17% in Junior High Schools/MTs did not finish their bachelor degree.
Furthermore, only two out of five Elementary schools/MIs and two out of three
Junior High Schools/MTs met the standard ratio of the number of students per

xx
learning group. Furthermore, only 5% of Elementary schools/MIs and two out of
three Junior High Schools/MTs had all (nine) national standard facilities and
equipments, and only 6% of Elementary Schools/MIs and 89% of Junior High
Scholls/MTs had science laboratories.
Access to basic education, either due to budget or distance was still a big problem.
Only one of six school-age children received scholarship. About 10% of children
ought to spend high transportation fees or spent a long time to reach their schools.
Efforts to improve the PKH program were not visible because the community did not
know the national standard for education services and therefore no complain was
filed. As the result of substandard quality, the teaching-learning process may not be
effective to reach the goal of PKH strengthening education.
Provision of basic health services faced challenges due to limited number and quality
of providers, drugs and vaccines, education materials, and lack of equipments and
poor infrastructure of health services. Uneven distribution of health providers
caused some districts do not have midwives in all villages. Most midwives live in the
capital of sub districts. Vaccines were generally available at Puskesmas, but some
Puskesmas had out of stock of particular drugs and vaccines in the last year.
Only half of the pregnant women who visited Puskesmas received complete
information about their health condition. On average, only 35% of them received
complete antenatal care, the lowest rate was 13% in South Kalimantan.
Spot check found out cases where PKH participants had to pay for antenatal care and
delivery , PKH participants were rejected to receive services because they did not
have Jamkesmas card and could not afford to pay. In East Java, half of the
Puskesmases surveyed did not implement the clinical protocols for postpartum
women.
Another finding of spot check is behavior of staff who did not understand PKH
concept. In addition, the staff did not consider quality of services as an important
issue or did not understand the need for it. Due to asymmetric nature of health
services and community’s difficulty to recognize service quality, no participant nor
did the community submit complaints about quality of health services. As a result,
xxi
utilization of health services is unlikely to be effective to reduce maternal and
children morbidity or mortality, thus it will hinder the achievement of PKH goals and
MDGs.
Complaint and resolution system has been already in place, but there were rooms
for improvements. Percentage of beneficiaries who had been informed on how to
submit complaints in West Java, East Java and South Kalimantan, varied between
20% and 30%, whereas in DKI Jakarta and West Nusa Tenggara the proportion
reached 50% and 60%. But, only 10% of beneficiaries in PKH 2007 and 17% of
beneficiaries in PKH 2008 knew the existence of Public Complaint Unit (Unit
Pengaduan Masyarakat, UPM). Additionally, the verbal culture made written
complaints were not submitted and or recorded in any form in the database. Only
7% of beneficiaries in PKH 2007 and 3% beneficiaries of PKH 2008 had submitted
written complaints. Out of those complainants, two-thirds received the solutions and
only two-thirds of those who received solution considered that they were 'satisfied'
to the solutions given.
Most complaints were related with payment, including incorrect amount of
payment, delays, long queues, and the Post Office was close or the staff of the post
office worked slowly. Operators received other types of complaints related with
unsatisfactory services given at faskes, fasdik and UPPKH office. In reality, 68% of all
facilitators who were surveyed, received complaints, at least verbally. Complaints
also came from community members on why they were not included as PKH
participants although they felt that they were poorer than those who were included
in PKH.
Some complaints were not resolved because they did not reach the central level or
the authority did not solve them. The shortage of forms impeded complaint reports
from participants or community. Out of seven operators who received written forms,
only five of them inputed the complaints. Low number of complaints was related
with suboptimum dissemination, the perception that government as the ruler and
should not be complained and fear of the consequences should they complain, and
the perception that the complaints would not be followed up. As a result, various

xxii
problems during program implementation were undetected and could not be
corrected.
Dissemination is an important program component that is ineffective yet. It is
reflected in the many officials in relevant sectors who did not show their
commitment to support PKH. Some relevant sector officials in the central,
district/city levels and service facilities still considered that PKH services were
additional burden for them. They reasoned that it was because they were not
involved from the beginning in the PKH. Kemenkominfo as the prime sector for
dissemination did not play their role as expected. Only 10% of operators and
facilitators said they knew Kemenkominfo conducted dissemination.
In addition to frequency, the quality of dissemination is an important element for
strengthening. Spot check findings indicated that during dissemination, participants
did not receive written materials; dissemination was delivered by inappropriate
personnel, limited time for dissemination so that not all essential materials were
discussed, and generally attendants did not report or further disseminate
information to their colleagues. Staff in fasdik and faskes also complained about the
lack of dissemination. Issues on funding availability and clarification of dissemination
funding responsibility become important and require correction. Weak
dissemination causes stakeholders to have misperception about PKH as if it is
unconditional cash transfer program.
Training to improve officers’ managerial and technical skills also needs
improvement. Operators and advisors in all areas have received training and
materials. They had received an average of five training sessions, or 2 to 3 times per
year. Types of training include initial training, Rakornas (national coordination
meeting), technical guidance, training, groups meetings, and training to alleviate
child labor. Most of the trainings (61%) were delivered by the central UPPKH and the
rest (18%) by Provincial UPPK. Most operators and facilitators said that the training
was quite good, only a few things should be improved, among others, the need to
involve fasdik and faskes personnel to ensure coordination, increase the training

xxiii
duration from three to four days, complete demonstration equipment, increase field
practice, attractive delivery and attention on participants’ diverse backgrounds.
Training to improve staff’s technical and managerial competency should increase
including skills to implement critical tasks of the program: validation and update,
verification of compliance, payment, acceptance and solution of complaints.
Coordination was one key to program effectiveness. Coordination within UPPKH
from central to district/city level runs well, but cross-sectoral coordination including
at service level did not run optimally. Personnel from relevant sectors at the central
still considered that Kemensos role was like cashier. Coordination meetings in many
districts were not routinely held, but only when the time came to payment.
Actors who attended dissemination meetings were often not the same people with
those who attended the previous ones and not all personnel of participating faskes
and fasdik were invited. Sectoral ego at the district impeded coordination. The
sectors are reluctant to attend coordination meeting if the invitation did not come
from the Bappeda as they perceived social sector as the same level and not having
power to them. Local governments considered PKH as a central level program so
they felt their commitment and authority are limited to attend coordination
meetings. Some districts have and some have not allocated budget for PKH
coordination meetings. Relevant sectors in many districts still considered that PKK
just added their workload/burden; they felt that they provided the services, but did
not get additional funding to support PKH.
In connection with weak coordination, the role and function of the TKPKD team was
not optimum. Relevant sectors at the central level did not directly instruct
subordinate offices to support PKH. Korwil’s (local coordinator) role in improve
function of monitoring and evaluation program was sub optimum. Central database
was not periodically analyzed to serve as feedback information for district/city
UPPKH. Poor supervision and guidance from central UPPKH c.q. korwil to operators
and facilitators hampered PKH function to motivate participants to utilize adequate
health and education services.

xxiv
Relevant sectors’s level of understanding about program rules and procedures, from
local governments, offices and community, was not as expected. Key personnel in
many sectors did not really understand the essence of PKH. Personnel interviewed at
the Health and Education offices and faskes as well fasdik staff in some districts did
not understand the connection between PKH and other poverty alleviation programs
such as Jamkesmas, school operational aids (BOS), and rice program for the poor.
Incomplete understanding was reflected through cases in some areas where RTSMs
that become beneficiaries of PKH were considered unqualified for other poverty
alleviation programs. These are the reflection of weak dissemination that does not
reach out to the relevant sectors and communities. In addition, dissemination
materials do not explain the relationship between PKH and other social and health
programs. Reluctance to read PKH implementation manual also caused poor
understanding of program rules and procedures. As a result, PKH implementation is
hindered and wrong perception created unrest and envy in communities.
SUMMARY AND RECOMMENDATIONS
Spot check concludeded that the newly launched PKH is implemented as a
conditional cash transfer program targeting very poor households. The goal of this
program is to improve health and education of poorest communities to be able to
exit out from poverty. The direct beneficiaries or recipients of PKH are women who
are the motor of the domestic life. PKH is a complex program having many
challenges in implementation. Most program functions, including data validation,
payment, data update, verification of compliance, service delivery, dissemination,
training and coordination have been in place, but they were suboptimum. All of
them contain problems that may hinder the achievement of PKH goals. Payment of
cash transfer is based on household composition, but conditional payments based
on participants’ compliance in utilizing basic health and education services gradually
started in early 2010.

xxv
To improve PKH implementation, Consultant team provides recommendations to the
relevant sectors as follow:
1. Bappeda at the city/district level should play more active roles in
implementing cross-sectoral coordination down to service level to
support PKH implementation. Bappenas and Bappeda should coordinate
to rearrange sectoral roles and responsibilities and disseminate the
decisions made to all related sectors including staff in education and
health service facilities. The decisions should unite all poverty reduction
programs under one roof.
2. BPS shall improve SPDKP implementation so poverty reduction program
database is complete and accurate. Special attention should be made to
improve accuracy of households’ names and addresses and avoid using
village staff as data collectors.
3. Relevant local offices, including Dinkes (District Health Offices), Disdik
(District Education Offices) and Kemenag (Ministry of Religion) shall
deliver all information about PKH activities to all personnel in their
offices.
4. Kemendiknas should conduct dissemination and coordination actively to
Disdik and fasdik so that the latter understand that PKH is an integral part
of basic education improvement programs. Dissemination needs to
emphasize that PKH participants are entitled to get scholarship for the
poor. In addition, there should be dissemination to the community about
national standards for education services and emphasize their right to
quality education. Furthermore, Kemendiknas should increase the
number of scholarships for teachers of elementary schools/MIs and
Junior High Schools/MTs to pursue bachelor degree , and coordinate
district offices to increase funding allocation to improve equipments and
infrastructures of education facilities to meet the national standards.

xxvi
5. Kemensos should increase effectiveness of dissemination to the
communities through facilitators and informed the urgency of reporting
changes in household composition, utilization of basic health and
education services, and submission of written complaints without fear.
They should also coordinate with the health sector so that all PKH
participants/beneficiaries are included covered by Jamkesmas and
scholarship for the poor. Kemensos, as the responsible ministry and
program implementer, should lead all dissemination activities and should
coordinate with Kemenkominfo jointly design and conduct dissemination
to relevant sectors and offices from central to district levels. The role of
Kemensos/District Social Offices as cross-sector mobilizer should be
improved.
6. Kemenkes should revise NSPK and develop standards for Puskesmas
including its networks and provide process indicators. Furthermore,
Kemenkes should disseminate to the community through Health Offices
and faskes about basic health service standards and the community right
to get quality health services. Furthermore, Kemenkes should increase
special fund allocation (DAK) to local governments to meet the standards
of basic health services. Kemenkes should improve coordination with
District Health Offices so that PKH all participants/beneficiaries receive
Jamkesmas card. Finally, Kemenkes should actively disseminate and
coordinate with District Health Offices and faskes that PKH is an integral
part of the basic health service programs.
7. PT Pos should improve payment processes by solving delays, long queues,
availability of cash, and staff hospitality. They should ensure timely
printing, distributing, and collecting verification forms as agreed
schedules.

xxvii
8. UPPKH as the responsible institution should do the following:
a. District/city UPPKH should improve training for staff of faskes and
fasdik on how to fill out verification forms and develop
incentive/reward system for those who complete the forms
accurately.
b. Through facilitators, District UPPKH should empower the
communities and guarantee them from fear to submit written
complaints, and prepares standard operating procedure (SOP) for
complaint handling and resolution. Furthermore, UPPKH should
also ensure responses and solution for each complaint submitted.
c. UPPKH should ensure that verification and update forms are
always available at fasdik and faskes.
d. Through facilitators, UPPKH shall improves dissemination to
participants/beneficiaries about the urgency to fulfill conditional
uses of basic health and education services, ensures timely
printing, distributing, and collecting verification forms. When
necessary UPPKH shall involve facilitators to review the tasks of PT
Pos.
e. District UPPKH should ensure payments as scheduled in the
guidelines; enforce sanction to those who deduct money from
beneficiaries, and develop better mechanism to link payment to
compliance requirements.
f. District UPPKH should ensure dissemination budget as an integral
part of PKH to cover the following activities: strengthening TKPKD,
improving central and local coordination, reinforcing
dissemination with target and clear strategies and at the same
time develop a special district dissemination team.

xxviii
g. Central UPPKH should strengthen the role of Korwil (locals) in the
dissemination and coordination of PKH from the provincial to the
facility levels, build routine cross-sectoral forums to monitor and
manage improvements of utilization of database, results of spot
check and other assessment to improve PKH implementation.
h. Central UPPKH should strengthen provincial and district team of
trainers, improve training programs with clear goals and strategies
(materials, method of delivery, and field practices).
i. Central UPPKH should submit written complaints from the public
and PKH participants to Kemendiknas and Disdik on issues related
to basic education services.
j. Central UPPKH should routinely file complaints from the public
and PKH participants to MOH and district Health Offices on issues
related to basic health services, request facilitators to disseminate
to the community about procedures for submitting complaints
about health services.
k. Central UPPKH should routinely distribute and disseminate
concise and communicative PKH manuals / guidelines to related
sectors.
l. Central UPPKH should develop a more practical training on PKH
procedures for operators, facilitators and service providers
involved in the program, supervise and facilitate PKH
implementation at district down to village levels, assure the
availability of forms at the facilitators, ensure that the data at the
district / city and district-central online network are up to date.
m. Personnel at Central UPPKH MIS should be more responsive to
updates made by the district operators in the PKH database to
ensure all validation, updates, verification, and complaints data
are recorded.

1
Chapter 1 Introduction
1.1. BACKGROUND
Indonesia is committed to achieve the MDGs and one of them is to reduce poverty
by implementing a number poverty alleviation programs, including the distribution
of subsidized rice for the poor (RASKIN), free health care for the poor (Jamkesmas),
direct cash transfer (BLT) and the Conditional Cash Transfer or Program Keluarga
Harapan. The BLT was started in 2005 as a government’s initiative to help poor
households to overcome the impact of decreasing fuel subsidy that was anticipated
to increase cost of living. Despite a lot of criticisms, the BLT program was re-
launched in 2007 to reduce the inflationary impact that caused by the reduction of
fuel subsidies in mid year 2007. The BLT program is an unconditional cash transfer
program, which was criticized as spoiling the poor; then it was modified as
Conditional Cash Transfer (CCT) program or Program Keluarga Harapan (PKH) in
Indonesian language.
The PKH was launched in July 2007 in seven provinces targeting very poor
households (RTSM) with a pregnant woman and / or children aged between 0-15
years and / or 16-18 years who have not completed primary education. RTSMs
received cash transfer every three months, paid directly through the Post Office. The
cash beneficiaries are women who are considered responsible for health and
education of the children in the family. The minimum amount of transfer is Rp
200,000 per RTSM per year, which can be increased up to Rp 2.2 million per year
depending on the composition of household members and compliance with
conditionality of utilizing basic education and health services. Pregnant women and
children under 6 years old should regularly check their health in accordance with
government program. For education, children between 7 and 15 years old must be
enrolled in school and must attend at least 85% of class activities. Exception is given
for children age between 15 and 18 years old who have not completed Junior High
PUSAT PENELITIAN KESEHATAN
UNIVERSITAS INDONESIA
2010
PUSAT PENELITIAN KESEHATAN
UNIVERSITAS INDONESIA
2010
2
School and have no access to regular education facilities, they should follow an
education program either through non-formal education or other equivalent
programs.
Program Keluarga Harapan aims to improve RTSM welfare as well as to strengthen
their capacity to exit from poverty. In the long run the program is expected to help
cut off the poverty cycle between generations by improving health and
education. Similar programs have been successfully implemented in Latin American
countries in the last decade by improving education, health and nutrition of the
RTSM.
Until Mid 2010, PKH was implemented in 13 provinces. Out of these thirteenth
provinces, seven provinces (West Sumatra, DKI Jakarta, West Java, East Java, North
Sulawesi, Gorontalo, and East Nusa Tenggara) implemented PKH since 2007, while
the other six provinces (Nanggroe Aceh Darussalam, North Sumatra, Banten,
Yogyakarta, South Kalimantan and West Nusa Tenggara) started PKH in 2008. The
Government is committed to expand this program to all provinces in Indonesia.
Implementation of the Program Keluarga Harapan involves a variety of sectors from
the central, provincial, district, sub district down to service provider levels. The
program is under the coordination of the Ministry of Social Affairs (previously the
Department for Social Affairs), while other ministries such as the Ministry of Health,
Ministry of Education and Ministry of Religion are responsible to provide education
and basic health services. Other than the ministries, other government institution
such as the Central Board of Statistics (BPS) also plays an important role to support
the successful implementation of PKH by providing data on PKH prospective
beneficiaries. In addition, the Post Office is responsible to distribute PKH fund to
beneficiaries, while the Ministry of Communications and Information communicate
and disseminate PKH at all levels. To facilitate implementation, a Regional
Coordinator (Korwil) is appointed in each province. An online computerized system is
established to support management information system, maintain updated
beneficiaries’ data and changes, payments, compliance to conditionality, and
complaints acceptance and solution.

3
At the provincial level, PKH is under the coordination of the Provincial Coordinating
Team led by the Governor and supported by the main actors from the Provincial
Social Office (Dinsos), involving the Health Office, Education Office, Regional Office
of the Ministry of Religion, BPS, PT Pos, and Bappeda. At the district level, the
program is under the coordination of the District Coordinator under the leadership
of the Regent and supported by the main actors from the Dinsos and other relevant
institutions such as Dinkes (the Health Office), Dinsos, District Office of the Ministry
of Religion, PT Pos, and Bappeda. At the sub district level, the program is under the
coordination of the facilitator team involving the Post Office, Puskesmas, local
elementary and junior high schools, chairperson of women’s group and facilitator.
Program Keluarga Harapan (PKH) is relatively new and the implementation is
complex, started with setting the target, validating and updating participant’s data,
verification of beneficiaries’ compliance, fund disbursement and payment, service
provision, until grievance procedures. Another aspect adding to the complexity is the
coordination between relevant sectors, within and between the sectors at the
central and local levels, and maintaining nupdated data of the Management
Information System.
Involvement of a number of sectors from the central up to the sub district levels and
service providers has the potential to cause operational problems. Although a
Standard Operating Procedure (SOP) was carefully developed, there is no guarantee
that relevant actors and institutions will comply to the specified rules and
procedures. Many problems were observed during PKH implementation, but there
has not been any official statement on their magnitude and extent the problems
affect to overall PKH. Spot check by an external party is needed to objectively assess
the size and patterns of problems in PKH implementation to explain why the
problem occurred, and to provide recommendations to solve or reduce problems
immediately. Spot check is also expected to provide feedback for the improvement
of the SOP/Guidelines.

4
1.2 OBJECTIVES
The main objective of the spot check is to assess various processes of the PKH
implementation. In particular, the review process includes: (a) data update; (2)
payment; (3) compliance with conditionality (4) provision of education and health
services; (5) acceptance and solution of complaints, and (6) dissemination, training
and coordination across actors. In addition, the spot check also explored
understanding by actors about program rules and procedures, among other PKH
beneficiaries, head of beneficiary groups, facilitators, providers, district UPPKH
operators, and key personnel in relevant sectors at the center and local levels.

5
CHAPTER 2 METHODOLOGY
The spot checks used quantitative and qualitative assessment with a focus on the
process, not the outcome or impacts of PKH, considering that PKH is newly
implemented. In addition to the process, the spot check also assessed relevant
actor’s knowledge about PKH rules and procedures. Specific spot check activities
were assessment of important processes in PKH including:
1. Data update, from report of households changes, data updates by the district
/ city operators, until approval of changes by the central UPPKH
2. Payment, including accuracy with household data, and compliance with
conditionality, schedule and frequency, and deduction
3. Verification of beneficiaries’ compliance to conditionality, including complete
record and confirmation of school attendance, health service utilization by
pregnant, or postpartum women and under-five children
4. Provision of education and health services, including adequacy of the number
of schools and the distribution of schools, puskesmas and its network,
availability of staff / teachers, classrooms, equipment or supporting
materials, availability of drugs and other medical supplies, and quality of
services
Acceptance and solution of complaints, starting from submission of written
complaints from beneficiaries and public, completion of complaint form by a person
with assistance from facilitator, acceptance of complaints by the district UPPKH,
submission to the central UPPKH and solution, dissemination, and training.
Complaints could cover implementation and effectiveness of targeting relevant
sectors at the central and local levels, service providers and the community,
understanding of relevant actors’ on program rules and procedures. Complaints

6
could be submitted by beneficiaries, head of the group, facilitators, service
providers, key personnel and other relevant sectors.
2.1 FRAMEWORK/ DETAIL OF PKH SPOT CHECK ACTIVITIES
The following table 1 helps explaining the framework of this spot check . The first
column shows the level of PKH implementation to be assessed which is mostly about
the process. The second column shows the process, activities or outputs to be
assessed. The third and fourth columns contain indicators and methods to measure
each evaluated process. The process was then analyzed by looking how far the
processes deviated from regulations, PKH Guidelines, and the reasons for deviations.
Table 2. 1. The Framework of The PKH Spot Check
Level Activity measured Indicator Method for Measurement
Process Data update matching of participant‘s household data from the spot check and the central database
Comparing participant’s household data from the spot check survey with the central database
Check the updating process from changes in the household data as reported by beneficiaries, entry into the district UPPKH, and end with central database
Process Payment Differences between the amount of cash transfer received and disbursed
Check data of beneficiaries’ household (number of pregnant women, children 0-15 years or 16-18 years who have not completed elementary education) then estimate the amount of cash transfer
Comparison of calculatedamount based on household spot check data with the amount paid by the post office (receipt)
Validation of cash transfer

7
Level Activity measured Indicator Method for Measurement
received by beneficiaries
Compliance to conditionality
Record and report of school attendance and the utilization of health services
Cross check PKH children’s school attendance through completeness and accuracy of record in the verification form
Cross check utilization of health services offered in the puskesmas by pregnant/delivering/postpartum women and children through completeness and accuracy of record in the verification form
Service provision Quantity and distribution of facilities and quality of service
Check the quantity and quality of education services in Elementary Schools/ MIs and Junior High Schools/ MTs, including number of teacher, qualification, number of student groups per grade, and sufficiency of school facilities and infrastructure
Check quantity and quality of health services, including number and qualification of health providers, education materials, availability of drugs and vaccines, and compliance to health service protocol
Acceptance and solution of complaints
Number of complaints received and were resolved
Number of beneficiaries who filed complaints and their types
Number of complaints received by the district UPPKH based on types and sources of complaints
Number of complaints traced to the source and resolved
Dissemination and trainings
Number and effectiveness of dissemination and
Verification of quantity, quality and effectiveness of dissemination through

8
Level Activity measured Indicator Method for Measurement
trainings documents in Kemenkominfo and Kemensos, relevant sectors, district UPPKH, facilitators, service providers, and the community Verification of quantity of training, types, number of beneficiaries, time and location through operators and facilitators
Output Relevant actors’ knowledge
Relevant actors’ understanding of program rules and procedures
Evaluation of understanding of relevant actors, including beneficiaries, group leaders, facilitators, operators, service providers, post office, key personnel from other sectors and relevant parties from central to local levels about program rules and procedures
2.2. DATA SOURCES
Survey was undertaken to collect relevant quantitative data from beneficiaries,
facilitators, operators, and service facilities. In-depth interviews were conducted to
central and local key personnel from relevant sectors and focus group discussions
were held with team leaders and advisors to collect relevant qualitative
data. Beneficiaries’ data for sampling, data update and payment were retrieved from
the central database. Other related data were taken from secondary sources.

9
Figure 2. 1. Source of Data and Assessment Verification of PKH Processes
Payment Process
PKH Beneficiaries Anak 0-18
Compliance to
conditionality
Service Deliveries
Database update
Complaint acceptance/solution
Dissemination &
Training
Sosialisasi &
Pelatihan Knowledge
Post Office
Elementary School
Puskesmas and network
Database
Peserta PKH
Complaint Database
Relevant stakeholders
National PKH Team Kemensos Bappenas BPS Kemenkominfo Kemendiknas Kemenkes
District UPPKH Post Office
Sub district UPPKH Facilitators Service Facility Head of the Group PKH beneficiaries
PKH Participant Form Process
Complaints Form Process
Facilitators/Head of the Group
Pendamping /
Ketua kelompok/
Penerima PKH

10
Survey to Relevant Stakeholders
Survey was conducted to national and community level stakeholders to collect
information about various processes in PKH and to assess their knowledge about
PKH rules and operationalization. Table 2 describes the survey, informants and data
collected in each survey.
Table 2. 2. Relevant Institutions / stakeholders, Informants, and Data
Relevant organizations
and stakeholders
Informants Number/ Unit
Data Collected
Central UPPKH
Relevant Kemensos staff
One or two people
Knowledge about program rules and procedures
Perception about the role and responsibility in policy development, quality assurance (coordination and training) and assessment (monitoring and evaluation, information system)
Relevant Bappenas staff
One or two people
Knowledge about program rules and procedures
Perception about the role and responsibility in program planning and budgeting
Relevant BPS staff
One or two people
Knowledge about program rules and procedures
Perception about role and responsibility in developing RTSM criteria, certification and accuracy of potential PKH beneficiaries’ data
Relevant Kemenkominfo staff
One or two people
Knowledge about program rules and procedures
Perception about the role and responsibility in program dissemination
Relevant Kemendiknas staff
One or two people
Knowledge about program rules and procedures
Perception about the role and responsibility in providing quality educational services
Relevant Kemenkes staff
One or two people
Knowledge about program rules and procedures
Perception about the role and

11
Relevant organizations
and stakeholders
Informants Number/ Unit
Data Collected
responsibility in providing quality health services
District UPPKH
Head of UPPKH, UPPKH Coordinator, staff from Complaint and Management Information System sections
9 districts/ cities
Knowledge about program rules and procedures
Dissemination and trainings
Quality assurance (including coordination) and assessment
Challenges and barrier in program implementation process: data validation and update, payment, compliance to conditionality, service delivery, complaint management process, dissemination and trainings
District/city Post Office
Director and related technical staff
9 district/ city post office
Knowledge about program rules and procedures
Dissemination and trainings
Cash transfer process (and information system)
Obstacles and barriers in the payment process
Sub District UPPKH
Coordinator and assistants (facilitators)
36 sub districts
Knowledge about program rules and procedures
Quality assurance (including coordination) and assessment
Dissemination and trainings
Obstacles and barriers in data update, payment, compliance to conditionality, service delivery, complaint management, dissemination and trainings
Sub District Post Office
Director and related technical staffs
36 sub district post offices
Knowledge about program rules and procedures
Dissemination and trainings
Cash transfer process (and information system)
Obstacles and barriers in the payment process
Sub district facilitator
Sub district facilitators
108 facilitators
Knowledge about program rules and procedures

12
Relevant organizations
and stakeholders
Informants Number/ Unit
Data Collected
Dissemination and trainings
Obstacles and barriers in program facilitation and implementation process
Elementary School/Junior High School
Headmaster and relevant staff
72 Elementary Schools and 36 Junior High Schools
Knowledge about program rules and procedures
Dissemination and trainings
Quality assurance
Type of services offered
Obstacles and barriers in service delivery
Puskesmas Head of Puskesmas, midwife coordinator, and immunization officer
36 puskesmas
Knowledge about program rules and procedures
Dissemination and trainings
Quality assurance
Type of services offered
Obstacles and barriers in service delivery
Head of the Group
Head of the Group
180 head of the groups
Knowledge about program rules and procedures
Dissemination and trainings
Obstacles and barriers in assisting PKH beneficiaries
PKH beneficiaries
PKH women beneficiaries
1,800 women who received PKH cash transfer
Knowledge about program rules and procedures
Data validation and update report
Cash transfer approval process
Service utilization and satisfaction
Complaints acceptance and solution
Relevant information acceptance report

13
2.3 INFORMANTS
At the national level, informants are policy makers and program managers in
relevant sectors: Kemensos, Bappenas, BPS, Kemenkominfo, Kemendiknas, and
Kemenkes. At the district level, informants include UPPKH key personnel (Head,
Coordinator, complaint and information system sections) and the Post Office (Head
and technical staff). At the sub district and community levels they include UPPKH
personnel (coordinator and assistant), the Post Office (Head and relevant staff),
Puskesmas (Head, midwife coordinator, immunization staff), elementary and Junior
High schools (head and relevant staff), facilitators, head of groups and PKH
beneficiaries.
2.4 LOCATION AND SAMPLES
The locations for the study were selected by choosing the province first, then
districts/cities were determined in the selected province, and finally the sub districts
were selected in each of these districts/cities. Out of 13 PKH provinces, five were
selected to represent the island of Java and outside Java. PKH in the island of Java
began in 2007 and outside Java in 2008. This situation made it difficult to explain the
differences in the performance of PKHs that started in 2007 and 2008. In this case,
the differences were the starting year or Java and outside Java. The selection of the
sub district took into account the access from the district capital. The five selected
provinces were: DKI Jakarta, West Java and East Java to represent PKH 2007, and
South Kalimantan and West Nusa Tenggara to represent outside Java for PKH 2008.
The framework for provincial, district, sub district and participant sampling refers to
beneficiaries’ data in the Central UPPKH database. Two districts were taken in each
selected province (except DKI Jakarta). In DKI Jakarta, spot check was only performed
in North Jakarta where PKH was implemented. Four sub districts were taken in each
selected district. Selection of districts and sub districts was based on the number of
PKH beneficiaries. A district or a subdistrict with large number of beneficiaries had a
greater opportunity to be selected as a sample. Then, 50 PKH beneficiaries were

14
sampled from each selected sub district. Sampling in selecting a beneficiary was
conducted by randomly selecting five villages from each selected sub district, and for
each selected village one participant was randomly selected with nine other
beneficiaries living close to her or in the vicinity. In addition, three facilitators, one
Puskesmas, two Elementary Schools and one Junior High School, and five group
woman leaders were selected in each selected sub district. Overall, spot check
covered five provinces, nine districts, 36 sub districts, 108 facilitators, 36 Puskesmas,
72 Elementary Schools, 36 Junior High Schools, 180 group leaders, and 1,800 PKH
woman beneficiaries (See Table 2).
2.5 PROCESS TO MAINTAIN QUALITY OF SPOT CHECK
All team members and involved personnel were equipped with clear and practical
guidelines for spot check. . It includes job description of team members and
personnel category, PKH implementation mechanisms and quality control of field
activities and data management, including research ethics, licensing, data collection
tools and protocols, trainings, and supervision.
2.6 ETHICAL REVIEW
Ethical review was conducted by the Ethical Review Committee of the Faculty of
Public Health, University of Indonesia prior to field activities. The committee
reviewed proposal, data collection plan, questionnaire and inform consent. Ethical
review is a compulsory process for all research under the Faculty of Public Health,
University of Indonesia to hinder violations of Human Rights during research
activities and nothing that may be harmful or detrimental to those involved.

15
2.7 PERMIT
Permit for the spot check is obtained from the Ministry of Home Affairs and local
authorities.
2.8 QUESTIONNAIRE AND DATA COLLECTION PROTOCOLS
Survey questionnaires were developed, piloted, revised and used to collect data
from relevant informants or respondents. For each informant category the Spot
Check used a different tool to assess the PKH implementation process indicators.
Spot check tool was piloted in Bogor, West Java.
2.9 PERSONNEL COMPETENCY
The research team incorporates CHR UI (PPKUI) staffs with various experiences in
large-scale surveys and understands the content. The team was led by experienced
PI and Co-PI with support from the research team members in line with their
respective expertise.
Data collection was coordinated by a survey manager who was responsible for the
overall collection and assurance that all activities at each location were well
coordinated. Close collaboration with relevant expert groups were also established.
In each province, a Provincial Field Coordinator was appointed from PPKUI who was
in charge for coordinating field activities. The PFC collaborated with local partners in
each province. Data management was led by a data manager in PPKUI with
assistance from local data operators (Local partners)
2.10 LOCAL PARTNERS AND CAPACITY IMPROVEMENT
Provincial local partners or PLC came from local university where spot check was
implemented include the Faculty of Economics of Padjadjaran University in Bandung
(West Java), the Faculty of Public Health of Airlangga University (East Java), Lambung
Mangkurat University (South Kalimantan), Mataram University (West Nusa

16
Tenggara), and the Faculty of Public Health of Universitas Indonesia (for DKI Jakarta).
The collaboration built local capacity to enable local institutions to implement similar
activities or to participate in the monitoring of similar programs in the future.
A Provincial Field Coordinator coordinated activities in each province, delivered
Training Of Trainers, ensured that tools were understood, developed field work plan
with PLC and district/city partners, discussed all constraints/ problems/challenges
and together with PLC looked for solutions.
2.11 TRAININGS
As part of the efforts to maintain high quality of spot check, the PI and Co-PI led
workshops/trainings to prepare for field activities involving all team members from
PPKUI (researchers, survey manager, data manager) and PFC. The goal of the
workshop was to ensure that reseach team members understood data collection
tools and processes. At provincial level, TOT was attended by PLC, DFC and
interviewers, led by a PFC. The training provided intensive explanations of each
question in the questionnaires, interview techniques, and how to complete the
questionnaires.
2.12 DATA COLLECTION
The Survey Manager led the entire data collection processes, was responsible for
ensuring that the process ran smoothly with good quality. In each district, the team
(DFC and the interviewer) stayed at the base camp to facilitate coordination and
interaction. Field coordinators ensured that no data were missing or inappropriate
answer was filled in. During routine data collection DFC checked the completed
questionnaires to look for completeness and clarity of answers. All activities are
recorded in a logbook and reported to the relevant PFC. Questionnaires that had
been completed were checked and edited. At least 10% of completed questionnaires
were randomly selected. The local teams visited selected data collection process to
ensure good data collection. If there was a problem, the interview process must be
17
repeated or closely supervised. Follow up visit was undertaken to re-interview
respondents for some unclear answer. Overall no serious problems were found so
DFC did not have to replace any of them.
2.13 SUPERVISION
During data collection, supervision was conducted to selected provinces and
districts. The team met and discussed the process with PLC, DFC and interviewer,
and took necessary steps to ensure high quality of data collected..
2.14 DATA ENTRY
At the end of the data collection period, the DFC and DLC compiled the
questionnaires and submitted them to PLC who was responsible for submitting the
questionnaires to PPKUI. Data correction and questionnaire compilation were done
by the data manager and staff of PPKUI. Questionnaires are stored in a safe place
with limited access only to data manager, principal and co-principal investigator.
EpiData was used for data entry and management.
2.15 DATA QUALITY MONITORING
The following efforts were taken to ensure high quality of data collected:
1. Data in the questionnaires were checked through a follow up visit
(10% of respondents) by PLC and DFC at the district level. PPKUI
developed a manual for questionnaire data checking
2. Peer-examination between interviewers covering completeness,
consistency, accuracy of all completed questionnaires
3. Checking and editing process by DFC and PFC to ensure completeness,
consistency, accuracy of all completed questionnaires

18
4. Regular meeting between DFC and interviewers and coordination
meeting with PFC discussed a number of important issues, such as
problems during interviews or sampling, and problems in completing
the questionnaires, etc.
5. data Entries were conducted by trained personnel and closely
supervised by the data manager
6. Data correction and accuracy were checked by examining frequency
distribution and consistency between all variables before analyses
were undertaken.
2.16 ANALYSIS
Analyses to estimate key parameters for each district and province were repeatedly
discussed by core team. The results (based on ninety-five percent confidence
interval) were then reported to select important key variables.

19
CHAPTER 3 CHARACTERISTICS OF PKH BENEFICIARIES
3.1 PREGNANCY, CHILDBIRTH AND CHILD(REN) UNDER 15 YEARS
OLD
Approximately 14% of RTSM beneficiaries had pregnancy or childbirth in the last 24
months. The percentage of women who had delivery was relatively the same across
four provinces ranging from 9% to 14% except in West Nusa Tenggara (23%).
Percentage of pregnant women during the survey was about one to two percent in
each province, except in NTB that was much higher (approximately 6%). Most
beneficiaries (95%) had child(ren) under 15 years old, with the highest proportion in
Jakarta (99%) and the lowest proportion in South Kalimantan (92%). Approximately
96% of beneficiary respondents had child(ren) under 15 years old and/or childbirth
in the last 24 months. Approximately 10% of respondents were group leaders.
Table 3.1. Percentage of households with childbirth in the last 24 months, child(ren) under 15 years old and pregnancy during survey.
DKI
Jakarta West Java East Java
West Nusa
Tenggara
South Kalimant
an Total
N
200
400
401
400
392
1,793
Households with childbirth in the last 24 months (1)
14.5
11.0
9.0
23.3
12.0
13.9
Households with child(ren) <= 15 years old (2)
99.0
96.8
96.8
94.3
92.3
95.5
Households without (1) and (2)
1.1
1.5
2.6
2.6
1.6
2.0
Households with childbirth in the last 24 months or child(ren) <15 years old
99.5
97.3
97.5
95.8
93.1
96.3
Households with a pregnant woman during survey 1.0 1.8 1.7 6.3 1.3 2.6
Households with women as group leader
11.2
9.3
8.2
11.4
9.2
9.7

20
3.2 DEMOGRAPHIC PROFILE OF HOUSEHOLD MEMBERS
Overall the survey collected data from 1,793 beneficiaries’ consisting of 8,322
people, with 49% of them were women. Approximately 45% were married or had
been married. The main activities of most household members were working (37%)
and students (31%). East Java and South Kalimantan had a larger proportion of
working household members than the three other provinces, while the largest
proportion of students was found in West Nusa Tenggara. This finding matches the
indication that West Nusa Tenggara had younger population compared to other
provinces. Province with the largest proportion of elderly (3%) was East Java. Out of
the total population covered by the survey, the largest proportion of senior high
school graduates was found in DKI Jakarta (10%), followed by West Nusa Tenggara
(6%), whereas other provinces had only 2% to 3% of senior high school graduates.

21
Table 3.2. Demographic characteristics of PKH household members
Province Total
DKI
Jakarta West Java
East Java
West Nusa Tenggara
South Kalimantan
N 1,071 1,919 1,687 1,937 1,708 8,322
Sex
Man 50.8 51.6 49.7 50.2 50.5 50.6
Woman 49.2 48.4 50.3 49.8 49.5 49.4
Marital Status
Unmarried 59.9 55.5 44.2 59.9 52.6 54.2
Married 35.4 39.6 49.7 36.9 43.0 41.2
Divorce 1.3 1.5 1.4 1.2 2.1 1.5
Widow 3.4 3.5 4.7 2.1 2.3 3.1
Main activities
Working 33.1 34.1 44.2 31.0 40.9 36.7
Student 34.0 30.1 27.5 35.7 30.8 31.5
RT personnel 8.9 11.9 9.1 9.3 8.4 9.6
Retired 0.1 0.1 0.1 0.0
Unemployed 12.7 10.9 6.5 4.9 6.2 7.9
Infants/preschool children 10.0 10.4 9.2 18.1 12.3 12.3
Mentally retarded/paralyzed/severely ill 0.1 0.5 0.4 0.2 0.1 0.3
Elderly 1.0 1.6 2.8 0.4 0.9 1.4
Others 0.2 0.4 0.4 0.4 0.4 0.4
Last education
Not finish elementary school 34.4 30.3 28.6 32.8 39.8 33.0
Elementary school/MI 26.2 37.1 37.6 22.1 34.7 31.8
Junior High School/MT/equal 15.9 9.1 10.9 11.0 9.2 10.8
Senior High School/MA/equal 10.4 2.2 3.4 5.9 2.9 4.5
Diploma 1, 2 or 3 years 0.1 0.1 0.1 0.1 0.1
Diploma 4 years/(S1) Bachelor 0.3 0.2 0.1 0.0
Not in school/not yet attend school 12.7 20.9 18.9 27.7 12.9 19.4
Unknown 0.1 0.4 0.4 0.3 0.3 0.3
3.3 MAIN JOB OF HEAD OF HOUSEHOLDS
The Spot check found that main job of head of household, except in DKI Jakarta,
were in agriculture, plantation, farming, fishery and forestry. In DKI Jakarta, the main
jobs were trading, transportation and services. The second province with highest
proportion of head of household working in service sector was West Java (18%). DKI
Jakarta had the highest proportion of head of household without jobs (12%),

22
whereas in the other four provinces the proportion of jobless head of household
varied from 3% to 5%.
Table 3.3. Distribution of head of households’ job
DKI
Jakarta West Java
East Java
West Nusa Tenggara
South Kalimantan
Total
Number of households 200 400 401 400 391 1,792
Plantation, farming, fishery, forestry
1.5 52.0 68.1 82.0 82.1 63.2
Mining 0.5 0.5 0.5 0.3 0.8 0.5
Processing Industry 1.5 1.8 1.2 0.5 0.3 1.0
Electricity, Gas, Water 1.0 0.5 0.2 0.8 0.4
Building construction 4.0 5.0 6.5 3.0 0.8 3.9
Trading, accommodation 12.0 8.0 4.5 2.0 1.0 4.8
Transportation 14.0 6.0 4.2 2.5 1.0 4.6
Financial Institution 0.3 0.2 0.3 0.2
Service 49.5 17.5 4.2 5.3 4.6 12.6
Others 4.5 3.0 5.2 0.8 5.9 3.8
Unemployed 11.5 5.5 5.0 3.0 3.3 5.0
100.0 100.0 100.0 100.0 100.0 100.0
3.4 POVERTY INDICATORS
In general, poverty indicators illustrated by the household socio-economic
characteristics is almost similar. More than half of those households stay in a house
of less than eight square meter, and the largest wall was mostly without cement-
covered (plaster) or covered with low quality of wood/bamboo/hatch, while more
than half of households had soil floor or covered with low quality wood/bamboo.
Most beneficiaries did not have saving or easy-to-sell goods. Half of them admitted
that they could not afford to pay medical treatment in Puskesmas. More than half
the beneficiaries could only buy one set of cloth per year, and approximately 45% of
them could eat only twice or less per day, and nearly three-quarters of respondents
were only able to consume foods cotaining protein once a week.

23
Table 3.4. Characteristics of socio economic of PKH beneficiaries’
DKI Jakarta West Java East Java
West Nusa Tenggara
South Kalimantan Total
% house size<8m2 86.7 43.8 28.3 82.9 64.0 58.2
% Head of household worked as farmer/unemployed 17.5 60.5 78.3 85.8 91.3 72.1
% with largest wall without plaster/wood 63.0 69.8 81.5 89.8 98.2 82.3
% with largest soil/wood floor 10.0 34.3 64.6 71.3 82.9 57.2
% with unprotected/rain water source 22.0 51.3 51.1 51.0 59.2 49.6
% with public/had no toilet 49.0 15.0 10.2 14.0 55.4 26.3
% with No electricity supply 1.3 1.5 33.0 28.1 14.1
% with no special space for kitchen 50.0 19.8 15.7 20.3 42.3 27.3
% with fuel oil/wood 18.5 52.5 89.0 100.0 99.2 77.7
% with no saving/easy- to-sell goods >500,000 Rupiahs 78.5 82.0 64.8 88.8 87.2 80.4
% unable to pay Puskesmas 6.0 47.5 36.4 76.8 68.4 51.5
% could buy 1 set of clothes per year 26.0 46.3 51.6 66.8 73.7 55.8
% could eat meals per day twice or less 41.5 62.3 26.4 42.5 52.8 45.5
% with once or less protein consumption per week 58.0 86.0 76.1 61.0 71.9 72.0
3.5 PARTICIPATION IN POVERTY ALLEVIATION PROGRAM
As PKH targets the very poor households, beneficiaries are assumed to receive aid
from other poverty alleviation programs; unfortunately the assumption was not met.
Approximately 60% of participants admitted they received BLT in the previous year,
the highest rate was in Jakarta and the lowest was in South Kalimantan. On average
three-quarters of the beneficiaries admitted that they received raskin (subsidized
rice for the poor), with the lowest proportion (30%) was found in South Kalimantan
Only 69% of beneficiaries were Jamkesmas participants as it was expected to be
100%. In DKI Jakarta only one fifth of beneficiaries were registered as Jamkesmas

24
members. However, in DKI Jakarta and West Java, if DKI residents do not have
Jamkesmas card, they could use their local identity card (KTP) to be covered by the
local health insurance program (JPK Gakin). Funding source of JPK Gakin is the local
government budget (APBD). Only 18% of beneficiaries received scholarship for the
poor; the largest proportion was in West Nusa Tenggara (45%) followed by East Java
(17%), and in three other provinces the proportion of respondents who received
school fellowship varied from 5% to 10%.
Table 3.5. Distribution of participants who received aid from other poverty alleviation programs
DK Jakarta West Java
East Java
West Nusa Tenggara
South Kalimantan Total
Number of sample (n) 200 400 401 400 392 1.793
Unconditional cash transfer 2005 76,5 66,3 68,6 73,3 23,0 60,0
Unconditional cash transfer 2008 75,5 54,8 74,3 65,8 56,1 64,2
Scholarship for the poor 4,5 10,8 17,0 45,0 6,1 18,1
Rice for the poor 78,5 89,8 92,3 93,0 30,4 76,8
Jamkesmas 20,0 62,3 83,0 84,3 71,7 69,2

25
3.6 SMOKING BEHAVIOR
Other than harmful for health, smoking behaviors disturb the fulfillment of basic
household needs. Due to habit and addictive reasons, smokers prioritized smoking
than fulfilling basic needs for their household members. As high as 73% of the
households surveyed had at least one family member who smoke. The proportion of
households that had smokers was higher in provinces in Java than outside Java. The
average number of smokers per household was one person with a range of one to
three people per household. The average number of cigarettes smoked per day was
12 sticks, with a range of 1 to 72 sticks. The average expenses for cigarette per
month per household was Rp 127,000.
Table 3.6. Smoking rate and expenses
DKI West Java East Java West Nusa
Tenggara South
Kalimantan Total
% household with smokers 77.0 79.3 79.8 70.8 60.2 73.1
Number of smokers in the household
Average 1 1 1 1 1 1
Lowest 1 1 1 1 1 1
Highest 3 3 3 3 3 3
Number of cigarettes (sticks) consumed per day
Average 10 12 11 9 16 12
Lowest 1 1 1 2 2 1
Highest 72 60 48 56 48 72
Smoking expense per month
Average
204,306 152,439 70,909 98,542 157,198 127,960
Lowest
7,000 3,400 1,600 4,000 4,000 1,600
Highest
960,000 900,000 450,000 725,000 900,000 960,000

26
CHAPTER 4 DATA VALIDATION AND UPDATE
Data validation should perform to all potential PKH beneficiaries initial meeting to
determine their eligibility and amount of cash transfer. Validation is done by
checking whether there is any pregnant woman, and/or under-16 children or
between 16-18 years old who have not completed junior high school and their
number. In addition to validation, the initial meeting with beneficiaries provides
information about rules and procedures.
Candidates who met the eligibility criteria were subsequently accepted as
beneficiaries, and the validated data will become the baseline for the central
database. Overtime, the central database should be updated to reflect
demographical changes in the households. Any change to household data should be
reported including address, pregnancy, miscarriage, birth, child moving out of the
family to go to another school, child moving out of the family to study to higher
level, changes in health service uses by beneficiaries and/or death. Data update
starts from household demographic changes reported by beneficiary, changes
reported by facilitators to district UPPKH, changes inputted by district operators, and
updating of the central database by the central UPPKP Management Information
System.

27
4.1 VALIDATION
4.1.1 Validation during the first meeting
Most beneficiaries attended the initial meeting. On average only 5% of beneficiaries
admitted that they did not attend the initial meeting because they were neither
available nor receive invitation. Percentage of participants who did not attend the
initial meeting varied from 7 to 10% in DKI Jakarta and West Java, respectively, but
less than 1% in West Nusa Tenggara. Not all beneficiaries who attended the initial
meeting were interviewed by PKH officer for validation regarding the number and
composition of their households. Out of all these beneficiaries, one third in East Java
and 5% to 15% in other four provinces admitted that they were not asked about
their household data. Furthermore, PKH guidelines require home visits to validate
household data of these beneficiaries. Yet only one fifth of these beneficiaries were
visited. Overall, only 83% of beneficiaries could be validated.
Table 4.1. Validation of beneficiary’s household data
DKI Jakarta
West Java
East Java
West Nusa Tenggara
South Kalimantan
Total
Number of respondents 200 400 401 400 392 1,793
% of attendance in the first meeting 89.5 93.0 94.8 99.3 95.9 94.8
% of attendance and validated 78.0 80.0 66.0 94.4 88.3 81.6
% of absence and validated 2.0 1.3 1.0 0.2 0.8 0.9
Total % validated 80.0 81.3 67.0 94.6 89.1 82.5
28
4.1.2 Constraints in conducting initial meeting
Sending invitation to beneficiary candidates to attend the initial meeting was not
always easy because in some cases the names and addresses were unclear and the
houses ware located in remote areas with difficult geographical conditions. The
situation is revealed in the informant’s statement below:
"... We found many unclear names & addresses. Residential location is spread out
and the geographical condition was difficult and often times they become
constraints ... "(UPPKH HSS operator in South Kalimantan)
"... And then there were also similar names, there were many people with the same
name in one village, and when distributing invitation card many were given wrong
name or a wrong address or a wrong person, so what happened was that the card
was automatically received by a wrong person as well ... "Operator, West Java)
".... The lurah was traumatized by the BLT so there was a concern that the
community would rush to his place, specific for Tj. Priok and I was not allowed to
borrow the hall, so I went door to door to 365 RTSMs, door to door, because it was
my duty and responsibility. For Sunter Jaya, 30% was door to door, 70% were in the
hall ... "(Operator, North Jakarta)
Facilitator’s thoroughness and diligence is required for validation to ensure accuracy
of database in the central UPPKH. During validation in the initial meeting, there was
a case where a facilitator had the initiative to cross out name of a candidate who
was considered as not meeting the criteria.
"... ... When I found someone who was not eligible, what I mean is that the data did
not qualify the person, what I found was only one person who received double, so I
had the initiative to cross out one of them, that was why from 311 RTSMs, it became
310. And what I did was that I crossed one of them, because how one person could
receive two benefits.... "(Facilitator, Subang District)
Many cases where PKH was given to the wrong people were still found. Facilitators
and community members in some villages reported ineligibility cases made
deliberately or inappropriate criteria of poverty on the field. Results of facilitators’
group discussion in one province revealed that some PKH beneficiaries were village
staff or their relatives who obviously did not qualify as RTSM. This situation

29
happened because the BPS survey in 2005 employed many village staff as data
collector.
"Some PKH beneficiaries did not qualify (too rich to be RTSM), in my village almost 60-70% of village staff was included as PKH candidates. Their names were on the list. This could provoke anger among the community members, because even without including the name of village staff, the community made a fuss, moreover if they found out that many village staff received PKH, so I reported this to the office of Social Affairs, they will decide that those names should be removed. But until now PKH beneficiaries were people who were close to the village staff ". (FGD Facilitator, Dompu, West Nusa Tenggara)
Another issue, many community members complained and reported to district
UPPKH or facilitator why they were not included as PKH beneficiaries while they
perceived themselves to be poorer than those who were listed as PKH beneficiaries.
The program delineates that PKH beneficiaries are the very poor households so that
they are eligible other poverty alleviation program, but spot check showed
otherwise. Spot check showed only 69% of PKH beneficiaries were also covered by
Jamkesmas and only 18% received scholarships for the poor.
4.2 DATA UPDATES
4.2.1 Household demographic changes reported by beneficiaries and
facilitators
Beneficiaries should immediately report household demographic changes to the
District UPPKH through the facilitators. However, the spot check showed that not all
beneficiaries with household demographics changes reported the changes.
At the time the survey was conducted, about half of the beneficiaries had household
changes, either due to school attendance, utilization of health services, or other
changes that should be reported. Out of all types of household changes, class
promotion or going to the next level of education are the largest proportion,
approximately 33%.

30
Table 4.2. Percentage of households who experienced changes since PKH recruitment until the time of this survey, by province
DKI Jakarta
West Java
East Java
West Nusa Tenggara
South Kalimantan
Total
Pregnancy 8.5 12.0 8.0 11.3 7.4 9.5
Miscarriage 1.5 1.0 0.5 0.3 0.6
Birth 9.5 14.3 8.5 13.0 7.7 10.7
Moved to another school 4.0 1.8 0.2 0.8 0.5 1.2
Went to the next level of education
48.5 38.0 38.9 26.5 20.9 33.1
Visited another Puskesmas 1.0 0.3 0.5 0.3 0.5 0.4
Died 0.5 3.5 2.5 1.5 0.3 1.8

31
Out of all beneficiaries who had household demographic changes, only 84% reported
them, and only 54% in 2007 PKH and 76% in 2008 PKH admitted to have signed the
change form. This fact indicates that some beneficiaries did not realize the
importance of reporting their household changes as mandated in the
guidelines. Whereas these changes were associated with the amount of cash
transfer that they would receive.
Table 4.3. Percentage of households that reported changes and signed the form out of all households that had these changes
Parameter DKI
Jakarta West Java
East Java
PKH 2007
West Nusa Tenggara
South Kalimantan
PKH 2008
Total
Number of sample (n) (115) (209) (197) 521 (170) (127) 297 (818)
Reported changes 96.5 79.4 82.2 84.3 89.4 77.2 84.2 84.2
Mengisi formulir 79.1 68.4 67.5 70.4 88.2 70.9 80.8 74.2
Menandatangi formulir 44.3 52.6 59.9 53.6 82.9 66.9 76.1 61.7
4.2.2 Database entry and management problems
Beneficiaries’ household demographic changes were not immediately inputted to
follow the schedule. Six of nine district/city operators who were interviewed
admitted that they entered changes only three times in 2009, while the guideline
requires monthly updates. In some districts, operator stated that updates were done
only when there is a plan for payment. Generally operators complained about the
limited number and capacity of personnel for data entry.
Entry of data changes in the district/city also faced various constraints, including:
problem in software application, electricity shutdown and poor telecommunication
networks that slowed down the on-line connection. Some districts even had
difficulty to access telecommunications providers.
"The application system often had problems so it often could not go online/connect
to the database and this sometimes slowed down the update process” (Operator,
West Nusa Tenggara)
"The timing was so tight, and then the number of PKH beneficiaries in Subang is the
largest throughout West Java, so it created the impression that we were slow, but
we were not slow, it was the bandwidth that was slow" (Operator, West Java)

32
"The application system often had problems .." (Operator, East Java)
Some informants expressed the limited operational cost, including computer
maintenance costs that obstructed the smoothness of data entry process. Operators
and also facilitators also complained scarcity of forms so that they often spent their
money to copy them.
"We were required to perform verification tasks, but the forms were only a few. I
often spent money from my own pocket.... "(Operator, South Kalimantan)
"If possible, there is additional operational fund ... "(Operator, West Java)
Data changes that have been inputted in the district/city UPPKH were often not
followed by changes in the central database. In some cases, the operators admitted
that they had entered the changes, but the beneficiary’s data printed in the cash
transfer did not change.
" According to the facilitators verification and update were clean, and rechecked for
confidence, and the RTSM data were by name and address, it turned out that a
RTSM child attended a school in Cirebon, nonetheless his name came out in the
local education facility here" (Facilitator, Subang district)
"The data that we found did not match the facts, for example a person who was not
pregnant was said to be pregnant." (In-depth at Puskesmas, Pekat sub district,
Dompu District)
4.2.3 Discrepancy of beneficiaries data in the central database and on the
field
Data of some beneficiaries in the central database was not the same with the results
of the spot check. The difference was caused by two possibilities: (a) a different
reference time between data update and spot check, and (2) poor updating process .
Based on the parameters of pregnant women, under-five or school-age children, the
data of 27% of beneficiaries in the spot check turned out to be different from data in
the central database. Suboptimum data update partly contributed to the
discrepancy.

33
“….Yes, at least before payment, the data have been updated, sis, and I always
report them. And I write all of those reports in the monthly report .. "(Operator,
Subang district)
“…because the instruction from there (central), twice a year every time payment will
be made, update will be conducted.... "(District HSS operator)
“…yes, basically a month before payment, (the data) should be final ..."(operator,
Cirebon district)
Table 4.4. Percentage of households with different data between central database and results of spot check
Parameter DKI
Jakarta West Java
East Java
PKH 2007
West Nusa Tenggara
South Kalimantan
PKH 2008
Total
(n) (200) (400) (401) 1001 (400) (392) 792 (1793)
Data Tidak sesuai 25.0 26.5 19.0 23.2 29.75 35.5 32.6 27.3
Bumil 2.5 3.3 3.2 3.1 8.5 2.3 5.4 4.1
Balita 11.0 10.0 7.7 9.3 8.3 6.1 7.2 8.4
Bumil atau balita 10.0 9.3 9.0 9.3 8.5 6.1 7.3 8.4
Anak usia SD 16.0 14.8 13.0 14.3 14.0 24.5 19.2 16.5
Anak usia SMP 11.5 13.3 5.5 9.8 13.0 14.0 13.5 11.4
The size of data discrepancy in the central database and spot check depended on the
parameters. Below is the discrepancy rate by parameter:
A. Data on pregnancy and under-five children
In terms of pregnant women, the data of 4.8% of beneficiaries in the spot check
were different from data in the central database . This percentage was relatively
higher because pregnancy rate seems to be no more than 10% of the total
population.
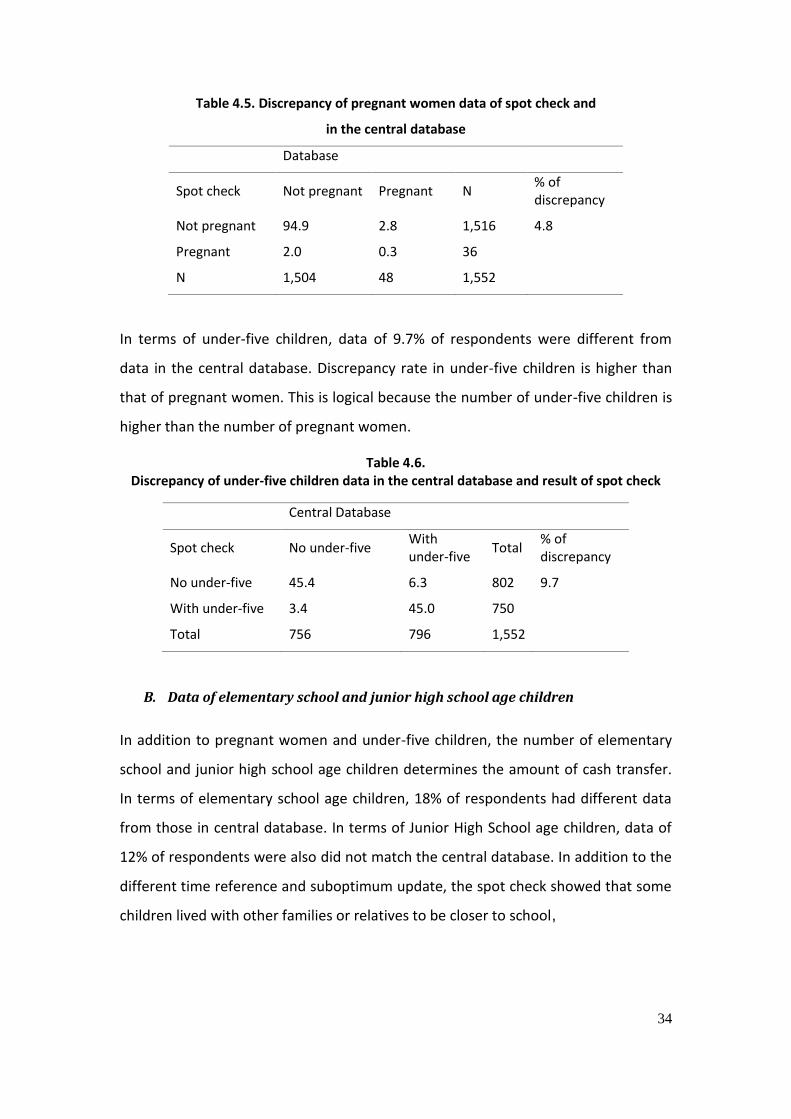
34
Table 4.5. Discrepancy of pregnant women data of spot check and
in the central database
Database
Spot check Not pregnant Pregnant N % of discrepancy
Not pregnant 94.9 2.8 1,516 4.8
Pregnant 2.0 0.3 36
N 1,504 48 1,552
In terms of under-five children, data of 9.7% of respondents were different from
data in the central database. Discrepancy rate in under-five children is higher than
that of pregnant women. This is logical because the number of under-five children is
higher than the number of pregnant women.
Table 4.6. Discrepancy of under-five children data in the central database and result of spot check
Central Database
Spot check No under-five With under-five
Total % of discrepancy
No under-five 45.4 6.3 802 9.7
With under-five 3.4 45.0 750
Total 756 796 1,552
B. Data of elementary school and junior high school age children
In addition to pregnant women and under-five children, the number of elementary
school and junior high school age children determines the amount of cash transfer.
In terms of elementary school age children, 18% of respondents had different data
from those in central database. In terms of Junior High School age children, data of
12% of respondents were also did not match the central database. In addition to the
different time reference and suboptimum update, the spot check showed that some
children lived with other families or relatives to be closer to school,

35
Table 4.7. Discrepancy of school age children data in the central database and the results of spot check
Database
Spot Check No elementary school age child(ren)
Elementary school age child(ren)
Total, N % of discrepancy
No elementary school age child(ren) 27.9 6.3 633 17.9 elementary school age child(ren) 11.6 54.3 1,219 Total N 730 1,122 1,852 Database
No Junior High School age child(ren)
Junior High School age child(ren)
Total % of discrepancy
No Junior High School age child(ren) 63.8 5.6 1,284 12.0 Junior High School age child(ren) 6.4 24.3 568 Total N 1,299 553 1,852
Confession of most operators who inputted the updates three times in 2009
reflected the suboptimum data update process. This was supported by facilitators’
complaints in one district on the lack of operators’ response to follow up data
updates that they did at district level. Below are some informants’ statements
related with problems in data updates.
“Every time we update data, especially during payment, data on non-eligible will
come up, address change will come up again, so it seems that update is useless
because operator did not enter them. Actually every time there is visit from central
level or others, facilitators will be blamed, they say inaccurate data update" (FGD
with facilitators, Banjar District).
“…I ask each of my members to update data, so they will submit it to me and I
forward it to the facilitator .... But seems that there is no change .... "(Group leader,
West Java)
Some cases indicated discrepancies between central database and reality, such as:
an old woman who lived alone with no little child received PKH, a Mrs. X was
reported dead, but she was still in the list, beneficiary X have moved, but the old
address was still printed, someone did not receive any payment but her’s name
remained in the payment list, a child who graduated from Junior High School was still
recorded in the P form, a woman who had delivered a baby but was still listed as

36
pregnant, etc. Below are some statements about suboptimum validation and data
update.
“An old woman who lives alone with no little child as ART, but she receives PKH”
(Banyuputih village, Sumberej sub district, East Java)
“According to the facilitator s/he was already crossed out but still in the list”
(Gunung Putri village, Suboh sub district, Bojonegoro)
“S/he passed away, but still in the database (Ketah village, Suboh sub district) (Olean
village, Situbondo sub district).” (Patokan village, Situbondo sub district)
“Already divorced, but it still in the list, the address changed.” (Talkandang village,
Situbondo sub district)
“A child who already finished school, but still recorded in the database, whereas the
data changed.”(Banjar district, South Kalimantan)
“A pregnant woman who should have delivered, is still listed as pregnant, and
Elementary school child(ren) is still listed as under-five child(ren).” (Banjar district,
South Kalimantan)
“There are families who do not cash transfer because the operator considers them no
longer eligible but their names remain in the list.” (Kertak Hanyar village, Banjar
district, South Kalimantan)

37
CHAPTER 5 THE PAYMENT PROCESS
Central UPPKH calculates the amount of payment to the beneficiaries based on
household composition data and compliance to conditionality. The amount of the
first payment is based on validated number of pregnant women, under-five
child(ren), and/or school-age child(ren) in the first meeting. The payment for the
next three months is based on updated household demographic changes during the
period. In addition, the amount of the second and the next payment is not only
based on household composition data, but also compliance to conditionality toward
utilization of basic health and education services. After calculating the amount, the
Central UPPKH gives the payment data to PT. Pos every three months and PT Pos
pays beneficiaries in each village every three months (quarterly) on an assigned date.
To receive the payment, beneficiaries should show their PKH identity card.
Spot check results indicated that the program has made payment to the
beneficiaries according to household composition as listed in the central database,
but did not consider compliance to conditionality as the basis for payment. When
this spot check was conducted, payment based on compliance to conditionality was
still a pilot project in 23 districts. The conditional cash transfer would be
implemented gradually in early 2010.
5.1 AMOUNT OF PAYMENT
5.1.1 Payment Based on Household Composition
The amout of payment up to Rp 2.2 million per year (depending on household
composition) will be given to the mother if the household members comply with the
PKH conditionality. The payment is calculated using the following formula
= 200,000 + 800,000*(pregnant woman/under-five child(ren)) + 400* number of
Elementary school-age child(ren) + 800,000* number of Junior high school-age

38
child(ren).
Based on spot check household survey , 75% of respondents received correct
payment, while 8% of them were underpaid and 17% of them were overpaid . The
average underpayment was Rp. 188,755 and overpayment was Rp. 204,562.
Table 5.1. Percentage of beneficiaries with correct and incorrect payment as compared to the household composition
Correct/ incorrect payment
DKI Jakarta
West Java East Java West Nusa Tenggara
South Kalimantan
Total
N 174 337 359 350 283 1,503
Correct payment 76.4 74.8 81.6 69.7 72.8 75.0
Underpayment 9.2 8.9 6.7 8.6 7.4 8.1
Overpayment 14.4 16.3 11.7 21.7 19.8 16.9
= 200,000+ 800,000**(pregnant woman/under-five child(ren)) + 400*Elementary school-age child(ren) + 800,000* Junior high school-age child(ren)
Table 5.2. The average of Incorrect Payment (Rupiah) as Compared to the household composition
Incorrect Payment DKI Jakarta
West Java East Java West Nusa Tenggara
South Kalimantan
Total
Underpayment 175,063
204,500
194,500
200,044
154,000
188,755
Overpayment 245,360
206,061
196,754
201,632
194,708
204,562
The discrepancy reflects the differences between household composition data
collected during the spot check against data from the Central Database. The
differences may occur due to the time lag ; the Central Database referred to
payment period before November 2009 while household survey data was collected
in January 2010. From November 2009 to January 2010 household composition
would possibly change. However, this might also reflects weakness of the updating
process.
Various cases of payment discrepancy and weak updating process were revealed
through group discussion with facilitators and in-depth interviews with beneficiaries.
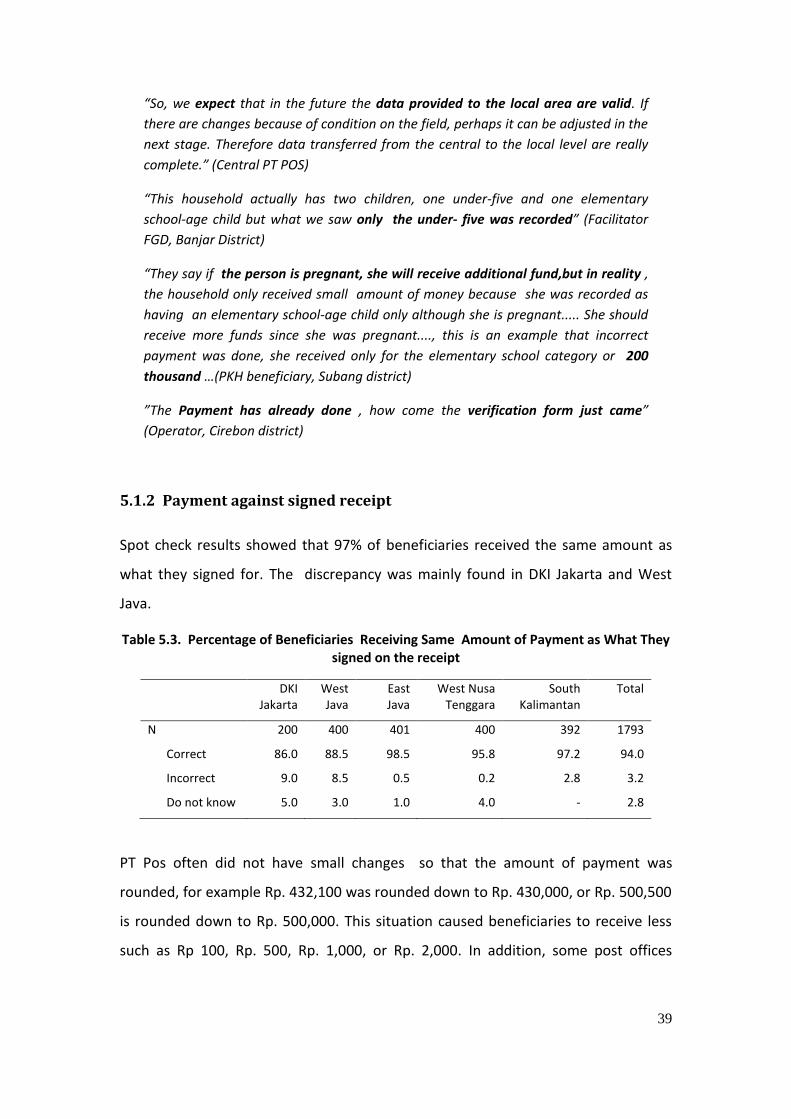
39
“So, we expect that in the future the data provided to the local area are valid. If
there are changes because of condition on the field, perhaps it can be adjusted in the
next stage. Therefore data transferred from the central to the local level are really
complete.” (Central PT POS)
“This household actually has two children, one under-five and one elementary
school-age child but what we saw only the under- five was recorded” (Facilitator
FGD, Banjar District)
“They say if the person is pregnant, she will receive additional fund,but in reality ,
the household only received small amount of money because she was recorded as
having an elementary school-age child only although she is pregnant..... She should
receive more funds since she was pregnant...., this is an example that incorrect
payment was done, she received only for the elementary school category or 200
thousand …(PKH beneficiary, Subang district)
”The Payment has already done , how come the verification form just came”
(Operator, Cirebon district)
5.1.2 Payment against signed receipt
Spot check results showed that 97% of beneficiaries received the same amount as
what they signed for. The discrepancy was mainly found in DKI Jakarta and West
Java.
Table 5.3. Percentage of Beneficiaries Receiving Same Amount of Payment as What They signed on the receipt
DKI Jakarta
West Java
East Java
West Nusa Tenggara
South Kalimantan
Total
N 200 400 401 400 392 1793
Correct 86.0 88.5 98.5 95.8 97.2 94.0
Incorrect 9.0 8.5 0.5 0.2 2.8 3.2
Do not know 5.0 3.0 1.0 4.0 - 2.8
PT Pos often did not have small changes so that the amount of payment was
rounded, for example Rp. 432,100 was rounded down to Rp. 430,000, or Rp. 500,500
is rounded down to Rp. 500,000. This situation caused beneficiaries to receive less
such as Rp 100, Rp. 500, Rp. 1,000, or Rp. 2,000. In addition, some post offices

40
requested beneficiaries to prepare certain amount of money for duty stamp
(meterai) when they receive payment, this was actually unncessary.
“If possible, the payment for this program should be rounded because it is very
difficult when the money is not rounded (needs small change).” (PT. Pos, Banjar
district)
“No small changes in the post office ),well ... that’s the policy..... For example if it is
Rp. 2,000 less, well, it is OK, what can we do?.” (PKH beneficiary, Cirebon district)
Approximately 38% of facilitators and 26% of the PT. POS officers that were
interviewed confirmed that some beneficiaries did not receive the correct amount.
Some beneficiaries did not know how much money they should receive. For them,
the most important thing was to receive the money from the government
regardless the amount (it’s better than nothing).
“Mada doho wati bademu ra raka ba mada doho sesuai ato bune, ma pentina mada
doho raka bantuan, syukur ra” (We do not know whether the amount that we receive is
correct or not, the important thing is that we receive cash transfer and are grateful for
it) (FGDPKH beneficiary, Bima district)
On the other hand, there are cases where beneficiaries tried to get more cash
transfer, i.e by admitting that she was pregnant although she was not or send her 4-
year old child to school.
"There was a data found that in reality never happenned , such as she was not
pregnant, but it was mentioned that she was”. (In-depth Puskesmas, Pekat
subdistrict, Dompul district)

41
5.2 THE PAYMENT PROCESS
5.2.1 Payment Reconciliation
Payment requires auditing process of validity and accuracy. To meet this
requirement, cclarification and verification of payment receipts will be done by
various parties using reconciliation mechanism. Almost all of the districts reconciled
the payment by verifying PT Pos’ back-up receipts with facilitators’ and/or
operator’s data.
5.2.2 Schedule and Delay of Payment
The study revealed that in many areas, schedule and frequency of the payment did
not always follow the guidelines. Frequency of payment should be four times
annualy , in reality in many areas it was three, even in 7 (seven) sub districts in West
Nusa Tenggara it was disbursed twice which was in June/July and
November/December 2009. Despite no reduction in the total annual fund
allocation, schedule as written in the guidelines was considered important and
should be followed because of it’s potential implication on beneficiaries’ plan to use
the money.
Central UPPKH set up the fourth payment schedule to be conducted within the last
three months of the referred year, from October to December, with the day and
date to be decided by each district/city. Spot check results indicated that about 11%
of beneficiaries admitted that they had 2 (two) week delay from the scheduled date.
Half of them did not know the reason for the delay.
“…Because by nature, PKH involves the district and city, say, to determine the
payment date. District/municipality government often asks to reschedule because
of the conflicting schedule with some activities in the area. Or, , the local
government would like to attend , but at the same time he/she has another meeting
So actually it was not a big problem, everything could be coordinated (Central PT.
Pos)

42
Table 5.4. Reason for payment delay (%)
DKI Jakarta
West Java
East Java
West Nusa Tenggara
South Kalimantan
Total
Number of respondent who reported the delay 55 46 42 21 20 184
Reason for the delay
Insufficient number of officers in PT. Pos 8.9 6.0 2.2 6.7 4.8 5.9
The election 12.5 10.0 8.9 0 0 7.9
Insufficient fund/central level had not transferred fund 17.9 28.0 11.1 16.7 38.1 20.8
Incomplete data/administration 5.4 10.0 0 6.7 14.3 6.4
Demonstration of the community who did not receive PKH cash transfer 0 2.0 26.7 10.0 0 7.9
Do not know 53.6 36.0 44.4 30.0 38.1 42.1
Discussions and interviews with facilitators and mother leaders confirmed the case
of delayed payment. One reason of the delay was conflicting schedule with BLT
payment to non PKH members.
“...for example the money was taken on Monday at the same time with BLT last year, so
the Post office could not distribute PKH, .....so BLT come first, and then one day interval,
and the next day we went there We told beneficiaries door to door that the cash
transfer was delayed because BLT disbursement was not finished yet, since we use the
same the post office so our turn would be the next day ..” (Mother leader, Cilincing sub
district)
“So for RTSMs who have not received the cash transfer, the process is delayed to
the next day, ...............so they went home empty-handed” (Facilitator, Banjar
district)
In another district, the reason for the delay was shortage of cash in the PT Pos at the
sub district.
“It happened sometimes, cash shortage to be distributed to the branch post offices.
Usually the payment was delayed for 1 or 2 days, then the RTSMs would go to
Kempo Post office.” (FGD facilitator, Dompu district)
43
5.2.3 The Role of Facilitator in the Payment Process
Most facilitators admitted that they notified beneficiaries and coordinated with the
operators and the Post Office to determine the location and time of payment. All
facilitators said that they accompanied beneficiaries when receiving the cash
transfer, but not all of them kept the beneficiaries’ payment receipt.
5.2.4 Payment Location and Transportation Cost
The location for payment is the Post Offices at the district and sub district. Sub
districts that do not have a post office will distribute the cash transfer fund in the
district or kelurahan office. To reach the post office or sub district office, some PKH
beneficiaries had to spend transportation fee. Generally the beneficiaries did not
think of the transportation fee as a burden. Average transportation fee to go to the
location was Rp. 3,560,-
5.2.5 Waiting Time in the Payment Location
Post office do not only serve PKH beneficiaries, but also other communities, so PKH
beneficiaries should wait for quite long to receive payment. Spot check result
showed 60 minutes as the median waiting time.
5.3 DEDUCTION OF THE CASH TRANSFER FUND
16% of beneficiaries admitted to have one or more types of deduction. The
deduction included administration fee, donations, or other fees. “Other fees”
including contribution (under the table fee), etc. were the most often. Average cash
transfer deductions for donation were Rp. 26,000 (PKH 2007) and Rp. 23,000 (PKH
2008).
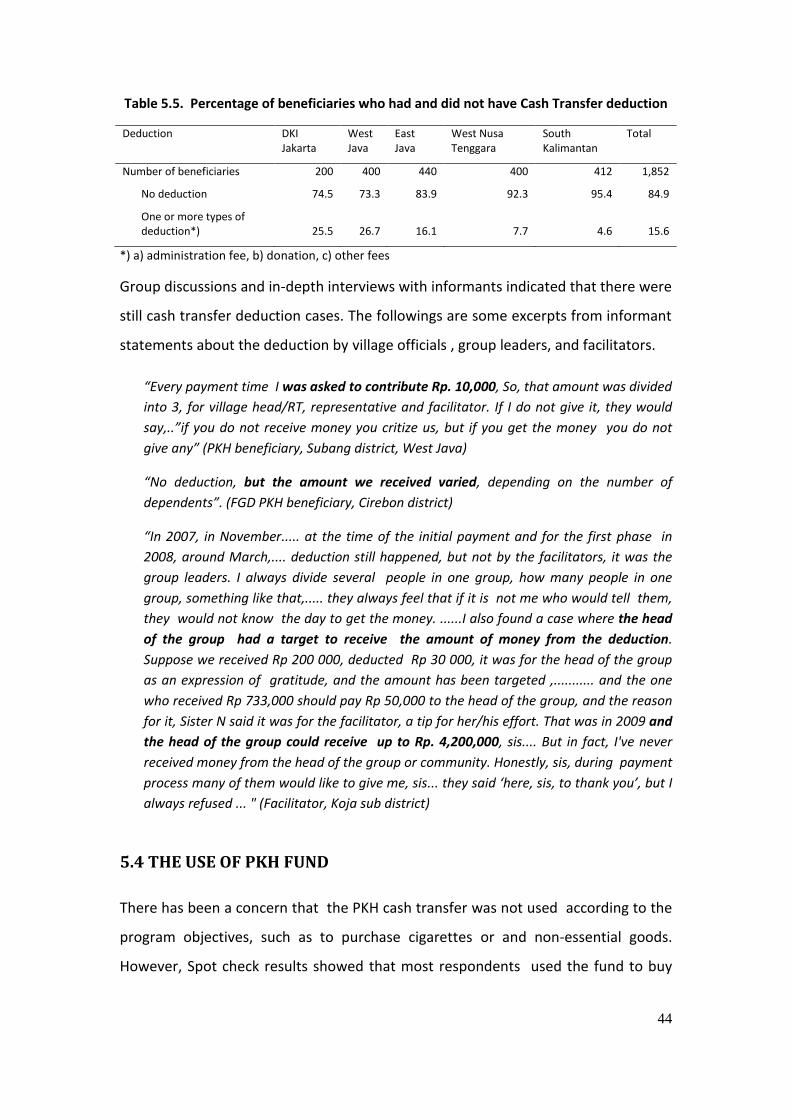
44
Table 5.5. Percentage of beneficiaries who had and did not have Cash Transfer deduction
Deduction DKI Jakarta
West Java
East Java
West Nusa Tenggara
South Kalimantan
Total
Number of beneficiaries 200 400 440 400 412 1,852
No deduction 74.5 73.3 83.9 92.3 95.4 84.9
One or more types of deduction*) 25.5 26.7 16.1 7.7 4.6 15.6
*) a) administration fee, b) donation, c) other fees
Group discussions and in-depth interviews with informants indicated that there were
still cash transfer deduction cases. The followings are some excerpts from informant
statements about the deduction by village officials , group leaders, and facilitators.
“Every payment time I was asked to contribute Rp. 10,000, So, that amount was divided
into 3, for village head/RT, representative and facilitator. If I do not give it, they would
say,..”if you do not receive money you critize us, but if you get the money you do not
give any” (PKH beneficiary, Subang district, West Java)
“No deduction, but the amount we received varied, depending on the number of
dependents”. (FGD PKH beneficiary, Cirebon district)
“In 2007, in November..... at the time of the initial payment and for the first phase in
2008, around March,.... deduction still happened, but not by the facilitators, it was the
group leaders. I always divide several people in one group, how many people in one
group, something like that,..... they always feel that if it is not me who would tell them,
they would not know the day to get the money. ......I also found a case where the head
of the group had a target to receive the amount of money from the deduction.
Suppose we received Rp 200 000, deducted Rp 30 000, it was for the head of the group
as an expression of gratitude, and the amount has been targeted ,........... and the one
who received Rp 733,000 should pay Rp 50,000 to the head of the group, and the reason
for it, Sister N said it was for the facilitator, a tip for her/his effort. That was in 2009 and
the head of the group could receive up to Rp. 4,200,000, sis.... But in fact, I've never
received money from the head of the group or community. Honestly, sis, during payment
process many of them would like to give me, sis... they said ‘here, sis, to thank you’, but I
always refused ... " (Facilitator, Koja sub district)
5.4 THE USE OF PKH FUND
There has been a concern that the PKH cash transfer was not used according to the
program objectives, such as to purchase cigarettes or and non-essential goods.
However, Spot check results showed that most respondents used the fund to buy

45
child(ren)’s school equipment (87%) and daily food (66%). Only 16% of respondents
used it for transportation to health facilities and 19% for transportation to school.
Table 5.6. Distribution (%) of the use of PKH cash transfer
DKI Jakarta
West Java East Java West Nusa Tenggara
South Kalimantan
Total
Number of Respondent 200 400 440 400 412 1852
Transportation to health facility
9.,0 15.9 1.2 38.0 15.1 16.2
Transportation to school 20.5 38.1 7.0 11.9 18.4 18.8
Child(ren)’s school equipment
84.5 90.4 89.0 90.0 85.1 87.2
Examination & treatment for sick family members
12.0 24.7 9.0 22.4 33.0 20.9
Daily food needs 48.0 67.4 42.4 97.9 70.3 66.0
Donation/contribution for other parties
0.5 11.6 4.5 8.2 1.5 5.7
Other needs 55.0 17.2 40.9 30.1 10.6 27.8
5.5 PAWNED BENEFICIARY’S CARD
Despite only few beneficiaries (1%) admitted that they use their PKH cards to borrow
money, concern that PKH card was pawned did occur in most provinces.
“We had an interesting experience in our area, there was a case where one group leader
who said that she/he acted on behalf of facilitators collected all PKH cards to be
pawned, fortunately at that time a member questioned it to the facilitator. " (FGD
Facilitator, Bima District)

46
CHAPTER 6 COMPLIANCE TO CONDITIONALITY
Sending elementary and Junior High School-age children to school, and utiziling
health facilities for under-five children, pregnant, laboring and post partum women
are the conditionality for PKH beneficiaries. Compliance to these conditionality is
assessed through registration form, school attendance and health service utilization
in Puskesmas and its network. It is compulsory for school-age children to be
registered in elementary schools/MIs or junior high school/MTs; or open type of
junior high schools/MTs’ package A/B program and attend at least 85% school
activities or required total number of face-to-face sessions every month. Under-five
children should get complete immunization; have weighing every month and vitamin
A twice a year. Pregnant women are required to have antenatal care at least 4 (four)
antenatal care during pregnancy (K1/first visit in the first trimester, K2/second visit
in the second trimester, and K3 and K4/third and forth visits in the third trimester).
Delivery should be assissted by skilled health provider, while post partum women
and newborns should have health examination at least twice within 28 days of
postpartum.
PKH is a conditional cash transfer program. To achieve program’s objective to meet
the conditionality, the program should have the ability to verify beneficiaries’
compliance. According to the guidelines, verification process includes the printing of
PT Pos verified forms to match the central database, distribution of the forms by PT
Pos to the education and health facilities, collection of completed forms by PT Pos
from the education and health facilities and forwarding them to the district/city
UPPKH, and entry of verified data on compliance by the district/city operators and
online reporting of the verified data to the Central UPPKH Management Information
System.
Spot check showed that the program compliance verification did not work well.
Some beneficiaries did not comply with conditionality on utilization of basic health
and education services. Even one district used different way to verify compliance,

47
such as asking the legalized copy of child's school raport or proof of child weighing
book (KMS).
6.1 UTILIZATION OF EDUCATION SERVICES
6.1.1 6-15 year-old child(ren) who do not go to school and drop Out
Spot check found 1.8% of school-age children did not go to school, with a relatively
high percentage in DKI Jakarta (2.5%) and in South Kalimantan (2.3%). The main
reason was because they were considered not old enough to go to elementary
school and will be enrolled in 2010. The percentage of school-age children who ever
attended school and then dropped out was approximately 2% with the highest rate
in West Java (4%). The reasons to quit school included they "do not want to go to
school", did not have the funds or helped parents to earn income. Only a small
proportion of school-dropout children were suggested to go back to school.
Approximately 80% of beneficiaries with school-dropout children admitted that no
one suggested these children to go back to school, or take open type of Junior High
School/MTs package A/B.
Table 6.1. Distribution (%) of school-age children who do not go to school and drop out
DKI Jakarta
West Java
East Java
West Nusa Tenggara
South Kalimantan
Total
Number of 6-15 year old children
284 526 425 529 480 2,244
Not in school age yet 2.5 1.9 1.6 1.1 2.3 1.8
Drop out 2.8 3.6 0.5 1.1 2.7 2.1
Drop out, but suggested to go back to school
0.7 0.8 0,0 0.6 0.2 0.4
Regarding children who did not go to or drop out of school, school in one sub district
in West Nusa Tenggara said that they never refuse school-age children of PKH
beneficiaries to enroll, and give free tuition for all students either PKH beneficiaries
or not.

48
"There are no constraints, because schools are free for the students from any cost,
this is the Dompu government program to give free tuition. PKH beneficiaries or not,
we invite them to enroll ... "(School at Woja sub district, Dompu)
6.1.2 Children 6-15 year old who go to school
Out of 6-15 year old children who went to school, 71% attended elementary school
or equivalent, while the rest were in junior high school or equivalent, with the
average percentage of attendance 98% or above the minimum requirement of 85%.
The parents who are PKH beneficiaries confirmed this high rate of school
attendance. Beneficiaries in one sub district in West Nusa Tenggara admitted that
their children were actively joining the school because they were afraid that the cash
transfer would be deducted if their children were often absent.
“Now my child(ren) are afraid if they do not go to school, because I explained that if
they were often absent, our money would be deducted ..." (PKH beneficiaries, Woja
subdistrict, Dompu)
“... The child(ren) who are lazy or even do not go to school and with PKH can go to
school, and I am satisfied with their marks and it is beyond my expectations, it is
because of the PKH money" (in-depth facilitator, North Jakarta City)
Table 6.2. Distribution of children 6-15 years who go to school by levels and attendance
DKI Jakarta
West Java
East Java West Nusa Tenggara
South Kaliman tan
Total
Number of 6-15 year old children 277 516 418 523 469 2,203
In elementary school / equivalent 65.3 69.4 66.3 75.3 75.3 70.9
in Junior High school / equivalent 31.8 29.7 31.8 23.7 22.6 27.4
Average percentage of school attendance in the last one week
96.1 97.9 98.1 98.8 99.1 98.2
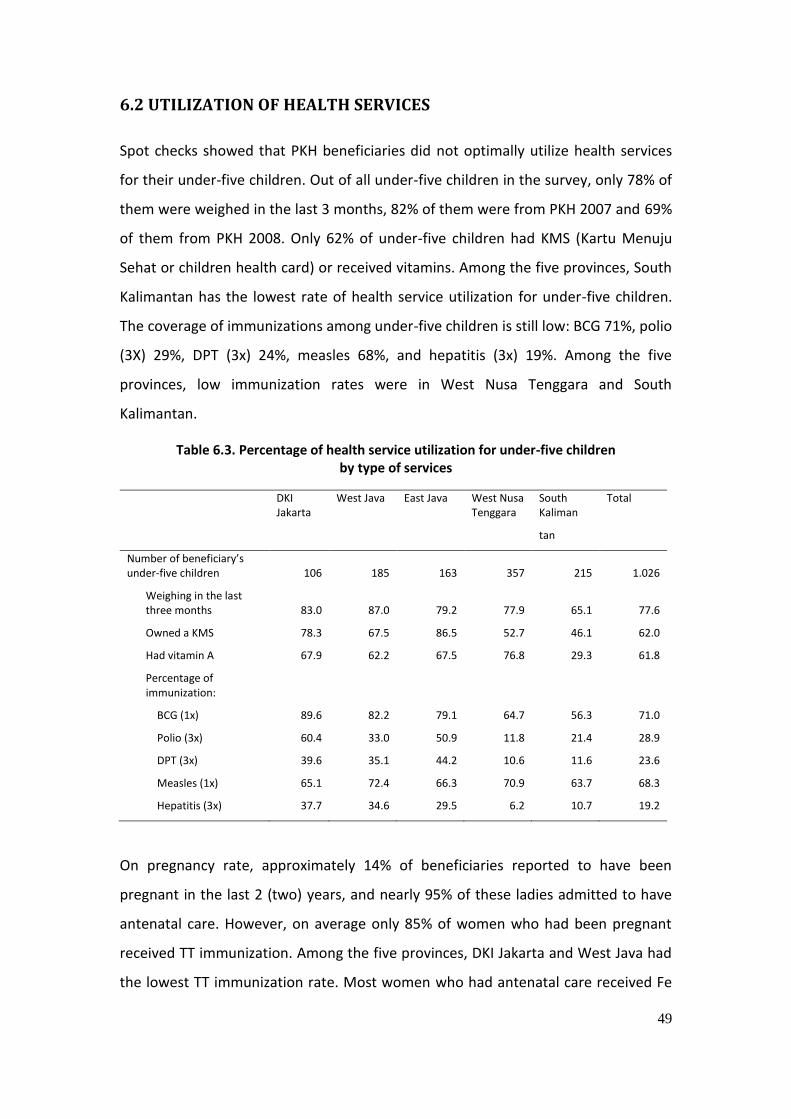
49
6.2 UTILIZATION OF HEALTH SERVICES
Spot checks showed that PKH beneficiaries did not optimally utilize health services
for their under-five children. Out of all under-five children in the survey, only 78% of
them were weighed in the last 3 months, 82% of them were from PKH 2007 and 69%
of them from PKH 2008. Only 62% of under-five children had KMS (Kartu Menuju
Sehat or children health card) or received vitamins. Among the five provinces, South
Kalimantan has the lowest rate of health service utilization for under-five children.
The coverage of immunizations among under-five children is still low: BCG 71%, polio
(3X) 29%, DPT (3x) 24%, measles 68%, and hepatitis (3x) 19%. Among the five
provinces, low immunization rates were in West Nusa Tenggara and South
Kalimantan.
Table 6.3. Percentage of health service utilization for under-five children by type of services
DKI Jakarta
West Java East Java West Nusa Tenggara
South Kaliman
tan
Total
Number of beneficiary’s under-five children 106 185 163 357 215 1.026
Weighing in the last three months 83.0 87.0 79.2 77.9 65.1 77.6
Owned a KMS 78.3 67.5 86.5 52.7 46.1 62.0
Had vitamin A 67.9 62.2 67.5 76.8 29.3 61.8
Percentage of immunization:
BCG (1x) 89.6 82.2 79.1 64.7 56.3 71.0
Polio (3x) 60.4 33.0 50.9 11.8 21.4 28.9
DPT (3x) 39.6 35.1 44.2 10.6 11.6 23.6
Measles (1x) 65.1 72.4 66.3 70.9 63.7 68.3
Hepatitis (3x) 37.7 34.6 29.5 6.2 10.7 19.2
On pregnancy rate, approximately 14% of beneficiaries reported to have been
pregnant in the last 2 (two) years, and nearly 95% of these ladies admitted to have
antenatal care. However, on average only 85% of women who had been pregnant
received TT immunization. Among the five provinces, DKI Jakarta and West Java had
the lowest TT immunization rate. Most women who had antenatal care received Fe

50
tablets, but women’s compliance to taking them was still low. Out of all pregnant
women who received Fe tablets, only 52% reported taking all of them as
recommended.
Table 6.4. Percentage of pregnant women who utilized health services by type of services
DKI Jakarta
West Java
East Java West Nusa Tenggara
South Kalimantan
Total
Number of PKH households 200 400 401 400 392 1,793
Women had been pregnant in the last two years
15.0 11.8 9.0 25.0 11.0 14.3
Women had ANC when pregnant 90.9 93.3 96.9 96.5 87.5 94.6
Women had TT when pregnant 75.0 75.0 80.6 92.7 86.7 85.2
Women had Fe tablets when pregnant 95.0 89.3 93.5 98.8 100.0 96.0
% of pregnant women who complied to taking Fe tablets
63.2 42.3 69.0 46.9 53.3 52.3
Not all deliveries assissted by trained health provider. Average percentage of skilled
birth attendance was just 79%. Among the five provinces, West Java and West Nusa
Tenggara had lower percentage of skilled birth attendance. Similarly, the average
percentage of newborns that were weighed was approximately 80%, with West Java
and West Nusa Tenggara being lower than the other three provinces. Compared to
antenatal and delivery care, the percentage of women who had post partum and
neonatal examinations was lower with 63% and 54% respectively.

51
Table 6.5. Percentage of Delivery , Post Partum and newborns who utilized health services
DKI Jakarta
West Java
East Java
West Nusa Tenggara
South Kalimantan
Total
Number of women in labor/postpartum period in the last two years 18 29 32 83 14 176
Deliveries attended by a health provider 100.0 75.9 81.3 72.3 92.9 79.0
Newborn weighing 100.0 89.7 78.1 73.5 84.6 80.6
Postpartum care 83.3 48.3 71.9 62.7 46.2 62.9
Newborn care 72.2 24.1 65.6 55.1 53.8 53.5
6.3 COMPLIANCE VERIFICATION PROCESS
The verification process of beneficiary’s compliance to conditionality in utilization of
basic health and education services includes the printing of verification form by PT
Pos based on the central database, distribution of the verification form by PT Pos to
education and health facilities, completion of verification forms by the officers in the
facilities, collection of completed forms from the facilities by PT Pos, delivery of the
forms to UPPKH District by PT Pos, data entry of verified data at the district / city
UPPKH by the operators, and adjustment by the Central UPPKH MIS Database based
on the verified data from the UPPKH district.
6.3.1 Printing of verification Forms
The printed verification forms containing a list of household members name who
should go to the appropriate education or health facilities, the list is written based
on the Central Data Base. Spot Check result showed that the printed list containing
names of pregnant or laboring women or school-age children were sometimes
incomplete or inaccurate. This problem is reflected on the statements from a
number of informants.
"Pregnant women who should have delivered is still listed as pregnant, the same
with a child who was already in elementary school, he is still listed as an under-
five" (FGD for facilitators, Banjar District)
"Already divorced, but still on the list or moved, but still on the list". (facilitator,
Kab Situbondo)

52
6.3.2 Verification form acceptance
Spot Check still found several puskesmas and schools with PKH student beneficiaries
who did not receive a verification form. The average percentage of facilities that
receive verification form from PT Pos was 90% of schools and 79% of puskesmas. DKI
Jakarta had the lowest schools and puskesmas that received verification forms, 50%
and 58% respectively. On the other hand, out of the 30 post offices in the survey,
93% stated that they never sent verification forms to the health and education
facilities.
Table 6.6. Verification forms received by the facilities
DKI Jakarta
West Java
East Java West Nusa Tenggara
South Kalimantan
Total
Number of puskesmas 12 24 24 24 24 108
Percentage of puskesmas that received verification forms 58.3 79.2 87.5 66.7 91.7 78.7
Number of schools 12 23 23 24 24 106
Percentage of schools that received verification forms 50.0 82.6 100.0 95.8 100.0 89.6
Timely distribution of verification form to health and education facilities and
collection of completed verification forms is crucial in the verification process of
beneficiary’s compliance. Distribution and collection of verification forms under the
responsibility of PT Pos did not run well because of geographical problems and
location of the facilities was so spread out.
"In general the problem in verification is the delayed in getting the forms, pick them
up, why did it happen, picking up data from schools, there were always excuses,
when we collected them, they were not completed, ..well, ....it is like that, ...but OK,
that means we take it into account, if PT POS said so, they have reasons for that"
(Ministry of Social Affairs)
"Obstacles in the distribution, is that the post office gave the verification form to
the person they trust other than the facilitators, that is why the distribution was
taken over directly by the facilitators." (In-depth with operator, Bima, West Nusa
Tenggara)

53
“PT. POS did not do their responsibility to send the verification forms, PT. POS
claimed to have sent to all health facilities, but it turned out that in Situbondo sub
district, the forms only received by one Pustu, that is Pustu Patokan village while
other facilities said that they did not receive the forms ... "(Facilitator in Situbondo,
East Java)
“Please pay attention to the welfare and safety of our employees, the location of the
Post Office and the destination that we had to reach was very far and risky. Even
for one delivery, our employees should spend one week before finishing the
distribution. It cost a lot of money, how do we pay for it if there is no subsidy from
the program. The government should pay attention to this. “(In-depth with the post
office, Pekat Sub District, Dompu district)
Untimely distribution and collection of verification forms affected officer’s
motivation to complete them. There were cases when the officers completed the
forms, but because PT Pos did not immediately collect them, these officers did not
have any motivation to fill in other forms.
"Some schools had verification schedule in November, December, & January, some
only in December. The delivery, some did it every three months, some delivered
every month, it was not the same, when we did that by ourselves (for April, May,
June) it was for three months we sent it once "(FGD facilitators, Banjar District, South
Kalimantan)
"The forms have never been collected until now since they were delivered by PT
POS officers, we are still waiting for the postman and also to ask about the forms'.
(In-depth to school /public elementary school, Dompu district)
Informants from PT Pos confirmed that some puskesmas and schools did not receive
verification forms due to the geographically challenging location of the service
facilities as in South Kalimantan. There were many rivers, but no bridges and limited
number of postmen.
"The problem is similar, the condition is that all villages that we went to were far
and the roads were damaged. If we cannot find the address, then we go to the head
of the village to ask for assistance ... "(Post Office at Kempo sub district, Dompu
district)
For areas with difficult geographical conditions, usually PT Pos sends the verification
forms to the UPTDs for education and health, and then these units are expected to

54
notify the puskesmas and schools to collect them. This situation is perceived by PT
Pos as they have already accomplished their task, regardless of whether the forms
have or have not been taken by the puskesmas and schools.
"The area of Aluh2 sub district is mostly separated by the river, because there is no
bridge. So we could not deliver directly, so sometimes deliveries were deposited at
the UPTD for education and Puskesmas in the sub district. Then the education and
health facilities returned them to the UPTD at the sub district, then the post office
took them at the sub district UPTD "(Post Office of Aluh2 sub district)
6.3.3 Completion of verification forms
This study showed that many education and health facilities providing services to
PKH beneficiaries did not complete the verification forms. Percentage of schools that
completed the form varied from the lowest in Jakarta with only 8% to the highest in
West Nusa Tenggara with 58%, the average for all schools in five provinces is 32%.
Consistent with this is the percentage of puskesmas that completed the verification
form also varied with DKI Jakarta being the lowest at 25% and West Nusa Tenggara
being the highest at 83%.
Table 6.7. Completion of verification forms at school and Puskesmas
DKI Jakarta
West Java East Java West Nusa Tenggara
South Kalimantan
Total
Number of schools 12 23 23 24 24 106
Percentage of schools that completed verification forms 8.3 17.4 21.7 58.3 41.7 32.1
Number of puskesmas 12 24 24 24 24 108
Percentage of puskesmas that completed verification forms 25.0 54.2 75.0 83.3 58.3 63.0
According to the facilitators in Jakarta, the puskesmas officers were reluctant to
complete the verification forms, it was useless because the Post Office never
collected them
".. The form has just existed in 2008, sister,..... in the beginning of the PKH, yes, it was completed, almost 100% was completed by the schools and puskesmas, but a few months later they felt that they took the time to complete the forms, did not get paid, but then it was not collected, ........Even to deliver these forms, they do not know where to send, because on the brown envelope it was written from the
55
Ministry of Social Affairs, there is no return address for the completed forms, because from the beginning they were told that someone from the POS would deliver and pick them up, but in reality on the field the forms was not collected .. "(Facilitator, Koja sub district, North Jakarta)
Absence of incentive, ignorance on how to fill in the form, discrepancy of names and
addresses listed on the form and not smooth collection of verification form were the
causes why many education and health facilities did not complete the form.
Interviews with school officials and puskesmas indicated that some officers in the
facilities did not understand how to fill in the verification form. In practice, staff of
puskesmas and network recorded patient visits on a log book at the puskesmas
according to the following cohort categories such as pregnant women, KMS,
immunization, weighing, and so on. But there was no separate recording in the log
book for PKH and non-PKH beneficiaries. For this, the health officers got confused to
match the names on the verification form with the names in the log book.
"Yes, how to fill in this form, sis? Please explain... "(Puskesmas Personnel, Kelurahan Cilincing 1) "Frankly speaking, I don’t know about the form, especially I’m still new here, replacing a colleague. And also I don’t understand how to fill in and distribute the form.” (Indepth Pustu, Langgudu Subdistrict, Bima, West Nusa Tenggara)
"In regards to this PKH program we are always ready. But we expect is coordination, so that the school did not just fill in the form the way they wanted it, perhaps facilitator can assist or at least give explanation on how to fill in the form." (In-depth with Headmaster/ Public Elementary School, Bima, West Nusa Tenggara)
"We have a special officer to manage the form recording, but there was a problem in filling the data when the information from the lower level is incomplete... and we found the data do not match reality, for example a woman who was not pregnant was said to be pregnant, this will become a dilemma for us because involving it concerns money / funds received by PKH beneficiaries, so until now we haven’t submitted the verification form, about this problem we wait for the local policy from the district... "(Puskesmas at Pekat sub district, Dompu)
Errors in the name or data listed in the verification form are still found. For example,
school children who have been listed as drop out or graduated from school were

56
found, but their names still remained in the form; women was written as pregnant
though they were not anymore.
"Yes many people accidentally exchanged data, for example this child goes to this
elementary school, but he appeared on the verification form as attending another
elementary school " (M. Nurrahman, facilitator of Subang district)
"There were children who have graduated, but still listed there though the data
have changed" (Facilitator, Bima)
6.3.4 Collection of verification forms from service facilities
All of PT Pos offices , except in DKI Jakarta and East Java, said that they collected the
completed verification forms from the puskesmas and schools.
Table 6.8. Collection of verification forms from service facilities by PT Pos
DKI Jakarta
West Java
East Java
West Nusa Tenggara
South Kalimantan
Total
Number of Post Offices 3 9 5 6 7 30
Percentage of post offices admitted to collect the forms from puskesmas 33.3 100.0 60.0 100.0 100.0 83.3
Percentage of post offices admitted to collect the forms from schools 33.3 88.9 60.0 100.0 100.0 80.0
However, staff of the schools and puskesmas said that the Post Office often did not
collect the verification forms from the facilities. Statements from facilitators and
school officers :
"The forms have not been collected until now after they were delivered by the Post
Officers, we are still waiting for the officer and also ask about the form ..." (School in
Woja Subdistrict, Dompu)
"Yes it's because there is no fee for filling in the forms so we feel uneasy to do it. The
Post officer said that the verification form have not been completed by the school, so
the forms were not collected, in the end they blame each other "(Operator, Subang
District, West Java)
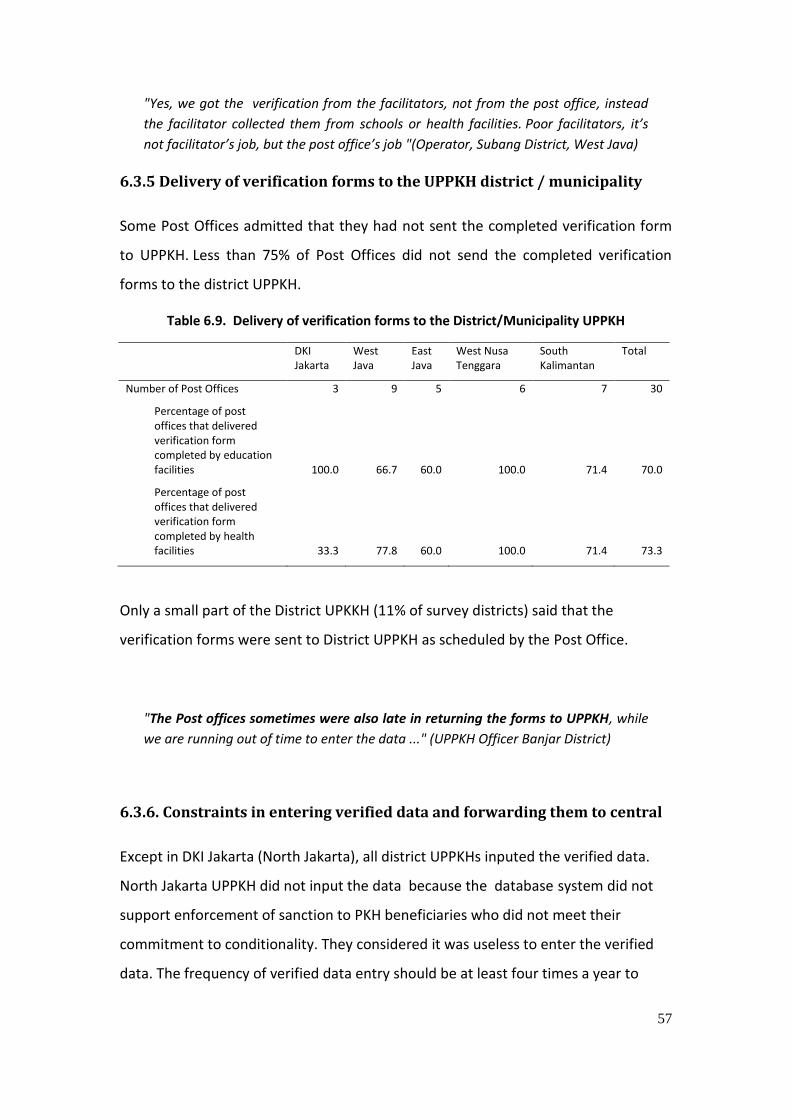
57
"Yes, we got the verification from the facilitators, not from the post office, instead
the facilitator collected them from schools or health facilities. Poor facilitators, it’s
not facilitator’s job, but the post office’s job "(Operator, Subang District, West Java)
6.3.5 Delivery of verification forms to the UPPKH district / municipality
Some Post Offices admitted that they had not sent the completed verification form
to UPPKH. Less than 75% of Post Offices did not send the completed verification
forms to the district UPPKH.
Table 6.9. Delivery of verification forms to the District/Municipality UPPKH
DKI Jakarta
West Java
East Java
West Nusa Tenggara
South Kalimantan
Total
Number of Post Offices 3 9 5 6 7 30
Percentage of post offices that delivered verification form completed by education facilities 100.0 66.7 60.0 100.0 71.4 70.0
Percentage of post offices that delivered verification form completed by health facilities 33.3 77.8 60.0 100.0 71.4 73.3
Only a small part of the District UPKKH (11% of survey districts) said that the
verification forms were sent to District UPPKH as scheduled by the Post Office.
"The Post offices sometimes were also late in returning the forms to UPPKH, while
we are running out of time to enter the data ..." (UPPKH Officer Banjar District)
6.3.6. Constraints in entering verified data and forwarding them to central
Except in DKI Jakarta (North Jakarta), all district UPPKHs inputed the verified data.
North Jakarta UPPKH did not input the data because the database system did not
support enforcement of sanction to PKH beneficiaries who did not meet their
commitment to conditionality. They considered it was useless to enter the verified
data. The frequency of verified data entry should be at least four times a year to

58
match frequency of payment. In reality, the frequency of data entry by the district
UPPKH is ranging from 1 (one) to 3 (three) times a year.
District/city operators faced many constraints in inputing verified data and
forwarding them to central. Constraints that were presented by operators in nine
districts were varied , such as : PT Pos often did not return the verification form on
schedule, hardware facilities were inadequate, inadequate data entry personnel
both quantity and quality ; electricity problem ; and problem on software
application and online system . South Kalimantan province often has rotation of
blackouts due to limited electricity supply and voltage drop. There were only 2 (two)
data entry personnel available and no capacity to handle data entry in such
condition.
Table 6.10. Distribution (in %) of data entry problems in UPPKH District/municipality
Problems in Inputing Verified Data (N=9)
The post office did not return the verification forms on schedule 66.7
The application was not working well 22,2
Network was not really/was not running (Internet / LAN) 22.2
Inadequate hardware (card reader, computer, etc.) 22.2
Entry personnel (inadequate, poorly qualified, etc.) 11.1
Electrical /electricity problems 33.3
Others 11.1
6.3.7. Utilization of verification results
According the Central UPPKH MIS, from November to January 2010 verified data
were used to determine the amount of payment to 40% of beneficiaries, and in the
next three months to 85% of them. However, spot check results showed that 38% of
the surveyed UPPKH leaders said that the verification results had not been utilized
for decision making of the next payment. Therefore, sanction for PKH beneficiaries
who did not meet the commitment is not enforced well.
"yes it should be like that, but the punishment is not imposed, plan just like for the
85% should be from the beginning, but in reality there is none" (Operator, Cirebon
district)
59
In 2008, North Jakarta UPPKH made an agreement with the facilitators and it was
approved by the Local Ministry of Social Office to proceed sanction enforcement to
PKH beneficiaries who did not meet their obligations. PKH beneficiaries in North
Jakarta were requested to submit a copy of school raport or KMS book or antenatal
care book legalized by the education or health facilities when receiving the PKH cash
transfer. If conditionality were not met, the name of the PKH family member was
deactivated/ removed from the list of the next payment. For example, if the child of
a PKH beneficiary did not meet the required school attendance, the operator will
remove the child’s name in the calculation of cash transfer amount.
"Yes, we asked for a legalized copy of school raport per semester, that’s one thing,
and for the health facility, we ask for the KMS ... as evidence that s/he weighed
her/his baby ..." (Facilitator, Tanjung Priok sub district)

60
CHAPTER 7 SERVICE PROVISION
PKH should be supported by provision of affordable, accessible and quality basic
education and health services. Accessible in terms of distance and affordable in
terms of cost. Quality means adequate in quantity, competency of human resources,
facilities and infrastructure.
7.1 PROVISION OF EDUCATION SERVICES
This section discusses two essential issues: (i) accessibility of education services for
beneficiaries, and (ii) quality of available education services. In general it can be
concluded that basic education services in terms of number of schools is adequate,
while in terms of quality, there are a lot of things to improve, including quantity and
quality of teachers, facilities and infrastructure.
7.1.1 Distance, travel time and modes of transportation to school
Most elementary schools/MIs and junior high schools/MTs can be reached on foot.
The distance from home to elementary schools/MIs on average is 0.8 km with travel
time approximately 15 minutes. The distance from home to junior high school/MTs
on average is 2.2 km with travel time approximately 22 minutes.
Table 7.1. Mean Distance (km) from Home to School
Province Elementary schools/MI Junior high schools/MTs
Mean Maximum Mean Maximum
DKI Jakarta 0.5 2 1.3 12
West Java 0.7 7 2.7 15
East Java 1.1 10 3.5 20
West Nusa Tenggara 0.6 5 1.2 12
South Kalimantan 0.9 4 1.5 12
All Provinces 0.8 10 2.2 20

61
Table 7.2. Travel time (minute) from home to school
Elementary schools/MIs
Junior High Schools/MTs
Mean Maximum
Mean Maximum
DKI Jakarta 14 45 20 65
West Java 16 60 28 90
East Java 15 75 24 60
West Nusa Tenggara
12 45 16 60
South Kalimantan 17 50 21 120
All Provinces 15 75 22 120
Approximately 72% of PKH beneficiary’s children go to school on foot, and 17% by
bicycle. The remaining 11% uses other modes of transportation and pays a fee since
it is impossible to walk the distance, and sometimes it takes a long time to get to
school.
Table 7.3. Distribution of transportation modes from home to school
Means of transportation DKI West
Java
East
Java
West Nusa
Tenggara
South
Kalimantan
Total
N 261 505 406 514 451 2137
On foot 69.7 74.5 47.0 89.5 73.2 72.0
Own bicycle 7.3 14.5 45.6 0.0 22.4 17.7
Four-wheel vehicle 19.5 9.3 4.2 0.8 0.9 5.8
Rented motorcycle plus rider
0.0 0.8 0.5 8.4 0.0 2.3
Rented bicycle plus rider 1.9 0.2 0.0 0.8 0.0 0.5
Take a hitch hike 0.0 0.6 0.7 0.2 0.2 0.4
Shuttle service 0.4 0.2 0.7 0.2 0.4 0.4
Others 0.4 0.0 0.7 0.0 0.9 0.4
Ship without motor 0.0 0.0 0.2 0.0 0.9 0.2
Motorboat 0.0 0.0 0.0 0.0 1.1 0.2
Three-wheel vehicle 0.8 0.0 0.2 0.0 0.0 0.1
Carriage 0.0 0.0 0.0 0.2 0.0 0.0

62
Those who used transportation services spent an average of Rp. 2,400 one way. This
means that in one month (24 school days), one student spent an average of Rp
50,000 to Rp 60,000. Some teachers reported cases of students who had to walk
quite far. The challenging geographical condition made them tired when they arrived
at school.
Table 7.4. Transportation Fee from Home to School
Province
% of transportatio
n fee Mean transportation fee (Rp)
Maximum transportation fee
(Rp)
DKI Jakarta 27.7 1,754
7,000
West Java 13.9 1,938
5,000
East Java 5.0 2,450
10,000
West Nusa tenggara 12.9 3,451
5,000
South Kalimantan 3.7 2,818
5,000
All Provinces 11.5 2,376
10,000
Note : - Data from informants who spent transportation fee
Difficult access to school was found in some areas with challenging topography (hilly,
river, damaged infrastructure) and spread out residential area such as in South
Kalimantan, West Nusa Tenggara, and West Java. The distance from home to school
is actually not far, but the condition prolongs travel time.
“Loksado sub district is the farthest and most difficult for spot check. The distance to
the sub district center approximately 35 km, that is from Kandangan city to Loksado,
with a lot of slopes and sharp turns. Not to mention going into selected villages for
spot check" (PKH Spot Check Field Coordinator, HSS district).
7.1.2. Tuition Fee
Students from PKH beneficiary family should get scholarship. However, spot check
found only one out of six PKH beneficiary’s children received scholarships. On the
other hand, about 11 percent of beneficiary’s children reported using PKH funds to

63
pay tuition fees. According to the Law of the National Education System, the Central
and Local Governments should ensure provision of compulsory education for at least
primary level without charging tuition fees.
Table 7.5. Percentage of PKH beneficiary’s school-age children who had scholarship and paid tuition fee
DKI Jakarta West Java East Java West Nusa
Tenggara South
Kalimantan Total
Sample (n) 200 400 401 400 392 1972
Received scholarship 6.5 5.3 13.1 37.0 8.4 15.2
Paid tuition fee 5.9 11.5 24.5 2.6 34.2 10.8
7.1.3 Quality of education services
Basic education services are adequate in quantity, but they do not meet national
quality standards.
A. Adequacy of Teachers
Number of teachers in sampled provinces varied in terms of school subjects and
types. For example, elementary schools/MIs use class and special subject (specifically
for Religion and PE subjects) teacher system, so ideally every school has one teacher
for one learning group (class as a learning unit), plus two teachers for special
subjects. If a school has six learning groups, ideally the school should have eight
teachers, incorporating six teachers for each class, plus 2 (two) for special subjects
(Religion and PE). In the spot check, adequacy of teachers in elementary schools/MIs
was measured by the ratio of number of teachers per learning group. If this ratio is
greater than one the adequacy of teachers is considered sufficient, and if less than
one, it is insufficient.
In the mean time, the system in junior high schools/MTs uses teacher for special
subjects. According to the National Education Standards, required number of
teachers is calculated per school subject, using the following formula: "the number
of hours for particular subject per week (SKS) multiplied by the number of learning
groups, divided by number of teaching session (24 hours)." If one junior high school
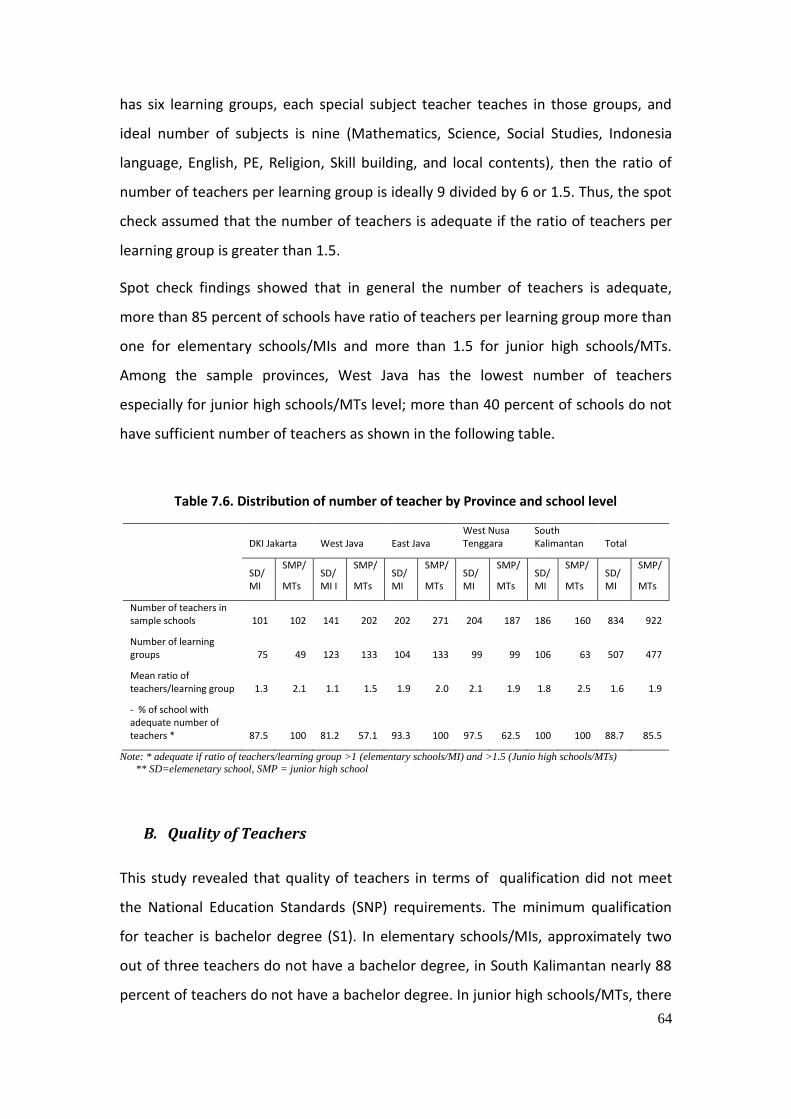
64
has six learning groups, each special subject teacher teaches in those groups, and
ideal number of subjects is nine (Mathematics, Science, Social Studies, Indonesia
language, English, PE, Religion, Skill building, and local contents), then the ratio of
number of teachers per learning group is ideally 9 divided by 6 or 1.5. Thus, the spot
check assumed that the number of teachers is adequate if the ratio of teachers per
learning group is greater than 1.5.
Spot check findings showed that in general the number of teachers is adequate,
more than 85 percent of schools have ratio of teachers per learning group more than
one for elementary schools/MIs and more than 1.5 for junior high schools/MTs.
Among the sample provinces, West Java has the lowest number of teachers
especially for junior high schools/MTs level; more than 40 percent of schools do not
have sufficient number of teachers as shown in the following table.
Table 7.6. Distribution of number of teacher by Province and school level
DKI Jakarta West Java East Java West Nusa Tenggara
South Kalimantan Total
SD/ MI
SMP/
MTs SD/ MI I
SMP/
MTs SD/ MI
SMP/
MTs SD/ MI
SMP/
MTs SD/ MI
SMP/
MTs SD/ MI
SMP/
MTs
Number of teachers in sample schools 101 102 141 202 202 271 204 187 186 160 834 922
Number of learning groups 75 49 123 133 104 133 99 99 106 63 507 477
Mean ratio of teachers/learning group 1.3 2.1 1.1 1.5 1.9 2.0 2.1 1.9 1.8 2.5 1.6 1.9
- % of school with adequate number of teachers * 87.5 100 81.2 57.1 93.3 100 97.5 62.5 100 100 88.7 85.5
Note: * adequate if ratio of teachers/learning group >1 (elementary schools/MI) and >1.5 (Junio high schools/MTs)
** SD=elemenetary school, SMP = junior high school
B. Quality of Teachers
This study revealed that quality of teachers in terms of qualification did not meet
the National Education Standards (SNP) requirements. The minimum qualification
for teacher is bachelor degree (S1). In elementary schools/MIs, approximately two
out of three teachers do not have a bachelor degree, in South Kalimantan nearly 88
percent of teachers do not have a bachelor degree. In junior high schools/MTs, there

65
are still 17 percent of teachers who do not have a bachelor degree, and South
Kalimantan province ranked the lowest with proportion of teachers who had
bachelor degree only 40 percent.
Table 7.7. Distribution of teachers who meet quality standard by province and school levels
Province Elementary schools/MI Junior high schools/MTs
Number of teacher in sample schools
% of teacher without bachelor degree
Number of teacher in sample schools
% of teacher without bachelor degree
DKI Jakarta 101 60.4 102 17.6
West Java 141 54.6 202 7.9
East Java 202 49.5 271 5.5
West Nusa Tenggara
204 70.1 187 23.5
South Kalimantan
186 87.6 160 40.0
Total 834 65.2 922 17.0
C. Condition of Facilities-Infrastructure
In terms of facilities-infrastructure, the National Education Standards require one
learning group to occupy one classroom, with the maximum number of students per
learning group is 28 for elementary schools/MIs, and 32 for junior high schools/MTs.
Spot check showed that not all schools meet these standards. At elementary
school/MI level approximately one out of five schools did not meet the standard
ratio of total learning group/classroom, and junior high school/MT level
approximately 6 percent of schools did not meet this standard.
In terms of ratio of students/learning group, approximately two out of five
elementary schools/MIs did not meet the standard, while the proportion of junior
high schools/MTs that did not meet the standard is two-thirds as listed in the table
below.

66
Table 7.8. Ratio of learning group per classrooms and number of students per learning group
Province DKI Jakarta
West
Java
East
Java West Nusa Tenggara
South Kalimantan Total
School level SD/MI
SMP/
MTs SD/ MI
SMP/
MTs SD/MI
SMP/
MTs SD/MI
SMP/
MTs SD/MI
SMP/
MTs SD/ MI
SMP/
MTs
Number of classroom in sample schools 68 47 105 133 103 133 96 94 103 63 475 470
Number of learning group 75 49 123 133 104 133 99 99 106 63 507 477
Number of students 2.712 1.878 3.990 5.360 2.082 4.518 2.603 3.502 2.182 1.927 13.569 1.7185
Mean ratio of learning groups/classrooms 1.1 1.0 1.2 1.0 1.0 1.0 1.0 1.1 1.0 1.0 1.1 1.0
- % of schools that did not meet classroom ratio 62.5 25.0 37.5 0.0 6.7 0.0 6.3 12.5 12.5 0.0 21.1 5.7
Mean number of students per learning group 36 38 32 40 20 34 26 35 21 31 27 36
- % of schools that did not meet number of students 75.0 100.0 81.3 85.7 13.3 87.5 43.8 62.6 18.8 25.0 43.7 68.6
Other than classroom, the National Education Standards also require that every
elementary and junior high schools provide science laboratory, library, principal's
office, teachers’ room, teachers’ toilet, students’ toilet, playground/sport area,
electricity, and clean water. Survey showed that not all schools met these standards.
At elementary school level, less than 5 percent of schools had nine of the required
facilities-infrastructure. The condition of junior high school/MTs is relatively better,
with approximately two out of three schools had nine of the required facilities-
infrastructure. Facilities-infrastructure that most schools did not have was science
Lab. Only six percent of elementary schools/MIs, and 89 percent of junior high
schools/MTs had it as listed in the following table.

67
Table 7.9. Percentage of facility-infrastructure at schools
Province DKI Jakarta West Java East Java
West
Nusa Tenggara
South
Kalimantan Total
School level SD/ MI
SMP/
MTs SD/ MI
SMP/
MTs SD/ MI
SMP/
MTs SD/ MI
SMP/
MTs SD/ MI
SMP/
MTs SD/ MI
SMP/
MTs
Science Lab 25.0 100.0 0.0 71.4 6.7 100.0 0.0 87.5 6.3 87.5 5.7 88.6
Library 37.5 100.0 37.5 100.0 53.3 100.0 53.3 75.0 62.5 100.0 50.0 94.1
Principal's office 100.0 100.0 46.7 100.0 73.3 100.0 100.0 100.0 93.8 87.5 81.2 97.1
Teachers’ room 87.5 100.0 73.3 100.0 93.3 100.0 53.3 87.5 100.0 100.0 81.2 97.1
Playground/sport area 87.5 100.0 87.5 85.7 80.0 100.0 66.7 87.5 93.8 100.0 82.9 94.3
Teachers’ toilet 87.5 100.0 75.0 100.0 73.3 100.0 93.3 100.0 93.8 87.5 84.3 97.1
Students’ toilet 75.0 100.0 93.8 100.0 93.3 100.0 100.0 87.5 93.8 100.0 92.9 97.1
Clean water 100.0 100.0 93.8 85.7 80.0 100.0 80.0 75.0 87.5 87.5 87.1 88.6
Electricity 100.0 100.0 87.5 100.0 100.0 100.0 80.0 100.0 93.8 100.0 91.4 100.0
% of realization of 9 facilities-infrastructure 77.8 100.0 65.3 92.1 72.6 100.0 69.6 88.9 80.6 94.4 72.7 94.6
% of schools that owned 9 facilities-infrastructure 12.5 100.0 0.0 57.1 6.7 100.0 0.0 37.5 6.3 62.5 4.3 68.6

68
7.2 PROVISION AND QUALITY OF HEALTH SERVICES
Provision of health services for PKH beneficiaries is expected to be easily accessible
and able to meet minimum service standards as required by the PKH health services
operational guidelines. In fact, health service delivery is still facing many challenges
including issues of distribution and quality of providers, adequacy of drugs and
vaccine, availability of health service supporting materials, and adequacy of facilities
and infrastructure.
7.2.1 Access to health services
In some areas, health facilities (puskesmas) are far or difficult to reach. This
condition makes the beneficiaries want to have more puskesmas. Currently, they
often go to village midwife for mild illnesses because the puskesmas is far.
“Well, puskesmas is far. If somebody is ill, go to a midwife. But if the disease is
severe, we have to go there (puskesmas).” (Beneficiary, Subang, West Java)
“There should be more health facilities to cover more community members.”
Woman beneficiary, Bima, West Nusa Tenggara)
“The expectation is to have an accessible health facility in terms of distance.” (PKH
beneficiary, Subang, West Java)
In some districts, many villages do not have a midwife. Most midwives live in the
capital of the sub district. For example, there is a complaint that a village midwife in
South Kalimantan does not live in her post, but in a different sub district. Thus, PKH
beneficiary should go to the other sub district for delivery.
"For health service, we have to admit that the number of midwives is inadequate.
Out of 168 villages, approximately 60 villages do not have a midwife. It is expected
that by 2011 all villages have a midwife. Another issue is the midwife does not live
in her post (in the village where s/he works). Then the number of Polindes is only 73
compared to 168 villages." (In-depth with District Health Office, West Nusa
Tenggara)
“For village midwife who does not live in the village, very poor woman should go to
another sub district for delivery.” (facilitator, Banjar – South Kalimantan)

69
7.2.2 Health Service Quality
A. Availability of health personnel in the health facilities
Doctors, nurses and village midwives are available in all sample puskesmas and its
network for the Spot Check. Other providers, including dentists, dental nurses,
midwives, public health officer, non-nursing paramedics, nutritionist /nutrition
assistant, pharmacist / assistant are not available in some puskesmas in East Java
and West Nusa Tenggara.
Table 7.10. Availability of Personnel in the Puskesmas by Type and Province (%)
Type of expertise DKI Jakarta
West Java East Java South Kalimantan
West Nusa Tenggara
Total
General practitioners 100.0 100.0 100.0 100.0 100.0 100.0
Dentists 100.0 100.0 100.0 100.0 87.5 97.2
Nurses/Orderlies 100.0 100.0 100.0 100.0 100.0 100.0
Dental nurses 100.0 100.0 75.0 100.0 100.0 94.4
Midwives 100.0 100.0 100.0 100.0 87.5 97.2
Village midwives - 100.0 100.0 100.0 100.0 100.0
Public health officer 100.0 100.0 50.0 100.0 100.0 89.1
Non-nursing paramedics 100.0 100.0 75.0 100.0 100.0 94.5
Nutritionist / nutrition assistant 100.0 100.0 62.5 100.0 100.0 91.7
Pharmacist / assistant 100.0 100.0 62.5 100.0 91.5 89.1
Administrative staff 100.0 100.0 100.0 100.0 87.5 97.2
Other health personnel 100.0 100.0 75.0 100.0 62.5 86.1
Cleaning service/drivers/ night guard 100.0 100.0 87.5 100.0 87.5 94. 6
Other staff 100.0 12.5 75.0 100.0 12.5 75.0
Most puskesmas provide health services needed by PKH beneficiaries, including
antenatal care by midwife and immunization services for infants and children.
Detailed distribution of health service provision by Puskesmas is listed in the
following table:

70
Table 7.11. Provision of Puskesmas Services by Provinces (%)
Type of Services DKI West Java
East Java South Kalimantan
West Nusa Tenggara
Total
Number of Puskesmas 4 8 8 8 8 36
Antenatal and delivery care
% of facilities providing Tetanus Toxoid Immunization for pregnant women
100.0 100 100.0 100.0 100.0 100
% of midwives providing antenatal care
100.0 100.0 100.0 87.5 100.0 97.2
% of doctors providing antenatal care
25.0 62.5 62.5 62.5 87.5 63.9
% of midwives providing delivery service
25.0 87.5 75.0 100.0 75.0 77.8
% of doctors providing delivery service
0.0 25.0 25.0 25.0 37.5 25.0
% of availability of labor and delivery room
25.0 75.0 50.0 100.0 37.5 61.1
Infant and child health services
% of facilities providing BCG, DPT, anti polio, measles, DPT Hep B combo immunization
100.0 100.0 100.0 100.0 100.0 100
% of facilities providing Hepatitis B immunization for under-five children
75.0 100.0 100.0 87.5 100.0 94.4
In-patient care
% of facilities providing in-patient care
25.0 50.0 37.5 87.5 50.0 52.8
Most medical equipment required for ANC and delivery care is available at the
puskesmas, except forceps and incubators. This spot check revealed that puskesmas
in South Kalimantan had morecomplete medical equipments (at least they have
vaginal speculum, uterine sound, straight and curved clamps, and scale). Health
personnel conveyed the information that puskesmas does not have 100% of
equipment because puskesmas does not provide management for delivery with
complications. If there are complications, they refer to a higher facility.

71
Table 7.12. Percentage of Puskesmas with ANC or Delivery Service Equipment by Province
Name of equipment DKI Jakarta
West Java
East Java
South Kalimantan
West Nusa Tenggara
Total
N 4 8 8 8 8 36
a. Hb Meter (HB Sahli Set)
75 87.5 100 87.5 100 91.7
b. Forceps 0 37.5 50 50 50 41.7
c. Vaginal Speculum 100 87.5 87.5 100 100 94.4
d. Tenaculum 75 62.5 75 100 75 77.8
e. Uterine sound 50 87.5 100 100 87.5 88.9
f. Gynecology bed 75 100 100 100 87.5 94.4
g. Straight and curved clamps
100 100 100 100 87.5 97.2
h. Oxygen tank 50 87.5 100 62.5 75 77.8
I. Incubator 25 50 37.5 75 25 44.4
j. Scale 75 100 100 100 87.5 94.4
k. Thermosk/ Vaccine Carrier
100 100 100 87.5 100 97.2
Complete ANC/ delivery care equipment
25 62.5 75 100 75 72.2
Vaccines for immunization are available at all puskesmas visited, except in East Java
where 12.5% of puskesmas didnot have complete vaccines stock, including BCG, DPT
and Hepatitis B or DPT Hepatitis Combo, Polio, and Measles. In West Java, half of
sample puskesmas during spot check had stock out of BCG vaccine for the last one
year.

72
Table 7.13. Percentage of Puskesmas that Had Vaccine Stock Out in the Last One Year by Province
Province DKI Jakarta
West Java East Java South Kalimantan
West Nusa Tenggara
Total
N 4 8 8 8 8 36
Vitamin A 0 0 28.6 0 0 5.7
BCG Vaccine 0 50 37.5 25 37.5 33.3
DPT 0 0 33.3 25 0 12.1
DPT Hep B Combo 0 12.5 12.5 12.5 12.5 11.1
Polio 0 12.5 12.5 0 12.5 8.3
Hepatitis B 0 0 25 12.5 12.5 11.1
Measles 0 12.5 12.5 0 0 5.6
Tetanus Toxoid 50 25 12.5 0 0 13.9
However, health personnel did not consider drug or vaccine stock-out as a problem,
as reflected in informants statement in West Nusa Tenggara.
“There was no significant obstacles so far, it was only about drugs availability"(The
Head of Puskesmas, Bima - NTB)
“At the time of vaccination and vitamin distribution, we did not have difficulties, but
when we came for treatment to the puskesmas, the services were not satisfactory.
Often there was shortage or no drugs at all, no orderlies .... "(Woman PKH
beneficiary, Bima NTB)
B. Vaccine storage facilities in the Puskesmas
Vaccine storage facilities are considered adequate if the puskesmas at least stored
their vaccines in a special box for cooling vaccine or in the freezer of a two-door
refrigerator, with one special door for the freezer. However, if specified by the
feasibility of storage facilities, Spot Check revealed that there was one puskesmas in
East Java that relied on one-door refrigerator to store vaccines. The ability of a single
door refrigerator to preserve the entire vaccine supply was not sufficient.

73
Table 7.14. Percentage of Puskesmas by Drugs and Vaccines Storage
DKI Jakarta
West Java
East Java
South Kalimantan
West Nusa Tenggara
Total
N 4 8 8 8 8 36
Cold chain/specific for vaccine
50,0 100,0 87,5 50,0 87,5 77,8
In the freezer (2-door refrigerator)
75,0 62,5 0,0 75,0 37,5 47,2
On the upper cabinet of the refrigerator (1-door refrigerator)
0,0 50,0 12,5 12,5 12,5 19,4
Others:
Cool pack 0,0 0,0 0,0 0,0 12,5 2,8
Small thermosk 0,0 0,0 0,0 0,0 12,5 2,8
C. Availability of supporting materials for services in the Puskesmas and
its network
Most Puskesmas have supporting materials for health services in line with PKH
operational guidelines. However, only three out of four Puskesmas have adequate
materials to support health services, including maternal cohort log book, KMS, and
immunization / MCH book. In East Java, the percentage of Puskesmas with complete
supporting materials for services is lower than the four other provinces.

74
Table 7.15. Availability of Supporting mmaterials for Services in Puskesmas
Province DKI
Jakarta West Java East Java South
Kalimantan West Nusa Tenggara Total
N 4 8 8 8 8 36
a. Maternal cohort log book 100.0 100.0 100.0 100.0 100.0 100.0
b. KMS (Health card) 75.0 75.0 62.5 100.0 75.0 77.8
c. Immunization / MCH book 100.0 100.0 87.5 100.0 100.0 97.1
d. Log book for weighing 100.0 87.5 87.5 100.0 100.0 94.4
e. Midwife’s kit 75.0 100.0 87.5 87.5 100.0 91.7
f. Posyandu kit 50.0 87.5 87.5 71.4 87.5 80.0
g. Antropomethric kit 0.0 75.0 87.5 100.0 75.0 74.3
Materials are complete 75.0 75.0 62.5 87.5 75.0 75.0
Qualitative study showed the case of inadequate supporting materials for services in
Posyandu. The available scale in Posyandu was the steelyard with a cloth on one
side, causing the children refused to be on it. Another case was the unavailability of
KMS in the posyandu, that made the community pay for xeroxing. The limited
facilities and infrastructure were indeed the barriers for providing quality health
services.
“There were under-five who are already big, 4 years, they were ashamed to be
weighed, because the Posyandu use steelyard for children." (Facilitators, Dompu
NTB).
“The village midwife did not have enough KMS in posyandu, there, when I told the
mothers to collect the KMS, they were confused and asked the midwife. In the end,
they just wrote it down and copied it from the midwife. ,A bad thing is that there
was a fee, they were asked money for xeroxingthey said." (Facilitator, Subang, West
Java)
“The barriers that we feel here is the limited equipment and infrastructure, nothing
else I think." (Village midwife, 34 years, Bima NTB)
“I think the barrier is still associated with the absence of complete equipment and
infrastructure for providing services, such as inadequate number of rooms, the
health instruments here are also still minimal. Maybe those are the barriers for us
and almost every Pustu / Polindes in this area." (the head of pustu, 30 years, Bima
NTB)

75
D. Providers’ compliance to health protocols
Most puskesmas have made 2 (two) postpartum visits within 28 days of delivery, but
in two provinces, half of the puskesmas do not do postpartum visits as required by
the health service protocols.
Table 7. 16. Percentage of Puskesmas that Did Postpartum Visits as Required by the Health Service Protocols
DKI Jakarta
West Java
East Java
South Kalimantan
West Nusa Tenggara Total
N 4 8 8 8 8 36
Meet the protocols* 50.0 100.0 50.0 100.0 100.0 83.3
Note*: protocols on postpartum care requires two visits to post partum mother within 28 days after delivery.
E. Items in antenatal care
ANC is considered complete if a pregnant woman obtains the following services:
weighing, height measurement, blood pressure measurement, blood test, abdominal
height measurement, fetal heart rate examinaton, vaginal examination, pelvis
measurement, and urine test. Overall, only a third of pregnant women who had ANC
reported to obtain full ANC services, with the highest frequency in West Nusa
Tenggara (44%) and the lowest in South Kalimantan (13%), while in other provinces it
ranges between 25-33%.
F. Complete information for pregnant women during ANC visit
Information is considered complete if it includes nutritious food for pregnant
women, recommendation to deliver in a health facility or hospital, and signs of
pregnancy complications. Only half of these pregnant women received complete
medical information during their ANC visit. In West Tenggara Barat, only one out of
five women received complete health information from health providers, while in
other provinces it is only 50-65%.
76
G. Fees at the Puskesmas
Although the puskesmas should not charge at all to PKH beneficiaries, in fact some of
them still pay. This finding is expressed by informants among facilitators and the
women PKH beneficiaries.
"These last few months we went to the puskesmas and stayed (for in-patient care)
and still had to pay because we did not have Jamkesmas, only have a PKH card, in
the end we paid Rp 150,000.” (Woman beneficiary, Bima NTB)
"(Services in the puskesmas) some are free, some are not free." (Woman PKH
beneficiary, West Java)
"Well, only in health (there are difficulties). Say a woman is ill ... goes to a
puskesmas, but she still has to pay. Cannot use the PKH card, not also KTM ...
(Facillitator, Subang, West Java)
"I once went to puskesmas West Dompu, I used the PKH card, but was told to use
Jamkesmas card, they said there was no definite place to claim for PKH, I reported
it to the facilitator, and the facilitator already visited the puskesmas, but still cannot,
for the time being just use the Jamkesmas." (FGD with woman beneficiaries, Dompu
district)
"There are problems in health, like when we go to a health facility (general hospital), we still have to pay although the commitment mentions it is free. It happened and the question goes to the quota in the Subang budget. The quota was only for a few thousand people. So if more than that, obviously it is impossible. The expectation of the RTSMs who are PKH beneficiaries is that the card should also be usable for medical treatment." (facilitator, Subang, West Java).
There were also facilitators and beneficiaries who did not understand that PKH
beneficiaries should not be charged at the puskesmas.
“Puskesmas has relatively easy process and no problem. In Puskesmas, payment is
just at registration only. (facilitator, Subang, West Java).
“It’s easy (at Puskesmas), not difficult, inexpensive, too. (PKH beneficiaries, Subang)
However, if the question is asked to the puskesmas, they explained that the
treatment was more because of the ignorance whether the patients were PKH
beneficiaries or not.

77
"... There are PKH beneficiaries who received delivery services, but still paid for the
cost of the delivery. The efforts to contact the relevant provider were done and the
answer was because the patient used certain (personal) drugs. (Facilitator, Dompu
NTB)
"Basically, puskesmas is always ready if it is related to standard services, it's just that
we were not able to identify whether the patients were PKH beneficiaries or not,
because the patient did not show the identity. Pustu and Posyandu may know more
about this, the report from a midwife’s log book showed that there were some PKH
beneficiaries who used the card to obtain health services. "(Head of Puskesmas,
Dompu NTB)
"There were only one or two cases for things like that (payment). That was because
the provider did not know that s/he was a PKH beneficiary and the wrong thing was
that s/he did not show the PKH card. So, it is fair that as a provider, already provided
the services, especially a village midwife. For puskesmas, if someone does not pay, it
is okay , no problem. But if it is a delivery, the midwife felt disadvantaged, same
thing in a hospital. "(The District Health Office, West Java)
Actually PKH is inseparable from Jamkesmas. RTSM as PKH beneficiary should also
receive Jamkesmas. Some officials from the health sector who are also informants
know about this.
"PKH beneficiaries should immediately get Jamkesmas card. So PKH data should
immediately be handed over to PT. Askes, and then to MOH. Because Jamkesmas
and PKH are interrelated ... "(district Health Office, West Java)
H. Rejection and Delay in Health Service Provision
Qualitative study found several cases of rejections when PKH beneficiaries sought
health services. In South Kalimantan, a Posyandu did not provide services to a PKH
beneficiarys’ child because the child was considered too old and becase the child
was a PKH beneficiary.
"The child is 4 years old, because s/he is big and known as a PKH beneficiary, then
s/he do not get the services. The midwife asked them to go to the Puskesmas."
(Facilitator, Banjar - South Kalimantan)
"If we go for treatment, though we have a PKH card, were are not accepted or
difficult to get services, we still have to pay for the medical expenses, but if there is a

78
Jamkesmas card, it is free of charge." (FGD woman beneficiary, Dompu District, West
Nusa Tenggara)
"... I was once rejected by the puskesmas. At that time somebody said, ma’am this is
not valid yet, so I did it as usual, pay for it. I did say that I had a PKH card, so it was a
recommendation that if anyone is ill, if we have this card, it is also possible, that was
why I had the courage to ask for it .. "(PKH beneficiary, Tanjung Priok sub district,
North Jakarta)
"Once my child was sick and was rejected (at puskesmas). In the end I went to Koja
(Public Hospital)" (PKH beneficiary, Koja sub district, North Jakarta)
"There are certain hospitals that made it difficult for PKH beneficiaries. Because
there is one hospital that always thought what is this PKH. Anyway they tried to
make it very complicated. One time, there was one case when a family member died
at the hospital lobby, s/he knew s/he brought the PKH card, also family card, there
should be a letter from the RT RW that s/he could not have at that time because s/he
was really sick, and the hospital finally washed their hands and s/he died in the
hospital. "(Facilitator, Jakarta).
There were cases when a puskesmas in a kelurahan in DKI Jakarta tried to delay
services for a sick PKH beneficiary, but the problem was then discussed by the
facilitator with the puskesmas sub district.
"Usually when a PKH beneficiary came, the ones who received services first were
the ones who pay. PKH will get them later, so at that time s/he slammed the card,
the PKH card. So he complained to my house because her/his child had a very high
fever.” (Facilitator, Jakarta).
In regards to delivery care, puskesmas does not reject the delivery. But if there are
indications that there will be delivery complications, they will refer to hospital.
"When there are indication that a woman will deliver normally, we accept her, but if
it is not possible for a normal birth, we just gave a referral letter to hospital," (head
of puskemas, DKI Jakarta)
Although cases that discriminated PKH beneficiaries were found, several informants
among health providers expressed their readiness to provide services to PKH’s
RTSMs. Basically they do not differentiate the services and there are also puskesmas
that understand the benefits of PKH for RTSMs.
79
"We are ready to provide services to PKH beneficiaries, also for PKH visits. We also
treat them the same with regular patient’s visit, we do not discriminate PKH and
non-PKH patients. "(Puskesmas, Jakarta)
".. We (Puskesmas) are always ready. Puskesmas has no problem, the important
thing is that when they come, they show the card. "(Puskesmas sub district, Jakarta)
“Well, it is the same. There is no difference between the one who has or does not have (PKH). "(Posyandu Kader, Jakarta). "We do not differentiate services for patients covered by any program, as long as the illness can be managed by the puskesmas equipment, they will certainly receive services properly. But we never know whether these patients were PKH beneficiaries or not, because most community members use Jamkesmas to obtain services."(Head of Puskesmas, Dompu NTB)
“Even from then, before PKH exists, we have Jamkesmas ... well, consider them
equal, no different services. Only, if there is distinction, for families who could afford
it ... they’re not very detailed in the bookkeeping. In a Jamkesmas family, PKH ... we
have to be more detail, the data will be different .... "(Village midwife, Subang, West
Java).
"PKH is also one of the priority areas in health. So I think, it will be very good to
collaborate with puskesmas that have Jamkesmas program and their drugs are
provided for free. But to come to such puskesmas will cost the person for
transportation. There, that cost might be filled in by PKH. So, they complement each
other, so the goal to give access to services for the poor community can be realized.
"(Puskesmas doctor, Subang, West Java)

80
CHAPTER 8 COMPLAINT RESOLUTION SYSTEM
Community Complaint Unit (Sistem Pengaduan Masyarakat or SPM) of Conditional
Cash Transfer (Program Keluarga Harapan or PKH) must be conducted by the Central
UPPKH, Municipal/District UPPKH, as well as PKH Facilitator. The objective of SPM is
to facilitate the PKH beneficiaries, the general public, NGOs, and the government,
both central and regional, in handling complaints related to PKH, and carrying out
the necessary solutions. Complaints may be done directly (through Mother Leaders,
Facilitators, or directly to UPPKH Municipal/District Office), or indirectly (through
other sources outside PKH, such as the mass media, research findings, Legislative
Body, etc).
The system of managing such community complaints is composed of several tiers,
starting from the Mother Leaders, Facilitators, Municipal/District UPPKH, Service
Provider, Municipal/District PKH Coordinating Teams, Provincial PKH Coordinating
Teams, Central UPPKH, up to the Central Technical Coordinating Team. Duration of
management of a complaint is 26 days at most, from documentation, analysis,
clarification of complaints, to informing the complainer the results of the
investigation.
Facilitators are to submit monthly reports on all complaints and their
resolution/management to Municipal/District UPPKH, which then are to continue
the report to the service providers, Municipal/District PKH Coordinating Teams, and
Central UPPKH. The results of managed complaints and reports are then to be
reported by the Central UPPKH to the Central Technical Coordinating Team.
This spot-check study concludes that the complaint resolution system has been
executed; nevertheless there are still some points which require mending. The facts
and findings of the complaint resolution system are as following.

81
8.1 BENEFICIARIES ARE NOT WELL-INFORMED ON HOW TO SUBMIT
COMPLAINTS
The percentage of beneficiaries who claimed to have been informed on how to
submit complaints varied, ranging from 20-30% in West Java, East Java, and South
Kalimantan, 50-60% in DKI Jakarta and West Nusa Tenggara (NTB). The total number
of beneficiaries who have ever submitted complaints were even smaller; only 6% of
total PKH beneficiaries, with the highest in Jakarta (16%) and the lowest in NTB
(2.3%).
Most complaints were related to payment issues, including inappropriate amount of
money received, delays, long queues, closed Post Office, or the slow processing by
the Post Office. Other types of complaints ever received have to do with services in
the health facilities, education facilities, and District UPPKH. Below is the detailed
description.
Of all 9 operators interviewed, only 7 confessed to having ever received forms for
complaints, mostly coming from the public, especially those who were not accepted
as beneficiaries. Of all 99 attendants interviewed, 69 confessed to having ever
received complaints from beneficiaries, mainly on payment issues, and from the
public who were not accepted as beneficiaries.
“Almost all forms for Complaint contain requests for becoming beneficiaries”.
(facilitator & operator of Situbondo District)
“Complaints (that we have received) are protests from thepoor community who were
not accepted as PKH beneficiaries, asking for the reasons for their exemption from
the program. However, after they were given explanations that the data comes from
BPS, they understood. So, there is no meaningful problem”. (Heads of Social Office,
Bima District)

82
Table 8.1. Percentage of types of complaints according to PKH beneficiaries
Type of complaint Jakarta
N=32
West Java
N=18
East Java
N=22
NTB
N=9
South Kalimantan
N=16
Total
N=97
Payment Delayed payment (%) 20.6 11.1 0 0 6.3 10.1
Long queues (%) 5.9 16.7 13.6 11.1 6.3 10.1
Inappropriate amount of money received (%)
41.2 22.2 36.4 33.3 12.5 31.3
Health facility Absent doctors/midwives (%)
0 0 0 22.2 0 2.0
Slow process by Puskesmas personnel (%)
0 5.6 0 0 6.3 2.0
Education facility
Absent teachers (%) 0 0 0 0 6.3 1.0
Slow work by teachers (%)
0 0 0 0 6.3 1.0
Substandard classroom/learning facilities (%)
0 0 0 11.1 0 1.0
PKH Office Closed office (%) 0 0 0 0 6.3 1.0
Absent officers (%) 0 0 0 22.2 0 2.0
Miscellaneous (%) 32.4 38.9 45.5 11.1 75.0 41.4
8.2 COMPLAINT MECHANISM IS NOT WELL RUNNING
Most PKH beneficiaries did not know about the presence of Community Complaint-
Management Unit (Unit Pengaduan Masyarakat or UPM). Of the respondents in the
study, only 13% of them were aware of UPM, consisting of 10% of PKH 2007
beneficiaries and 17% 2008 beneficiaries, with the highest percentage in NTB where
one third of respondents were aware of the presence of UPM. More than one third
of the respondents (35%) claimed to have been informed on how to submit
complaints, and its percentage is higher among those who participated since the
year 2008 than 2007 (43% to 29%, respectively). Among the 6% beneficiaries who
have ever submitted complaints, most of them submitted them directly to their
Operators/Facilitators, and some others through their Mother Leaders. Of all
respondent Facilititors, 68% confessed to having ever received complaints.
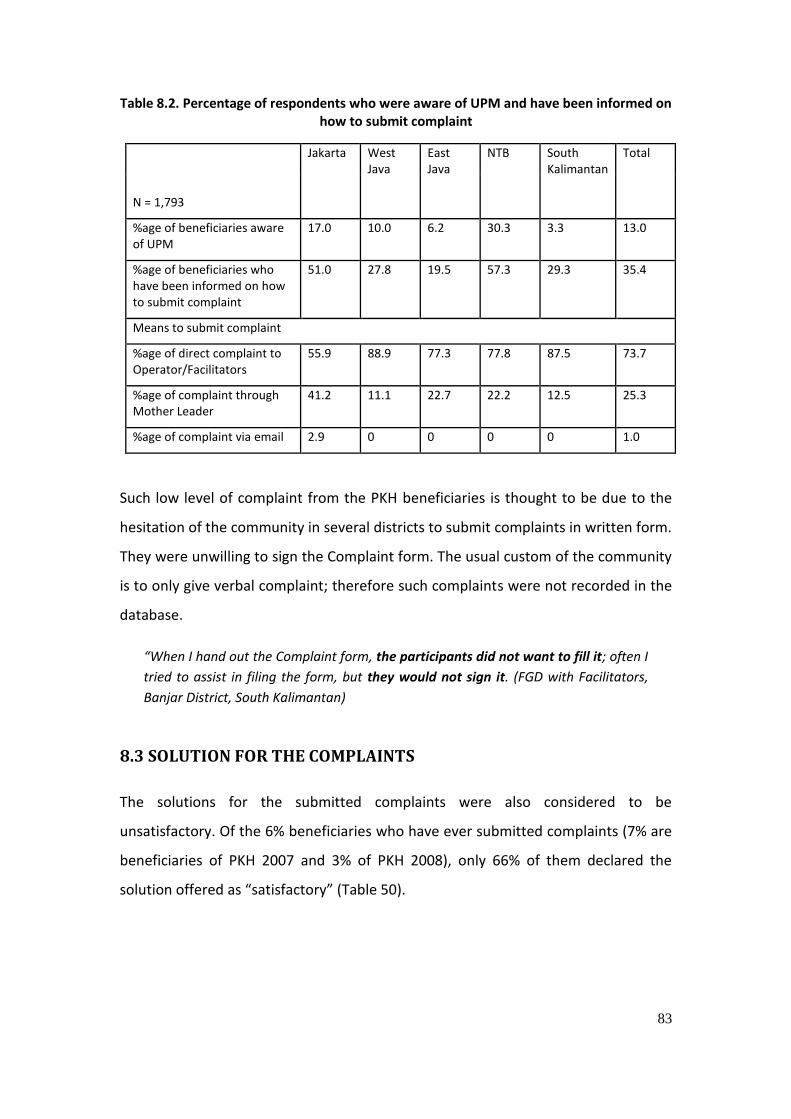
83
Table 8.2. Percentage of respondents who were aware of UPM and have been informed on how to submit complaint
N = 1,793
Jakarta West Java
East Java
NTB South Kalimantan
Total
%age of beneficiaries aware of UPM
17.0 10.0 6.2 30.3 3.3 13.0
%age of beneficiaries who have been informed on how to submit complaint
51.0 27.8 19.5 57.3 29.3 35.4
Means to submit complaint
%age of direct complaint to Operator/Facilitators
55.9 88.9 77.3 77.8 87.5 73.7
%age of complaint through Mother Leader
41.2 11.1 22.7 22.2 12.5 25.3
%age of complaint via email 2.9 0 0 0 0 1.0
Such low level of complaint from the PKH beneficiaries is thought to be due to the
hesitation of the community in several districts to submit complaints in written form.
They were unwilling to sign the Complaint form. The usual custom of the community
is to only give verbal complaint; therefore such complaints were not recorded in the
database.
“When I hand out the Complaint form, the participants did not want to fill it; often I
tried to assist in filing the form, but they would not sign it. (FGD with Facilitators,
Banjar District, South Kalimantan)
8.3 SOLUTION FOR THE COMPLAINTS
The solutions for the submitted complaints were also considered to be
unsatisfactory. Of the 6% beneficiaries who have ever submitted complaints (7% are
beneficiaries of PKH 2007 and 3% of PKH 2008), only 66% of them declared the
solution offered as “satisfactory” (Table 50).

84
Table 8.3. Percentage of beneficiaries who were offered solutions and who considered them to be satisfactory
N = 97
Jakarta West Java
East Java
NTB
South Kalimantan
Total
%age of beneficiaries who were offered solution for their complaints
58.8 72.2 72.7 66.7 87.5 69.7
%age of beneficiaries who considered the solution to be satisfactory
64.7 55.6 59.1 66.7 87.5 65.7
8.4 PROBLEMS ENCOUNTERED IN SUBMITTING COMPLAINTS
Several complaints went unresolved because the complaints did not reach the
central PKH office or the parties with appropriate authority to solve the issue. This is
brought about by, among others, the shortage of Complaint forms, which caused the
complaint processing from the beneficiaries or community to the district level to be
hindered.
”At present, and for quite a while now, there is no Complaint form; in the beginning
(of the program) in 2007 there were still Complaint forms (in stock)” (Post office,
Dauwan Sub-district, Subang District)
In addition only 7 operators claimed to have ever received Complaint form, and 5
who performed complaint entry process. Of the 5 operators who performed
complaint data-entry, 2 claimed the problem faced in the data-entry process is poor
performance of the application, and 1 operator faced electrical problem. It was also
found from interview with MIS (Management Information System) Central UPPKH
that complaints that were submitted to the complaint database generally were not
followed-up by the Central UPPKH.
“…there are so many non-participants who complained, asking why they were not
included to receive PKH funds, while they were more impoverished than those who
did receive the funds. We only could collect their complaints, write them down in
Complaint forms, and insert them into the online application. But we are not
aware of how the follow-up is; bottom line is we have reported (the complaints) to

85
the Central UPPKH”. (Indepth interview with Operators, Dompu District, West
Nusa Tenggara)
The problem mentioned above is caused by: (1) poor socialization of the UPM, (2)
the public perception that the government, as ruler, was so powerful that they were
afraid of the consequences, and (3) the growing perception among the public that
complaints are not followed-up.
If the roots of the problems are unsolved, they may bring about delayed
management of the program’s shortcomings that the improvement of quality of
service cannot take place.

86
CHAPTER 9 SOCIALIZATION, TRAINING, AND COORDINATION
Socialization defines as providing or sharing the information to all stakeholders
related to objectives, implementation and support needs in order to improve the
implementation of the Conditional Cash Transfer (CCT) program and considered as
part of national social security system. Meanwhile, the trainings conducted will
improve the understanding and skill of CCT responsible parties, managers and
implementing agencies so they are more competent in program management and
implementation. Coordination at all levels among responsible parties, managers and
implementers of the program is crucially needed to ensure program is being
implemented according to the national policy.
9.1 SOCIALIZATION
9.1.1 Ineffective socialization to other sectors
Socialization is one of program components which is not yet effectively executed.
Socialization has been conducted in each location but unfortunately no follow up
after that, the activity seems like ordinary meeting. To encourage more commitment
from related parties and to make socialization is more effective then a follow up
action is necessary to be done. For example, district UPPKH is encouraged to provide
routine progress update report to related parties on services have been provided to
beneficiaries, including inputs for program improvement. Therefore, sectors will be
taken into account and have active involvement in CCT program implementation and
finally they will contribute to successful implementation of the program.
“When CCT program was firstly launched, there was coordination system set up between cross sectors, at national and sub national level. Another system set up was cross sectoral coordination at sub national level, between sub nationals and between sub national and central. In the beginning of program implementation, there was misconception rose among people involved, they felt it is a burden for them. The

87
Ministry of Social Affairs thought they are the paymaster, not necessary to have close coordination with other sector. In fact, CCT is a cross program type, the measurable indicator is not only amount of money disbursed and distributed but it also measures the output indicator which shows sectoral coordination”. (Ministry of Health).
Ineffective socialization results on poor commitment from sector key person to
support CCT program. Some of the key persons have been exposed to socialization
but it was not comprehensively explained, or some of them have not yet been
attending any socialization session.
“Socialization was conducted 2 times since 2008 (2008 and June 2009) involving
CCT-related sectors in Banjar District including representative from District Health
Office. Unfortunately, there was no follow up coordination after meeting, to discuss
program implementation achievement. District Health Office thought the
socialization is not effective. Incomplete data found such as villages receiving CCT is
not well informed to District Health Office, very hard for the institution to monitor
those villages” (Banjar District Health Office, South Kalimantan).
“I just knew about CCT from you (red: interviewer)” (MoNE Office at Cirebon District)
"We knew about CCT socialization through District Education Office only, limited to
information saying that there will be CCT program, we really do not know about
program sustainalibility and run down. A lot of things we do not know yet about
this program. Schools were not involved in providing list of students eligible".
(Indepth interview to schools/Elementary School, Dompu District),
So many things we do not know about CCT, such as how is it related to and
differences with Jamkesmas, etc., to whom the CCT patient claimed when using the
card. Midwives had the same questions too when providing assistance to normal
delivery at Polindes or Puskesmas". (Indepth interview with Puskesmas staff, Bima
District).
”i was assigned to manage CCT program for the last 6 months, replacing previous
friend. Informant never had formal socialization on the program, but he had CCT-
related books from his colleague and some information searched from the internet.
Last month, informant become key speaker for Health CCT on CCT socialization for
sub district mayor (camat), district mayor (Kades/Lurah), supervisor and related
sectors” (Banjar District Health Office, South Kalimantan).
“I was just returned back to Education Office, previously I worked for government
tourism office, and before that, I worked as head of UPTD pendidikan kecamatan
(subdistrict education office). I knew more about CCT when I was the head of UPTD
pendidikan kecamatan in 2008 until early 2009. As institution, Education Office is

88
always invited to CCT socialization activity and sometimes different person coming
representing the institution”. (Banjar District Education Office, South Kalimantan).
Complaints on lack of CCT socialization also come from educational and health
facilities staff. In addition, less competent program management skill of the staff
causes barriers in conducting socialization. The absence of program quality control,
inadequate supervision and monitoring, no feedback from central/regional
coordinator on performance of operator or facilitator and frequent staff rotation
have worsen the situation.
“The main point during socialization is how information come to community
completely. The problem is the Ministry of Social Affairs does not have control on this
issue”. (National Planning and Development Board or Bappenas).
“Staff rotation become the challenge in socialization activity. Ministry of Social
Affairs since 2010 applies a rewuirement that regional coordinator should be from
related province. Recruitment of the coordinator is now open by the Ministry”. (The
Ministry of Social Affairs).
“Please check field coordinator availability, how many days he is in the filed and how
many days in Jakarta. He should be the leader and know real problem and program
achievement in the field. In terms of complaints management, does he know what
are the complaints and what to do with it? How will they understand all complaints if
they only 2-3 days in the field and 4 days in Jakarta?” (Bappenas).
"In 2009, Mr “T” become the Regional Coordinator, he came once to Dompu and
stay one day, and one day only in Bima too. I think it is because he is not from NTB
so monitoring and evaluation to Dompu is not yet enough’. (Indepth Interview to
Operator, Bima District)
"Lack of field monitoring and supervision, meanwhile the facilitators and operators
are ready to have performance evaluation, this should be conducted once in 3
months. If coordination and evaluation process is well conducted (attended by all
related sectors) there will be no problems such as special fee required for filling in
verification form, etc. Maybe it happens because of lack of fund ". (In depth Interview
with Operator, Dompu District).
"No field supervision and monev yet from regional office/central post office ". (In
depth Interview with staff at Dompu District Post Office)

89
9.1.2 Unclear Roles & Responsibilities for Sectors Implementing Socialization, Mainly Ministry of Communications and Information Technology (MCIT)
Socialization has been conducted in all study location. There are 2 out of 71 people
or 3% of facilitator who never attended socialization session, meanwhile all
operators attended the session. Based on information from operator and facilitator
who attended socialization session, the average number of socialization per district
per year is 7 times, and each socialization lasts for 1 day only. In North Jakarta (10%),
East Java (28%), and NTB (23%), most of socialization participants did not receive the
materials.
Among sectors or service delivery points, it can be seen that there is unclear job
distribution on who is taking role during socialization. The Ministry of Social Affairs
(MSA) thought socialization is the responsibility of the Ministry of Communications
and Information Technology (MCIT), and each sector responsible to share the
information within its department. Bappenas suggested to MCIT for not taking
central role in socialization, since in the past experience on cash transfer or Bantuan
Langsung Tunai (BLT) in 2005 its performance was not sufficient. But then MSA has
decided to ask MCIT to have bigger role in socialization.
“In the program design and manual in 2007, Bappenas wanted MSA to do
socialization because it has facilitator working with community. MCIT will do similar
thing at sub district level and upper level. But it happened reversely, MSA changed
the mechanism because it has more power to assign other sector. MCIT had a
mistake since beginning. Experience from BLT program in 2005, MCIT did not
socialize the program well. Bappenas had critized MCIT performance on this”.
(Bappenas)
“ Each department has responsibility to socialize the program within its
department. Meanwhile, RTSM of CCT beneficiaries will be done by facilitator.
There should be 1-2 persons who is consistently atetnding CCT coordination
meetings. It is expected that the socialization is continuosly conducted although
there is intensive staff rotation”. (The Ministry of Social Affairs)
“Job distribution among sectors have been clearly explained, program socialization
should be the responsibility of each sector, example PT Pos does cash transfer and
MCIT takes care of socialization-related issue. For community, socialization will be
done by facilitator. MCIT is the leading sector for socialization, community relations
at local government office specifically information division will do this at district

90
(depends on each district). Funding allocation for the activity is still centralized, on
MCIT”. (The Ministry of Social Affairs)
Internal program socialization has been implemented by UPPKH or MSA to
district/city UPPKH, mainly to operator and facilitator. Most of the time, the
operators and facilitators were attending socialization session from 2 different
institutions. District UPPKH executed most of socialization activities (51%), the least
is Local Planning and Development Board (8%).

91
Table 9.1. Percentage of Operator and Facilitator Who Ever Exposed to or Know About Socialization Activity by CCT Implementing Organization
Socialization conducted by
West Java North Jakarta
East Jakarta
South Kalimantan
NTB Total
N 19 10 18 6 26 79
National CCT Team 36,8 20,0 27,8 66,7 50,0 39,2
Provincial CCT Team 36,8 60,0 22,2 16,7 19,2 29,1
District/City CCT Team
42,1 40,0 55,6 83,3 50,0 50,6
MSA 15,8 30,0 22,2 19,2 19,0
Provincial office of Social Affairs
63,2 30,0 27,8 16,7 26,9 35,4
MCIT 10,5 22,2 7,7 10,1
Local planning and development board
5,3 5,6 16,7 11,5 7,6
Role of MCIT as the leading sector remains unseen. Only 10% of operator and
facilitator who know socialization was conducted by MCIT. In North Jakarta and
South Kalimantan, none of operator and facilitator mentioned the session was
organized by MCIT.
9.1.3 Unqualified socialization
Interview with operator and group discussion with facilitator revealed that
participants attending socialization meeting did not receive any written documents,
presented by incompetent person, limited time so some materials were not
explained, participants did not make report or share the information to other
colleagues, and no activity report from committee.
“Very limited time, other topics were not explained and discussed, the key person is
very busy, he only had 2 to 3 hours to explain, although we want this full day, we
have many questions to ask”. (Operator, Subang, West Java)
The above mentioned problems have caused CCT key points were still poorly and
incomprehensively understood by decision makers, they often create policy which
inhibits CCT implementation. Example, CCT beneficiaries are considered not eligible

92
or have right to be counted for other pro poor programs. This is an incorrect
understanding and will against government policy if applies.
“...Many School Principal did not know CCT Program …the school received
government money through BOS Program and other supports, once they know a
parent accepts CCT money then the chlid will be deleted from BOS’s recipient list.
The truth is that the CCT money is not for paying the school fee, it is for transport fee
for the student”. (Facilitator, North Jakarta)
Many facilitators found lack of socialization and coordination on CCT Program to
services delivery points in many places. This causes uneven understanding of the
program at that point. The situation reflects the imperfect socialization process at
the institution (service delivery points/educational facilities) up to service delivery
points and respondents admitted these facts.
"Education office has not yet optimally perform coordination or socialization tasks.
This condition results in poor management of CCT program by the schools, we hope
they pay attention to this better ". (FGD with Facilitators, Bima District)
“We do not understand some issues about CCT program, such as how is the relation
and difference with Jamkesmas, etc., where to claim when a patient uses CCT Card.
Similar issues happened to our friends, the midwives, who assisted deliveries in
Polindes or Puskesmas”. (Puskesmas, Bima)
Ineffective socialization has made sectors do not provide significant support,
including education office and health office, which are very important as institution
verifiying the CCT disbursement. Some sectors felt they were not involved on CCT
Program, therefore, they are reluctant to optimally support to and minimum self
belonging of the program.
”District Education Office of HSS (Diknas HSS) felt it never been involved to support
CCT Program. There should be a follow up from CCT responsible person in District
HSS explaining Education Office tasks and responsibilities. The institution does not
know what to do if students receiving CCT money or have to continue coordinating
schools under its responsibility area”. (Education Office, Hulu Sungai Selatan or HSS,
South Kalimantan)
"School staff never attended socialization, we get information on CCT from a
facilitator when we received a form sent by PT. POS Dompu. We do not know many

93
things such as: program model, working system and to whom we should responsible
". (In depth interview to school/MI, Dompu District).
“I or my institution never received any invitation to come to CCT program
socialization. But I know that program after a facilitator visited me asking to assist a
woman who is giving birth here”. (Pustu, Bima)
Understanding of CCT beneficiaries in terms of program design and rule need to be
improved. Only half of respondents said that they never had explanation on things
they should do as CCT beneficiaries. In terms of CCT program knowledge, those
recruited in 2008 has better understanding than those in 2007 for all knowledge
indicators (see table below). Respondents might have better capacity in memorizing
and understanding the things explained during socialization session. Regardless time,
this fact shows that refreshing sessions for improving pasticipants capacity was not
working. Role and function of facilitator to refresh participants’ knowledge is very
important when having group discussion.
Table 9.2. Percentage of respondents who ever received socialization materials
Materials
DKI
Jakarta
West
Java
East
Java
PKH
2007
NTB South
Kalimantan
CCT
2008
Total
Sample size (n) (200) (400) (401) 1001 (400) (392) 792 1793
Explanation on CCT 48.5 45.8 43.1 45.3 84.3 41.6 63.1 53.2
Beneficiaries
Requirements 43.0 48.5 37.7 43.1 83.3 39.3 61.5 51.2
Health-related
obligation 58.0 49.0 46.4 49.8 83.8 42.6 63.4 55.8
Education-related
obligation 61.0 50.0 52.1 53.0 83.5 44.4 64.1 57.9
Funding rights 44.5 40.8 33.7 38.7 76.8 37.0 57.1 46.8
Household
demographic update
report 59.5 41.5 39.7 44.4 78.3 36.0 57.3 50.1
Complaints
mechanism 42.0 30.5 23.9 30.2 54.0 21.7 38.0 33.6

94
Ineffective socialization is probably due to the following problems 1) role and
function of the Local Coordination Team on Poverty Alleviation or Tim Koordinasi
Pengentasan Kemiskinan Daerah (TKPKD) is not optimally underway. 2) Role of MSA
attn. Social Office as an activator is not yet optimum because it depends on MCIT for
program socialization 3) funding allocation for the activity is centralized at MCIT and
this is considered not effective. 4) socialization meeting is treated as an ordinary
meeting which is not important and does not need follow up.
Implications occur if the problems identified did not well taken care of, first, lack of
support from sector and its involvement for making CCT program implementation
successful. Second, program personnel and target community did not understand
program implementation.
9.2 TRAINING
All trainings were conducted in all locations, especially training for operator and
facilitator. Average number of trainings attended by operator and facilitator is 5
trainings, similar number applied on average number of trainings conducted by each
location, except North Jakarta (4 times). In the last 12 months, most of operator and
facilitator have been trained 3 times except in West Java and North Jakarta (2 times).
Training duration lasts for 3 days in the average. Two (2) % training participants said
they did not receive training materials from the last training they attended, mainly in
West Java and East Java.
CCT training is conducted mainly by the central UPPKH (61%) and province UPPKH
(18%). The training comprises : early education and training (Pendidikan dan
Pelatihan), national coordination meeting, technical assistance, and
enterpreneurship training. In West Java, International Labour Organization (ILO)
developed a similar program supporting the CCT program,with children labour as the
target (training for children labour and persuade them to come back to school). They
also provided trainings for targeted facilitator and RTSM.
“Training is often conducted, either general training for operator and facilitator, or
special training only for operator. Resource person and materials were prepared by

95
the Central Team. No problem found with those trainings”. (Operator, in South
Kalimantan)
“In general, training materials and methods for CCT facilitators are okay and easily
understood, just a little input for trainers to be more energetic to stimulate
participants to be more energetic too and understand the materials better, we know
that training participants are from various background”. (Operator, in NTB)
Assessment result to training organization is good in general, and some inputs for
improvement should be considered. 42% of training participants said training
materials are good and easy to read, 52% participants said facilitators are clear in
explaining the materials. 19% of participants said the training tool aid are bad
meanwhile 15% of participants thought training duration is okay.
“The CCT training is good for us to improve our knowledge about this program, only
one weakness I guess, it does not clearly explained what outputs to focus on, quite
unclear”. (Operator, West Java)
“Trainers and materials are good, training methods should be improved, very hard
to apply those theories. Trainers only used presentations”. (Operator, West Java)
“The training is interesting and very enjoyable, materials are easy to understand and
thrainers are explaining it very good, but I do not know if other participants have the
same opinion with me because we have different educational background. I think
the trainers are very competent and master the materials. I suggest trainers
provide less serious materials, example a little game in the middle of sessions, to
make the situation more alive” (Facilitator, Bima, NTB)
Table 9.3. Value scale on Training Organization conducted by Operator and Facilitator (%)
Value scale (1= very bad; 5= very good)
1 2 3 4 5
Easy to read/understand of materials
2,5 40,5 41,8 15,2
Facilitator explains clearly 6,3 32,9 51,9 8,9
Good aid tool 1,3 17,7 29,1 35,4 16,5
Enough training duration 1,3 13,9 46,8 26,6 11,4
It is important to carry on a training for personnel providing services (health facility
and educational facility) with focus topic on how filling in and reporting the
verification forms. Most of them do not know how to do it. This situation was

96
indicated from verification forms which only 83% completed, and not all of it
correctly filled in especially the health verification form.
Assessment results to training organization are as follow: trainings were conducted
with some improvements needed, more people from health and education facility to
be invited to ensure good coordination system, additional 1 day of the training
duration (from 3 to 4 days), more training aid to be used, more field exercise to do,
more various training method (not only presentation), more respect to various
background of training participants.
In optimum training will cause inappropriate technical competence and managerial
skill, including in managing program: data validation and update, compliance
verification, payment and complaints management.
9.3 COORDINATION
Coordination is one of program effectiveness to measure. It is found that
coordination between Central UPPKH with district/city UPPKH is excellent, but need
improvement on cross sectoral and services delivery points coordination. Internal
coordination at UPPKH (central to sub national) is relatively good. At operator level,
coordination function is already excellent by conducting regular meeting with
facilitators. Median value on of coordination with facilitators is 16 times in the last
year, with range value 3-48 times.
Some challenges being faced in cross sectoral coordination. It is clearly mentioned
that all operators ever had coordination meeting with related sectors. Median value
for this is 4 times with range value 1-15 times. Institutions invited to coordination
meetings are Bappeda, Social Office, Health Office, Statistics Office Dinas, Sub
District, etc. (village, school and Puskesmas).
In optimum coordination function is also due to perception of personnel at central
UPPKH that they think of MSA function is only for payment officer. Coordination
meeting is irregular and merely held at the time when payment date is due, not all
personnel from health and education facility invited, and sectoral ego still exist and
inhibit coordination function.

97
Below is quotation of fact supporting the finding that personnel at central UPPKH
still think that MSA officers is only acting as payment officer.
“CCT program socialization is still weak, maybe it is not an important thing to do.
MSA thinks this should be done by them since money for the program is channeled
through its institution. So merely not only act as payment officer. CCT is a
comprehensive program, it is developed by Bappenas (program developer), MSA
(program implementer), MCIT (program socialization), MOH (health services
provider), MONE (educational services provider). It is good, but please remember,
Indonesia is a huge country”. (The Ministry of Health)
In depth interview with many stakeholders revealed that coordination meeting is
irregularly held, merely at the same time when the payment is due. Classic problems
risen wwere persons coming to the meeting keeps on changing. This situation has
made an ineffective meeting because organizer should explain over and over again
about the CCT program to audience. Personnel from health and educational facility
are sometimes not invited or not come to the meeting. The following sentences are
facts related to coordination matters.
"We saw there is a lack of coordination among related sectors, not all of them
understand the program ". (In depth interview with staff of Puskesmas, District of
Bima)
"At district, Social Office invited the stakeholders including the Bappeda, Religion
Office, Education Office, Elementary and Junior High School Principals. Only once
coordination meeting then no more meetings after that, we knew some friends in
the field are working on this. Bappeda must have an initiative for organizing the
next coordination meetings, because the nature function of the institution is for
coordination ". (In depth interview with Education Office, Dompu District)
“The lower divisions within sectors are not well coordinated, still a challenge ( UPPKH
Coordinator, District of Banjar)
“Educational and Health Offices are very slow response for coordinating the CCT
program (FGD among facilitators, District of Banjar)
“All problems come because of lack of coordination among sectors, when we shared
this in a meeting where multi sectors came, direct instruction from the head of the
Dinas was issued to support the program. I personally never heard of anything bad
or negative that influence UPPKH performance (Facilitator, Bima, NTB)
98
“During coordination meeting, I found some participants did not understand what
we were talking about, the persons keep on changing, I am reluctant to say from
what sector but it is irritating when we have to explain the same thing in every single
meeting”. (Facilitator, Subang, Jabar)
“... staff from educational and health facility did not understand the CCT program,
the supervisors came on the first meeting but they did not share the information to
the staff, . .when we asked them to send report, we knew that the supervisor who
used to come to the meeting has been replaced...” (Facilitator, North Jakarta).
In addition to the above mentioned problems, the heaviest challenge for
coordination is sectoral ego in each district. This ego often inhibits coordination
related activities. Sectors are reluctant to participate in coordination meeting if it is
not organized by the Bappeda.
“During the meeting, one sector said that his sector is just the member of Bappeda,
the coordinator is the Bappeda, but this sector or others never comes“. (Facilitator,
Subang, West Java)
”Staff from Educational Office always comes to coordination meeting organized by
the Bappeda. Although there is no letters from the Ministry of Health about the CCT
program to monitor students receiving the program, but in some meetings with the
school principals and head of education office, they discussed about this issue”.
(Educational Office, Banjar, South Kalimantan)
The local government assumes the CCT program is government program and they
task is only for organizing coordination meeting. Few districts have and have not
allocated some fund for coordination meeting. Districts that have not allocated the
budget thought it is a national program, therefore, all funding support will be given
from the central government, except there is a letter or instructions issued for the
districts to allocate some budget. It seems that lack of funding support is become a
big problem for coordination arrangement and improvement.
“Bappeda already allocated some fund for coordination meeting every quarter (4
times a year) and for evaluating CCT program implementation. When there is a
crucial thing to be discussed then the meeting could be held more than 4 times. The
description of the fund is for coordination meeting, stationeries and field monitoring
visits. Total funding allocated is Rp44.5 Million; Rp23.5 Million for coordination
meeting, Rp12 Million for field monitoring visit and the rest is for stationaries and
administration expenses”. (Bappeda, Banjar, South Kalimantan)

99
"We did not have coordination meetings in 2008 and 2009, because we did not
have budget for this. But we do have informal discussions with related sectors
whenever we had chance. In 2010, we have allocated Rp36 Million for meetings
and monitoring visits ". (In depth interview with Head of Bappeda, District of
Dompu)
“Since there is no instructions from the central government so BAPPEDA has not yet
allocated the budget within Local Budget system. There are programs intended to
the support the poor, but no special budget for PKH (Bappeda, HSS, South
Kalimantan)
District sectors assumed that CCT program made them do some more works and
made them overload. They have provided the services without funding support,
either for CCT program implementation or incentives for filling in verification forms.
"Health Office is fully support the CCT program. But we think it should be supported
with provision of some fund for coordination meetings with our subordinates,
example, monthly meeting. Please do not count on the report only from Facilitator.
Facilitator is too dominant, until now I never heard my staff at Puskesmas were
trained on CCT program by them. As we know, these people have direct contact to
CCT beneficiaries. I suggest to improve coordination ". (In depth interview with Head
of Health Office, District of Dompu)
I suggest to set up coordination system between Social Office, Health Office,
Educational Office, Bappeda and Facilitator. I think we still poor on coordination,
very difficult to manage the schools and puskesmas. I remember only one meeting
held for coordination ". (FGD Facilitator, District of Dompu)
”They are lazy to complete the forms because no fee or incentives. Post office staffs
said schools have not completed the verification forms, so they did not take the
forms, and ended with blaming each other. (Operator, Subang, West Java)
“No instructions from supervisor (Health Office/Educational Office), “Services
providers are reluctant to complete the forms because they said no instructions from
supervisors. Sometimes I found staff from service provider who asked for some
money for completing the verification forms”. (UPPKH, Banjar, South Kalimantan)
The above mentined challenges are because of the following situations 1) role and
function of the TKPKD team is not yet optimum. 2) sectors at central level have not
shared instructions to their subordinates to support the CCT program
implementation. 3) Regional Coordinator who is based at national, monitoring and
evalution of program is inactive. 4) central database is not yet analized and to be

100
used as feedback for district UPPKH. 5) lack of supervision and assistance from
central UPPKH attn. Regional Coordinator to operator and facilitator.
There will be an implications to program being implemented if the government do
not have solutions to overcome those problems. Few implications might arise are
inappropriate program implemention for providing health and education services,
disobeyence of conditional requirements for verification process and it will make the
CCT program similar with Cast Transfer (Bantuan Langsung Tunai/BLT) program, and
last, interupted payment schedule and frequency.

101
CHAPTER 10 KNOWLEDGE OF PROGRAM RULES AND PROCEDURES
In order to achieve the goals of the Conditional Cash Transfer (Program Keluarga
Harapan or PKH), the persons in charge (PICs), the program manager and executives,
and the PKH benericiaries as well as related stakeholders in all levels and areas need
to comprehend the management of the program, including the beneficiaries criteria
and the terms and conditions for payment. A fine level of comprehension and
knowledge is expected to be resulted from a good socialization, training and
coordination.
In general, it can be concluded that the knowledge of all related parties, starting
from the regional government and offices, to services and communities, is yet to be
optimum. Many key personnel of the various sectors have to understand fully the
essence of PKH. They have not understood the relations between PKH and other
poverty-resolving programs, such as (Jaminan Kesehatan Masyarakat or Jamkesmas,
School Operational Aid (Bantuan Operasional Sekolah or BOS), Rice for the Poor
(Beras Miskin or Raskin).
The PKH beneficiaries should be well-informed on their rights and obligations. They
have the right to cash donations, but only after they fulfilled several conditions, such
as: they must admit their children into the compulsory education program until
Junior HIgh School (SLTP) with an acceptable rate of attendance (85%); pregnant
women in their families have to do monthly ante-natal visit to health facilities and to
have their deliveries assisted by trained health personnel; they must complete the
immunization program and other health programs for families with children aged
under five years.
The result of a spot-check study done in 5 provinces shows that most (72% - 91%) of
the mothers who were beneficiaries understood that the amount of the money they
received were adjusted with the conditionality, and that they must fulfill their

102
responsibilities, and sending their children to school until 9th grade (SLTP). However,
many (64% - 86%) of them did not know where to go to consult or give their
complaints, or that the money could be used for other purposes, or how to calculate
the amount of money they should receive based on their families’ composition. The
beneficiaries in Jakarta in general had a better understanding of the program
compared to that of other provinces, and that beneficiaries in South Kalimantan
were found to have the least understanding. The result for spot-check on the
beneficiaries level of knowledge on PKH is shown in the table below.
Table 10.1. The knowledge of beneficiaries on PKH
DKI
Jakarta
Java, West Java
East Java NTB
South Kalimantan Total
PKH Knowledge % % % % % %
Knew the amount of the aid is different in every family (according to condition) 85.0 80.2 74.8 68.8 58.7 72.3
Knew the terms and conditions to be PKH beneficiaries 96.5 94.0 87.0 91.8 87.7 90.8
Knew that one of the obligation as a beneficiary is to send children to school until 9
th grade (SLTP) 90.5 74.7 75.6 75.3 56.5 72.8
Knew that one of the obligation as a beneficiary is to have health personnel to assist in pregnancies and deliveries 96.0 91.5 86.5 91.2 77.8 87.8
Knew where to go to give complaints or consult on issues related to PKH 66.0 42.4 31.9 42.8 11.5 36.0
Knew the aid can be used for other necessities 18.5 11.5 13.2 21.5 8.7 14.3
Knew how to calculate the amount of aid to be received based on the family conditions 57.0 42.1 37.4 35.0 10.2 34.2
The objective of PKH is to alleviate poverty and to improve the quality of human
resource in Indonesia. In its implementation, PKH needs to be supported by other
poverty- alleviation programs ie. Jamkesmas, BOS, Raskin, and Direct Cash Aid
(Bantuan Langsung Tunai or BLT). Even so, not all program managers and executives,
even officers who are directly involved with PKH such as the Education Office and
the Health Office, understand the rules and procedures of the program. This occured
because of many reasons, such as their never-having had any socialization, the

103
opinion that PKH is merely a sector-based program, or the lack of communication
and coordination with fellow PKH Operators/Facilitators/Managers.
The following excerpts of interviews reveal that not all related officers in Education
Office and Health Office as well as program officers at the level of health facilities
and education facilities understand fully PKH and various other poverty-alleviation
programs. It was often found that PKH beneficiaries were given the same treatment
as any other member of the community, instead of receiving their rights as PKH
beneficiaries.
“So, actually, it was our idea to set a mechanism for complaint resolution , as well as
its coordination. Well…now it seems that it does not run well. I strongly believe, the
reason why, chiefly, on the field level, in the management, there is still no full
understanding on the concept of PKH. It is as if the facilitators work on their own,
with no umbrella…like a chick without its mother-hen” (Bappenas).
“…I have been rejected by Puskesmas. I was told then that this (program) does not
apply yet, so I would have to pay as usual. I have told them that I was a PKH
beneficiary, and that I was informed that a card-carrying participant of PKH can also
(receive free service), and that was the reason I was brave enough to claim…” (A PKH
beneficiary, Tanjung Priok Sub-district, DKI Jakarta province)
”...The education facilities are still asking questions on PKH...” (A facilitator,
Situbondo District, East Java)
The following case was an example that a PKH beneficiary is considered to be no
longer appropriate to accept other poverty aids. They were denied, with the reason
of a fair distribution of aid. Another reason the above case occurred is that the
current policy which applies is that only poor citizens who own Jamkesmas card are
allowed to receive free health service; hence PKH beneficiaries who did not own
Jamkesmas card were asked to pay for health service in Puskesmas.
Even though, at the central level, policies have been set to regulate that PKH
beneficiaries are also appropriate to accept free health services in health facilities,
the fact on the field shows differently. This really speaks loudly on the lack of
integration of the various existing poverty-resolving programs in Indonesia.
104
“Actually, the government is not yet solid, in terms of the efforts to resolve poverty.
So far, there are PKH, Jamkesmas, and PNPM programs. But in reality, who is there
to facilitate all these poverty-alleviation programs. Don’t let it be that in this place
they make something, while in that place they make something different. No
connection between them. Meanwhile, a lot of money has been spent. If you’re
interested to study this, the public will be so grateful”. (Ministry of Health)
“Many Puskesmas do not know yet that a PKH-card holder must be treated the
same with as a Jamkesmas-card holder. During vaccination and vitamin distribution
we face no trouble, but during visitation to Puskesmas, the service is unsatisfactory.
Often there are shortages of medicines, no health personnel (mantra)... When we
come to seek treatment by bringing our PKH card, we were not accepted...it was
hard to receive service… We had to still pay for the service…while if we have
Jamkesmas card, we would not be asked for payment (FGD with beneficiary mothers
of PKH, Bima District, NTB province)
"In the last few months we were in the Puskesmas and had to be admitted for
inpatient treatment, and we still had to pay because we did not have Jamkesmas
card, we only had PKH card…Eventually we had to pay 150.000". (FGD with
beneficiary mothers of PKH, Bima District, NTB province)
“…we were able to know which children have received PKH, so that they would not
receive other aids, so that there is fair distribution with other children. (If they) have
received PKH, why should they be able to accept other (assistance)? It will be unfair
for the other children…” (Headmaster, Jakarta).
“the beneficiaries still have to pay for service in health facilities because the PKH
card holders are not acknowledged as free health insurance recipients as well, and
when we are eventually exempted from payment, the treatment by health
personnel to us was slow and was given second priority to those who did pay. The
personnel in health care facilities also did not understand the application of a PKH
card for health insurance… I have been (rejected by Puskesmas). I was told then that
this (program) does not apply yet, so I would have to pay as usual. I have told them
that I was a PKH recipient, and that I was informed that a card-carrying participant
of PKH can also (receive free care), and that that was the reason I was brave enough
to claim…” (A PKH beneficiary, Tanjung Priok Sub-district, North Jakarta, DKI Jakarta
Province)
The survey found that numerous program executives, especially personnel in health
and education (in Puskesmas and schools) still mistake their roles in the PKH
program. This is shown by their lack of comprehension on how to fill the verification
form. This may be due to their not having had any explanation on how to fill the
verification form, be it through training or direct explanation by the Facilitators.

105
“…So…how should this form be filled? Can you please explain to me?” (Indepth
interview with Puskesmas personnel, Cilincing Sub-district, North Jakarta, DKI Jakarta
province)
"The schools have never joined any socialization. We obtained information on PKH
from our facilitators when we received the forms sent by the Post Office. There is a
lot of information that we have not understood, such as: what is the model of this
program; how does the system work, and whom the person in charge has to answer
to". (Indepth interview with Teachers/Islamic Elementary School, NTB province)
The problems revealed above are at least affected by three main causes; first, the
socialization has not reached the various sectors and levels of the community;
secondly, the content of the socialization has not explained enough the relationship
of PKH with the many other social and health programs; and thirdly, the hesitation to
read the guidelines on PKH.
If such root causes are not settled, several conditions may occur such as: the
implementation PKH may not be run according to the decided procedures; there will
be very low support by the public and the related fields; Consequently PKH
implementation is hindered and wrong perception created unrest and envy in
communities.

106
CHAPTER 11. Discussions, Conclusion and Recommendation
This chapter discusses and concludes the Spot Check results, and proposes
recommendations, targeted to UPPKH and related sectors and stakeholders, on the
critical issues to be addressed towards improved PKH implementation.
11.1. DISCUSSIONS
Spot Chek was conducted with the objectives to assess whether PKH has been
implemented as planned; to examine which process has been well running and
which ones not yet; and to identify critical factors constraining and challenging the
program implementation. Spot Check was focused on the critical processes of PKH
implementation, including data validation and update, payment, compliance to
conditionality, service provision, complaint resolution system, socialization and
training, and knowledge of relevant actors on program rules and operations. These
critical processes are interrelated and need to run well to follow the program rules
and procedures as stipulated in the PKH Implementation Guideline.
Results of the Spot Check indicated that all the critical processes, except the
conditional payment, have been taking place. However, there were still many
constraints and challenges faced by the program to make the critical processes run
well. The Spot Check has noted the critical role of facilitators in making the critical
process happened as expected. The facilitators have been bridging the messages
and information from the UPPKH at the district and central levels to the beneficiaries
and vice versa from the beneficiaries and communities to UPPKH at upper levels as
well as horizontal communication and coordination to related sectors and service
providers at Kecamatan and lower levels. In addition, the Spot Check also noted the
role of sectors at the province level has been minimal.

107
Another surprising finding from the Spot Check is the fact that 73% of PKH
households have one or two members are smokers. A smoker smokes on the
average 12 cigarettes per day. Further, the household spent on the average IDR
127,000 per month or IDR 1,524,000 per year for buying the cigarettes. It is irony
that the amount for buying cigarettes is in fact about 70% of the maximum amount
of payment provided by PKH.
Database validation and update
The beneficiary household data should be validated at the first recruitment meeting
to determine the beneficiary eligibility and the amount of first payment. In the
course of time, the beneficiary validated household data should be updated regularly
for demographic composition changes. This data update should be done
immediately or within three months at the latest in order to determine the amount
of next payment.
The Spot Check indicated that data validation and update has been in the process,
but a significant proportion of beneficiaries were not validated at the time of
recruitment and not all the demographic changes among the beneficiaries have been
updated. Inaccurate names and addresses and remote location of the beneficiaries
have challenged the facilitators to validate the household data at the time of
recruitment. Regarding update for demographic changes, many beneficiaries have
not yet been aware of which changes should be reported immediately to the
facilitator. In some cases, the entry process of validated or updated data by
operator at the district level faced the various constraints so that some validated or
updated data already entered, even online, might not appear in the Central
Database. Some cases of inaccuracies in names and demographic status printed in
the verification forms indicate that the beneficiary database validation and update
has not been optimal.
In turn, the inaccuracy of the Central Database would affect the amount of payment
paid to the beneficiary, and also the verification process on compliance of
beneficiaries to conditionality. Hence, the amount of payment paid to the
beneficiary might not be correct. As the Spot Check has shown some beneficiaries

108
might receive more but others received less then the amount of payment based on
the household data verified in the field. The inaccuracy of the Central Database
would result into the inaccuracy of data printed in the verification form and this
would disturb the verification process of compliance at school or health facility.
Payment
Different from BLT (Bantuan Langsung Tunai) or a Unconditional Cash Transfer (UCT)
Program, PKH is in fact a Conditional Cash Transfer (CCT) Program. In PKH, payment
to the beneficiary is based on conditionality, which means only if the beneficiary
complies with the condition of using the basic education and health services. Thus,
payment to the beneficiary provided by PKH is based not only on the household
demographic data (number of pregnant and post partum women and school aged
children), but more importantly also compliancy to conditionality. Payment will be
deducted if the beneficiary does not fulfill the conditionality.
Nevertheless, Spot Check indicated that the payment based on compliance to
conditionality has not yet happened. A key person at the UPPKH said that the
program has not yet fully implemented payment based on compliance to
conditionality, but at the time of Spot Check a pilot test of such conditional payment
was ongoing in 23 districts. According to the UPPKH, the program since the
beginning of 2010 has just started operating the conditional payment in stages. If
the program does not implement the conditional payment, then PKH does not differ
from BLT.
By the time of Spot Check, the payment is based only on the validated and updated
number of pregnant and postpartum women and school aged children. However, as
previously mentioned, Spot Check indicated some beneficiaries received more and
some others received less than the ‘should be’ payment. This is because the number
of pregnant women and number of school aged children for some beneficiaries were
not matched between the Central Database and the survey data at the Spot Check.
Another important issue of payment is related to the timing and frequency of
payment. Because of various reasons, including not enough cash and conflicting
109
schedule, the payment was often delayed. The payment should be scheduled 4
times a year according to the program rule, but in reality the common frequency of
payment was 3 times a year and in some places even only two times a year. The
three time payment frequency per year often made the payment to be rounded
down. This rounded payment can create abuse of fund. Also, the less frequency of
payment might not correspond to the continuing need of beneficiaries.
Even in a small proportion, the beneficiaries received payment less than the amount
they signed because of rounding or other reasons. More worrying was the facts that
some beneficiaries reported their fund were cut by certain individuals in a significant
amount, between IDR 10,000 to IDR 50,000 depending to the amount of money they
received. Some beneficiaries, however, did not care whether the money is cut or not
since they should have thanked because already received fund. There has been no
systematic action taken to avoid the cutting of fund received by the PKH
beneficiaries.
Compliance to conditionality
Spot Check indicated significant proportions of beneficiaries in all localities have not
yet complied with conditionality. The data showed that not all birth deliveries were
attended by health personnel; not all under-five children weighed regularly every
three-month, and not all children were completely immunized by age of 12 months.
In regard to schooling, however, only a small proportion of school aged children not
going to school because of various reasons, including not having enough money.
There were several factors that explain why the beneficiaries did not comply with
conditionality. Some beneficiaries were not aware of the conditionality and some
others did not motivate to comply as they still receive payment even not comply
with conditionality.
Even though program has put efforts to properly verify compliance of beneficiaries
to conditionality, the process has not been optimal. Problems occurred in all levels
of verification process. At first, the Central UPPH sends the database to be verified
to PT Pos. Then, PT Pos at the district level prints the verification forms to be
distributed to the targeted service facilities. Spot Check indicated some cases of

110
verifications forms with inaccurate data, which would create confusion among
service personnel when they would complete the verification form. As previously
mentioned, these cases were related to the problem of database validation and
update.
PT Pos has not been able to properly distribute the verification forms to the targeted
service facilities. Spot Check indicated still many schools and health centers have not
yet received the verification forms. Limited PT Pos personnel and remote location of
service facilities were among the reasons why PT Pos have not yet distributed the
verification forms to all service facilities.
Among service facilities already received verification forms, only a small portion
complete the forms. No knowledge on how to complete the form, inaccurate names
and data, and unmotivated to complete the form because not picked up, no
incentive or not really their work were among the reasons cited by the service
personnel in both the education and the health facilities.
Completed verification forms at service facilities should be picked up timely by PT
Pos every month or within three months at the latest. Cases of not picking up timely
PT Pos were noted. This delayed pick up of completed verification forms were
related to the fact that operator at the district received late the verification form.
Besides receiving late the completed verification form, other issues including
inadequate hardware facilities, limited data entry personnel, common blackout
electricity, and problems related to data entry software application and online
communication were among the factors constraining the timely data entry activities
operators at the district level.
Service provision
While PKH requests beneficiaries to use basic education and health services, PKH at
the same time should ensure that the available basic education and health services
are meeting the quality standard and accessible to the beneficiaries in need of
services. Regarding the basic education facilities, notably the elementary school or
the same level of other school and the junior high school or the same level of other

111
school, the Spot Check indicated that the number is relatively adequate but a
significant proportion were still below the national standard, in particular the
elementary schools. In the Spot Check, the education service quality was defined
according to several parameters, including number and qualification of school
teachers, and adequacy of teaching materials and laboratories.
Concerning the basic health facilities, including health center and its networking,
such as maternal hut, posyandu, the Spot Check indicated the problem of health
personnel distribution as well as quality of health services. In many of the surveyed
districts, almost half of the villages did not have village midwife. The majority of
midwives stayed in the sub-district capital or villages around that capital. This mal
distribution of health personnel made the women in need difficult to access the
midwife. Several health centers were faced with inadequate supply of vaccine and
basic commodities, including essential drugs. Not all the health centers were able to
provide quality services to the beneficiaries.
There were still cases of schools and health facilities rejecting services to PKH
beneficiaries. There were also cases of some health centers in one district accepted
but discriminated the PKH beneficiaries. Cases of PKH beneficiaries should pay for
services at education or health facility were also noted.
The issue of service quality in both education and health is particularly critical since
without quality, efforts to make women and children productive and healthy would
not be effective. PKH should inform the beneficiaries and communities about the
need of having quality education and health services.
Complaint acceptance and resolution system
As a critical program function to improve services, the complaint acceptance and
resolution process has been taking place. However, not all the beneficiaries were
aware about their right to complain the poor services. Spot Check indicated many
beneficiaries did not know how to complaint the poor services they received or any
PKH related problems encountered in the field. Only a small portion of beneficiaries
noted about the presence of Community Complaint Unit at the district level.
112
Even if the beneficiaries or other community members have the complaint, they are
avoiding the complaint in writing or putting their signature. Culture of submitting
complaint is in verbal expression, not in the written form. Community members
were still traumatic with bad experiences during the past government dictatorship.
Thus, from the complaints expressed by beneficiaries or community members, only a
small portion reached to the UPPKH district and processed at the central level. In
addition, the limited complaint form available had also reduced the number of
complaints submitted to the UPPKH district and central levels.
Spot Check indicated that complaints were submitted not only by beneficiaries but
also other community members. The majority of complaints from beneficiaries were
related to payment, including the amount was not correct, delayed payment, long
queue of obtaining payment, and poor services by PT Pos. Complaints from
beneficiaries were mostly submitted through either facilitator or the mother leader.
On the other hand, complaints from other community members were mostly related
to the question why they were not accepted as PKH beneficiaries. These
complainers felt that they were poorer than those accepted as PKH beneficiaries.
Socialization, training and coordination
Socialization is considered essential for ensuring support and participation from
related sectors, service providers and communities. Spot Check indicated that PKH
socialization has not been effective. Commitment of related sectors particularly at
district levels has not yet at the level to fully support the PKH operations. Many key
personnel of related sectors were still on the position to regard PKH as additional
burden to their main tasks. Personnel at the key sectors, notably the education and
health sectors, felt they have not been asked to really involve in the program
operations.
Supposed to be the leading sector for socializing the PKH, the Ministry of
Communication and Information (MOCI) has in fact not yet optimally performed the
tasks. Operators and facilitators involved in the socialization admitted that quality of
most socialization has not yet in the level of expectation, for example, lack of written
materials and lack of follow up. Spot Check indicated that TKPKD (Local Coordination

113
Team for Poverty Eradication) at many districts has not yet been properly
functioning. Ministry of Social Affairs (MOSA), including the Dinsos at the provincial
dan district levels, as the PKH leading sector has relied much on MOCI in the conduct
of socialization.
Training has important function to make related personnel have adequate technical
and managerial competence in operating PKH. Training program has been running,
but the quality needs to be improved. The training curriculum should be improved
to include not only the theory, but also more field practices. Inputs from the field
suggested the need to expand the training coverage to include training of service
personnel, especially about the compliance verification process.
As a key of program success, coordination is relatively adequate within the UPPKH
but weak between related sectors and service providers. Key personnel in related
sectors at central level are still in the opinion that the role of MOSA in PKH is only as
the ‘payment disburser’. Coordination meeting was not yet routine but conducted
only before the payment time. The local government commitment in supporting
PKH has not yet in the level to support better coordination of related sectors.
Culture of ego sector has in many cases constrained for better coordination. Not all
the local governments have allocated funding for coordination meeting.
Supervision and facilitation from the Central UPPKH has been lacking. Data and
information regarding PKH operations have not yet been optimally utilized in
feedback to local government and sectors and UPPKH personnel at local levels.
Using data for socialization would likely be more effective.
Knowledge of program rules and procedures
Knowledge of related actors on program ruled and procedures has been optimal.
This situation is consistent with the fact that socialization has not been effective.
Many key personnel of related sectors did not know comprehensively about PKH
rules and procedures, including the relationship between PKH and other social
protection programs, such as Jamkesmas, School Operational Assistance, and Raskin.
This situation has been reflected with the fact of cases by which PKH beneficiaries

114
were rejected to receive free services and assistance from other social protection
programs. The incorrect knowledge of PKH rules and procedures might have various
implications, including barriers for program implementation and community
misperception with social jealousy.
11.2. CONCLUSION AND RECOMMENDATIONS
Spot check concludes that the newly launched PKH is implemented as a conditional
cash transfer program targeting very poor households. The goal of this program is to
improve health and education of poorest communities to be able to exit out from
poverty. The direct recipients of PKH are women who are the motor of the domestic
life. PKH is a complex program having many challenges in implementation. Most
program functions, including data validation, payment, data update, verification of
compliance, service delivery, dissemination, training and coordination have been in
place, but they were suboptimum. All of them contain problems that may hinder the
achievement of PKH goals. Payment of cash transfer is based on household
composition, but conditional payments based on participants’ compliance in utilizing
basic health and education services gradually started in early 2010.
To improve PKH implementation, Consultant team provides recommendations to the
relevant sectors as follow:
1. Bappeda at the city/district level should play more active roles in
implementing cross-sectoral coordination down to service level to
support PKH implementation. Bappenas and Bappeda should coordinate
to rearrange sectoral roles and responsibilities and disseminate the
decisions made to all related sectors including staff in education and
health service facilities. The decisions should unite all poverty reduction
programs under one roof.
2. BPS shall improves SPDKP implementation so poverty reduction program
database is complete and accurate. Special attention should be made to
improve accuracy of households’ names and addresses and avoid using
village staff as data collectors.
115
3. Relevant local offices, including Dinkes (District Health Offices), Disdik
(District Education Offices) and Kemenag (Ministry of Religion) shall
deliver all information about PKH activities to alll personnel in their
offices.
4. Kemendiknas should conduct dissemination and coordination actively to
Disdik and fasdik so that the latter understand that PKH is an integral part
of basic education improvement programs. Dissemination needs to
emphasize that PKH participants are entitled to get scholarship for the
poor. In addition, there should be dissemination to the community about
national standards for education services and emphasize their right to
quality education. Furthermore, Kemendiknas should increase the
number of scholarships for teachers of elementary schools/MIs and
Junior High Schools/MTs to pursue bachelor degree , and coordinate
district offices to increase funding allocation to improve equipments and
infrastructures of education facilities to meet the national standards.
5. Kemensos should increase effectiveness of dissemination to the
communities through facilitators and informed the urgency of reporting
changes in household composition, utilization of basic health and
education services, and submission of written complaints without fear.
They should also coordinate with the health sector so that all PKH
participants/beneficiaries are included covered by Jamkesmas and
scholarship for the poor. Kemensos, as the responsible ministry and
program implementer, should lead all dissemination activities and should
coordinate with Kemenkominfo jointly design and conduct dissemination
to relevant sectors and offices from central to district levels. The role of
Kemensos/District Social Offices as cross-sector mobilizer should be
improved.
6. Kemenkes should revise NSPK and develop standards for Puskesmas
including its networks and provide process indicators. Furthermore,
Kemenkes should disseminate to the community through Health Offices

116
and faskes about basic health service standards and the community right
to get quality health services. Furthermore, Kemenkes should increase
special fund allocation (DAK) to local governments to meet the standards
of basic health services. Kemenkes should improve coordination with
District Health Offices so that PKH all participants/beneficiaries receive
Jamkesmas card. Finally, Kemenkes should actively disseminate and
coordinate with District Health Offices and faskes that PKH is an integral
part of the basic health service programs.
7. PT Pos should improve payment processes by solving delays, long queues,
availability of cash, and staff hospitality. They should ensure timely
printing, distributing, and collecting verification forms as agreed
schedules.
8. UPPKH as the responsible institution should do the following:
a. District/city UPPKH should improve training for staff of faskes and
fasdik on how to fill out verification forms and develop
incentive/reward system for those who complete the forms
accurately.
b. Through facilitators, District UPPKH should empower the
communities and guartee them from fear to submit written
complaints, and prepares standard operating procedure (SOP) for
complaint handling and resolution. Furthermore, UPPKH should
also ensure responses and solution for each complaint submitted.
c. UPPKH should ensure that verification and update forms are
always available at fasdik and faskes.
d. Through facilitators, UPPKH shall improves dissemination to
participants/beneficiaries about the urgency to fulfill conditional
uses of basic health and education services, ensures timely
printing, distributing, and collecting verification forms. When
necessary UPPKH shall involve facilitators to review the tasks of PT
Pos.

117
e. District UPPKH should ensure payments as scheduled in the
guidelines; enforce sanction to those who deduct money from
benefiaries, and develop better mechanism to link payment to
compliance requirements.
f. District UPPKH sould ensure dissemination budget as an integral
part of PKH to cover the following activities: strengthening TKPKD,
improving central and local coordination, reinforcing
dissemination with target and clear strategies and at the same
time develop a special district dissemination team.
g. Central UPPKH should strengthen the role of Korwil (locals) in the
dissemination and coordination of PKH from theprovincial to the
facility levels, build routine cross-sectoral forums to monitor and
manage improvements of utilization of database, results of spot
check and other assessment to improve PKH implementation.
h. Central UPPKH should strengthen provincial and district team of
trainers, improve training programs with clear goals and strategies
(materials, method of delivery, and field practices).
i. Central UPPKH should submit written complaints from the public
and PKH participants to Kemendiknas and Disdik on issues related
to basic education services.
j. Central UPPKH should routinely file complaints from the public
and PKH participants to MOH and district Health Offices on issues
related to basic health services, request facilitators to disseminate
to the community about procedures for submitting complaints
about health services.
k. Central UPPKH should routinely distribute and disseminate
concise and communicative PKH manuals / guidelines to related
sectors.

118
l. Central UPPKH should develop a more practical training on PKH
procedures for operators, facilitators and service providers
involved in the program, supervise and facilitate PKH
implementation at district down to village levels, assure the
availability of forms at the facilitators, ensure that the data at the
district / city and district-central online network are up to datte.
m. Personnel at Central UPPKH MIS should be more responsive to
updates made by the district operators in the PKH database to
ensure all validation, updates, verification, and complaints data
are recorded.