physiotherapy modalities · massage has been a therapeutic modality in all cultures since early...
TRANSCRIPT
Br J Sp Med 1993; 27(1)
Physiotherapy Modalities
The role of massage in the management of theathlete: a reviewMichael J. Callaghan GradDipPhys, MCSPDepartment of Physiotherapy, Royal Liverpool University Hospital, Liverpool, UKHonorary Chartered Physiotherapist, British Cycling Federation
Massage has been a therapeutic modality in all culturessince early civilization and has had a long tradition of usein the sporting context. However, there has been a paucityof scientific evidence of the physiological, psychologicaland therapeutic effects of commonly used massagetechniques. This paper reviews the early and more recentstudies on the effects of massage and also the more recentliterature on its use on the sports person. Little agreementwas found in English publications of the efficacy ofmassage and there were contradictory findings as to theoptimum technique and length of time of application. It isclear that the role of massage - a time-consumingtechnique for a physiotherapist to perform - needs to beevaluated further in order to resolve some contentiousissues arising about this mode of treatment and to justifyits use.
Keywords: Massage, therapeutic effects, physiologicaleffects, sportsperson, physiotherapy
Massage has been a therapeutic modality used byman since early civilization. Kamenetz' described theorigin of the history of massage starting in the earlycivilizations of Babylon, Assyria, China, India,Ancient Greece and Rome. Massage continued to beused in the middle ages, the Renaissance, andthrough to the 20th century.
In the early 19th century, medicine and sciencemade great progress in a desire for greater accuracy,understanding and the questioning of establisheddoctrine. It was mainly in the last quarter of the 19thcentury that massage began to be studied andresearched, while the 20th century saw the develop-ment of new techniques and systems. Kamenetz1concluded that massage had declined over the greaterpart of the 20th century and proposed three reasonsfor this decline:1. The development of the pharmaceutical industry2. New machines supplanted older forms of physical
therapy3. Dehumanization in the relationship between
therapist and patient.
Address for correspondence: Michael J. Callaghan, Department ofPhysiotherapy, Royal Liverpool University Hospital, PrescotStreet, Liverpool L7 8XP, UK
© 1993 Butterworth-Heinemann Ltd0306-3674/93/010028-06
Scu112 advocated the use of massage as an 'indispens-able agency' in the control of significant features ofdiverse syndromes such as poliomyelitis, anaemia,arthritis, cardiac oedema and nervous conditions.The physiological basis for these techniques wasspeculative.
It was also noted that the nucleus of physicaltherapy of rest, massage, heat and exercise had notchanged over many years except for the use of X-raysand radium and that massage should be administeredby a person of technical skill with anatomical,physiological and pathological knowledge.Whereas the use of massage advocated by Scull2
has all but disappeared from use in hospitalphysiotherapy departments, the use of massage forthe sports person has maintained a high profile and isan integral part of an athlete's conditioning3 eventhough its role may have been partially overvalued4.From a scientific viewpoint, however, the use of
massage in the sporting context has become conten-tious and flaws have been found in the claims byworkers in the early part of the 20th century.
Massage techniquesAlthough massage technique may vary considerablybetween therapists, classical massage consists of anumber of basic techniques which have remainedessentially unchanged for centuries4 5. These techni-ques are referred to as Swedish massage6'7 and arecomfortable, palliative and favoured by charteredphysiotherapists.There are also diverse forms of massage such as
connective tissue massage4'8'9; underwater mas-sage4; shiatsu and acupressure5.The five basic techniques of classical massage are
effleurage, petrissage, friction, tap6tement and vibra-tion.
Effleurage (or stroking) is a deep stroking thatshould be in the direction of venous or lymph flow.Superficial effleurage should be centripetal. The palmof the hand is used and should conform to thecontour of the body being treated. It was hinted2 thatevery massage session should begin and end witheffleurage simply because it was the most gentletechnique and it served as an introductory procedureto the other techniques.
28 Br J Sp Med 1993; 27(1)
on April 22, 2020 by guest. P
rotected by copyright.http://bjsm
.bmj.com
/B
r J Sports M
ed: first published as 10.1136/bjsm.27.1.28 on 1 M
arch 1993. Dow
nloaded from
Massage in the management of athletes: M. J. Callaghan
Petrissage (or kneading) is a deeper technique thaneffleurage and is directed towards the muscles. Thefingers and closed thumbs work like tongs graspingthe tissues gently. The direction being distal toproximal centripetally. A distinction has been madebetween petrissage and kneading in that more tissueis lifted, squeezed and moved in kneading5.
Friction (or rubbing) should be done in a slowelliptical or circular movement with the thenareminence or, more specifically, the finger tips.Frictions should begin with light pressure andbecome progressively deeper. 'Gelotripsy' has beendescribed as a violent removal of muscle hardening, atechnique which could cause bleeding within amuscle due to deep, strong pressure4. The use in thiscontext is therefore controversial.Deep friction massage should not be confused with
deep transverse frictions which have been describedas having a fourfold effect:
1. Traumatic (local) hyperaemia2. Movement of the deep tissues and prevention of
adhesion formation3. Increased tissue perfusion4. Mechanoreceptor stimulation10.
Local hyperaemia was said to have a lastingenhancement of the blood supply and hence analge-sia by increasing the speed of destruction of Lewis's Psubstance which is a factor responsible for pain. Itwas not explained how or if this differed fromincreased tissue perfusion.Tapotement (or hacking) is a series of gentle blows
with the ulnar border of each hand. Other thancausing hyperaemia in the skin, the primary effect isacoustic and could be detrimental if not used withextreme caution and restraint4. There have beenvague guidelines stated by some authors cautioningagainst over-vigorous application of some techni-ques4'10 and equally vague comments by others10 thatgentle massage was neither useful nor harmful.Vibration (or shaking) is used on the extremities
and is said to lower muscle tone4. The therapist canelevate the extremity to encourage the venous andlymphatic return and then shake the limb.
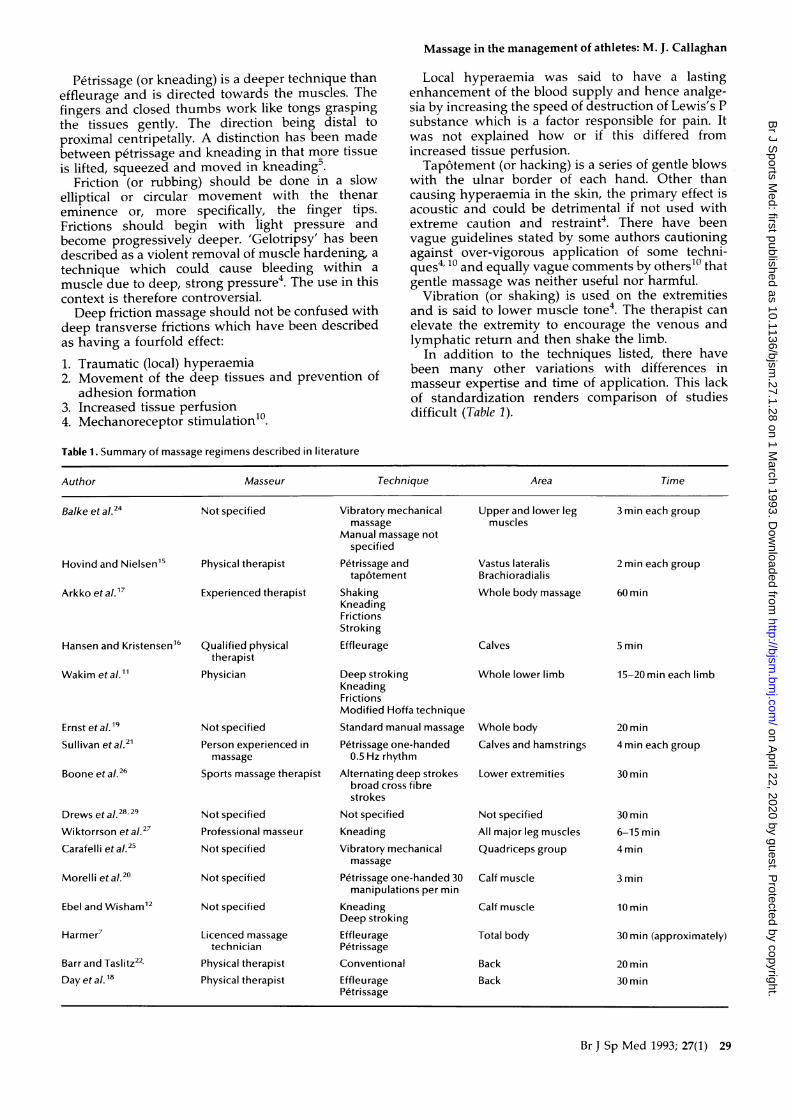
In addition to the techniques listed, there havebeen many other variations with differences inmasseur expertise and time of application. This lackof standardization renders comparison of studiesdifficult (Table 1).
Table 1. Summary of massage regimens described in literature
Author Masseur Technique Area Time
Balke et al.24 Not specified Vibratory mechanical Upper and lower leg 3 min each groupmassage muscles
Manual massage notspecified
Hovind and Nielsen15 Physical therapist Petrissage and Vastus lateralis 2 min each grouptap6tement Brachioradialis
Arkko et a!.7 Experienced therapist Shaking Whole body massage 60 minKneadingFrictionsStroking
Hansen and Kristensen16 Qualified physical Effleurage Calves 5 mintherapist
Wakim et a!." Physician Deep stroking Whole lower limb 15-20 min each limbKneadingFrictionsModified Hoffa technique
Ernst et al.9 Not specified Standard manual massage Whole body 20 minSullivan et a!.21 Person experienced in Petrissage one-handed Calves and hamstrings 4 min each group
massage 0.5 Hz rhythm
Boone et al.26 Sports massage therapist Alternating deep strokes Lower extremities 30 minbroad cross fibrestrokes
Drews et al.2829 Not specified Not specified Not specified 30 minWiktorrson et a!.27 Professional masseur Kneading All major leg muscles 6-15 minCarafelli et a/.25 Not specified Vibratory mechanical Quadriceps group 4 min
massage
Morelli et a!.20 Not specified Petrissage one-handed 30 Calf muscle 3 minmanipulations per min
Ebel and Wisham12 Not specified Kneading Calf muscle 10 minDeep stroking
Harmer7 Licenced massage Effleurage Total body 30 min (approximately)technician Petrissage
Barr and Taslitz22' Physical therapist Conventional Back 20 minDay et a.18 Physical therapist Effleurage Back 30 min
Petrissage
Br J Sp Med 1993; 27(1) 29
on April 22, 2020 by guest. P
rotected by copyright.http://bjsm
.bmj.com
/B
r J Sports M
ed: first published as 10.1136/bjsm.27.1.28 on 1 M
arch 1993. Dow
nloaded from
Massage in the management of athletes: M. J. Callaghan
Effects on circulationBecause of the perceived effect of massage on thecirculation3, a proportion of the studies into massagehave investigated this aspect1-19.
Early studies11 used venous occlusion plethysmo-graphs to determine the effects of two massagetechniques on the blood flow in normal and diseasedextremities. One technique (Table 1) resulted inconsistent and significant increases in average bloodflow.The second technique was described as deep
stroking and kneading massage which only gave riseto a moderate change in total blood flow in patientswith flaccid paralysis. It was noted that vigorousstimulating, forceful massage was not a routineprocedure and that it may actually damage flaccidmuscle and other soft tissues if performed incorrect-ly, although no evidence was presented to supportthis note of caution. This paper also noted that it wasimpossible to determine whether the cause of anincrease in temperature (hence blood flow) was dueto mechanical action or reflex stimulation. The reflexeffect was also investigated by Ebel and Wisham12who noted a considerable increase in skin tempera-ture in all subjects on the massaged calf and alsoslightly on the opposite limb. This contralateraleffect, it was speculated, was reflex in nature.Animal experiments have been performed to study
the effect of various procedures on the flow oflymph13. By observing the flow of lymph from thethoracic ducts of dogs, this study concluded thatpassive and active exercises to the hind legs andthighs of dogs were just as effective as massage inincreasing lymph flow. However, the kneading andstroking massage was only introduced when the dogsdeveloped leg oedema due to hypoproteinaemia,making the results difficult to extrapolate to normalsubjects or athletes.A study on the denervated gastrocnemius muscles
of cats suggested that massage was effective inmaintaining weight and strength but only in com-bination with electrical stimulation14. Other methodsused to evaluate effects on the circulation haveincluded xenon-133 as a tracer15 16. These studies areamong the few to use comparable methods ofinvestigation. Both studies revealed an increase inclearance rate with tap6tement and effleurage, butthese changes were small and transient. It wasassumed that tapotementl5 was vigorous andtraumatic enough to have caused muscular contrac-tions sufficient to affect blood flow and that thereason effleurage16 had an effect on xenon-133clearance was due to the centripetal force emptyingthe capillaries and venous beds. However, this wassuch a small effect that even light muscular exercisewould cause a greater increase in blood flow.Other studies17-19 have attempted to evaluate the
effects of massage on blood parameters. Massage,which was described as 'fairly vigorous conventionalwhole-body', was applied to nine healthy volun-teers17; 22 blood parameters were measured. Theonly significant rises were in creatine kinase (CK) andlactate dehydrogenase (LDH). This was explained bythe mechanical trauma to the muscles and subse-
quent increase of cell membrane activity caused bythe vigorous massage technique. This is an importantobjective measurement of the damage that can becaused to muscle through injudicious use of massage.Massage has also been shown to have no signifi-
cant effect on serum levels of 3-endorphin and13-lipotrophin levels'8. Unfortunately, this was per-formed on a small number of pain-free subjects whichthe authors concede may have influenced theirresults.However, the lack of any other blood changes
contrasted with other work19, the results of whichindicated that whole-body massage induced an acutedecrease in blood and plasma viscosity and haema-tocrit in both ankylosing spondylitis patients andhealthy subjects. These findings were explained bymassage causing a decrease in sympathetic tone or,alternatively, by a reactive hyperaemia causinghaemodilution. It was also postulated that mechanic-al, muscular manipulation may reintroduce stagnantflow from the microvasculature into the activecirculation. Interstitial fluid could also be mechanical-ly compressed into the circulation by the samemethod. Although the benefits of these findings arethe amelioration of muscle perfusion in ankylosingspondylitis patients, the benefits to athletes have notbeen studied. There have also been studies to verifythe effects of massage on skeletal muscle tone20 21,and on autonomic functions22.The clinical implications for athletes could be
reduction of muscle spasm or cramps due to injury orfatigue.
Objective measurement of muscle tone was ob-tained using the Hoffman reflex (H reflex). Thismeasurement of muscle tone is used extensively todetermine the excitability of the spinal reflex pathwayand has been used previously to investigate theefficacy of other therapies, such as ice, tendonpressure and passive muscle stretching. This studycould compare these techniques with massage usingthe same objective measurement.
In one study20 the calf muscle of nine healthyindividuals was massaged one-handed using apetrissage technique for 3min. Results showed thatthere was only a significant decrease in H reflexamplitudes during the application of treatment (P <0.01; one-way repeated measures analysis of variancewith Neumann Keuls post hoc procedures). Theseamplitudes returned to normal immediately ontermination of the massage. This seemed to indicatethat massage not only reduces the level of moto-neuron excitability and consequently of muscle reflexactivity, but is quite specific with much less effect onthe contralateral limb than previously thought andwith inhibition taking place only during treatment.This was confirmed in a later study using the sametechniques of massage and H reflex measurement21.The question is, how can massage with its multi-dimensional sensory input cause a decrease in thelevel of motoneuron excitability? It is suggested21 thatthe petrissage used may have the same effect asintermittent pressure techniques such as muscletapping, which also reduces the H reflex.
Studies on the autonomic functions of the bodyindicated a small trend towards an increase of
30 Br J Sp Med 1993; 27(1)
on April 22, 2020 by guest. P
rotected by copyright.http://bjsm
.bmj.com
/B
r J Sports M
ed: first published as 10.1136/bjsm.27.1.28 on 1 M
arch 1993. Dow
nloaded from
Massage in the management of athletes: M. J. Callaghan
sympathetic activity following massage to the back22.Unfortunately, this paper is unable to establishwhether the changes were due to physical or mentalprocesses. This would be an important considerationfor a physiotherapist treating an athlete beforecompetition as the parameters measured were heartrate, body temperature, respiratory rate and sweatingwhich athletes would be trying to control in thestressful pre-event environment. There were alsosubjective observations such as thirst and sleep.To summarize - studies on the physiological effects
have been contradictory and difficult to compare andevaluate due to different massage techniques utilized(Table 1) and different methods of analysis. As yetthere has not been any definite and consistentevidence that massage enhances body physiologyapart from its effect on skeletal muscle tone. Animportant finding has been an increase in LDH andCK after vigorous massage indicating muscle trauma.
Post-event massagePost-event massage is often applied to the athlete inthe belief that this will overcome fatigue and helprecovery23.One study24 evaluated the effects of two types of
massage (manual and mechanical) on recovery fromoverall muscular and physiological fatigue (Table 1). Itwas concluded that there were definite recuperativebenefits physiologically and locally from the twotypes of massage, but not from rest. Results were notanalysed statistically and the subject numbers weresmall. The study also failed to explain the processesby which fatigue could be countered by massage andif the manual massage technique was similar to thevigorous vibratory massage of the 'thumper'machine. However, the use of a mechanical massagerfor athletes without availability or finance for amasseur was advocated.A more recent study25 also investigated the effects
of vibratory mechanical massage on short-termrecovery from muscular fatigue. Using 12 moderatelyhealthy men, the results of this experiment indicatedthat there was no statistically significant difference inthe rate of fatigue in either static exercises or afterdynamic exercise (cycling) between vibratory mecha-nical massage or rest in the quadriceps muscles(repeated measures analysis of variance and post hocanalysis with correlated t tests). The reason whymassage had no effect on the rate of fatigue wasdiscussed. If one of the reasons for fatigue isrestriction of blood to the active muscle due to musclecontractions, then delivery and washout must occurbetween contractions.
If during strenuous muscle contractions the motorunit firing declines, this may be due to a decrease inblood flow. It seemed reasonable to suggest that anincrease in blood flow in excess of metabolicrequirements would enhance the return of allprocesses to homeostatic levels.
Increased blood flow was thought to be a majoreffect of vibratory massage, yet this type of massagedid not help recovery in this study. The reason forthis was that the mechanical massage set up a tonic
vibration reflex when it was used on muscles.Therefore, when the mechanical massage was beingapplied for 4min, the muscle was actively contract-ing. The study speculated that any beneficial effectsof blood flow (which were small) would be expendedin recovering from the effects of the tonic vibrationreflex set up by the massage. It was concluded thatshort-term recovery from intense muscular activitywas not augmented by vibratory mechanical mas-sage.
Pre-event massageMassage is often used by athletes before an event, yetthere has also been little scientific evidence to supportthe hypothesis that pre-event massage will enhancean athlete's performance.A physiological evaluation of massage in this
context26 was undertaken on 10 healthy men. Eachsubject was in either a control group (no massage) orthe treatment group (with massage) before 10 minsubmaximal exercise (Table 1). Parameters measuredwere Vo2, cardiac output, heart rate, stroke volume,a-v'2diff and blood pressure. It was found that thepre-event massage did not provide the subjects withan increased oxygen flow to the tissues, thereforeboth exercise tests at 80% of maximum heart raterequired the same oxygen consumption. There wereno significant differences in any other parameters (P> 0.05; paired t test). Without massage, the subjectsexercised just as efficiently as when they received thetreatment. It was concluded that it was justifiable tostate that the physiological effects of sports massagewere questionable. Additionally, this study tested forlactic acid levels which is a commonly quotedparameter that massage is said to affect. There wereno significant differences in the levels of lactic acidbuild-up after 10 min steady-state exercise, with orwithout massage.A previous study27 investigated the effect of
pre-event massage (Table 1) on joint range ofmovement and quadriceps and hamstring strength.The experiments were in the following order:
1. General warm-up2. Warm-up and massage3. Massage only4. Warm-up and stretching.The results showed that warm-up and stretching
(4) gave significant increases in all ranges ofmovement (Student's t test). The only other signifi-cant finding was that massage and warm-up, bothseparately and in combination, increased the range ofmovement at the calf, which seemed to be readilyinfluenced by the action of the ergometer and also bythe passive elongation by massage of the muscle andtendon. Muscle strength recorded showed a decreasein isokinetic strength of the hamstrings and inisometric strength of the quadriceps.Other treatment groups had no effect on strength.It was concluded that general warm-up and
stretching were a better way to increase flexibility. Italso had the advantage of being performed by theathlete him/herself without any expensive equip-ment. This paper highlights the common request
Br J Sp Med 1993; 27(1) 31
on April 22, 2020 by guest. P
rotected by copyright.http://bjsm
.bmj.com
/B
r J Sports M
ed: first published as 10.1136/bjsm.27.1.28 on 1 M
arch 1993. Dow
nloaded from

Massage in the management of athletes: M. J. Callaghan
from athletes for massage in the belief that this willsubstitute for any warm-up or stretching and helpprevent injury. The results are of clinical importanceand this is one of few papers published whichcompares three common strategies used beforecompetition.More recently, an investigation of the effects of
pre-performance massage on the stride frequency ofsprinters was undertaken7. This used a counter-balance design to identify the presence of order orlearning effect. Results showed no statistically signifi-cant difference between the group trials or anyinteraction (P > 0.05; Student's t test). However, themagnitude and direction of the means between theconditions did show a trend towards a positive effecton stride frequency of pre-performance massage. Itwas emphasized that the results were due to 30minof extensive and conscientious treatment by anexperienced masseur and that cursory massage maybe of less value. The author also speculated that theconventional level of significance (P < 0.05) may betoo stringent when studying sprinters. He bases thison the assumption that massage is not detrimental(which it may be17) and that it is low in cost.Although true in terms of materials this is not true interms of the number of hours taken to applymassage.To summarize - although massage is widely used
in the belief that it helps muscle recover from fatigueand can enhance performance, the studies to confirmthis are few in number and contradictory. It shouldbe noted that these studies are almost all performedin a laboratory setting. Although this enablesaccurate analysis and data collection, it may notreflect the effects of stress of competition and otherpsychological factors.
Sports-specific massageMassage can be regarded as sports specific. Differentsports and even different disciplines within a sportmay require a different type or amount of massage.This may create problems if results of the effects ofmassage in one sport are extrapolated to anothersport.
Cycling has traditionally regarded a masseur as anintegral part of its team. Recent studies haveinvestigated the scientific evidence of the effects ofmassage on elite cyclists28 29. In the first study28, sixelite cyclists performed a 4-day stage race (161 kmday-1) by computerized race simulation. After eachstage the cyclists were given either massage for20 min, or 30 min blind placebo microwave.The race simulation was repeated 18 days later but
the post-race treatments were altered. Parametersmeasured were serum muscle and liver enzymes todetect muscle damage and recovery status. Therewere no significant differences between massage andplacebo in pre-race, post-race, post-treatment, or 3days post-race parameters (P < 0.05). There were alsofound to be no differences in performances measuredby 40-km split times or final 161-km times.
It was concluded that post-event massage did notexpedite muscle recovery or improve performancetimes from ultra-endurance cycling. Although under
laboratory conditions, this study was one of the fewto place athletes under physical stress similar to thatin competition. It is after the types of conditionsreplicated in this study that a masseur is normallyused rather than a 1-day stage race.Owing to the emphasis placed on the emotional
and psychological effect that massage can have on anathlete's mood and performance, the same resear-chers undertook a second study29. Six elite cyclists inthe same experimental conditions were assessed as tothe effects of post-race massage on Ratings ofPerceived Exertion, Feeling Scale and Profile of MoodState. Results revealed no significant differencebetween the massage and the placebo conditions onany of the psychological profiles (repeated measuresanalysis of variance with Neumann Keuls post hocanalysis). It was concluded that post-race massagedid not provide ergogenic enhancement of psycholo-gical status or performance capacity when comparedwith placebo. This contrasted with results from anearlier study by Weinberg et al.30, which concludedthat there was a greater relationship betweenmassage and positive mood enhancement thanbetween exercise (running) and positive moodenhancement.
ImplicationsWatt (personal communication, 1992) stated that 50non-specific massages were performed on the UKteam within 2 days at the European Indoor AthleticChampionships in 1986 (i.e. general leg or bodymassage not for a specific problem). The number ofmassages carried out by physiotherapists and mas-seurs for the UK Team at the Winter Olympics atAlbertville in 1992 was at least 164. The numbercarried out for the UK Team at the Summer Olympicsat Barcelona in 1992 was at least 787 (Brown, personalcommunication, 1992). There are many requests fromathletes competing at the elite level for this techniqueand yet at present there is little or no evidence that itis beneficial.
Rather than massaging a limb it may be necessaryfor a physiotherapist to supervise and performpassive stretching and give advice on warming up inpreparing an athlete for competition. A furtherimplication is based on the assumption by a numberof authors that massage is not detrimental. Arkko etal. 17 demonstrated mechanical trauma to muscle by avigorous massage technique. On this evidence thecare of an elite athlete should not be left toinexperienced or unqualified practitioners.Massage continues to be a contentious issue in the
sporting context. Recent studies on healthy indi-viduals and elite athletes suggest that caution shouldbe used when extrapolating results from the subjectsof earlier studies in the hospital setting.Lack of comparable instrumentation and different
research designs have led to little agreement amongresearchers over the type of massage to be employedor the length of time needed to be effective. Indeed,the length of time and degree of use are often basedsolely on the athlete's preference and not on scientificdata.
32 Br J Sp Med 1993; 27(1)
on April 22, 2020 by guest. P
rotected by copyright.http://bjsm
.bmj.com
/B
r J Sports M
ed: first published as 10.1136/bjsm.27.1.28 on 1 M
arch 1993. Dow
nloaded from
Massage in the management of athletes: M. J. Callaghan
It is clear that the role of massage in the athleteneeds to be evaluated further in an attempt to resolvesome of these points and in an attempt to justify therequests from athletes for a time-consuming techni-que.
AcknowledgementsThe author wishes to thank an anonymous reviewer for helpfulcomments and Mr Peter Keen for his help and advice.
References1 Kamenetz HL. History of massage. In: Basmajian JV, ed.
Manipulation, Traction and Massage. Baltimore, USA: Williamsand Wilkins, 1985: 211-49.
2 Scull CW. Massage - physiologic basis. Arch Phys Med 1945;26: 159-67.
3 Stamford B. Massage for athletes. Physician and Sports Medicine1985; 13: 178.
4 Kuprian W. Physical Therapy for Sports. Philadelphia, USA: WBSaunders, 1981: 7-51.
5 Hofkosh JM. Classical massage. In: Basmajian JV, ed.Manipulation, Traction and Massage. Baltimore, USA: Williamsand Wilkins, 1985: 263-9.
6 Holey E. Connective tissue techniques (Letter to the Editor).Physiotherapy 1991; 77: 460.
7 Harmer PA. The effect of pre-performance massage on stridefrequency in sprinters. Athletic Training 1991; 26: 55-9.
8 Palastanga N. Connective tissue massage. In: Grieve GP, ed.Modern Manual Therapy of the Vertebral Column. Edinburgh,UK: Churchill Livingstone, 1986: 827-33.
9 Goats GC, Weir KAI. Connective tissue massage. Br I SportsMed 1991; 25: 131-3.
10 Cyriax J. Textbook of Orthopaedic Medicine: Treatment byManipulation, Massage and Traction, Volume 2. London, UK:Bailliere Tindall, 1980.
11 Wakim KG, Martin GM, Terrier JC, Elkins EC, Krusen FH.The effects of massage on the circulation in normal andparalysed extremities. Arch Phys Med 1949; 30: 135-44.
12 Ebel A, Wisham LH. Effect of massage on muscle tempera-ture and radiosodium clearance. Arch Phys Med 1952; 33:399-405.
13 Elkins EC, Herrick JF, Grindlay JH, Mann FC, Deforest RE.Effect of various procedures on the flow of lymph. Arch PhysMed 1953; 34: 31-9.
14 Suskind MI, Hajek NM, Hines HM. Effects of massage ondenervated skeletal muscle. Arch Phys Med 1946; 27: 133-5.
15 Hovind H, Nielsen SL. Effect of massage on blood flow inskeletal muscle. Scand J Rehabil Med 1974; 6: 74-7.
16 Hansen TI, Kristensen JH. Effect of massage, shortwavediathermy and ultrasound upon 133Xe disappearance ratefrom muscle and subcutaneous tissue in the human calf.Scand J Rehabil Med 1973; 5: 179-82.
17 Arkko PJ, Pakarinen AJ, Kari-Koskinen 0. Effects of wholebody massage on serum protein and hormone concentra-tions, enzyme activities and haematological parameters. IntSports Med 1983; 4: 265-7.
18 Day JA, Mason RR, Chesrown SE. Effect of massage on serumlevel of P-endorphin and P-lipotrophin in healthy adults. PhysTher 1987; 67: 926-30.
19 Ernst E, Matrai A, Magyarosy I, Liebermeister RGA, Eck M,Breu MC. Massages cause changes in blood fluidity.Physiotherapy 1987; 73: 43-5.
20 Morelli M, Seaborne DE, Sullivan J. Changes in H-reflexamplitude during massage of triceps surae in healthysubjects. I Orthop Sports Phys Ther 1990; 12: 55-9.
21 Sullivan SJ, Williams LRT, Seaborne DE, Morelli M. Effects ofmassage on alpha motoneuron excitability. Phys Ther 1991; 71:555-60.
22 Barr JS, Taslitz N. The influence of back massage onautonomic functions. Phys Ther 1970; 50: 1679-91.
23 Wakim KG. Physiologic effects of massage. In: Basmajian JV,ed. Manipulation, Traction and Massage. Baltimore: Williamsand Wilkins, 1985, 256-61.
24 Balke B, Anthony J, Wyatt F. The effects of massage treatmenton exercise fatigue. Clin Sports Med 1989; 1: 189-96.
25 Carafelli E, Sim J, Carolan B, Libesman J. Vibratory massageand short term recovery from muscular fatigue. Int Sports Med1990; 11: 474-8.
26 Boone T, Cooper R, Thompson WR A physiologic evaluationof the sports massage. Athletic Training 1991; 26: 51-4.
27 Wiktorsson-Moller M, Oberg B, Eksrand J, Gillquist J. Effectsof warming up, massage and stretching on range of motionand muscle strength in the lower extremity. Am J Sports Med1983; 11: 249-52.
28 Drews T, Krieder B, Drinkard B et al. Effects of post eventmassage therapy on repeated endurance cycling. Int J SportsMed 1990; 11: 407.
29 Drews T, Krieder RB, Drinkard B, Jackson CW. Effects of postevent massage therapy on psychological profiles of exertion,feeling and mood during a four day ultraendurance cyclingevent. Med Sci Sport Exerc 1991; 23: 91.
30 Weinberg RE, Jackson A, Kolodny K. The relationship ofmassage and exercise to mood enhancement. Sports Psycholog-ist 1988; 2: 202-11.
Br J Sp Med 1993; 27(1) 33
on April 22, 2020 by guest. P
rotected by copyright.http://bjsm
.bmj.com
/B
r J Sports M
ed: first published as 10.1136/bjsm.27.1.28 on 1 M
arch 1993. Dow
nloaded from