phn role in mental health - walter kmet june 2016
TRANSCRIPT

1
PHN role in Mental Health Reform
Adj. A/Prof Walter KmetCEO WentWest, WSPHN
Implementing Mental Health Reform1 June 2016

2
PHN role in mental health reform1. Context of our work
2. Commissioning
3. Consumer engagement
4. Integration

3
4
Key system wide problems*
More efficient and sustainable approaches are needed to improve the system for individuals, across the life course and across illness severity, and to improve targeting of efforts.
• Fragmentation, inefficiency, duplication and a lack of planning and coordination at a local level
• Service delivery based on the needs of providers, rather than on consumer choice
• Waiting too late to intervene to offer services for people with mental illness, with an imbalanced focus on acute, crisis and disability services rather than prevention and early intervention
• A ‘one size fits all’ approach to service delivery that does not optimally match or meet individual needs
• Underutilisation of innovative approaches to use workforce and technology
Government Response to Mental Health Review 2015

5
Identifying opportunities for health system improvement
Western Sydney PHN –Health system Improvement opportunities
Whole-of-system (Macro level): Enhanced structural integration across the various health services serving the population of western Sydney and covering both private and public health sectors.
Care/population groups (Meso level): Enhanced service integration for targeted health initiatives including local and national priority focus areas and/or sub-populations that have been identified as a result of PHN population needs analyses.
Patient-centric integrated and coordinated care (Micro level): Improved delivery of patient-centric health services to individuals and their carers through a coordinated set of care interventions that ensure the right care is provided in the right place at the right time.
Advocacy
Commissioning
Integration
Western Sydney PHN – Health
system Improvement opportunities
6
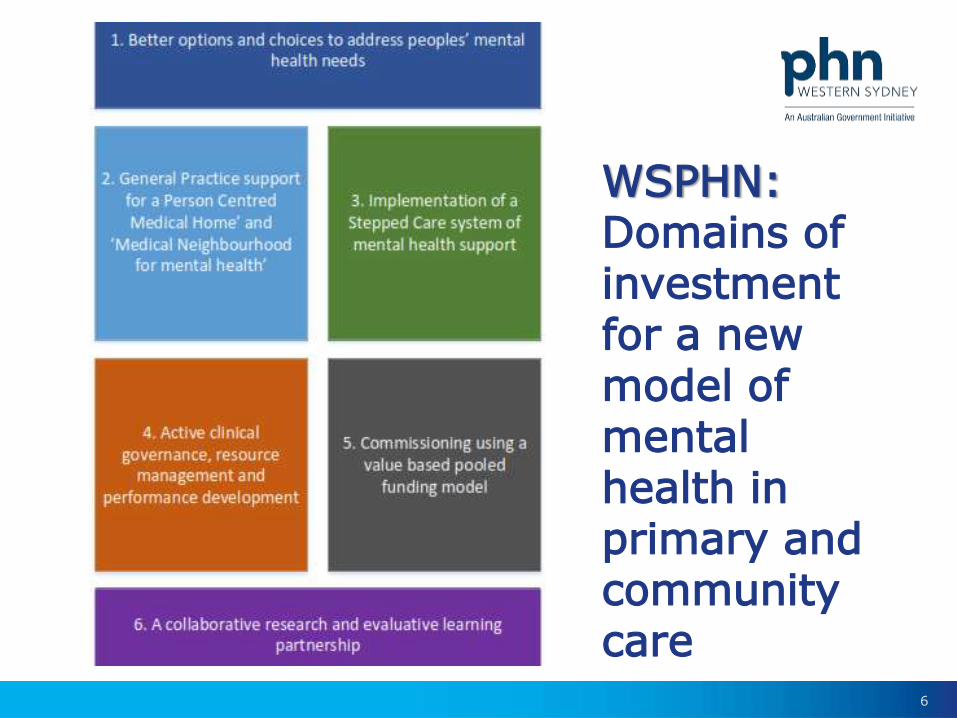
WSPHN: Domains of investment for a new model of mental health in primary and community care

7
PHN mental health priority areas
1. Aboriginal and Torres Straits Islander People
2. Low intensity services
3. Psychological Services to hard to reach groups
4. Children and Youth
5. Severe Mental illness and care packages in Primary Care
6. Suicide Prevention
7. Regional Plan
8. Stepped care

8
Strengthening mental health across continuum of care
Stepped Care

9
• undertake comprehensive regional mental health planning and identify primary mental health care service gaps within a stepped care approach
• develop approaches to new service areas to broaden the service mix, such as low intensity services and, and services for young people with severe mental illness
• promote a stepped care approach and better target appropriate referral to mental health and related services
• develop linkages with and between relevant services and supports
• establish mental health specific clinical governance arrangements
In 16-17 PHNs will be expected to:

10
Longer term PHNs will be expected to:
• implement the core elements of a stepped care approach
• plan, develop, target and/or commission services to achieve an appropriate service mix
• address the six priorities identified for the flexible funding pool within a stepped care approach
• ensure most efficient use of resources develop and implement efficient and timely service pathways
• actively promote use of the digital mental health gateway as a core element of a stepped care approach
• support GPs in their critical role in ensuring

11
Shifting focus & investment

12
PHN role in mental health reform1. Context of our work
2. Commissioning
3. Consumer engagement
4. Integration

13
Commissioning is “a strategic process of working with the market to co-design, co-deliver and actively manage services to most effectively and efficiently meet the needs and improve outcomes of a defined population within resources available”

14
1. Understand the needs of the community by analysing data, engaging and consulting with consumers, clinicians, carers and providers, peak bodies, community organisations and funders.
2. Engage with potential service providers well in advance of commissioning new services.
3. Putting outcomes for users at the heart of the strategic planning process.
4. Adopt a whole of system approach to meeting health needs and delivering improved health outcomes.
5. Understand the fullest practical range of providers including the contribution they could make to delivering outcomes and addressing market failure and gaps, and encourage diversity in the market.
6. Co-design solutions; engage with stakeholders, including consumer representatives, peak bodies, community organisations, potential providers and other funders, to develop evidence-based and outcome-focused solutions.
PHN Commissioning Principles

15
7. Consider investing in the capacity of providers and consumers, particularly in relation to hard-to-reach groups.
8. Ensure procurement and contracting processes are transparent and fair, facilitating the involvement of the broadest range of suppliers, including alternative arrangements such as consortia building where appropriate.
9. Manage through relationships; work in partnership, building connections at multiple levels of partner organisations and facilitate links between stakeholders.
10.Develop environments high in trust through collaborative governance, shared decision-making and collective performance management.
11.Ensure efficiency, value for money, and service enhancement.
12.Monitor and evaluate through regular performance reports; consumer, clinician, community and provider
PHN Commissioning Principles

16
Underpinning need for effective collaborations and partnerships

17

18
Our role beyond “health”
Impact on the health system is largely a function of the environment people live in
health environment

19
Critical success factors –some thoughts
• Shared vision and principles of operation
• Building on existing relationships, some formal
• Leadership and investment in developing change
• Providing consumers with great transparency about their options and progress in dealing with health issues
• Defining where existing silos/organisationsand “pitch in” and add value roles and responsibilities
• Allocating resources including systems and money
Small deliberate decisions on an ongoing

20
PHN role in mental health reform1. Context of our work
2. Commissioning
3. Consumer engagement
4. Integration

21
What We Know
Just one third of people experiencing mental health distress (illness) had received services for their mental health problems.
Two thirds of the people with a mental health problem did not seek help, with over 90% reported that they did not need services.
National Survey of Mental Health & Wellbeing 2009

22
75%
22%
3%
One disorder
Two disorders
Three disorders
Mental Health Comorbidity
National Survey of Mental Health & Wellbeing 2009
23
People Diagnosed with a Mental IllnessDie 10 – 32 Years younger than average (exc Suicide)
70% Unemployed (more than an other disability)
17% contact with friends or family 4 – 8 times per year
20% of people referred to MH Services are identified as having significant problems with their living conditions
3X more likely to be in debt that other people
More likely to be divorced and many never have children
National Report Care MHC 2012
24
Cultural Diversity
For recent arrivals from Somalia, Sri Lanka and Myanmar it is unlikely that relevant cultural issues will be understood and incorporated in to the treatment program.
Many Communities particularly, Asian Communities, access public mental health service at less that half the rate of the general population.
MHIMA 2013
25
There are gaps – a “missing middle”• Lack of high intensity day care
- Deskilling of the day care staff – shift to NGOs
• Lack of residential care (24 hours non medical support)
• Lack of community intensive residential care (24 hours medical support provided outside the hospital)
• Lack of comprehensive information in the non-health sector
- Housing: not able to know how many properties for people with MH problems
- Problem for indicator-based planning
• A reactive system, rather than proactive long term planning (based on short term care programs).
• High availability of services aimed at care coordination and mobile care
Western Sydney Mental Health Atlas 2015
26
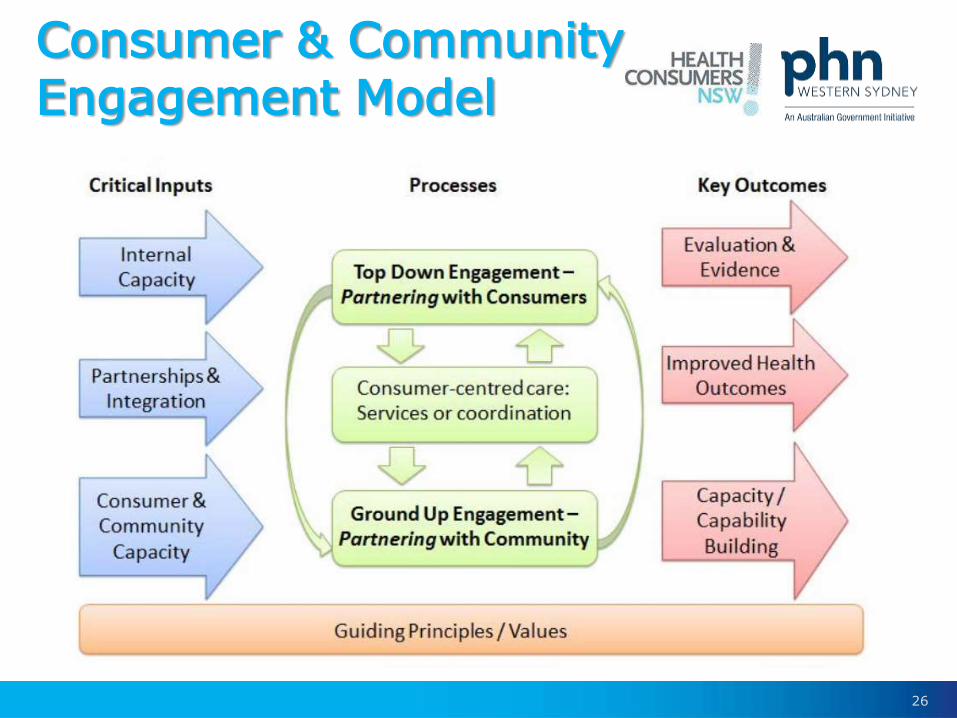
Consumer & Community Engagement Model

27
Consumers being involved at all levels• Investment of better literacy, support and
transparency of information• Governance, planning and design of
service provision• Evaluation of services • Opportunities for peer engagement
“Nothing about us without us”
Consumer centred co-design

28
PHN role in mental health reform1. Context of our work
2. Commissioning
3. Consumer engagement
4. Integration

29

30
A vision for our health system
Care, which imposes the patient’s perspective as the organising principle
of service delivery and makes redundant old supply-driven models of
care provision. Integrated care enables health and social care
provision that is flexible, personalised, and seamless.
(Lloyd & Wait 2005)The structure of service delivery should be a function what
we need now not the default of what has always been there

31
Defining an outcome from integration
At its heart , it can be defined as an approach that seeks to improve the quality of care
for individual patients, service users and carers by ensuring
that services are well co-ordinated around their needs
(Kings Fund 2012)“Improving the patient journey through developing integrated and coordinated services”

32
Strengthening building blocks of an integrated care system
Support with Enablers
Payment Governance Information Leadership Support
“Quadruple Aim”
Organise Delivery
Protocols
Care plans
Performancereview
Carecoordinationand delivery
Understand Needs
Low risk
Moderate risk
High risk
Very low risk
Very high risk

33
The Quadruple Aim of Effective Care
34
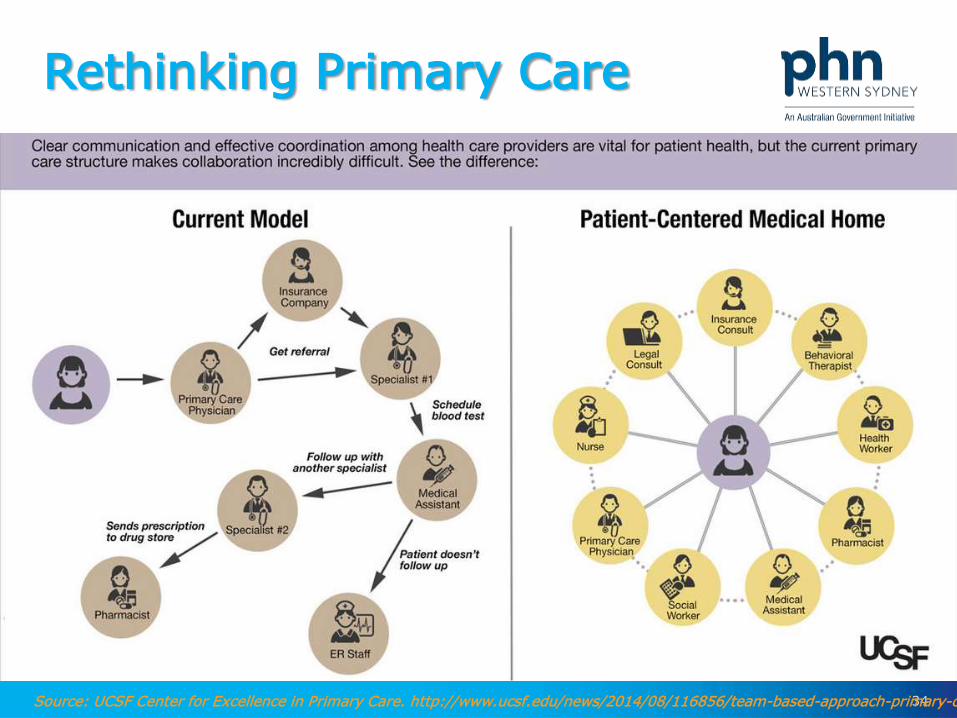
Rethinking Primary Care
Source: UCSF Center for Excellence in Primary Care. http://www.ucsf.edu/news/2014/08/116856/team-based-approach-primary-care
35
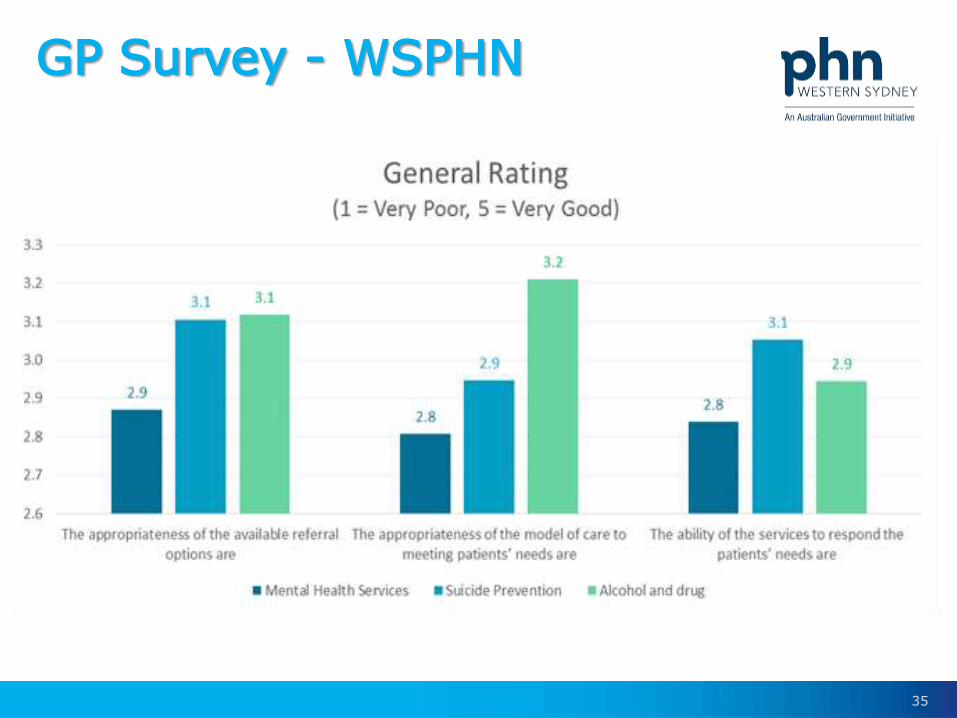
GP Survey - WSPHN

36
A shared care plan is a structured, comprehensive plan developed jointly by the patient and their
family/carer and health professional(s). It may include a
summary of personal health information, a person’s health
goals, and the treatment and follow up care they receive.
National Health IT Board NZ

37
Integration of mental health & primary care• Taking in account the local context
• Engaging in formal/informal partnerships
• Articulating governance/identifying leadership
• Reforming the way we pay
• Establishing (common) infrastructure
• Accounting for organisational culture
• Encouraging respectful communication
• Providing inter-professional education
• Reducing stigmatisation & discrimination
• Collecting data/information to assess quality
PCHRIS 2015

38
How do we integrate care?
Connecting/coordinating
AND
Changing/transforming

39
Thank you
@WKmet
40
As the Western Sydney Primary Health Network,WentWest is focused on addressing both regionaland national health challenges. Together withhealth professionals, partners from both thehealth and hospital sector, consumers and thebroader community, WentWest seeks to identifygaps and commission solutions for better healthoutcomes.