pg2-non-hazardous sterile preparations - · pdf filegap analysis – non‐hazardous...
TRANSCRIPT

Gap Analysis – Non-Hazardous Sterile Preparations Overview
The College has produced this Gap Analysis document based on the Community and Hospital Assessment Criteria. Criteria have been taken from the relevant legislation, policies,
guidelines or standards of practice. These gap analysis documents have been provided as tools to assist pharmacy professionals in assessing gaps in their sterile compounding
practice and determining next steps required to meet the Model Standards of Pharmacy Compounding for Non-Hazardous Sterile Preparations and Hazardous Sterile Preparations.
They can also be used to track and monitor progress. The documents are not meant to replace the standards.
If you have a practice assessment coming up, we encourage you to fill out the document ahead of time for discussion with your practice advisor. While the College does not require
you to fill out or submit this analysis, and you are welcome to use other resources that might be available, we believe it will be very helpful in ensuring that your pharmacy is
prepared for upcoming deadlines.
References:
Pharmacy Act, 1991; https://www.ontario.ca/laws/statute/91p36
Drug and Pharmacies Regulation Act, R.S.O. 1990; https://www.ontario.ca/laws/statute/90h04
NAPRA Model Standards for Pharmacy Compounding of Non-Hazardous Sterile Preparations, 2015;
http://www.napra.ca//Content_Files/Files/Mdl_Stnds_Pharmacy_Compounding_NonHazardous_Sterile_Preparations_Nov2016_Revised.pdf
OCP Guidelines for Compounding Preparations, 2006; http://www.ocpinfo.com/regulations-standards/policies-guidelines/compounding/
USP 797; http://www.usp.org/usp-healthcare-professionals/compounding
Instructions This document is a fillable PDF so you can either chose to complete it on a computer, or print it out and complete it by hand. Please do not complete the form online within your web browser; your data will not be saved. Please save it to your computer first, and then fill it out.
Criteria:
Each criteria has been taken from relevant legislation, policies, guidelines or standards of practice..
Criteria Components:
The criteria components column illustrates specific insights or activities required to ensure adherence to the criteria and is provided to assist practitioners in understanding expectations and preparing for a practice assessment.
Comments: Please add your notes relating to the criteria, or any comments or questions you would like to discuss with the Practice Advisor.
Pharmacy Name: …………………………………………………… Accreditation Number: ……………………………………… Date: ……………………………………
Overview
Gap Analysis – Non-Hazardous Sterile Preparations

Gap Analysis – Non‐Hazardous Sterile Preparations Page 1 of 13
Criteria Criteria Components / Guidance Comments
The pharmacy does not manufacture drug products.
The pharmacy does not manufacture drug products. The pharmacy is not in violation of the Food and Drug Regulations Division IA Establishment Licensing requirements.
There is a list of all recipients of compounded products prepared by the pharmacy
The pharmacist provides oversight for all pharmacy operations for all sterile drug compounding activities.
A pharmacist provides oversight of all sterile compounding activities. There is pharmacist oversight during pharmacy hours of operation and there is coverage on evening and weekends during leaves of absence including vacations, etc.
The pharmacy has a policy specifying which parenteral medication products must be prepared by pharmacy staff in a LAFW/CAI.
The pharmacy has a list of sterile compounded products that are prepared by pharmacy.
The pharmacist provides preparation instructions and administration information when a medication for parenteral use is dispensed for a care provider to prepare.
Preparation instructions and administration information for medication is accessible if the information is not provided on the medication label.
The pharmacy has a system to assess and update policies and procedures to ensure consistency with current standards and best practices for sterile compounding of non‐hazardous drugs.
The pharmacy has a system to ensure policies and procedures are routinely reviewed and updated to comply with current standards for sterile compounding of non‐hazardous drugs.
The pharmacy has the current version of the NAPRA compounding standards, USP 797 or other relevant references.
Policies and procedures related to the sterile compounding of non‐hazardous drugs meet current standards. (e.g. assignment of BUDs, personnel training, personnel and environmental monitoring and facility cleaning)
The pharmacy has a policy in place to specify the dating of single dose and multi‐dose vials in the compounding of sterile products.
The pharmacy has a policy that meets the NAPRA compounding standards and USP 797.
The pharmacy ensures that ingredients used for sterile compounding are of established quality and standards.
The pharmacy has written procedures to verify the correct identity, quality, and amounts of ingredients used in sterile compounded products that have not been already approved for use by Health Canada.
Active pharmaceutical ingredients (API) used in compounding meet an acceptable pharmacopeia standard (e.g. USP, NF) for human consumption.
Gap Analysis – Non‐Hazardous Sterile Preparations Page 2 of 13
The pharmacy personnel receive appropriate orientation and the required training to premises‐specific procedures and equipment, relevant to the services provided.
The pharmacy has a process to ensure the pharmacist, pharmacy technician and/or other pharmacy staff work within their scope of practice, duties and competencies.
The orientation and training materials are sufficiently detailed to ensure consistency of practice/reproducibility of process (that comply with standards) and they are used as a reference and a standard for all staff after their training period.
Orientation and training processes are documented.
The sterile compounding supervisor must have successfully completed training.
Staff is provided with access to appropriate medication information resources, current protocols, clinical guidelines and dosing recommendations required for sterile compounding of non‐hazardous drugs.
The medication information resources available to pharmacy staff are appropriate for services provided and patient populations cared for.
Pharmacy staff are knowledgeable of, and know how to access the resources available.
Staff members wear appropriate personal protective equipment (PPE) in accordance with standards required for sterile compounding of non‐hazardous drugs.
Compounding personnel comply with hand and forearm hygiene and PPE standards for sterile compounding including the conduct when entering the cleanroom and anteroom beyond the demarcation area.
The pharmacy has a policy in place to ensure the use of Sterile Isopropyl Alcohol (IPA) for the disinfection of surfaces/ equipment/ supplies used in the compounding of sterile products.
The pharmacy has a policy that meets the NAPRA compounding standards and USP 797.
The pharmacy requires sterile IPA wipes.
The pharmacy requires single use sterile IPA bottles. (i.e. no refilling)
The pharmacy must use only sterile IPA in the cleanroom.
The pharmacy has a policy for the cleaning and disinfection of sterile compounding areas in accordance with established standards.
The pharmacy has a policy for the cleaning and disinfection of sterile compounding areas in accordance with established standards.
Cleaning staff are trained prior to performing cleaning and disinfection activities in sterile compounding areas in accordance with established standards.
Cleaning staff received appropriate training according to established standards which is documented and retained for 10 years.
Gap Analysis – Non‐Hazardous Sterile Preparations Page 3 of 13
The pharmacy has a policy and procedure for quality assurance and environmental verification in accordance with established standards.
The pharmacy has a policy and procedure for quality assurance and environmental verification in accordance with established standards.
The pharmacy has a process to monitor environmental controls, personnel and equipment as required by NAPRA standards and USP 797.
The pharmacy is able to provide rationale and supporting records related to environmental control measures undertaken in each compounding area.
The pharmacy is able to provide rationale and supporting records related to environmental control measures undertaken in each compounding area.
Policies and procedures establish alert and action limits, corrective actions and required documentation of corrective actions if excursion of action limits occurs.
Action plans developed, corrective actions taken and results of re‐testing are documented after non‐compliant results of quality monitoring.

Gap Analysis – Non‐Hazardous Sterile Preparations Page 4 of 13
Compounded Sterile Product (CSP) Preparation
A master formula record developed by a pharmacist is retained for each sterile compounded drug product.
The pharmacy has a policy that ensures master formulas are developed, reviewed and updated by a pharmacist and specify ingredients, compounding processes and references.
There is a process used to ensure sterile compounding procedures and assigned beyond use dates are compliant with the NAPRA compounding standards and USP 797.
Pharmacy staff compound CSP's following the sequence of steps and processes specified in the master formula, and in policies and procedures.
Records are retained for a time period not less than 10 years from the last professional pharmacy service.
Compounding related records are retained for 10 years after the expiry date of the sterile compounded product dispensed.
All records are readily retrievable.
The pharmacy ensures a system of auditability and traceability to the patient for each CSP.
The pharmacy ensures a system of auditability and traceability to the patient for each bulk or patient specific product.
The pharmacy is able to identify; each component used, the individual(s) providing final verification, the patient receiving the compounded product, the date/amount/quantity received and the manufacturer, lot and expiry date for each sterile compounded product dispensed.
Written policies and procedures are in place for CSP labels that comply with standards and are consistent.
Written policies and procedures are in place for CSP labels that comply with standards and are consistent.
The pharmacy has policies and procedures for labelling compounded bulk sterile products.
The pharmacy has policies and procedures for labelling patient specific CSPs.

Gap Analysis – Non‐Hazardous Sterile Preparations Page 5 of 13
The pharmacy has quality control mechanism in place for the final product.
The Pharmacy has quality control mechanism in place for the final product.
The pharmacy has a system to validate that the correct ingredients and quantities are added to the final product.
The pharmacy has a process for performing a final check on compounded sterile products.
The final product is tamper evident until administered to the patient.
Staff are trained on the process.
The pharmacy performs and documents periodic quality assurances of the sterile compounding and distribution processes.
The compounding supervisor performs and documents periodic quality assurances of the sterile compounding and distribution processes.
The pharmacy administrator/designate or Designated Manager perform assessments of sterile compounding practices and environment to comply with standards and policies and procedures.
Periodic quality assurances are documented and records retained for 10 years.
Staff performance is assessed for continued ongoing competency and after return to work from an extended leave.
Staff performance is assessed for continued ongoing competency and after return to work from an extended leave.
The pharmacy monitors staff engaged in compounding as required by the NAPRA compounding standards and USP 797. The frequency of this monitoring/assessment meets standards as determined by risk level assigned to the sterile compounded product.
Assessment includes gloved fingertip sampling and media fill and didactic session including successful completion of questionnaire for compounding personnel.
Assessment includes didactic session including successful completion of questionnaire for personnel who check/verify sterile compounded products.
Policies and procedures specify random periodic audits, the frequency of audits, individuals and the components audited (e.g. what is audited specifically). Audits are documented and records retained for 10 years.

Gap Analysis – Non‐Hazardous Sterile Preparations Page 6 of 13
The pharmacy has a system to report, investigate and follow up on medication incidents, drug related incidents and adverse drug reactions related to CSPs.
The pharmacy has a system to report, investigate and follow up on medication incidents.
The pharmacy has a system to report, investigate and follow up on drug related incidents.
The pharmacy has a system to report, investigate and follow up on adverse drug reactions.
A pharmacist in a management role reviews all incidents and adverse drug reactions related to compounded sterile drug products in a timely manner to determine patterns and causal factors that contribute to patient risks.
A pharmacist in a management role reviews all incidents and adverse drug reactions related to compounded sterile drug products in a timely manner to determine patterns and causal factors that contribute to patient risks.
The pharmacy has a process to identify and resolve drug‐related incidents, medication incidents and adverse drug events and meets requirements outlined in NAPRA standards.
Education is provided to pharmacy staff about incidents related to compounded sterile preparations.
Education is provided to pharmacy staff about incidents related to compounded sterile preparations.
Staff are educated on reporting criteria and procedures to submit adverse drug reactions related to CSPs to Health Canada and the manufacturer.
Gap Analysis – Non-Hazardous Sterile Preparations Page 7 of 13
Specialized Sterile Compounding
Pharmacy maintains a list of specialized CSPs The pharmacy has a list of specialized sterile
compounded products that are prepared by pharmacy.
Compounding personnel preparing specialized CSPs receive specialized training to obtain the required competencies.
Compounding personnel preparing specialized CSPs receive specialized training to obtain the required competencies.
Competency assessment is completed annually and documented.
Policies and procedures for compounding all CSPs are sufficiently detailed to prevent process variation in practice among compounding personnel.
Policies and procedures for compounding all CSPs are sufficiently detailed to prevent process variation in practice among compounding personnel and comply with standards. These policies and procedures are readily available for staff reference after training.
Master formula records are standardized, developed by a pharmacist and are used to guide the compounding of specialized CSPs.
The pharmacy has a policy that ensures master formulas are developed, reviewed and updated by a pharmacist; and specify ingredients, compounding processes and references.
The process used to determine compounding procedures and beyond use date is compliant with the NAPRA compounding standards and USP 797.
Pharmacy staff compound non-sterile products following the sequence of steps and processes specified in the formula, and in policies and procedures.
For pharmacies using IV workflow software, there are policies and procedures that ensure that the final check of the programming has been completed by a pharmacist who is an expert or super user, prior to using the program for dispensing.
For pharmacies using IV workflow software, there are policies and procedures that ensure that the final check of the programming has been completed by a pharmacist who is an expert or super user, prior to using the program for dispensing.
For pharmacies using automated IV compounding devices, there are standard operating procedures.
For pharmacies using automated IV compounding devices, there are standard operating procedures.
Only trained personnel can use the automated IV compounding devices to compound. This training is documented and records are retained for 10 years.
Gap Analysis – Non‐Hazardous Sterile Preparations Page 8 of 13
There is a policy and procedure for final verification of all CSP.
The pharmacy has a policy and procedure for verifying manually prepared CSP's.
The pharmacy has a policy and procedure for verifying CSPs prepared using automation, and address; performing a visual check to verify the accuracy of all diluents and drugs, the steps that must be checked, the parameters at each step as well as the individuals and include documentation.
Gap Analysis – Non‐Hazardous Sterile Preparations Page 9 of 13
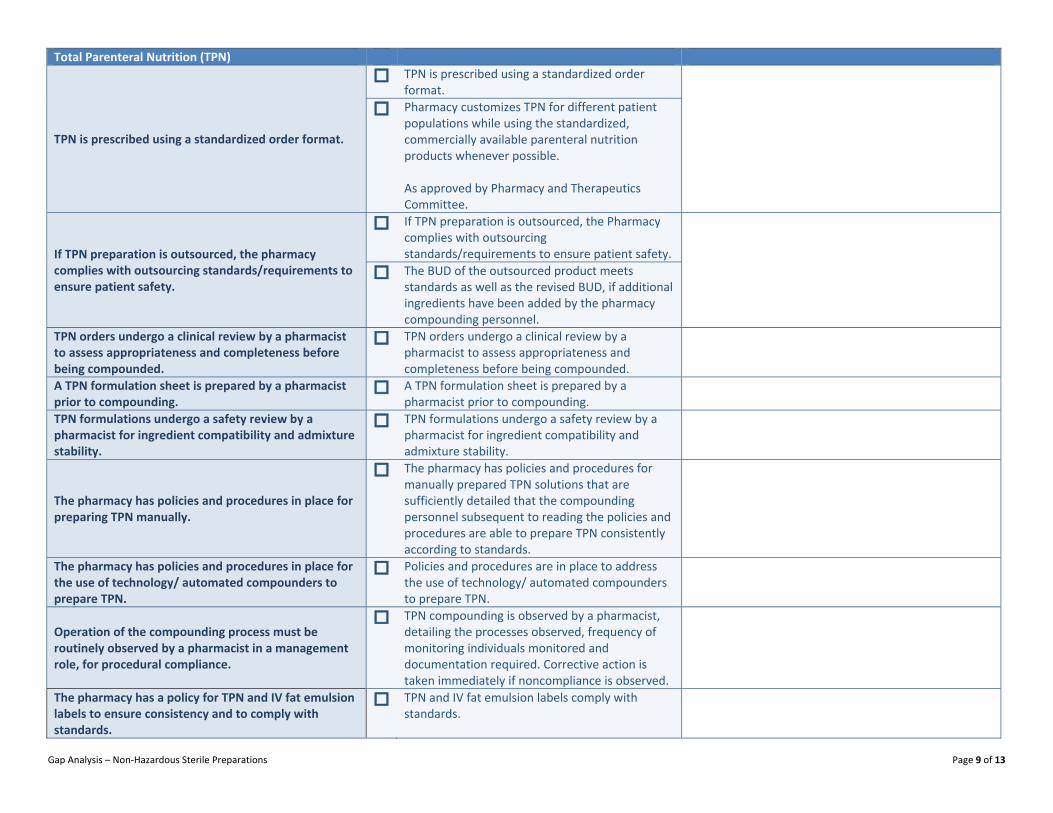
Total Parenteral Nutrition (TPN)
TPN is prescribed using a standardized order format.
TPN is prescribed using a standardized order format.
Pharmacy customizes TPN for different patient populations while using the standardized, commercially available parenteral nutrition products whenever possible. As approved by Pharmacy and Therapeutics Committee.
If TPN preparation is outsourced, the pharmacy complies with outsourcing standards/requirements to ensure patient safety.
If TPN preparation is outsourced, the Pharmacy complies with outsourcing standards/requirements to ensure patient safety.
The BUD of the outsourced product meets standards as well as the revised BUD, if additional ingredients have been added by the pharmacy compounding personnel.
TPN orders undergo a clinical review by a pharmacist to assess appropriateness and completeness before being compounded.
TPN orders undergo a clinical review by a pharmacist to assess appropriateness and completeness before being compounded.
A TPN formulation sheet is prepared by a pharmacist prior to compounding.
A TPN formulation sheet is prepared by a pharmacist prior to compounding.
TPN formulations undergo a safety review by a pharmacist for ingredient compatibility and admixture stability.
TPN formulations undergo a safety review by a pharmacist for ingredient compatibility and admixture stability.
The pharmacy has policies and procedures in place for preparing TPN manually.
The pharmacy has policies and procedures for manually prepared TPN solutions that are sufficiently detailed that the compounding personnel subsequent to reading the policies and procedures are able to prepare TPN consistently according to standards.
The pharmacy has policies and procedures in place for the use of technology/ automated compounders to prepare TPN.
Policies and procedures are in place to address the use of technology/ automated compounders to prepare TPN.
Operation of the compounding process must be routinely observed by a pharmacist in a management role, for procedural compliance.
TPN compounding is observed by a pharmacist, detailing the processes observed, frequency of monitoring individuals monitored and documentation required. Corrective action is taken immediately if noncompliance is observed.
The pharmacy has a policy for TPN and IV fat emulsion labels to ensure consistency and to comply with standards.
TPN and IV fat emulsion labels comply with standards.
Gap Analysis – Non‐Hazardous Sterile Preparations Page 10 of 13
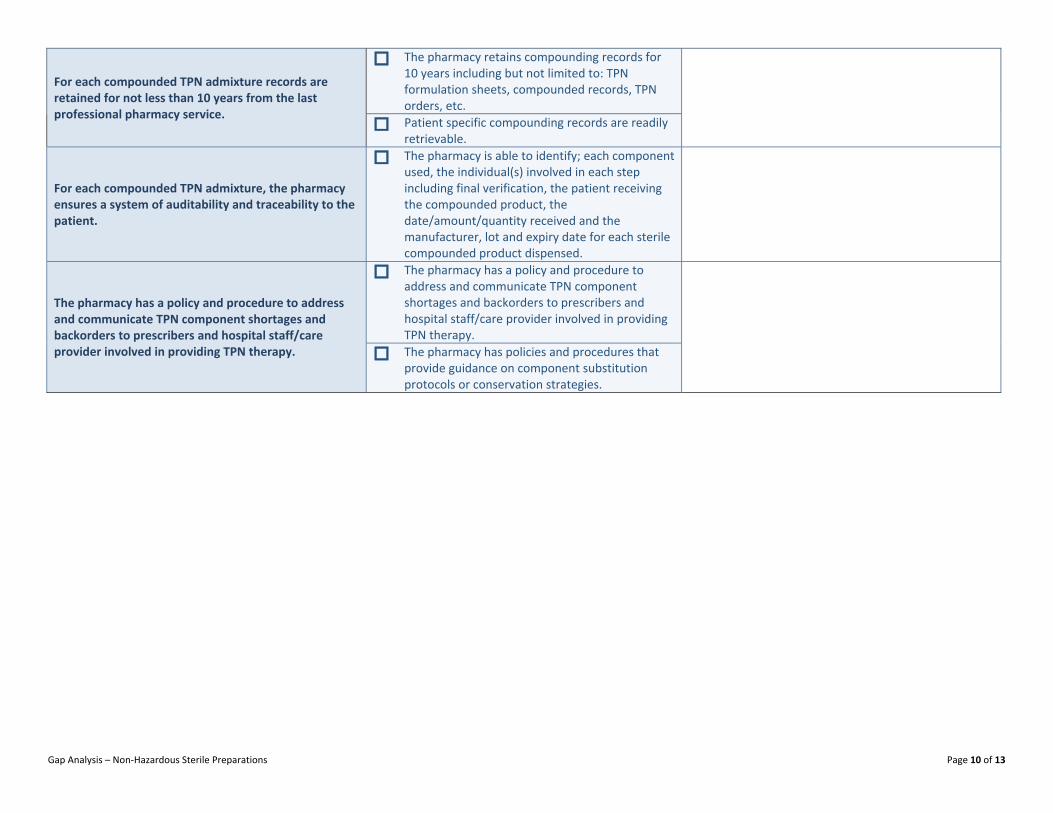
For each compounded TPN admixture records are retained for not less than 10 years from the last professional pharmacy service.
The pharmacy retains compounding records for 10 years including but not limited to: TPN formulation sheets, compounded records, TPN orders, etc.
Patient specific compounding records are readily retrievable.
For each compounded TPN admixture, the pharmacy ensures a system of auditability and traceability to the patient.
The pharmacy is able to identify; each component used, the individual(s) involved in each step including final verification, the patient receiving the compounded product, the date/amount/quantity received and the manufacturer, lot and expiry date for each sterile compounded product dispensed.
The pharmacy has a policy and procedure to address and communicate TPN component shortages and backorders to prescribers and hospital staff/care provider involved in providing TPN therapy.
The pharmacy has a policy and procedure to address and communicate TPN component shortages and backorders to prescribers and hospital staff/care provider involved in providing TPN therapy.
The pharmacy has policies and procedures that provide guidance on component substitution protocols or conservation strategies.
Gap Analysis – Non‐Hazardous Sterile Preparations Page 11 of 13
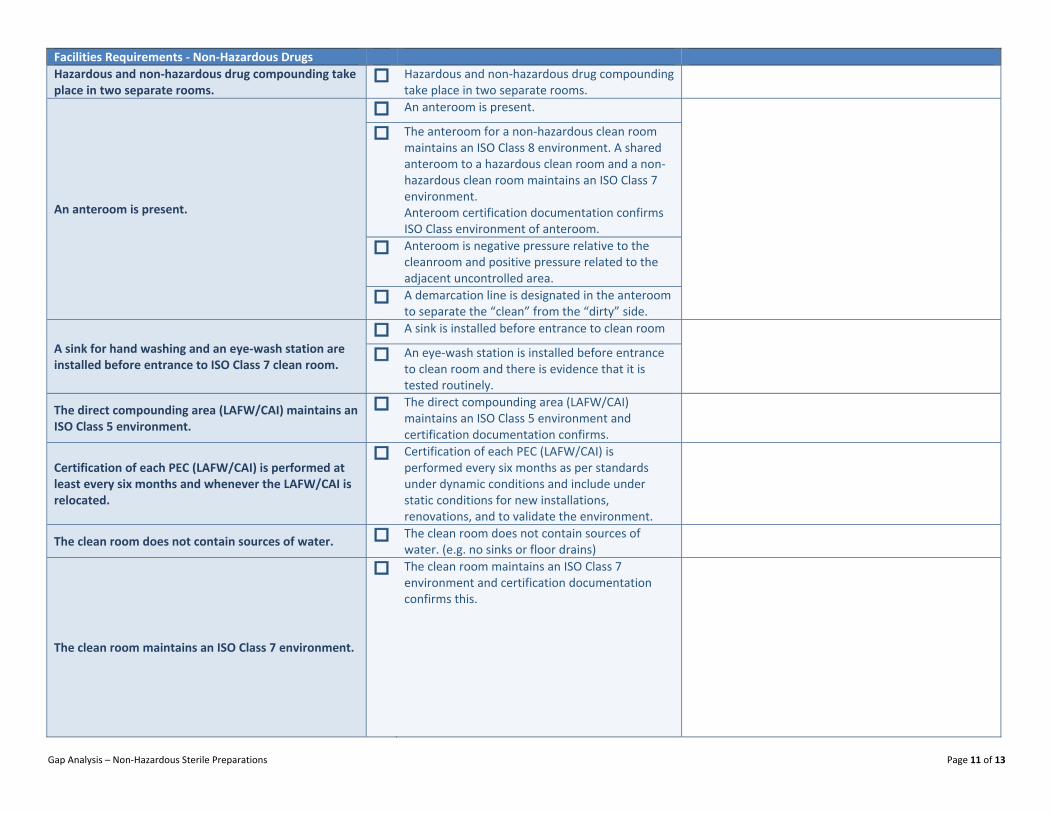
Facilities Requirements ‐ Non‐Hazardous Drugs Hazardous and non‐hazardous drug compounding take place in two separate rooms.
Hazardous and non‐hazardous drug compounding take place in two separate rooms.
An anteroom is present.
An anteroom is present.
The anteroom for a non‐hazardous clean room maintains an ISO Class 8 environment. A shared anteroom to a hazardous clean room and a non‐ hazardous clean room maintains an ISO Class 7 environment. Anteroom certification documentation confirms ISO Class environment of anteroom.
Anteroom is negative pressure relative to the cleanroom and positive pressure related to the adjacent uncontrolled area.
A demarcation line is designated in the anteroom to separate the “clean” from the “dirty” side.
A sink for hand washing and an eye‐wash station are installed before entrance to ISO Class 7 clean room.
A sink is installed before entrance to clean room
An eye‐wash station is installed before entrance to clean room and there is evidence that it is tested routinely.
The direct compounding area (LAFW/CAI) maintains an ISO Class 5 environment.
The direct compounding area (LAFW/CAI) maintains an ISO Class 5 environment and certification documentation confirms.
Certification of each PEC (LAFW/CAI) is performed at least every six months and whenever the LAFW/CAI is relocated.
Certification of each PEC (LAFW/CAI) is performed every six months as per standards under dynamic conditions and include under static conditions for new installations, renovations, and to validate the environment.
The clean room does not contain sources of water. The clean room does not contain sources of water. (e.g. no sinks or floor drains)
The clean room maintains an ISO Class 7 environment.
The clean room maintains an ISO Class 7 environment and certification documentation confirms this.

Gap Analysis – Non‐Hazardous Sterile Preparations Page 12 of 13
Certification of the clean room is performed at a frequency as per standards.
Certification of the clean room is performed every six months as per standards under dynamic conditions and include under static conditions for new installations, renovations, and to validate the environment.
Test results include viable and non‐viable air particle sampling, surface sampling as well as the results of a smoke test that demonstrates unidirectional flow of air.
HEPA‐filtered air is introduced at the ceiling with returns to be low mounted on the wall to create a top‐down dilution.
HEPA‐filtered air is introduced at the ceiling with returns to be low mounted on the wall to create a top‐down dilution in the clean room.
HEPA‐filtered air is introduced at the ceiling with returns to be low mounted on the wall to create a top‐down dilution in the anteroom.
Clean room air pressure is positive relative to all adjacent spaces.
Clean room air pressure is positive relative to all adjacent spaces. Documentation confirms this.
Differential pressures are monitored daily.
There is a log (manual or electronic) of differential pressures monitored daily.
An audible alarm warns staff when the pressure cascade is compromised.
Staff are aware of and comply with the policy and procedure addressing alarm warnings.
Ceiling/flooring/equipment/chairs shall be non‐porous, smooth, free of cracks, non‐shedding, cleanable and disinfectable.
All surfaces are non‐porous, non‐shedding, smooth and free of cracks, cleanable and disinfectable in the clean room.
All surfaces are non‐porous, non‐shedding, smooth and free of cracks, cleanable and disinfectable in the anteroom.
Dust‐collecting overhangs, such as ceiling pipes and window‐sills are not in evidence.
All surfaces are non‐porous, non‐shedding, smooth and free of cracks, cleanable and disinfectable in the clean room.
All surfaces are non‐porous, non‐shedding, smooth and free of cracks, cleanable and disinfectable in the anteroom.
Gap Analysis – Non‐Hazardous Sterile Preparations Page 13 of 13
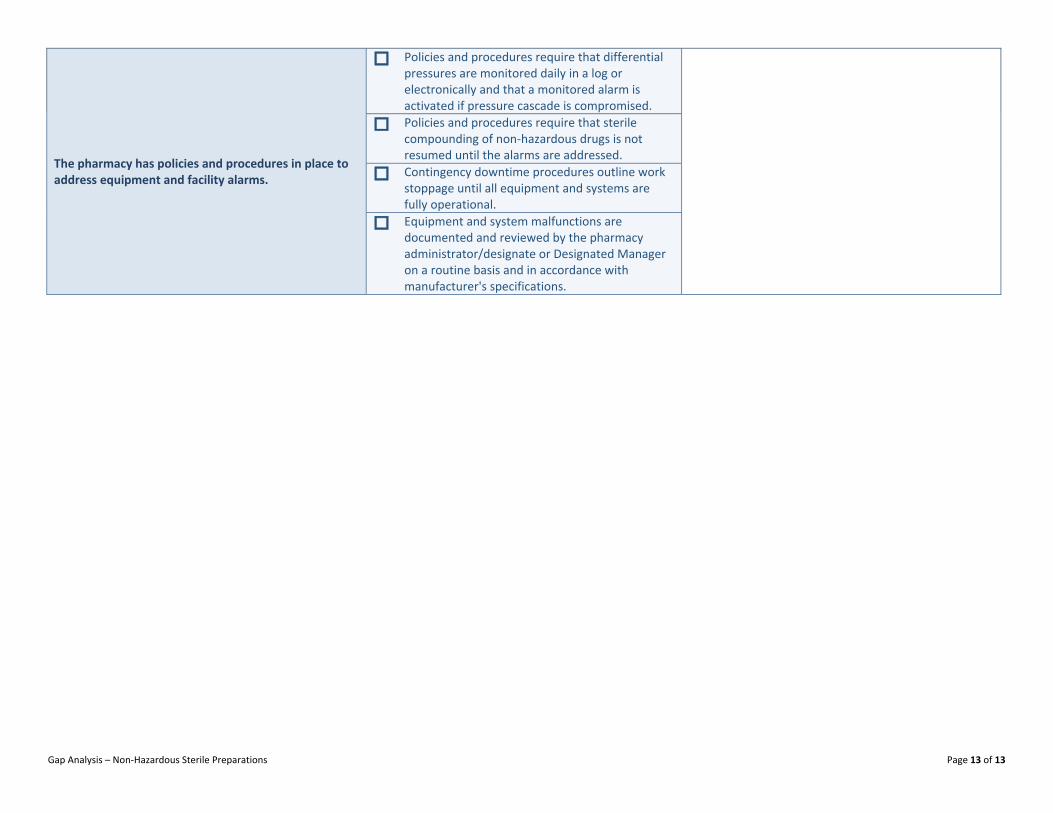
The pharmacy has policies and procedures in place to address equipment and facility alarms.
Policies and procedures require that differential pressures are monitored daily in a log or electronically and that a monitored alarm is activated if pressure cascade is compromised.
Policies and procedures require that sterile compounding of non‐hazardous drugs is not resumed until the alarms are addressed.
Contingency downtime procedures outline work stoppage until all equipment and systems are fully operational.
Equipment and system malfunctions are documented and reviewed by the pharmacy administrator/designate or Designated Manager on a routine basis and in accordance with manufacturer's specifications.