peripheral neuropathy david saperstein, md
TRANSCRIPT
Peripheral Neuropathy
David Saperstein, MDDirector, Center for Complex Neurology, EDS & POTS
Clinical Assoc Prof. of Neurology, Univ. of AZ College of MedicinePhoenix, AZ

Disclosures
• Chief Medical Officer, Neuropath Diagnostics
• Will discuss off-label treatment of small fiber neuropathy with IVIG
EDS/HSD and Peripheral Neuropathy?
• Numbness & tingling are common symptoms in those with EDS/HSD• 63% (468/747) of patients seen in my center for EDS/HSD over last 2 yrs• Usually this is a peripheral nerve issue• Most common causes of these symptoms:
• Increased susceptibility to pressure• Small fiber neuropathy• Compression/Entrapment neuropathies

Peripheral Neuropathy in EDS/HSD
• Some form of neuropathy is common• Typically only sensory manifestations• Frequently involves only small nerve fibers• Has not been well studied



What is Peripheral Neuropathy?
• Any disorder that affects peripheral nervous system• Radiculopathy• Plexopathy• Focal neuropathy• Polyneuropathy

Cutaneous Distributions of Nerve and Roots

Different Patterns of Neuropathy
Common Symptoms of Peripheral Neuropathy
• Numbness and tingling• Pain• Impaired balance• Weakness

Sorting it Out
• Brain and spine• History, exam, imaging
• Root• History, exam, imaging, NCS/EMG
• Plexus• History, exam, imaging, NCS/EMG
• Nerve• History, exam, NCS/EMG, skin biopsy, autonomic testing
Examination in Peripheral Neuropathy
• Sensory• Light touch, pinprick ± temperature• Timed vibration• Joint position sense• Romberg
• Reflexes• Strength• Gait
Electromyography (EMG) Made Simple
• When most people refer to “EMG” they are referring to both nerve conduction studies (NCS) and EMG. • NCS use electrical stimuli to test nerve function. • EMG uses needle electrodes inserted into muscle
to record muscle fiber signals.• Can identify nerve or muscle pathology.• Can show patterns of nerve or root involvement.• Abnormalities from nerve problems not seen before ~ 2-3 weeks.

Nerve Conduction Studies• Three parameters are measured:• latency • conduction velocity• amplitude

If Exam and NCS/EMG are Normal
• Pretty much excluded• Large or mixed fiber polyneuropathy
• Unlikely• Entrapment neuropathy
• Not excluded• Root• Plexus (muscular thoracic outlet syndrome)• Small fiber neuropathy

Small Fiber Neuropathy

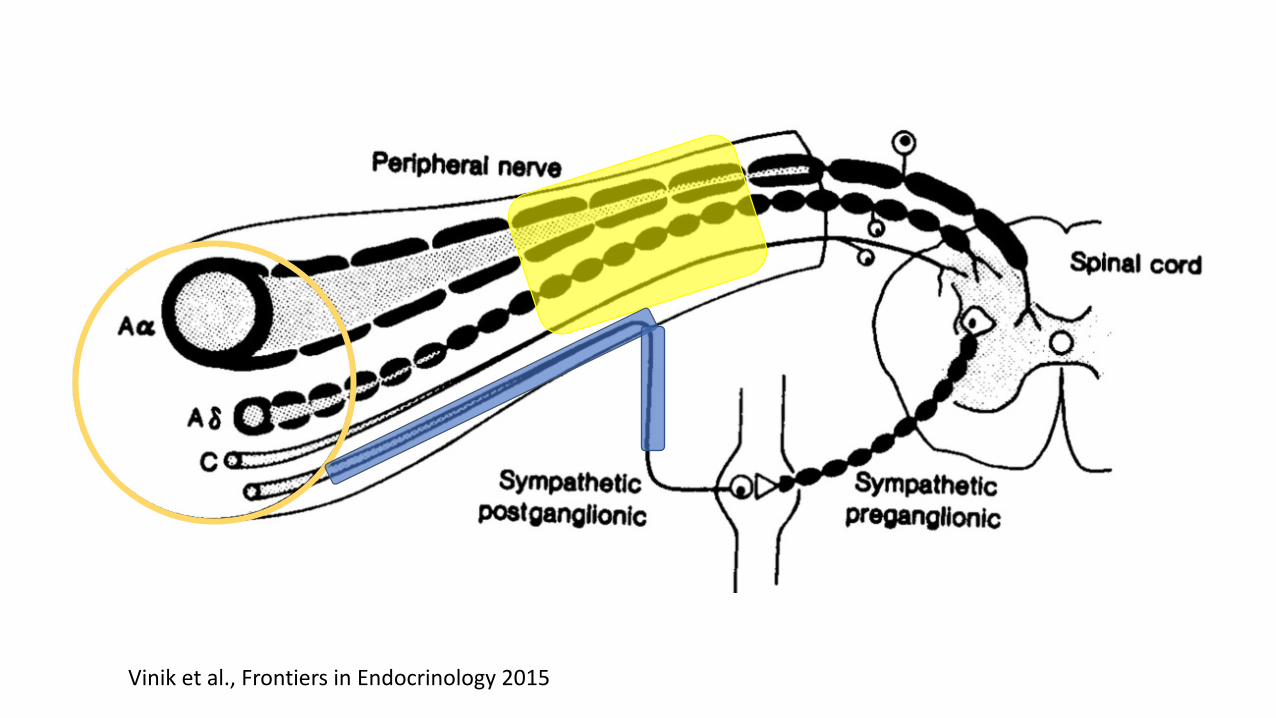
Sensory Nerve Fiber Types
Fiber Type Diameter (µm) C.V. (m/s) Modality
A-alpha 13-20 80-120 proprioception
A-beta 6-12 35-75 touch
A-delta 1-5 5-35 pain, temperature
C 0.2-1.5 0.5-2.0 pain, temperature

Sensory Nerve Fiber Types
Fiber Type Diameter (µm) C.V. (mph) Modality
A-alpha 13-20 4.5 proprioception
A-beta 6-12 3.0 touch
A-delta 1-5 1.0 pain, temperature
C 0.2-1.5 0.07 pain, temperature

Vinik et al., Frontiers in Endocrinology 2015
Vinik et al., Frontiers in Endocrinology 2015

What is Meant by Small Fiber Neuropathy?
• Neuropathy affecting exclusively small nerve fibers• Most neuropathies are “mixed” (large and small fibers)
Small Fiber Neuropathy (SFN)
• Frequently cause pain• Large fiber modalities unaffected• Nerve conduction studies (NCS/EMG) normal• Autonomic neuropathy may coexist• Autonomic symptoms in 25% (25/101)
• Retrospective study (MacDonald et al., Muscle & Nerve 2018)

Small Fiber Neuropathy (SFN)
• Sensory exam may be completely normal in ~35% of cases1
• Symptoms may be intermittent2
• Not always painful1,3• 12-30% without pain
• Often non-length dependent2• 30 to 50%
1Devigili et al., Brain 20082Saperstein et al., Int J Neuroscience 20133Thaisetthawatkul et al., Neurol Sci. 2014

Small Fiber Neuropathy (SFN)
• Sensory exam may be completely normal in ~35% of cases1
• Symptoms may be intermittent2
• Not always painful1,3• 12-30% without pain
• Often non-length dependent2• 30 to 50%
1Devigili et al., Brain 20082Saperstein et al., Int J Neuroscience 20133Thaisetthawatkul et al., Neurol Sci. 2014

Non-Length Dependent SFN• Those with non-length dependent SFN are more likely to:• be female• be younger• have an immune-mediated cause
Small Fiber NeuropathyExam Findings
• Normal strength• Normal deep tendon reflexes• Normal proprioception• Normal vibratory sensation
• Usually decreased pinprick, light touch• patients may have normal exams

Causes of SFN
• Idiopathic • Diabetes/impaired glucose tolerance• Sjogren’s Syndrome, other autoimmune diseases• Sarcoidosis• Vitamin B12 deficiency• Celiac Disease• HIV• Hepatitis C• Amyloidosis• Chemotherapy• Genetic
• Amyloidosis, Fabry’s, sodium channelopathies, EDS??

2016
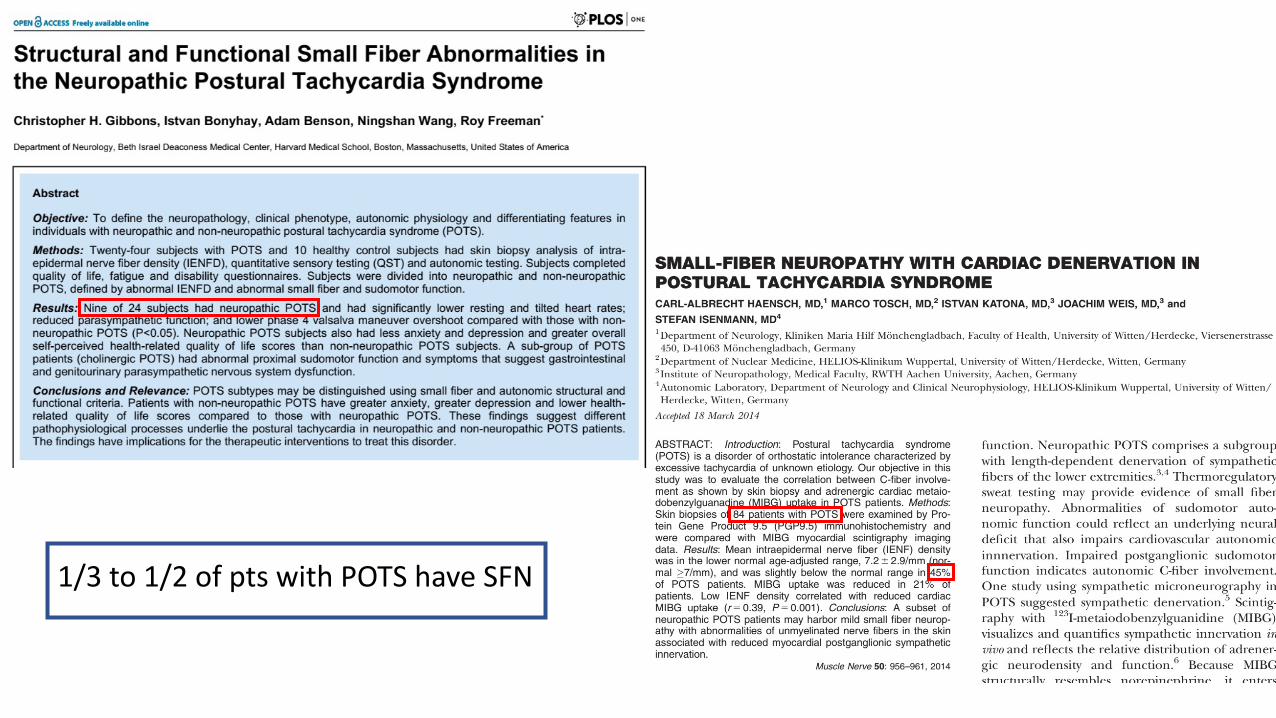
1/3 to 1/2 of pts with POTS have SFN

Testing Options for SFN
• Quantitative sensory testing (QST)• Autonomic testing• Skin biopsy• Confocal corneal microscopy• Other• Laser evoked potentials (LEPs)• Contact heat evoked potentials (CHEPs)
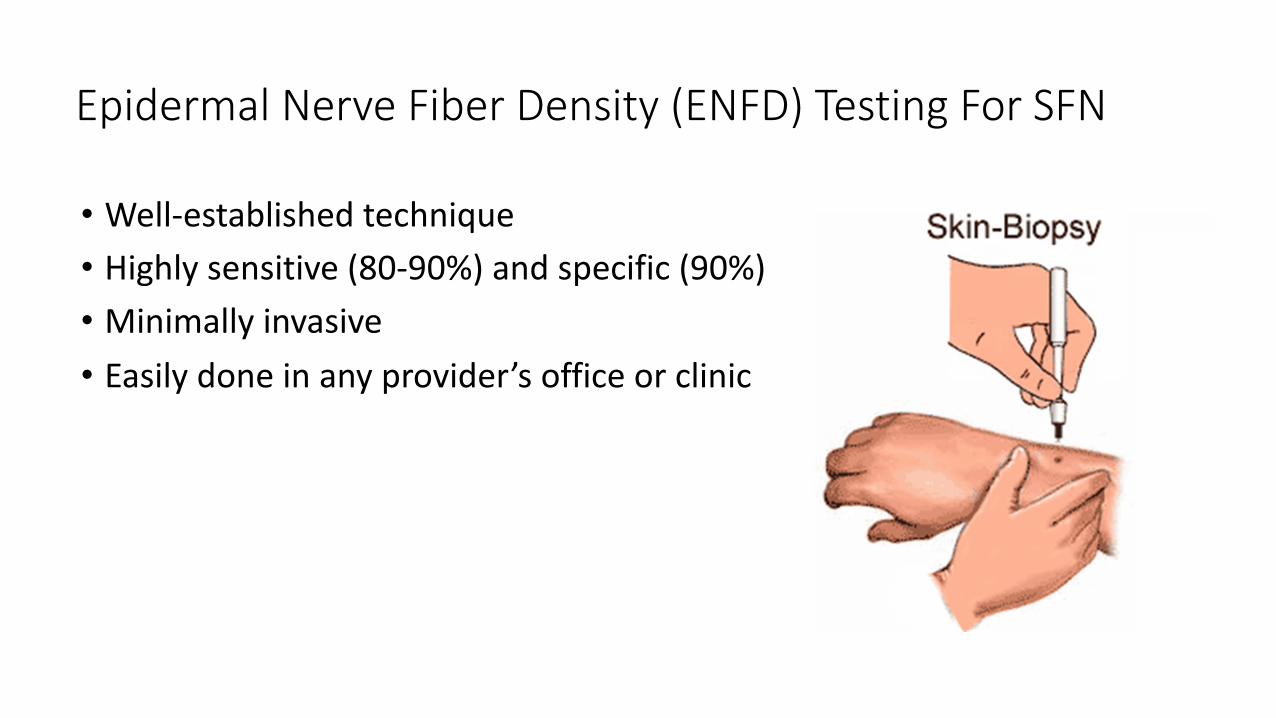
Epidermal Nerve Fiber Density (ENFD) Testing For SFN
• Well-established technique• Highly sensitive (80-90%) and specific (90%)• Minimally invasive• Easily done in any provider’s office or clinic

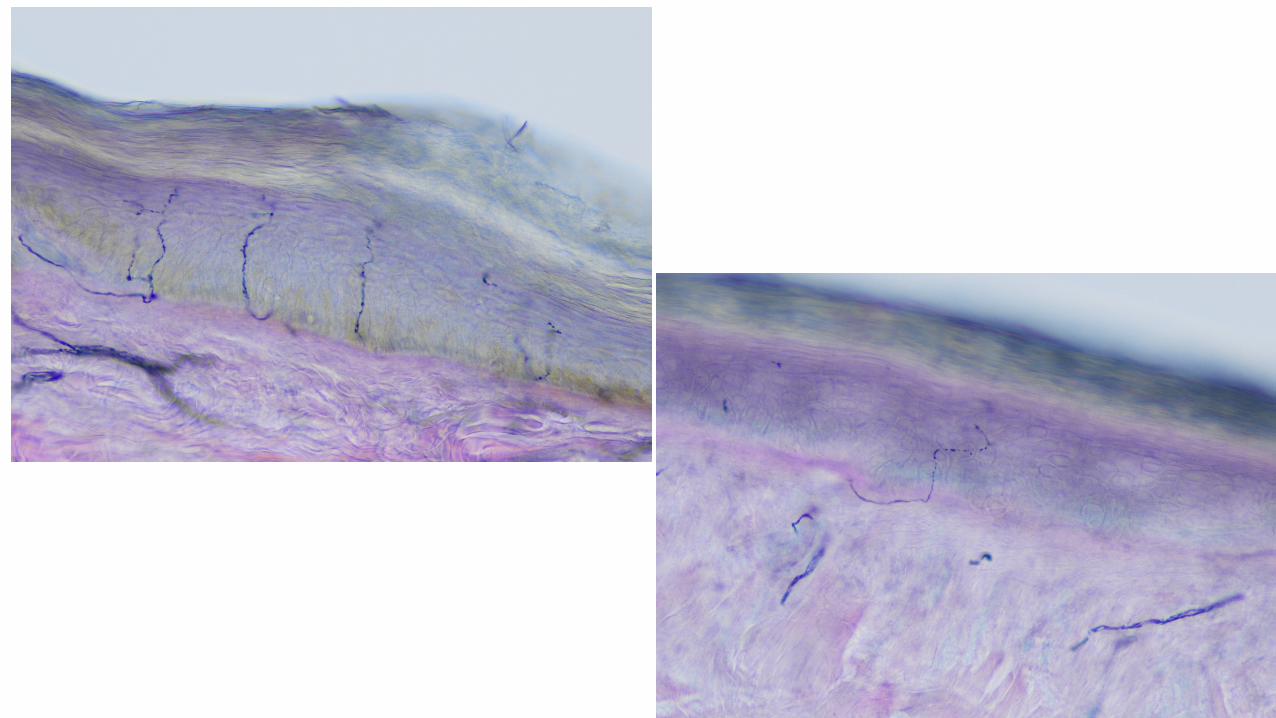
ENFD Testing For SFN
• Specimens placed in fixative• Shipped overnight to lab• Frozen sections, thick• Several day immunostaining process (PGP 9.5)• Manually counted

ENFD Testing For Small Fiber Neuropathy
• Well-established normative data• by convention abnormal is < than 5th percentile• differ by age and gender
• Multiple biopsy sites encouraged to assess length-dependency
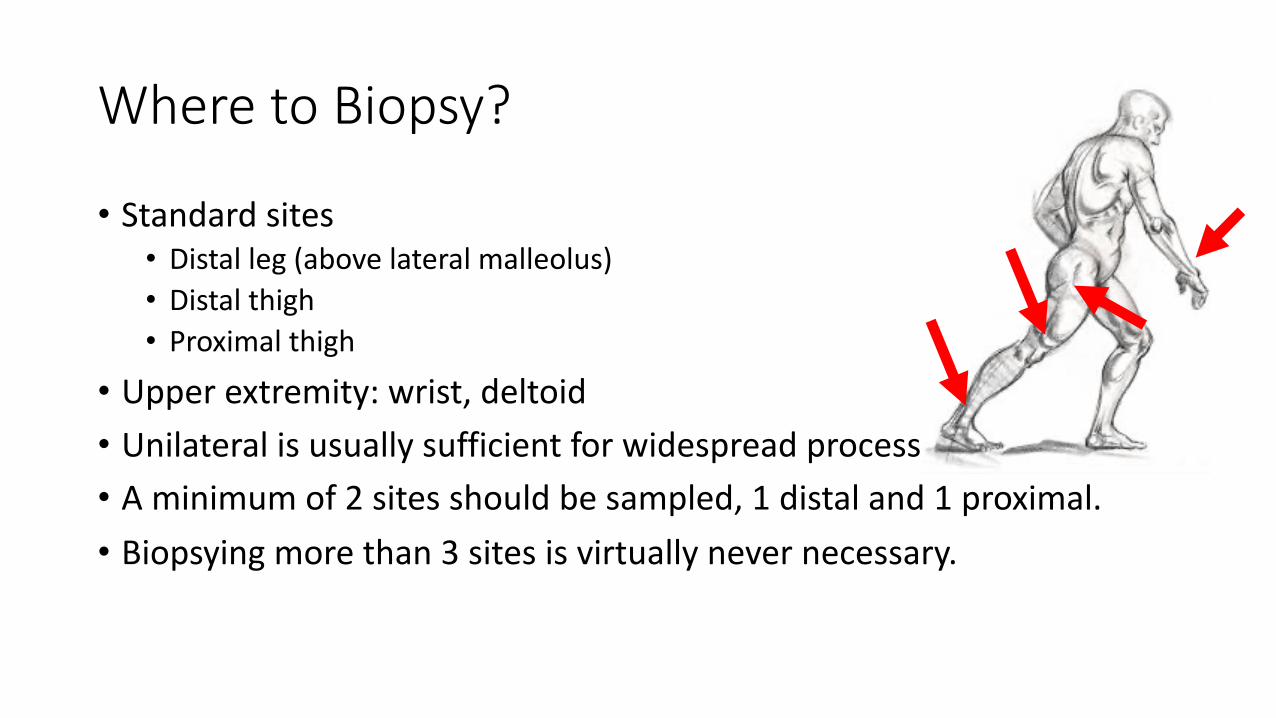
Where to Biopsy?
• Standard sites• Distal leg (above lateral malleolus)• Distal thigh• Proximal thigh
• Upper extremity: wrist, deltoid• Unilateral is usually sufficient for widespread process• A minimum of 2 sites should be sampled, 1 distal and 1 proximal. • Biopsying more than 3 sites is virtually never necessary.

When Skin Biopsy Testing is Normal
• Patients with suspected SFN but normal ENFD can show abnormal QST or QSART1,2
• It is not clear how often QST or QSART are abnormal when ENFD is normal• These different tests have additional value for diagnosing SFN
• if ENFD testing is normal, an alternative test of small nerve fiber function can be of diagnostic value
• The usefulness of QST and QSART limited by the fact that they are not readily available to most clinicians
• QSART can be affected by a number of medications
1Lacomis D., Muscle & Nerve 20022Devigili et al. Brain 2008

Other Work-Up?

Condition Test
Diabetes, impaired glucose tolerance Fasting glucose, oral glucose tolerance test or fasting insulin
Vitamin B abnormalities Vitamin B1, B6, B12, methylmalonic acid, homocysteine
Kidney, liver disease Complete metabolic profile
Thyroid dysfunction TSH, T4
Autoimmune Disorders CRP, ANA, SSA, SSB
Sarcoidosis Angiotensin converting enzyme (ACE) level
Paraprotein, amyloidosis Serum immune fixation electrophoresis
Celiac disease Gliadin antibodies, tissue transglutaminase
Infectious Hepatitis C, HIV
Inherited
Familial amyloid TTR gene sequencing
Sodium channel mutations SCN9A, SCN10A gene sequencing
Fabry’s disease Alpha-galactosidase assay or gene sequencing
Immune-mediated Elevated CSF protein, anti-nerve antibodies, paraneoplastic antibodies

Management of SFN
• Symptomatic treatment• Tend to be harder to treat than mixed fiber neuropathies• Non length-dependent respond less well than length-dependent
• Treat underlying cause• At least half are “idiopathic”• Unclear what percent are immune-mediated
• 921 pts with SFN• Idiopathic: 53%• Immune mediated: 3%• Sarcoidosis• Sjogren's• Celiac • “Other”
• Nonspecific immune lab: 16%2018

• 55 patients diagnosed with SFN• 27% had an autoimmune connective tissue disorder (SS, SLE, RA, vasculitis)• 20% had an organ specific autoimmune disease (Hashimoto’s, IBD, Graves)• 80% had positive serology (ANA, ESR, SSA, SSB, low complement)
• 74% were deemed “improved” by their physician
Potential Indicators of an Immune-Mediated SFN• Associated with a diagnosed autoimmune disease• Sjogren’s, SLE, etc
• Sudden onset• Albumincytologic dissociation (increased CSF protein, normal WBC)• Standard antibodies • ANA, etc
• Anti-neural antibodies• “Paraneoplastic” antibody panel• IgM to Fibroblast Growth Factor-3 (FGFR-3)• IgG to Trisulfated Heparin Disaccharide (TS-HDS)

2020
• 155 patients with biopsy confirmed SFN• 48% positive for antibody
• 37% TS-HDS• 15% FGFR-3
• 322 pts with suspected SFN• 45% positive for antibody
• 28% TS-HDS• 17% FGFR-3
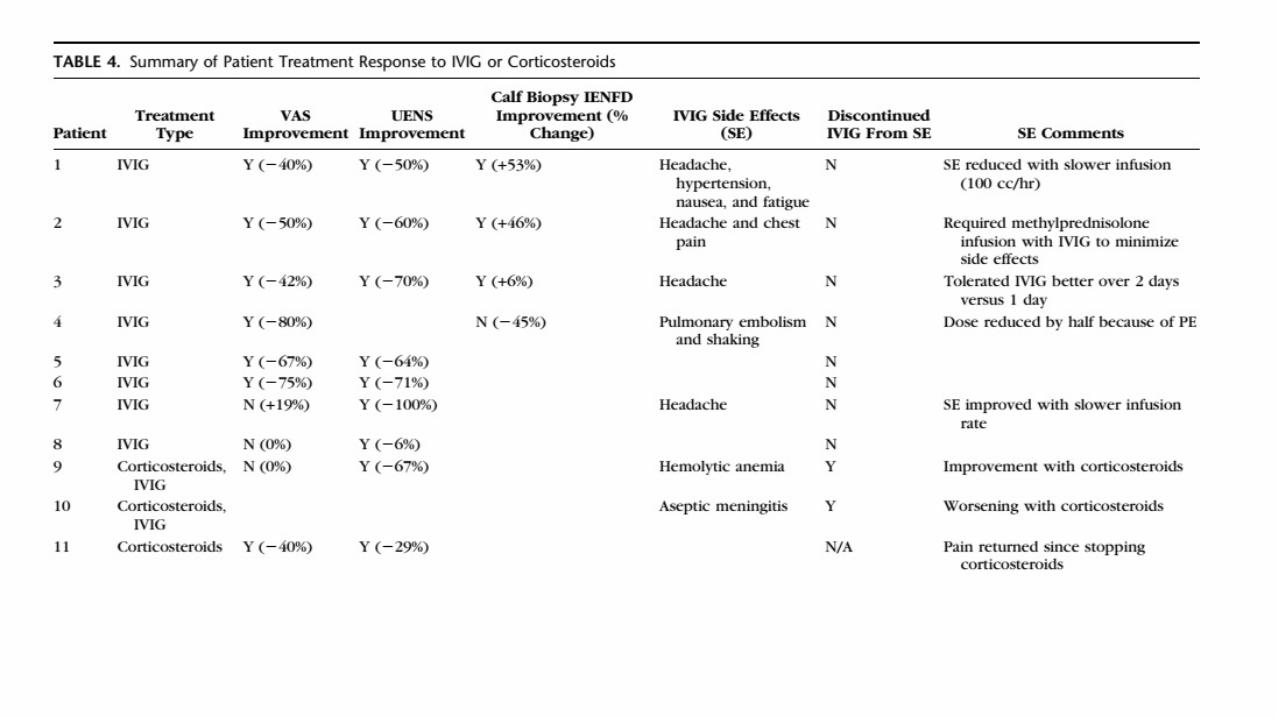
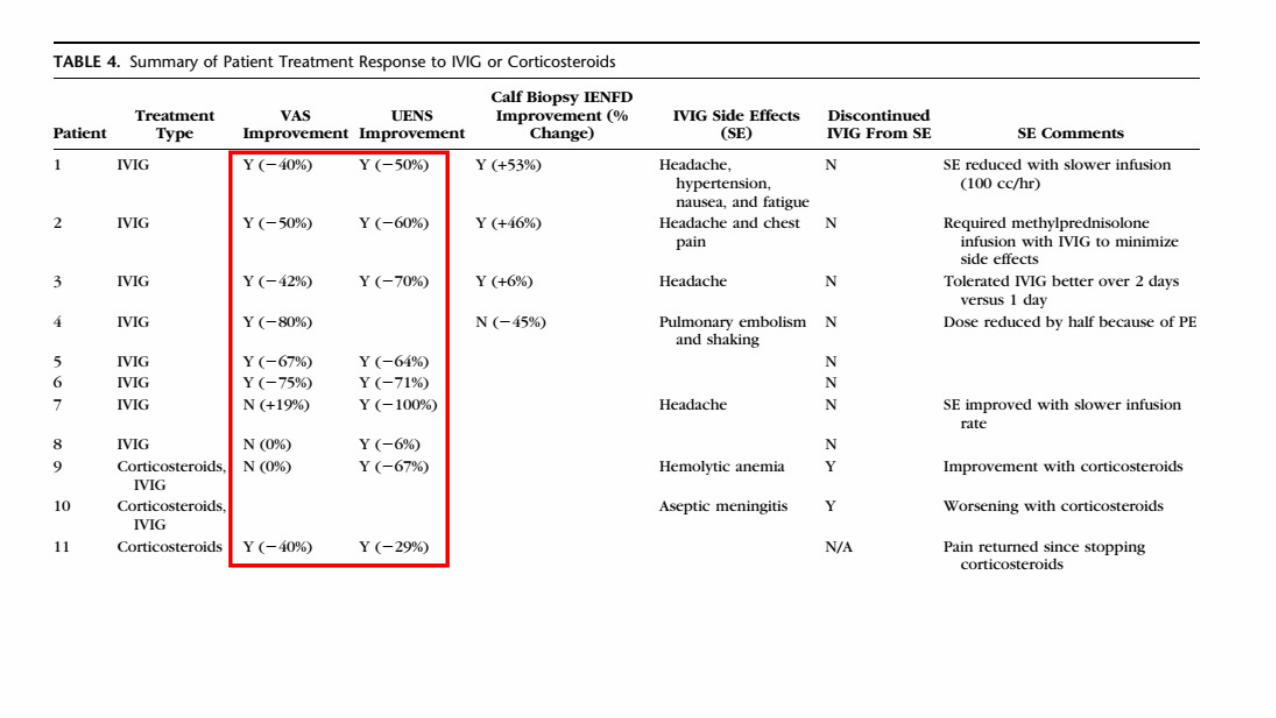
• 40 cases SFN, retrospective• 55% TS-HDS or FGFR-3• 77% TS-HDS
• 8 pts treated with IVIG improved


What is Natural History of ENFD?
JAMA Neurology 2016
• 52 patients• 25 idiopathic SFN• 13 IGT• 14 DM
• Repeat biopsies after > 12 m• ENFD never improved
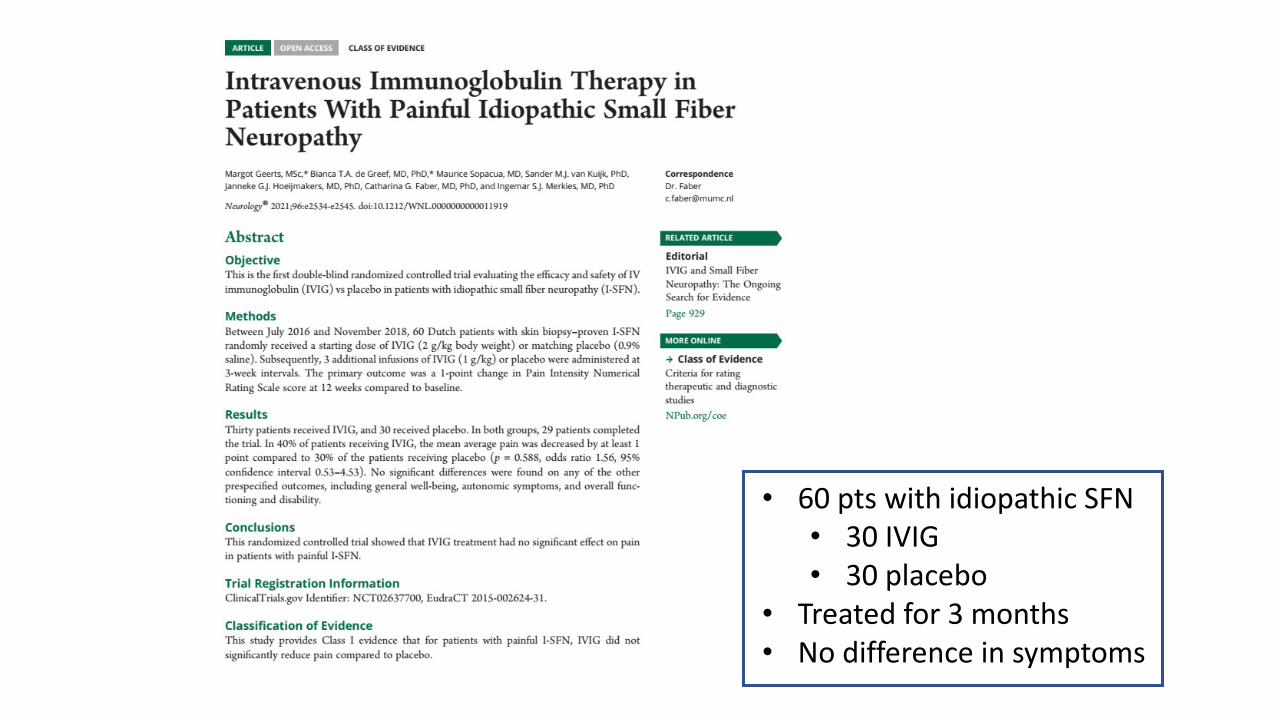
• 60 pts with idiopathic SFN• 30 IVIG• 30 placebo
• Treated for 3 months• No difference in symptoms

Why IVIG?
• Familiar to Neurologists• Effective treatment for certain immune-mediated neuropathies• Tends to show improvement quickly• Relatively safe and well-tolerated

Why not IVIG?
• Cost• Risk• Unproven efficacy• Hard to get insurance to cover

Peripheral Neuropathy and EDS/HSD
• Common• History, exam, and NCS/EMG will sort out most cases• Majority of neuropathy in EDS/HSD appears to be small fiber

SFN and EDS/HSD
• Very common• Cause not known
• Is it related to EDS/HSD, or POTS, or MCAS, or autoimmune, or other?• All (or some) of the above?
• Role of IVIG treatment in SFN?• Very reasonable in pts who also have an apparent autoimmune disorder• Role of more widespread use unclear; further research needed
• Role of other immune-modulating medications?• Unknown• Needs more study